Submitted:
26 January 2026
Posted:
27 January 2026
You are already at the latest version
Abstract
Background: Care partners play a critical role in supporting physical activity among older adults. This study assesses how care partners’ attitudes to and engagement in physical activity relate to their perceived benefits of exercise for older adults. Methods: For this cross-sectional study, 305 care partners completed validated surveys on the perceived benefits of physical activities among older adults (outcome), attitudes towards, and practices of physical activities (predictors). For all three surveys, higher scores indicate greater perceived benefit, more positive attitudes, and greater engagement in physical activities. We assessed the relationship between the predictor and outcome variables using multivariable quantile regression models adjusted for sociodemographic, caregiving, and health-related covariates. We reported the adjusted median difference (aMD) and 95% confidence intervals (CI). Results: The population was predominantly young adults (18-34 years, 58%), female (53%), who had been providing caregiving services for three or more years (43%). The median perceived physical activity benefit for older adults, personal attitude toward physical activity, and physical activity practice scale scores were 60.0 (52.0 – 66.0), 29.0 (25.0 – 33.0), and 33.0 (28.0 – 39.0), respectively. After adjusting for covariates, a unit increase in both attitude towards physical activity (aMD: 1.14; 95% CI: 0.96 – 1.33) and physical activity practice (aMD: 0.60; 95% CI: 0.45 – 0.75) was associated with increased median score of perceived benefit of physical activity among older adults. Conclusion: Care partners with positive attitudes and greater engagement in their personal physical activity perceive physical activities as beneficial for older adults.
Keywords:
care partners
; older adults
; physical activity
; perception
; attitude
; practice
; knowledge
1. Introduction
Regular physical activity and exercise (hereafter referred to as physical activity) is one of the most effective strategies for maintaining health, independence, and quality of life in older adults [1,2]. Physical activity reduces the risk and severity of chronic diseases [3,4], preserves mobility and cognitive function [5,6], prevents falls [7], and lowers mortality [8,9,10]. Despite these well-documented benefits, physical activity and exercise remain markedly low among older adults [8].
Care partners, defined as family members, neighbors, or friends who assist older adults with daily activities [11], play a critical role in influencing health behaviors among care recipient older adults, including physical activity [12,13]. Their perceptions and beliefs on physical activity and exercise may influence the care recipients’ knowledge, attitudes toward, and engagement in physical activity and exercise. A positive care partner’s view of engagement in physical activity and exercise may influence the care recipient’s perception of these activities as feasible, safe, or worth prioritizing. On the other hand, a care partner’s negative attitude toward physical activity may dissuade the care recipient from engaging in it.
One way to evaluate care partners’ attitudes and practices regarding physical activity is through the Knowledge, Attitudes, and Practices (KAP) behavioral model. The KAP model, widely applied across multiple health behavior domains [14,15,16,17,18,19,20,21,22], posits that individuals first acquire knowledge, which then shapes their attitudes and ultimately informs their practices [23]. Although the KAP model traditionally assumes that knowledge influences attitudes, which in turn influence practices [23], a dyadic framework introduces an additional mechanism. Individuals may generalize the benefits or harms they personally experience and project them onto their dyadic partners [24]. Specifically, within a care partner–care recipient framework, care partners’ experiential benefits, shaped by their own knowledge of, attitudes toward, and engagement in physical activity, may inform their perceptions of the potential benefits of their care recipients’ engagement in physical activity.
This study, therefore, centers on a key yet underexplored question: Do care partners with more positive attitudes toward and greater engagement in physical activity view such activities as beneficial for their older care recipients? Understanding how care partners’ attitudes and practices shape their perceptions of the benefits of physical activity for older adults can inform interventions to promote physical activity among older adults. The aim of this study, therefore, is to assess how care partners’ attitudes towards and engagement in physical activities relate to their perceived benefits of physical activities for older adults. We hypothesized that higher attitudinal and practice scores among care partners would be associated with higher perceived benefits of physical activity for older adults.
2. Materials and Methods
Study Design and Participants
We conducted a cross-sectional online survey study of care partners of older adults enrolled in the pilot and validation phase of the Activity Tracking, Care Partner Co-Participation, Text Reminders, Instructional Education, Virtual Physical Therapy, and Exercise (ACTIVE) study. Study participants were recruited through ResearchMatch, a national online registry supported by the National Institutes of Health that connects individuals interested in research with investigators [25]. Recruitment notices were distributed via the platform’s email listserv, and eligible participants who consented to participate completed the survey. All data were collected using REDCap, a secure, web-based data management system [26].
Eligibility Criteria
Care partners were eligible if they were aged 18 years or older, provided ongoing, unpaid support to an older adult aged 65 years or older, could read English, and had internet access to complete the survey. The exclusion criteria included individuals who served in a formal or paid caregiving capacity and those who indicated difficulty completing the online questionnaire due to cognitive, sensory, or communication limitations.
Outcome Variable
The main outcome was the physical activity benefits for older adults, assessed using the Perceived Physical Activity Benefits for Older Adults survey instrument (Appendix Table A1). The survey instrument comprises 14 items that assess understanding of the health, functional, and cognitive benefits, as well as awareness of exercise guidelines for older adults. The instrument, scored from 14 to 70, has been validated among care partners and demonstrates strong internal consistency in (Cronbach alpha (α) = 0.88). Higher scores reflected greater perceived benefit of exercise for older adults.
