
Submitted:
26 January 2026
Posted:
27 January 2026
You are already at the latest version
Abstract
Partial anomalous pulmonary venous return (PAPVR) with dual drainage is a very rare congenital heart anomaly. We report the case of a 6-year-old boy with PAPVR in whom the both upper pulmonary veins (PVs) drain anomalously into the systemic venous circulation, while having preserved intrapulmonary collateral venous connection with remaining pulmonary veins draining into the left atrium. Careful balloon occlusion testing of the anomalous PVs was performed, simultaneously with measurements of pulmonary pressures and control angiography proving the absence of venous congestion in the upper lung fields during the pulmonary venous phase. Transcatheter occlusion using vascular plugs was safely and successfully performed.
Keywords:
partial anomalous pulmonary venous return
; dual drainage
; transcatheter correction
; vascular plug
1. Introduction
Partial anomalous pulmonary venous return (PAPVR) occurs when one or more, but not all, pulmonary veins (PVs) drain into the systemic venous circulation. Left-sided PVs typically connect anomalously to the left innominate vein (IV) via a persistent embryological vessel, known as vertical vein (VV), or less commonly to the coronary sinus. Right-sided PVs typically connect to superior vena cava (SVC) or inferior vena cava (IVC) [1]. In most cases, anomalous PVs connect to these systemic veins and lack a normal connection to the left atrium [2].
In this case report we describe a rare variant of PAPVR in which the right upper pulmonary vein (RUPV) drains directly into the SVC, while the left upper pulmonary vein (LUPV) is connected to the IV via a VV. Both PVs have a preserved intrapulmonary collateral venous connection to the left atrium [3].
2. Case Report
A 6-year-old boy was evaluated at our outpatient clinic of a tertiary care university center because of a systolic murmur and mildly reduced exertion tolerance. Apart from frequent respiratory infections, the remaining history was unremarkable. Transthoracic echocardiography demonstrated a patent foramen ovale, without evidence of significant shunt, and confirmed normal drainage of the right lower pulmonary vein (RLPV). However, the right upper pulmonary vein was not clearly visualized. The left PVs were not visualized, but a VV with a diameter of about 6 mm was identified, draining pulmonary venous blood into the brachiocephalic vein, with unobstructed flow. The SVC was dilated with increased flow velocity. After discussion in the combined pediatric cardiology and surgical meeting, the consensus was to proceed with diagnostic cardiac catheterisation and possible transcatheter closure.
After routine preparation, we performed right heart catheterization under general anesthesia via transfemoral approach. Oximetry samples were obtained from the SVC, IVC, and main pulmonary artery (MPA) (Table 1).
A pigtail catheter was introduced into the SVC and then advanced into a VV, when venography was performed, pressures were measured in MPA and its branches and samples for oximetry were obtained. Pulmonary angiography from the MPA showed normal arborization of the pulmonary arteries (PA). In the venous phase, anomalous pulmonary venous return was visualized and the LUPV drained via a large VV. Selective angiography of the left PA revealed normal drainage of the left lower pulmonary vein (LLPV). Selective angiography of the right PA showed anomalous drainage of the RUPV directly into the SVC, just before it entered the right atrium (Figure 1).
The RLPV drained normally. A 5 Fr sheath was placed in the left femoral vein. Balloon occlusion testing was performed using a 10 × 20 mm balloon in RUPV and LUPV followed by selective left and right PA angiography, respectively (Figure 2). No residual anomalous venous pathways were visualized in either upper pulmonary lobe. Pulmonary venous return drained freely and rapidly into the left atrium, with no significant increase in MPA pressure during prolonged balloon occlusion. A 12 mm Amplatzer Vascular Plug II was deployed in the RUPV (Figure 3).
Device position was verified, and control angiography showed no venous congestion in the right upper lobe before release. A 7 Fr sheath was then placed in the left femoral vein, and a 7 Fr right guiding catheter was advanced into the VV. A 12 mm Amplatzer Vascular Plug I was delivered. After verifying correct position and excluding pulmonary venous congestion, the device was released (Figure 4).
