Submitted:
22 January 2026
Posted:
27 January 2026
You are already at the latest version
Abstract
Background: The biopsychosocial model positions fibromyalgia (FM) as the result of altered pain modulation shaped by trauma, psychological vulnerability, and structural stressors. The Sense of Coherence (SOC) may be a key resilience factor explaining differences in symptom severity after similar hardships. Objectives: To evaluate whether SOC mediates and/or moderates associations between trauma-related adver-sity and symptom burden in FM, and whether comorbidities, medication use, healthcare factors, or treatment engagement modify these relationships. Methods: In this cross-sectional study, 2,099 women with FM completed an online survey assessing adversity, psychosocial factors, core symptoms, healthcare support, treatment engagement, and medication use. A theo-ry-driven SOC composite followed Antonovsky’s model (comprehensibility, manageability, meaningfulness). Linear regression evaluated adversity–symptom associations, SOC mediation, and moderation by SOC and medication classes. Results: Higher adversity predicted lower SOC (e.g., cumulative abuse: B=−0.25), and lower SOC predicted higher symptom burden (e.g., Fibromyalgia Impact Questionnaire (FIQ): B=−6.77), producing robust indirect effects (cognitive symptoms: 0.22; FIQ: 1.69). SOC also moderated the effects of adversity on fatigue and global impact, weakening associations at higher SOC. Comorbidities showed modest influence: hypertension had minor indirect effects (ab=0.27), scheduled consultation produced small interactions (cognition β=−0.38 to −0.46; fatigue β=0.36), and stroke showed the only clinically meaningful moderation (β≈4.9–5.2), all far smaller than SOC effects. Conclusions: SOC plays a central mechanistic role linking trauma to FM symptoms, acting as both a pathway and resilience factor. Strengthening SOC may reduce symptom burden and improve outcomes.
Keywords:
fibromyalgia
; coherence sense
; trauma exposure
; psychosocial deprivation
; resilience
; mediation analysis
1. Introduction
Fibromyalgia (FM) is a chronic pain syndrome characterized by widespread musculoskeletal pain, fatigue, non-restorative sleep, cognitive difficulties, and impaired quality of life [1]. Fibromyalgia affects an estimated 2%–5% of the global population, with consistently higher prevalence in women (4%–7%) than in men (1%–2%) [2,3]. In Brazil, the condition affects approximately 2.5% of adults [4]. Its impact extends beyond individual suffering: a large Danish cohort showed markedly higher healthcare spending, reduced income, and increased disability pension rates among patients and even their spouses, with financial losses beginning years before diagnosis and societal costs reaching €27,000 per patient annually [5]. These findings highlight FM as a multidimensional condition. Consistent with this broader impact, a UK Biobank study of 475,171 adults demonstrated that individuals with chronic widespread pain—a phenotype closely aligned with FM—had a significantly increased risk of major cardiovascular events, with hazard ratios ranging from 1.14 to 1.48 after full adjustment [6].
This broader complexity aligns with the biopsychosocial model, which frames FM as a condition characterized by altered central pain modulation and multisystem dysregulation, shaped by emotional, cognitive, and social factors [7]. Psychological vulnerability, emotional dysregulation, and adversity contribute to greater symptom severity [8,9,10,11]. However, biological mechanisms alone do not provide a complete explanation for chronic pain conditions. The social dimension is often operationalized through individual-level traits, potentially underestimating the role of broader structural factors. Macro-level determinants—economic instability, job insecurity, discrimination, environmental stressors, and barriers to healthcare—shape vulnerability to chronic pain and worsen outcomes [12,13,14]. These structural pressures interact with neurobiological and psychological mechanisms across the life course, contributing to cumulative stress and dysregulation consistent with allostatic load models [15,16,17]. Complementary theoretical frameworks—such as the fear-avoidance model [18] and the maladaptive learning model [19] illustrate how catastrophizing, avoidance behaviors, and negative symptom interpretation reinforce pain persistence and contribute to disability in fibromyalgia.
A large body of evidence highlights trauma and adverse life experiences as key contextual factors in FM. Histories of childhood abuse, sexual violence, persistent verbal and emotional aggression, and significant interpersonal loss are far more common among individuals with FM than in the general population [20]. They are associated with earlier disease onset, greater symptom severity, and higher psychological comorbidity [21]. Yet not all trauma-exposed individuals develop FM, and among those who do, symptom trajectories vary widely, suggesting the presence of resilience mechanisms that modulate vulnerability. Antonovsky’s salutogenic model provides an essential conceptual lens for understanding these resilience processes. At the center of this model is the construct of Sense of Coherence (SOC). This global orientation reflects the degree to which individuals perceive their lives as comprehensible, manageable, and meaningful [22]. People with a higher SOC tend to experience less emotional distress, adopt healthier habits, and manage chronic illnesses more effectively. Studies have shown that low SOC levels are associated with greater fatigue, emotional distress, and higher symptom burden [23,24]. Trauma exposure has been shown to weaken the Sense of Coherence (SOC). Early evidence demonstrated that traumatic experiences reduce SOC [25], while complementary findings showed that SOC shapes how individuals interpret and respond to adverse events, thereby influencing their impact on health outcomes [26,27]. Contemporary evidence further reinforces this pattern: SOC is sensitive to cumulative emotional and psychological load and tends to decline under sustained adversity, with lower SOC consistently associated with greater psychological distress in chronic pain populations [24]. In addition, SOC has been identified as a resilience factor that influences mental health trajectories across development and adulthood, supporting its role as a key psychological resource in contexts of chronic stress [28]. Integrating SOC into the biopsychosocial-structural perspective suggests that fibromyalgia severity reflects not only nociplastic mechanisms and life-course adversity but also individual differences in how people make sense of and cope with illness-related stressors. This contemporary evidence reinforces the understanding that trauma exposure weakens SOC and that SOC, in turn, shapes how adversity becomes biologically and psychologically embedded in health outcomes.
While the concept of SOC holds significance, research on it within the context of fibromyalgia remains limited. Earlier studies have faced challenges, including using small groups of participants, varying techniques for assessing trauma, and relying on superficial explanations rather than examining deeper causes [29,30]. SOC may mediate and moderate the adversity-symptom relationship, but most evidence comes from chronic pain studies rather than FM [24]. Few studies have evaluated these mechanisms across key clinical domains—pain, fatigue, cognition, sleep, and global impact—in large, well-defined FM cohorts simultaneously, while also incorporating patient-level factors such as treatment adherence, quality of care received, medication use, chronic comorbid conditions, and occupational/labor status. Medication use adds another underexplored layer to the trauma–symptom relationship. Individuals with greater adversity and more severe symptoms are more likely to use dual-action or tricyclic antidepressants, benzodiazepines, hypnotics, opioids, or multiple analgesics [31]. These medications may influence trauma–symptom associations through pharmacological effects or confounding by indication [32] and may also shape coping and neurobiological pain-modulation pathways. However, no study has evaluated whether medication classes moderate trauma–symptom associations in FM or how these effects interact with SOC within a unified framework.
In this study, we address these gaps using a large, community-based Brazilian cohort of women with fibromyalgia, extensively characterized across adverse life experiences, cumulative abuse indices, psychological and functional measures, chronic medical comorbidities, aspects of care received, medication use, and symptom severity (fibromyalgia impact, fatigue, cognitive symptoms, non-restorative sleep, and functioning). Our primary objective was to evaluate whether Sense of Coherence (SOC) operates as both a mediator and an effect modifier in the relationship between trauma-related variables and fibromyalgia symptoms. Secondary objectives were to examine whether commonly used medications (e.g., antidepressants, hypnotics, analgesics, opioids) moderate trauma–symptom associations and to explore combined pharmacological and psychological influences on symptom burden. We hypothesized that adversity would relate to higher symptom severity, that SOC would mediate and potentially moderate adversity–outcome associations, and that medication classes would show differential moderation patterns reflecting pharmacological and clinical selection mechanisms.
2. Materials and Methods
2.1. Design Overview, Setting, and Participants
This cross-sectional study followed the STROBE guidelines. All participants provided written informed consent prior to participation through a signed informed consent form (ICF). The study was conducted in accordance with the ethical principles of the Declaration of Helsinki. The protocol was approved by the Research Ethics Committee of Hospital de Clínicas de Porto Alegre, Brazil (IRB #2023-0210). The recruitment period ran from August 1, 2023, to November 30, 2023.
2.2. Recruitment, Inclusion, and Exclusion Criteria
Individuals volunteered after responding to announcements in public spaces or advertisements on websites such as Facebook and Craigslist. These advertisements were shared through the networks of the National Association of Fibromyalgia and Related Diseases (ANFIBRO). A live online session introduced the project and addressed public questions. A message explaining the study’s purpose was shared on social media to invite people to take part.
Interested individuals accessed the study through a provided link. After confirming their interest, they received an informed consent form. Upon signing, participants received a questionnaire about sociodemographic data and the American College of Rheumatology (ACR-2016) questionnaire [1], via the REDCap (Research Electronic Data Capture) platform. The evaluation collected medical history and symptom details to confirm diagnoses. The research team managed recruitment by sending up to three messages per individual. If registration remained incomplete after 10 days, an additional reminder was sent. After participants completed their registration, they did not receive any additional messages.
To participate, individuals had to be at least 18 years old, able to read, and have a confirmed fibromyalgia diagnosis according to the 2016 American College of Rheumatology [1]. The 2016 ACR criteria stipulate that: (1) generalized pain, defined as pain in at least 4 of 5 regions, must be present; (2) symptoms must be persistent for at least 3 months; (3) the Widespread Pain Index (WPI) must be ≥7 with a Symptom Severity Scale (SSS) score ≥5, or a WPI of 4–6 with an SSS score ≥9; and (4) the diagnosis is valid regardless of other comorbid conditions, and the presence of fibromyalgia does not exclude additional clinically relevant illnesses. Consistent with these criteria, participants needed a combined WPI + SSS score ≥13. Participants were excluded if they didn’t meet the 2016 ACR criteria or did not complete study questionnaires after three follow-up attempts.
2.3. Instruments and Assessment
After providing consent, participants completed the questionnaires via REDCap. To minimize misunderstanding, each item included accessible instructions. All instruments were validated for the Brazilian population, ensuring accurate and reliable measurement. The research team was trained to guide the recruitment process and instruct participants on how to meet the study's requirements. Response monitoring was conducted continuously, and in cases of incomplete answers, up to three follow-up contacts were made to ensure correction. Weekly meetings were held to address any doubts that arose during the study, enabling evaluators to calibrate. Instructions for all procedures and assessment methods were included in a standardized instruction manual.
2.4. Primary Outcome Measures (Dependent Variables)
The Fibromyalgia Impact Questionnaire (FIQ) was used to assess the impact of fibromyalgia on function, symptoms, and overall quality of life across 10 domains, with higher scores indicating greater disease burden (e.g., physical functioning, pain intensity, fatigue, stiffness, sleep quality, mood, work impairment, and ability to perform daily activities), with higher scores indicating greater disease burden. We used the version validated for the Brazilian population [33].
The Symptom Severity Scale (SSS) from the 2016 revision of the American College of Rheumatology (ACR) fibromyalgia diagnostic criteria was used to assess the severity of three core somatic symptom domains: fatigue, waking unrefreshed, and cognitive symptoms. Each symptom was rated according to its severity over the past week on a 4-point scale ranging from 0 (no problem) to 3 (severe, pervasive, continuous, or life-disturbing problems) [1].
2.4.1. Adversity and Psychosocial Measures (Primary Predictors)
Adversity was operationalized using both specific event indicators and cumulative indices reflecting overall trauma burden. Trauma-related variables were assessed using dichotomous items (yes/no) evaluating whether participants associated the onset or worsening of fibromyalgia symptoms with specific adverse experiences, including:
- (i)
- major life events (e.g., loss of a loved one, marriage, job loss);
- (ii)
- verbal aggression causing ongoing distress;
- (iii)
- emotional aggression causing ongoing distress; and
- (iv)
- sexual abuse, including unwanted physical contact, coercive advances, verbal harassment, emotional pressure, or non-consensual sexual acts.
A cumulative adversity index (cumulative abuse; range 0–4) was derived by summing exposure across abuse-related domains, providing an overall measure of trauma burden. In addition, an appraisal-related adversity variable captured self-reported perception that fibromyalgia symptoms were related to persistent physical aggression, reflecting subjective attribution of symptom onset or worsening to aggressive experiences. Thus, adversity was represented in the analyses by both the cumulative abuse index and by specific adversity indicators, allowing evaluation of global trauma load as well as domain-specific effects.
For descriptive analyses, cumulative abuse was additionally categorized into three groups (0, 1, and ≥2 types of abuse) to characterize exposure profiles in Table 1 and Table 2; however, all regression, mediation, and moderation models used the continuous cumulative abuse score (range 0–4) to preserve dose–response information and maximize statistical power.
