
Submitted:
27 January 2026
Posted:
28 January 2026
You are already at the latest version
Abstract
Background and Objectives: Combined orthodontic–orthognathic treatment is the standard approach for managing severe dentofacial deformities. Nevertheless, its potential impact on periodontal tissues, particularly gingival recession, remains a matter of clinical concern. This study aimed to evaluate the relationship between orthodontic–orthognathic procedures and gingival recession based on available clinical evidence, with particular focus on potential risk modifiers, including orthodontic mechanics, surgical factors, and periodontal phenotype. Materials and Methods: This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Me-ta-Analyses (PRISMA) 2020 guidelines. The review question was formulated using the PICO framework. Results: Across the seven included studies, the presence and extent of gingival recession following combined orthodontic–orthognathic treatment varied according to surgical procedure, adjunctive therapy, and patient-specific factors.
Conclusions: The risk of gingival recession appears to be related primarily to periodontal phenotype and orthodontic tooth movement (especially in the mandibular incisor region) rather than to orthognathic surgery itself. Careful interdisciplinary planning and peri-odontal risk assessment may help reduce postoperative gingival recession.
Keywords:
gingival recession
; periodontal recession
; orthodontic – orthognathic treatment
; le fort I osteotomy
; sagittal split osteotomy
1. Introduction
Severe dentomaxillary and skeletal anomalies represent a unique category of pathology in oral and maxillofacial surgery, as their management is complex and extends over a prolonged period of time [1]. Owing to disorders of maxillary and mandibular bone development in relation to the cranial base, an exclusively orthodontic therapeutic approach carries a high risk of failure [2]. In such complex cases, orthognathic surgery is a mandatory and distinct stage in patient management [3]. Surgical procedures are generally performed at the completion of craniofacial growth and are preceded and followed by orthodontic treatment [4]. Orthognathic surgery may range from relatively simple procedures, such as surgically assisted rapid palatal expansion (SARPE), to more complex bimaxillary interventions involving controlled maxillary (Le Fort I) and mandibular (bilateral sagittal split osteotomy—BSSO) osteotomies. These procedures allow for advancement, retrusion, rotation, impaction, or disimpaction of the jaws, with the aim of restoring craniofacial symmetry, functional balance, and aesthetic harmony [5].
Failure to address this type of pathology in a multidisciplinary manner, or incorrect timing in the orthodontic–orthognathic approach, can lead to the development of major functional and aesthetic disorders such as facial asymmetry, periodontal disease with gingival recession (GR), temporomandibular joint disorders (TMD), facial pain, and chewing, speech, or swallowing disorders in severe cases [6]. Within this clinical picture, preoperatively present gingival recession has a major impact on facial aesthetics [7]. Uneven transmission of masticatory forces in patients with severe malocclusions, or improperly conducted orthodontic treatments, can lead to pathological bone resorption with secondary gingival recession and exposure of the tooth roots [1,2,3,4]. This may result in dental hypersensitivity of varying degrees, an increased risk of carious lesions, or dental mobility in severe cases [7,8]. Poor oral hygiene in these patients can further aggravate these symptoms, leading to faster disease progression and irreversible complications [9].
Orthodontic–orthognathic treatment aims to establish craniofacial skeletal harmony by achieving improved facial balance, proportions, and functional occlusion, with a normal condyle–centric relation (CR) [2]. These corrections also aim to improve the patient’s periodontal health by halting the progression of gingival recession (GR) or even preventing its occurrence in cases where it is not yet present [7,8,9]. A major concern, however, is the development of GR secondary to surgical interventions when it was not previously present [1,2,3,4,5,6]. This outcome has been reported by several authors, all of whom consider it a sign of significant treatment failure [1,2,3,4,5,6]. Postoperative GR may be caused by multiple factors, including intraoperative surgical trauma to the periodontium, the patient’s gingival phenotype, improperly conducted orthodontic treatment, or a combination of these factors [1,2,3,4,5,6]. However, there is currently no consensus in the literature regarding the primary causes of postoperative GR, nor are there clear recommendations for its prevention, as authors’ opinions remain divided [7,8,9].
In light of these limitations, this systematic review aims to evaluate the available clinical evidence on gingival recession following combined orthodontic–orthognathic treatment, with particular focus on potential risk modifiers, including orthodontic mechanics, surgical factors, and periodontal phenotype.
2. Materials and Methods
2.1. Study Design and Protocol Registration
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines. The review question was formulated using the PICO framework.
2.2. Focused Research Question
The focused research question was: “What is the presence and extent of gingival recession following combined orthodontic–orthognathic treatment compared with baseline or control conditions?”
