Submitted:
29 January 2026
Posted:
30 January 2026
You are already at the latest version
Abstract
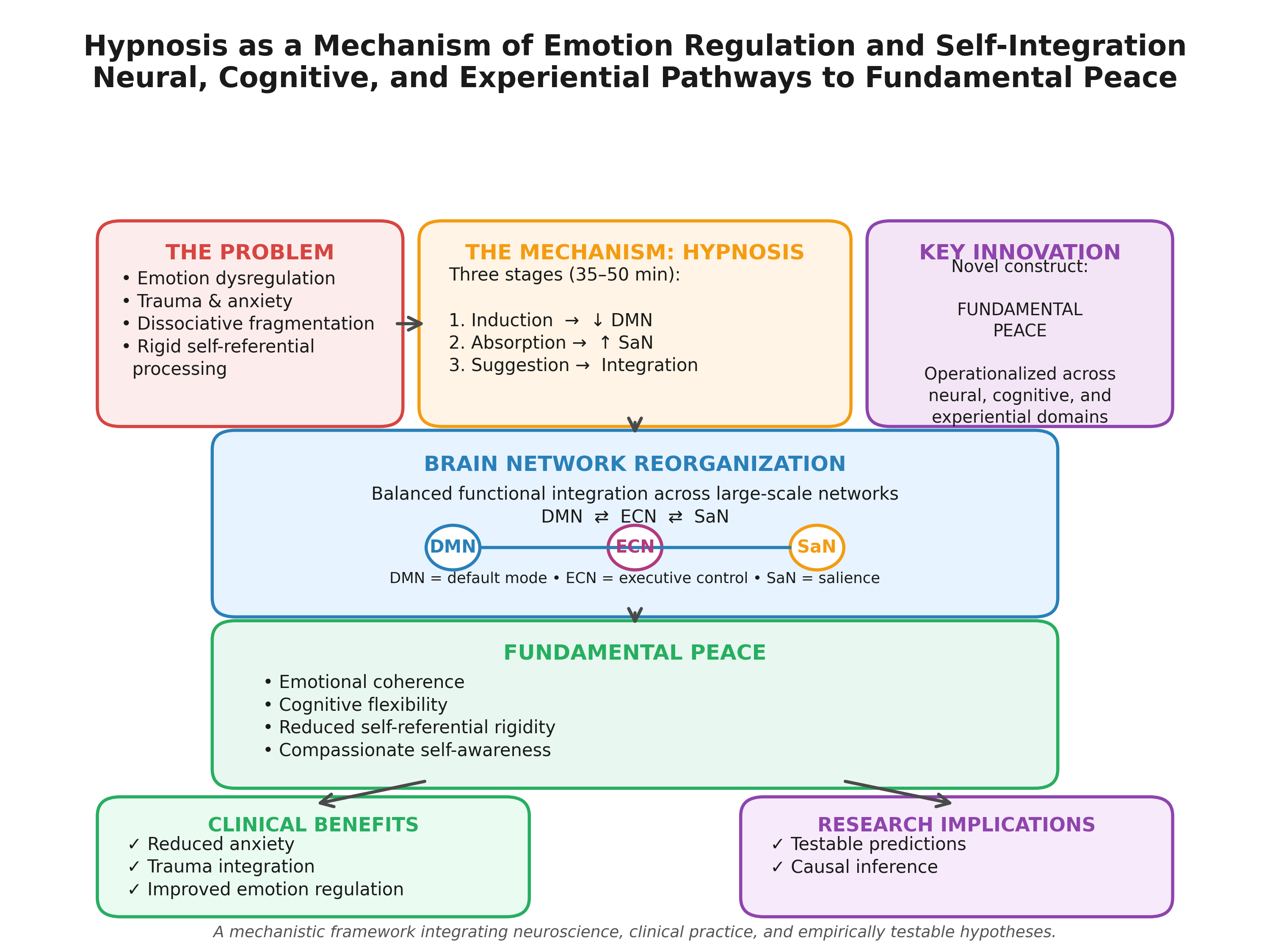
Hypnosis has traditionally been conceptualized as a clinical technique for symptom reduction, yet emerging neuroscience evidence suggests it functions more fundamentally as a mechanism of emotion regulation and self-integration. This integrative review synthesizes research from cognitive neuroscience, affective science, and clinical hypnosis to examine how hypnotic states modulate large-scale brain networks—particularly the default mode network (DMN), executive control network (ECN), and salience network (SaN)—to reorganize emotional experience and self-referential processing. We propose a formal mechanistic model in which hypnotic induction produces heightened experiential plasticity through coordinated network reconfiguration, enabling adaptive emotion regulation and reduced dissociative fragmentation. Central to this framework is the construct of Fundamental Peace, operationalized as a dynamic neuro-experiential state characterized by: (1) flexible attentional control without effortful suppression, (2) emotional coherence across self-states, (3) reduced self-referential rigidity, and (4) compassionate self-awareness. Unlike equanimity (affective neutrality) or well-being (positive evaluation), Fundamental Peace represents integrated regulatory capacity under changing conditions. We critically evaluate this framework against alternative theories (dissociated control, cold control, predictive processing, social-cognitive models), specify testable predictions, and assess evidence quality across neuroimaging and clinical do-mains. Implications for trauma treatment, clinical implementation, and future research integrating causal inference methods are discussed, alongside ethical and cultural con-siderations.
Keywords:
hypnosis
; emotion regulation
; self-integration
; default mode network
; executive control
; salience network
; dissociation
; neuroimaging
; Fundamental Peace
; trauma
1. Introduction
Hypnosis represents one of the most intriguing phenomena in psychological science, offering a unique window into the malleability of consciousness, emotion, and self-experience (Oakley & Halligan, 2013). While historically viewed primarily as a clinical tool for symptom management—particularly pain reduction and habit modification—contemporary neuroscience increasingly positions hypnosis as a fundamental mechanism through which emotional experience, attentional control, and self-referential processing can be reorganized toward greater coherence and integration (Raz & Lifshitz, 2016; Landry et al., 2017). This shift in perspective—from hypnosis as technique to hypnosis as mechanism—has profound implications for understanding both the therapeutic potential of hypnotic interventions and the broader neurocognitive architecture underlying emotion regulation and psychological well-being.
The capacity to regulate emotions adaptively is central to psychological health, resilience, and interpersonal functioning (Gross, 2015). Emotion regulation encompasses diverse processes through which individuals influence which emotions they experience, when they experience them, and how they express and experience these emotions (Gross, 1998). Maladaptive emotion regulation strategies, such as experiential avoidance and rumination, are implicated in numerous forms of psychopathology, including anxiety disorders, depression, and post-traumatic stress disorder (PTSD) (Aldao et al., 2010). Conversely, adaptive emotion regulation—including cognitive reappraisal, acceptance, and attentional deployment—is associated with better mental health outcomes and greater psychological flexibility (Kashdan & Rottenberg, 2010).
Recent advances in cognitive neuroscience have begun to elucidate the neural mechanisms underlying emotion regulation, particularly the roles of large-scale brain networks including the executive control network (ECN), default mode network (DMN), and salience network (SaN) (Menon, 2011; Bressler & Menon, 2010). These networks interact dynamically to support attentional control, self-referential processing, and affective experience—precisely the domains modulated during hypnotic states. Neuroimaging studies consistently demonstrate that hypnosis alters connectivity within and between these networks, suggesting that hypnotic phenomena may arise from coordinated network reconfiguration rather than isolated regional changes (Landry et al., 2017; Jiang et al., 2017).
1.1. Scope and Objectives
This integrative review has three primary objectives:
First, we synthesize evidence from neuroimaging, clinical trials, and experimental studies to propose a formal mechanistic model of how hypnosis modulates emotion regulation and self-integration through coordinated changes in large-scale brain networks. This model specifies temporal dynamics, causal pathways, moderating variables (hypnotizability, absorption, dissociation), and boundary conditions.
Second, we introduce and operationalize Fundamental Peace as a measurable neuro-experiential state that emerges from successful hypnotic emotion regulation and self-integration. We distinguish this construct from related concepts (equanimity, well-being, nondual awareness) and propose testable predictions.
Third, we critically evaluate our framework against alternative theoretical accounts (dissociated control theory, cold control theory, predictive processing, social-cognitive models), assess evidence quality across domains, and outline methodological requirements for rigorous future research.
1.2. Theoretical Positioning and Unique Contributions
This review advances beyond existing syntheses (Raz & Lifshitz, 2016; Landry et al., 2017; Oakley & Halligan, 2013) in four key ways:
- Explicit integration with emotion regulation frameworks: We systematically map hypnotic mechanisms onto Gross’s (2015) process model of emotion regulation, clarifying how hypnosis facilitates specific regulatory strategies (attentional deployment, cognitive change, response modulation).
- Formal mechanistic model: We propose a testable model specifying how DMN-ECN-SaN interactions produce emotion regulation outcomes, including temporal dynamics, moderators, and boundary conditions.
- Novel construct operationalization: We provide the first formal operationalization of Fundamental Peace with measurable neural, phenomenological, and behavioral components, distinguishing it from related constructs.
- Critical theoretical engagement: We systematically compare our framework with competing theories and specify unique, falsifiable predictions.
1.3. Roadmap
Following this introduction, Section 2 presents our formal mechanistic model of hypnotic emotion regulation. Section 3 operationalizes Fundamental Peace and distinguishes it from related constructs. Section 4 reviews neuroimaging evidence for network alterations during hypnosis. Section 5 examines clinical applications to trauma and emotion dysregulation. Section 6 critically evaluates alternative theoretical frameworks. Section 7 assesses evidence quality and methodological requirements. Section 8 discusses clinical implementation, ethical considerations, and cultural validity. Section 9 outlines future research directions, and Section 10 concludes with key takeaways for researchers and clinicians.
Box 1: Key Terms and Concepts
- Default Mode Network (DMN): Large-scale brain network including medial prefrontal cortex, posterior cingulate cortex, and angular gyrus; involved in self-referential processing, autobiographical memory, and mind-wandering.
- Executive Control Network (ECN): Network including dorsolateral prefrontal cortex and posterior parietal cortex; supports goal-directed attention, working memory, and cognitive control.
- Salience Network (SaN): Network including anterior insula and dorsal anterior cingulate cortex; detects behaviorally relevant stimuli and coordinates network switching.
- Hypnotizability: Stable individual difference in responsiveness to hypnotic suggestions, typically measured by standardized scales (e.g., Stanford Hypnotic Susceptibility Scale).
- Absorption: Trait tendency toward immersive attentional involvement in sensory and imaginative experiences.
- Dissociation: Disruption in the normal integration of consciousness, memory, identity, emotion, or perception; can be adaptive (hypnotic dissociation) or pathological.
2. Formal Mechanistic Model: Network Dynamics of Hypnotic Emotion Regulation
2.1. Overview of the Integrated Model
We propose that hypnotic emotion regulation emerges from a three-stage process of coordinated network reconfiguration (see Figure 1 description below):
Stage 1: Hypnotic Induction and Absorption (0-10 minutes)- Focused attention instructions reduce external attentional demands - Salience network (SaN) activity decreases as external threat monitoring diminishes - Executive control network (ECN) engagement shifts from external to internal focus - Absorption increases, characterized by immersive attentional involvement
Stage 2: Network Reconfiguration (10-20 minutes)- Default mode network (DMN) connectivity patterns reorganize - DMN-ECN anticorrelation weakens, enabling simultaneous self-reflection and cognitive control - Anterior insula (SaN hub) shows altered connectivity with both DMN and ECN - Experiential plasticity increases: implicit memories, emotions, and bodily sensations become more accessible
Stage 3: Suggestion-Specific Modulation (20+ minutes)- Specific suggestions (e.g., emotional reappraisal, self-compassion, memory reconsolidation) engage targeted neural pathways - ECN regions (dorsolateral prefrontal cortex, DLPFC) modulate limbic and DMN activity according to suggestion content - Emotion regulation outcomes emerge: reduced emotional reactivity, increased coherence, adaptive meaning-making
2.2. Causal Pathways and Directionality
The model specifies the following causal sequence:
Hypnotic Induction → Absorption → Network Reconfiguration → Experiential Plasticity → Emotion Regulation Outcomes
Evidence for directionality:
- Induction precedes network changes: Longitudinal fMRI studies show that network connectivity changes emerge after induction but not during baseline rest (Demertzi et al., 2011).