2.4.2. Psychosocial and Central Pain Processing Measures
Psychological and pain-processing constructs relevant to nociplastic mechanisms were assessed using validated instruments. Pain catastrophizing was measured using the Pain Catastrophizing Scale (PCS; total score 0–52), covering rumination, magnification, and helplessness domains [34]. Central sensitization symptoms were assessed using the Central Sensitization Inventory (CSI; 0–100), capturing diffuse pain, fatigue, non-restorative sleep, cognitive difficulties, headaches, and urological complaints [35]. Depressive symptoms were evaluated using the Patient Health Questionnaire-9 (PHQ-9; 0–27), with scores ≥9 indicating clinically relevant depression in Brazilian populations [36]. Psychiatric diagnosis burden was defined as non-depressive psychiatric comorbidity and operationalized as a cumulative count of self-reported lifetime diagnoses of anxiety disorders, bipolar disorder, panic disorder, and post-traumatic stress disorder (PTSD); this variable was analyzed separately from depressive symptoms, which were assessed exclusively using the PHQ-9 total score. Kinesiophobia was measured using the Tampa Scale for Kinesiophobia (TSK), reflecting fear of movement and perceived threat related to physical activity [37]. Alcohol consumption patterns were screened using the Alcohol Use Disorders Identification Test – Consumption (AUDIT-C) [38].
2.4.3. Sociodemographic and Clinical Characteristics
Demographic and clinical covariates included: age (years), educational attainment (years or level of formal schooling), body mass index category, occupational status (unemployed, employed/student/self-employed, retired, disability benefits), and fibromyalgia duration (years) and history of medical comorbidities.
2.5. Sense of Coherence (SOC) Composite and Indicator Variables
A dedicated SOC questionnaire was not administered. Instead, we constructed a theory-driven SOC surrogate aligned with Antonovsky’s salutogenic framework, operationalizing three theoretical domains: Meaningfulness, Manageability, and Comprehensibility. This SOC surrogate represents an integrated psychosocial functioning profile rather than a stable personality trait, and therefore mediation effects should be interpreted as statistical decomposition of shared psychosocial vulnerability rather than causal psychological pathways. Accordingly, indicators included in each domain were not intended to represent symptom severity per se, but rather perceived bodily threat, predictability, and coherence of illness experience, as well as perceived coping resources and engagement with care, consistent with the theoretical structure of the SOC framework.
The meaningfulness domain was constructed from affective and cognitive-emotional burden indicators, including pain catastrophizing (total PCS score), depressive symptom severity assessed exclusively by the PHQ-9 total score, and psychiatric diagnosis burden reflecting non-depressive psychiatric comorbidity, operationalized as a cumulative count of self-reported lifetime diagnoses of anxiety disorders, bipolar disorder, panic disorder, and post-traumatic stress disorder (PTSD). These variables represent affective and cognitive valuation of symptoms and life context, capturing the extent to which individuals perceive their experiences as emotionally meaningful and interpretable.
The Manageability domain incorporated indicators of functional coping resources, behavioral engagement, and healthcare-related support, including work status (categorical variable: unemployed, employed, student, caregiver, self-employed, retired, and receiving disability benefits), physical activity (regular participation in physical activities). Medication-adherence behaviors (consistent medication use as prescribed, adherence to the recommended treatment plan, frequent medication forgetfulness [reverse-coded], and self-initiated medication interruption [reverse-coded]), treatment engagement and perceived control (collaborative treatment decision-making, patient input on prescribed treatment, waiting time for fibromyalgia specialist consultation, and global treatment quality assessment), and complexity of pharmacological treatment (number of medication classes in use). These variables represent internal and external coping resources. Together, they capture perceived control over health-related demands.
Comprehensibility reflected cognitive understanding and perceived predictability of symptoms, incorporating indicators related to bodily threat appraisal and illness interpretation, including diagnosis of other pain conditions (musculoskeletal and neuropathic pain), central sensitization (CSI score), kinesiophobia (TSK score), perceived linkage between symptoms and physical aggression, and age at fibromyalgia onset (before 18 years, 19–25 years, 26–40 years, and >40 years). Although CSI and TSK are commonly used as symptom-related instruments, in this composite they were conceptualized as proxies of bodily threat appraisal and illness predictability rather than as outcome measures, consistent with the theoretical structure of the comprehensibility component of SOC. Together, these indicators capture perceived threat, coherence, and interpretability of bodily experiences, consistent with the comprehensibility component of the SOC framework.
All indicators were directionally aligned so that higher values consistently reflected stronger SOC, and subsequently standardized (z-scores) to ensure comparability across scales. Domain-specific SOC scores were calculated as the means of standardized indicators within each domain. A global SOC composite was computed as the mean of the three domain scores and then standardized (SOC_new_composite_z) for use in all regression, mediation, and moderation analyses. A detailed flowchart of the data transformation process and the full list of variables included in each domain are provided in Supplementary Figure S1.
Figure 1 summarizes the conceptual framework underlying the SOC composite and its role within the biopsychosocial pathways linking adverse experiences to fibromyalgia severity. The model integrates SOC dimensions with cumulative biological and psychosocial stress (allostatic load), illustrating how lower SOC amplifies symptom burden and functional impairment.
2.6. Covariates Included in Adjusted Models
All adjusted regression, mediation, and moderation models controlled for age, educational attainment, body mass index category and disability due to pain in daily activities.
2.7. Medication Constructs
For exploratory moderation analyses, we considered several medication groups as potential effect modifiers: (i) Antidepressants: tricyclic antidepressants, dual-action antidepressants, a combined tricyclic/dual indicator, and SSRIs (selective serotonin reuptake inhibitors). (ii) Sleep-related medications: melatonin, zolpidem, and benzodiazepines. (iii) Analgesic variables: non-opioid analgesics (NSAIDs, dyclonine/dyprinon, acetaminophen), use opioid (any opioid use), and specific of opioid agents (codeine, morphine, oxycodone, methadone, and tramadol).
2.8. Efforts to Address Potential Sources of Bias
To minimize potential sources of bias, all study procedures were fully standardized through REDCap, ensuring identical administration, automated data capture, and removal of duplicate entries. Recruitment was broad and public, and all instruments used were validated for the Brazilian population, reducing measurement error. Sensitive items (e.g., trauma exposures) were self-administered online to limit bias to social desirability. The research team followed a structured operations manual, with weekly calibration meetings and continuous data-quality monitoring. Incomplete responses triggered up to three automated reminders to reduce attrition bias.
For the construction of the SOC composite, indicators were theory-driven and grouped into meaningfulness, manageability, and comprehensibility domains. All indicators were standardized, and reverse-coded, when necessary, to maintain consistent directionality. By selecting conceptually distinct and non-redundant indicators, we minimized collinearity within SOC domains and avoided inflation of mediation or moderation effects. All regression models were adjusted for key demographic and clinical confounders (age, education, BMI, disability due to pain in daily activities) to reduce residual confounding.
Missing data was minimized through structured follow-up to reduce incomplete questionnaires. SOC domain scores were calculated from the means of available indicators, preserving the construct’s theoretical structure and avoiding listwise deletion at the domain-construction stage. For inferential analyses, complete-case datasets were used, and all regression models were estimated to use the same analytic sample, as reflected by the uniform sample size reported in the tables. This approach ensures comparability across models and outcomes while avoiding biases introduced by data imputation.
2.9. Statistical Analysis
Descriptive analyses were conducted by categorizing participants according to cumulative abuse exposure (no abuse, one type of abuse, and two or more types of abuse), as presented in Table 1 and Table 2. Baseline characteristics were summarized across these groups to examine differences in sociodemographic, clinical, and psychosocial profiles. Categorical variables were expressed as frequencies and percentages, and continuous variables as means and standard deviations. Group comparisons were performed using χ² tests for categorical variables and independent-sample t tests or Mann–Whitney U tests for continuous variables, as appropriate. For descriptive purposes, cumulative abuse was categorized into three clinically interpretable groups; however, all inferential analyses used the continuous cumulative abuse score (range 0–4) to preserve dose–response information and maximize statistical power. Because cumulative abuse categories were derived from the same adversity indicators presented in descriptive tables, these variables are not independent across groups and should be interpreted as characterization of exposure profiles rather than as independent between-group comparisons.
All inferential analyses were conducted using linear regression models, with cumulative abuse (range 0–4) as the main adversity predictor and fibromyalgia impact (FIQ total score) as the primary outcome. Secondary outcomes included fatigue, cognitive symptoms, and non-restorative sleep, as measured by the Symptom Severity Scale. Unadjusted associations were first examined using simple linear regression (Outcome = β₀ + β₁ × Cumulative_abuse + ε). Adjusted models were then estimated including age (years), educational attainment (years of schooling), body mass index (BMI category), and disability due to pain in daily activities, excluding SOC from the covariate set. All mediation and moderation models were additionally adjusted for the same covariates.
To evaluate whether sense of coherence (SOC_new_composite_z) mediated the associations between cumulative abuse and each clinical outcome, regression-based mediation models were specified using a path-analytic framework: SOC_new_composite_z = α₀ + α₁ × Cumulative_abuse + εₐ (path a), and Outcome = γ₀ + γ₁ × Cumulative_abuse + γ₂ × SOC_new_composite_z + εᵧ (paths b and c′). Indirect effects were calculated as the product a × b and tested using Sobel tests, and were additionally confirmed using nonparametric bootstrapped confidence intervals based on 5,000 resamples of the original dataset. Mediation analyses were conducted separately for each outcome and for each adversity indicator (cumulative abuse and specific adversity domains).
To test whether SOC modified the association between cumulative abuse and clinical outcomes, interaction models were estimated as Outcome = δ₀ + δ₁ × Cumulative_abuse + δ₂ × SOC_new_composite_z + δ₃ × (Cumulative_abuse × SOC_new_composite_z) + ε. A statistically significant interaction coefficient (δ₃) was interpreted as evidence that SOC modifies (buffers or amplifies) the effect of adversity on symptom severity. Exploratory moderation analyses were also conducted to examine whether medication classes and selected clinical variables modified adversity–outcome associations, using the same interaction framework.
Missing data were minimized through structured follow-up. SOC domain scores were calculated from the means of available indicators to preserve the construct’s theoretical structure and avoid listwise deletion at the domain-construction stage. For inferential analyses, complete-case datasets were used, and all regression models were estimated using the same analytic sample, as reflected by the uniform sample size reported in the tables. For all models, regression coefficients, 95% confidence intervals, and p values were reported. Model assumptions (linearity, homoscedasticity, and normality of residuals) were assessed using standard diagnostic plots. All statistical analyses were performed using IBM SPSS Statistics for Windows, version 22 (IBM Corp., Armonk, NY, USA), and R software (version 4.4.2; R Foundation for Statistical Computing, Vienna, Austria). Statistical significance was set at p < 0.05 (two-tailed).
3. Results
3.1. Sample Baseline Characteristics
From the publicly available online survey, 4,200 individuals initiated the questionnaire. After removal of duplicate entries, 3,500 unique respondents remained, of whom 2,495 (71.3%) completed all required instruments. After excluding 295 respondents who did not meet fibromyalgia screening criteria and 101 men due to insufficient sample size for sex-stratified analyses, the final analytical cohort comprised 2,099 women.
Table 1 summarizes the demographic, socioeconomic, clinical, medication-use, and healthcare engagement characteristics of the study sample. Participants exposed to higher levels of cumulative abuse presented a more vulnerable social and clinical profile, including higher rates of work disability, greater use of psychotropic and pain-related medications, and indicators of lower treatment adherence and access to specialized care. These differences characterize a population with greater clinical complexity and justify adjustment for age, body mass index, and work disability in subsequent regression models.
3.2. Fibromyalgia Severity and Psychological Burden
Table 2 presents symptom severity scores according to cumulative abuse exposure categories (no abuse, one type of abuse, and two or more types of abuse). A graded increase in symptom burden was observed across abuse categories, particularly for fibromyalgia impact, cognitive symptoms, and non-restorative sleep, indicating a dose–response pattern between adversity exposure and clinical severity. Differences in fatigue scores across groups were comparatively smaller.
3.3. Validation and Distribution of SOC Surrogate
Discriminant validity was evaluated using correlation analyses between SOC domains and clinical outcomes (Supplementary Table S2). Correlations were of low to moderate magnitude, and no coefficients approached unity, indicating that SOC constructs are related to, but not redundant with, symptom severity measures. These findings support the conceptual distinctiveness of the SOC surrogate in relation to clinical outcomes, suggesting that it captures psychosocial organization of coping and illness interpretation rather than simply reflecting symptom burden.
3.4. Association between Cumulative Abuse and Clinical Outcomes
Table 3 summarizes adjusted linear regression models examining the association between cumulative abuse exposure (range 0–4) and symptom severity across four clinical domains: fibromyalgia impact (FIQ), cognitive dysfunction, fatigue, and non-restorative sleep. After adjustment for age, body mass index (BMI), and disability due to pain in daily activities, cumulative abuse was significantly associated with higher symptom burden across all outcomes. The positive linear coefficients indicate a dose–response relationship between increasing levels of lifetime adversity and multidimensional clinical severity.
Supplementary Table S3 shows analogous models using individual adversity indicators, with generally weaker and less consistent associations across symptom domains compared with cumulative abuse.
3.5. Sense of Coherence and Symptom Outcomes
3.5.1. Mediation Analysis: SOC as a Pathway Linking Adversity to Symptom Severity
Mediation models were estimated to test whether SOC_new_composite_z mediated the associations between adversity indicators and each clinical outcome.
