Submitted:
27 January 2026
Posted:
28 January 2026
You are already at the latest version
Abstract
Hypertension is a major health issue, both globally and in Japan. Potassium-rich foods help prevent hypertension by promoting sodium excretion. We evaluated whether dadacha-mame (a local potassium-rich edamame variety) improves sodium excretion and influences dietary behavior. This 2-week stratified randomized exploratory trial included 54 (mean age: 20.5±1.4 years; 53.7% females) adults assigned to an intervention group [15 g/day of dried dadacha-mame; n = 27] or a control group [usual diet; n = 27]. Urinary sodium-to-potassium (Na/K) ratios were compared. Shifts in dietary behavior-change stages (pre-contemplation and contemplation) were assessed at baseline and post-intervention. No significant between-group baseline differences were observed. While no overall effect on the Na/K ratio was observed, subgroup analysis showed a significant reduction in the Na/K ratio in the intervention group (4.39 vs. 5.91 in Control, p=0.020). The intervention prompted positive dietary behavior changes, with the proportion of participants in the pre-contemplation stage decreasing from 50.0% at baseline to 33.3% post-intervention. Dietary intervention with dadacha-mame can significantly improve sodium excretion in individuals at a higher risk of hypertension and encourage healthier dietary behaviors. Utilizing local potassium-rich foods may be a valuable public health strategy, creating added value for agricultural products and benefiting community health.
Keywords:
agri-based well-being
; dietary intervention
; hypertension
; social implementation
; sodium-potassium ratio
; urine
1. Introduction
Hypertension has become a global concern, with the number of patients with hypertension doubling over the past 30 years [1]. It is the most common lifestyle-related disease in Japan, affecting an estimated one in three Japanese individuals [2]. Although hypertension is a major risk factor for cerebrovascular disease, ischemic heart disease, and chronic heart failure, many people do not receive appropriate treatment or achieve their treatment goals. A previous study [3] found a positive relationship between the urinary Na/K ratio and hypertension, particularly in participants with higher urinary Na/K ratios, suggesting that reductions in this ratio in this group have a more significant impact. Therefore, limiting dietary salt intake is essential to prevent hypertension.
The target salt intake for the Japanese population, established by the Ministry of Health, Labor and Welfare, is <7.5 g/day for men and 6.5 g/day for women [4]. However, current salt consumption exceeds these targets, averaging 10.8 g/day for men and 9.2 g/day for women. Although the benefits of salt reduction in preventing hypertension are well recognized, maintaining and practicing this reduction remains challenging.
The Committee on Salt Reduction and Nutrition of the Japan Society of Hypertension highlights that promoting salt reduction through individual efforts alone is challenging because of the rising consumption of processed foods and the increasing trend of eating out. They emphasize that government and corporate initiatives are essential. Changing eating habits established in adulthood is challenging, and the psychological burden of salt reduction is acknowledged [5]. For these reasons, early intervention targeting young people is necessary.
In recent years, increasing potassium intake, which promotes sodium excretion, has gained attention as a strategy for preventing hypertension. According to the 2019 “National Health and Nutrition Survey” conducted by the Ministry of Health, Labour, and Welfare [6], potassium intake among Japanese adults aged ≥20 years averages 2,439 mg/day for men and 2,273 mg/day for women, falling short of the target values of 3,000 mg/day for men and 2,600 mg/day for women. Consistent daily consumption of potassium-rich vegetables is expected to prevent hypertension.
The urinary Na/K ratio has been used as an indicator to evaluate the balance between dietary sodium and potassium intake, with studies reporting that a decrease in this ratio contributes to lowering blood pressure [3]. However, few intervention studies have examined the effectiveness of potassium intake in preventing hypertension in humans, and the evidence remains limited.
Salt intake behavior is influenced not only by environmental factors but also significantly by individual awareness and readiness to change. The behavioral change stage model (Transtheoretical Model) [7,8,9] describes health behavior change as progressing through stages, such as the “indifference stage,” “interest stage,” and “preparation stage,” with perceptions and responses to interventions varying depending on the stage. Therefore, understanding the stages of awareness regarding dietary behavior improvement before and after an intervention is crucial for comprehensively evaluating changes in awareness and their relationship with actual changes in salt intake.
However, domestic studies implementing dietary interventions that focus on changes in behavioral stages are limited, with few tracking continuous behavioral changes over extended periods. Moreover, research examining the effects of dietary interventions targeting young people, who tend to show less interest in health behaviors, remains scarce. Therefore, this exploratory study aimed to provide important insights into this area.
The purpose of this study was to examine the effect of salt (NaCl) reduction through the consumption of local foods that were cultivated, managed, processed, and analyzed for their ingredients, as well as to assess changes in attitudes toward improving dietary behavior among participants in the intervention trial.