2.3. Eligibility Criteria
- Studies were considered eligible if they met the following criteria:
- Population: Human subjects undergoing combined orthodontic and orthognathic treatment
- Intervention: Any orthodontic–orthognathic surgical approach (single or bimaxillary)
- Outcome: Presence, prevalence, or severity of gingival recession measured clinically
- Study design: Randomized controlled trials, non-randomized clinical trials, prospective or retrospective cohort studies, and case–control studies
- Language: Articles published in English
- Publication status: Full-text articles available
The following studies were excluded: case reports, case series with fewer than 10 patients, reviews, editorials, letters, and conference abstracts; animal or in vitro studies; studies evaluating orthodontic treatment alone without orthognathic surgery; studies not reporting gingival recession as an outcome; studies with insufficient or unclear outcome data.
2.4. Information Sources and Search Strategy
A comprehensive electronic literature search was conducted in the following databases: PubMed/MEDLINE, Web of Science, Cochrane. Library The search covered all available records from database inception to the most recent update prior to manuscript preparation. A combination of Medical Subject Headings (MeSH) terms and free-text keywords was used. The search strategy was adapted for each database. Keyword used were: gingival recession, periodontal recession, gingival margin, orthognathic surgery, LeFort I Osteotomy, maxillary osteotomy, mandibular osteotomy, jaw surgery, sagittal split osteotomy. Additionally, the reference lists of included studies and relevant reviews were manually screened to identify further eligible articles.
2.5. Study Selection
All identified records were imported into reference management software, and duplicates were removed. Two independent reviewers screened titles and abstracts for eligibility. Full-text articles were then assessed independently for inclusion. Any disagreements were resolved through discussion or consultation with a third reviewer. The study selection process was documented using a PRISMA flow diagram.
2.6. Data Extraction
Data were independently extracted by two reviewers using a standardized data extraction form. The following information was collected: Author(s) and year of publication, Study design, Sample size and demographic characteristics, Type of orthodontic–orthognathic treatment, Duration of follow-up, Methods used to assess gingival recession, Main outcomes related to gingival recession, Confounding factors and limitations. Any discrepancies in data extraction were resolved by consensus.
2.7. Risk of Bias Assessment
The methodological quality and risk of bias of the included studies were assessed independently by two reviewers. The following tools were used according to study design: Cochrane Risk of Bias tool for randomized controlled trials; Newcastle–Ottawa Scale (NOS) for observational studies. Studies were classified as having low, moderate, or high risk of bias.
2.8. Data Synthesis
Due to anticipated heterogeneity in study design, outcome measures, and follow-up periods, a qualitative synthesis was primarily performed. When sufficient homogeneous data were available, quantitative analysis was considered. Results were summarized descriptively and presented in tables.
3. Results
3.1. Study Selection
The literature search across PubMed/MEDLINE, Web of Science, and the Cochrane Library yielded 312 records. After removal of 84 duplicates, 228 articles underwent title and abstract screening. 197 records were excluded because they did not address combined orthodontic–orthognathic treatment with clinical gingival recession outcomes or were ineligible study designs (e.g., case reports, reviews). 31 full-text articles were assessed for eligibility; 24 were excluded owing to lack of recession data, absence of combined treatment, or inadequate outcome reporting. Ultimately, 7 clinical studies met all inclusion criteria and were included in this systematic review (Figure 1).
3.2. Characteristics of Included Studies
The characteristics of the included studies are summarized in Table 1. All seven investigations were observational clinical studies evaluating gingival or mucogingival outcomes in patients undergoing combined orthodontic–orthognathic treatment. Sample sizes ranged from 24 to 40 patients, with outcomes assessed at the level of individual teeth or tooth regions. Follow-up periods varied from immediate postoperative evaluation to long-term observation, and outcome measures primarily consisted of clinical assessments of gingival recession and mucogingival parameters.
Liu et al. (2024) conducted a retrospective cohort study in skeletal Class III patients undergoing bimaxillary orthognathic surgery, with or without adjunctive periodontally accelerated osteogenic orthodontics (PAOO). The authors assessed gingival thickness, keratinized gingiva width, and gingival recession at the mandibular incisors during post-treatment follow-up of up to 12 months [10].
Saab et al. (2023) performed a comparative observational study evaluating gingival recession of mandibular incisors immediately after treatment in Class III patients managed with either compensatory orthodontic treatment or combined orthodontic–orthognathic surgery [11].
Two prospective clinical studies by Weinspach et al. (2011) evaluated the short-term periodontal effects of orthognathic surgery, including bilateral sagittal split osteotomy with or without Le Fort I osteotomy. Both studies reported quantitative periodontal changes, with particular emphasis on early postoperative buccal gingival recession assessed at 6 weeks [12,13].
Ari-Demirkaya et al. (2008) conducted a case–control study examining periodontal changes in the mandibular incisor region following mandibular setback surgery, focusing on the influence of postoperative relapse forces during a follow-up period of 6 to 12 months [14].