Figure 2 (a–d) presents the mediation analyses assessing whether SOC_new_composite_z mediated the associations between multiple adversity indicators and the four clinical domains: symptoms of cognitive dysfunction, fatigue, non-restorative sleep, and global fibromyalgia impact (FIQ). Each adversity variable (including cumulative abuse, physical, verbal, emotional aggression, loss events, sexual abuse and the appraisal variable (self-reported perception that fibromyalgia symptoms are related to persistent physical aggression) was entered separately as the predictor, SOC_new_composite_z as the mediator, and one symptom domain as the outcome. Across all mediation models, the pattern was consistent and theoretically coherent. Higher adversity was associated with lower SOC (negative a-paths), In turn, higher SOC was associated with lower symptom severity, reflected in negative b-paths. Consequently, indirect effects (the product a × b) were uniformly positive, indicating that adversity contributes to symptom burden in part through reductions in SOC.
Title: SOC Mediates the Impact of Adversity on Cognitive, Fatigue, Sleep, and Global Symptom Burden
3.5.2. Mediation Findings across Clinical Domains
Table 4 provides full mediation models for all adversity indicators across cognitive symptoms, fatigue, non-restorative sleep, and global fibromyalgia impact (FIQ). Adversity exposures consistently predicted lower SOC (negative a-paths), and lower SOC was strongly associated with greater symptom severity (negative b-paths). In many cases, indirect effects exceeded direct effects and, at times, surpassed the magnitude of the total effect, indicating predominant or near-complete mediation. These effects were strongest for fatigue and cognitive dysfunction.
Overall, SOC emerges as a central regulatory mechanism linking adverse experiences to clinical symptomatology, explaining a meaningful proportion of symptom variability in fibromyalgia, and reinforcing the importance of SOC as a target for both mechanistic understanding and potential intervention strategies.
3.6. Moderation Analyses: SOC and Clinical Factors as Modifiers of Adversity Effects
This section examines whether the associations between adverse experiences and clinical outcomes vary according to individual and clinical contextual factors. First, we evaluated whether sense of coherence (SOC) modifies the strength of adversity–symptom relationships. Subsequently, we explored whether medication use and selected clinical variables act as additional moderators of these associations.
3.6.1. Moderation by Sense of Coherence (SOC)
To determine whether SOC also modified (moderated) the strength of adversity–symptom associations, we estimated models including adversity × SOC_new_composite_z interaction terms. For symptoms of cognitive dysfunction and non-restorative sleep, none of the adversity × SOC interactions reached conventional statistical significance, indicating that SOC influences these domains primarily as a mediating pathway rather than as a moderator of adversity effects.
In contrast, SOC significantly moderates the impact of adversity on fatigue. Positive interaction coefficients were observed for loss (β = 0.052, p = .009), verbal aggression (β = 0.060, p = .004), emotional aggression (β = 0.057, p = .005), sexual abuse (β = 0.057, p = .027), two abuses; β = 0.024, p = .001), and three or more abuses (β = 0.026, p = .028). These positive interaction terms indicate that the association between adversity and fatigue varies across SOC levels. Individuals with lower SOC exhibited stronger adversity–fatigue associations, whereas individuals with higher SOC showed attenuated associations. In the context of the strong negative main effect of SOC on fatigue, this pattern reflects a dual role for SOC, functioning both as a mediator and as a buffer of adversity-related fatigue.
A similar moderating pattern emerged for fibromyalgia impact. SOC significantly modified the associations between FIQ and verbal aggression (β = 1.58, p = .002), emotional aggression (β = 1.44, p = .004), sexual abuse (β = 2.11, p = .001), two abuses (β = 0.75, p < .001), and three or more abuses (β = 0.57, p = .039). As with fatigue, positive interaction terms, combined with the strong protective main effects of SOC on FIQ, indicate that SOC shapes the degree to which adversity is expressed in global fibromyalgia impact. Higher SOC diminishes the translation of adversity into disability and symptom burden, demonstrating that SOC functions not only as a pathway (mediator) but also as a contextual factor (moderator) that alters the magnitude of adversity-related clinical severity. Together, Figure 3 demonstrates that SOC not only mediates but also moderates the clinical expression of adversity, particularly for fatigue and global impact, highlighting SOC as a multidimensional regulatory factor in fibromyalgia.
Title: SOC as a Moderator of the Association between Adversity Exposure and Clinical Outcomes
Overall, the moderation models shown in Table 5 reveal a clear and domain-specific pattern: SOC did not moderate the relationship between adversity and cognitive symptoms or non-restorative sleep but consistently modified the effects of adversity on fatigue and global fibromyalgia impact (FIQ). The significant positive interaction terms for multiple adversity indicators in these two domains indicate that individuals with lower SOC exhibit steeper adversity–symptom slopes, whereas those with higher SOC show attenuated associations. This pattern confirms that SOC functions as a clinically meaningful buffer specifically for fatigue and global impact, but not for cognitive or sleep-related symptoms.
3.6.2. Medication Use and Clinical Factors as Moderators
Regression models with interaction terms for adversity × medication were estimated for cognitive symptoms, FIQ, and non-restorative sleep. Medications included antidepressants (tricyclics, dual-action agents, combined tricyclic plus dual agents, and SSRIs), benzodiazepines, sleep agents (melatonin and zolpidem), non-opioid analgesics, and opioids (codeine, morphine, oxycodone, methadone, and tramadol).
3.7. Comorbidities and Medication Use as Moderators and Mediators of Adversity–Outcome Associations
Moderation effects were most evident for cognitive symptoms. Dual-action antidepressants amplified the association between persistent physical aggression and cognitive dysfunction (β = 0.21, p = .002), with a smaller effect for combined dual-plus-tricyclic therapy (β = 0.12, p = .023). Two types of abuse also interacted positively with dual-action antidepressants (β = 0.05, p = .034). No consistent medication-moderation effects emerged for non-restorative sleep. Zolpidem showed a potential buffering effect on global fibromyalgia impact, with a negative interaction with persistent physical aggression (β = −4.55, p = .041).
Overall, dual-action antidepressants amplified adversity–cognition associations, whereas zolpidem attenuated adversity–FIQ effects; both patterns remain exploratory and require replication.
Table 6A summarizes the moderation and mediation analyses examining whether clinical comorbidities and medication use modify or partially explain the associations between adverse experiences and symptom severity. Moderation models assessed interaction effects involving scheduled consultations, stroke, and several medication classes—including antidepressants, benzodiazepines, sleep agents, non-opioid analgesics, and opioids—across cognitive dysfunction, fatigue, non-restorative sleep, and global fibromyalgia impact (FIQ). Significant interactions were observed for specific medication classes and clinical factors, indicating that these variables can alter the strength or direction of adversity–symptom relationships.
Table 6B Mediation analyses further evaluated whether hypertension, diabetes, and related comorbidities served as intermediary pathways linking adversity to clinical outcomes. While small but statistically significant indirect effects were detected, their magnitude was modest compared to psychosocial mechanisms, reinforcing the limited explanatory contribution of comorbidities and medication use to the adversity–symptom pathways.
4. Discussion
4.1. Main Findings
This study examined associations among cumulative adversity, sense of coherence (SOC), and clinical severity in individuals with fibromyalgia within a cross-sectional observational framework. Greater exposure to adverse experiences was consistently associated with higher symptom burden across multiple domains, including fibromyalgia impact (FIQ), fatigue, cognitive symptoms, and non-restorative sleep. Lower SOC was associated with worse outcomes, and SOC statistically accounted for a substantial proportion of the observed adversity–symptom associations. In addition, SOC modified the strength of adversity-related effects for selected outcomes, particularly fatigue and global disease impact. All findings should be interpreted as associations, not as evidence of causal directionality or biological mechanisms.
4.2. Construct Validity of the SOC Surrogate
SOC was conceptualized according to Antonovsky’s salutogenic framework (Antonovsky, 1987[21]) and operationalized using a theory-driven composite integrating emotional appraisal, coping resources, engagement with care, and cognitive interpretation of bodily symptoms. Indicators included depressive symptoms, pain catastrophizing, fatigue, central sensitization, kinesiophobia, psychiatric comorbidity burden, functional status, physical activity, and treatment engagement. Because several of these indicators are intrinsically related to symptom experience in fibromyalgia, potential overlap with outcome measures represents an important concern. However, correlation analyses showed only moderate associations between SOC domains and clinical outcomes, suggesting that the constructs are not redundant. In addition, exploratory latent structure analyses supported separable latent dimensions for SOC and symptom severity. These findings are consistent with prior work showing that resilience-related constructs capture broader psychosocial vulnerability beyond symptom intensity alone [27,39]. Nevertheless, SOC in this study cannot be interpreted as an entirely independent psychological trait, as it incorporates dimensions closely linked to emotional distress and functional impairment. Rather, it reflects an integrated psychosocial profile related to how individuals interpret, cope with, and manage chronic illness.
4.3. SOC as a Psychosocial Pathway Linking Adversity and Symptoms
Mediation analyses indicated that SOC statistically accounted for a substantial proportion of the association between cumulative adversity and symptom severity, particularly for fatigue and cognitive dysfunction. This finding reflects statistical decomposition of cross-sectional associations and does not imply that SOC constitutes a biological or temporal causal pathway. Rather, SOC likely represents an integrated psychosocial vulnerability profile encompassing emotional distress, coping resources, functional engagement, and illness appraisal. In the clinical context of fibromyalgia—a prototypical nociplastic pain condition—this profile may reflect heightened vulnerability to symptom amplification, consistent with current conceptualizations of stress-related dysregulation and nociplastic pain mechanisms documented in the literature [40,41]. Therefore, any reference to nociplastic mechanisms should be interpreted as conceptual plausibility rather than empirical confirmation. Reverse and bidirectional relationships remain plausible, whereby persistent symptoms and disability may further erode perceived coherence and coping capacity, reinforcing maladaptive cycles. Longitudinal designs are required to disentangle directionality.
Although quantitative sensory testing was not performed in the present study, and indicators related to central sensitization, movement-related fear, and rumination do not provide direct evidence of altered nociceptive processing, these measures reflect dimensions commonly associated with nociplastic pain mechanisms in fibromyalgia and related conditions [41,42]. In this context, SOC may represent an integrated psychosocial manifestation of vulnerability to central pain amplification in fibromyalgia, rather than a purely psychological disposition. However, reverse and bidirectional relationships remain plausible, as persistent symptoms and disability may further erode perceived coherence and coping capacity, reinforcing maladaptive cycles. Therefore, longitudinal studies are required to clarify temporal sequencing and causal pathways.
Beyond psychological appraisal, SOC may also reflect downstream biological embedding of chronic stress. Recent evidence highlights associations among fibromyalgia and other nociplastic pain conditions, autonomic dysfunction, HPA axis dysregulation, and low-grade systemic inflammation, as well as complex alterations in neural network connectivity and stress-processing systems [40]. Although biological markers were not assessed in the present study, the strong mediation effects observed suggest that SOC may capture an integrated vulnerability phenotype linking adversity exposure to altered pain processing and multisystem symptom expression in individuals with fibromyalgia. This interpretation is consistent with broader biopsychosocial and allostatic load frameworks of chronic pain, in which cumulative stress leads to progressive dysregulation of physiological regulatory capacity and amplification of persistent symptoms. Our findings support sense of coherence as an integrative construct linking psychological, behavioral, and contextual resources to symptom burden in fibromyalgia. Lower SOC may reflect reduced ability to interpret bodily sensations as predictable, diminished confidence in available coping resources, and increased affective vulnerability, which together may amplify nociplastic pain mechanisms and functional impairment. This framework helps explain why cumulative adversity translates into greater clinical impact across multiple symptom domains.
4.4. SOC as a Modifier of Vulnerability
Moderation analyses indicated that sense of coherence (SOC) attenuated the associations between cumulative adversity and selected symptom domains, suggesting a buffering effect consistent with contemporary resilience and self-regulation frameworks [43]. This statistical interaction suggests differential vulnerability rather than direct physiological buffering mechanisms. In current stress–pain models, psychosocial resources such as perceived control, coping flexibility, and self-efficacy modulate how stressors are translated into symptom burden, influencing both behavioral responses and physiological stress reactivity [44]. The absence of uniform moderation across all outcomes likely reflects the heterogeneity of fibromyalgia mechanisms, with psychological and behavioral processes exerting stronger influence on some symptom clusters than on others. This buffering effect also highlights the patient's active role in symptom regulation. Higher SOC may facilitate engagement in adaptive behaviors, adherence to therapeutic recommendations, pacing strategies, and sustained participation in physical and social activities, all of which are central targets in contemporary multimodal management of fibromyalgia [45]. In this sense, SOC may operate not only as a cognitive appraisal construct but also as a functional driver of self-management capacity, mediating how patients interact with symptoms, health services, and rehabilitation strategies.