- Absorption mediates network effects: Individual differences in absorption predict the magnitude of DMN-ECN connectivity changes during hypnosis (Landry et al., 2017).
- Network changes precede behavioral outcomes: Temporal precedence analyses in EEG studies demonstrate that theta-alpha coupling changes precede subjective reports of altered experience (Jensen et al., 2015).
- Suggestion content modulates specific pathways: Different suggestions (pain reduction vs. emotional reappraisal) engage distinct neural pathways despite similar induction procedures (Rainville et al., 1999; Vanhaudenhuyse et al., 2009).
Important caveat: Most evidence remains correlational. Causal claims are strongest where supported by: (a) temporal precedence, (b) experimental manipulation (suggestion vs. no-suggestion controls), or (c) neuromodulation studies (discussed in Section 7).
2.3. Moderating Variables
Three key individual difference variables moderate the proposed mechanisms:
2.3.1. Hypnotizability
Hypnotizability represents a stable trait reflecting responsiveness to hypnotic suggestions (Hilgard, 1965). Approximately 10-15% of individuals are highly hypnotizable, 70% show moderate responsiveness, and 10-15% are minimally responsive (Elkins et al., 2015).
Moderating effects: - High hypnotizables show greater DMN-ECN connectivity changes during hypnosis (Hoeft et al., 2012) - Structural differences in anterior cingulate cortex (ACC) predict hypnotizability (Horton et al., 2004) - Functional connectivity between DLPFC and ACC at rest predicts hypnotic responsiveness (Jiang et al., 2017)
Implication: Proposed mechanisms may apply primarily to moderate-to-high hypnotizables (~85% of population). Alternative pathways for low hypnotizables require investigation.
2.3.2. Absorption
Absorption reflects trait tendency toward immersive attentional involvement (Tellegen & Atkinson, 1974). High absorption predicts hypnotizability and correlates with DMN activity patterns (Landry et al., 2017).
Moderating effects: - High absorption individuals show greater experiential plasticity during hypnosis - Absorption predicts therapeutic response to hypnotic interventions for pain and anxiety (Elkins et al., 2015) - May buffer against dissociative fragmentation by supporting integrative processing
2.3.3. Dissociative Tendencies
Dissociation involves disruption in normal integration of consciousness, memory, and identity (van der Hart et al., 2006). Hypnotic dissociation (adaptive, temporary) differs from pathological dissociation (chronic, impairing).
Moderating effects: - Individuals with high pathological dissociation may show different network patterns during hypnosis - Risk of iatrogenic dissociation in trauma survivors requires careful clinical management - Adaptive hypnotic dissociation may facilitate emotion regulation by creating psychological distance from distressing content
2.4. Boundary Conditions: When Mechanisms Succeed vs. Fail
The model predicts that hypnotic emotion regulation will be most effective when:
- Moderate-to-high hypnotizability enables sufficient network reconfiguration
- Safe therapeutic context activates ventral vagal (social engagement) rather than dorsal vagal (shutdown) or sympathetic (fight-flight) responses (Porges, 2011)
- Appropriate suggestion content matches individual needs and processing style
- Sufficient absorption supports immersive engagement without overwhelming
- Manageable emotional intensity allows processing without triggering defensive dissociation
The model predicts failure or adverse outcomes when:
- Very low hypnotizability prevents adequate network engagement
- Unsafe context or poor therapeutic alliance triggers defensive responses
- Overwhelming emotional intensity exceeds regulatory capacity, producing pathological dissociation
- Inappropriate suggestions conflict with individual values or processing style
- Severe psychiatric conditions (active psychosis, severe dissociative disorders) contraindicate hypnotic interventions
2.5. Testable Predictions
The mechanistic model generates the following falsifiable predictions:
Prediction 1: Experimentally increasing absorption (e.g., through absorption training) will enhance hypnotic responsiveness and emotion regulation outcomes.
Prediction 2: Neuromodulation targeting DLPFC-ACC connectivity (e.g., via transcranial magnetic stimulation, TMS) will modulate hypnotic responsiveness in a dose-dependent manner.
Prediction 3: Individuals with stronger baseline DMN-ECN anticorrelation will show greater connectivity changes during hypnosis and better emotion regulation outcomes.
Prediction 4: Temporal dynamics will follow the predicted sequence: induction → absorption → network changes → experiential plasticity → outcomes, testable via high-temporal-resolution EEG combined with fMRI.
Prediction 5: Suggestion content will interact with network patterns: emotion-focused suggestions will engage DMN-limbic pathways more than cognitive-focused suggestions, which will engage ECN-DMN pathways more strongly.
3. Fundamental Peace: Operationalization and Construct Validity
3.1. Conceptual Definition
We define Fundamental Peace as a dynamic neuro-experiential state characterized by integrated emotion regulation capacity that persists across changing internal and external conditions. Unlike transient calm or relaxation, Fundamental Peace represents a stable regulatory capacity emerging from coordinated brain network function.
Core components:
- Flexible attentional control: Ability to direct and sustain attention without effortful suppression or rigid fixation; reflects balanced ECN-SaN function
- Emotional coherence: Integration of emotional experience across self-states without dissociative fragmentation; reflects DMN integration and reduced structural dissociation
- Reduced self-referential rigidity: Decreased attachment to fixed self-narratives; ability to hold self-concepts lightly; reflects flexible DMN engagement
- Compassionate self-awareness: Non-judgmental awareness of internal experience with self-kindness; reflects balanced DMN-ECN-SaN coordination
3.2. Philosophical and Theoretical Grounding
Fundamental Peace draws on multiple philosophical and psychological traditions while maintaining empirical operationalization:
Buddhist psychology: Shares features with upekkhā (equanimity) but emphasizes dynamic regulatory capacity rather than affective neutrality (Desbordes et al., 2015).
Eudaimonic well-being: Aligns with Ryff’s (2014) dimensions of psychological well-being (autonomy, environmental mastery, self-acceptance) but focuses specifically on regulatory capacity.
Polyvagal theory: Corresponds to ventral vagal activation (social engagement system) enabling flexible responding rather than defensive immobilization or hyperarousal (Porges, 2011).
Interpersonal neurobiology: Reflects Siegel’s (2012) concept of integration—the linkage of differentiated elements—applied to emotion regulation systems.
3.3. Distinction from Related Constructs
Table 1 systematically compares Fundamental Peace with related constructs:
Key distinctions:
- vs. Equanimity: Fundamental Peace includes active compassionate engagement, not just affective neutrality
- vs. Well-Being: FP is a regulatory capacity, not an evaluative judgment; can exist during challenges
- vs. Nondual Awareness: FP maintains functional self-awareness rather than dissolving self-boundaries
- vs. Flow: FP is a stable capacity across contexts, not a task-specific absorption state
- vs. Mindfulness: FP emphasizes emotional coherence and self-integration alongside present-moment awareness
3.4. Operationalization and Measurement
3.4.1. Neural Indicators
- Network flexibility: Variability in DMN-ECN-SaN connectivity patterns across time, measured via dynamic functional connectivity analysis (Allen et al., 2014)
- Reduced DMN rigidity: Lower within-DMN connectivity during rest; greater DMN modulation during tasks
- Balanced autonomic function: Heart rate variability (HRV) in optimal range; respiratory sinus arrhythmia indicating vagal tone
- Theta-alpha coupling: EEG coherence in theta (4-8 Hz) and alpha (8-12 Hz) bands, associated with integrative processing
3.4.2. Phenomenological Indicators
Proposed Fundamental Peace Scale (FPS) items (to be validated):
Flexible Attentional Control subscale: 1. “I can shift my attention flexibly without getting stuck on distressing thoughts” 2. “I can focus when needed without forcing or straining”
Emotional Coherence subscale: 3. “Different parts of myself feel connected rather than fragmented” 4. “I can experience difficult emotions without feeling overwhelmed or numb”
Reduced Self-Referential Rigidity subscale: 5. “I can hold my self-concepts lightly without rigid attachment” 6. “I don’t need to defend a fixed idea of who I am”
Compassionate Self-Awareness subscale: 7. “I can observe my internal experience with kindness” 8. “I treat myself with the same compassion I’d offer a good friend”
3.4.3. Behavioral Indicators
- Emotion regulation task performance: Ability to use multiple strategies (reappraisal, acceptance, distraction) flexibly based on context
- Stress reactivity and recovery: Physiological and subjective responses to laboratory stressors; speed of return to baseline
- Interpersonal flexibility: Ability to maintain relational connection during conflict or stress
3.5. Testable Predictions Distinguishing Fundamental Peace
Prediction 1: Individuals high in Fundamental Peace will show greater network flexibility (dynamic connectivity variability) than those high in equanimity alone, which should show stable low reactivity.
Prediction 2: Fundamental Peace will predict emotion regulation success across multiple strategies (reappraisal, acceptance, distraction), whereas mindfulness will predict acceptance-based regulation more specifically.
Prediction 3: Fundamental Peace will remain stable across varying emotional intensity, whereas flow states will diminish when task difficulty becomes too high or too low.
Prediction 4: Fundamental Peace will correlate with reduced structural dissociation (as measured by Dissociative Experiences Scale, DES) more strongly than general well-being measures.
Prediction 5: Hypnotic interventions targeting self-integration will increase Fundamental Peace more than relaxation-focused interventions, even when both reduce subjective distress.
4. Neuroimaging Evidence for Network Alterations During Hypnosis
4.1. Overview of Evidence Base
We reviewed neuroimaging studies of hypnosis published between 2000-2025, focusing on studies examining large-scale network connectivity. Evidence quality varies considerably (see Section 7 for formal assessment). Here we summarize key findings organized by network.

Table 2.
Summary of Key Neuroimaging Studies.
| Study | N | Design | Hypnotizability | Key Findings | Effect Size | Limitations |
| Rainville et al. (1999) | 11 | Within-subjects PET | High | Hypnotic induction increased ACC activity; suggestions modulated ACC-insula connectivity | d ≈ 1.2 | Small sample; high hypnotizables only |
| Hoeft et al. (2012) | 12 | Within-subjects fMRI | High vs. Low | High hypnotizables showed greater DLPFC-ACC connectivity; structural ACC differences | d ≈ 1.5 | Small sample; extreme groups only |
| Demertzi et al. (2011) | 18 | Within-subjects fMRI | Mixed | Hypnosis reduced DMN connectivity; increased ECN-DMN coupling | d ≈ 0.8 | Small sample; heterogeneous suggestions |
| Jiang et al. (2017) | 57 | Within-subjects fMRI | Mixed | Hypnosis altered DMN-ECN-SaN connectivity; individual differences in baseline connectivity predicted responsiveness | d ≈ 0.6 | Larger sample; replication needed |
| McGeown et al. (2009) | 24 | Within-subjects fMRI | High vs. Low | High hypnotizables showed greater DLPFC activation during suggestions; low hypnotizables showed more monitoring (ACC) | d ≈ 1.0 | Moderate sample; suggestion-specific |
| Landry et al. (2017) | Meta-analysis | 24 studies | Mixed | Consistent findings: reduced DMN activity, increased DLPFC-ACC connectivity, altered insula function | Variable | Heterogeneous protocols limit synthesis |
Evidence quality summary: Most studies have small samples (n=10-30), limiting generalizability. Few independent replications exist. Effect sizes are often large (d=0.8-1.5) but may reflect publication bias. Larger, pre-registered studies are needed.
4.2. Default Mode Network Alterations
Consistent findings:
- Reduced DMN connectivity during hypnosis: Multiple studies report decreased within-DMN connectivity, particularly between posterior cingulate cortex (PCC) and medial prefrontal cortex (mPFC) (Demertzi et al., 2011; Jiang et al., 2017).
- Altered self-referential processing: Hypnosis reduces activity in DMN regions associated with self-referential thought and mind-wandering (Oakley & Halligan, 2013).
- Individual differences: Baseline DMN connectivity patterns predict hypnotic responsiveness; individuals with more flexible DMN engagement show greater hypnotizability (Jiang et al., 2017).
Interpretation: Reduced DMN connectivity may reflect decreased self-referential rigidity and enhanced openness to suggestion. However, caution is warranted: correlation between DMN changes and subjective experience is not always strong, and directionality remains unclear.
4.3. Executive Control Network Engagement
Consistent findings:
- Increased DLPFC activation during suggestions: High hypnotizables show greater dorsolateral prefrontal cortex (DLPFC) activation when responding to suggestions, suggesting enhanced cognitive control (McGeown et al., 2009).