Final pulmonary angiography showed no residual anomalous venous drainage. A mild increase in MPA pressure was noted. Following the occlusion of the VV and the RUPV, a decrease in venous oxygen saturation is observed in the SVC and the MPA (Table 1). The procedure was completed without complications, aside from transient contact-related arrhythmias.
At two-years follow-up, the patient had a single prolonged respiratory infection one-month post-procedure, resolving completely without complications. Transthoracic echocardiography (TTE) shows normal right-side heart dimensions without pulmonary hypertension (PH), physiological tricuspid valve regurgitation and normal movements of interventricular septum. Chest X-ray showed normal pulmonary-vascular pattern without pulmonary congestion.
Our case describes the safety and feasibility of percutaneous closure of PAPVR and the positive impact on hemodynamic and chamber measures.
3. Discussion
The prevalence of PAPVR in the pediatric population is less than 1% [4]. The hemodynamic consequences are directly correlated with the number of anomalous PVs and the size of the ASD. Children with PAPVR are usually asymptomatic, which suggests that the actual prevalence may be higher than reported. The natural course of the disease is similar to that of left-to-right shunt anomalies. Although congestive heart failure may rarely develop during childhood, the main consequence of excessive pulmonary blood flow is pulmonary hypertension (PH), typically occurring in the third and fourth decades of life [5].
For the classification of PVs anomalies, adequate knowledge of the embryological development of the pulmonary vascular bed (PVB) and PVs is essential. The PVB develops from a portion of the splanchnic plexus. During early gestation, the primitive lungs drain into the systemic circulation through the vitelline, umbilical, and cardinal venous systems. At the beginning of the seventh week of gestation, a solid structure known as the common pulmonary vein separates from the dorsal mesocardium, establishing a connection between the splanchnic venous plexus and the primitive cardiac tube.
With the gradual formation of a lumen within the common pulmonary vein, it becomes incorporated into the posterior wall of the left atrium, between the right and left horns of the sinus venosus, to the left of the septum primum and superior to the coronary sinus. Following the establishment of this communication, the original connections between the pulmonary and systemic venous systems regress. In the presented case, the anomalous pulmonary venous connection resulted from a disturbance in the embryogenesis of the common pulmonary vein [6].
Alsoufi et al. classified PAPVR into 5-types: (1) right PAPVR to the SVC, (2) right PAPVR to the right atrium, (3) right PAPVR to the IVC, (4) left PAPVR to left IV via ascending VV, and (5) bilateral PAPVR. Of note, this classification didn’t include a dual pulmonary venous connection [7]. Patel et al. described the concept which includes “extrapulmonary” and “intrapulmonary” separation of the dual drainage [8,9]. Therefore, our patient can be categorized as having Alsoufi type 5 (bilateral PAPVR) combined with Patel’s intrapulmonary dual drainage type.
PAPVR is commonly associated with an ASD, most frequently of the superior sinus venosus type. In our patient, only a small defect was observed in the region of the fossa ovalis. The clinical course of PAPVR is often insidious, with patients remaining asymptomatic or only minimally symptomatic for many years. In cases with a significant left-to-right shunt, the natural history of the condition includes progressive pulmonary vascular remodeling. While these changes are initially reversible, they may become irreversible by the third decade of life, ultimately resulting in the development of PH.
The definition of PH in children has traditionally mirrored that of adults, with a mean pulmonary arterial pressure (mPAP) ≥ 20mmHg [10]. The 6th World Symposium on Pulmonary Hypertension (6th WSPH) proposed a revised definition of PH in adults as mPAP >20 mmHg, along with the inclusion of pulmonary vascular resistance (PVR) ≥3 WU for the identification of pre-capillary pulmonary hypertension. In pediatric PH, particularly in the context of congenital heart disease, it is recommended to assess PVR indexed (PVRI) to body surface area in order to evaluate the presence of PH, which is defined as PVRI ≥3 WU/m2 [11].
