Submitted:
26 January 2026
Posted:
27 January 2026
You are already at the latest version
Abstract
The burnout syndrome is conceptualized as a work-related psychological condition primarily marked by persistent exhaustion, emotional and cognitive impairment, and mental distancing. In addition to these core dimensions, burnout may give rise to secondary symptoms, including psychological distress, psychosomatic complaints, and depressive mood. The Burnout Assessment Tool (BAT) includes specific measures for both primary and secondary symptoms. This study aimed to evaluate the validity evidence of the BAT's secondary symptoms Brazilian version scale (BAT-S). The sample consisted of 1.750 professionals (71% women), with a mean age of 39 years (SD = 11). Confirmatory Factor Analyses indicated that a two oblique first-order factors model, differentiating psychological distress from psychosomatic complaints, provided a superior fit compared to the unidimensional solution. The scale also presented satisfactory internal consistency for the scales Psychological Distress (α =.88 and ω =.90) and Psychosomatic Complaints (α =.85 and ω =.87). The BAT-S represents a reliable tool to assess these secondary symptoms of burnout, advancing research that integrates behavioral and physiological markers, offering practical applications for occupational health interventions and preventive strategies in the workplace.
Keywords:
burnout
; secondary symptoms
; validity
; reliability
1. Introduction
A rising body of studies on burnout syndrome has made it a well-known term, recently categorized as a work-related disorder in the ICD-11 [1]. Although it has been studied since the 1970s it is still a subject of conceptual debate, and therefore it is considered a challenge for academics in areas such as organizational psychology and occupational health psychology. Furthermore, its accurate assessment is vital for identifying at-risk individuals and informing organizational interventions aimed at promoting mental health and sustainable work conditions. During the COVID-19 pandemic, occupational health has gained unprecedented importance [2], highlighting burnout as a critical phenomenon that organizational decision-makers worldwide seek to understand better.
Burnout is defined as a state of mental exhaustion and as an occupational phenomenon that results from chronic stress in the workplace [1]. The traditional approach to burnout, mainly influenced by The Maslach Burnout Inventory (MBI), characterizes the syndrome through three dimensions: emotional exhaustion, depersonalization, and reduced capacity (occupational overload) [3]. Even though the validity and reliability of the MBI questionnaires have been statistically validated in multiple studies, there are still conceptual, psychometric, and practical shortcomings [4]. These limitations led Schaufeli et al. (2020) to develop the Burnout Assessment Tool (BAT), as an alternative instrument that would overcome the limitations identified in MBI. The latter is criticized for emphasizing emotional exhaustion while neglecting other dimensions like cognitive processes, for the lack of a general burnout score that shows the level of burnout developed and for conflating burnout with stress or depression. BAT addresses these limitations by incorporating both core and secondary symptoms into a multidimensional framework, thereby offering a more comprehensive and clinically relevant assessment approach. The present study searches for theoretical implications for burnout conceptualization and assessment. This study aims to explore the theoretical implications for the conceptualization and assessment of burnout. Burnout research has long faced criticism regarding theoretical fragility, measurement issues, and limited clinical utility [5,6]
BAT was developed by applying an inductive and deductive approach to select the items that constitute the instrument [7]. An important feature of the BAT is the assessment of burnout as a state with a total score, complementing the evaluation of its constituent dimensions. The complete work-related version of the BAT contains 33 items and consists of the BAT-C for the core symptoms and BAT-S for secondary symptoms. The BAT-C assesses the four core dimensions (exhaustion, mental distance, emotional impairment, and cognitive impairment) and contains 23 items. These core symptoms can be assessed using either a long-form version of the instrument, consisting of 23 items, or a short-form version comprising 12 items; there is even the ultra-short 4-item version already validated [8]. The BAT-S assesses the two secondary dimensions: Psychological distress (e.g., sleep problems, tension, and worrying) and Psychosomatic complaints (e.g., headaches, chest, and muscle pain) and contains 10 items. Both are rated on a five-point Likert scale ranging from never (1) to always (5) [7].
The BAT-C has been adapted and validated in multiple countries, such as: Brazil [9], Croatia [10], Ecuador [11], Finland [12], Greece [13], Italy [14,15,16,17], Japan [18], Korea [19], Lithuania [20], Netherlands [21], Poland [22], Portugal [23], Romania [24,25], South Africa [26] and Turkey [27]. Moreover, studies by De Beer et al. (2020) and Sinval et al. (2022) have demonstrated that the BAT 's second-order factor structure remains invariant across countries, suggesting its utility for reliable and valid cross-national comparisons.
The BAT's conceptualization of burnout as a syndrome needs the generation of both a composite score that represents the overall burnout syndrome and individual scores for each of the four core symptoms. To evaluate the structure of the BAT, researchers have compared a four-factor model, in which the BAT-C consists of four correlated subscales, with a second-order model, where all subscales load onto a higher-order burnout factor. Empirical evidence supports the superiority of the second-order model, which aligns with the syndrome conceptualization of burnout, over the four-dimensional model [28]. The internal consistency of the BAT-C has also been extensively tested, with results indicating high reliability (exceeding 0.80 for the subscales and 0.90 for the overall scale) across various countries, including Austria, the Netherlands, Ireland, Belgium (Flanders), Finland, Germany [29], Japan [18], Italy [14], Ecuador [11], Korea [19], Brazil [9], Portugal [23], and Romania [24].
In terms of discriminant validity, research has demonstrated that the BAT is distinct from related constructs, such as job boredom, depressed mood, workaholism, and work engagement [7]. These results were also replicated in a Romanian sample evaluating burnout through BAT-12 [24]. In a Brazilian sample, burnout assessed through BAT-12 showed discriminant validity with respect to depressive symptoms, anxiety, and irritability, indicating that BAT scores captured variance distinct from these affective domains [30]. Additionally, Yokoyama et al. (2022) found positive correlations of burnout with workaholism and negative with work engagement measured by the BAT-C of 12 items, both directly and indirectly through self-endangering behavior.
In the BAT research, the secondary dimensions are described as follows: (1) Psychological distress, which encompasses unpleasant emotions associated with heightened arousal that negatively impact functioning and interfere with daily activities; (2) psychosomatic complaints, referring to physical symptoms that are believed to be caused or aggravated by psychological factors; and (3) depressed mood, which, while distinct from major depressive disorder or other mood disorders, represents a common emotional response to disappointment rather than a psychiatric disorder. These three symptoms are considered atypical for burnout as they theoretically, do not reflect either an inability or unwillingness to spend necessary effort at work, which are seen at the hallmark of burnout [31]. Therefore classified as secondary symptoms, they may also appear in other physical and mental disorders, such as hyperthyroidism, cancer, mood disorder, or anxiety disorder and depression [7]. The secondary symptoms that are evaluated through the BAT-S scale in this paper, assess only two secondary symptoms (psychological distress and psychosomatic complaints) and does not include a subscale for depressed mood, as this aspect of well-being has already been effectively operationalized in several other questionnaires, as the Four-Dimensional Symptom Questionnaire (4DSQ) [32]; therefore, there was no specific need to develop a new scale [7].