The domain-specific nature of the moderation effects observed suggests that SOC may differentially influence symptom clusters through distinct behavioral and neurophysiological pathways. Fatigue and global functional impairment are strongly shaped by motivational processes, behavioral activation, activity avoidance, and coping strategies—domains closely linked to the manageability and meaningfulness components of SOC [43,45]. In contrast, cognitive dysfunction and sleep disturbances may be more directly associated with neurobiological dysregulation, circadian rhythm disruption, and altered arousal and salience networks, which may be less responsive to psychosocial buffering alone [40,46]. This differential pattern reinforces the view that fibromyalgia is not a unitary symptom construct, but rather a constellation of partially overlapping pathophysiological processes with variable susceptibility to psychosocial modulation. Such heterogeneity supports stratified and mechanism-informed treatment approaches, in which psychosocial interventions may preferentially benefit functional and fatigue-related domains, while cognitive and sleep symptoms may require complementary neurobiological and chronobiological strategies [40,47].
4.5. Interpretation Relative to Biomedical Comorbidities
Clinical comorbidities and medication classes showed modest moderation and mediation effects compared with SOC. This is expected, as SOC incorporates psychological distress, functional capacity, and health behavior engagement, which are directly linked to nociplastic pain expression. These findings should not be interpreted as minimizing biomedical contributions, but rather as highlighting that psychosocial processes are tightly interwoven with clinical manifestations of fibromyalgia [48,49]. Although hypertension, diabetes, stroke, and healthcare utilization showed statistically detectable effects in moderation and mediation models, their magnitude was consistently small compared with psychosocial pathways. This pattern suggests that while biomedical comorbidities contribute to clinical complexity, they explain only a limited proportion of symptom variability in high-impact fibromyalgia, particularly when central sensitization and psychosocial dysregulation are prominent. The amplification of adversity–cognition associations among users of dual-action antidepressants likely reflects confounding by indication, as patients with higher emotional distress and cognitive burden are more frequently prescribed these agents. This underscores the importance of interpreting medication-related moderation effects within the clinical context rather than as pharmacological mechanisms per se.
4.6. Clinical and Translational Implications
The present findings highlight the relevance of psychosocial dimensions—such as coping strategies, illness understanding, treatment engagement, and physical activity—in the clinical expression of fibromyalgia, in addition to pharmacological management. However, this study does not allow inference regarding treatment efficacy or prevention strategies. Contemporary evidence indicates that fibromyalgia treatment should be multimodal, personalized, and mechanism-informed, integrating psychosocial, physical, and pharmacological strategies according to dominant symptom domains and underlying pathophysiological processes [47]. In this framework, behavioral and educational interventions are particularly relevant for improving functional capacity and fatigue, whereas cognitive dysfunction and sleep disturbances may require complementary neurobiological and chronobiological approaches. Accordingly, multimodal programs including pain neuroscience education, graded exercise, behavioral activation, and shared decision-making may enhance manageability and comprehensibility, thereby reducing the clinical impact of adversity and facilitating sustained engagement in rehabilitation [45,46]. SOC-related constructs may also help identify patient subgroups with heightened vulnerability to persistent symptoms, supporting stratified and personalized treatment strategies.
From a translational perspective, these findings support incorporating resilience-oriented constructs into both clinical assessment and intervention design. Screening for SOC-related dimensions—such as illness understanding, perceived controllability, and engagement with care—may help identify patients at higher risk for persistent disability and suboptimal response to pharmacological strategies alone. Interventions explicitly targeting coherence-building processes, including structured pain neuroscience education, acceptance-based therapies, narrative approaches, and goal-oriented rehabilitation programs, may strengthen adaptive coping and enhance treatment responsiveness [43,44]. Importantly, these approaches may be particularly relevant for patients with high trauma burden, in whom purely biomedical interventions are unlikely to adequately address the multifactorial drivers of symptom persistence.
4.7. Limitations
Several limitations must be considered when interpreting these findings. First, the cross-sectional design precludes temporal and causal inference, and bidirectional relationships between adversity, SOC, and symptom severity are likely [50]. .Second, trauma exposure and psychosocial indicators were assessed retrospectively by self-report, which may be influenced by recall bias and current emotional state [51]. Third, SOC was operationalized using a theory-driven surrogate derived from secondary indicators rather than a validated SOC questionnaire, which may not fully capture all theoretical dimensions of the construct and may overrepresent emotion–related components, potentially inflating associations with symptom-based outcomes. Although discriminant validity analyses supported partial construct separation, SOC in this study should be interpreted as an integrated psychosocial vulnerability profile rather than an independent psychological trait [24,52]. Fourth, the cumulative adversity index did not assess severity, timing, or duration of exposure, limiting developmental inferences and preventing evaluation of sensitive periods [53]. Fifth, recruitment through online platforms and patient advocacy networks may have introduced selection bias toward individuals with higher symptom burden and healthcare engagement [54]. Finally, the sample consisted exclusively of women with high-impact fibromyalgia and substantial psychiatric comorbidity, which limits generalizability but reflects the clinical population most affected by persistent disability.
An additional conceptual limitation concerns the potential circularity inherent to psychosocial mediation models in chronic symptom conditions, as mediator constructs may partially overlap with emotional distress and functional impairment. Although internal validation procedures were applied, future longitudinal studies using independent SOC instruments and biological stress markers are required to confirm the temporal and mechanistic ordering proposed.
4.8. Conclusions
In this cohort of individuals with fibromyalgia, cumulative adversity was consistently associated with greater symptom burden, and lower sense of coherence was associated with worse clinical outcomes across multiple domains. SOC functioned both as an intermediate psychosocial pathway linking adversity to symptom severity and, for selected outcomes, as a modifier of vulnerability to adversity-related symptom amplification. These findings support the relevance of integrated biopsychosocial frameworks and highlight the importance of psychosocial resilience-related processes in the clinical expression of fibromyalgia.
Authors Contributions
Prof. Caumo and Prof Fregni had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Concept and design: Caumo, Fregni; Acquisition of data: Bueno, Bueno, Mayer De Freitas, Lopes, Coelho, Gomes Venturini, Louzada, Peres, Moreira, Drafting of the manuscript: Caumo, Torres, Fregni. Critical review of the manuscript for important intellectual content: Caumo, Fregni. Statistical analysis: Caumo, Fregni.. Obtained funding: Caumo. Supervision: Caumo. All authors have read and agreed to the published version of the manuscript.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Figure S1— Construction and Validation of the SOC Composite. Table S1. Variables included in the construction of SOC domains. Table S2. Correlations between SOC domains and core clinical outcomes (FIQ, fatigue, non-restorative sleep, and cognitive symptoms) (n=2099). Table S3. Associations between Adversity Indicators and Symptom Outcomes (n=2099).
Funding
The Committee for the Development of Higher Education Personnel (CAPES) (Grant #2022-2023) founded GB Master Scholarships. National Council for Scientific and Technological Development (CNPq) for research grants (WC: PQ no. 306606/2021-6; CB scientific initiation grant). Caumo funded by Foundation for the Support of Research at Rio Grande do Sul (FAPERGS) Ministry of Science and Technology. National Council for Scientific and Technological Development—(CNPq)/Health Secretary of State of Rio Grande do Sul, Brazil (SEARS), 08/2020 (PPSUS) (no. 21/2551-0000129-1). The project was funded by the Postgraduate Research Group at the Hospital de Clínicas de Porto Alegre—FIPE HCPA (support project no. 2023-0210). National Council for Scientific and Technological Development—(CNPq)/Chamada CNPq/MCTI Nº 10/2023 – UNIVERSAL Processo no403813/2023-9. Role of the Funder/Sponsor: The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Institutional Review Board Statement
The study was conducted in accordance with the ethical principles of the Declaration of Helsinki and was approved by the Research Ethics Committee of Hospital de Clínicas de Porto Alegre, Brazil (IRB #2023-0210). The recruitment period ran from August 1, 2023, to November 30, 2023.
Informed Consent Statement
All participants provided written informed consent prior to participation through a signed informed consent form (ICF).
Data Availability Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request. All data are fully de-identified to protect participant confidentiality. Requests for data access can be directed to: wcaumo@hcpa.edu.br.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
ACR — American College of Rheumatology
AUDIT-C — Alcohol Use Disorders Identification Test – Consumption
BMI — Body Mass Index
COPD — Chronic Obstructive Pulmonary Disease
CSI — Central Sensitization Inventory
FIQ — Fibromyalgia Impact Questionnaire
FM — Fibromyalgia
FS — Fibromyalgia Severity (WPI + SSS)
HCPA — Hospital de Clínicas de Porto Alegre
ICF — Informed Consent Form
IRB — Institutional Review Board
NPS — Numeric Pain Scale
NSAIDs — Non-Steroidal Anti-Inflammatory Drugs
PCS — Pain Catastrophizing Scale
PHQ-9 — Patient Health Questionnaire-9
PTSD — Post-Traumatic Stress Disorder
REDCap — Research Electronic Data Capture
SOC — Sense of Coherence
SSRI — Selective Serotonin Reuptake Inhibitor
SSS — Symptom Severity Scale
STROBE — Strengthening the Reporting of Observational Studies in Epidemiology
TSK — Tampa Scale for Kinesiophobia
UFRGS — Universidade Federal do Rio Grande do Sul
WPI — Widespread Pain Index
References
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Häuser, W.; Katz, R.L.; Mease, P.J.; Russell, A.S.; Russell, I.J.; Walitt, B. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin. Arthritis. Rheum. 2016, 46, 319–329. [Google Scholar] [CrossRef]