Carroll et al. (1992) performed a comparative clinical study assessing long-term periodontal outcomes in patients treated with orthodontics alone versus those receiving combined orthodontic and Le Fort I orthognathic surgery, with follow-up ranging from 1 to 10 years [15].
Finally, Foushee et al. (1985) conducted an observational clinical study evaluating mucogingival changes in the mandibular anterior region following orthognathic surgery, reporting the prevalence of clinically significant gingival recession during a 6- to 12-month post-treatment period [16].
3.3. Gingival Recession Following Combined Treatment
3.3.1. Overall Recession Outcomes
The evidence regarding gingival recession following combined orthodontic–orthognathic treatment is heterogeneous. Liu et al. (2024) found a significant increase in gingival recession in the mandibular incisor region among patients without PAOO adjunctive therapy. In the non-PAOO (NS) group, gingival recession increased by 47.62%, with the odds of recession after orthodontic-orthognathic treatment being 14.77 times higher than in the PAOO group (p < 0.05). Gingival thickness and keratinized gingiva width also decreased significantly in the NS group but increased in the PAOO group [10]. In contrast, Saab et al. (2023) reported no statistically significant difference in gingival recession of mandibular incisors when comparing immediate postsurgical outcomes with compensatory orthodontic treatment alone, suggesting that the orthognathic surgical component per se did not independently increase recession in their cohort [11].
Weinspach et al. (2011) observed significant increases in buccal gingival recession from 0.10 ± 0.16 mm at baseline to 0.31 ± 0.31 mm at six weeks after surgery (p < 0.001), indicating short-term recession changes following surgery [12]. Also, Weinspach et al. (2011) identified, no significant microbiological changes. Between one and six weeks postop, PPD increased on oral sites and GR on buccal sites. In the incision area the development of GR was significantly higher on the test (buccal) than on the control sites (oral). [13]
Ari-Demirkaya et al. (2008) research indicated that decompensation orthodontic movement prior to mandibular setback did not significantly worsen periodontal structures in the short term, and early postoperative relapse forces did not exhibit additional adverse periodontal effects, implying that orthodontic biomechanics may have a larger impact than surgical movements alone [14]. Carroll et al. (1992) identified no significant long-term differences in periodontal status, including gingival recession, when comparing patients treated with orthodontics alone versus those with combined orthognathic therapy, although minor changes in probing depths and attachment level occurred in specific osteotomy subgroups [15]. Foushee et al. (1985) reported that a statistically significant decrease in keratinized and attached gingiva occurred after orthognathic therapy in the mandibular anterior region, and clinically significant recession was present in 6 of 24 patients [16].
3.4. Mandibular Incisor Region
Six of the included studies directly assessed mandibular incisor gingival outcomes (Table 2). Taken together, these studies demonstrate that mandibular incisor recession may occur following combined treatment, particularly where periodontal phenotype is thin or adjunctive periodontal procedures are not performed, but the contribution of the surgical component remains inconsistent across studies.
3.5. Additional Influencing Factors
Several studies identified clinical factors that may influence gingival recession outcomes.Periodontal phenotype variables, such as gingival thickness and alveolar bone dimensions, were significantly associated with recession risk. Multivariate regression in Liu et al. (2024) showed that thin gingiva (<0.72 mm), alveolar bone height >2.36 mm, and bone thickness <0.45 mm were significant predictors of postoperative recession [10]. Orthodontic decompensation (inclination) magnitude and preoperative periodontal conditions in studies examining relapse forces contributed to periodontal variability, but did not uniformly predict recession outcomes [10,11,12,13,14,15,16].
3.6. Risk of Bias and Evidence Certainty
Using the Newcastle–Ottawa Scale (NOS) for observational studies, the methodological quality ranged from moderate to high across included studies, with concerns primarily related to retrospective designs, variability in follow-up durations, and lack of standardized recession measurement methods. Overall certainty of evidence remains low to moderate due to these limitations.

Table 3.
Newcastle–Ottawa Scale assessment for the included studies.
| Study | Selection Bias | Comparability | Outcome Assessment | Follow-Up Adequacy | Overall Risk of Bias |
| Liu et al., 2024 [10] | Low | Low | Low | Low | Low |
| Saab et al., 2023 [11] | Moderate | Moderate | Moderate | Not reported | Moderate |
| Weinspach et al., 2011 [12] | Moderate | Moderate | Moderate | Short-term only | Moderate |
| Weinspach et al., 2011 [13] | Moderate | Moderate | Moderate | Short-term only | Moderate |
| Ari-Demirkaya et al., 2008 [14] | Moderate | Moderate | Moderate | Adequate | Moderate |
| Carroll et al., 1992 [15] | Moderate | Moderate | Moderate | Long-term | Moderate |
| Foushee et al., 1985 [16] | High | Moderate | Moderate | Limited | High |
3.7. Data Synthesis
Due to considerable heterogeneity in outcome definitions, measurement techniques, and follow-up intervals, quantitative meta-analysis was not possible. Therefore, a qualitative synthesis and direction of effect summary were conducted (Table 4).