Predictor Variables
Our predictor variables were attitude towards physical activity and physical activity engagement (Appendix Table A1). Attitude was measured using the Attitude toward Physical Activity Scale, a seven-item survey, scored from 7 to 35. Practice was measured using the Physical Activity Practice Scale, a nine-item survey scored from 9 to 45. Both instruments have been validated among care partners of older adults, and they exhibited good internal consistency (Attitude Scale: α = 0.86; Practice Scale: α = 0.76). Higher scores for both attitude and practice measures reflect more favorable attitudes and greater engagement in physical activity, respectively.
Potential Confounders
We adjusted for sociodemographic, caregiving, and health characteristics. Sociodemographic characteristics included age, sex, race/ethnicity, educational attainment, and marital status. Caregiving characteristics included relationship with care recipient (spouse, child/sibling, other relatives, and friend/neighbor), co-residence with the older adult, duration of caregiving (less than a year, 1 -2 years, and 3 or more years), and hours of caregiving per week (less than 10 hours, 10 – 19 hours, 20 – 39 hours, 40 hours or more). Health characteristics included self-rated health (fair/poor, good, very good/excellent) and the Charlson comorbidity index, a predictor of 10-year mortality, computed from 16 chronic diseases [27,28]. We computed the Charlson comorbidity index as a weighted sum of chronic diseases, ranging from 0 to 24, consistent with prior studies [29,30], and defined it as a continuous variable.
Missing Data
A total of 329 eligible care partners consented to participate in the survey, but 24 did not complete it. We deleted these 24 respondents because missingness was not at random [31], and large portions of the survey were unanswered. All remaining 305 respondents completed the survey.
Data Analysis
We reported the means and standard deviations (SD) and median and interquartile ranges (Q1, Q3) for continuous variables and frequencies and proportions for categorical variables. Of note, the perceived physical activity benefit score exhibited a non-normal distribution. Hence, for the bivariate association, we reported the median (Q1, Q3) distribution of the perceived physical activity benefit score across all categorical variables and assessed differences using Mann-Whitney U and Kruskal-Wallis tests. We created two separate multivariable models – a perceived benefit – attitude model (model 1) and a perceived benefit – practice model (model 2). We performed multivariable quantile regressions for each model to assess how care partners' attitudes towards and engagement in physical activity are associated with their perceived benefits of physical activity among older adults. For each model, we controlled for potential confounders and reported the adjusted median difference (aMD) and 95% confidence intervals (CI). All analyses were performed using Stata version 16 [32].
Ethical Considerations
The study protocol was approved by the NYU Langone Health Institutional Review Board (IRB# i25-00450; 08/21/2025). All participants provided electronic informed consent prior to participation. Study procedures adhered to ethical principles for human research and complied with institutional and federal guidelines.
3. Results
A total of 305 care partners participated in the study. The population was predominantly aged 18–34 years (58%), female (53%), non-Hispanic White (35%), married (78%), with college degrees (56%) (Table 1). Most of the care partners were spouses (28%), children or siblings (10%), or other family members (37%) of the older care recipients. Also, most of the care partners live with their older care recipient (80%), provide 10–19 hours of caregiving per week (35%), and have been caring for their older care recipient for three or more years (43%). Also, most of the care partners had no comorbid conditions (84%), and 77% rated their health as very good or excellent. The median (IQR) Physical Activity Benefit Scale score was 60.0 (52.0 – 66.0) while the Attitude towards Physical Activity Scale and Physical Activity Practice Scale scores were 29.0 (25.0 – 33.0) and 33.0 (28.0 – 39.0), respectively.
Several sociodemographic and caregiving characteristics were significantly associated with the Physical Activity Benefit Scale score, with higher scores among care partners aged 18–34 years (p<0.001), non-Hispanic Blacks (p < 0.001), and those with graduate degrees (p < 0.001) (Table 2). Significant bivariate relationships were also observed with marital status (p = 0.003), relationship with the care recipient (p = 0.002), hours per week spent on caregiving (p < 0.001), comorbidity index (p < 0.001), and self-rated health (p < 0.001).
After adjusting for potential confounders in the Perceived Benefit – Attitude model, a unit increase in the Attitude towards Physical Activity score was associated with a significant increase in the median difference in Perceived Physical Activity Benefit score (Model 1; aMD: 1.17; 95% CI: 0.99 – 1.35, Table 3). Also, after adjusting for potential confounders in the Perceived Benefit – Practice model, a unit increase in the Physical Activity Practice score was associated with a significant increase in the median difference in Perceived Physical Activity Benefit (Model 2; aMD: 0.60; 95% CI: 0.45 – 0.75). The predicted Physical Activity Benefit score increased linearly with every unit increase in the attitude (Figure 1A) and the practice scores (Figure 1B).
4. Discussion
In this cross-sectional study of care partners, we found that individuals who reported more positive attitudes toward physical activity and greater personal engagement in exercise were also more likely to endorse stronger beliefs in the benefits of physical activity for older adults. These findings suggest that care partners’ own behaviors and attitudes may reinforce their understanding of the value of physical activity, potentially influencing how they encourage, model, or facilitate physical activity for older care recipients [33].
Prior research has identified a range of factors that influence older adults’ physical activity. These include but are not limited to clinical factors (such as chronic medical conditions, pain, and functional limitations) [34,35,36,37], psychological factors (such as knowledge, attitudes, self-efficacy, motivation, and fear of falling) [38,39], and environmental factors (such as neighborhood safety and walkability, access to parks and gyms, home environment, weather, and transportation [39,40,41,42].
Care partner encouragement and exercise behavior modeling have also been identified as important facilitators of older adults’ engagement in physical activity [43]. Our findings extend this literature by highlighting that not only do older adults’ own attitudes matter, but the attitudes and behaviors of the people who support them may play a complementary role.