Evidence indicates that work-related stressful conditions encompass job stress, employment status, job insecurity, and imbalance between work and family life. Nakao et al. (2010) emphasized that job stress models and unstable employment conditions have major implications for both clinical and research contexts in psychosomatic medicine. Work-related conditions consistently emerge as the most frequent stressors experienced by individuals, followed by health and financial problems, all associated with adverse physical and mental outcomes, such as cardiovascular diseases and insomnia [33].
Extensive research has shown that psychosocial aspects of the working environment are strongly linked to adult health outcomes [34,35], particularly in the early manifestations of psychosomatic complaints and psychological distress, which overlap with symptoms commonly described in depression and burnout. This underlines the importance of incorporating complementary tools for assessing burnout in occupational contexts and understanding burnout severity by capturing its consequences alongside its core manifestations. Therefore, secondary symptoms reflect a broader impact of prolonged work related stressors, on psychological distress and psychosomatic functioning and are especially relevant because they frequently represent the reason why individuals seek professional help.
In the cross-national validation of the BAT, secondary symptoms correlated strongly with primary symptoms [23,29]. Supporting this interpretation, structural models indicate that secondary symptoms are best represented as correlating with primary burnout symptoms rather than as part of the latent core construct [7]. Furthermore, the Lithuanian validation study [20] confirmed the two-factor structure of secondary symptoms (psychological distress and psychosomatic complaints), demonstrating a significant difference (p < 0.001) between the unidimensional and two-factor models. The CFA showed a strong correlation between the two factors (r = .72) and confirmed they are positively associated with core burnout symptoms. Overall, these findings support the rationale for testing this two-factor structure in the present study’s confirmatory analysis of secondary symptoms.
Theoretically, distinguishing psychological distress from psychosomatic complaints reflects the multidimensional progression of burnout, whereby prolonged exposure to chronic work stress initially impacts emotional and cognitive functioning (e.g., irritability, concentration difficulties), which may subsequently evolve into physical manifestations (e.g., headaches, sleep disturbances) [36,37]. This cascading process underscores that psychological and psychosomatic complaints, while strongly associated, are not redundant dimensions but complementary indicators of the broader syndrome. Practically, this differentiation enhances the diagnostic and preventive utility of the BAT-S, as it allows practitioners to identify whether secondary symptoms manifest primarily in the psychological or psychosomatic domain, thereby informing targeted interventions and monitoring strategies. Findings from the original BAT research also conclude into the recommendation for the application of the 6-item depression subscale from the Four-Dimensional Symptom Questionnaire (4-DSQ) [7,32].
The present study aims to assess psychometric evidence for the Brazilian Portuguese version of the Burnout Assessment Tool for Secondary Symptoms (BAT Brazil-S), testing the hypothesized models. Specifically, the assessment of BAT-S dimensionality, internal consistency, and convergent validity in the Brazilian context. The following hypotheses were proposed: (1) It is expected that the hypothesized two-factor oblique structure of the BAT-S will demonstrate a satisfactory fit to the data collected in Brazil, supporting evidence of its validity. (2) Based on previous studies [7,9], the BAT-S dimensions (psychological distress and psychosomatic complaints) are anticipated to demonstrate adequate internal consistency estimates (≥ .80). Therefore, this study seeks to provide further reliability evidence for the Brazilian version. (3) Another relevant source of validity evidence lies in the association between secondary symptom scores and burnout core symptoms. It is hypothesized that BAT-S scores will show positive correlations with general burnout and its core dimensions.
2. Materials and Methods
2.1. Participants
A convenience sample of 1.750 professionals in Brazil was analyzed. The participants lived in the four Brazilian macroeconomic regions, with 78.5% in the Center-South, 17.6% in the Northeast, 2.7% in the Legal Amazon, and 1.2% in the administrative region (Federal District). The participants met the inclusion criteria with a work status that required them to perform paid occupational activities autonomously or in an organization at the time of the research. At the time of the survey, the sample was composed of 11% white collar workers and 48.4% blue collar workers, and 26.5% were health workers. The majority (50.4%) had a postgraduate degree, with 24.9% having a college degree or ongoing and 24.7% having completed high school. The predominant salary range was between three to six salaries (40%). In the final sample, the mean age was 39 years (SD = 11), with 29% (n = 507) men and 71% (n = 1243) women.
2.2. Measures and Instruments
Sociodemographic and Labor Questionnaire: Created by the authors of the research with information about gender, age, education, and employment status.
The Burnout Assessment Tool, BAT-C and BAT-S: Burnout levels and their dimensions were assessed using the BAT developed by Schaufeli et al. (2020) and adapted to the Brazilian context by Vazquez et al. (2025). The BAT-C scale (short version) for the work context consists of 12 items, which assess symptoms of exhaustion (3 items), mental distance (3 items), cognitive impairment (3 items), and emotional impairment (3 items). The BAT-S scale comprises 10 items designed to assess the two secondary dimensions of burnout symptoms, which are operationalized through the subscales Psychological Distress - PD (5 items) and Psychosomatic Complaints - PC (5 items). BAT-C and BAT-S are rated on a five-point Likert scale ranging from never (1) to always (5). The adaptation and validation conducted by Vazquez et al. (2025) provided strong evidence for the psychometric adequacy of BAT-12 in Brazil, with a hierarchical structure of four first-order dimensions (exhaustion, mental distance, emotional impairment, and cognitive impairment) that load on a second-order factor that assesses burnout. The reliability indices of the BAT-12 scale were satisfactory (α=.91, ω=.91, and C. R. =.90). The scale also showed satisfactory goodness-of-fit indexes (CFI = .984, TLI = .978 and RMSEA = .067 [90%, .060 - .073]). The global score can be evaluated at four levels of burnout: low (< 25th percentile); moderate (25th percentile to 75th percentile); high (75th percentile to 95th percentile); and very high (> 95th percentile), based on the average score of participants’ responses [38,39].
2.3. Data Collection
The survey was administered between 2019 to 2024, with participants completing the instruments via an online platform and in-person. Then, participants answered the sociodemographic questionnaire, BAT-C and BAT-S. The survey took approximately 15 minutes to complete. After excluding participants with invalid or incomplete information on BAT-C or BAT-S, univariate or multivariate outliers, the final analytic sample was of 1750 participants. Participants, whether from in-person or online data collection, accessed the instruments after expressing their consent to participate in the research by agreeing to the Informed Consent Form (ICF) for in-person collection and the Online Consent Form Registration (RCEO) for online collection. These terms ensured the confidentiality and anonymity of the participants’ identities and information which detailed the research's significance, and objectives.