Across the seven included studies, the presence and extent of gingival recession following combined orthodontic–orthognathic treatment varied according to surgical procedure, adjunctive therapy, and patient-specific factors. Liu et al. (2024) [10] reported that patients undergoing orthodontic–orthognathic treatment without PAOO experienced significantly higher mandibular incisor recession compared with those who received PAOO, who exhibited minimal recession. Saab et al. (2023) [11] found no significant difference in recession between patients who received compensatory orthodontic treatment versus those who underwent surgical treatment, suggesting that surgery per se did not independently increase recession. Weinspach et al. (2011) [12,13] observed small but statistically significant increases in buccal gingival recession following BSSO and/or Le Fort I surgery (from 0.10 ± 0.16 mm at baseline to 0.31 ± 0.31 mm postoperatively).
Long-term outcomes from the Carroll et al. (1992) [15] indicated no significant increase in gingival recession over 1–10 years, although minor localized effects were noted. Similarly, in the study of Foushee et al. (1985) [16], authors reported clinically significant recession in six out of 24 patients, primarily affecting the labial surfaces. In contrast, the Ari-Demirkaya et al. (2008) [14] demonstrated that mandibular setback combined with orthodontic decompensation did not significantly influence incisor recession, highlighting the potential role of orthodontic mechanics rather than surgical movements. Finally, the study of Weinspach et al. [12,13] observed small increases in gingival recession on labial surfaces in the early postoperative period, suggesting a transient effect associated with surgery.
4. Discussion
The present review evaluated the presence and extent of gingival recession (GR) following combined orthodontic–orthognathic treatment. The overall findings indicate that although GR may occur—particularly in the mandibular incisor region—it is not a uniform or inevitable outcome of orthognathic surgery. Instead, recession appears to be influenced by a multifactorial interaction between periodontal phenotype, orthodontic biomechanics, presurgical decompensation, and adjunctive periodontal measures, rather than by the surgical procedure itself [1,3,4].
4.1. Is the Orthodontic–Orthognathic Approach a True Risk Factor?
The question of whether combined orthodontic–orthognathic treatment represents a major risk factor for gingival recession remains controversial. The systematic review by Mota de Paulo et al. [3] reported that gingival recession may be observed following combined treatment. The authors emphasized the heterogeneity of study designs and outcomes and concluded that the available evidence does not allow surgery to be isolated as an independent etiological factor [3]. This conclusion aligns with the findings of Carroll et al. [15] and Ari-Demirkaya et al. [14], both of whom found no clinically significant long-term periodontal deterioration attributable to orthognathic surgery.
This interpretation is further supported by the evidence-based review by Al-Jewair [17], who concluded that orthodontic–orthognathic surgical treatment may not be a major risk factor for gingival recession when appropriate orthodontic control, periodontal assessment, and oral hygiene are ensured. Collectively, these data suggest that recession observed after combined treatment is more likely related to patient-specific and orthodontic variables rather than to orthognathic surgery per se [17].
4.2. Orthodontic Decompensation and Periodontal Limits
A key finding emerging from both the included studies and the external literature is the role of orthodontic decompensation (in particular mandibular incisor repositioning) as a critical determinant of gingival recession risk. Excessive labiolingual movement beyond the alveolar envelope may predispose patients to alveolar bone dehiscence and subsequent recession, especially in individuals with thin periodontal phenotype [3,18].
The study by Demirsoy et al. [18] addressed this issue, demonstrating the development of periodontal bone defects during presurgical orthodontic decompensation in Class III double-jaw surgery patients. These findings support the concept that periodontal compromise may develop before surgery, thereby increasing vulnerability to postoperative recession. This observation is in line with the results of Liu et al. [10], who identified gingival thickness and alveolar bone dimensions as strong predictors of postoperative recession, and demonstrated a protective effect of PAOO in high-risk patients.
4.3. Periodontally Compromised Patients and Multidisciplinary Care
The feasibility of orthodontic–orthognathic treatment in patients with compromised periodontal conditions has also been explored in the literature. Halimi and Zaoui [19] reported successful surgical–orthodontic management of patients with severe periodontal disorders, emphasizing the importance of strict periodontal control, conservative orthodontic mechanics, and interdisciplinary coordination. Although limited by its case-based nature, this study reinforces the notion that periodontal vulnerability does not represent an absolute contraindication to combined treatment when managed appropriately [19].
Similarly, the case report by Liu et al. [2] highlighted the benefits of integrating periodontal phenotype modification into the orthognathic treatment pathway. Their multidisciplinary approach demonstrated improved periodontal stability and reduced risk of recession, supporting current consensus recommendations advocating for periodontal phenotype assessment and modification in high-risk patients [8].