A conceptual explanation may account for how care partners’ attitudes and engagement in physical activity associate with their perceived benefits of exercise among older adults. Care partners who regularly participate in physical activity are directly exposed to its benefits, which can shape their beliefs about exercise and its value for themselves and potential benefits for their older adult care recipient. Likewise, those with positive attitudes toward physical activities may be more likely to pay attention to information on the benefits of physical activity among older adults. In this way, a care partner’s own attitudes and practices are both behavioral expressions of self-acquired knowledge, consistent with the KAP model [23], and serve as meaningful predictors of perceived benefits of physical activity among older adults, which may then influence behavioral change among their older adult care recipients.
These findings have several implications. First, promoting physical activity among older adults may require leveraging the presence of care partners with positive attitudes towards and engagement in physical activity. Secondly, interventions that enhance care partners’ knowledge, foster positive attitudes, and encourage their own engagement in exercise may strengthen older care recipients’ participation in physical activity [44,45]. Third, clinicians’ and health educators’ encouragement is an important motivational factor in older adults’ engagement in physical activity [46,47]. Incorporating care partners with positive attitudes and strong engagement in physical activity into counseling and activity planning may further strengthen older adults’ motivation to participate. More broadly, programs that promote caregiver wellness, facilitate active lifestyles, and reduce barriers to physical activities may produce ripple effects that extend to both older adults and their care partners.
Our study has its limitations. Our cross-sectional design does not permit causal inference. Our sample was recruited from an online registry, which may overrepresent individuals with greater interest in health research or higher digital literacy, thereby limiting generalizability. All measures were self-reported and, therefore, susceptible to self-report and social desirability bias [48,49]. Although we controlled for sociodemographic, health, and care partner-care recipient measures, other measures, such as broader social network, community or environmental supports, and access to caregiving resources, may influence care partners’ perceived benefits of exercise among older adults. Despite these limitations, our study represents one of the few studies that provides insights into how care partners’ attitudes towards and engagement in physical activities associate with their perceived physical activity benefits among older adults.
5. Conclusions
Care partners who hold more favorable attitudes toward physical activity and engage in it are more likely to perceive it as highly beneficial for older adults. These findings highlight the intertwined nature of caregiver and care recipient health behaviors and suggest that strategies and interventions that promote physical activity in older adults may be strengthened by addressing the beliefs and practices of their care partners.
Author Contributions
Conceptualization, O.A.; Methodology, O.A.; Software, O.A., J.C.; Formal Analysis, O.A.; Data Curation, O.A.; Writing – Original Draft Preparation, O.A.; Writing – Review & Editing, O.A., T.C., G.O., D.B., J.C.; Visualization, O.A.; Supervision, J.C.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was reviewed and approved by the NYU Langone Health Institutional Review Board (IRB#: i25-00450; 08/21/2025).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The original data presented in the study are openly available in FigShare at 10.6084/m9.figshare.30801278.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| PBAS | Perceived Physical Activity Benefit Scale for older adults |
| APAS | Attitude towards Physical Activity Scale |
| PAPS | Physical Activity Practice Scale |
| ACTIVE | Activity Tracking, Care Partner Co-Participation, Text Reminders, Instructional Education, Virtual Physical Therapy, and Exercise |
| KAP | Knowledge, Attitudes, and Practices |
| aMD | Adjusted Median Difference |
| CI | Confidence Interval |
Appendix A

Table A1.
List of the items in the Perceived Physical Activity Benefit Scale for older adults, Attitude towards Physical Activity Scale, and Physical Activity Practice Scale .
Table A1.
List of the items in the Perceived Physical Activity Benefit Scale for older adults, Attitude towards Physical Activity Scale, and Physical Activity Practice Scale .
| Perceived Physical Activity Benefits Scale (PABS) |
|---|
| Regular physical activity is essential for maintaining good health in older adults. |
| Older adults who engage in physical activity experience improved quality of life. |
| Exercise helps older adults maintain independence in daily activities. |
| Engaging in regular exercise reduces the risk of premature death in older adults. |
| The benefits of exercise outweigh the risks for most older adults. |
| Regular physical activity improves heart health and reduces the risk of cardiovascular disease. |
| Strength training exercises help prevent osteoporosis and maintain bone health. |
| Exercise can reduce the risk of falls by improving strength and balance. |
| Regular exercise enhances cognitive function and reduces the risk of dementia. |
| Physical activity can help manage chronic conditions such as diabetes and arthritis. |
| Older adults should engage in at least 150 minutes of moderate-intensity physical activity per week. |
| Strength training exercises should be performed at least twice a week for older adults. |
| Even light-intensity activities, such as walking, provide significant health benefits for older adults. |
| It is never too late for older adults to start exercising and gain health benefits. |
| Attitude Towards Physical Activities Scale (APAS) |
| I enjoy engaging in physical activity. |
| Exercise is an important part of a healthy lifestyle. |
| I feel motivated to exercise regularly. |
| I believe I can still benefit from exercise regardless of my age. |
| Exercising with others makes it more enjoyable for me. |
| I would be more likely to exercise if I had proper guidance. |
| Encouragement from family or friends increases my likelihood of exercising. |
| Physical Activity Practice Scale (PAPS) |
| I engage in physical activity at least 3 times a week. |
| I perform strength-training exercises at least twice a week. |
| I engage in moderate-to-vigorous physical activity for at least 150 minutes per week. |
| I incorporate light physical activities (e.g., walking, stretching) into my daily routine. |
| I participate in group-based or social exercise programs. |
| I do balance or flexibility exercises to prevent falls. |
| I track my physical activity levels using a device or app. |
| My healthcare provider has advised me (or the older adult I care for) to exercise regularly. |
| I (or the older adult I care for) follow an exercise plan or routine. |
References
- Langhammer, B.; Bergland, A.; Rydwik, E. The Importance of Physical Activity Exercise among Older People. Biomed Res Int 2018, 2018, 7856823. [Google Scholar] [CrossRef] [PubMed]
- WHO. Physical activity. Available online: https://www.who.int/news-room/fact-sheets/detail/physical-activity.