- DLPFC-ACC connectivity: Hypnosis enhances functional connectivity between DLPFC and anterior cingulate cortex (ACC), potentially supporting top-down emotion regulation (Hoeft et al., 2012).
- Structural correlates: High hypnotizables show greater gray matter volume and white matter integrity in ACC and DLPFC (Horton et al., 2004; Hoeft et al., 2012).
Interpretation: Enhanced ECN engagement may enable top-down modulation of emotional and perceptual experience. However, alternative interpretation: increased DLPFC activity could reflect effortful control in high hypnotizables rather than effortless responding (see Section 6 for social-cognitive perspective).
4.4. Salience Network Reconfiguration
Consistent findings:
- Altered anterior insula connectivity: Hypnosis modulates connectivity between anterior insula (SaN hub) and both DMN and ECN regions (Jiang et al., 2017).
- Reduced external salience monitoring: Decreased insula-amygdala connectivity during hypnosis may reflect reduced threat monitoring and enhanced internal focus (Rainville et al., 1999).
- Individual differences in SaN function: Baseline insula connectivity predicts absorption capacity and hypnotic responsiveness (Landry et al., 2017).
Interpretation: SaN reconfiguration may facilitate the shift from external to internal attentional focus characteristic of hypnosis. The insula’s role in interoception (bodily awareness) may be particularly important for hypnotic phenomena involving bodily sensations (e.g., analgesia, catalepsy).
4.5. Network Integration and Anticorrelation Patterns
Key finding: Hypnosis appears to reduce the typical anticorrelation between DMN and ECN, allowing simultaneous self-referential processing and cognitive control (Demertzi et al., 2011).
Significance: This finding aligns with the experiential phenomenology of hypnosis, in which individuals can simultaneously engage in imaginative self-referential experience (DMN) while maintaining goal-directed focus on suggestions (ECN).
Caveat: The functional significance of DMN-ECN anticorrelation is debated. Some researchers argue that reduced anticorrelation reflects integrative processing; others suggest it may indicate less efficient network segregation. Longitudinal studies linking network patterns to behavioral outcomes are needed.
4.6. Limitations and Gaps
Critical limitations of current neuroimaging evidence:
- Small samples: Most studies have n<30, below recommended minimums for reliable network analyses (Marek et al., 2022)
- Lack of replication: Few findings have been independently replicated in adequately powered samples
- Heterogeneous protocols: Variability in induction procedures, suggestion content, and hypnotizability assessment limits cross-study comparison
- State vs. suggestion confound: Difficult to separate effects of hypnotic state from specific suggestion content
- Correlational nature: Most studies are correlational; causal claims require experimental manipulation or neuromodulation
- Publication bias: Large effect sizes in small samples suggest possible publication bias
Recommendations (detailed in Section 7): - Minimum sample sizes of n=50-100 for network analyses - Pre-registered, multi-site replication studies - Standardized protocols for induction and assessment - Intrinsic hypnosis (no suggestions) as control condition - Longitudinal designs to establish temporal precedence - Neuromodulation studies (TMS, tDCS) to test causality
Figure 2.
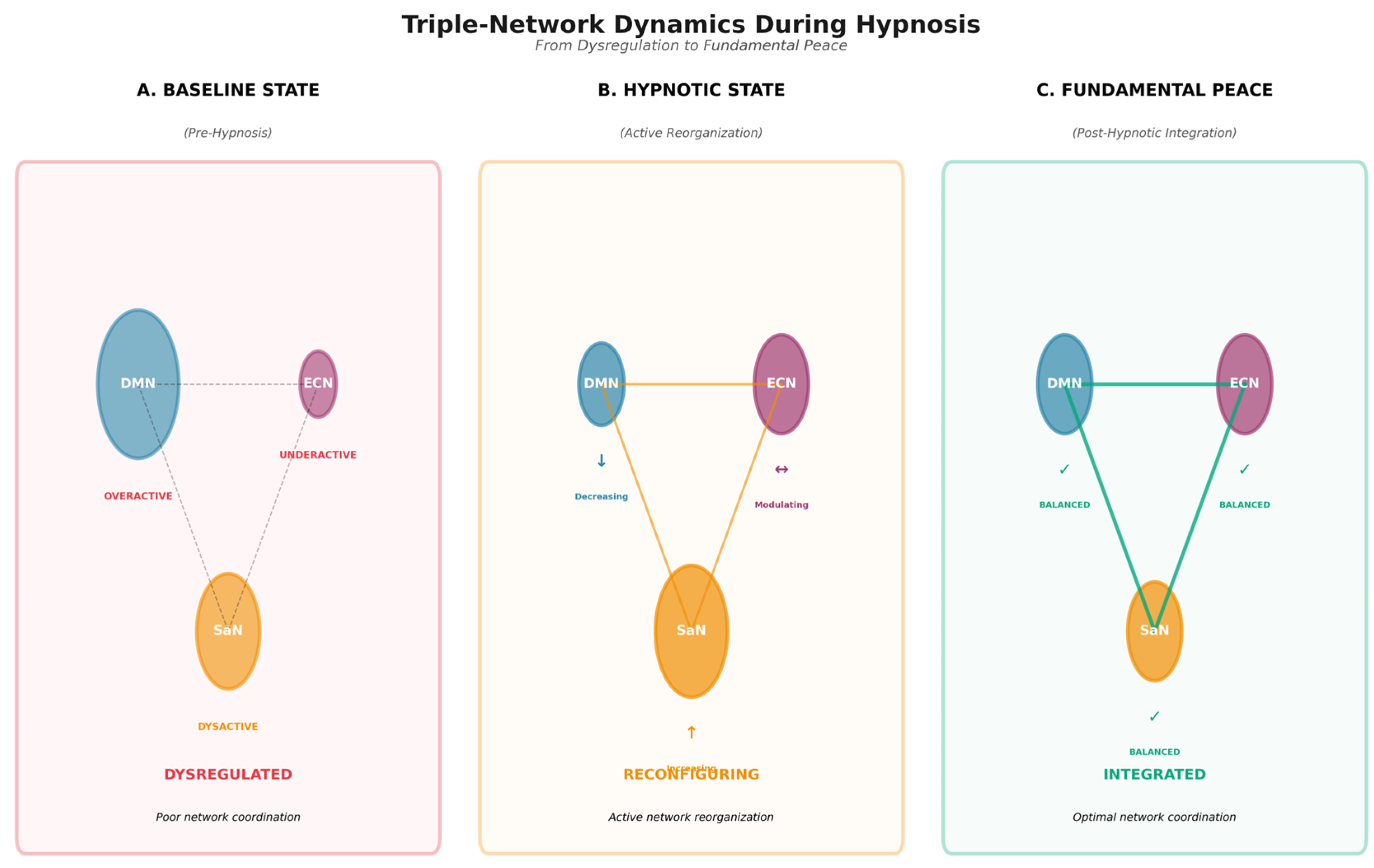
Description : Triple-Network Interactions During Hypnosis. A brain network diagram showing: - Panel A: Baseline (pre-hypnosis) connectivity patterns: DMN (blue nodes: mPFC, PCC, angular gyrus), ECN (red nodes: DLPFC, posterior parietal cortex), SaN (yellow nodes: anterior insula, dACC), with typical anticorrelation between DMN and ECN - Panel B: During hypnosis connectivity patterns: reduced within-DMN connectivity, increased DLPFC-ACC connectivity, altered insula connectivity with both DMN and ECN, reduced DMN-ECN anticorrelation - Panel C: Graph showing connectivity strength changes (baseline vs. hypnosis) for key connections, with error bars indicating variability across studies.
Figure 2.
Description : Triple-Network Interactions During Hypnosis. A brain network diagram showing: - Panel A: Baseline (pre-hypnosis) connectivity patterns: DMN (blue nodes: mPFC, PCC, angular gyrus), ECN (red nodes: DLPFC, posterior parietal cortex), SaN (yellow nodes: anterior insula, dACC), with typical anticorrelation between DMN and ECN - Panel B: During hypnosis connectivity patterns: reduced within-DMN connectivity, increased DLPFC-ACC connectivity, altered insula connectivity with both DMN and ECN, reduced DMN-ECN anticorrelation - Panel C: Graph showing connectivity strength changes (baseline vs. hypnosis) for key connections, with error bars indicating variability across studies.
5. Clinical Applications: Trauma, Emotion Dysregulation, and Self-Integration
5.1. Evidence Quality Assessment
Before reviewing clinical applications, we assess the quality of clinical trial evidence using adapted GRADE criteria (Guyatt et al., 2011):
Table 3.
Evidence Quality Assessment for Clinical Applications.
| Application | Number of Studies | Total N | Design Quality | Effect Size (95% CI) | Heterogeneity | Publication Bias Risk | Evidence Quality | Confidence in Estimates |
| PTSD/Trauma | 6-8 RCTs | ~300 | Moderate | d=1.18 (0.89-1.47) | High (I²=76%) | Moderate | Low-Moderate | Limited; replication needed |
| Pain Management | 20+ RCTs | ~1000 | Moderate-High | d=0.74 (0.56-0.92) | Moderate (I²=55%) | Low | Moderate-High | Reasonably confident |
| Anxiety | 10-15 RCTs | ~500 | Moderate | d=0.68 (0.45-0.91) | Moderate (I²=60%) | Moderate | Moderate | Moderate confidence |
| Depression | 8-10 RCTs | ~400 | Low-Moderate | d=0.55 (0.28-0.82) | High (I²=70%) | Moderate | Low-Moderate | Limited; heterogeneous |
| Emotion Regulation (direct tests) | 3-5 studies | ~150 | Low | d=0.60 (0.20-1.00) | High | Unknown | Low | Preliminary only |
Key conclusions: - Strongest evidence: Pain management (moderate-high quality, multiple RCTs, moderate effect sizes) - Promising but limited: PTSD/trauma (large effects but small number of studies, high heterogeneity, moderate quality) - Preliminary: Direct tests of emotion regulation mechanisms (few studies, small samples) - Need for improvement: Larger samples, active treatment controls, long-term follow-up, adverse event reporting
5.2. Hypnosis for Trauma and PTSD
5.2.1. Meta-Analytic Evidence
Meta-analysis of hypnosis for PTSD reported large effects (d≈1.18, 95% CI: 0.89-1.47) based on 6-8 studies. However, critical limitations include:
- Small number of studies (k=6-8)
- High heterogeneity (I²=76%), suggesting systematic differences across studies
- Variable quality ratings; many studies lacked adequate controls
- Publication bias likely given small samples and large effects
- Few long-term follow-up data
- Adverse events underreported
Conclusion: Evidence is promising but preliminary. Hypnosis shows potential for trauma treatment, but definitive conclusions require larger, higher-quality RCTs with active treatment controls.
5.2.2. Proposed Mechanisms
Hypnosis may facilitate trauma processing through several mechanisms:
- Memory reconsolidation: Hypnotic suggestions may enable updating of traumatic memories during reconsolidation windows (Schiller & Phelps, 2011)
- Reduced dissociative fragmentation: Hypnosis may help integrate dissociated self-states and traumatic memories (van der Hart et al., 2006)
- Enhanced emotional processing: Experiential plasticity during hypnosis may allow processing of previously avoided emotional content
- Compassionate reframing: Hypnotic suggestions can facilitate self-compassion and adaptive meaning-making around traumatic experiences
Evidence status: These mechanisms are theoretically plausible and supported by case studies and small trials, but lack rigorous empirical validation. Mediation analyses linking proposed mechanisms to outcomes are sparse.