PAPVR is a silent congenital cardiac anomaly that may present at any stage of life. In cases where TTE demonstrates right heart enlargement without an identifiable cause, it is essential to consider the possibility of anomalous PVs drainage and to pursue further diagnostic evaluation. One of the main limitations of TTE is its inability to reliably visualize the entire interatrial septum and detect anomalous PVs. Elevated oxygen saturation levels in the SVC are indicative of a left-to-right shunt and support the diagnosis of PAPVR [8,12,13]. In our case, RHC revealed an oxygen saturation of 96% in the SVC prior to the site of the shunt. Subsequently, selective catheterization of both anomalous PVs was performed, demonstrating oxygen saturation levels of 99% within these vessels. A potential concern during transcatheter closure of PAPVR is passive hyperemia and an increase in pressure within the pulmonary vascular bed. Therefore, during the procedure, a balloon occlusion test is routinely performed to monitor any rise in pressure within the MPA. In our case, only a minimal increase in pressure was observed (Table 1). Closure should not be performed if a mPAP rises ≥10 mmHg [14].
The concept of duplicated intrapulmonary venous drainage proposed by Patel et al. cannot be reliably demonstrated using angiography alone. Consequently, balloon test occlusion was performed prior to definitive closure to assess the hemodynamic impact of vessel occlusion. The absence of an increase in MPA pressure during test occlusion indicated sufficient decompression of the pulmonary vascular bed, likely mediated by collateral vessels within the pulmonary parenchyma [9].
In the case reported by Wilson et al., dual drainage of PAPVR was extrapulmonary. Angiography via a transjugular approach demonstrated that the LUPV drained into the IV through a VV while maintaining a direct connection to the left atrium. Following test balloon occlusion of the VV, no significant rise in proximal venous pressure was observed, allowing safe device closure. This finding supports the feasibility of transcatheter occlusion in selected cases of dual-drainage PAPVR when adequate PVs return to the left atrium is preserved [14].
Nowadays there is a growing experience of percutaneous transcatheter device closure. It offers many advantages over surgical treatment such as fast recovery, avoidance of mechanical ventilation, pediatric cardiac intensive care unit stay, short in-hospital stay, low cost and more patient satisfaction.
In this case, occlusion was performed using Amplatzer vascular plugs type I and type II, both self-expanding devices made of braided nitinol mesh. Type I has a single-lobe design, while type II features a triple-lobe configuration to enhance occlusive performance. Device selection depends on the target vessel diameter, with oversizing of 30–50% recommended. Both devices are effective in occluding arteriovenous fistulas, aortopulmonary collaterals, Blalock–Taussig shunts, fenestrations in Fontan circulation, and, as demonstrated in this case, can also be used to occlude venous vessels [15].
4. Conclusions
Although surgery is the treatment of choice, transcatheter correction may be a feasible alternative in a carefully selected patients with intrapulmonary or extrapulmonary dual drainage of anomalous PVs.
The Amplatzer Vascular Plug I and II are good choices for occlusion of anomalous venous vessels of this type (VV and RUPV in our case) via a transfemoral approach.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, V.P. and M.D.; methodology, I.S., A.P. and J.P.; resources, M.D., D.A. and I.S.; data curation, M.T.; writing—original draft preparation, D.A., J.P., I.S. and M.T.; writing—review and editing, M.B., M.D. and M.K.; visualization, D.A.; supervision, V.P., M.Dj. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board.
Informed Consent Statement
Informed consent for publication of data was obtained from legal guardians of the patient.