- Anderson, E.; Durstine, J.L. Physical activity, exercise, and chronic diseases: A brief review. Sports Med Health Sci 2019, 1, 3–10. [Google Scholar] [CrossRef]
- Booth, F.W.; Roberts, C.K.; Laye, M.J. Lack of exercise is a major cause of chronic diseases. Compr Physiol 2012, 2, 1143–1211. [Google Scholar] [CrossRef]
- Zhao, E.; Tranovich, M.J.; Wright, V.J. The role of mobility as a protective factor of cognitive functioning in aging adults: a review. Sports Health 2014, 6, 63–69. [Google Scholar] [CrossRef]
- Martín-Rodríguez, A.; Dalamitros, A.A.; Madrigal-Cerezo, R.; Sánchez-Conde, P.; Clemente Suárez, V.J.; Tornero Aguilera, J.F. Move to Remember: The Role of Physical Activity and Exercise in Preserving and Enhancing Cognitive Function in Aging—A Narrative Review. Geriatrics 2025, 10, 143. [Google Scholar] [CrossRef]
- NIH. Falls and Fractures in Older Adults: Causes and Prevention. Available online: https://www.nia.nih.gov/health/falls-and-falls-prevention/falls-and-fractures-older-adults-causes-and-prevention.
- Adeyemi, O.; Chippendale, T.; Ogedegbe, O.; Boatright, D.; Chodosh, J. Activity Intensity and All-Cause Mortality Following Fall Injury Among Older Adults: Results from a 12-Year National Survey. Healthcare 2025, 13. [Google Scholar] [CrossRef] [PubMed]
- Leitzmann, M.F.; Park, Y.; Blair, A.; Ballard-Barbash, R.; Mouw, T.; Hollenbeck, A.R.; Schatzkin, A. Physical Activity Recommendations and Decreased Risk of Mortality. Archives of Internal Medicine 2007, 167, 2453–2460. [Google Scholar] [CrossRef]
- Martínez-Vizcaíno, V.; Fernández-Rodríguez, R.; Reina-Gutiérrez, S.; Rodríguez-Gutiérrez, E.; Garrido-Miguel, M.; Núñez de Arenas-Arroyo, S.; Torres-Costoso, A. Physical activity is associated with lower mortality in adults with obesity: a systematic review with meta-analysis. BMC Public Health 2024, 24, 1867. [Google Scholar] [CrossRef] [PubMed]
- Schulz, R.; Beach, S.R.; Czaja, S.J.; Martire, L.M.; Monin, J.K. Family Caregiving for Older Adults. Annu Rev Psychol 2020, 71, 635–659. [Google Scholar] [CrossRef]
- Kim, E.; Ullrich-French, S.; Bolkan, C.; Hill, L.G. The Role of Caregivers in Physical Activity for Older Adults With Alzheimer’s Disease. American Journal of Alzheimer's Disease & Other Dementias® 2018, 33, 122–130. [Google Scholar] [CrossRef]
- Liu, C.K.; Seo, J.; Lee, D.; Wright, K.; Tamura, M.K.; Moye, J.; Weiner, D.E.; Bean, J.F. The Impact of Care Partners on the Mobility of Older Adults Receiving Hemodialysis. Kidney Medicine 2022, 4, 100473. [Google Scholar] [CrossRef]
- Adeyemi, O. An Assessment of the Knowledge, Attitude, and Practice of Phone Use While Driving and Crash Outcomes Among Drivers in Oyo State, Nigeria. International Research and Review 2022, 25. [Google Scholar]
- Adeyemi, O.J.; Siman, N.; Goldfeld, K.S.; Cuthel, A.M.; Bouillon-Minois, J.B.; Grudzen, C.R. Emergency Providers' Knowledge and Attitudes Toward Hospice and Palliative Care: A Cross-Sectional Analysis Across 35 Emergency Departments in the United States. J Palliat Med 2023. [Google Scholar] [CrossRef] [PubMed]
- Alsaad, S.M.; Alabdulwahed, M.; Rabea, N.M.; Tharkar, S.; Alodhayani, A.A. Knowledge, Attitudes, and Practices of Nurses toward Risk Factors and Prevention of Falls in Older Adult Patients in a Large-Sized Tertiary Care Setting. Healthcare (Basel) 2024, 12. [Google Scholar] [CrossRef]
- Bachani, A.M.; Risko, C.B.; Gnim, C.; Coelho, S.; Hyder, A.A. Knowledge, attitudes, and practices around drinking and driving in Cambodia: 2010-2012. Public health 2017, 144s, S32–s38. [Google Scholar] [CrossRef]
- Maduakolam, I.O.; Osude, C.P.; Ede, S.S.; Onyekachi-Chigbu, A.C.; Osuorah, C.S.; Okoh, C.F. Knowledge, Attitude and Practice of Physical Exercise Among Elderly People in Enugu Metropolis, Nigerian. Physical Activity and Health 2023. [Google Scholar] [CrossRef]
- Shamsipour, M.; Khajehkazemi, R.; Haghdoost, A.A.; Setayesh, H.; KarimanMajd, S.; Mostafavi, E. Knowledge, Attitude, and Practice of Clerical Students with Respect to HIV/AIDS in Iran, 2011. Journal of religion and health 2016, 55, 26–37. [Google Scholar] [CrossRef]
- Sun, T.; Zhang, H.; Kong, Z.; Yang, J.; Jia, X. Knowledge, attitude, and practice of body shape and fitness among university students in China. BMC Public Health 2023, 23, 1208. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Wang, W.; Zhao, J.; Wang, J.; Zhao, T. Knowledge, attitude, and practice of healthcare professionals toward clinically applying graduated compression stockings: results of a Chinese web-based survey. Journal of thrombosis and thrombolysis 2019, 47, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Laing, S.S.; Silver, I.F.; York, S.; Phelan, E.A. Fall prevention knowledge, attitude, and practices of community stakeholders and older adults. J Aging Res 2011, 2011, 395357. [Google Scholar] [CrossRef]
- Gumicio, S.; Merica, M.; Luhman, N.; Fauvel, G.; Zompi, S.; Ronsse, A. The KAP Survey Model (Knowledge, Attitudes & Practices). Available online: https://issuu.com/medecinsdumonde/docs/47-the-kap-survey-model-knowledge-a.