2.4. Ethical Considerations
The research project was submitted for evaluation by the Research Ethics Committee (CEP) in the university where it was developed in strict compliance with the applicable norms, guidelines, and ethical recommendations. Participants were invited to take part in the study voluntarily. Those who consented to participate completed the instrument after providing their agreement through the online Informed Consent Form. All collected material is for the exclusive use of the research team and will be used solely for the purpose of providing data for conducting the research itself and any resulting publications. Both in the research and in the production of the article, the confidentiality of the data and information that could identify participants will be ensured. The data collected will not be sold or disclosed in any way that could harm the participants and will be stored for at least five years, after which they may be destroyed.
2.5. Data Analysis
Evidence of validity for the internal structure of the Brazilian version of the BAT was examined using the total sample (N = 1750), randomly divided into two equal subsamples: one for exploratory analyses (n = 875) and another for confirmatory analyses (n = 875). Reliability and external validity were evaluated with the full sample.
Exploratory Graph Analysis (EGA) [40] was conducted on the first subsample to identify the dimensional structure. EGA estimates partial correlations among items using graphical LASSO (λ = .10) with model selection based on the extended Bayesian information criterion (EBIC;γ = .50)[41]. The walktrap algorithm [40] was applied to detect clusters, and item stability was assessed via bootstrapping, with values ≥ .75 considered acceptable [42]. Analyses were conducted in R (R Core Team, 2024) with the EGAnet package [43].
Confirmatory Factor Analysis (CFA) was performed on the second subsample, testing three models: (a) the EGA-derived structure, (b) a two-factor oblique model, and (c) a bifactor model with two oblique factors. Models were estimated with the ULSMV estimator, appropriate for ordinal data, using BFGS optimization. ULSMV has been shown to provide robust parameter estimates and χ² statistics [44,45,46] Model fit was evaluated using χ², CFI, TLI, RMSEA, and SRMR, with cutoffs of CFI/TLI ≥ .95, RMSEA ≤ .06, and SRMR ≤ .08 [47]. CFA analyses were conducted in R using lavaan [48].
Differential Item Functioning (DIF) was tested across age, gender, and educational level using ordinal logistic regression for polytomous items [49]. Three nested models were compared: (a) a baseline model including only the latent trait (θ), (b) a uniform DIF model adding the group variable, and (c) a non-uniform DIF model including the interaction between group and trait. DIF was flagged when the likelihood ratio test was significant (p < .01) and ΔR² ≥ .035 [50]. Analyses were performed with the lordif package [49].
Finally, Structural Equation Modeling (SEM) was used to examine associations between BAT dimensions (Exhaustion, Mental Distance, Cognitive impairment and Emotional impairment) and the validated constructs. SEM was conducted in R with lavaan [48] using the ULSMV estimator. Model fit was evaluated via RMSEA, SRMR, CFI, and TLI, with benchmarks from Hu and Bentler (1999). Correlations were interpreted according to magnitude, direction, and statistical significance (p < .05).
3. Results
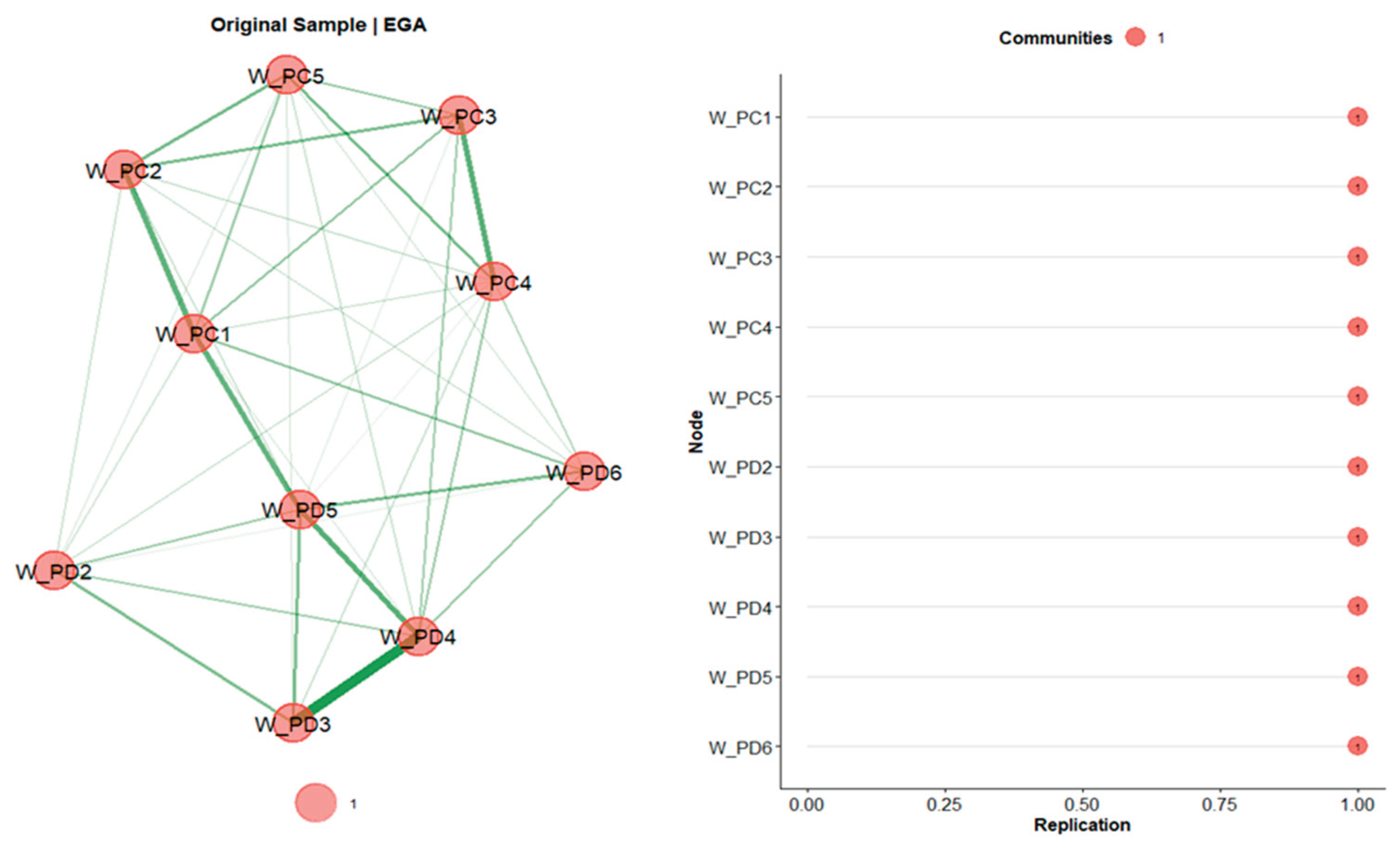
We conducted an Exploratory Graph Analysis (EGA) including only the secondary symptoms of the instrument. The community structure obtained from EGA revealed a single cohesive cluster, suggesting a unidimensional solution for BAT-S. Each item demonstrated a replication index of 1, indicating strong structural stability and consistent item contribution to a single latent factor.