Data Availability Statement
The original contributions presented in this study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| PAPVR | Partial Anomalous Pulmonary Venous Return |
| PVs | Pulmonary Veins |
| IV | Innominate Vein |
| VV | Vertical Vein |
| SVC | Superior Vena Cava |
| IVC | Inferior Vena Cava |
| RUPV | Right Upper Pulmonary Vein |
| LUPV | Left Upper Pulmonary Vein |
| RLPV | Right Lower Pulmonary Vein |
| MPA | Main Pulmonary Artery |
| PA | Pulmonary Arteries |
| LLPV | Left Lower Pulmonary Vein |
| TTE | Transthoracic Echocardiography |
| PH | Pulmonary Hypertension |
| PVB | Pulmonary Vascular Bed |
References
- Konduri, A.; Aggarwal, S. Partial and Total Anomalous Pulmonary Venous Connection. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2025. [Google Scholar]
- Tanaka, N.; Jujo, T.; Sugiura, T.; Matsuura, K.; Kobayashi, T.; Naito, A.; Shimazu, K.; Kasai, H.; Suda, R.; Nishimura, R.; et al. Partial anomalous pulmonary venous return with dual drainage to the superior vena cava and left atrium with pulmonary hypertension. Respir. Med. Case Rep. 2018, 25, 112–115. [Google Scholar] [CrossRef] [PubMed]
- Bigdelu, L.; Maadarani, O.; Azari, A.; Heidari-Bakavoli, A.; Bitar, Z. Double Connection of Left-Sided Partial Anomalous Pulmonary Vein Return in a Young Man. JACC Case Rep. 2024, 29, 102398. [Google Scholar] [CrossRef] [PubMed]
- Hegde, M.; Manjunath, S.C.; Usha, M.K. Isolated Partial Anomalous Pulmonary Venous Connection: Development of Volume Overload and Elevated Estimated Pulmonary Pressure in Adults. J. Clin. Imaging Sci. 2019, 9, 29. [Google Scholar] [CrossRef] [PubMed]
- Dimopoulos, K.; Wort, S.J.; Gatzoulis, M.A. Pulmonary hypertension related to congenital heart disease: A call for action. Eur. Heart J. 2014, 35, 691–700. [Google Scholar] [CrossRef] [PubMed]
- Pandey, N.N.; Taxak, A.; Kumar, S. Normal pulmonary venous anatomy and non-anomalous variations demonstrated on CT angiography: What the radiologist needs to know? Br. J. Radiol. 2020, 93, 20200595. [Google Scholar] [CrossRef] [PubMed]
- Al-Muhaya, M.A.; Alkodami, A.A.; Khoshhal, S.; Najjar, A.H.A.; Al-Mutairi, M.; Abdelrehim, A.R. Transcatheter occlusion of the vertical vein in a partial anomalous pulmonary venous connection with dual Drainage, case series with literature review. Int. J. Cardiol. Heart Vasc. 2021, 37, 100889. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, V.; Mohamed, A.K.; Said, S.M. Partial anomalous venous connection with intrapulmonary dual drainage: Transcatheter treatment of a rare entity. Ann. Pediatr. Cardiol. 2023, 16, 229–230. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.; Saini, A.P.; Weber, H.S. Transcatheter device closure of partial anomalous pulmonary venous return with “intrapulmonary duplicating drainage”—A newly described entity and a single center experience. Int. J. Cardiol. 2014, 174, 770–771. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, R.T.; Raj, J.U.; Austin, E.D. Recent Advances in Pediatric Pulmonary Hypertension: Implications for Diagnosis and Treatment. Clin. Ther. 2023, 45, 901–912. [Google Scholar] [CrossRef] [PubMed]
- Galiè, N.; McLaughlin, V.V.; Rubin, L.J.; Simonneau, G. An overview of the 6th World Symposium on Pulmonary Hypertension. Eur. Respir. J. 2019, 53, 1802148. [Google Scholar] [CrossRef] [PubMed]
- El-Kersh, K.; Homsy, E.; Daniels, C.J.; Smith, J.S. Partial anomalous pulmonary venous return: A case series with management approach. Respir. Med. Case Rep. 2019, 27, 100833. [Google Scholar] [CrossRef] [PubMed]
- Alsoufi, B.; Cai, S.; Van Arsdell, G.S.; Williams, W.G.; Caldarone, C.A.; Coles, J.G. Outcomes after surgical treatment of children with partial anomalous pulmonary venous connection. Ann. Thorac. Surg. 2007, 84, 2020–2026, Discussion 2020-6. [Google Scholar] [CrossRef] [PubMed]
- Wilson, W.; Horlick, E.; Benson, L. Successful transcatheter occlusion of an anomalous pulmonary vein with dual drainage to the left atrium. Catheter. Cardiovasc. Interv. 2015, 85, 1212–1216. [Google Scholar] [CrossRef] [PubMed]
- Gomez, J.; Soledispa, C. Redirection of anomalous venous pulmonary flow to left atrium using a vascular plug II. J. Invasive Cardiol. 2012, 24, E96-8. [Google Scholar] [PubMed]
Figure 1.
Selective venography of anomalous RUPV.