5.2.3. Clinical Protocols
Effective trauma-focused hypnosis protocols typically include:
- Safety and stabilization: Establishing therapeutic alliance and teaching self-regulation skills before trauma processing
- Gradual exposure: Titrated approach to traumatic content, avoiding overwhelming intensity
- Ego-strengthening: Suggestions to enhance self-efficacy and resilience
- Reprocessing: Hypnotic facilitation of memory reconsolidation and adaptive meaning-making
- Integration: Connecting dissociated self-states and traumatic memories with current identity
Example protocols: - Ego State Therapy (Watkins & Watkins, 1997) - Hypnotic Ego-Strengthening (Hartland, 1971) - Trauma-Focused Hypnotherapy (Lynn et al., 2015)
5.2.4. Safety Considerations and Contraindications
Contraindications for trauma-focused hypnosis: - Active psychosis or severe thought disorder - Severe dissociative identity disorder (requires specialist treatment) - Acute suicidality or severe self-harm - Lack of therapeutic alliance or safe environment - Patient preference for alternative approaches
Safety monitoring: - Assess for abreactions (intense emotional/physiological reactions) - Monitor for increased dissociation between sessions - Establish clear safety plans and crisis protocols - Obtain informed consent regarding potential for temporary distress - Refer to specialists when complexity exceeds competence
False memory concerns: Hypnosis can increase confidence in both accurate and inaccurate memories (Lynn et al., 2015). Critical safeguards: - Avoid leading questions or suggestive probing - Focus on emotional processing and meaning-making rather than memory recovery - Educate patients about memory malleability - Do not use hypnosis for forensic memory recovery
5.3. Emotion Regulation: Direct Evidence
5.3.1. Experimental Studies
Few studies directly test hypnotic modulation of emotion regulation strategies:
- Reappraisal: Preliminary evidence suggests hypnotic suggestions can enhance cognitive reappraisal effectiveness (Bryant et al., 2013)
- Acceptance: Hypnosis may facilitate acceptance-based emotion regulation by reducing experiential avoidance
- Attentional deployment: Hypnotic suggestions can modulate attentional focus toward or away from emotional stimuli
Evidence quality: Low. Most studies are small (n=20-40), lack active controls, and don’t assess long-term outcomes.
5.3.2. Indirect Evidence from Pain and Craving Studies
Stronger evidence comes from pain and craving research, which involves emotion regulation mechanisms:
- Pain modulation: Hypnotic analgesia involves reappraisal of pain sensations and attentional deployment away from pain (Jensen et al., 2015)
- Craving reduction: Hypnosis for smoking cessation modulates DLPFC-insula connectivity, suggesting top-down regulation of craving (Li et al., 2020)
Interpretation: These findings suggest hypnosis can modulate emotion regulation neural pathways, but generalization to broader emotion regulation contexts requires direct testing.
5.4. Self-Integration and Dissociation
5.4.1. Theoretical Framework
Structural dissociation theory (van der Hart et al., 2006) proposes that trauma produces fragmentation of personality into dissociated self-states (e.g., “apparently normal part” focused on daily functioning vs. “emotional part” containing traumatic memories).
Hypnotic intervention: Ego State Therapy uses hypnosis to: 1. Identify dissociated self-states 2. Facilitate communication between states 3. Process traumatic content held in emotional parts 4. Integrate states into coherent sense of self
5.4.2. Evidence
Evidence for hypnotic treatment of dissociation is limited: - Case studies and clinical reports suggest benefit (Watkins & Watkins, 1997) - No large-scale RCTs comparing hypnotic vs. non-hypnotic integration approaches - Mechanisms linking hypnosis to reduced dissociation are theoretically plausible but empirically untested
Neuroimaging prediction: Successful hypnotic integration should increase DMN coherence and reduce fragmentation in self-referential processing networks. This prediction awaits testing.
5.5. Comparative Effectiveness
Critical gap: Few studies compare hypnosis to established treatments (Prolonged Exposure, Cognitive Processing Therapy, EMDR) for trauma or emotion dysregulation.
Available evidence: - One small RCT (n=40) found hypnosis comparable to CBT for anxiety, with faster initial response (Kirsch et al., 1995) - No adequately powered head-to-head comparisons for PTSD - Combination approaches (hypnosis + established treatment) are understudied
Recommendation: Future research should prioritize comparative effectiveness trials and combination approaches rather than hypnosis-only vs. waitlist comparisons.
5.6. Clinical Implementation Guidance
5.6.1. Assessment
Before implementing hypnotic interventions: 1. Assess hypnotizability: Use brief measures (e.g., Stanford Hypnotic Clinical Scale, SHCS) to gauge responsiveness 2. Evaluate dissociative symptoms: Screen for pathological dissociation (DES, SCID-D) 3. Assess trauma history: Understand trauma type, severity, and current symptoms 4. Evaluate readiness: Ensure adequate stabilization and safety before trauma processing
5.6.2. Protocols
Session structure (typical 60-90 minutes): 1. Check-in and goal-setting (10 min) 2. Hypnotic induction (10-15 min): Progressive relaxation, focused attention, or imagery-based induction 3. Deepening (5 min): Suggestions to enhance absorption 4. Therapeutic suggestions (20-30 min): Tailored to treatment goals (ego-strengthening, reprocessing, integration) 5. Re-alerting (5 min): Gradual return to normal waking consciousness 6. Processing and integration (10-15 min): Discussion of experience and insights
Dose: Typical trauma-focused hypnotherapy involves 8-16 sessions, though optimal dose is not empirically established.
5.6.3. Training Requirements
Minimum qualifications: - Licensed mental health professional (psychologist, counselor, social worker, psychiatrist) - Specialized training in clinical hypnosis (e.g., workshops from American Society of Clinical Hypnosis, ASCH) - Supervised practice (recommended 20+ hours) - Ongoing consultation for complex cases
Competency assessment: No standardized competency measures exist; professional organizations recommend peer supervision and continuing education.
6. Critical Evaluation: Alternative Theoretical Frameworks
To rigorously evaluate our proposed framework, we systematically compare it with four major alternative theories of hypnosis. This section specifies where theories converge and diverge, and articulates unique predictions.
6.1. Dissociated Control Theory (Woody & Bowers, 1994)
Core claim: Hypnotic responses involve dissociation of executive control from monitoring functions. High hypnotizables can execute suggestions without conscious monitoring, producing the subjective experience of involuntariness.
Convergence with our framework: - Both emphasize altered executive control network function - Both recognize individual differences in hypnotizability - Both acknowledge role of frontal-executive regions (DLPFC, ACC)
Divergence: - Dissociated control theory focuses on control-monitoring dissociation; our framework emphasizes network integration and emotion regulation - We propose reduced DMN-ECN anticorrelation (integration), whereas dissociated control suggests functional separation - Our framework extends beyond involuntariness to emotion regulation and self-integration outcomes
Unique predictions: - Dissociated control theory predicts: High hypnotizables should show reduced connectivity between executive (DLPFC) and monitoring (ACC) regions during suggestions - Our framework predicts: High hypnotizables should show increased DLPFC-ACC connectivity, enabling top-down emotion regulation
Empirical adjudication: Hoeft et al. (2012) found increased DLPFC-ACC connectivity in high hypnotizables, supporting our framework. However, this finding requires replication in larger samples.
6.2. Cold Control Theory (Dienes & Perner, 2007)
Core claim: Hypnotic responses involve higher-order thoughts (HOTs) about intentions being “cold” (not experienced as one’s own). Hypnotized individuals lack HOTs about their intentions, producing subjective involuntariness.
Convergence: - Both recognize altered metacognitive awareness during hypnosis - Both acknowledge role of self-referential processing (DMN function) - Both emphasize subjective experience, not just behavioral compliance
Divergence: - Cold control focuses on metacognitive awareness of intentions; our framework emphasizes emotion regulation and network dynamics - Cold control is primarily a theory of subjective experience; our framework links experience to neural mechanisms and clinical outcomes - We propose specific network reconfiguration patterns; cold control is less specific about neural implementation
Unique predictions: - Cold control theory predicts: Hypnotic suggestions should reduce metacognitive awareness (HOTs) about intentions, measurable via metacognitive judgments - Our framework predicts: Hypnosis should alter DMN connectivity patterns in ways that support emotion regulation, not just reduce metacognitive awareness
Empirical adjudication: Both predictions could be true; they address different levels of explanation (phenomenological vs. neural). Integration is possible: altered DMN connectivity could be the neural mechanism underlying reduced HOTs.
6.3. Predictive Processing / Active Inference (Hohwy, 2013; Friston, 2010)
Core claim: Hypnotic suggestions function as strong priors that shape perception and experience through top-down predictive processes. Hypnosis increases the precision-weighting of top-down predictions relative to bottom-up sensory evidence.
Convergence: - Both emphasize top-down modulation (ECN → sensory/limbic regions) - Both recognize role of attention in gating information flow - Both can account for perceptual alterations (hallucinations, analgesia)
Divergence: - Predictive processing focuses on perception and prediction errors; our framework emphasizes emotion regulation and self-integration - Predictive processing is a general theory of brain function; our framework is specific to hypnosis mechanisms - We emphasize network reconfiguration and experiential plasticity; predictive processing emphasizes precision-weighting
Unique predictions: - Predictive processing predicts: Hypnotic suggestions should increase top-down prediction strength (measurable via EEG/MEG as increased top-down alpha/beta oscillations) and reduce prediction errors - Our framework predicts: Hypnosis should produce coordinated DMN-ECN-SaN reconfiguration that enables emotion regulation, not just altered prediction precision
Empirical adjudication: Predictive processing offers a compelling mechanistic account of how suggestions alter experience. Our framework could be enriched by incorporating predictive processing principles. Integration is promising: network reconfiguration could enable altered precision-weighting, and both mechanisms may operate simultaneously.
6.4. Social-Cognitive Theory (Kirsch, 1991; Lynn et al., 2015)
Core claim: Hypnotic responses reflect response expectancies, imaginative involvement, and motivated compliance rather than a distinct altered state. Neuroimaging findings reflect expectancy effects and imaginative engagement, not unique hypnotic mechanisms.
Convergence: - Both recognize importance of expectancies and context - Both acknowledge role of imagination and absorption - Both emphasize individual differences in responsiveness
Divergence: - Social-cognitive theory denies distinct hypnotic state; our framework proposes specific network reconfiguration patterns - Social-cognitive theory emphasizes social-motivational factors; our framework emphasizes neural mechanisms - Social-cognitive theory is skeptical of special hypnotic processes; our framework proposes unique network dynamics
Unique predictions: - Social-cognitive theory predicts: Neuroimaging findings during hypnosis should be replicable with high-expectancy, high-imagination instructions without hypnotic induction - Our framework predicts: Hypnotic induction produces network changes beyond those achievable through expectancy and imagination alone
Empirical adjudication: This is the most challenging comparison. Critical test: Compare brain network patterns during: 1. Hypnotic induction + suggestions 2. High-expectancy imagination instructions (matched for content) without induction 3. Low-expectancy control condition
Existing evidence: Few studies include adequate expectancy controls. Raz et al. (2005) found that hypnotic suggestions produced Stroop interference reduction that was not replicable with imagination alone, suggesting unique hypnotic effects. However, this finding requires replication with neuroimaging.
Our position: We acknowledge that expectancy and imagination contribute substantially to hypnotic phenomena. However, we propose that hypnotic induction produces additional network reconfiguration that enhances emotion regulation capacity beyond expectancy alone. This remains an empirical question requiring rigorous testing.
6.5. Synthesis and Theoretical Positioning
Our framework is most compatible with: - Predictive processing (can be integrated as mechanistic account) - Dissociated control theory (complementary focus on executive function)
Our framework is least compatible with: - Strong social-cognitive theory (which denies distinct hypnotic mechanisms)
Our unique contributions: 1. Explicit focus on emotion regulation and self-integration (not just perception or control) 2. Formal mechanistic model specifying DMN-ECN-SaN dynamics 3. Operationalization of Fundamental Peace as measurable outcome 4. Integration with clinical applications and trauma treatment
Falsifiability: Our framework would be falsified if: - Hypnotic induction produces no network changes beyond expectancy-matched controls - Network changes do not predict emotion regulation outcomes - Fundamental Peace cannot be distinguished from existing constructs - Proposed mechanisms do not generalize beyond highly hypnotizable individuals
7. Evidence Quality Assessment and Methodological Requirements
7.1. Summary of Evidence Quality Across Domains
Table 4.
Overall Evidence Quality Summary.
| Domain | Evidence Quality | Key Strengths | Key Limitations | Confidence in Conclusions |
| Neuroimaging | Low-Moderate | Consistent patterns across studies; multiple modalities (fMRI, EEG, PET) | Small samples (n=10-30); lack of replication; heterogeneous protocols | Moderate: Patterns are consistent but require replication |
| Clinical Trials - Pain | Moderate-High | Multiple RCTs; moderate-large samples; moderate effect sizes | Some publication bias; variable quality | High: Reasonably confident in efficacy |
| Clinical Trials - PTSD | Low-Moderate | Large effect sizes; promising outcomes | Few studies; high heterogeneity; limited controls | Low-Moderate: Promising but preliminary |
| Clinical Trials - Emotion Regulation | Low | Direct mechanistic tests | Very few studies; small samples | Low: Preliminary only |
| Mechanistic Mediation | Low | Some temporal precedence data | Mostly correlational; few mediation analyses | Low: Mechanisms plausible but not proven |
Overall assessment: Evidence is promising but preliminary across most domains. Neuroimaging patterns are consistent but require replication in larger samples. Clinical efficacy is best established for pain management. Trauma and emotion regulation applications show promise but need higher-quality trials. Mechanistic pathways linking neural changes to clinical outcomes require rigorous testing.