Figure 1.
Results of the Exploratory Graph Analysis With Bootstrap and Item Stability. Note. W_PC1 to W_PC5 represent items from the Psychosomatic Complaints scale: 1 = palpitations or chest pain; 2 = stomach and/or intestinal complaints; 3 = headaches; 4 = muscle pain; 5 = getting sick often. From W_PD2 to W_PD6 represent items from the Psychological distress scale: 2 = trouble falling or staying asleep; 3 = worry; 4 = tense and stressed; 5 = anxious and/or suffer from panic attacks; 6 = noise and crowds are disturbing. The W_PD1 item was not considered as it was excluded in the original validation study.
Figure 1.
Results of the Exploratory Graph Analysis With Bootstrap and Item Stability. Note. W_PC1 to W_PC5 represent items from the Psychosomatic Complaints scale: 1 = palpitations or chest pain; 2 = stomach and/or intestinal complaints; 3 = headaches; 4 = muscle pain; 5 = getting sick often. From W_PD2 to W_PD6 represent items from the Psychological distress scale: 2 = trouble falling or staying asleep; 3 = worry; 4 = tense and stressed; 5 = anxious and/or suffer from panic attacks; 6 = noise and crowds are disturbing. The W_PD1 item was not considered as it was excluded in the original validation study.
Three alternative models for BAT-S were assessed through Confirmatory Factor Analysis (CFA): (1) the unidimensional model, derived from the Exploratory Graphic Analysis (EGA), (2) two factor oblique model (e.g, correlated) aligned with the conceptualization of burnout as a syndrome within the framework of the BAT [38], (3) bifactor with two oblique factors, according to previous validation studies have tested alternative factorial models [23,29] such as the higher-order structure for the core symptoms, this selected model reflects more precisely the secondary symptoms theorized structure in the BAT framework [7].
The unidimensional model exhibited the poorest fit (CFI = .951, TLI = .937, RMSEA = .115), in comparison to the other solutions. The two oblique-factor first-order factors showed an improvement across all indices (CFI = .972, TLI = .963, RMSEA = .088). Finally, the bifactor model with two correlated factors demonstrated the best overall fit (CFI = .992, TLI = .985, RMSEA = .056), indicating superior representation of the data structure (Table 1).
Although the bifactor solution provided the best global fit, it also absorbed a substantial portion of variance from the content-specific factors, thereby reducing their explanatory contribution of the latent dimensions that constitute BAT-S (Table 2), concluding with the selection of the two-factor oblique model as the most adequate solution. The factor loadings for the Psychosomatic Complaints scale indicated the items need to be interpreted with more parsimony than the Psychological Distress. For the Psychosomatic Complaints the item “I suffer from headaches” showed the lowest factorial loading that provides the least discrimination, whereas the item “I suffer from muscle pain, for example in the neck, shoulder or back” discriminates most effectively, reflecting a greater sensitivity of the item to differences in the subscale and more representativity of the latent trait. In the case of Psychological distress, the item “Noise and crowds disturb me” with the lowest factor loading discriminates less, and the item “I feel tense and stressed” showed the highest factor loading in the scale, representing this latent trait and reflecting the item with the higher sensitivity to differences in the latent trait [51].
The two oblique-factor first order factors model exhibited adequate to good internal consistency (i.e., coefficients ≥ .80). Specifically, the Psychological Distress (PD) factor showed reliability coefficients of α = .88 and ω = .90, while the Psychosomatic Complaints (PC) factor demonstrated reliability coefficients of α = 0.85 and ω = 0.87, indicating satisfactory measurement precision for both constructs.
When conducting Differential Item Functioning (DIF) analysis with the full sample, all items were invariant (i.e., no item showed p < .01 combined with Nagelkerke’s pseudo R² ≥ .035) across gender, age, and educational level (Table 3 and Table 4).
The Structural Equation Modeling (SEM) analysis with the measurement models [0.049, 0.056]), CFI = 0.973, and TLI = 0.968), indicating that the specified model and factor correlations showed adequate fit (SRMR = 0.034, RMSEA = 0.052 (90% CI adequately fit the data. Exhaustion was strongly and positively correlated with Mental distance (r = .714, p < .001) and Cognitive emotional impairment (r = .576, p < .001). Mental distance was also positively correlated with Cognitive emotional impairment (r = .679, p < .001).
Regarding the scales validated in this study, Psychosomatic Complaints and Psychological Distress showed positive associations with all burnout symptoms. In particular, exhaustion emerged as the most strongly related symptom, presenting the highest correlations with both Psychosomatic Complaints (r = .661, p < .001) and Psychological Distress (r = .748, p < .001). In addition, both scales were positively correlated with mental distance and cognitive impairment and emotional impairment, with all remaining associations being moderate to strong (r > .47). Finally, Psychosomatic Complaints and Psychological Distress were strongly and significantly correlated with each other (r = .86, p < .001).
4. Discussion
The present study, as the first in Brazil, aimed to examine the psychometric properties of the Brazilian adaptation of the BAT-S, focused on its structural validity, internal consistency, and its relations with burnout core symptoms. The findings provide robust support for the proposed hypotheses, reinforcing the adequacy of the BAT-S as an instrument for assessing secondary symptoms of burnout in the Brazilian occupational context, in line with the results shown by Lazauskaitė-Zabielskė et al. (2023) in the Lithuanian context.
The dimensionality analysis represents a central contribution of this study, as it clarifies the factorial structure of the BAT-S. Consistent with H1 and based on the results from Lazauskaitė-Zabielskė et al. (2023), the hypothesized two-factor oblique model structure of the BAT-S demonstrated a satisfactory fit to the data collected in Brazil, supporting evidence of its validity. This result aligns with cross-cultural validations and demonstrates the flexibility of the BAT-S to capture nuanced symptom profiles across diverse contexts. It is important to note that unidimensional structure is discarded based on the evidence from the CFA and other studies [20,38]. The evidence from this study shows that BAT-S scale should not be conceptualized as unidimensional, as its two factors represent complementary yet distinct manifestations of secondary symptoms, which should be examined together rather than collapsed into a single general dimension. Understanding the differential role of these two secondary symptom domains could make a difference in burnout assessment and prevention. Literature defines psychological distress as a series of psychophysiological and behavioral reactions that are nonspecific to any single pathology, encompassing anxious and depressive responses, irritability, cognitive decline, and sleep disturbances [52]. When left untreated, psychological distress may evolve into serious but reversible health conditions (e.g., hypertension, severe depression, alcoholism, burnout) [52], which are also associated with the emergence of psychosomatic complaints that, over time, may lead to irreversible outcomes such as permanent disability, premature death, or severe chronic cardiovascular and neuropsychiatric diseases [53]. Therefore, the early detection of secondary symptoms in organizational settings is critical to identifying health deterioration at its onset and enabling timely preventive interventions [54].