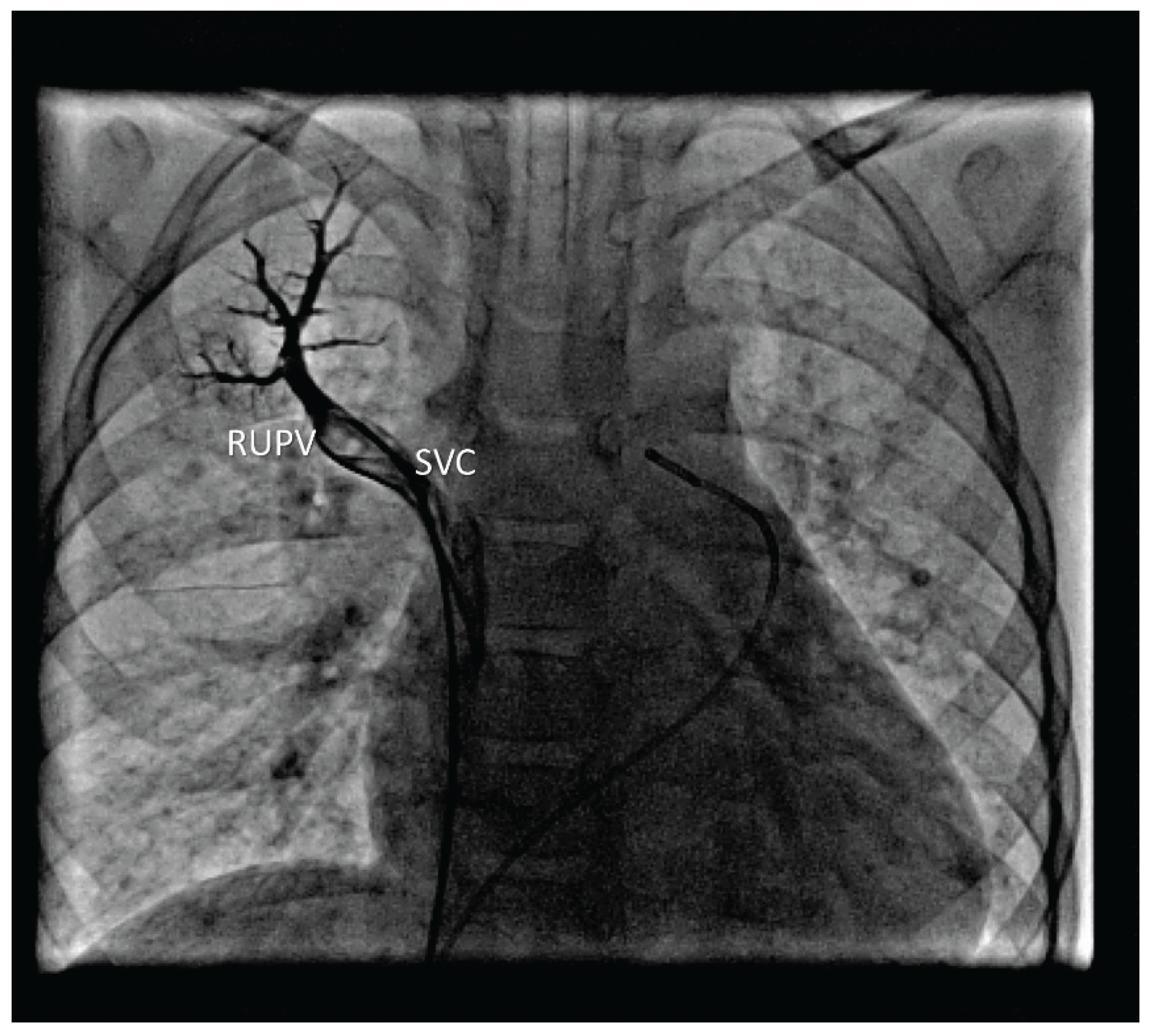
Figure 2.
Balloon test occlusion of the RUPV.