2. Methods
2.1. Study Design
The study design was a stratified, randomized controlled trial. Stratified random assignment was made by the study investigator to intervention (n = 27) and control (n = 27) groups based on sex and Na/K ratio (<4.0 or ≥4.0). Allocations were made using a cutoff value of 4.0, which is the feasible target value for the Na/K ratio in the Japanese population [10]. As a baseline study, participants’ early morning urine samples were collected, and urinary Na/K ratios were measured for three days in mid-November 2023, and the mean value was calculated. Urinary Na/K ratios were measured using a Na/K meter (Omron Corporation, Kyoto, Japan). This study is reported in accordance with the CONSORT Statement, which aims to improve the reporting quality of randomized controlled trials [11]. The study was conducted in accordance with the principles outlined in the Declaration of Helsinki (1975, revised in 2013), and approved by the Ethics Review Committee of Yamagata University Faculty of Medicine (Approval No.: 2022-335; date: June 22, 2023). The trial was registered in the UMIN Clinical Trials Registry, URL: https://qr.paps.jp/45sSA (No. UMIN000056934; Date: February 04, 2025).
2.2. Study Population
The participants were 60 non-medical undergraduate and graduate students (25 males and 35 females) living in a local city.
Regarding the inclusion criteria, participants were eligible if they met all the following conditions: adults (male or female), residing in the community, able to participate continuously throughout the study period, capable of understanding the purpose of the study, and providing written informed consent. Participants were excluded if they met any of the following conditions: currently receiving medical treatment for hypertension or renal disease; regularly taking medications that affect electrolyte balance, such as diuretics, antihypertensive agents, or corticosteroids; pregnant or lactating; or having known allergies to the intervention foods. Participants were assigned to any of the following two groups, stratified by Na/K ratio of <4.0 and >4.0, using the feasible target urinary Na/K ratio of 4.0 for Japanese as the cutoff: an intervention group (n = 27) or a control group (n = 27). A total of 54 participants were included in the analysis, excluding six who dropped out due to illness or other reasons during the intervention.
2.3. Sample Size and Sampling
Assuming an effect size of 0.5, power of 0.90, and α = 0.05, the required sample size was calculated using G*Power 3.1 (University of Düsseldorf, Düsseldorf, Germany), resulting in a minimum required sample size of 52 participants, which was achieved in this study.
2.4. Study Procedures
2.4.1. Interventions
During the intervention period, the intervention group consumed the target food daily. Early morning urine samples from all participants were collected again for three consecutive days immediately after the intervention, and the Na/K ratio was measured. The Na/K ratio results were returned to the participants in October 2024 after all analyses were completed. The target food in the intervention study was dadacha-mame, a local edamame variety grown and harvested in Tsuruoka City, Japan. The intervention group consumed 15 g/day of heat-dried (Shinsei Bio Heat Dryer) dadacha-mame for 2 weeks. Nutrient analysis showed that the potassium content of dadacha-mame was 255 mg/15 g. In comparison, the potassium content of common edamame is reported to be 73.5 mg/15 g (Standard Tables of Food Composition in Japan, 8th Revision, Supplement 2023), indicating that dadacha-mame has a high potassium content. According to the Dietary Reference Intakes for Japanese (2020 edition), the recommended daily potassium intake is 2,500 mg for men and 2,000 mg for women aged ≥18 years. The potassium content of the dadacha-mame used in this study was within the standard intake range, with no concerns regarding health risks due to excessive intake. Participants in the control group were instructed to maintain their usual diet and lifestyle habits and to avoid consuming dadacha-mame. The intervention was implemented during the winter months when dadacha-mame was unavailable.
2.4.2. Outcome
In this study, early morning urine samples were collected from all participants, and urinary Na/K ratios were measured for three consecutive days in November 2023. Participants were stratified into two groups based on a Na/K ratio of 4.0, which is a feasible target value for Japanese individuals: <4.0 and ≥4.0. Urinary Na/K ratios were measured using a Na/K meter (Omron Corporation). The 2-week intervention was conducted in December 2023. Early morning urine samples from all participants were again collected for three consecutive days immediately after the intervention, and the Na/K ratio was remeasured. The results of the Na/K ratio were returned to the participants in November 2024 after all analyses and the recommended actions were completed.
In the baseline survey, we recorded sex, age, sleep duration, frequency of alcohol consumption, eating habits (BDHQ) [12], and stages of behavioral change related to improving eating behavior, based on the “Lifestyle Survey” by the Ministry of Health, Labour and Welfare (see reference). The following options were set up corresponding to the indifference, interest, preparation, implementation, and maintenance stages of the behavioral change model [7,8,9]: “I do not intend to change my behavior within 6 months,” “I intend to change my behavior within 6 months,” “I intend to change my behavior within 1 month,” “I have changed my behavior less than 6 months,” and “I have changed my behavior more than 6 months.” At the time of returning the pre- and post-intervention Na/K ratio results (one year after the intervention), we surveyed participants’ stage of behavior change regarding awareness of improving dietary behavior.
2.4.3. Randomization
Participants were randomly assigned to the intervention or control group in a 1:1 ratio. Allocation was based on a computer-generated random number table stratified by sex and Na/K ratio.
2.4.4. Blinding
Due to the nature of the intervention, blinding of the participants and intervention providers was not feasible. However, the outcome assessment was conducted by independent assessors blinded to the group allocation to reduce detection bias. Additionally, objective outcome measures (Na/K ratio) were used to minimize the influence of participant or investigator expectations on the results.
2.5. Data Collection
Data were collected at multiple time points to assess physiological and behavioral indicators. The sodium/potassium ratios (Na/K ratios) were measured at two time points: before the intervention (baseline) and at the end of the intervention. The participants collected urine samples at home in the morning according to standardized procedures and submitted their specimens to the laboratory.