All items presented adequate factor loadings, reinforcing the conceptualization of secondary symptoms as consequences of sustained exposure to work-related stressors rather than exclusive features of burnout [7]. In both Psychosomatic complaints and Psychological distress, items with higher factor loadings (Item ‘muscle pain’ for Psychosomatic complaints and ‘tense and stressed’ for the Psychological distress) demonstrated greater representativity of the latent trait, respectively whereas items related to headaches or sensitivity to noise (Item ‘headaches’ for the Psychosomatic complaints and ‘noise and crowds are disturbing’ for Psychological distress) showed weaker representation of the dimensions. For the higher factor loading items, this reflects a more global physiological activation (e.g., generalized muscle tension or psychological tension and stress) that made sense as more stable allostatic load processes that accumulate over time, making them stronger indicators of chronic dysregulation. In contrast, items with the lower factorial loadings are more situational, or stimulus-dependent reactions capturing fluctuations that may be reactive rather than baseline-defining, and therefore load on less central variance of the latent construct [56]. From a practical perspective, in assessment, this distinction is critical, as higher-loading items may serve as earlier and more sensitive markers of chronic health deterioration, whereas lower-loading items may reflect context-specific discomfort that is less predictive of long-term impairment.
Consistent with H2, the BAT-S demonstrated excellent internal consistency, with Cronbach’s alpha and McDonald’s omega coefficients exceeding the .80 threshold for both subscales [56]. These results confirm that the BAT-S provides reliable and stable measurement of secondary symptoms in Brazilian professionals, supporting its utility in both research and clinical applications [20].
In support of H3, the BAT-S showed strong positive correlations with the core dimensions of burnout, mental exhaustion, mental distancing, cognitive impairment, and emotional impairment. Mental exhaustion exhibited the strongest associations with psychological distress and psychosomatic complaints, suggesting that exhaustion plays a central role in triggering secondary symptoms. This is consistent with theoretical models positing that secondary symptoms are downstream consequences of primary burnout symptoms [7]. From a practical perspective, the validation of the BAT-S in Brazil enhances its applicability for occupational health monitoring and intervention. Identifying secondary symptoms, psychological distress, and psychosomatic complaints, can help individuals identify the initial stages of stress impact on psychological distress and psychosomatic complaints, facilitating timely intervention.
The validation of the BAT-S within the Brazilian context represents a significant step toward standardized burnout assessment in both research and applied settings. By enabling the evaluation of secondary symptoms alongside core dimensions, the BAT supports a more comprehensive conceptualization of burnout, facilitating early detection, accurate diagnosis, and personalized intervention strategies. This approach aligns with international recommendations for multidimensional assessment and strengthens occupational health policies focused on prevention and well-being promotion [57,58].
5. Conclusions
In conclusion, the Brazilian BAT-S demonstrates satisfactory psychometric properties and theoretical coherence, confirming its utility for research, clinical practice, and occupational health management. This study’s strengths include its large sample and the use of robust psychometric methods (EGA and CFA) to examine structural validity. However, some limitations warrant consideration; the cross-sectional design precludes causal inference or conclusions about the temporal development of symptoms. Additionally, the sample was predominantly female (71%), which may limit the generalizability of the results. By bridging conceptual gaps and addressing previous measurement limitations, the BAT-S contributes to advancing burnout diagnosis, prevention, and intervention in both national and international contexts.
Future research should investigate the longitudinal stability of the BAT-S structure and its predictive validity regarding health and performance outcomes. Moreover, integrating psychometric data with biomarkers (e.g., cortisol levels) and objective behavioral indicators could enhance the clinical utility and diagnostic precision of the BAT-S. Cross-cultural comparisons should also be conducted to advance the global standardization of burnout assessment. Further research is needed to investigate the role of the BAT-S as a complementary tool with BAT-C in clinical practice.
Author Contributions
Conceptualization, W.B.S. and H.D.W.; data curation, A.M.V.-S., and A.C.S.V.; formal analysis, A.M.V.-S. and C.P.P.d.F.; funding acquisition, C.A.P.Ch. and C.P.P.d.F; investigation, A.M.V.-S.; methodology,A.M.V.-S. and C.P.P.d.F.; project administration, C.P.P.d.F. and J.d.C.R; resources, C.A.P.Ch., and A.C.S.V., and C.P.P.d.F; software, C.P.P.d.F.; supervision, J.d.C.R., and C.P.P.d.F.; validation, C.P.P.d.F., W.B.S. and H.D.W.; visualization, A.M.V.-S.; writing—original draft, A.M.V.-S., J.d.C.R. and C.P.P.d.F.;writing—review and editing, W.B.S., H.D.W. and A.C.S.V. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Comissão Nacional de Pesquisa - CNPq - Universal, Brazil and by Universidad Espíritu Santo, Ecuador.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Research Ethics Committee (CAAE 78617617.8.0000.5345) and followed the ethical Resolution 466/2012 of the Brazilian National Health Council.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
In this section, you can acknowledge any support given which is not covered by the author contribution or funding sections. This may include administrative and technical support, or donations in kind (e.g., materials used for experiments).
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A

Table A1.
Portuguese version of BAT-S.
| Nunca (Never) | Raramente (Rarely) | Algumas vezes (Sometimes) | Com frequência (Frequently) | Sempre (Always) | |
| 1 | 2 | 3 | 4 | 5 | |
| Queixas Psicológicas | |||||
| 1. Tenho dificuldades em adormecer ou ficar dormindo | |||||
| 2. Tendo a ser preocupado | |||||
| 3. Sinto-me tenso e estressado | |||||
| 4. Sinto-me ansioso e/ou sofro de ataques de pânico | |||||
| 5. Barulho e multidões me perturbam | |||||
| Queixas Psicossomáticas | 1 | 2 | 3 | 4 | 5 |
| 1. Sofro de palpitações ou dores no peito | |||||
| 2. Sofro de dores no estômago e/ou intestinais | |||||
| 3. Sofro de dores de cabeça | |||||
| 4. Sofro de dores musculares, como, no pescoço, ombro ou costas | |||||
| 5. Fico doente muitas vezes |
References
- World Health Organization. International Classification of Diseases, 11th Revision (ICD-11); World Health Organization: Geneva, 2019; Available online: https://icd.who.int/.