- Weir, P.T.; Harlan, G.A.; Nkoy, F.L.; Jones, S.S.; Hegmann, K.T.; Gren, L.H.; Lyon, J.L. The Incidence of Fibromyalgia and Its Associated Comorbidities. Am. J. Clin. Oncol. 2006, 12, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Solmaz, D.; Eder, L.; Aydin, S.Z. Update on the epidemiology, risk factors, and disease outcomes of psoriatic arthritis. Best Pr. Res. Clin. Rheumatol. 2018, 32, 295–311. [Google Scholar] [CrossRef] [PubMed]
- Assumpção, A.; Cavalcante, A.B.; Capela, C.E.; Sauer, J.F.; Chalot, S.D.; Pereira, C.A.B.; et al. Prevalência de fibromialgia na população urbana de São Paulo. Rev Bras Reumatol. 2009, 49, 369–374. [Google Scholar]
- Amris, K.; Ibsen, R.; Duhn, P.H.; Olsen, J.; Lolk, K.; Kjellberg, J.; Kristensen, L.E. Health inequities and societal costs for patients with fibromyalgia and their spouses: a Danish cohort study. RMD Open 2024, 10, e003904. [Google Scholar] [CrossRef] [PubMed]
- Halasz, G.; Piepoli, M.F. Editor comment: Focus on pharmacology and pharmacotherapy. Eur. J. Prev. Cardiol. 2022, 29, 1299–1300. [Google Scholar] [CrossRef]
- Mengshoel, A.M.; Skarbø, Å.; Hasselknippe, E.; Petterson, T.; Brandsar, N.L.; Askmann, E.; Ildstad, R.; Løseth, L.; Sallinen, M.H. Enabling personal recovery from fibromyalgia – theoretical rationale, content and meaning of a person-centred, recovery-oriented programme. BMC Heal. Serv. Res. 2021, 21, 339. [Google Scholar] [CrossRef]
- Mayer, S.; Spickschen, J.; Stein, K.V.; Crevenna, R.; E Dorner, T.; Simon, J. The societal costs of chronic pain and its determinants: The case of Austria. PLOS ONE 2019, 14, e0213889. [Google Scholar] [CrossRef]
- Häuser, W.; Fitzcharles, M.-A. Facts and myths pertaining to fibromyalgia. Dialog- Clin. Neurosci. 2018, 20, 53–62. [Google Scholar] [CrossRef]
- Ilzarbe, L.; Fàbrega, M.; Quintero, R.; Bastidas, A.; Pintor, L.; García-Campayo, J.; Gomollón, F.; Ilzarbe, D. Inflammatory Bowel Disease and Eating Disorders: A systematized review of comorbidity. J. Psychosom. Res. 2017, 102, 47–53. [Google Scholar] [CrossRef]
- Engel, G.L. The Need for a New Medical Model: A Challenge for Biomedicine. Science 1977, 196, 129–136. [Google Scholar] [CrossRef]
- Macfarlane, G.J.; Norrie, G.; Atherton, K.; Power, C.; Jones, G.T. The influence of socioeconomic status on the reporting of regional and widespread musculoskeletal pain: results from the 1958 British Birth Cohort Study. Ann. Rheum. Dis. 2009, 68, 1591–1595. [Google Scholar] [CrossRef]
- Kapos, F.P.; Craig, K.D.; Anderson, S.R.; Bernardes, S.F.; Hirsh, A.T.; Karos, K.; Keogh, E.; Losin, E.A.R.; McParland, J.L.; Moore, D.J.; et al. Social Determinants and Consequences of Pain: Toward Multilevel, Intersectional, and Life Course Perspectives. J. Pain 2024, 25, 104608. [Google Scholar] [CrossRef] [PubMed]
- Grol-Prokopczyk, H.; Huang, R.; Yu, C.; Chen, Y.-A.; Kaur, S.; Limani, M.; Lin, T.-H.; Zajacova, A.; Zimmer, Z.; Cowan, P.; et al. Over 50 years of research on social disparities in pain and pain treatment: a scoping review of reviews. Pain 2025, 166, 2458–2472. [Google Scholar] [CrossRef] [PubMed]
- McEwen, BS; Stellar, E. Stress and disease mechanisms. Arch Intern Med. 1993, 153, 2093–101. [Google Scholar] [CrossRef] [PubMed]
- McEwen, B.S. Stress, Adaptation, and Disease: Allostasis and Allostatic Load. Ann. N. Y. Acad. Sci. 1998, 840, 33–44. [Google Scholar] [CrossRef]
- Peters, A.; McEwen, B.S. Editorial introduction. Physiol. Behav. 2012, 106, 1–4. [Google Scholar] [CrossRef]
- Vlaeyen, J.W.; Crombez, G.; Linton, S.J. The fear-avoidance model of pain. Pain 2016, 157, 1588–1589. [Google Scholar] [CrossRef]
- Nadler, J.W.; Nawrot, M.; Angelaki, D.E.; DeAngelis, G.C. MT Neurons Combine Visual Motion with a Smooth Eye Movement Signal to Code Depth-Sign from Motion Parallax. Neuron 2009, 63, 523–532. [Google Scholar] [CrossRef]
- Häuser, W.; Kosseva, M.; Üceyler, N.; Klose, P.; Sommer, C. Emotional, physical, and sexual abuse in fibromyalgia syndrome: A systematic review with meta-analysis. Arthritis Care Res. 2011, 63, 808–820. [Google Scholar] [CrossRef]
- Legge, A.; Kirkland, S.; Rockwood, K.; Andreou, P.; Bae, S.; Gordon, C.; Romero-Diaz, J.; Sanchez-Guerrero, J.; Wallace, D.J.; Bernatsky, S.; et al. Prediction of Hospitalizations in Systemic Lupus Erythematosus Using the Systemic Lupus International Collaborating Clinics Frailty Index. Arthritis Care Res. 2021, 74, 638–647. [Google Scholar] [CrossRef]
- Antonovsky, A. Unraveling the Mystery of Health: How People Manage Stress and Stay Well; Jossey-Bass: San Francisco, CA, USA, 1987. [Google Scholar]
- Super, S.; Wagemakers, M.A.E.; Picavet, H.S.J.; Verkooijen, K.T.; Koelen, M.A. Strengthening sense of coherence: opportunities for theory building in health promotion: Fig. 1. Heal. Promot. Int. 2016, 31, 869–878. [Google Scholar] [CrossRef] [PubMed]
- Aguilar-Latorre, A.; Asensio-Martínez, Á.; Oliván-Blázquez, B.; Álvarez-Bueno, C.; Cavero-Redondo, I.; Lionis, C.; Symvoulakis, E.K.; Magallón-Botaya, R. Association between sense of coherence and depression in patients with chronic pain: A systematic review and meta-analysis. PLOS ONE 2023, 18, e0279959. [Google Scholar] [CrossRef] [PubMed]
- Schnyder, U.; Büchi, S.; Sensky, T.; Klaghofer, R. Antonovsky’s Sense of Coherence: Trait or State? Psychother. Psychosom. 2000, 69, 296–302. [Google Scholar] [CrossRef]
- Surtees, P.; Wainwright, N. SOC as predictor under adversity. Psychol Med. 2000, 30, 735–45. [Google Scholar]
- Eriksson, M.; Lindström, B. Antonovsky's sense of coherence scale and the relation with health: A systematic review. J. Epidemiol. Comm. Health 2006, 60, 376–381. [Google Scholar] [CrossRef]
- Carlén, K.; Suominen, S.; Lindmark, U.; Saarinen, M.M.; Aromaa, M.; Rautava, P.; Sillanpää, M. Sense of coherence predicts adolescent mental health. J. Affect. Disord. 2020, 274, 1206–1210. [Google Scholar] [CrossRef]
- Cohen-Biton, L.; Buskila, D.; Nissanholtz-Gannot, R. Resilience and Sense of Coherence among Female Fibromyalgia Patients Living in a Conflict Zone Who Underwent Fibrotherapy Intervention. Biomed 2024, 4, 78–88. [Google Scholar] [CrossRef]
- Kieraité, M.; Novoselac, A.; Bättig, J.J.; Rühlmann, C.; Bentz, D.; Noboa, V.; Seifritz, E.; Egger, S.T.; Weidt, S. Relationship between sense of coherence and depression, a network analysis. Curr. Psychol. 2024, 43, 23295–23303. [Google Scholar] [CrossRef]
- Häuser, W.; Walitt, B.; Fitzcharles, M.-A.; Sommer, C. Review of pharmacological therapies in fibromyalgia syndrome. Arthritis Res. Ther. 2014, 16, 201. [Google Scholar] [CrossRef]
- Goldenberg, D.L.; Clauw, D.J.; Palmer, R.E.; Clair, A.G. Opioid Use in Fibromyalgia: A Cautionary Tale. Mayo Clin. Proc. 2016, 91, 640–648. [Google Scholar] [CrossRef]
- Marques, A.P.; Santos, A.M.B.; Assumpção, A.; Matsutani, L.A.; Lage, L.V.; Pereira, C.A.B. Validação da versão brasileira do Fibromyalgia Impact Questionnaire (FIQ). Rev. Bras. de Reum. 2006, 46, 24–31. [Google Scholar] [CrossRef]
- Sehn, F.; Chachamovich, E.; Vidor, L.P.; Dall-Agnol, L.; de Souza, I.C.C.; Torres, I.L.S.; Fregni, F.; Caumo, W. Cross-Cultural Adaptation and Validation of the Brazilian Portuguese Version of the Pain Catastrophizing Scale. Pain Med. 2012, 13, 1425–1435. [Google Scholar] [CrossRef]
- Caumo, W.; Ruehlman, L.S.; Karoly, P.; Sehn, F.; Vidor, L.P.; Dall-Ágnol, L.; Chassot, M.; Torres, I.L.S. Cross-Cultural Adaptation and Validation of the Profile of Chronic Pain: Screen for a Brazilian Population. Pain Med. 2013, 14, 52–61. [Google Scholar] [CrossRef] [PubMed]
- Santos, I.S.; Tavares, B.F.; Munhoz, T.N.; de Almeida, L.S.P.; da Silva, N.T.B.; Tams, B.D.; Patella, A.M.; Matijasevich, A. Sensibilidade e especificidade do Patient Health Questionnaire-9 (PHQ-9) entre adultos da população geral. Cad. de Saude publica 2013, 29, 1533–1543. [Google Scholar] [CrossRef]
- Siqueira, F.B.; Teixeira-Salmela, L.F.; Magalhães, L.C. Tampa Scale for Kinesiophobia – Brazil. Acta Ortop Bras. 2007, 15, 19–24. [Google Scholar] [CrossRef]
- Corradi-Webster, C. M.; et al. Capacitação de Profissionais do Programa de Saúde da Família em Estratégias de Diagnóstico e Intervenções Breves para o Uso Problemático de Álcool. Revista smad, Ribeirão Preto. Disponível em:. Acesso em. 2005, v. 1.
- Iannuccelli, C.; Favretti, M.; Dolcini, G.; Di Carlo, M.; Pellegrino, G.; Bazzichi, L.; Atzeni, F.; Lucini, D.; Varassi, G.; Leoni, M.L.G.; et al. Fibromyalgia: one year in review 2025. Clin. Exp. Rheumatol. 2025, 43, 957–969. [Google Scholar] [CrossRef]
- Walsh, D.A.; Boeri, M.; Abraham, L.; Atkinson, J.; Bushmakin, A.G.; Cappelleri, J.C.; Hauber, B.; Klein, K.; Russo, L.; Viktrup, L.; et al. Exploring patient preference heterogeneity for pharmacological treatments for chronic pain: A latent class analysis. Eur. J. Pain 2022, 26, 648–667. [Google Scholar] [CrossRef] [PubMed]
- Giglio, M.; et al. The putative role of immune and inflammatory mechanisms in nociplastic pain activation and amplification. Explor Pain. 2025, 2, 15–28. [Google Scholar] [CrossRef]
- Goubert, L.; Trompetter, H. Towards a science and practice of resilience in the face of pain. Eur. J. Pain 2017, 21, 1301–1315. [Google Scholar] [CrossRef]
- Eccleston, C.; Crombez, G. Advancing psychological therapies for chronic pain. F1000Research 2017, 6, 461. [Google Scholar] [CrossRef]
- Martinez-Calderon, J.; Flores-Cortes, M.; Morales-Asencio, J.M.; Luque-Suarez, A. Intervention Therapies to Reduce Pain-Related Fear in Fibromyalgia Syndrome: A Systematic Review of Randomized Clinical Trials. Pain Med. 2020, 22, 481–498. [Google Scholar] [CrossRef]
- Nijs, J.; Malfliet, A.; Nishigami, T. Nociplastic pain and central sensitization in patients with chronic pain conditions: a terminology update for clinicians. Braz. J. Phys. Ther. 2023, 27, 100518. [Google Scholar] [CrossRef]
- Jurado-Priego, L.N.; Cueto-Ureña, C.; Ramírez-Expósito, M.J.; Martínez-Martos, J.M. Fibromyalgia: A Review of the Pathophysiological Mechanisms and Multidisciplinary Treatment Strategies. Biomedicines 2024, 12, 1543. [Google Scholar] [CrossRef] [PubMed]
- Clauw, D.J. Fibromyalgia and Related Conditions. Mayo Clin. Proc. 2015, 90, 680–692. [Google Scholar] [CrossRef] [PubMed]
- Häuser, W.; Ablin, J.; Fitzcharles, M.-A.; Littlejohn, G.; Luciano, J.V.; Usui, C.; Walitt, B. Fibromyalgia. Nat. Rev. Dis. Prim. 2015, 1, 15022. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Biopsychosocial model of fibromyalgia severity and the modulating role of sense of coherence (SOC). Adverse life events increase emotional, psychological, and physiological load, leading to greater symptom severity through allostatic dysregulation. SOC influences this process by mediating the impact of adversity and buffering its effects on functional impairment. Lower SOC is associated with higher symptom burden and greater vulnerability to the effects of cumulative stress, representing a key mechanism linking adverse experiences to fibromyalgia severity.
Figure 1.
Biopsychosocial model of fibromyalgia severity and the modulating role of sense of coherence (SOC). Adverse life events increase emotional, psychological, and physiological load, leading to greater symptom severity through allostatic dysregulation. SOC influences this process by mediating the impact of adversity and buffering its effects on functional impairment. Lower SOC is associated with higher symptom burden and greater vulnerability to the effects of cumulative stress, representing a key mechanism linking adverse experiences to fibromyalgia severity.
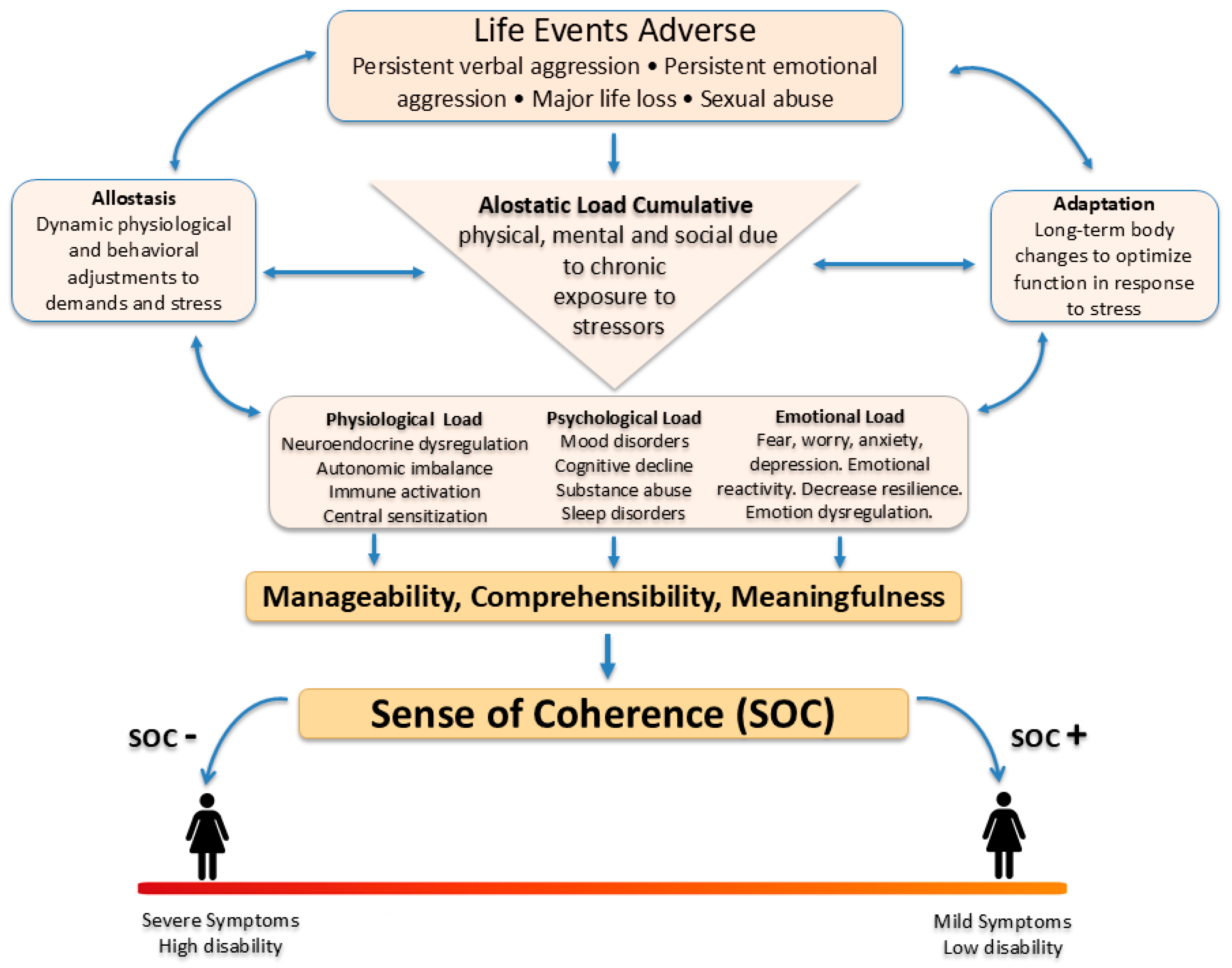
Figure 2.