4.4. Surgical Technique and Segmental Osteotomies
More recent studies have demonstrated that orthognathic procedures such as bilateral sagittal split osteotomy and Le Fort I osteotomy may indirectly influence gingival margins by modifying soft tissue tension, muscular attachments, and local vascular supply [21]. Although these changes are generally transient, they may increase susceptibility to marginal tissue displacement in patients with thin gingival biotypes or reduced alveolar thickness [21].
Concerns have been raised regarding the potential periodontal impact of more complex surgical techniques, such as segmental maxillary osteotomies performed in conjunction with bimaxillary surgery. However, available evidence suggests that these procedures are generally safe when proper surgical principles are applied [12,13,20,21].
Case-based and cohort analyses further suggest that mandibular incisors represent a particularly vulnerable region following orthodontic–orthognathic treatment [12,13,20,21]. Retrospective data indicate that gingival recession in this area is more closely associated with postoperative orthodontic tooth positioning and periodontal phenotype than with the surgical procedure itself [2]. This supports the concept that orthognathic surgery acts as a modifying factor rather than a primary etiological agent.
Posnick et al. [20] reported favorable outcomes and acceptable complication rates for segmental maxillary osteotomies, without identifying gingival recession as a frequent or severe adverse outcome. These findings support the view that surgical complexity alone does not necessarily translate into periodontal deterioration.
Short-term studies, such as those by Weinspach et al. [12,13], have documented small but statistically significant increases in buccal gingival recession in the early postoperative period. These changes are likely related to transient surgical trauma and healing dynamics rather than permanent periodontal damage, particularly in the absence of long-term follow-up demonstrating progression. Overall, current evidence indicates that gingival recession following orthodontic–orthognathic treatment is primarily influenced by individual periodontal susceptibility and treatment mechanic [12,13,19,20,21].
According to Liu et al. [2] and Weinspach et al. [12,13], orthognathic surgery has a clear but generally mild causal relationship with gingival recession. The recession is procedure-related rather than disease-driven, predominantly affects buccal sites, and is highly dependent on pre-existing periodontal phenotype. Importantly, periodontal augmentation strategies such as PAOO can significantly mitigate this risk, transforming orthognathic surgery from a periodontal risk factor into a controllable variable.
4.5. Reconciling Conflicting Evidence
The variability in gingival recession outcomes across studies likely reflects differences in baseline periodontal phenotype, orthodontic biomechanics, extent of decompensation, surgical protocols, and follow-up duration [3]. Studies with short-term follow-up may capture transient postoperative changes, whereas long-term investigations tend to show stabilization of periodontal tissues over time. This heterogeneity explains the conflicting conclusions in the literature and justifies the qualitative synthesis approach adopted in the present review [10-16.
Overall, the evidence suggests that gingival recession following combined orthodontic–orthognathic treatment should not be regarded as an unavoidable complication [3,17]. Instead, it should be considered a potentially preventable outcome through careful case selection, controlled orthodontic mechanics, periodontal phenotype assessment, and interdisciplinary treatment planning [3,17].
4.6. Strengths and Limitations
This systematic review followed PRISMA guidelines and applied strict inclusion criteria, focusing exclusively on clinical studies evaluating gingival recession after combined orthodontic–orthognathic treatment. The structured risk-of-bias assessment and comprehensive qualitative synthesis allowed for critical interpretation of both short- and long-term periodontal outcomes. Additionally, integration of contemporary and classical studies provides a broad perspective on evolving clinical concepts.
The primary limitation is the low-to-moderate certainty of evidence, as all included studies were observational in nature. Significant heterogeneity in study design, outcome definitions, follow-up duration, and recession measurement methods precluded quantitative meta-analysis. Furthermore, key modifying factors such as orthodontic force magnitude, incisor torque control, periodontal phenotype, and oral hygiene were inconsistently reported, limiting causal interpretation.
5. Conclusions
Gingival recession may occur following combined orthodontic–orthognathic treatment, but it is not an inevitable outcome. The risk appears to be primarily associated with periodontal phenotype and orthodontic tooth movement, particularly in the mandibular incisor region, rather than orthognathic surgery itself. Careful interdisciplinary planning and periodontal risk assessment may help minimize postoperative recession. Further prospective studies are needed to establish standardized preventive strategies.
Author Contributions
“Conceptualization, A.M. and A.T.; methodology, A.M and A.G..; software, D.S..; validation, O.F and S.B.; formal analysis, A.M. and A.T .; investigation, A.M. and A.T.; resources, A.M. and A.T.; data curation, X.X.; writing—original draft preparation, . A.M. and A.T; writing—review and editing, O.F and S.B visualization, A.G and D.S.; supervision O.F. and B.S.; project administration B.S. All authors have read and agreed to the published version of the manuscript.”.