- Robbins, J.M.; Krueger, J.I. Social projection to ingroups and outgroups: a review and meta-analysis. Pers Soc Psychol Rev 2005, 9, 32–47. [Google Scholar] [CrossRef]
- ResearchMatch. What is ResearchMatch? Available online: https://www.researchmatch.org/ (accessed on 11/22/2025).
- Harris, P. Research Electronic Data Capture (REDCap). Journal of the Medical Library Association 2018. [Google Scholar] [CrossRef]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. Journal of Clinical Epidemiology 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Charlson, M.E.; Carrozzino, D.; Guidi, J.; Patierno, C. Charlson Comorbidity Index: A Critical Review of Clinimetric Properties. Psychotherapy and psychosomatics 2022, 91, 8–35. [Google Scholar] [CrossRef] [PubMed]
- Adeyemi, O.J.; Meltzer-Bruhn, A.; Esper, G.; DiMaggio, C.; Grudzen, C.; Chodosh, J.; Konda, S. Crosswalk between Charlson Comorbidity Index and the American Society of Anesthesiologists Physical Status Score for Geriatric Trauma Assessment. Healthcare 2023, 11. [Google Scholar] [CrossRef]
- Konda, S.R.; Dedhia, N.; Ranson, R.A.; Tong, Y.; Ganta, A.; Egol, K.A. Loss of Ambulatory Level and Activities of Daily Living at 1 Year Following Hip Fracture: Can We Identify Patients at Risk? Geriatric Orthopaedic Surgery and Rehabilitation 2021, 12. [Google Scholar] [CrossRef]
- Fox-Wasylyshyn, S.M.; El-Masri, M.M. Handling missing data in self-report measures. Res Nurs Health 2005, 28, 488–495. [Google Scholar] [CrossRef]
- StataCorp Stata Statistical Software: Release 16. StataCorp LLC: College Station, TX, 2017.
- Zeng, X.; Card, A.; Choi, N.G.; Zhou, Y. Care Partner Engagement in Fall Risk Management Programs for Community-Dwelling Older People with Cognitive Impairment: A Systematic Review. Clin Interv Aging 2025, 20, 2195–2217. [Google Scholar] [CrossRef] [PubMed]
- Angulo, J.; El Assar, M.; Álvarez-Bustos, A.; Rodríguez-Mañas, L. Physical activity and exercise: Strategies to manage frailty. Redox Biol 2020, 35, 101513. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Maurya, P.; Muhammad, T. Number of chronic conditions and associated functional limitations among older adults: cross-sectional findings from the longitudinal aging study in India. BMC geriatrics 2021, 21, 664. [Google Scholar] [CrossRef]
- Fisher, K.; Griffith, L.E.; Gruneir, A.; Kanters, D.; Markle-Reid, M.; Ploeg, J. Functional limitations in people with multimorbidity and the association with mental health conditions: Baseline data from the Canadian Longitudinal Study on Aging (CLSA). PLOS ONE 2021, 16, e0255907. [Google Scholar] [CrossRef]
- Gates, M.L.; Hunter, E.G.; Dicks, V.; Jessa, P.N.; Walker, V.; Yoo, W. Multimorbidity patterns and associations with functional limitations among an aging population in prison. Archives of Gerontology and Geriatrics 2018, 77, 115–123. [Google Scholar] [CrossRef]
- Lee, Y.-H.; Fan, S.-Y. Psychosocial and environmental factors related to physical activity in middle-aged and older adults. Scientific reports 2023, 13, 7788. [Google Scholar] [CrossRef]
- Meredith, S.J.; Cox, N.J.; Ibrahim, K.; Higson, J.; McNiff, J.; Mitchell, S.; Rutherford, M.; Wijayendran, A.; Shenkin, S.D.; Kilgour, A.H.M.; et al. Factors that influence older adults' participation in physical activity: a systematic review of qualitative studies. Age Ageing 2023, 52. [Google Scholar] [CrossRef] [PubMed]