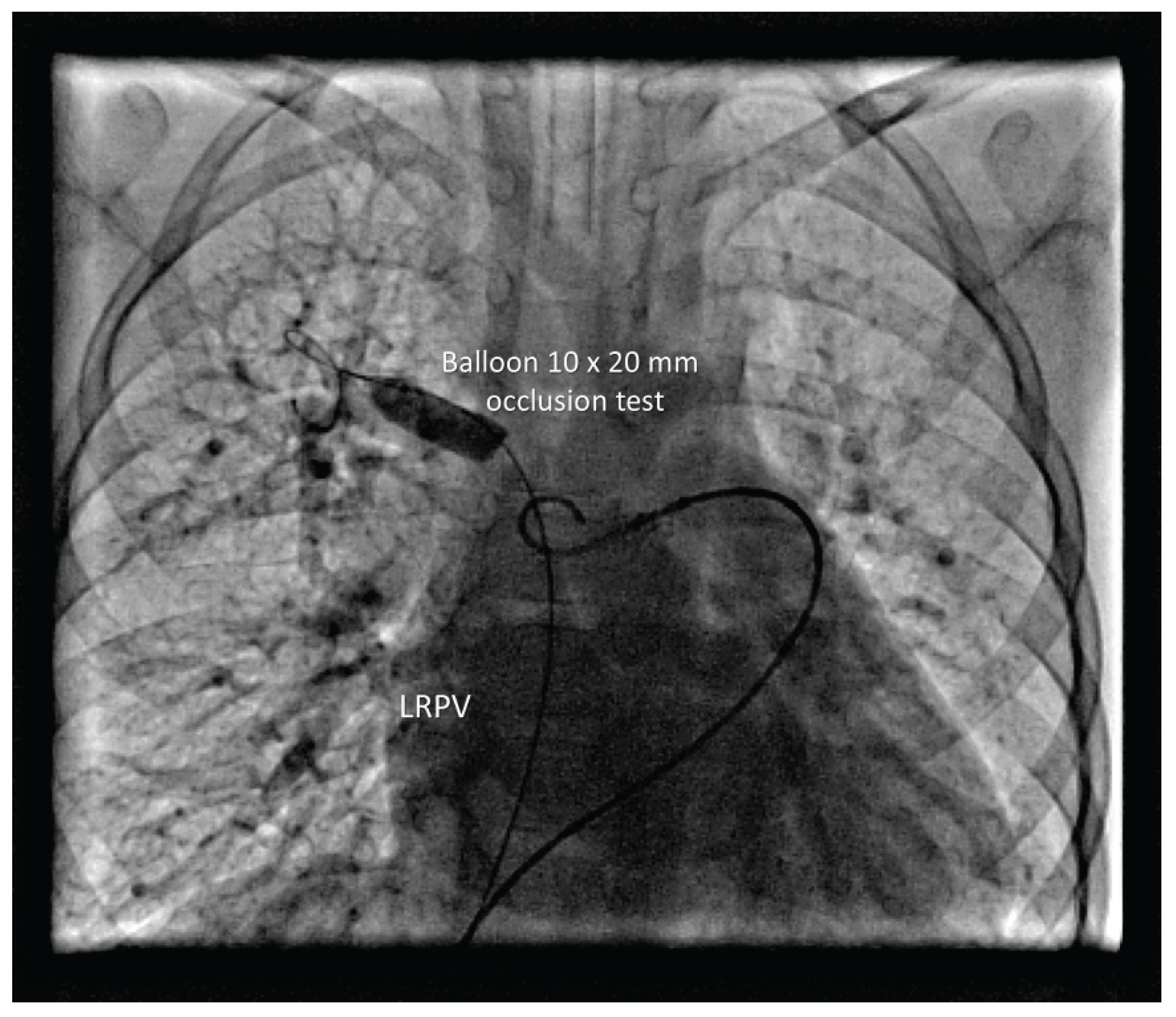
Figure 3.
Vascular pluge in RUPV without right upper pulmonary lobe congestion. Anomalous LUPV drains via VV and IV into SVC.
Figure 3.
Vascular pluge in RUPV without right upper pulmonary lobe congestion. Anomalous LUPV drains via VV and IV into SVC.