Mediation models showing how the Sense of Coherence (SOC) transmits the effects of adversity to distinct fibromyalgia symptom domains. Panels (a–d) present parallel mediation structures across four clinical domains. In all models, higher adversity was associated with lower SOC (path a), and lower SOC was associated with worse outcomes (path b), resulting in positive indirect effects (a × b) that were larger than the remaining direct effects (c′). (a) Cognitive symptoms: All adversity indicators showed strong mediated effects. For persistent physical aggression, adversity predicted lower SOC (a = −0.98), and higher SOC predicted fewer cognitive symptoms (b = −0.23). The total effect was modest (c_total = 0.11), while the indirect effect (a × b = 0.22) was nearly twice as large. After including SOC, the direct effect was small and negative (c′ = −0.11). Comparable patterns were observed for loss, emotional and verbal aggression, sexual abuse, and cumulative abuse scores. (b) Fatigue: SOC strongly mediated the association between adversity and fatigue severity. For persistent physical aggression, adversity predicted lower SOC (a = −0.98), and higher SOC predicted lower fatigue (b = −0.28). The total effect was small (c_total = 0.09), whereas the indirect effect was larger (a × b = 0.28); the direct effect became negative after adjusting for SOC (c′ = −0.19). (c) Non-restorative sleep: Adversity indicators were negatively associated with SOC, and lower SOC was associated with more severe non-restorative sleep (negative a- and b-paths). The indirect effects were smaller than in cognitive symptoms and fatigue but remained consistent and statistically meaningful. (d) Global fibromyalgia impact (FIQ): For cumulative abuse, adversity predicted lower SOC (a = −0.25), and higher SOC predicted lower FIQ scores (b = −6.77). The indirect effect (a × b = 1.69) approximated the total effect (c_total = 1.64), and the direct effect was minimal and slightly negative (c′ = −0.05). This pattern was similar across all other adversity indicators.
Figure 2.
Mediation models showing how the Sense of Coherence (SOC) transmits the effects of adversity to distinct fibromyalgia symptom domains. Panels (a–d) present parallel mediation structures across four clinical domains. In all models, higher adversity was associated with lower SOC (path a), and lower SOC was associated with worse outcomes (path b), resulting in positive indirect effects (a × b) that were larger than the remaining direct effects (c′). (a) Cognitive symptoms: All adversity indicators showed strong mediated effects. For persistent physical aggression, adversity predicted lower SOC (a = −0.98), and higher SOC predicted fewer cognitive symptoms (b = −0.23). The total effect was modest (c_total = 0.11), while the indirect effect (a × b = 0.22) was nearly twice as large. After including SOC, the direct effect was small and negative (c′ = −0.11). Comparable patterns were observed for loss, emotional and verbal aggression, sexual abuse, and cumulative abuse scores. (b) Fatigue: SOC strongly mediated the association between adversity and fatigue severity. For persistent physical aggression, adversity predicted lower SOC (a = −0.98), and higher SOC predicted lower fatigue (b = −0.28). The total effect was small (c_total = 0.09), whereas the indirect effect was larger (a × b = 0.28); the direct effect became negative after adjusting for SOC (c′ = −0.19). (c) Non-restorative sleep: Adversity indicators were negatively associated with SOC, and lower SOC was associated with more severe non-restorative sleep (negative a- and b-paths). The indirect effects were smaller than in cognitive symptoms and fatigue but remained consistent and statistically meaningful. (d) Global fibromyalgia impact (FIQ): For cumulative abuse, adversity predicted lower SOC (a = −0.25), and higher SOC predicted lower FIQ scores (b = −6.77). The indirect effect (a × b = 1.69) approximated the total effect (c_total = 1.64), and the direct effect was minimal and slightly negative (c′ = −0.05). This pattern was similar across all other adversity indicators.
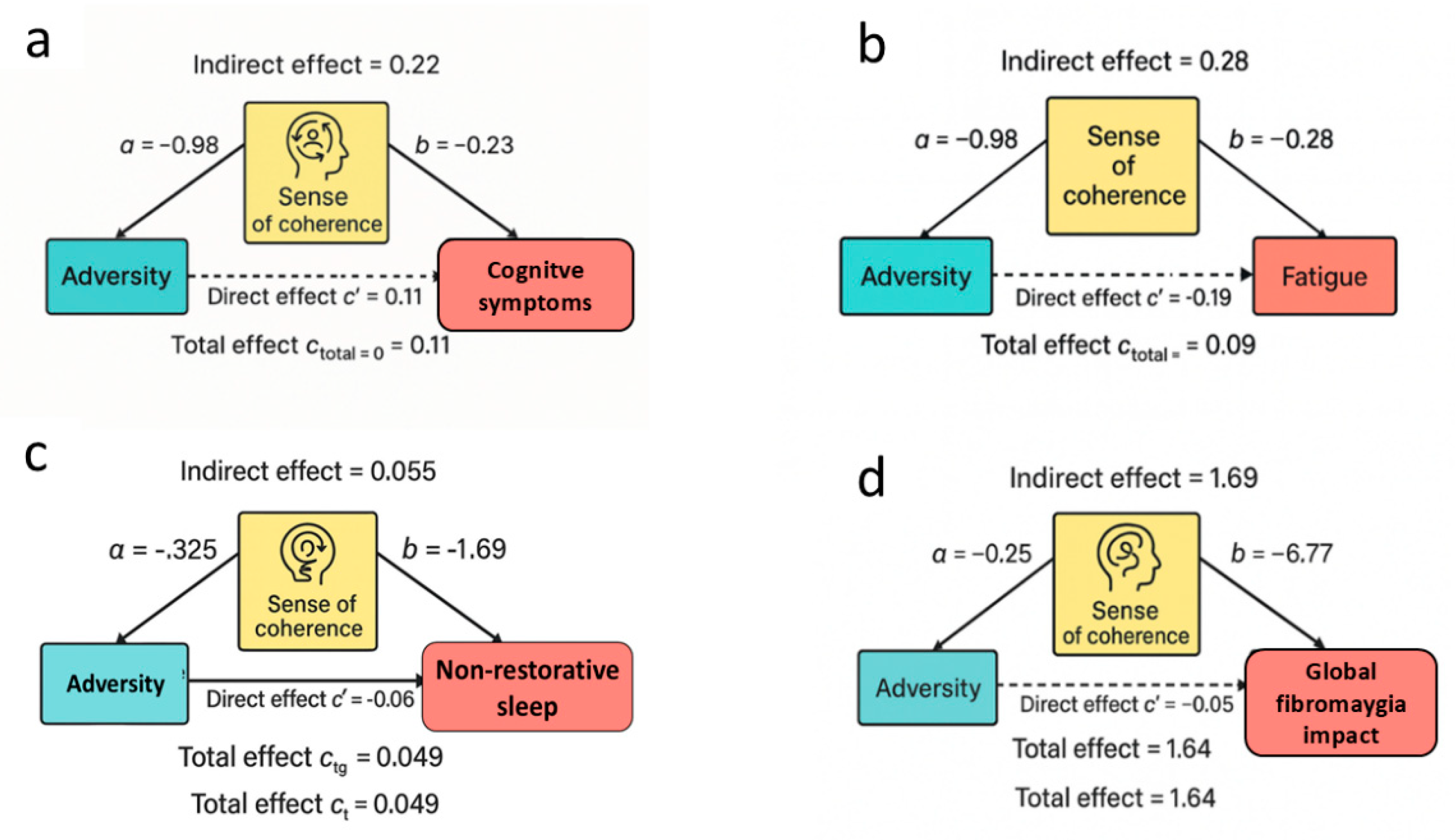
Figure 3.
The plots illustrate the moderating role of sense of coherence (SOC) on the association between cumulative adversity exposure and two key fibromyalgia outcomes: fatigue (left) and global fibromyalgia impact (FIQ; right). Predicted values are shown separately for individuals with low SOC (dashed yellow line) and high SOC (solid blue line), with 95% confidence bands. Steeper slopes in the low-SOC group indicate stronger adversity–symptom relationships, demonstrating that SOC attenuates the translation of adversity into clinical severity. In both panels, the x-axis represents cumulative adversity exposure, whereas the y-axes represent standardized symptom severity (z-scores). Negative z-scores in the fatigue panel reflect greater fatigue severity, while positive values in the FIQ panel indicate worse global impact. The opposite directions of the slopes reflect domain-specific effects of adversity across outcomes.
Figure 3.
The plots illustrate the moderating role of sense of coherence (SOC) on the association between cumulative adversity exposure and two key fibromyalgia outcomes: fatigue (left) and global fibromyalgia impact (FIQ; right). Predicted values are shown separately for individuals with low SOC (dashed yellow line) and high SOC (solid blue line), with 95% confidence bands. Steeper slopes in the low-SOC group indicate stronger adversity–symptom relationships, demonstrating that SOC attenuates the translation of adversity into clinical severity. In both panels, the x-axis represents cumulative adversity exposure, whereas the y-axes represent standardized symptom severity (z-scores). Negative z-scores in the fatigue panel reflect greater fatigue severity, while positive values in the FIQ panel indicate worse global impact. The opposite directions of the slopes reflect domain-specific effects of adversity across outcomes.
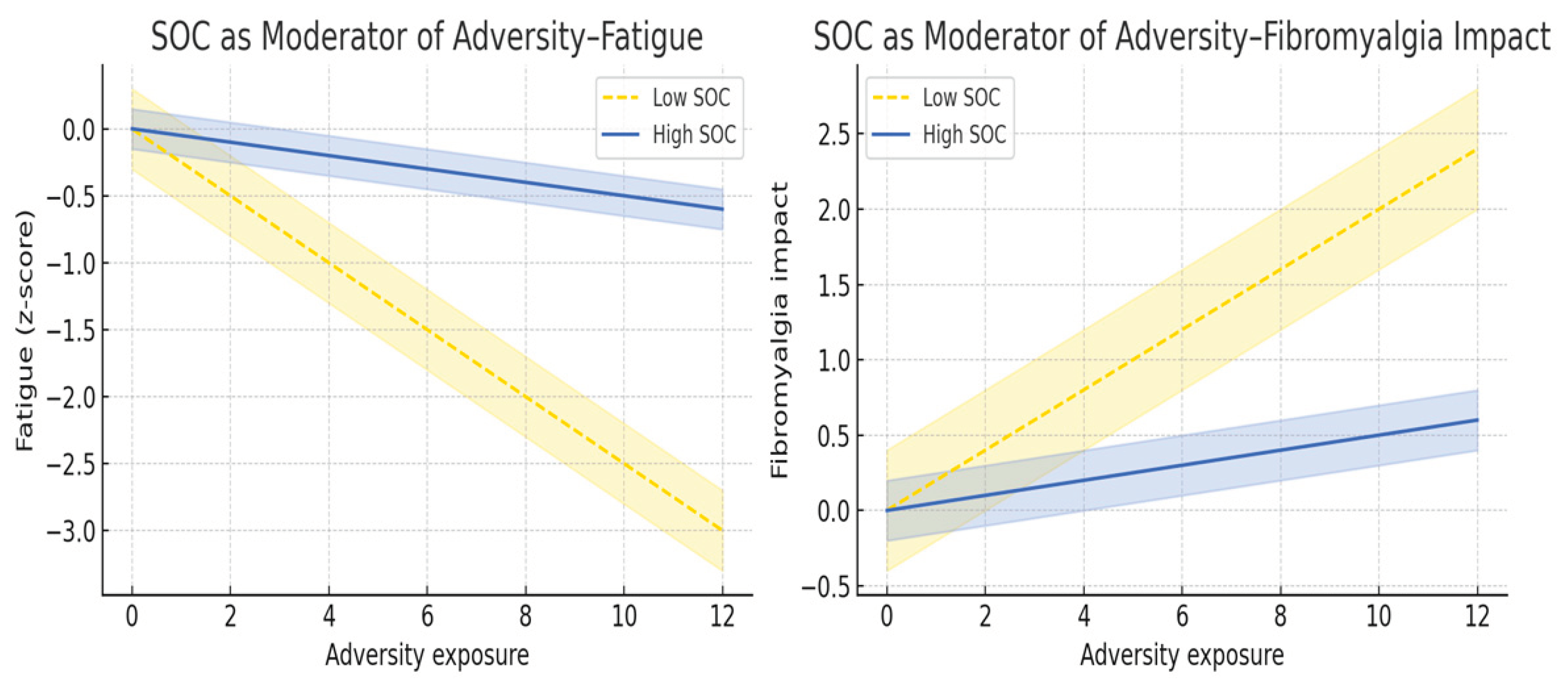

Table 1.