- Palombi, T.; Chirico, A.; Cazzolli, B.; Zacchilli, M.; Alessandri, G.; Filosa, L.; Borghi, A.; Fini, C.; Antoniucci, C.; Pistella, J.; et al. Motivation, psychological needs and physical activity in older adults: a qualitative review. Age and Ageing 2025, 54, afaf180. [Google Scholar] [CrossRef] [PubMed]
- Park, C.H.; Elavsky, S.; Koo, K.M. Factors influencing physical activity in older adults. J Exerc Rehabil 2014, 10, 45–52. [Google Scholar] [CrossRef]
- Zhou, F.; Zhang, H.; Wang, H.Y.; Liu, L.F.; Zhang, X.G. Barriers and facilitators to older adult participation in intergenerational physical activity program: a systematic review. Aging Clinical and Experimental Research 2024, 36, 39. [Google Scholar] [CrossRef]
- Kim, E.; Ullrich-French, S.; Bolkan, C.; Hill, L.G. The Role of Caregivers in Physical Activity for Older Adults With Alzheimer's Disease. American journal of Alzheimer's disease and other dementias 2018, 33, 122–130. [Google Scholar] [CrossRef]
- Cardoso, C.; Lumini, M.J.; Martins, T. Effects of physical exercise in reducing caregivers burden: a systematic review. Front Public Health 2025, 13, 1474913. [Google Scholar] [CrossRef] [PubMed]
- Marshall, E.; LaCaille, R.A.; LaCaille, L.J.; Lee, J.E.; Peterson, E. Effects of physical activity interventions for caregivers of adults: A meta-analysis. Health psychology: official journal of the Division of Health Psychology, American Psychological Association 2022, 41, 585–598. [Google Scholar] [CrossRef]
- Cress, M.E.; Buchner, D.M.; Prohaska, T.; Rimmer, J.; Brown, M.; Macera, C.; DePietro, L.; Chodzko-Zajko, W. Best practices for physical activity programs and behavior counseling in older adult populations. European Review of Aging and Physical Activity 2006, 3, 34–42. [Google Scholar] [CrossRef]
- Hirvensalo, M.; Heikkinen, E.; Lintunen, T.; Rantanen, T. The effect of advice by health care professionals on increasing physical activity of older people. Scand J Med Sci Sports 2003, 13, 231–236. [Google Scholar] [CrossRef]
- Van de Mortel, T.F. Faking it: social desirability response bias in self-report research. Australian Journal of Advanced Nursing, The 2008, 25, 40. [Google Scholar]
- Donaldson, S.I.; Grant-Vallone, E.J. Understanding self-report bias in organizational behavior research. Journal of business and Psychology 2002, 17, 245–260. [Google Scholar] [CrossRef]
Figure 1.
Predicted estimates of perceived physical activity benefit score for older adults (PABS Score) and personal (A.) attitude towards physical activities (APAS) and (B.) engagement in physical activities using the physical activity practice scale (PAPS Score). Each model adjusted for age, sex, race/ethnicity, educational attainment, marital status, relationship with care recipient, living situation, length of caregiving, weekly duration of caregiving, self-rated health, and Charlson comorbidity index.
Figure 1.
Predicted estimates of perceived physical activity benefit score for older adults (PABS Score) and personal (A.) attitude towards physical activities (APAS) and (B.) engagement in physical activities using the physical activity practice scale (PAPS Score). Each model adjusted for age, sex, race/ethnicity, educational attainment, marital status, relationship with care recipient, living situation, length of caregiving, weekly duration of caregiving, self-rated health, and Charlson comorbidity index.
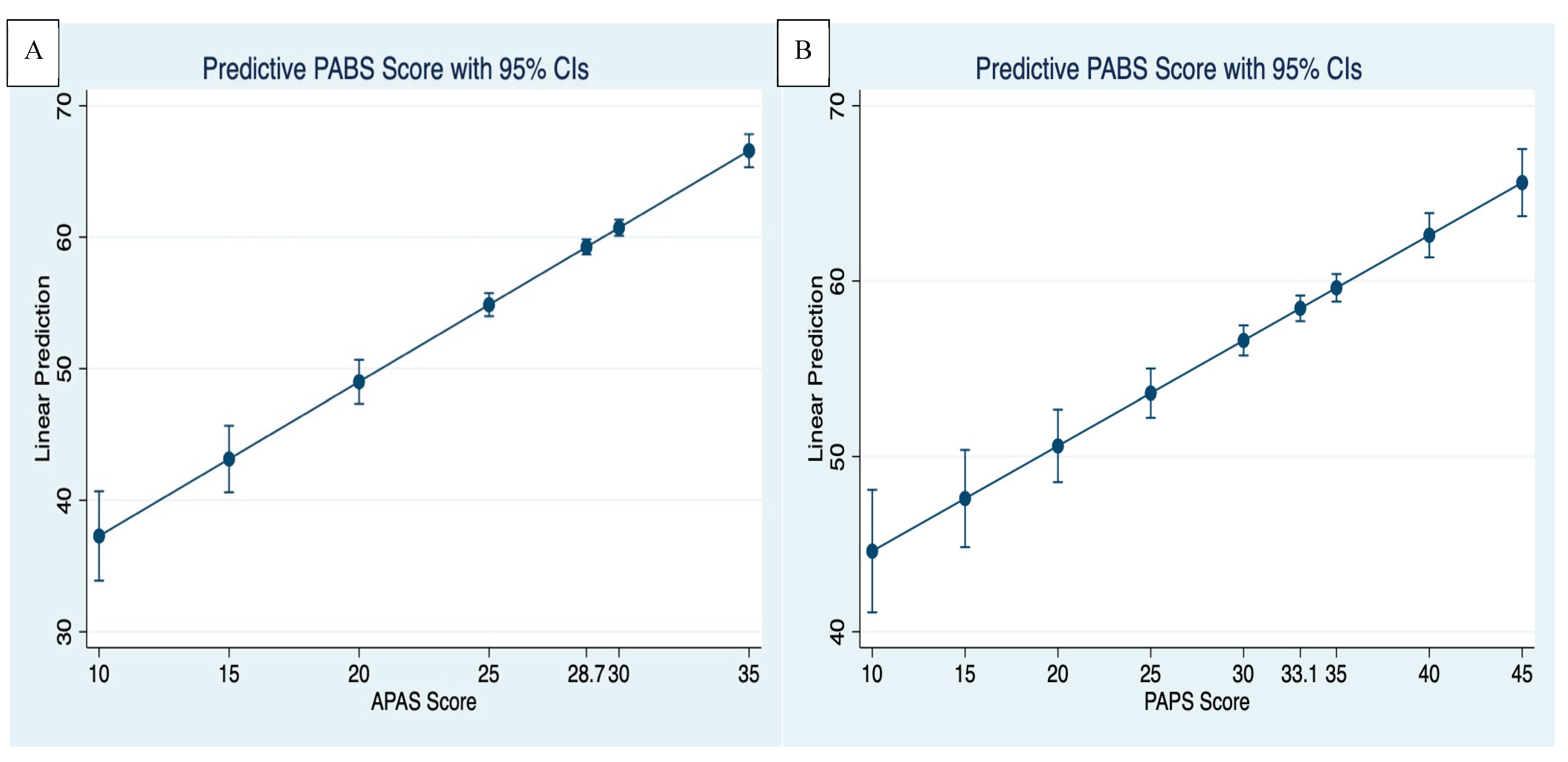
Table 1.