Changes in eating behavior were assessed using a self-administered questionnaire based on the Transtheoretical Model (Behavior Change Stage Model). The questionnaire was administered at three time points: before the intervention, at the end of the intervention, and one year after the intervention, when the Na/K ratio results were returned.
Data collection was performed by trained staff who were not involved in the implementation of the intervention and were trained in allocation and open labeling.
2.6. Statistical Analysis
Participants’ characteristics were summarized using descriptive statistics. Continuous variables are presented as mean ± standard deviation, and categorical variables as frequency and percentage.The effect of potassium-rich food intake on the Na/K ratio was examined in the intervention and control groups using a paired t-test. Statistical significance was set at p<0.05. All statistical analyses were performed using SPSS Statistics 29 for Windows (IBM Corp., Armonk, NY, USA).
The Behavior Change Stage Model (Transtheoretical Model) was used to assess awareness regarding the improvement of eating behavior. Participants selected one of the following five stages that most closely resembled their current state: (1) indifference, (2) interest, (3) preparation, (4) implementation, and (5) maintenance. The distribution of each stage at baseline and pre- and post-intervention was calculated.
3. Results
3.1. Basic Attributes of Study Participants
A total of 60 persons were screened, and 54 participants were included in the analysis, excluding six who dropped out due to illness or other reasons during the intervention (Figure 1). The mean age of the 54 participants was 20.5 ± 1.4 years, the majority were female (53.7%), and their mean Na/K ratio was 5.01 (Table 1). Half of the participants were randomized into the intervention (n = 27) and control groups (n = 27). Participants in the intervention group did not differ from those in the control group in terms of age, sex, or Na/K ratio.
3.2. Salt Removal Effect of Intervention Food Intake
The Na/K ratios were 4.73 in the intervention group and 4.57 in the control group, with no significant difference (p = 0.72) (Figure 2). The baseline Na/K ratios for participants with values ≥4.0 were 5.01 in the intervention group and 5.18 in the control group, showing no significant difference (p = 0.77).
Next, we examined the effect of salt elimination on those in the intervention group, those with baseline Na/K ratios >4.5, and those in the control group (Figure 3); those with Na/K ratios >4.5 had significantly lower Na/K ratios than those in the control group (p < 0.05).
3.3. Participants’ Attitudes toward Improving Eating Behavior
Table 2 shows the proportion of participants in each behavioral change stage at baseline, post-intervention, and after the return of results based on questionnaire responses. The response rates were 100% at baseline, 93.3% after the intervention, and 71.7% 1 year after the intervention. Overall, 42 participants who completed all questionnaires (70% follow-up rate) were included in the analysis of their attitudes toward improving eating behavior.
The proportion of participants in the indifferent stage decreased from 50.0% at baseline to 33.3% after the intervention and to 23.8% after the return of the questionnaire results. Those in the interested stage increased from 21.4% at baseline to 23.8% after the intervention and 26.2% after the return of results. Participants in the preparation stage increased from 16.7% at baseline to 21.4% after the intervention and to 31.0% after the return of results. The proportion of patients in the implementation stage increased from 2.4% at baseline to 14.3% after the intervention and then decreased to 9.5% after the return of results. The proportion of patients in the maintenance stage decreased from 9.5% at baseline to 7.1% after the intervention and increased again to 9.5% after the return of the questionnaire.
4. Discussion
This study investigated whether the consumption of dadacha-mame could promote sodium excretion and encourage positive dietary behavior changes among healthy young adults. The study findings demonstrated that dietary intervention significantly reduced salt intake and promoted desirable dietary behavior changes, particularly among individuals at a high risk for hypertension (defined by a urinary Na/K ratio ≥4.5). These findings suggest that reducing sodium intake and improving the Na/K ratio may help mitigate the risk of hypertension. Dietary potassium intake is known to promote urinary sodium excretion through several physiological mechanisms, including inhibition of renal sodium reabsorption, increased natriuresis, and modulation of the renin–angiotensin–aldosterone system. Higher potassium intake also enhances distal tubular sodium excretion, thereby contributing to improvements in the urinary Na/K ratio. These mechanisms provide a physiological basis for the observed effects of potassium-rich food consumption in the present study.
Consistent with these results, a previous 6-month quasi-experimental dietary intervention in a workplace setting reported a reduction in salt intake from 10.7 g to 9.3 g, although no significant change in the Na/K ratio was observed [13]. In that study, improvements in the dietary environment, such as introducing low-sodium menus, potassium-rich foods, and providing nutritional information in workplace cafeterias, were associated with reduced sodium intake.
Systematic reviews have also supported the effectiveness of behavior-change interventions in reducing salt consumption. These interventions led to decreased purchases of high-sodium foods, increased use of salt substitutes, and a reduction in urinary sodium levels across 32 studies [14]. These findings highlight the importance of improving Na/K ratios through dietary interventions. Additional evidence suggests that the use of low Na/K ratio seasonings and potassium-rich dairy products in corporate cafeterias can enhance the dietary Na/K balance [15]. In our study, improvements in the food environment were associated with reductions in urinary Na/K ratios, further supporting the effectiveness of environmental modifications.