- Amanullah, S.; Shankar, R.R. The Impact of COVID-19 on Physician Burnout Globally: A Review. Healthcare 2020, 8, 421. [Google Scholar] [CrossRef] [PubMed]
- Maslach, C.; Schaufeli, W.B.; Leiter, M.P. Job Burnout. Annu. Rev. Psychol. 2001, 52, 397–422. [Google Scholar] [CrossRef] [PubMed]
- De Beer, L.T.; Schaufeli, W.B.; De Witte, H.; Hakanen, J.J.; Kaltiainen, J.; Glaser, J.; Seubert, C.; Shimazu, A.; Bosak, J.; Procházka, J.; et al. Revisiting a Global Burnout Score With the Burnout Assessment Tool (BAT) Across Nine Country Samples. Eur. J. Psychol. Assess. 2024. [Google Scholar] [CrossRef]
- Nadon, L.; De Beer, L.T.; Morin, A.J.S. Should Burnout Be Conceptualized as a Mental Disorder? Behav. Sci. 2022, 12, 82. [Google Scholar] [CrossRef]
- Vinueza-Solórzano, A. M.; Martins, G. M.; Siciliano, C. M.; Sanvicente-Vieira, B.; Freitas, C. P. P.; Rodrigues, J. C. Interventions in burnout and their effects on biomarkers: A systematic review. Revista Psicologia: Organizações e Trabalho 2025, 25, e25443. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; Desart, S.; De Witte, H. Burnout Assessment Tool (BAT)—Development, Validity, and Reliability. Int. J. Environ. Res. Public Heal. 2020, 17, 9495. [Google Scholar] [CrossRef]
- Hadžibajramović, E.; Schaufeli, W.; De Witte, H. The ultra-short version of the Burnout Assessment Tool (BAT4)–development, validation, and measurement invariance across countries, age and gender. PLOS ONE 2024, 19, e0297843. [Google Scholar] [CrossRef]
- Vazquez, A. C. S.; Freitas, C. P. P. D.; Schaufeli, W. B.; Witte, H. D.; Hutz, C. S. Evidence of Validity for the Brazilian Burnout Assessment Tool (BAT-Brazil). Avaliação Psicológica 2025, 24. [Google Scholar] [CrossRef]
- Tomas, J.; Seršić, D.M.; Mikac, U.; Rebernjak, B.; Buško, V.; De Witte, H. Validation of the Croatian version of the short form of the Burnout Assessment Tool: Findings from a nationally representative sample. Int. J. Sel. Assess. 2023, 32, 40–53. [Google Scholar] [CrossRef]
- Vinueza-Solórzano, A.M.; Portalanza-Chavarría, C.A.; de Freitas, C.P.P.; Schaufeli, W.B.; De Witte, H.; Hutz, C.S.; Vazquez, A.C.S. The Ecuadorian Version of the Burnout Assessment Tool (BAT): Adaptation and Validation. Int. J. Environ. Res. Public Heal. 2021, 18, 7121. [Google Scholar] [CrossRef]
- Hakanen, J.; Kaltiainen, J. Työuupumuksen arviointi Burnout Assessment Tool (BAT) -menetelmällä [Assessment of burnout using the Burnout Assessment Tool (BAT) method; In Finnish); Finnish Institute of Occupational Health (Työterveyslaitos): Helsinki, 2022; Available online: www.ttl.fi.
- Androulakis, G.S.; Georgiou, D.A.; Lainidi, O.; Montgomery, A.; Schaufeli, W.B. The Greek Burnout Assessment Tool: Examining Its Adaptation and Validity. Int. J. Environ. Res. Public Heal. 2023, 20, 5827. [Google Scholar] [CrossRef] [PubMed]
- Consiglio, C.; Mazzetti, G.; Schaufeli, W.B. Psychometric Properties of the Italian Version of the Burnout Assessment Tool (BAT). Int. J. Environ. Res. Public Heal. 2021, 18, 9469. [Google Scholar] [CrossRef] [PubMed]
- Angelini, G.; Buonomo, I.; Benevene, P.; Consiglio, P.; Romano, L.; Fiorilli, C. The Burnout Assessment Tool (BAT): A Contribution to Italian Validation with Teachers’. Sustainability 2021, 13, 9065. [Google Scholar] [CrossRef]
- Mazzetti, G.; Consiglio, C.; Santarpia, F.P.; Borgogni, L.; Guglielmi, D.; Schaufeli, W.B. Italian Validation of the 12-Item Version of the Burnout Assessment Tool (BAT-12). Int. J. Environ. Res. Public Heal. 2022, 19, 8562. [Google Scholar] [CrossRef]
- Romano, L.; Angelini, G.; Consiglio, P.; Fiorilli, C. An Italian Adaptation of the Burnout Assessment Tool-Core Symptoms (BAT-C) for Students. Educ. Sci. 2022, 12, 124. [Google Scholar] [CrossRef]
- Sakakibara, K.; Shimazu, A.; Toyama, H.; Schaufeli, W.B. Validation of the Japanese Version of the Burnout Assessment Tool. Front. Psychol. 2020, 11, 1819. [Google Scholar] [CrossRef]
- Cho, S. A Preliminary Validation Study for the Korean version of the Burnout Assessment Tool (K-BAT). Korean J. Ind. Organ. Psychol. 2020, 33, 461–499. [Google Scholar] [CrossRef]
- Lazauskaitė-Zabielskė, J.; Žiedelis, A.; Jakštienė, R.; Urbanavičiūtė, I.; De Witte, H. The Lithuanian version of the Burnout Assessment Tool (BAT-LT): psychometric characteristics of the primary and secondary symptoms scales. Front. Psychol. 2023, 14, 1287368. [Google Scholar] [CrossRef]
- De Beer, L.T.; Christensen, M.; Sørengaard, T.A.; Innstrand, S.T.; Schaufeli, W.B. The psychometric properties of the Burnout Assessment Tool in Norway: A thorough investigation into construct-relevant multidimensionality. Scand. J. Psychol. 2023, 65, 479–489. [Google Scholar] [CrossRef]
- Basińska, B.; Gruszczyńska, E.; Schaufeli, W. The Polish adaptation of the Burnout Assessment Tool (BAT-PL) by Schaufeli et al. Psychiatr. Polska 2023, 57, 223–235. [Google Scholar] [CrossRef]
- Sinval, J.; Vazquez, A.C.S.; Hutz, C.S.; Schaufeli, W.B.; Silva, S. Burnout Assessment Tool (BAT): Validity Evidence from Brazil and Portugal. Int. J. Environ. Res. Public Heal. 2022, 19, 1344. [Google Scholar] [CrossRef] [PubMed]
- Oprea, B.; Iliescu, D.; De Witte, H. Romanian Short Version of the Burnout Assessment Tool: Psychometric Properties. Evaluation Heal. Prof. 2021, 44, 406–415. [Google Scholar] [CrossRef] [PubMed]
- Popescu, B.; Maricuțoiu, L.P.; De Witte, H. The student version of the Burnout assessement tool (BAT): psychometric properties and evidence regarding measurement validity on a romanian sample. Curr. Psychol. 2023, 43, 2037–2051. [Google Scholar] [CrossRef] [PubMed]