Funding
No Funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The following supporting information are available from the corresponding author on demand.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Harrington, C.; Gallagher, J.R.; Borzabadi-Farahani, A. A retrospective analysis of dentofacial deformities and orthognathic surgeries using the index of orthognathic functional treatment need (IOFTN). Int. J. Pediatr. Otorhinolaryngol. 2015, 79, 1063–1066. [CrossRef]
- Liu, J.Y.; Li, G.F.; Tang, Y.; Yan, F.H.; Tan, B.C. Multi-disciplinary treatment of maxillofacial skeletal deformities by orthognathic surgery combined with periodontal phenotype modification: A case report. World J. Clin. Cases 2022, 10, 8980–8989. [CrossRef]
- Mota de Paulo, J.P.; Herbert de Oliveira Mendes, F.; Gonçalves Filho, R.T.; Marçal, F.F. Combined Orthodontic-Orthognathic Approach for Dentofacial Deformities as a Risk Factor for Gingival Recession: A Systematic Review. J. Oral Maxillofac. Surg. 2020, 78, 1682–1691. [CrossRef]
- Jepsen, S.; Caton, J.G.; Albandar, J.M.; Bissada, N.F.; Bouchard, P.; Cortellini, P.; Demirel, K.; de Sanctis, M.; Ercoli, C.; Fan, J.; Geurs, N.C.; Hughes, F.J.; Jin, L.; Kantarci, A.; Lalla, E.; Madianos, P.N.; Matthews, D.; McGuire, M.K.; Mills, M.P.; Preshaw, P.M.; Reynolds, M.A.; Sculean, A.; Susin, C.; West, N.X.; Yamazaki, K. Periodontal manifestations of systemic diseases and developmental and acquired conditions: Consensus report of workgroup 3 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89 (Suppl. 1), S237–S248.
- Te Veldhuis, E.C.; Te Veldhuis, A.H.; Bramer, W.M.; Wolvius, E.B.; Koudstaal, M.J. The effect of orthognathic surgery on the temporomandibular joint and oral function: a systematic review. Int. J. Oral Maxillofac. Surg. 2017, 46, 554–563. [CrossRef]
- Junior, O.L.H.; Guijarro-Martínez, R.; Gil, A.P.S.; Meirelles, L.S.; Oliveira, R.B.; Hernández-Alfaro, F. Stability and surgical complications in segmental Le Fort I osteotomy: a systematic review. Int. J. Oral Maxillofac. Surg. 2017, 46, 1071–1087.
- Eslami, S.; Faber, J.; Fateh, A.; Sheikholaemmeh, F.; Grassia, V.; Jamilian, A. Treatment decision in adult patients with class III malocclusion: surgery versus orthodontics. Prog. Orthod. 2018, 19, 28. [CrossRef]
- Kao, R.T.; Curtis, D.A.; Kim, D.M.; et al. American Academy of Periodontology best evidence consensus statement on modifying periodontal phenotype in preparation for orthodontic and restorative treatment. J. Periodontol. 2020, 91, 289–298. [CrossRef]
- Tepedino, M.; Franchi, L.; Fabbro, O.; Chimenti, C. Post-orthodontic lower incisor inclination and gingival recession—a systematic review. Prog. Orthod. 2018, 19, 17. [CrossRef]
- Liu, J.; Xu, X.; Yang, H.F.; Han, Y.; Pan, M.Q.; Xu, L.; Hou, J.X.; Li, X.T. A nomogram prediction of gingival recession in mandibular incisors of orthodontic-orthognathic treated skeletal class III malocclusion with or without PAOO: A retrospective cohort study. Heliyon 2024, 10, e33478.
- Saab, F.J.S.; Freitas, K.M.S.; [et al.]. Comparison of gingival recession of mandibular incisors of Class III patients immediately after compensatory or surgical orthodontic treatment. Eur. J. Dent. 2023, 17, 1089–1096.
- Weinspach, K.; [et al.]. Influence of orthognathic surgery on periodontal tissues. Int. J. Periodontics Restor. Dent. 2011, 31, 165–172.
- Weinspach, K.; [et al.]. Short-term periodontal and microbiological changes following orthognathic surgery. J. Orofac. Orthop. 2011, 72, 97–105.
- Ari-Demirkaya, A.; Ilhan, I. Effects of relapse forces on periodontal status of mandibular incisors following orthognathic surgery. J. Periodontol. 2008, 79, 2210–2217.
- Carroll, W.J.; Haug, R.H.; Bissada, N.F.; Goldberg, J.; Hans, M.G. The effects of the Le Fort I osteotomy on the periodontium. J. Oral Maxillofac. Surg. 1992, 50, 1190–1196.