Moreover, combining casual urine Na/K ratio measurements with health counseling during routine physical examinations has been shown to promote salt reduction and better hypertension management [16]. The present study supports the use of the urinary Na/K ratio as an outcome measure. Previous research has also demonstrated that urinary Na/K ratios are associated with blood pressure levels in healthy adolescents, indicating their relevance even in younger populations [17].
Importantly, efforts to reduce salt intake often fail due to reliance on inhibitory strategies, which have been shown to be less effective in changing dietary behaviors and are known to be particularly resistant to change [18]. Dietary behaviors are especially difficult to modify compared to other health behaviors [19]. For individuals with high Na/K ratios who struggle to sustain sodium restriction, a “salt elimination” approach that focuses on increasing potassium intake may provide a more sustainable behavioral strategy [20]. This approach does not rely solely on strict sodium restriction but instead leverages physiological sodium–potassium interactions to facilitate sodium excretion while maintaining dietary acceptability. Additionally, personal experiences with health risks may serve as a catalyst for behavioral change among individuals who are otherwise indifferent to their health. However, few studies have investigated whether disclosing post-intervention Na/K ratio results can shift attitudes in this group. In our study, some participants (n = 9) showed regression in their stage of behavioral change after receiving feedback. Among them, eight noted that their Na/K ratios remained high despite dietary efforts, suggesting a lack of perceived benefits and limited motivation for continued behavioral change. Alternative approaches are required for such individuals [21].
A major strength of this study is its real-world implementation in community and workplace settings, which enhances the generalizability and practical relevance of the findings. The high follow-up completion rate minimized attrition bias and increased the reliability of the outcomes. Furthermore, the use of objective biochemical indicators, specifically the urinary Na/K ratio, helped address the limitations inherent in self-reported dietary data.
Nonetheless, this study had some limitations. First, the relatively small sample size in the stratified groups may have limited the statistical power and introduced variability. Second, the intervention period was relatively short (2 weeks), which may not be sufficient to capture long-term physiological adaptations or sustained dietary behavior changes. Short-term improvements in the urinary Na/K ratio do not necessarily indicate long-term blood pressure control or behavioral maintenance. Third, the non-crossover design did not account for seasonal variations in the Na/K ratios. Fourth, some behavioral variables were measured using single-item scales, potentially limiting precision. To address these limitations, objective biomarkers were used, and stratified analyses were conducted.
Future research should employ larger-scale randomized controlled trials with multiple time-point measurements to validate these findings. Longer intervention periods and extended follow-up are particularly important to assess the sustainability of potassium-rich dietary interventions and their long-term effects on sodium excretion, blood pressure regulation, and behavioral adherence. Incorporating Na/K ratio screening and personalized feedback into routine workplace health programs, alongside improvements in the food environment (e.g., sodium-reduced meals and potassium-rich options), may effectively encourage salt-reduction behavior. For individuals who find sodium restriction challenging, strategies focusing on increasing potassium intake may offer feasible and sustainable alternatives.
Future studies should also develop tailored interventions for individuals showing limited behavioral change and explore psychological and motivational barriers to dietary modification. Long-term follow-up is essential to evaluate the sustainability of blood pressure control and behavioral changes. In addition, the economic impact of integrating local agricultural products into health interventions should be assessed. Further research is warranted on the combined effects of behavioral techniques, such as nudging, goal setting, and social support, in promoting healthier dietary behaviors.
5. Conclusions
This study demonstrated that short-term consumption of potassium-rich vegetables resulted in changes in the urinary Na/K ratio among healthy young adults. The findings suggest a potential association between potassium-rich dietary intake and dietary awareness in individuals with higher Na/K ratios, including those previously indifferent to dietary improvement.
Author Contributions
Conceptualization, S.G.; methodology, S.G.; software, S.G.; validation, S.G. and M.T.; formal analysis, S.G. and M.T.; investigation, M.T., Y.K., M.To., H.M., Y.O., A.K., A.E., and K.H.; resources, S.G.; data curation, S.G.; writing—original draft preparation, S.G., M.Y., and M.T.; writing—review and editing, S.G., and M.Y.; visualization, S.G., M.Y., and M.T.; supervision, S.G.; project administration, S.G.; funding acquisition, S.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by Yamagata University Faculty of Agriculture Regional Industry-Academia-Government Collaboration Council, Yamagata University Friendship Association, Yamagata University Advanced Agri-Food System Research Center (YAAS), Yamagata University Institute of Well-being, and YU-COE (Yamagata University Center of Excellence for Advanced Research) Grant.
Institutional Review Board Statement
The study was conducted in accordance with the principles outlined in the Declaration of Helsinki (1975, revised in 2013), and approved by The Ethical Review Committee of Yamagata University Faculty of Medicine (Approval No.: 2022-335; date: June 22, 2023). The trial was registered in the UMIN Clinical Trials Registry, URL: https://qr.paps.jp/45sSA (No. UMIN000056934; Date: February 04, 2025).
Informed Consent Statement
Informed consent was obtained from all participants involved in the study.
Written
informed consent has been obtained from the participantsto publish this paper.