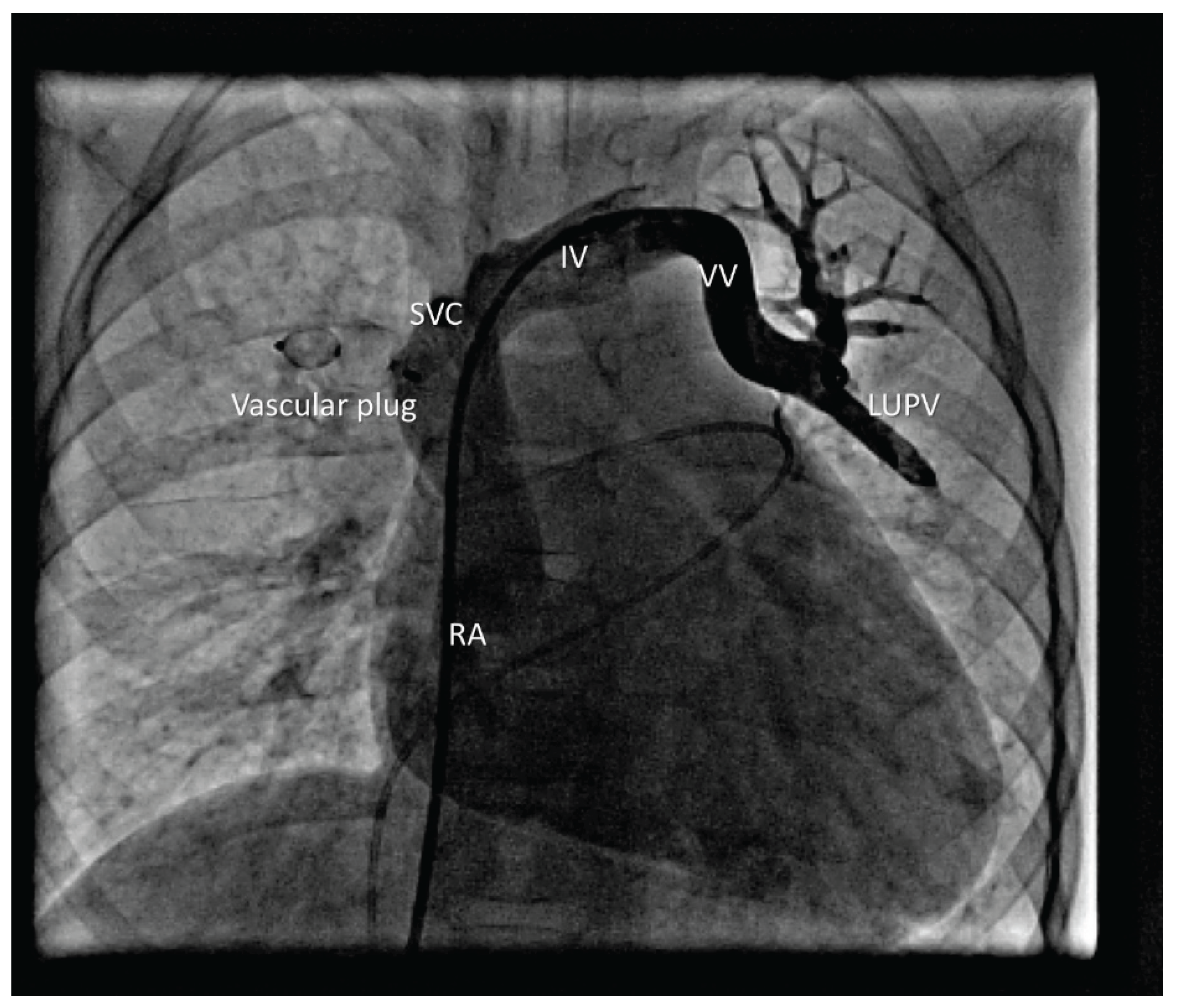
Figure 4.
Vascular plug in the LUPV.