Sociodemographic, health, and behavioral characteristics among care partners of older adults (N=305).
Table 1.
Sociodemographic, health, and behavioral characteristics among care partners of older adults (N=305).
| Variables | Frequency / Summary Statistics |
| Demographic Characteristics | |
| Age (Mean, SD) | 35.3 (10.1) |
| 18 – 34 years | 176 (57.7) |
| 35 – 64 years | 114 (37.4) |
| 65 years and older | 15 (4.9) |
| Sex | |
| Male | 144 (47.2) |
| Female | 161 (52.8) |
| Race/Ethnicity | |
| Non-Hispanic White | 107 (35.1) |
| Non-Hispanic Black | 90 (29.5) |
| Hispanic | 92 (30.2) |
| Other Races | 16 (5.2) |
| Highest Educational Degree | |
| High School Diploma | 64 (21.0) |
| College Degree | 170 (55.7) |
| Graduate Degree | 71 (23.3) |
| Marital Status | |
| Married | 239 (78.4) |
| Never Married | 35 (11.5) |
| Widowed/Separated/Divorced | 31 (10.1) |
| Social Characteristics | |
| Relationship with Care Recipient | |
| Spouse | 86 (28.2) |
| Child/Sibling | 31 (10.2) |
| Other Relatives | 113 (37.0) |
| Friend/Neighbor | 75 (24.6) |
| Living Situation | |
| Living with care recipient | 243 (79.7) |
| Not living with care recipient | 62 (20.3) |
| Length of Caregiving | |
| Less than a year | 67 (21.9) |
| 1 – 2 years | 106 (34.8) |
| 3 years or more | 132 (43.3) |
| Hours/Week Spent on Caregiving | |
| Less than 10 hours | 86 (28.2) |
| 10 – 19 hours | 108 (35.4) |
| 20 – 39 hours | 94 (30.8) |
| 40 hours or more | 17 (5.6) |
| Health Characteristics | |
| Charlson Comorbidity Score | |
| 0 | 257 (84.3) |
| 1 | 30 (9.8) |
| 2 or more | 18 (5.9) |
| Self-Rated Health | |
| Fair/Poor | 234 (76.7) |
| Good | 55 (18.0) |
| Very Good/Excellent | 16 (5.3) |
| Behavioral Characteristics | |
| PABS Score | 60.0 (52.0 – 66.0) |
| APAS Score | 29.0 (25.0 – 33.0) |
| PAPS Score | 33.0 (28.0 – 39.0) |
1 Perceived Physical Activity Benefit Scale Score: PABS Score; Attitude towards Physical Activities Scale Score: APAS Score; Physical Activity Practice Scale Score: PAPS Score.
Table 2.
Bivariate association between perceived physical activity benefits for older adults and sociodemographic and health characteristics of care partners (N=305).
Table 2.
Bivariate association between perceived physical activity benefits for older adults and sociodemographic and health characteristics of care partners (N=305).
| Variables | PABS Score | p-value |
| Demographic Characteristics | ||
| Age Categories | ||
| 18 – 34 years | 61.0 (55.0 – 68.0) | <0.001# |
| 35 – 64 years | 57.0 (51.0 – 63.0) | |
| 65 years and older | 58.0 (39.0 – 61.0) | |
| Sex | ||
| Male | 60.0 (52.0 – 68.0) | 0.327## |
| Female | 59.0 (53.0 – 65.0) | |
| Race/Ethnicity | ||
| Non-Hispanic White | 60.0 (56.0 – 65.0) | <0.001# |
| Non-Hispanic Black | 67.0 (61.0 – 70.0) | |
| Hispanic | 50.0 (45.0 – 57.0) | |
| Other Races | 59.0 (58.0 – 60.5) | |
| Highest Educational Degree | ||
| High School Diploma | 57.0 (54.0 – 60.0) | <0.001# |
| College Degree | 58.5 (48.0 – 65.0) | |
| Graduate Degree | 66.0 (61.0 – 70.0) | |
| Marital Status | ||
| Married | 60.0 (51.0 – 66.0) | 0.003# |
| Never Married | 60.0 (59.0 – 66.0) | |
| Widow/Separated/Divorced | 56.0 (52.0 – 60.0) | |
| Social Characteristics | ||
| Relationship with Care Recipient | ||
| Spouse | 59.5 (46.0 – 68.0) | 0.002# |
| Child/Sibling | 56.0 (47.0 – 60.0) | |
| Other Relatives | 60.0 (55.0 – 64.0) | |
| Friend/Neighbor | 63.0 (56.0 – 68.0) | |
| Living Situation | ||
| Living with care recipient | 60.0 (56.0 – 65.0) | 0.550## |
| Not living with care recipient | 59.0 (52.0 – 66.0) | |
| Length of Caregiving | ||
| Less than a year | 61.0 (57.0 – 65.0) | 0.238# |
| 1 – 2 years | 59.0 (50.0 – 66.0) | |
| 3 years or more | 58.0 (52.0 – 66.5) | |
| Hours/Week Spent on Caregiving | ||
| Less than 10 hours | 66.5 (59.0 – 70.0) | <0.001# |
| 10 – 19 hours | 57.0 (51.5 – 62.0) | |
| 20 – 39 hours | 58.0 (48.0 – 65.0) | |
| 40 hours or more | 59.0 (53.0 – 62.0) | |
| Health Characteristics | ||
| Charlson Comorbidity Score | ||
| 0 | 60.0 (55.0 – 66.0) | <0.001# |
| 1 | 49.5 (43.0 – 58.0) | |
| 2 or more | 53.0 (49.0 – 60.0) | |
| Self-Rated Health | ||
| Fair/Poor | 60.0 (53.0 – 67.0) | <0.001# |
| Good | 58.0 (47.0 – 60.0) | |
| Very Good/Excellent | 59.5 (55.0 – 64.5) |
#: Kruskal-Wallis test performed; ##: Mann-Whitney U test performed. Perceived Physical Activity Benefit Scale Score: PABS Score;.