Data Availability Statement
The data presented in this study are available on request from the corresponding author due to ethical restrictions, as the data include personal health information collected from the participants.
Acknowledgments
We would like to thank all the subjects who participated in this project, Sato, a 5th year student of the Food and Agriculture Business School, Konta of Yamagata University School of Medicine, the members of the Ethics Review Committee of Yamagata University School of Medicine, Section Chief Kokubu, Nagamine of the Faculty of Engineering, and Coordinator Mr. Takahashi. We thank all the participants in this study.
Conflicts of Interest
The authors declare no conflicts of interest. The sponsors had no role in the design, execution, interpretation, or writing of the study.
Abbreviations
The following abbreviations are used in this manuscript:
| Na/K ratio | Sodium/Potassium Ratio |
References
- NCD Risk Factor Collaboration (NCD-RisC). Long-term and recent trends in hypertension awareness, treatment, and control in 12 high-income countries: an analysis of 123 nationally representative surveys. Lancet 2019, 394(10199), 639–651. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Hypertension Japan 2023 country profile. Available online: https://www.who.int/publications/m/item/hypertension-jpn-2023-country-profile (accessed on 6 July 2025).
- Kogure, M.; Nakaya, N.; Hirata, T.; Tsuchiya, N.; Nakamura, T.; Narita, A.; Suto, Y.; Honma, Y.; Sasaki, H.; Miyagawa, K.; Ushida, Y.; Ueda, H.; Hozawa, A. Sodium/potassium ratio change was associated with blood pressure change: possibility of population approach for sodium/potassium ratio reduction in health checkup. Hypertens. Res. 2021, 44(2), 225–231. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health; Labour and Welfare of Japan. Dietary Reference Intakes for Japanese, 2020. Available online: https://www.mhlw.go.jp/stf/shingi/other-kenkou_539644.html (accessed on 6 July 2025).
- Japan Society of Hypertension. Come on Reduce Salt! (to the general public from the Salt Reduction and Nutrition Committee). Available online: https://www.jpnsh.jp/general_salt_02.html (accessed on 6 July 2025).
- Ministry of Health; Labour and Welfare of Japan. Report on the National Health and Nutrition Survey in 2019. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/kenkou_iryou/kenkou/eiyou/r1-houkoku_00002.html (accessed on 6 July 2025).
- Prochaska, J.O.; DiClemente, C.C. Stage and processes of self-change of smoking: toward an integrative model of change. J. Consult. Clin. Psychol. 1983, 51(3), 390–395. [Google Scholar] [CrossRef] [PubMed]
- Prochaska, J.O.; Velicer, W.F. The transtheoretical model of health behavior change. Am. J. Health Promot. 1997, 12(1), 38–48. [Google Scholar] [CrossRef] [PubMed]
- Prochaska, J.O.; Redding, C.A.; Evers, K.E. The transtheoretical model and stages of change. In Health Behavior and Health Education: Theory, Research, and Practice, 4th ed.; Glanz, K., Rimer, B.K., Viswanath, K., Eds.; Jossey-Bass: San Francisco, USA, 2008; pp. 97–121. [Google Scholar]