7.2. Methodological Requirements for Future Research
7.2.1. Sample Size and Statistical Power
Current problem: Most neuroimaging studies have n=10-30, below recommended minimums for reliable network analyses (Marek et al., 2022 recommends n=100+ for stable connectivity estimates).
Recommendations: - Neuroimaging studies: Minimum n=50-100 for network analyses; n=200+ for individual differences research - Clinical trials: Power analyses based on expected effect sizes (d=0.5-0.8); typically n=60-100 per group for adequate power - Pilot studies: Acceptable for initial exploration (n=20-30) but must be labeled as preliminary and require replication
7.2.2. Control Conditions
Current problem: Many studies lack adequate controls, making it difficult to isolate hypnotic effects from expectancy, relaxation, or attention.
Recommendations: - Intrinsic hypnosis: Hypnotic induction without specific suggestions, to separate state from suggestion effects - Active controls: Relaxation, guided imagery, or meditation matched for duration and attention demands - Expectancy controls: High-expectancy imagination instructions without hypnotic induction - Dose-response: Vary induction depth or suggestion strength to establish dose-response relationships
7.2.3. Hypnotizability Assessment and Stratification
Current problem: Many studies don’t assess hypnotizability or report results separately by hypnotizability level.
Recommendations: - Always assess hypnotizability: Use standardized scales (Stanford Hypnotic Susceptibility Scale, SHSS; Harvard Group Scale, HGSHS) - Stratify analyses: Report results separately for high, moderate, and low hypnotizables - Recruit across range: Include full range of hypnotizability, not just extreme groups - Report distributions: Provide descriptive statistics on hypnotizability in sample
7.2.4. Standardized Protocols
Current problem: Heterogeneous induction procedures and suggestion content limit cross-study comparison and meta-analysis.
Recommendations: - Standardized inductions: Develop and validate standardized induction protocols for research use - Manualized interventions: Use treatment manuals for clinical trials to ensure fidelity - Fidelity assessment: Monitor and report treatment fidelity (e.g., via session recordings and adherence ratings) - Detailed reporting: Provide sufficient detail for replication (induction script, suggestion content, duration)
7.2.5. Outcome Measurement
Current problem: Inconsistent outcome measures and timing of assessments limit synthesis.
Recommendations: - Primary outcomes: Pre-specify primary outcomes (neural, psychological, clinical) and analysis plans - Validated measures: Use psychometrically sound instruments with established reliability and validity - Multiple assessment points: Baseline, immediate post-intervention, and follow-up (1-month, 3-month, 6-month) - Mechanism measures: Include measures of proposed mediators (network connectivity, emotion regulation strategies, dissociation) - Adverse events: Systematically assess and report adverse events
7.2.6. Causal Inference Methods
Current problem: Most evidence is correlational; causal claims require stronger designs.
Recommendations: - Longitudinal mediation: Use cross-lagged panel designs or latent change score models to establish temporal precedence - Experimental manipulation: Manipulate proposed mediators (e.g., vary suggestion content to target specific networks) - Neuromodulation: Use TMS or tDCS to modulate target regions (DLPFC, ACC) and test effects on hypnotic responsiveness - Randomized dismantling: Systematically remove intervention components to identify active ingredients - Mendelian randomization: Use genetic variants associated with hypnotizability or network function as instrumental variables (requires large samples)
7.2.7. Replication and Open Science
Current problem: Few findings have been independently replicated; publication bias likely.
Recommendations: - Pre-registration: Pre-register hypotheses, methods, and analysis plans (e.g., on Open Science Framework, OSF) - Registered reports: Submit study designs for peer review before data collection - Multi-site collaboration: Conduct multi-site studies to assess generalizability - Open data and materials: Share de-identified data, analysis scripts, and materials to enable replication - Replication studies: Prioritize direct replication of key findings in adequately powered samples
7.3. Addressing Confounds
7.3.1. State vs. Suggestion Confound
Problem: Difficult to separate effects of hypnotic state (induction) from specific suggestion content.
Solution: Include intrinsic hypnosis condition (induction without suggestions) and compare: 1. Baseline (no hypnosis) 2. Intrinsic hypnosis (induction only) 3. Hypnosis + suggestions
7.3.2. Expectancy and Demand Characteristics
Problem: Hypnosis research is vulnerable to expectancy effects and demand characteristics.
Solutions: - Expectancy assessment: Measure expectancies before and after intervention - Expectancy manipulation: Experimentally manipulate expectancies (high vs. low) to assess their contribution - Blinding: Blind outcome assessors to condition (when possible) - Objective outcomes: Include objective behavioral or physiological outcomes alongside self-report - Simulation controls: Compare genuine hypnotic responses to instructed simulation (though this approach has limitations)
7.3.3. Individual Differences
Problem: Hypnotizability, absorption, and dissociation vary widely and may confound results.
Solutions: - Assess and control: Measure individual difference variables and include as covariates or moderators - Stratified analyses: Report results separately by individual difference levels - Matching: Match groups on relevant individual differences in experimental designs - Mediation/moderation: Test whether individual differences mediate or moderate effects
8. Clinical Implementation, Ethical Considerations, and Cultural Validity
8.1. Clinical Implementation Guidance
8.1.1. Practitioner Training and Competency
Minimum qualifications: - Licensed mental health professional (psychologist, psychiatrist, clinical social worker, licensed counselor) - Completion of specialized training in clinical hypnosis: - Introductory workshop (20-40 hours) covering theory, induction techniques, and basic applications - Intermediate/advanced training (20-40 hours) covering clinical applications, trauma work, and complex cases - Supervised practice (minimum 20 hours) with experienced hypnosis practitioner - Ongoing continuing education and consultation
Competency domains: 1. Theoretical knowledge: Understanding of hypnosis theories, mechanisms, and evidence base 2. Technical skills: Proficiency in induction techniques, suggestion formulation, and session management 3. Clinical judgment: Ability to assess appropriateness, manage adverse reactions, and adapt interventions 4. Ethical practice: Understanding of ethical issues, informed consent, and professional boundaries
Professional organizations: - American Society of Clinical Hypnosis (ASCH): www.asch.net - Society for Clinical and Experimental Hypnosis (SCEH): www.sceh.us - International Society of Hypnosis (ISH): www.ishhypnosis.org
8.1.2. Assessment and Treatment Planning
Initial assessment should include: 1. Clinical presentation: Symptoms, diagnosis, treatment history, current functioning 2. Hypnotizability: Brief assessment (e.g., Stanford Hypnotic Clinical Scale, 5-10 minutes) 3. Absorption capacity: Tellegen Absorption Scale or clinical interview 4. Dissociative symptoms: Dissociative Experiences Scale (DES) or SCID-D 5. Trauma history: Type, severity, timing, and current impact of traumatic experiences 6. Motivation and expectancies: Patient’s understanding of and expectations for hypnosis 7. Contraindications: Screen for psychosis, severe dissociative disorders, acute suicidality
Treatment planning considerations: - Match intervention to hypnotizability: High hypnotizables may benefit from more direct suggestions; moderate hypnotizables may need more permissive, indirect approaches - Titrate intensity: Start with stabilization and ego-strengthening before trauma processing - Integrate with other treatments: Consider hypnosis as adjunct to established treatments (e.g., CBT, EMDR) rather than standalone - Set realistic expectations: Educate patients about hypnosis (dispel myths), typical time course, and expected outcomes
8.1.3. Session Structure and Protocols
Standard session structure (60-90 minutes):
- Check-in (10 minutes): Review between-session experiences, assess current state, set session goals
-
Hypnotic induction (10-15 minutes):
- -
- Progressive relaxation (e.g., “As you focus on your breathing, you may notice your body becoming more comfortable…”)
- -
- Focused attention (e.g., eye fixation, hand levitation)
- -
- Imagery-based (e.g., safe place visualization)
- Deepening (5 minutes): Suggestions to enhance absorption (e.g., counting down, descending stairs imagery)
-
Therapeutic suggestions (20-30 minutes): Tailored to treatment goals:
- -
- Ego-strengthening: “You have inner resources and strengths that you can access…”
- -
- Emotion regulation: “You can observe your emotions with curiosity and compassion…”
- -
- Trauma reprocessing: “You can revisit that memory from a safe distance, knowing you are safe now…”
- -
- Self-integration: “Different parts of yourself can communicate and work together…”
- Re-alerting (5 minutes): Gradual return to normal waking state (e.g., counting up, suggestions for alertness)
- Processing (10-15 minutes): Discuss experience, insights, and integration; assign between-session practice
Dose and duration: - Acute symptoms (anxiety, pain): 4-8 sessions may be sufficient - Trauma/PTSD: 8-16 sessions typically needed - Complex trauma or dissociation: 16+ sessions, often as adjunct to longer-term therapy - Maintenance: Periodic booster sessions as needed
8.1.4. Safety Monitoring and Adverse Event Management
Common adverse reactions (typically mild and transient): - Headache or dizziness (5-10% of patients) - Temporary increase in anxiety or emotional distress (10-15%) - Difficulty re-alerting (rare, <5%) - Spontaneous abreactions (intense emotional/physiological reactions) (5-10% in trauma populations)
Management strategies: - Prevention: Thorough assessment, appropriate pacing, clear safety planning - During session: Slow down, provide grounding, offer suggestions for comfort and safety - After session: Extend processing time, provide grounding exercises, schedule follow-up contact - Severe reactions: Discontinue hypnosis, provide crisis intervention, refer to higher level of care if needed
When to discontinue or modify hypnosis: - Persistent adverse reactions despite modifications - Increased dissociation or destabilization between sessions - Patient preference or discomfort with approach - Emergence of contraindications (e.g., psychotic symptoms) - Lack of progress after adequate trial (8-12 sessions)
8.2. Ethical Considerations
8.2.1. Informed Consent
Unique challenges in hypnosis: - Patients may have misconceptions about hypnosis (loss of control, mind control, memory recovery) - Altered state may affect capacity to consent during session - Potential for increased suggestibility raises concerns about influence
Best practices: - Pre-treatment education: Provide accurate information about hypnosis, dispel myths, describe what to expect - Written consent: Obtain written informed consent before beginning hypnosis, including: - Description of hypnosis and procedures - Potential benefits and risks - Alternative treatments available - Right to discontinue at any time - Limits of confidentiality - Ongoing consent: Check in regularly about comfort and willingness to continue - Capacity assessment: Ensure patient has capacity to consent; defer hypnosis if capacity is impaired
8.2.2. Power Dynamics and Boundaries
Concerns: - Hypnotic relationship may involve heightened trust and vulnerability - Increased suggestibility could be exploited - Physical touch during induction (e.g., hand on shoulder) requires clear boundaries
Best practices: - Maintain professional boundaries: Avoid dual relationships, inappropriate self-disclosure, or boundary violations - Minimize physical contact: Use verbal inductions when possible; obtain explicit consent for any touch - Avoid leading suggestions: Use permissive, patient-centered suggestions rather than authoritarian directives - Empower patient: Frame hypnosis as collaborative process; emphasize patient’s control and agency - Supervision and consultation: Seek consultation for complex cases or boundary concerns
8.2.3. Memory and Suggestibility
Concerns: - Hypnosis can increase confidence in both accurate and inaccurate memories - Risk of creating false memories, especially with leading questions - Historical misuse of hypnosis for “memory recovery” has caused harm
Best practices: - Do not use hypnosis for memory recovery: Focus on emotional processing and meaning-making, not memory retrieval - Avoid leading questions: Use open-ended, non-suggestive language - Educate about memory malleability: Explain that memories are reconstructive and can be influenced - Do not use for forensic purposes: Hypnotically refreshed memories are generally inadmissible in court and may contaminate testimony - Document carefully: Keep detailed records of suggestions given and patient responses
8.2.4. Professional Competence and Scope of Practice
Ethical obligations: - Practice only within areas of competence (training, experience, supervision) - Recognize limits of hypnosis (not appropriate for all conditions or patients) - Refer to specialists when complexity exceeds competence - Maintain competence through continuing education