- Foushee, D.L.; [et al.]. Effects of mandibular orthognathic treatment on mucogingival tissues. J. Periodontol. 1985, 56, 467–472.
- Al-Jewair, T. Orthodontic–orthognathic surgical treatment may not be a major risk factor for gingival recession. J. Evid.-Based Dent. Pract. 2021, 21, 101613. [CrossRef]
- Demirsoy, K.K.; Ertürk, E.; Gümüş, H.; et al. How much should incisors be decompensated? Periodontal bone defects during presurgical orthodontic treatment in Class III double-jaw orthognathic surgery patients. J. Stomatol. Oral Maxillofac. Surg. 2022, 123, e133–e139.
- Halimi, A.; Zaoui, F. Surgical–orthodontic treatment of patients suffering from severe periodontal disorders—A clinical case study. Int. Orthod. 2013, 11, 314–332. [CrossRef]
- Posnick, J.C.; Fantuzzo, J.J.; Troost, T. Segmental Maxillary Osteotomies in Conjunction with Bimaxillary Orthognathic Surgery: Indications—Safety—Outcome. J. Oral Maxillofac. Surg. 2016, 74, 1422–1440. [CrossRef]
- Mirabella, D.; Macca, U.; Pancari, C.; Giunta, G.; Lombardo, L. Detailed three-dimensional orthodontic tooth repositioning to improve restorative outcome. Angle Orthod. 2022, 92, 415–425. [CrossRef]
Figure 1.
Prisma flow chart.
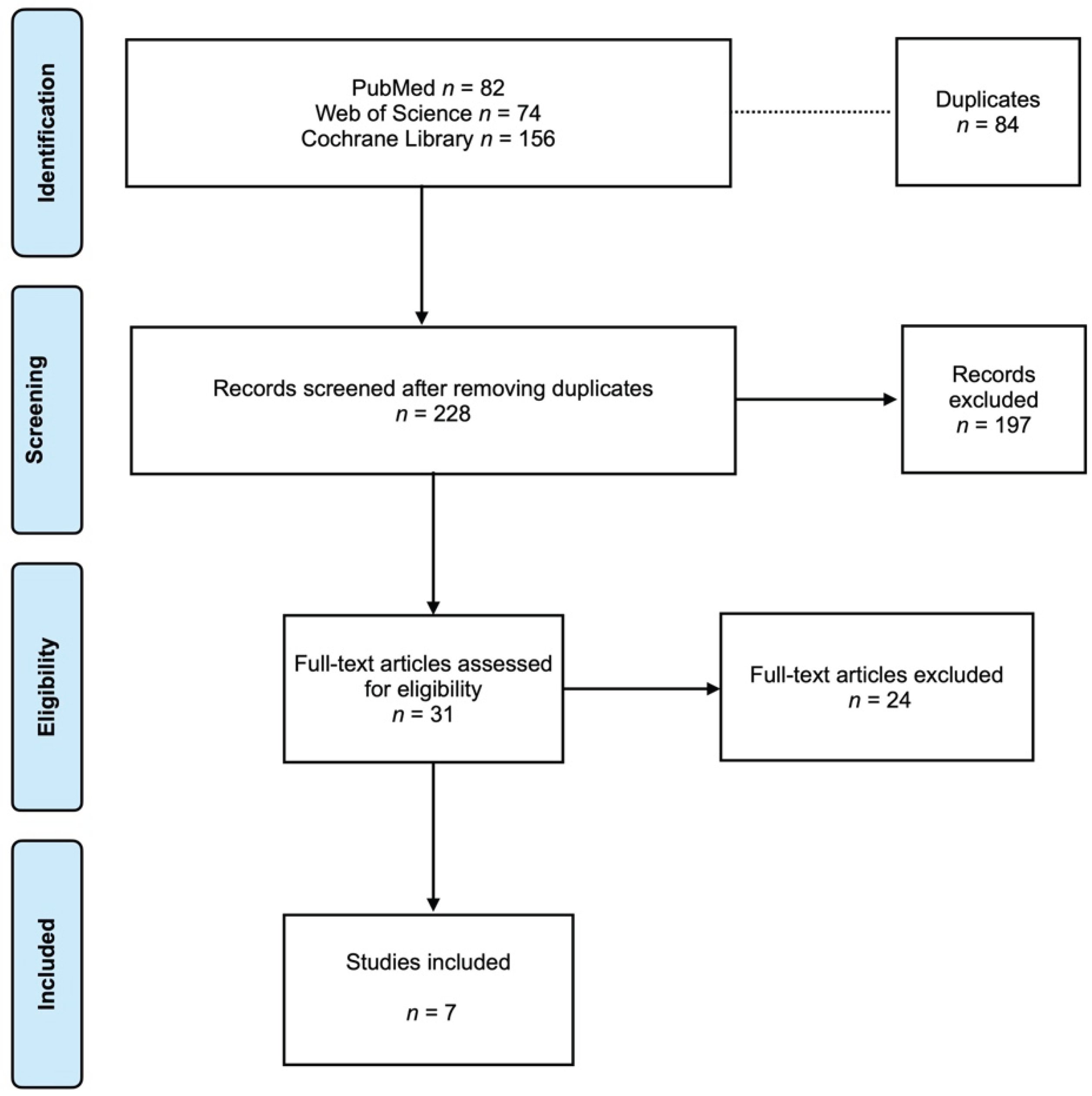
Table 1.