- Hisamatsu, T.; Kogure, M.; Tabara, Y.; Hozawa, A.; Sakima, A.; Tsuchihashi, T.; Yoshita, K.; Hayabuchi, H.; Node, K.; Takemi, Y.; Ohkubo, T.; Miura, K. Japanese Society of Hypertension Working Group on Urine Sodium-to-Potassium Ratio. Practical use and target value of urine sodium-to-potassium ratio in assessment of hypertension risk for Japanese: consensus statement by the Japanese Society of Hypertension Working Group on Urine Sodium-to-Potassium Ratio. Hypertens. Res. 2024, 47(12), 3288–3302. [Google Scholar] [CrossRef] [PubMed]
- Schulz, K.F.; Altman, D.G.; Moher, D.; CONSORT Group. CONSORT 2010 Statement: updated guidelines for reporting parallel group randomised trials. B.M.J. 2010, 340, c332. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, S.; Honda, S.; Murakami, K.; Sasaki, S.; Okubo, H.; Hirota, N.; Notsu, A.; Fukui, M.; Date, C. Both comprehensive and brief self-administered diet history questionnaires satisfactorily rank nutrient intakes in Japanese adults. J. Epidemiol. 2012, 22(2), 151–159. [Google Scholar] [CrossRef] [PubMed]
- Sakaguchi, K.; Takemi, Y.; Hayashi, F.; Koiwai, K.; Nakamura, M. Effect of workplace dietary intervention on salt intake and sodium-to-potassium ratio of Japanese employees: a quasi-experimental study. J. Occup. Health 2021, 63(1), e12288. [Google Scholar] [CrossRef] [PubMed]
- Khalesi, S.; Williams, E.; Irwin, C.; Johnson, D.W.; Webster, J.; McCartney, D.; Jamshidi, A.; Vandelanotte, C. Reducing salt intake: a systematic review and meta-analysis of behavior change interventions in adults. Nutr. Rev. 2022, 80(4), 723–740. [Google Scholar] [CrossRef] [PubMed]
- Okuda, N.; Higashiyama, A.; Tanno, K.; Yonekura, Y.; Miura, M.; Kuno, H.; Nakajima, T.; Nagahata, T.; Taniguchi, H.; Kosami, K.; Kojima, K.; Okayama, A. Na and K intake from lunches served in a Japanese company cafeteria and the estimated improvement in the dietary Na/K ratio using low-Na/K seasonings and dairy to prevent hypertension. Nutrients 2024, 16(10), 1433. [Google Scholar] [CrossRef] [PubMed]
- Hisamatsu, T. Optimal timing for measuring the casual urine Na/K ratio using a single sample: insights from a comparison with 24-h urine samples. Hypertens. Res. 2025, 48(2), 849–851. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Miyai, N.; Utsumi, M.; Miyashita, K.; Arita, M. Spot urinary sodium-to-potassium ratio is associated with blood pressure levels in healthy adolescents: the Wakayama Study. J. Hum. Hypertens. 2024, 38(3), 238–244. [Google Scholar] [CrossRef] [PubMed]
- Bouton, M.E. Why behavior change is difficult to sustain. Prev. Med. 2014, 68, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, F. The use of nudges in changing eating behavior: usefulness and challenges in primary prevention. J. Jpn. Soc. Health Educ. 2023, 31, 75–82. [Google Scholar]
- Shimazaki, T.; Okoshi, H.; Yamauchi, T.; Takenaka, K.; Suka, M. The process of behavioral change in individuals who are uninterested in health: a qualitative study based on professional health knowledge. Environ. Health Prev. Med. 2022, 27, 32. [Google Scholar] [CrossRef] [PubMed]
- McEwan, D.; Rhodes, R.E.; Beauchamp, M.R. What happens when the party is over?: sustaining physical activity behaviors after intervention cessation. Behav. Med. 2022, 48(1), 1–9. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flow diagram of participant allocation in the stratified randomized controlled trial according to baseline Na/K ratio.
Figure 1.
Flow diagram of participant allocation in the stratified randomized controlled trial according to baseline Na/K ratio.
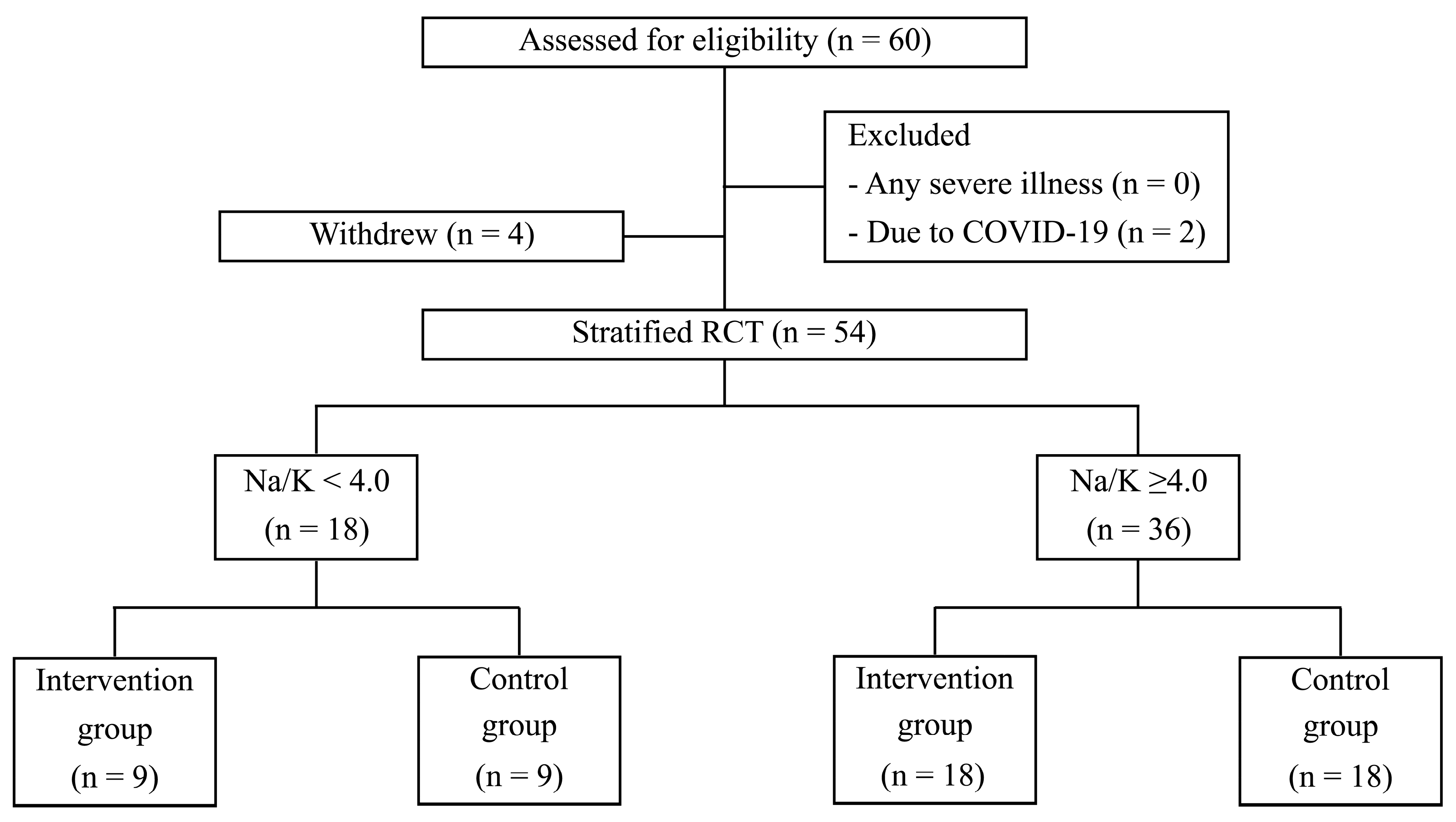
Figure 2.