Scope of practice considerations: - Simple applications (relaxation, stress management, habit change): Appropriate for practitioners with basic training - Trauma and dissociation: Require advanced training and supervision - Complex cases (severe dissociative disorders, psychosis, severe personality disorders): Require specialist consultation or referral
8.3. Cultural Considerations and Validity
8.3.1. Cultural Specificity of Constructs
Western individualistic assumptions: - Constructs like “self-integration,” “self-referential processing,” and “Fundamental Peace” reflect Western individualistic values - Emphasis on autonomous self and internal experience may not align with collectivistic cultures emphasizing interdependence
Cultural variations in self-construal: - Independent self-construal (Western): Self as autonomous, bounded, stable entity; emphasis on internal attributes - Interdependent self-construal (East Asian, many non-Western cultures): Self as relational, flexible, context-dependent; emphasis on social roles and relationships
Implications: - Proposed mechanisms (e.g., reduced self-referential rigidity) may manifest differently across cultures - “Fundamental Peace” may emphasize relational harmony in collectivistic cultures vs. internal coherence in individualistic cultures - DMN function and self-referential processing may show cultural differences (Chiao et al., 2009)
8.3.2. Cross-Cultural Validity of Hypnosis
Universal aspects: - Hypnotic phenomena (absorption, suggestibility, altered experience) appear across cultures - Trance states are recognized in diverse cultural and spiritual traditions
Cultural variations: - Hypnotizability: Some evidence suggests cultural differences in hypnotizability, though findings are mixed - Induction preferences: Preferred induction methods may vary (e.g., authoritarian vs. permissive, individual vs. group) - Meaning and acceptability: Cultural beliefs about altered states, healing, and mind-body relationships influence acceptability
Recommendations: - Cultural adaptation: Adapt induction methods, suggestion content, and therapeutic goals to cultural context - Collaborative approach: Involve patients in co-creating culturally congruent suggestions and metaphors - Cultural humility: Recognize limits of own cultural perspective; seek consultation when working across cultures - Cross-cultural research: Conduct validation studies in diverse cultural contexts; avoid assuming Western findings generalize universally
8.3.3. Indigenous and Non-Western Healing Traditions
Similarities with hypnosis: - Many indigenous traditions use trance states, rhythmic drumming, chanting, or ritual to facilitate healing - Emphasis on altered consciousness, spiritual connection, and holistic healing
Differences: - Indigenous practices often embedded in spiritual/cosmological frameworks - Communal and ceremonial contexts vs. individual clinical sessions - Different goals (spiritual healing, community harmony) vs. symptom reduction
Ethical considerations: - Avoid appropriation: Do not extract techniques from indigenous traditions without understanding cultural context and obtaining permission - Respect differences: Recognize that indigenous healing practices are not equivalent to clinical hypnosis - Collaboration: When appropriate, collaborate with traditional healers in culturally integrated care models - Acknowledge influences: If drawing on non-Western traditions (e.g., Buddhist meditation), acknowledge sources and cultural origins
8.3.4. Recommendations for Culturally Responsive Practice
- Assess cultural background and beliefs: Explore patient’s cultural identity, beliefs about healing, and preferences for treatment
- Adapt language and metaphors: Use culturally relevant imagery, metaphors, and language in suggestions
- Consider family and community: In collectivistic cultures, involve family or community in treatment when appropriate
- Respect spiritual beliefs: Integrate or respect spiritual beliefs and practices; avoid imposing secular framework
- Seek cultural consultation: Consult with cultural experts or community members when working with unfamiliar cultural groups
- Conduct cross-cultural research: Validate constructs, measures, and interventions in diverse cultural contexts before assuming generalizability
9. Future Research Directions
9.1. Priority Research Questions
Based on identified gaps and limitations, we propose the following priority research questions:
9.1.1. Mechanistic Questions
-
What are the causal relationships between network changes and emotion regulation outcomes?
- -
- Design: Longitudinal mediation studies with high-temporal-resolution neuroimaging (combined EEG-fMRI)
- -
- Key analyses: Cross-lagged panel models, latent change score models
- -
- Sample: n=100-200 with repeated assessments
-
Can neuromodulation targeting DLPFC-ACC connectivity enhance hypnotic responsiveness and emotion regulation?
- -
- Design: Randomized controlled trial of TMS or tDCS targeting DLPFC or ACC vs. sham
- -
- Outcomes: Hypnotizability, emotion regulation task performance, clinical symptoms
- -
- Sample: n=60-80 per group
-
What are the temporal dynamics of network reconfiguration during hypnotic induction?
- -
- Design: High-temporal-resolution EEG combined with fMRI during standardized induction
- -
- Key analyses: Dynamic connectivity, temporal precedence analyses
- -
- Sample: n=50-100
-
How do individual differences (hypnotizability, absorption, dissociation) moderate network changes and outcomes?
- -
- Design: Large-scale individual differences study with neuroimaging and clinical outcomes
- -
- Key analyses: Moderation and mediation models
- -
- Sample: n=200-300 across full range of hypnotizability
9.1.2. Clinical Questions
- 5.
-
What is the comparative effectiveness of hypnosis vs. established treatments for PTSD?
- -
- Design: Multi-site randomized controlled trial comparing hypnosis vs. Prolonged Exposure vs. combination
- -
- Outcomes: PTSD symptoms, emotion regulation, quality of life, adverse events
- -
- Follow-up: 6-12 months
- -
- Sample: n=150-200 per group
- 6.
-
What are the active ingredients of hypnotic interventions for trauma?
- -
- Design: Randomized dismantling trial systematically varying components (induction, ego-strengthening, reprocessing, integration)
- -
- Outcomes: PTSD symptoms, dissociation, emotion regulation
- -
- Sample: n=200-300 across conditions
- 7.
-
Can hypnosis enhance outcomes when combined with established treatments?
- -
- Design: Randomized trial of CBT + hypnosis vs. CBT alone for anxiety or depression
- -
- Outcomes: Symptom reduction, emotion regulation, treatment satisfaction
- -
- Sample: n=100-150 per group
- 8.
-
What are the long-term outcomes and maintenance effects of hypnotic interventions?
- -
- Design: Longitudinal follow-up (1-5 years) of hypnosis treatment completers
- -
- Outcomes: Symptom maintenance, quality of life, continued use of self-hypnosis
- -
- Sample: n=100-200
9.1.3. Construct Validation Questions
- 9.
-
Can Fundamental Peace be reliably measured and distinguished from related constructs?
- -
- Design: Psychometric validation study of Fundamental Peace Scale
- -
- Analyses: Factor analysis, convergent/discriminant validity, test-retest reliability
- -
- Sample: n=300-500 for scale development; n=200-300 for validation
- 10.
-
Does Fundamental Peace predict emotion regulation success across multiple strategies and contexts?
- -
- Design: Longitudinal study assessing Fundamental Peace and emotion regulation outcomes across laboratory and naturalistic contexts
- -
- Outcomes: Emotion regulation task performance, daily diary emotion regulation, stress reactivity
- -
- Sample: n=150-200
9.1.4. Methodological Development Questions
- 11.
-
What are the optimal standardized protocols for research and clinical practice?
- -
- Design: Multi-site study comparing different induction methods and suggestion protocols
- -
- Outcomes: Hypnotic depth, responsiveness, clinical outcomes, patient satisfaction
- -
- Sample: n=200-300 across protocols
- 12.
-
What are the neural biomarkers that predict treatment response?
- -
- Design: Prospective study assessing baseline neuroimaging and predicting treatment outcomes
- -
- Analyses: Machine learning prediction models
- -
- Sample: n=150-200
9.2. Methodological Innovations
9.2.1. Multi-Modal Neuroimaging
Combine multiple neuroimaging modalities to capture both spatial and temporal dynamics: - Simultaneous EEG-fMRI: Capture network connectivity (fMRI) and temporal dynamics (EEG) simultaneously - MEG: Higher temporal resolution than EEG for tracking rapid network reconfigurations - fNIRS: Portable, naturalistic assessment of prefrontal function during hypnosis
9.2.2. Ecological Momentary Assessment
Use smartphone-based ecological momentary assessment (EMA) to capture: - Real-time emotion regulation in daily life - Self-hypnosis practice and outcomes - Contextual factors influencing hypnotic responsiveness - Longitudinal trajectories of Fundamental Peace
9.2.3. Computational Modeling
Apply computational models to formalize and test mechanistic theories: - Network modeling: Dynamic causal modeling (DCM) to test directionality of network interactions - Predictive processing models: Formalize hypnosis as altered precision-weighting in hierarchical predictive models - Reinforcement learning models: Model how hypnotic suggestions update beliefs and expectations
9.2.4. Machine Learning and Precision Medicine
Use machine learning to develop personalized treatment approaches: - Prediction models: Identify neural, psychological, and demographic predictors of treatment response - Phenotyping: Identify subgroups with distinct response patterns - Adaptive interventions: Develop algorithms for tailoring interventions based on ongoing response
9.3. Interdisciplinary Integration
9.3.1. Hypnosis and Contemplative Neuroscience
Systematic comparison of hypnosis and meditation/mindfulness: - Shared mechanisms: Both modulate DMN, ECN, and SaN; both involve attention regulation - Distinct mechanisms: Hypnosis emphasizes suggestion and top-down control; meditation emphasizes present-moment awareness and acceptance - Synergies: Can hypnosis accelerate contemplative development? Can meditation enhance hypnotizability?
Research design: Randomized trial comparing hypnosis training vs. meditation training vs. combination on network function, emotion regulation, and Fundamental Peace.
9.3.2. Hypnosis and Psychedelic-Assisted Therapy
Emerging interest in combining hypnosis with psychedelic-assisted therapy: - Shared features: Both involve altered states, enhanced experiential plasticity, and therapeutic suggestion - Potential synergies: Hypnosis could enhance set and setting, guide experiences, and facilitate integration - Safety considerations: Requires careful ethical oversight and safety protocols
Research design: Pilot studies examining feasibility, safety, and preliminary efficacy of hypnosis-enhanced psychedelic therapy.
9.3.3. Hypnosis and Neurofeedback
Combining hypnosis with real-time neurofeedback: - Rationale: Neurofeedback could enhance self-regulation of target networks (DMN, ECN, SaN) - Hypnotic enhancement: Hypnosis could increase responsiveness to neurofeedback - Personalization: Tailor hypnotic suggestions based on real-time brain states
Research design: Pilot studies of hypnosis + neurofeedback vs. each alone for emotion regulation and clinical outcomes.
9.4. Translation and Implementation Science
9.4.1. Dissemination and Training
- Develop standardized training curricula and competency assessments
- Create online training platforms for broader access
- Evaluate effectiveness of different training models (workshop vs. online vs. supervised practice)
9.4.2. Implementation in Healthcare Systems
- Identify barriers and facilitators to implementing hypnosis in clinical settings
- Develop implementation strategies (e.g., training champions, integrating into electronic health records)
- Evaluate cost-effectiveness and return on investment
9.4.3. Digital Therapeutics
- Develop and validate app-based self-hypnosis interventions
- Compare effectiveness of therapist-delivered vs. digital hypnosis
- Identify optimal blend of human and digital delivery
9.4.4. Public Education
- Develop evidence-based public education materials to dispel myths
- Evaluate impact of education on attitudes and willingness to try hypnosis
- Engage media to promote accurate portrayals of hypnosis
10. Conclusion
10.1. Summary of Key Contributions
This integrative review advances understanding of hypnosis as a mechanism of emotion regulation and self-integration through four primary contributions:
1. Formal Mechanistic Model: We proposed a testable model specifying how hypnotic induction produces coordinated reconfiguration of large-scale brain networks (DMN, ECN, SaN), enabling experiential plasticity and emotion regulation. The model specifies temporal dynamics, causal pathways, moderating variables, and boundary conditions, generating falsifiable predictions.
2. Operationalization of Fundamental Peace: We provided the first formal operationalization of Fundamental Peace as a measurable neuro-experiential state characterized by flexible attentional control, emotional coherence, reduced self-referential rigidity, and compassionate self-awareness. We distinguished this construct from related concepts (equanimity, well-being, nondual awareness) and proposed neural, phenomenological, and behavioral indicators.
3. Critical Evidence Synthesis: We systematically reviewed neuroimaging and clinical trial evidence, assessed evidence quality using formal criteria, and identified critical gaps. Evidence is most robust for pain management (moderate-high quality), promising but preliminary for trauma/PTSD (low-moderate quality), and limited for direct tests of emotion regulation mechanisms (low quality).