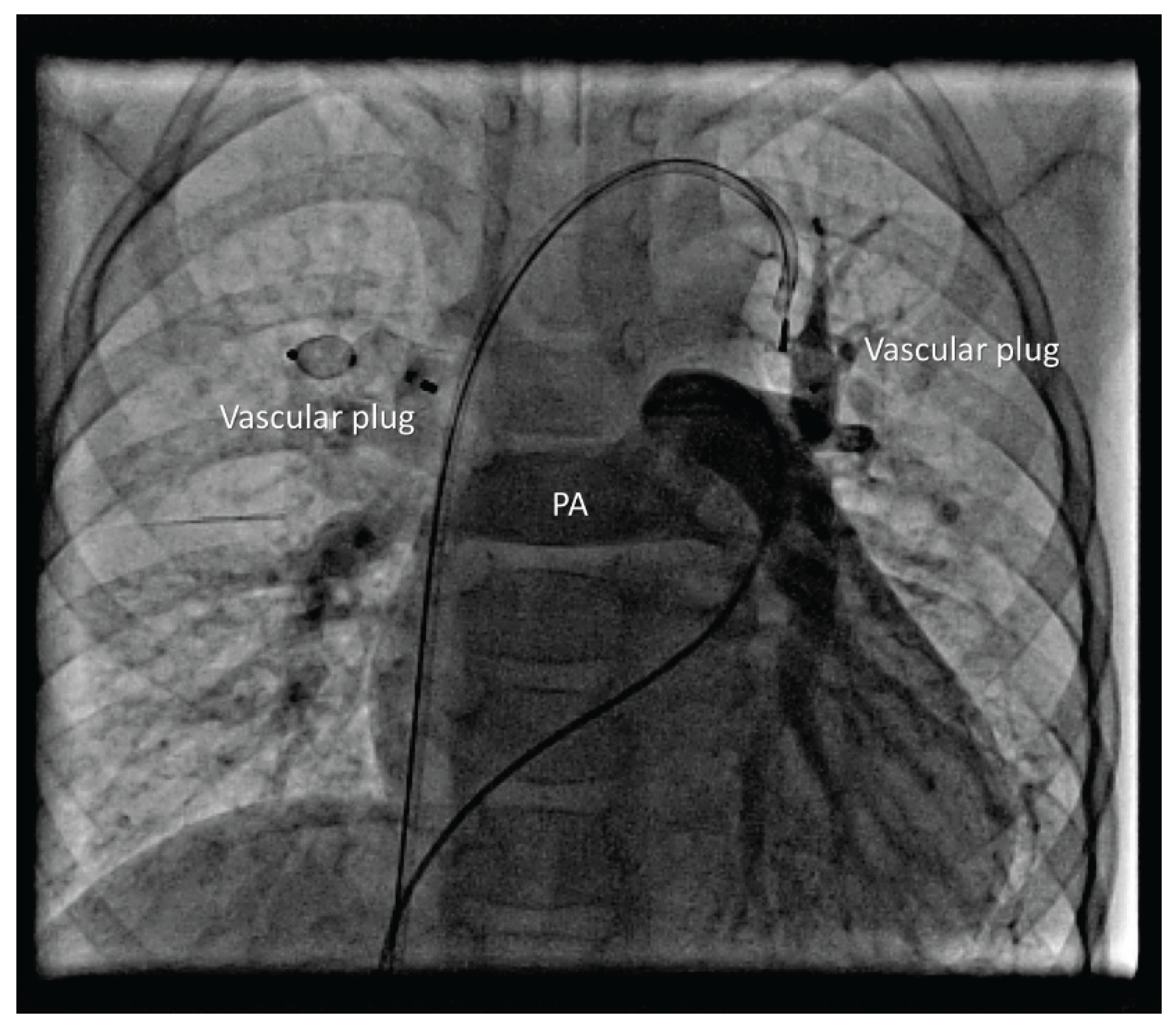

Table 1.
Oximetry and manometry findings during right heart catheterization.
| Pressure Before Occlusion (mmHg) | Pressure After Occlusion (mmHg) | SpO2 Before (%) | SpO2 After (%) | |
|---|---|---|---|---|
| SVC | / | / | 96 | 89 |
| IVC | / | / | 86 | / |
| MPA | 29/15/21 | 31/18/25 | 94 | 86 |
| PVs | / | / | 99 | / |
SVC—superior vena cava, IVC—inferior vena cava, MPA—main pulmonary artery, PVs—pulmonary veins, SpO2—oxygen saturation.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