Effect of salt removal in the intervention and control groups.
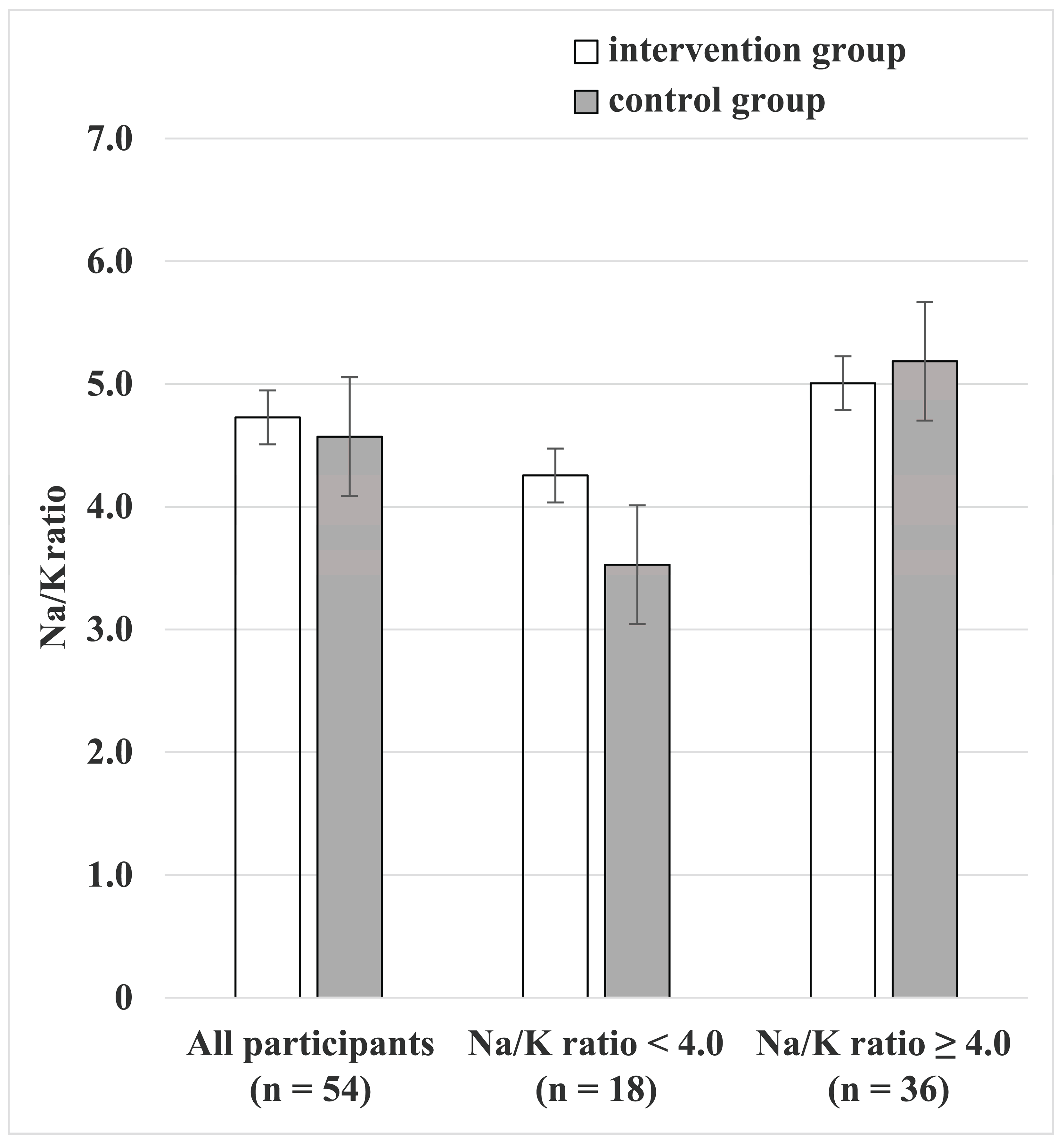
Figure 3.
Effect of salt removal in the intervention and control groups at Na/K ratios >4.5.