Characteristics of Included Studies.
| Study | Study Design | Sample Size | Type of Orthognathic Surgery | Orthodontic Phase Evaluated | Follow-Up Duration | Tooth Region Assessed | Baseline Periodontal Status Reported | Main Gingival Recession Outcome |
| Liu et al., 2024 [10] | Retrospective cohort | 33 patients (131 mandibular incisors) | Bimaxillary orthognathic surgery ± PAOO | Post-treatment | Up to 12 months | Mandibular incisors | Yes | Significantly higher GR in non-PAOO group |
| Saab et al., 2023 [11] | Comparative observational | Not reported | Orthognathic surgery vs compensatory orthodontics | Immediate post-treatment | Immediate | Mandibular incisors | Not reported | No significant difference between groups |
| Weinspach et al., 2011 [12] | Prospective clinical study | 15 patients | BSSO ± Le Fort I | Early postoperative | 6 weeks | Buccal and oral surfaces | Yes | Small but significant increase in buccal GR |
| Weinspach et al., 2011 [13] | Prospective clinical study | 15 patients | BSSO ± Le Fort I | Early postoperative | 6 weeks | Buccal and oral surfaces | Yes | Transient buccal GR increase post-surgery |
| Ari-Demirkaya et al., 2008 [14] | Case–control | 36 patients | Mandibular setback surgery | Post-treatment | 6–12 months | Mandibular incisors | Yes | No significant effect of relapse forces on GR |
| Carroll et al., 1992 [15] | Comparative clinical study | 40 patients | Le Fort I ± orthodontics | Long-term post-treatment | 1–10 years | Anterior dentition | Not reported | No clinically significant long-term GR |
| Foushee et al., 1985 [16] | Observational clinical study | 24 patients | Mandibular orthognathic surgery | Post-treatment | 6–12 months | Mandibular anterior region | Not reported | Clinically significant GR in 6 patients |
Table 2.
Mandibular incisor recession outcome.
| Study | Recession Outcome |
| Liu et al. (2024) [10] | Significantly higher recession in NS compared to PAOO group post-treatment |
| Saab et al. (2023) [11] | No significant difference between compensatory and surgical groups |
| Weinspach et al. (2011) [13] | Small but statistically significant buccal recession post-surgery |
| Ari-Demirkaya et al. (2008) [14] | No significant effect of relapse on recession |
| Carroll et al. (1992) [15] | No clinically significant increase long term |
| Foushee et al. (1985) [16] | Clinically significant recession in subset |
Table 4.
Summary of Gingival Recession Outcomes.
| Study | Surgical Procedure | Follow-Up Duration | Tooth Region | Direction of Gingival Recession | Magnitude of Recession | Timing of Detection | Key Risk Modifier Identified |
| Liu et al., 2024 [10] | Bimaxillary ± PAOO | ≤12 months | Mandibular incisors | ↑ Increase (non-PAOO); ↔ Stable (PAOO) | Clinically relevant | Post-treatment | Thin phenotype; absence of PAOO |
| Saab et al., 2023 [11] | Orthognathic vs compensatory | Immediate | Mandibular incisors | ↔ No significant change | Not reported | Immediate post-treatment | None identified |
| Weinspach et al., 2011 [12] | BSSO ± Le Fort I | 6 weeks | Buccal surfaces | ↑ Increase | ~0.2 mm (mean) | Early postoperative | Surgical site proximity |
| Weinspach et al., 2011 [13] | BSSO ± Le Fort I | 6 weeks | Buccal surfaces | ↑ Increase | Small, statistically significant | Early postoperative | Surgical trauma (transient) |
| Ari-Demirkaya et al., 2008 [14] | Mandibular setback | 6–12 months | Mandibular incisors | ↔ No significant change | Not clinically significant | Post-treatment | None identified |
| Carroll et al., 1992 [15] | Le Fort I ± orthodontics | 1–10 years | Anterior teeth | ↔ Stable | Clinically insignificant | Long-term | None identified |
| Foushee et al., 1985 [16] | Mandibular orthognathic surgery | 6–12 months | Mandibular anterior region | ↑ Increase (subset) | Clinically significant in 6/24 | Post-treatment | Reduced keratinized gingiva |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