Sociodemographic, Clinical and Care-Engagement Characteristics according to cumulative abuse exposure (no abuse, one type of abuse, and two or more types of abuse). Data area presented as mean (SD), median (interquartile) or % (n = 2099).
Table 1.
Sociodemographic, Clinical and Care-Engagement Characteristics according to cumulative abuse exposure (no abuse, one type of abuse, and two or more types of abuse). Data area presented as mean (SD), median (interquartile) or % (n = 2099).
| Cumulative abuse exposure | |||||
| Variables | No history of abuse (n=1149) |
One type of abuse (n=354) | Two or more types of abuse (n=596) | P-value | |
| Demographic, Educational, and Occupational Characteristics | |||||
| Age (ys) | 50.94 (10.50) | 49.91 (9.66) | 50.69 (10.01) | 0.25 | |
| Formal education (ys) | 10.8 (4.2) | 9.6 (4.1) | 8.9 (3.80) | <0.001 | |
| Alcohol Use Disorders Identification Test Consume (AUDIT-C) | 1.38 (1.82) | 1.63 (2.10) | 1.64 (2.19) | 0.01 | |
| Race/Ethnicity (Black/Brown) (Yes) | 196 (52.4%) | 65 (17.4%) | 113 (30.2%) | 0.59 | |
| Occupational status category | |||||
| Unemployed (Yes) | 144 (12.5%) | 46 (13.0%) | 100 (16.8%) | 0.04 | |
| Employed / Student / Caregiver / Self-employed (Yes) | 630 (54.8%) | 195 (55.1%) | 306 (51.3%) | 0.33 | |
| Retired (Yes) | 212 (18.5%) | 57 (16.1%) | 93 (15.6%) | 0.22 | |
| Disability Benefits (Yes) | 163 (14.2%) | 56 (15.8%) | 97 (16.3%) | 0.47 | |
| Body Mass Index (BMI) | |||||
| Underweight (BMI < 18.5) | 6 (0.5%) | 3 (0.9%) | 6 (1.0%) | 0.50 | |
| Normal weight (BMI 18.5–24.9 kg/m²) | 252 (22.1%) | 72 (20.5%) | 123 (20.7%) | 0.71 | |
| Overweight (BMI 25.0–29.9 kg/m²) | 389 (34.1%) | 129 (36.6%) | 220 (37.0%) | 0.41 | |
| Obesity (BMI ≥ 30 kg/m²) | 494 (43.3%) | 148 (42.0%) | 245 (41.2%) | 0.70 | |
| Clinical chronic disease (Yes) | |||||
| Hypertension (HAS) | 762 (66.3%) | 213 (60.2%) | 416 (69.8%) | 0.01 | |
| Diabetes | 356 (31.0%) | 96 (27.1%) | 172 (28.9%) | 0.32 | |
| Stroke | 129 (11.2%) | 32 (9.0%) | 57 (9.6%) | 0.36 | |
| Asthma | 18 (1.6%) | 1 (0.3%) | 8 (1.3%) | 0.17 | |
| Chronic Obstructive Pulmonary Disease (COPD) | 237 (20.6%) | 63 (17.8%) | 141 (23.7%) | 0.09 | |
| Medication Profile: Psychotropic and Analgesic Agents | |||||
| Psychotropic_medication_use (Yes) | |||||
| Use of anticonvulsants | 602 (52.4%) | 191 (54.0%) | 361 (60.6%) | 0.00 | |
| Use of tricyclic/dual antidepressants | 568 (49.4%) | 201 (56.8%) | 280 (47.0%) | 0.01 | |
| Use of benzodiazepines | 146 (12.7%) | 47 (13.3%) | 138 (23.2%) | <0.001 | |
| Use of zolpidem | 92 (8.0%) | 27 (7.6%) | 61 (10.2%) | 0.22 | |
| Analgesic use (Yes) | |||||
| Non-opioid analgesics (≥2 types) | 831 (72.3%) | 268 (75.7%) | 460 (77.2%) | 0.07 | |
| Opioid use (any) | 552 (48.0%) | 191 (54.0%) | 320 (53.7%) | 0.03 | |
| Tramadol use | 413 (35.9%) | 149 (42.1%) | 250 (41.9%) | 0.01 | |
| Morphine use | 58 (5.0%) | 13 (3.7%) | 35 (5.9%) | 0.32 | |
| ≥1 pain-related medications | 260 (22.6%) | 82 (23.2%) | 169 (28.4%) | 0.02 | |
| Assessment of care received (Yes) | |||||
| Fibromyalgia specialist wait time – consultation schedule (ys) | |||||
| Less than one | 628 (54.7%) | 194 (54.8%) | 331 (55.5%) | 0.94 | |
| One to three | 250 (21.8%) | 86 (24.3%) | 123 (20.6%) | 0.41 | |
| Four to five | 66 (5.7%) | 17 (4.8%) | 37 (6.2%) | 0.66 | |
| More than five reference | 204 (17.8%) | 57 (16.1%) | 105 (17.6%) | 0.76 | |
| Global treatment quality assessment (0 to 10) | 4.99 (3. 91%) | 5.03 (3.11%) | 5.06 (3.41%) | 0.91 | |
| Treatment Engagement and Adherence | |||||
| Collaborative treatment decision-making | 892 (77.6%) | 285 (80.5%) | 472 (79.2%) | 0.46 | |
| Patient input on prescribed treatment | 882 (76.8%) | 276 (78.0%) | 470 (78.9%) | 0.59 | |
| Adherence to recommended treatment plan | 188 (16.4%) | 49 (13.8%) | 99 (16.6%) | 0.47 | |
| Self-initiated medication interruption | 221 (10.5%) | 45 (13.7%) | 82 (13.8%) | 0.11 | |
| Frequent medication forgetfulness | 134 (11.7%) | 46 (13.0%) | 88 (14.8%) | 0.18 | |
| Consistent medication uses as prescribed | 965 (84.0%) | 300 (84.7%) | 519 (87.1%) | 0.22 | |
| Exact adherence to prescribed dosage | 1028 (89.5%) | 309 (87.3%) | 514 (86.2%) | 0.11 | |
Groups reflect cumulative exposure profiles and are not statistically independent by construction.
Table 2.
Fibromyalgia Severity, Pain Impact, Psychological Measures, and Adversity Profiles according to cumulative abuse exposure (no abuse, one type of abuse, and two or more types of abuse). Data area presented as mean (SD), median (interquartile) or % (n=2099).
Table 2.
Fibromyalgia Severity, Pain Impact, Psychological Measures, and Adversity Profiles according to cumulative abuse exposure (no abuse, one type of abuse, and two or more types of abuse). Data area presented as mean (SD), median (interquartile) or % (n=2099).
| Cumulative abuse exposure | |||||
| Variable | No history of abuse (n=1149) |
One type of abuse (n=354) | Two or more types of abuse (n=596) |
P-value | |
| Fibromyalgia Symptom Severity and Diagnostic Criteria (ACR 2016) | |||||
| Widespread pain index (WPI) | 10.75 (3.26) | 10.55 (3.29) | 10.72 (3.37) | 0.60 | |
| Symptom Severity Score (SSS) | 9.66 (1.62) | 9.73 (1.60) | 10.06 (1.43) | <0.001 | |
| Fibromyalgia Severity (FS) - (WPI score plus SSS) | 20.40 (3.92) | 20.27 (3.91) | 20.77 (4.03) | 0.09 | |
| Pain conditions and impact on daily life | |||||
| Diagnosis of other pain conditions | |||||
| Musculoskeletal (Yes) | 565 (49.2%) | 161 (45.5%) | 322 (54.0%) | 0.029 | |
| Neuropathic Pain (Yes) | 237 (20.6%) | 59 (16.7%) | 166 (27.9%) | <0.001 | |
| Pain intensity – last 7 days (NPS 0-10) | 7.94 (1.57) | 7.83 (1.58) | 8.02 (1.54) | 0.19 | |
| Pain interfered with enjoyment of life (NPS 0-10) | 7.81 (2.30) | 7.74 (2.36) | 8.16 (2.13) | 0.00 | |
| Pain interfered with activities (NPS 0-10) | 7.93 (2.09) | 7.94 (1.94) | 8.15 (1.93) | 0.08 | |
| During the past three months, disability due to pain in daily activities? | |||||
| Some days | 396 (34.50%) | 124 (35.1%) | 177 (29.7%) | 0.17 | |
| Most days | 752 (65.4%) | 229 (64.9%) | 418 (70.3%) | 0.18 | |
| Psychological, Kinesiphobia and Central Sensitization Domains | |||||
| Tampa Scale for Kinesiophobia (TSK) | 45.47 (8.21) | 45.12 (8.20) | 47.54 (7.83) | <0.001 | |
| Central Sensitization Inventory (CSI) | 67.39 (11.91) | 68.06 (10.86) | 72.50 (10.99) | <0.001 | |
| Pain Catastrophizing Scale (PCS) | |||||
| PCS – Magnification | 8.10 (3.02) | 8.22 (2.79) | 8.95 (2.76) | <0.001 | |
| PCS – Helplessness | 16.07 (5.10) | 16.25 (4.78) | 17.62 (4.59) | <0.001 | |
| PCS – Rumination | 11.93 (3.19) | 12.16 (3.07) | 12.68 (2.91) | <0.001 | |
| PCS – Total score | 36.11 (10.56) | 36.63 (9.91) | 39.26 (9.57) | <0.001 | |
| History of psychiatric diagnosis (Yes) | 509 (44.3%) | 156 (44.1%) | 364 (61.1%) | <0.001 | |
| Major depression disorders | 415 (36.1%)) | 132 (37.3%) | 314 (52.7%) | <0.001 | |
| Anxiety disorder | 398 (34.6%) | 125 (35.3%) | 302 (50.7%) | <0.001 | |
| Bipolar disorder | 110 (9.6%) | 22 (6.2%) | 76 (12.8%) | 0.004 | |
| Panic disorder ( | 110 (9.6%) | 23 (6.5% | 99 (16.6%) | <0.001 | |
| Post-traumatic stress disorder (PTSD) | 53 (4.6%) | 15 (4.2% | 73 (12.2%) | <0.001 | |
| Non-depressive psychiatric comorbidity (cumulative count) mean (SD) | 0.94 (1.22%) | 0.89 (1.17%) | 1.45 (1.41%) | <0.001 | |
| Patient Health Questionnaire-9 (PHQ-9) - mean (SD) | 16.75 (6.14%) | 17.03 (5.92%) | 18.84 (5.78%) | <0.001 | |
| Life adverse events | |||||
| Persistent physical aggression (Yes) | 160 (13.9%) | 57 (16.1%) | 282 (47.3%) | <0.001 | |
| Persistent verbal aggression (Yes) | 131 (11.4%) | 4 (1.1%) | 596 (100.0%) | <0.001 | |
| Persistent emotional aggression (Yes) | 360 (31.3%) | 122 (34.5%) | 596 (100.0%) | <0.001 | |
| Sexual abuse (Yes) | 97 (8.4%) | 46 (13.0%) | 222 (37.2%) | <0.001 | |
| Fibromyalgia_onset_related_to_major_life_event (Yes) | 269 (23.4%) | 228 (64.4%) | 596 (100.0%) | <0.001 | |
| Duration of fibromyalgia (ys) | 15.15 (11.83) | 14.18 (11.49) | 15.86 (11.16) | 0.09 | |
| Age at onset of fibromyalgia (ys) | 34.56 (12.11) | 32.93 (11.37) | 31.76 (11.78) | <0.001 | |
| Age at onset of fibromyalgia categories (ys) | |||||
| Onset before 18 ys | 88 (7.9%) | 29 (8.5%) | 75 (13.4%) | 0.001 | |
| 19–25 ys | 164 (14.8%) | 71 (20.8%) | 101 (18.0%) | 0.021 | |
| 26–40 ys | 501 (45.2%) | 147 (43.1%) | 245 (43.7%) | 0.723 | |
| > 40 ys | 355 (32.0%) | 94 (27.6%) | 140 (25.0%) | 0.008 | |
| Physical activities performed regularly | 572 (49.8%) | 178 (50.3%) | 309 (51.8%) | 0.42 | |
Groups reflect cumulative exposure profiles and are not statistically independent by construction. Non-depressive psychiatric comorbidity (cumulative count): cumulative number of self-reported lifetime diagnoses of anxiety disorders, bipolar disorder, panic disorder, and post-traumatic stress disorder (PTSD).
Table 3.
Dose–response associations between cumulative abuse exposure and fibromyalgia-related symptom severity and functional impact. (n=2099).