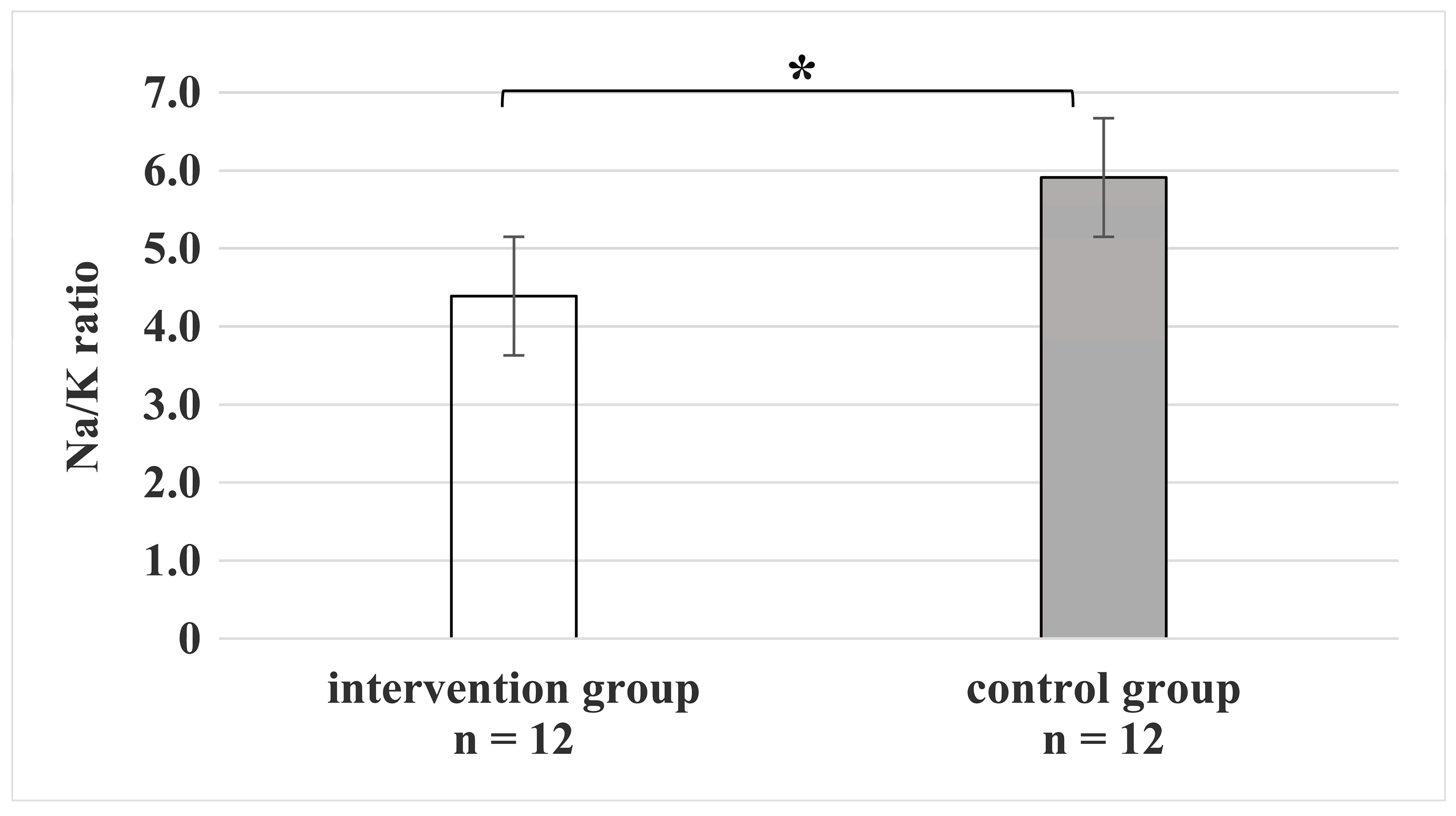

Table 1.
Baseline Characteristics and Changes in Na/K Ratio among Participants in the Intervention and Control Groups Following Dadacha-mame Intake.
Table 1.
Baseline Characteristics and Changes in Na/K Ratio among Participants in the Intervention and Control Groups Following Dadacha-mame Intake.
| Variable | All Participants (n = 54) |
Intervention Group (n = 27) |
Control Group (n = 27) |
p-value |
| Age (years) | 20.5 ± 1.4 | 20.3 ± 1.3 | 20.7 ± 1.6 | 0.32 |
| Sex (%) | ||||
| Men | 46.3 | 51.9 | 40.7 | 0.41 |
| Women | 53.7 | 48.1 | 59.3 | |
| Na/K Ratio | ||||
| Pre-intervention average | 5.01 | 5.03 | 5.00 | 0.64 |
| Post-intervention average | 4.65 | 4.73 | 4.53 | 0.73 |
| Post-intervention (Na/K ≥ 4.5) (n = 24; 12 per group) |
5.15 | 4.39 | 5.91 | <0.05 |
| Post-intervention (Na/K ≥ 4) (n = 36; 18 per group) |
5.10 | 5.01 | 5.18 | 0.77 |
| Post-intervention (Na/K < 4) (n = 18; 9 per group) |
3.89 | 4.25 | 3.53 | 0.27 |
Table 2.
Proportion of the number of people by behavior-change stage.
| Baseline | After intervention | 1 year after (after seeing Na/K ratio results) |
|
| Pre-contemplation | 50.0% | 33.3% | 23.8% |
| Contemplation | 21.4% | 23.8% | 26.2% |
| Preparation | 16.7% | 21.4% | 31.0% |
| Action | 2.4% | 14.3% | 9.5% |
| Maintenance | 9.5% | 7.1% | 9.5% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