- De Beer, L.T.; Schaufeli, W.B.; Bakker, A.B. Investigating the validity of the short form Burnout Assessment Tool: A job demands-resources approach. Afr. J. Psychol. Assess. 2022, 4, 9. [Google Scholar] [CrossRef]
- Koçak, Ö.; Gençay, O.; Schaufeli, W. BAT-TR: Tükenmişlik Ölçme Aracı’nın (BAT) Türkçeye Uyarlanması. Stud. Psychol. Calismalari Derg. 2022, 42, 509–549. [Google Scholar] [CrossRef]
- Hadžibajramović, E.; Schaufeli, W.; De Witte, H. A Rasch analysis of the Burnout Assessment Tool (BAT). PLOS ONE 2020, 15, e0242241. [Google Scholar] [CrossRef]
- de Beer, L.T.; Schaufeli, W.B.; De Witte, H.; Hakanen, J.J.; Shimazu, A.; Glaser, J.; Seubert, C.; Bosak, J.; Sinval, J.; Rudnev, M. Measurement Invariance of the Burnout Assessment Tool (BAT) Across Seven Cross-National Representative Samples. Int. J. Environ. Res. Public Heal. 2020, 17, 5604. [Google Scholar] [CrossRef]
- Macedo, M.J.d.A.; de Freitas, C.P.P.; Bermudez, M.B.; Vazquez, A.C.S.; Salum, G.A.; Dreher, C.B. The shared and dissociable aspects of burnout, depression, anxiety, and irritability in health professionals during COVID-19 pandemic: A latent and network analysis. J. Psychiatr. Res. 2023, 166, 40–48. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; Taris, T.W. The conceptualization and measurement of burnout: Common ground and worlds apart. Work. Stress 2005, 19, 256–262. [Google Scholar] [CrossRef]
- Terluin, B.; van Marwijk, H.W.; Adèr, H.J.; de Vet, H.C.; Penninx, B.W.; Hermens, M.L.; A van Boeijen, C.; van Balkom, A.J.; van der Klink, J.J.; AB Stalman, W. The Four-Dimensional Symptom Questionnaire (4DSQ): a validation study of a multidimensional self-report questionnaire to assess distress, depression, anxiety and somatization. BMC Psychiatry 2006, 6, 34–34. [Google Scholar] [CrossRef]
- Nakao, M. Work-related stress and psychosomatic medicine. Biopsychosoc. Med. 2010, 4, 4–4. [Google Scholar] [CrossRef]
- Dressler, W.W. Psychosomatic symptoms, stress, and modernization: A model. Cult. Med. Psychiatry 1985, 9, 257–286. [Google Scholar] [CrossRef]
- Marchand, A.; Demers, A.; Durand, P. Does work really cause distress? The contribution of occupational structure and work organization to the experience of psychological distress. Soc. Sci. Med. 2005, 61, 1–14. [Google Scholar] [CrossRef]
- Maslach, C.; Leiter, M. Understanding the burnout experience: recent research and its implications for psychiatry. World psychiatry 2016, 15, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Salvagioni, D.A.J.; Melanda, F.N.; Mesas, A.E.; González, A.D.; Gabani, F.L.; De Andrade, S.M. Physical, psychological and occupational consequences of job burnout: A systematic review of prospective studies. PLoS ONE 2017, 12, e0185781. [Google Scholar] [CrossRef] [PubMed]
- Desart, S.; De Witte, H. Burnout 2.0 — A new look at the conceptualization of burn-out. In The fun and frustration of modern working life; Taris, T., Peeters, M., De Witte, H., Eds.; Pelckmans Pro: Kaltmthout, 2019; pp. 1430–152. [Google Scholar]
- Schaufeli, W.B.; De Witte, H.; Hakanen, J.J.; Kaltiainen, J.; Kok, R. How to assess severe burnout? Cutoff points for the Burnout Assessment Tool (BAT) based on three European samples. Scand. J. Work. Environ. Heal. 2023, 49, 293–302. [Google Scholar] [CrossRef]
- Golino, H.F.; Epskamp, S. Exploratory graph analysis: A new approach for estimating the number of dimensions in psychological research. PLOS ONE 2017, 12, e0174035. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Chen, Z. Extended Bayesian information criteria for model selection with large model spaces. Biometrika 2008, 95, 759–771. [Google Scholar] [CrossRef]
- Golino, H.; Shi, D.; Christensen, A.P.; Garrido, L.E.; Nieto, M.D.; Sadana, R.; Thiyagarajan, J.A.; Martinez-Molina, A. Investigating the performance of exploratory graph analysis and traditional techniques to identify the number of latent factors: A simulation and tutorial. Psychol. Methods 2020, 25, 292–320. [Google Scholar] [CrossRef]
- Christensen, A.P.; Golino, H. Estimating the Stability of Psychological Dimensions via Bootstrap Exploratory Graph Analysis: A Monte Carlo Simulation and Tutorial. Psych 2021, 3, 479–500. [Google Scholar] [CrossRef]
- Forero, C.G.; Maydeu-Olivares, A.; Gallardo-Pujol, D. Factor Analysis with Ordinal Indicators: A Monte Carlo Study Comparing DWLS and ULS Estimation. Struct. Equ. Model. A Multidiscip. J. 2009, 16, 625–641. [Google Scholar] [CrossRef]
- Savalei, V.; Rhemtulla, M. The performance of robust test statistics with categorical data. Br. J. Math. Stat. Psychol. 2012, 66, 201–223. [Google Scholar] [CrossRef] [PubMed]
- Yang-Wallentin, F.; Jöreskog, K.G.; Luo, H. Confirmatory Factor Analysis of Ordinal Variables With Misspecified Models. Struct. Equ. Model. A Multidiscip. J. 2010, 17, 392–423. [Google Scholar] [CrossRef]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Rosseel, Y. lavaan: An R package for structural equation modeling. Journal of statistical software 2012, 48(1), 1–36. [Google Scholar] [CrossRef]
- Choi, S.W.; Gibbons, L.E.; Crane, P.K. lordif: An. RPackage for Detecting Differential Item Functioning Using Iterative Hybrid Ordinal Logistic Regression/Item Response Theory and Monte Carlo Simulations 2011, 39, 1–30. [Google Scholar] [CrossRef]
- Jodoin, M.G.; Gierl, M.J. Evaluating Type I Error and Power Rates Using an Effect Size Measure With the Logistic Regression Procedure for DIF Detection. Appl. Meas. Educ. 2001, 14, 329–349. [Google Scholar] [CrossRef]
- Lima, M. Conceitos da teoria de resposta ao item (TRI) que você precisa conhecer. Blog Psicometria Online. 2024. Available online: https://www.blog.psicometriaonline.com.br/conceitos-da-teoria-de-resposta-ao-item-que-voce-precisa-conhecer.