Table 3.
Dose–response associations between cumulative abuse exposure and fibromyalgia-related symptom severity and functional impact. (n=2099).
| Fatigue symptoms | β | SE | p-value | |
| Cumulative abuse (range 0–4) | 0.02 | (0.01, 0.04) | 0.004 | Adjusted R² = 0.06 |
| Age (ys) | 0.00 | (-0.00, 0.00) | 0.131 | |
| Education level (ys) | 0.20 | 0.12 to 0.29 | <0.001 | |
| Disability due to pain in daily activities | 0.00 | -0.00 to 0.00 | 0.689 | |
| Body mass index (BMI) | 0.20 | 0.12 to 0.29 | <0.001 | |
| Cognitive dysfunction symptoms | Adjusted R²=0.04 | |||
| Cumulative abuse (range 0–4) | 0.05 | (0.03, 0.07) | 0.000 | |
| Age (ys) | -0.00 | (-0.01, -0.00) | 0.006 | |
| Education level (ys) | 0.20 | 0.09 to 0.32 | <0.001 | |
| Disability due to pain in daily activities | 0.00 | (-0.02, 0.02) | 0.998 | |
| Body mass index (BMI) | 0.01 | (-0.02, 0.05) | 0.521 | |
| Waking unrefreshed | Adjusted R²=0.03 | |||
| Cumulative abuse (range 0–4) | 0.03 | (0.01, 0.05) | 0.001 | |
| Age (ys) | -0.00 | (-0.00, 0.00) | 0.755 | |
| Education level (ys) | 0.17 | 0.08 to 0.26 | <0.001 | |
| Disability due to pain in daily activities | 0.01 | (-0.01, 0.02) | 0.530 | |
| Body mass index (BMI) | 0.03 | (0.00, 0.06) | 0.038 | |
| Fibromyalgia Impact Questionnaire (FIQ) | Adjusted R²=0.14 | |||
| Cumulative abuse (range 0–4) | 1.33 | (0.92, 1.74) | 0.000 | |
| Age (ys) | -0.07 | (-0.13, -0.02) | 0.011 | |
| Education level (ys) | 7.99 | 5.98 to 10.01 | <0.001 | |
| Disability due to pain in daily activities | 0.99 | (0.56, 1.41) | 0.000 | |
| Body mass index (BMI) | 1.67 | (0.98, 2.36) | 0.000 | |
1. β represents the change in outcome per one-unit increase in cumulative abuse (range 0–4). β represents the standardized regression coefficient; SE = standard error. Model R² indicates the proportion of variance in each symptom domain explained by adversity indicators after covariate adjustment.
Table 4.
Mediation analysis: Regression model for four clinical domains: symptoms of cognitive dysfunction, fatigue, non-restorative sleep, and global fibromyalgia impact (FIQ) (n-2076).
Table 4.
Mediation analysis: Regression model for four clinical domains: symptoms of cognitive dysfunction, fatigue, non-restorative sleep, and global fibromyalgia impact (FIQ) (n-2076).
| a_coef | b_coef | c_total | c_prime | indirect_ab | prop_mediated | |
| Symptoms of cognitive dysfunction | ||||||
| Major life loss (Yes) | -0.325 | -0.207 | 0.101 | 0.033 | 0.067 | 0.667 |
| Persistent physical aggression (Yes) | -0.976 | -0.229 | 0.113 | -0.110 | 0.223 | 1.969 |
| Persistent verbal aggression (Yes) | -0.493 | -0.205 | 0.137 | 0.036 | 0.101 | 0.739 |
| Persistent emotional aggression (Yes) | -0.425 | -0.207 | 0.107 | 0.019 | 0.088 | 0.820 |
| Sexual abuse (Yes) | -0.565 | -0.211 | 0.097 | -0.022 | 0.119 | 1.228 |
| Two types of abuse | -0.273 | -0.212 | 0.053 | -0.005 | 0.058 | 1.090 |
| Three or more types of abuse | -0.250 | -0.204 | 0.081 | 0.030 | 0.051 | 0.630 |
| Fatigue | ||||||
| Major life loss (Yes) | -0.325 | -0.255 | 0.034 | -0.049 | 0.083 | 2.418 |
| Persistent physical aggression (Yes) | -0.976 | -0.284 | 0.087 | -0.190 | 0.277 | 3.182 |
| Persistent verbal aggression (Yes) | -0.493 | -0.260 | 0.046 | -0.082 | 0.128 | 2.806 |
| Persistent emotional aggression (Yes) | -0.425 | -0.258 | 0.036 | -0.074 | 0.110 | 3.067 |
| Sexual abuse (Yes) | -0.565 | -0.259 | 0.044 | -0.103 | 0.146 | 3.343 |
| Two types of abuse | -0.273 | -0.275 | 0.024 | -0.051 | 0.075 | 3.163 |
| Three or more types of abuse | -0.250 | -0.258 | 0.024 | -0.041 | 0.064 | 2.692 |
| Non-restorative sleep | ||||||
| Major life loss (Yes) | -0.325 | -0.169 | 0.048 | -0.006 | 0.055 | 1.133 |
| Persistent physical aggression (Yes) | -0.976 | -0.179 | 0.116 | -0.059 | 0.174 | 1.506 |
| Persistent verbal aggression (Yes) | -0.493 | -0.170 | 0.065 | -0.019 | 0.084 | 1.291 |
| Persistent emotional aggression (Yes) | -0.425 | -0.174 | 0.018 | -0.056 | 0.074 | 4.049 |
| Sexual abuse (Yes) | -0.565 | -0.169 | 0.081 | -0.015 | 0.096 | 1.187 |
| Two types of abuse | -0.273 | -0.177 | 0.030 | -0.019 | 0.048 | 1.624 |
| Three or more types of abuse | -0.250 | -0.169 | 0.037 | -0.005 | 0.042 | 1.130 |
| Fibromyalgia Impact Questionnaire (FIQ) | ||||||
| Major life loss (Yes) | -0.325 | -6.802 | 1.709 | -0.503 | 2.212 | 1.294 |
| Persistent physical aggression (Yes) | -0.976 | -7.542 | 2.948 | -4.416 | 7.364 | 2.498 |
| Persistent verbal aggression (Yes) | -0.493 | -6.810 | 2.919 | -0.440 | 3.359 | 1.151 |
| Persistent emotional aggression (Yes) | -0.425 | -6.803 | 2.500 | -0.392 | 2.893 | 1.157 |
| Sexual abuse (Yes) | -0.565 | -6.823 | 3.090 | -0.768 | 3.859 | 1.249 |
| Two types of abuse | -0.273 | -7.060 | 1.297 | -0.629 | 1.926 | 1.485 |
| Three or more types of abuse | -0.250 | -6.770 | 1.642 | -0.050 | 1.691 | 1.030 |
a_coef – effect of abuse on the mediator (SOC); b_coef – effect of the mediator (SOC) on the outcome, controlling for abuse; c_total – total effect of abuse on the outcome; c_prime – direct effect of abuse on the outcome, controlling for SOC; indirect_ab – indirect (mediated) effect of abuse through SOC (a × b); Prop_mediated – proportion of the total effect mediated by SOC.
Table 5.
Moderation analysis: regression models for symptoms of cognitive dysfunction, fatigue, non-restorative sleep, and global fibromyalgia impact (FIQ) (n = 2,076).
Table 5.
Moderation analysis: regression models for symptoms of cognitive dysfunction, fatigue, non-restorative sleep, and global fibromyalgia impact (FIQ) (n = 2,076).
| Adversity indicator | Beta-interaction | P-value | |
| Outcome: symptoms of cognitive dysfunction | |||
| Major life loss (Yes) | 0.023 | 0.401 | |
| Persistent physical aggression (Yes) | 0.003 | 0.940 | |
| Persistent verbal aggression (Yes) | 0.040 | 0.167 | |
| Persistent emotional aggression (Yes) | 0.035 | 0.215 | |
| Sexual abuse (Yes) | 0.035 | 0.334 | |
| Two types of abuse | 0.017 | 0.099 | |
| Three or more types of abuse | 0.017 | 0.282 | |
| Outcome: Fatigue | |||
| Major life loss (Yes) | 0.052 | 0.009 | |
| Persistent physical aggression (Yes) | 0.039 | 0.139 | |
| Persistent verbal aggression (Yes) | 0.060 | 0.004 | |
| Persistent emotional aggression (Yes) | 0.057 | 0.005 | |
| Sexual abuse (Yes) | 0.057 | 0.027 | |
| Two types of abuse | 0.024 | 0.001 | |
| Three or more types of abuse | 0.024 | 0.028 | |
| Outcome: Non-restorative sleep | |||
| Major life loss (Yes) | 0.027 | 0.228 | |
| Persistent physical aggression (Yes) | 0.050 | 0.087 | |
| Persistent verbal aggression (Yes) | 0.031 | 0.179 | |
| Persistent emotional aggression (Yes) | 0.015 | 0.496 | |
| Sexual abuse (Yes) | 0.044 | 0.121 | |
| Two types of abuse | 0.012 | 0.133 | |
| Three or more types of abuse | 0.014 | 0.265 | |
| Outcome: Fibromyalgia Impact Questionnaire (FIQ) | |||
| Major life loss (Yes) | 0.804 | 0.100 | |
| Persistent physical aggression (Yes) | 1.154 | 0.072 | |
| Persistent verbal aggression (Yes) | 1.583 | 0.002 | |
| Persistent emotional aggression (Yes) | 1.437 | 0.004 | |
| Sexual abuse (Yes) | 2.106 | 0.001 | |
| Two types of abuse | 0.751 | 0.000 | |
| Three or more types of abuse | 0.569 | 0.039 | |
β-interaction represents the coefficient of the adversity × SOC interaction term in the regression model. Positive β-interaction values indicate that adversity–symptom associations are stronger among individuals with lower SOC and attenuated among those with higher SOC, consistent with a buffering (protective) moderating effect of SOC. Non-significant interaction coefficients indicate absence of moderation.
Table 6.
Interaction (Moderation) and Mediation Effects Linking Adversity to Clinical Outcomes (n=2076).
Table 6.
Interaction (Moderation) and Mediation Effects Linking Adversity to Clinical Outcomes (n=2076).
| A. Moderation Effects | ||||||||
| Outcomes variables – Clinical variable and interaction variables | β_interaction | p-value | ||||||
| Symptoms of cognitive dysfunction | ||||||||
| Scheduled consultation × Persistent physical aggression | -0.46 | .022 | ||||||
| Scheduled consultation × Persistent verbal aggression | -0.38 | .036 | ||||||
| Dual-action antidepressants × Persistent physical aggression | 0.21 | .002 | ||||||
| Antidepressant tricyclic antidepressants × Persistent physical aggression | 0.12 | .023 | ||||||
| Dual-action antidepressants × Other abuse types | 0.05 | .034 | ||||||
| Fatigue | ||||||||
| Scheduled consultation ×Emotional aggression | 0.36 | .004 | ||||||
| Stroke ×Sexual abuse | 0.19 | .034 | ||||||
| Fibromyalgia Impact Questionnaire (FIQ) | ||||||||
| Stroke ×Major life loss | 4.94 | .007 | ||||||
| Stroke ×. Sexual abuse | 5.15 | .023 | ||||||
| Zolpidem ×Persistent physical aggression | -4.55 | .041 | ||||||
| B. Mediation Effects | ||||||||
| Fatigue | ||||||||
| Mediator | Adversity | a-path | p(a) | b-path | p(b) | Indirect (ab) | ||
| Hypertension (HAS) | Physical aggression | 0.07 | .006 | 0.12 | <.001 | 0.01 | ||
| Hypertension (HAS) | Emotional aggression | 0.05 | .023 | 0.12 | <.001 | 0.006 | ||
| Hypertension (HAS) | Cumulative abuse | 0.02 | .009 | 0.12 | <.001 | 0.002 | ||
| Diabetes | Major life loss | -0.05 | .01 | 0.08 | <.001 | 0.004 | ||
| Non-restorative sleep | ||||||||
| Hypertension (HAS) | Cumulative abuse | -0.03 | 0.01 | 0.07 | <.01 | ≤0.01 | ||
| Outcome: Fibromyalgia Impact Questionnaire (FIQ) | ||||||||
| Hypertension (HAS) | Physical aggression | 0.07 | .006 | 4.03 | <.001 | 0.27 | ||
| Hypertension (HAS) | Emotional aggression | 0.05 | .023 | 3.98 | <.001 | 0.19 | ||
| Hypertension (HAS) | Cumulative abuse | 0.02 | .009 | 4.03 | <.001 | 0.08 | ||
| Diabetes | Major life loss | -0.05 | .01 | 1.47 | .017 | 0.07 | ||
Tabel 6A. β_interaction denotes the coefficient of the interaction term (Adversity × Moderator). Significant values indicate that the slope of the adversity–the moderator modifies outcome relationship.” Tabel 6B. a-path: effect of adversity on the mediator (adjusted for the predictor e.g., hypertension or diabetes); b-path: effect of the mediator on the clinical outcome (fatigue, non-restorative sleep, or FIQ), adjusted for adversity; p(a) and p(b): corresponding significance values.”.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