Table 3.
Multivariable quantile regression models between perceived physical activity benefits for older adults and personal attitudes towards and engagement in physical activities (N=305).
Table 3.
Multivariable quantile regression models between perceived physical activity benefits for older adults and personal attitudes towards and engagement in physical activities (N=305).
| Variables | Model 1: PABS - APAS | Model 2: PABS - PAPS |
| Coeff (95% CI) | Coeff (95% CI) | |
| Predictor Variables | ||
| APAS Score | 1.17 (0.99, 1.35) | |
| PAPS Score | 0.60 (0.45, 0.75) | |
| Demographic Characteristics | ||
| Age | 0.11 (0.03, 0.18) | 0.05 (-0.04, 0.15) |
| Sex | ||
| Male | -0.18 (-1.44, 1.08) | -0.92 (-2.54, 0.70) |
| Female | Ref | Ref |
| Race/Ethnicity | ||
| Non-Hispanic White | Ref | Ref |
| Non-Hispanic Black | 1.71 (-0.11, 3.54) | 0.26 (-2.12, 2.63) |
| Hispanic | -4.78 (-6.68, -2.88) | -8.87 (-11.16, -6.58) |
| Other Races | 0.77 (-2.16, 3.69) | 1.43 (-2.28, 5.15) |
| Highest Educational Degree | ||
| High School Diploma | Ref | Ref |
| College Degree | -2.57 (-4.27, -0.87) | -2.01 (-4.27, 0.26) |
| Graduate Degree | -1.43 (-3.56, 0.70) | -0.36 (-3.30, 2.47) |
| Marital Status | ||
| Married | Ref | Ref |
| Never Married | -0.93 (-3.21, 1.36) | 1.21 (-1.71, 4.14) |
| Widow/Separated/Divorced | -1.79 (-3.97, 0.40) | -1.36 (-4.16, 1.45) |
| Social Characteristics | ||
| Relationship with Care Recipient | ||
| Spouse | Ref | Ref |
| Child/Sibling | 0.07 (-2.20, 2.35) | 0.76 (-3.67, 2.15) |
| Other Relatives | 0.89 (-0.80, 2.57) | 0.74 (-1.42, 2.90) |
| Friend/Neighbor | 0.64 (-1.27, 2.55) | 0.94 (-1.50, 3.39) |
| Living Situation | ||
| Living with care recipient | -1.01 (-2.71, 0.68) | -1.10 (-3.27, 1.08) |
| Not living with care recipient | Ref | Ref |
| Length of Caregiving | ||
| Less than a year | Ref | Ref |
| 1 – 2 years | -1.59 (-3.34, 0.16) | -2.53 (-4.78, -0.27) |
| 3 years or more | -1.40 (-3.08, 0.28) | -1.20 (-3.36, 0.96) |
| Hours/Week Spent on Caregiving | ||
| Less than 10 hours | Ref | Ref |
| 10 – 19 hours | -2.28 (-4.04, -0.53) | -1.98 (-4.25, 0.28) |
| 20 – 39 hours | -1.90 (-3.74, -0.08) | -2.83 (-5.18, -0.49) |
| 40 hours or more | -4.14 (-7.32, -0.96) | -3.67 (-7.13, 0.39) |
| Health Characteristics | ||
| Charlson Comorbidity Score | -0.37 (-1.05, 0.32) | -1.32 (-2.19, -0.44) |
| Self-Rated Health | ||
| Fair/Poor | 2.13 (-0.66, 4.92) | 4.28 (0.61, 7.94) |
| Good | 2.01 (0.29, 3.72) | 1.65 (-0.55, 3.86) |
| Very Good/Excellent | Ref | Ref |
Model 1: PABS – APAS; Model assessing the association between the Perceived Physical Activity Benefit Scale for older adults Score (PABS Score) and Attitude towards Physical Activities Scale Score:(APAS Score); Model 2: PABS – PAPS; Model assessing the association between the Perceived Physical Activity Benefit Scale for older adults Score (PABS Score) and Physical Activity Practice Scale Score (PAPS Score). Each model controlled for the listed sociodemographic and health characteristics. Coeff: Coefficient.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