- Marchand, A.; Blanc, M. Occupation, work organisation conditions and the development of chronic psychological distress. Work 2011, 40, 425–435. [Google Scholar] [CrossRef]
- Adamsson, A.; Bernhardsson, S. Symptoms that may be stress-related and lead to exhaustion disorder: a retrospective medical chart review in Swedish primary care. BMC Fam. Pr. 2018, 19, 172. [Google Scholar] [CrossRef]
- Bes, I.; Shoman, Y.; Al-Gobari, M.; Rousson, V.; Canu, I.G. Organizational interventions and occupational burnout: a meta-analysis with focus on exhaustion. Int. Arch. Occup. Environ. Heal. 2023, 96, 1211–1223. [Google Scholar] [CrossRef]
- Tavakol, M.; Wetzel, A. Factor Analysis: a means for theory and instrument development in support of construct validity. Int. J. Med Educ. 2020, 11, 245–247. [Google Scholar] [CrossRef]
- Tavakol, M.; Dennick, R. Making sense of Cronbach's alpha. Int. J. Med. Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef]
- Maslach, C. Burnout: A multidimensional perspective. In Professional burnout, 1st ed; Routledge: Abingdon, UK, 1993. [Google Scholar]
- Schaufeli, W.B.; Maslach, C.; Marek, T. The future of burnout. In Professional burnout; Routledge; pp. 253–259.
Table 1.
Fit Indices for the models tested.
| Model |
χ²(gl) [p-value] |
CFI | TLI | RMSEA [IC 90%] | SRMR |
| Unidimensional (EGA) |
439.718 (35) [p < .001] |
.951 | .937 | .115 [0.106 – 0.125] | .055 |
| Two-Factor Oblique | 262.529 (34) [p < .001] |
.972 | .963 | .088 [0.078 - 0.098] | .041 |
| Bifactor with Two Oblique Factors | 90.354 (24) [p < .001] |
.992 | .985 | .056 [0.044 - 0.069] | .023 |
Table 2.
Factor Loadings for the Tested Models.
| Item | Model | |||||
| Unidimensional | Two-Factor Oblique | Bifactor with Two Oblique Factors | ||||
| PC1. palpitations or chest pain | .724 | .755 | .877 | .015 | ||
| PC2. stomach and/or intestinal complaints | .699 | .733 | .658 | .319 | ||
| PC3. Headaches | .663 | .698 | .514 | .540 | ||
| PC4. Muscle pain | .722 | .758 | .529 | .668 | ||
| PC5. Getting sick often | .670 | .704 | .598 | .371 | ||
| PD2. trouble falling or staying asleep | .690 | .711 | .581 | .394 | ||
| PD3. worry | .761 | .790 | .535 | .654 | ||
| PD4. tense and stressed | .844 | .875 | .608 | .700 | ||
| PD5. anxious and/or suffer from panic attacks | .842 | .871 | .754 | .409 | ||
| PD6. Noise and crowds are disturbing. | .677 | .696 | .602 | .329 | ||
Table 3.
DIF Statistics for Items in the Psychosomatic Complaints Scale.
| Item | Group | p-value | Pseudo R² Nagelkerke | ||||
| Model 1 vs Model 2 | Model 1 vs Model 3 | Model 2 vs Model 3 | Model 1 vs Model 2 | Model 1 vs Model 3 | Model 2 vs Model 3 | ||
| Palpitations or chest pain | Sex | .0038 | .0139 | .6818 | .0026 | .0027 | .0001 |
| Stomach and/or intestinal complaints | Sex | .8816 | .475 | .2259 | 0 | .0004 | .0004 |
| Headaches | Sex | .5449 | .6471 | .4778 | .0001 | .0002 | .0001 |
| Muscle pain | Sex | .8519 | .224 | .0855 | 0 | .0006 | .0006 |
| Getting sick often | Sex | .0033 | .0123 | .6896 | .0024 | .0024 | 0 |
| Palpitations or chest pain | Age | .7037 | .0699 | .0186 | .0002 | .0027 | .0025 |
| stomach and/or intestinal complaints | Age | .3612 | .4687 | .4668 | .0005 | .0009 | .0004 |
| Headaches | Age | .0001 | .0002 | .334 | .0042 | .0047 | .0005 |
| Muscle pain | Age | .0049 | .0259 | .8123 | .0022 | .0023 | .0001 |
| Getting sick often | Age | .1462 | .3022 | .6028 | .0011 | .0014 | .0003 |
| palpitations or chest pain | Education | .0278 | .0782 | .5408 | .0027 | .0032 | .0005 |
| Stomach and/or intestinal complaints | Education | .8104 | .4145 | .1723 | .0001 | .0012 | .0011 |
| Headaches | Education | .1941 | .0382 | .0324 | .0009 | .0028 | .0019 |
| Muscle pain | Education | .0054 | .0222 | .6156 | .0027 | .003 | .0002 |
| Getting sick often | Education | .2161 | .4865 | .8273 | .0009 | .0011 | .0001 |
Table 4.
DIF Statistics for Items in the Psychological Distress Scale.
| Item | Group | p-value | Pseudo R² Nagelkerke | ||||
| Model 1 vs Model 2 | Model 1 vs Model 3 | Model 2 vs Model 3 | Model 1 vs Model 2 | Model 1 vs Model 3 | Model 2 vs Model 3 | ||
| Trouble falling or staying asleep. | Sex | .6072 | .7703 | .6117 | .0001 | .0002 | .0001 |
| Worry. | Sex | .1364 | .3227 | .8339 | .0003 | .0003 | 0 |
| Tense and stressed. | Sex | .0898 | .2215 | .7112 | .0003 | .0003 | 0 |
| Anxious and/or suffer from panic attacks. | Sex | .0291 | .0758 | .5277 | .0009 | .001 | .0001 |
| Noise and crowds are disturbing. | Sex | .0346 | .1064 | .8983 | .0016 | .0016 | 0 |
| Trouble falling or staying asleep. | Age | 0 | 0 | .3356 | .0174 | .0181 | .0007 |
| Worry. | Age | .6434 | .9269 | .9992 | .0001 | .0001 | 0 |
| Tense and stressed. | Age | .0001 | .0008 | .5328 | .0016 | .0017 | .0001 |
| Anxious and/or suffer from panic attacks. | Age | .0283 | .0236 | .1253 | .0013 | .0021 | .0008 |
| Noise and crowds are disturbing. | Age | .0123 | .0553 | .8005 | .0031 | .0033 | .0002 |
| Trouble falling or staying asleep. | Education | .43 | .5482 | .5041 | .0007 | .0013 | .0006 |
| Worry. | Education | .9241 | .27 | .0815 | 0 | .0009 | .0009 |
| Tense and stressed. | Education | .7487 | .9274 | .8603 | .0001 | .0001 | 0 |
|
Anxious and/or suffer from panic attacks. |
Education | .3853 | .4732 | .4441 | .0005 | .0009 | .0004 |
| Noise and crowds are disturbing. | Education | .8451 | .101 | .0245 | .0001 | .0033 | .0031 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