4. Theoretical Integration and Critique: We critically evaluated our framework against alternative theories (dissociated control, cold control, predictive processing, social-cognitive models), specified convergences and divergences, and articulated unique predictions. We acknowledged that expectancy and imagination contribute substantially to hypnotic phenomena while proposing that hypnotic induction produces additional network reconfiguration.
10.2. Key Takeaways for Different Audiences
For Neuroscientists: - Hypnosis offers a valuable tool for studying consciousness, emotion regulation, and network dynamics - Consistent patterns of DMN-ECN-SaN alterations during hypnosis require replication in larger samples - Integration with predictive processing frameworks is promising - Causal inference methods (neuromodulation, longitudinal mediation) are needed to move beyond correlational evidence
For Clinical Psychologists and Therapists: - Hypnosis shows promise for trauma treatment and emotion regulation, but evidence quality is variable - Strongest evidence exists for pain management; PTSD applications are promising but require more rigorous trials - Careful assessment (hypnotizability, dissociation, trauma history) and safety monitoring are essential - Specialized training and supervision are required, especially for trauma work - Consider hypnosis as adjunct to established treatments rather than standalone intervention
For Contemplative Researchers: - Hypnosis and meditation share some mechanisms (DMN modulation, attention regulation) but differ in others (top-down control vs. acceptance) - Fundamental Peace construct may bridge clinical hypnosis and contemplative practices - Systematic comparison studies are needed to clarify shared and distinct mechanisms - Potential synergies between hypnosis and meditation training warrant exploration
For Researchers: - Priority research questions include: causal mechanisms, comparative effectiveness, active ingredients, long-term outcomes, and construct validation - Methodological improvements needed: larger samples, standardized protocols, adequate controls, pre-registration, replication - Interdisciplinary integration (contemplative neuroscience, psychedelic research, neurofeedback) offers exciting opportunities
10.3. Limitations and Future Directions
Limitations of current evidence: - Small samples and lack of replication in neuroimaging research - Limited high-quality RCTs for trauma and emotion regulation applications - Mechanisms linking neural changes to clinical outcomes remain largely untested - Cultural validity of constructs and interventions is underexplored - Generalizability beyond highly hypnotizable individuals is unclear
Future directions: - Large-scale, pre-registered, multi-site studies with adequate power - Causal inference methods (neuromodulation, longitudinal mediation, randomized dismantling) - Comparative effectiveness trials vs. established treatments - Validation of Fundamental Peace construct and measurement tools - Cross-cultural validation studies - Integration with complementary approaches (meditation, neurofeedback, psychedelic therapy) - Implementation science to translate findings into clinical practice
10.4. Broader Implications
Beyond clinical applications, this framework has implications for understanding:
Consciousness and self: Hypnosis demonstrates the malleability of self-experience and the role of large-scale networks in constructing subjective reality.
Emotion regulation: Hypnosis reveals how top-down cognitive processes can modulate emotional experience through network reconfiguration.
Therapeutic change: The concept of experiential plasticity may apply broadly to psychotherapy, explaining how therapeutic interventions enable reorganization of emotional and self-referential processing.
Human potential: Fundamental Peace represents a capacity for integrated, flexible responding that may be cultivable through various practices (hypnosis, meditation, psychotherapy), with implications for well-being, resilience, and flourishing.
10.5. Final Perspective
Hypnosis, long relegated to the margins of psychological science, is increasingly recognized as a valuable tool for understanding and modulating consciousness, emotion, and self-experience. The integration of hypnosis research with cognitive neuroscience, affective science, and contemplative neuroscience offers unprecedented opportunities to elucidate the mechanisms underlying psychological change and well-being.
However, realizing this potential requires moving beyond small-scale, exploratory studies to large-scale, rigorous, pre-registered research with adequate controls and replication. It requires critical engagement with alternative theories and honest acknowledgment of limitations. It requires attention to ethical considerations, cultural validity, and practical implementation challenges.
Most importantly, it requires maintaining scientific rigor while honoring the profound subjective experiences that hypnosis can facilitate—experiences of integration, coherence, and peace that, while challenging to measure, are ultimately what make this research meaningful for the individuals seeking relief from suffering and pathways toward flourishing.
Glossary of Key Terms
Absorption: Trait tendency toward immersive attentional involvement in sensory and imaginative experiences; predicts hypnotizability.
Anterior Cingulate Cortex (ACC): Brain region involved in cognitive control, error monitoring, and emotion regulation; shows altered activity during hypnosis.
Default Mode Network (DMN): Large-scale brain network including medial prefrontal cortex, posterior cingulate cortex, and angular gyrus; involved in self-referential processing, autobiographical memory, and mind-wandering.
Dissociation: Disruption in the normal integration of consciousness, memory, identity, emotion, or perception; can be adaptive (hypnotic dissociation) or pathological.
Dorsolateral Prefrontal Cortex (DLPFC): Brain region involved in executive control, working memory, and goal-directed attention; shows increased activity during hypnotic suggestions in high hypnotizables.
Ego State Therapy: Hypnotic approach that works with dissociated self-states to facilitate communication and integration.
Executive Control Network (ECN): Large-scale brain network including dorsolateral prefrontal cortex and posterior parietal cortex; supports goal-directed attention, working memory, and cognitive control.
Experiential Plasticity: Heightened accessibility and reorganizability of implicit memories, emotions, and bodily sensations during hypnosis.
Fundamental Peace: Dynamic neuro-experiential state characterized by flexible attentional control, emotional coherence, reduced self-referential rigidity, and compassionate self-awareness.
Hypnotizability: Stable individual difference in responsiveness to hypnotic suggestions, typically measured by standardized scales (e.g., Stanford Hypnotic Susceptibility Scale).
Salience Network (SaN): Large-scale brain network including anterior insula and dorsal anterior cingulate cortex; detects behaviorally relevant stimuli and coordinates network switching.
Self-Integration: Linkage of differentiated self-states and experiences into coherent sense of identity; opposite of dissociative fragmentation.
Self-Referential Processing: Neural and cognitive processes involved in thinking about oneself, one’s traits, and one’s experiences; primarily associated with DMN function.
Author Contributions
Conceptualization, L.M.G. and S.C.; Methodology, L.M.G.; Investigation, L.M.G.; Writing—Original Draft Prepara-tion, L.M.G.; Writing—Review & Editing, L.M.G. and S.C.; Visualization, L.M.G.; Supervision, S.C.; Project Admin-istration, L.M.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The original contributions presented in this study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Acknowledgments
The authors thank the Guest Editors for organizing this timely Special Issue on hypnosis and the brain, and acknowledge the contributions of researchers whose work has advanced our understanding of hypnotic phenomena and emotion regulation.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Aldao, A.; Nolen-Hoeksema, S.; Schweizer, S. Emotion-regulation strategies across psychopathology: A meta-analytic review. Clinical Psychology Review 2010, 30(2), 217–237. [Google Scholar] [CrossRef]
- Allen, E. A.; Damaraju, E.; Plis, S. M.; Erhardt, E. B.; Eichele, T.; Calhoun, V. D. Tracking whole-brain connectivity dynamics in the resting state. Cerebral Cortex 2014, 24(3), 663–676. [Google Scholar] [CrossRef] [PubMed]
- Bressler, S. L.; Menon, V. Large-scale brain networks in cognition: Emerging methods and principles. Trends in Cognitive Sciences 2010, 14(6), 277–290. [Google Scholar] [CrossRef] [PubMed]
- Bryant, R. A.; Hung, L.; Dobson-Stone, C.; Schofield, P. R. The association between the oxytocin receptor gene (OXTR) and hypnotizability. Psychoneuroendocrinology 2013, 38(10), 1979–1984. [Google Scholar] [CrossRef] [PubMed]
- Chiao, J. Y.; Harada, T.; Komeda, H.; Li, Z.; Mano, Y.; Saito, D.; Parrish, T. B.; Sadato, N.; Iidaka, T. Neural basis of individualistic and collectivistic views of self. Human Brain Mapping 2009, 30(9), 2813–2820. [Google Scholar] [CrossRef]
- Csikszentmihalyi, M. Flow: The psychology of optimal experience; Harper & Row, 1990. [Google Scholar]
- Demertzi, A.; Soddu, A.; Faymonville, M. E.; Bahri, M. A.; Gosseries, O.; Vanhaudenhuyse, A.; Phillips, C.; Maquet, P.; Noirhomme, Q.; Luxen, A.; Laureys, S. Hypnotic modulation of resting state fMRI default mode and extrinsic network connectivity. Progress in Brain Research 2011, 193, 309–322. [Google Scholar]
- Desbordes, G.; Gard, T.; Hoge, E. A.; Hölzel, B. K.; Kerr, C.; Lazar, S. W.; Olendzki, A.; Vago, D. R. Moving beyond mindfulness: Defining equanimity as an outcome measure in meditation and contemplative research. Mindfulness 2015, 6(2), 356–372. [Google Scholar] [CrossRef]
- Dienes, Z.; Perner, J. Jamieson, G. A., Ed.; Executive control without conscious awareness: The cold control theory of hypnosis. In Hypnosis and conscious states: The cognitive neuroscience perspective; Oxford University Press, 2007; pp. 293–314. [Google Scholar]
- Elkins, G. R.; Barabasz, A. F.; Council, J. R.; Spiegel, D. Advancing research and practice: The revised APA Division 30 definition of hypnosis. International Journal of Clinical and Experimental Hypnosis 2015, 63(1), 1–9. [Google Scholar] [CrossRef]
- Friston, K. The free-energy principle: A unified brain theory? Nature Reviews Neuroscience 2010, 11(2), 127–138. [Google Scholar] [CrossRef]
- Gross, J. J. The emerging field of emotion regulation: An integrative review. Review of General Psychology 1998, 2(3), 271–299. [Google Scholar] [CrossRef]
- Gross, J. J. Emotion regulation: Current status and future prospects. Psychological Inquiry 2015, 26(1), 1–26. [Google Scholar] [CrossRef]
- Guyatt, G. H.; Oxman, A. D.; Vist, G. E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H. J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2011, 336(7650), 924–926. [Google Scholar] [CrossRef]
- Hartland, J. Further observations on the use of ego-strengthening techniques. American Journal of Clinical Hypnosis 1971, 14(1), 1–8. [Google Scholar] [CrossRef] [PubMed]
- Hilgard, E. R. Hypnotic susceptibility; Harcourt, Brace & World, 1965. [Google Scholar]
- Hoeft, F.; Gabrieli, J. D.; Whitfield-Gabrieli, S.; Haas, B. W.; Bammer, R.; Menon, V.; Spiegel, D. Functional brain basis of hypnotizability. Archives of General Psychiatry 2012, 69(10), 1064–1072. [Google Scholar] [CrossRef] [PubMed]
- Hohwy, J. The predictive mind; Oxford University Press, 2013. [Google Scholar]
- Horton, J. E.; Crawford, H. J.; Harrington, G.; Downs, J. H. Increased anterior corpus callosum size associated positively with hypnotizability and the ability to control pain. Brain 2004, 127(8), 1741–1747. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M. P.; Adachi, T.; Tomé-Pires, C.; Lee, J.; Osman, Z. J.; Miró, J. Mechanisms of hypnosis: Toward the development of a biopsychosocial model. International Journal of Clinical and Experimental Hypnosis 2015, 63(1), 34–75. [Google Scholar] [CrossRef]
- Jiang, H.; White, M. P.; Greicius, M. D.; Waelde, L. C.; Spiegel, D. Brain activity and functional connectivity associated with hypnosis. Cerebral Cortex 2017, 27(8), 4083–4093. [Google Scholar] [CrossRef]
- Josipovic, Z. Neural correlates of nondual awareness in meditation. Annals of the New York Academy of Sciences 2014, 1307(1), 9–18. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Full catastrophe living: Using the wisdom of your body and mind to face stress, pain, and illness; Delacorte, 1990. [Google Scholar]
- Kashdan, T. B.; Rottenberg, J. Psychological flexibility as a fundamental aspect of health. Clinical Psychology Review 2010, 30(7), 865–878. [Google Scholar] [CrossRef]
- Kirsch, I. Lynn, S. J., Rhue, J. W., Eds.; The social learning theory of hypnosis. In Theories of hypnosis: Current models and perspectives; Guilford Press, 1991; pp. 439–465. [Google Scholar]
- Kirsch, I.; Montgomery, G.; Sapirstein, G. Hypnosis as an adjunct to cognitive-behavioral psychotherapy: A meta-analysis. Journal of Consulting and Clinical Psychology 1995, 63(2), 214–220. [Google Scholar] [CrossRef]
- Landry, M.; Lifshitz, M.; Raz, A. Brain correlates of hypnosis: A systematic review and meta-analytic exploration. Neuroscience & Biobehavioral Reviews 2017, 81(Part A), 75–98. [Google Scholar] [CrossRef]
- Li, Z.; Hu, B.; Zheng, X.; Yi, J.; Zhu, J.; Li, Q.; Zhang, Q. Altered brain network connectivity as a potential biomarker of smoking cessation treatment outcome. Frontiers in Human Neuroscience 2020, 14, 574557. [Google Scholar]
- Lynn, S. J.; Laurence, J. R.; Kirsch, I. Hypnosis, suggestion, and suggestibility: An integrative model. American Journal of Clinical Hypnosis 2015, 57(3), 314–329. [Google Scholar] [CrossRef]
- Marek, S.; Tervo-Clemmens, B.; Calabro, F. J.; Montez, D. F.; Kay, B. P.; Hatoum, A. S.; Dosenbach, N. U. Reproducible brain-wide association studies require thousands of individuals. Nature 2022, 603(7902), 654–660. [Google Scholar] [CrossRef] [PubMed]
- McGeown, W. J.; Mazzoni, G.; Venneri, A.; Kirsch, I. Hypnotic induction decreases anterior default mode activity. Consciousness and Cognition 2009, 18(4), 848–855. [Google Scholar] [CrossRef] [PubMed]
- Menon, V. Large-scale brain networks and psychopathology: A unifying triple network model. Trends in Cognitive Sciences 2011, 15(10), 483–506. [Google Scholar] [CrossRef] [PubMed]
- Oakley, D. A.; Halligan, P. W. Hypnotic suggestion: Opportunities for cognitive neuroscience. Nature Reviews Neuroscience 2013, 14(8), 565–576. [Google Scholar] [CrossRef]
- Porges, S. W. The polyvagal theory: Neurophysiological foundations of emotions, attachment, communication, and self-regulation; W. W. Norton & Company, 2011. [Google Scholar]
- Rainville, P.; Duncan, G. H.; Price, D. D.; Carrier, B.; Bushnell, M. C. Pain affect encoded in human anterior cingulate but not somatosensory cortex. Science 1997, 277(5328), 968–971. [Google Scholar] [CrossRef]
- Rainville, P.; Hofbauer, R. K.; Paus, T.; Duncan, G. H.; Bushnell, M. C.; Price, D. D. Cerebral mechanisms of hypnotic induction and suggestion. Journal of Cognitive Neuroscience 1999, 11(1), 110–125. [Google Scholar] [CrossRef]
- Raz, A.; Lifshitz, M. Elkins, G. R., Ed.; Hypnosis and meditation: Towards an integrative science of conscious planes. In Handbook of medical and psychological hypnosis: Foundations, applications, and professional issues; Springer, 2016; pp. 17–39. [Google Scholar]
- Raz, A.; Shapiro, T.; Fan, J.; Posner, M. I. Hypnotic suggestion and the modulation of Stroop interference. Archives of General Psychiatry 2002, 59(12), 1155–1161. [Google Scholar] [CrossRef]
- Ryff, C. D. Psychological well-being revisited: Advances in the science and practice of eudaimonia. Psychotherapy and Psychosomatics 2014, 83(1), 10–28. [Google Scholar] [CrossRef]
- Schiller, D.; Phelps, E. A. Does reconsolidation occur in humans? Frontiers in Behavioral Neuroscience 2011, 5, 24. [Google Scholar] [CrossRef]
- Siegel, D. J. The developing mind: How relationships and the brain interact to shape who we are, 2nd ed.; Guilford Press, 2012. [Google Scholar]
- Tellegen, A.; Atkinson, G. Openness to absorbing and self-altering experiences (“absorption”), a trait related to hypnotic susceptibility. Journal of Abnormal Psychology 1974, 83(3), 268–277. [Google Scholar] [CrossRef]
- van der Hart, O.; Nijenhuis, E. R.; Steele, K. The haunted self: Structural dissociation and the treatment of chronic traumatization; W. W. Norton & Company, 2006. [Google Scholar]
- Vanhaudenhuyse, A.; Boly, M.; Balteau, E.; Schnakers, C.; Moonen, G.; Luxen, A.; Lamy, M.; Degueldre, C.; Brichant, J. F.; Maquet, P.; Laureys, S.; Faymonville, M. E. Pain and non-pain processing during hypnosis: A thulium-YAG event-related fMRI study. NeuroImage 2009, 47(3), 1047–1054. [Google Scholar] [CrossRef]
- Watkins, J. G.; Watkins, H. H. Ego states: Theory and therapy; W. W. Norton & Company, 1997. [Google Scholar]
- Woody, E. Z.; Bowers, K. S. Lynn, S. J., Rhue, J. W., Eds.; A frontal assault on dissociated control. In Dissociation: Clinical and theoretical perspectives; Guilford Press, 1994; pp. 52–79. [Google Scholar]
Figure 1.
Description: Integrated Mechanistic Model of Hypnotic Emotion Regulation. A multi-panel figure showing: - Panel A: Timeline of three stages (Induction, Network Reconfiguration, Suggestion-Specific Modulation) with approximate durations - Panel B: Brain network diagram showing DMN (blue), ECN (red), and SaN (yellow) nodes and connections, with arrows indicating connectivity changes during hypnosis - Panel C: Flowchart showing causal pathway: Hypnotic Induction → Absorption → Network Reconfiguration → Experiential Plasticity → Emotion Regulation Outcomes - Panel D: Moderating variables (hypnotizability, absorption, dissociation) shown as factors influencing the strength of pathways - Panel E: Feedback loops showing how emotion regulation outcomes can reinforce absorption and network patterns in subsequent sessions.
Figure 1.
Description: Integrated Mechanistic Model of Hypnotic Emotion Regulation. A multi-panel figure showing: - Panel A: Timeline of three stages (Induction, Network Reconfiguration, Suggestion-Specific Modulation) with approximate durations - Panel B: Brain network diagram showing DMN (blue), ECN (red), and SaN (yellow) nodes and connections, with arrows indicating connectivity changes during hypnosis - Panel C: Flowchart showing causal pathway: Hypnotic Induction → Absorption → Network Reconfiguration → Experiential Plasticity → Emotion Regulation Outcomes - Panel D: Moderating variables (hypnotizability, absorption, dissociation) shown as factors influencing the strength of pathways - Panel E: Feedback loops showing how emotion regulation outcomes can reinforce absorption and network patterns in subsequent sessions.
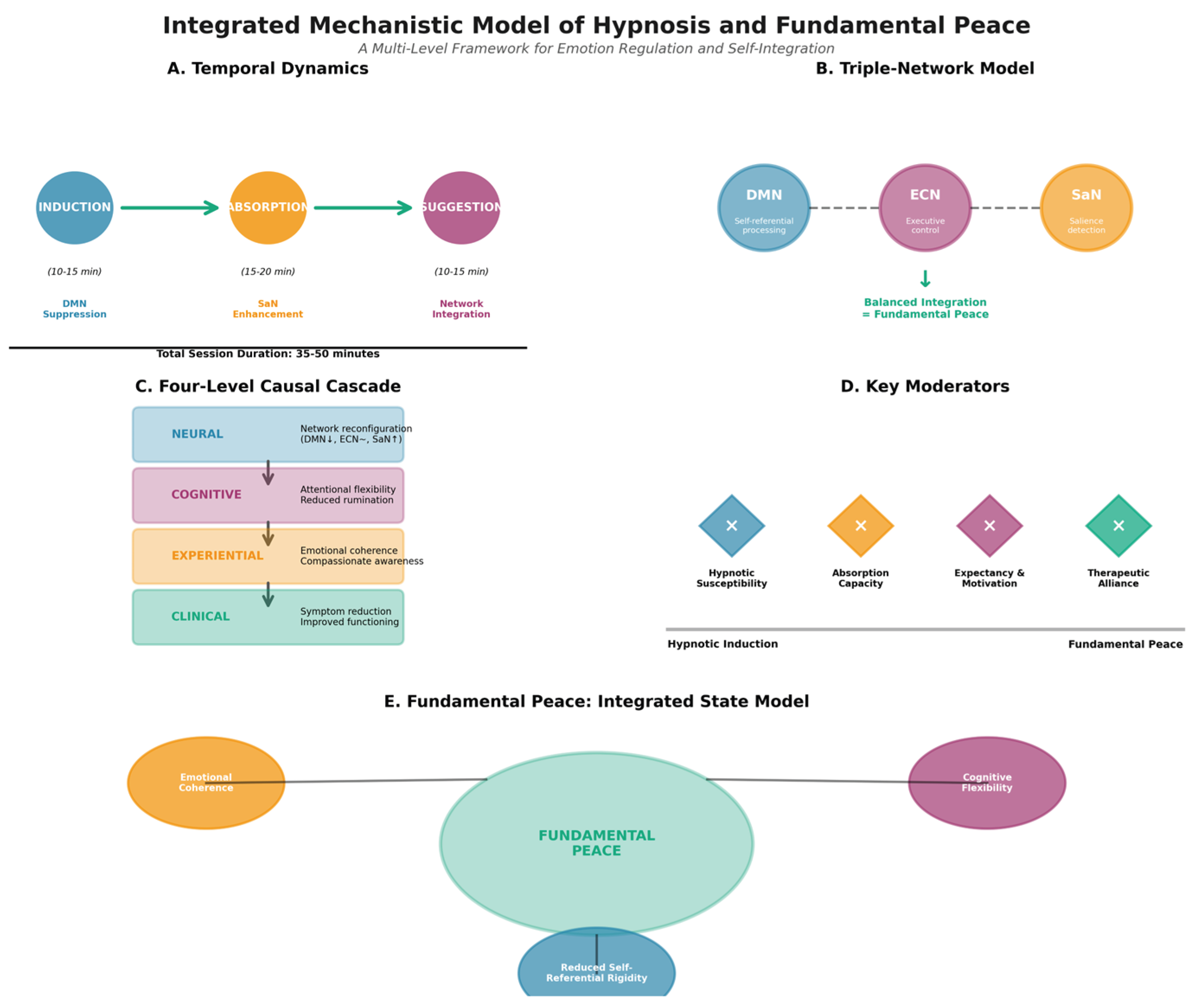
Table 1.
Fundamental Peace vs. Related Constructs.
| Construct | Definition | Key Features | Neural Correlates | Measurement | Distinction from Fundamental Peace |
| Fundamental Peace | Dynamic integrated emotion regulation capacity | Flexible attention, emotional coherence, reduced self-rigidity, compassionate awareness | Balanced DMN-ECN-SaN coordination; flexible network reconfiguration | FP Scale (proposed); network flexibility metrics; behavioral regulation tasks | Emphasizes dynamic regulatory capacity, not static state |
| Equanimity (Desbordes et al., 2015) | Even-minded mental state; affective neutrality | Non-reactivity to pleasant/unpleasant; balanced affect | Reduced amygdala reactivity; altered insula-amygdala connectivity | Equanimity Scale; affect ratings | FP includes active engagement, not just neutrality; emphasizes coherence across self-states |
| Psychological Well-Being (Ryff, 2014) | Positive evaluation of life and self | Autonomy, mastery, growth, purpose, positive relations, self-acceptance | Diverse; includes reward circuits, prefrontal regions | Ryff Scales of Psychological Well-Being | FP is regulatory capacity, not evaluative judgment; can exist amid challenges |
| Nondual Awareness (Josipovic, 2014) | Awareness without subject-object division | Dissolution of self-other boundary; pure consciousness | Reduced DMN activity; altered posterior cingulate function | Nondual Awareness Dimensional Assessment | FP maintains functional self-awareness; emphasizes integration, not dissolution |
| Flow (Csikszentmihalyi, 1990) | Optimal experience during challenging activity | Absorption, loss of self-consciousness, time distortion | Transient hypofrontality; reduced DMN activity | Flow State Scale | FP is stable capacity, not task-specific state; includes self-awareness |
| Mindfulness (Kabat-Zinn, 1990) | Present-moment awareness with acceptance | Non-judgmental attention to present | Altered DMN-ECN connectivity; increased insula activation | FFMQ, MAAS | FP emphasizes emotional coherence and self-integration more than present-focus |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



