Submitted:
24 January 2026
Posted:
26 January 2026
You are already at the latest version
Abstract
Toxoplasma gondii causes toxoplasmosis, a zoonosis of global importance, seriously affecting foetuses congenitally infected by their mother. Although early detection is important to prevent adverse fetal outcomes, maternal infections are frequently asymptomatic or present with mild, nonspecific signs. The present systematic review sought to synthesize evidence on early signs, risk factors, and diagnosis of toxoplasmosis in pregnant women. The study was conducted following the PRISMA 2020 guidelines. A literature search was conducted across PubMed, Scopus, ResearchGate, and Google Scholar for studies published between 2000 and 2025. The articles were exported to Zotero, citation management software. Duplicate articles were merged; those not published in English and lacking reference materials were excluded. After secondary screenings, 31 out of 407 articles met the inclusion criteria. Major maternal signs were lymphadenopathy (19.4%) and flu-like symptoms (19.4%), while major foetal effects were congenital anomalies (25.8%) and miscarriage (22.6%). Associated risk factors were contact with cat faeces and contaminated soil, consumption of undercooked or raw meat, raw vegetables, and contaminated water. Diagnosis was mainly by ELISA (65.5%). Therefore, routine screening awareness campaigns and timely diagnosis are recommended to safeguard maternal and fetal health in high-risk regions with limited diagnostic resources.
Keywords:
Toxoplasmosis
; early warning signs and symptoms
; risk factors
; diagnosis
; pregnant women
; systematic review
1. Introduction
Toxoplasmosis is a widely occurring zoonotic disease caused by the protozoan parasite Toxoplasma gondii, which can infect all warm-blooded animals, including humans. The disease is endemic in developing countries in Africa and Latin America and mainly spreads through ingestion of oocysts shed by infected cats or consumption of undercooked meat containing tissue cysts [1,2]. Although infections are often asymptomatic, they can cause serious health problems in immunocompromised people and pregnant women [3].
In pregnant women, toxoplasmosis is of special concern because of the risk of transmitting the infection to the unborn fetus [4]. If a primary infection occurs during pregnancy, it can lead to miscarriage, stillbirth, or birth defects such as hydrocephalus, intracranial calcifications, and chorioretinitis [5,6]. Most maternal infections are either asymptomatic or present with mild, nonspecific signs such as swollen lymph nodes, fatigue, and fever, making early diagnosis difficult [7,8]. Recognizing these subtle signs early is therefore crucial to enable prompt action and help prevent adverse effects on the fetus [9].
Despite its public health importance, early detection of toxoplasmosis in pregnant women is often difficult due to a lack of clear clinical signs [9]. Diagnosis primarily relies on serological screening and molecular methods, such as PCR, to confirm acute infection [2,10]. Recognizing the early warning signs and risk factors associated with T. gondii infection in pregnant women is crucial for improving diagnosis, treatment outcomes, and preventing severe complications [11].
The present systematic review aimed to identify and synthesize available evidence on early warning signs and symptoms, risk factors, and diagnostic methods for toxoplasmosis in pregnant women. By highlighting key indicators of infection, this review seeks to inform surveillance, clinical diagnosis, and public health interventions for this widely neglected parasitic disease.
2. Materials and Methods
This review was conducted in two phases: a preliminary scoping study, followed by a full systematic review. The scoping phase mapped the existing literature on early warning signs and symptoms of toxoplasmosis in pregnant women and identified gaps that warranted a more detailed synthesis. The findings from this phase informed the development of the review questions, inclusion criteria, and search strategy for the systematic review.
2.1. Search Strategy
A comprehensive literature search was conducted across Google Scholar, Scopus, ResearchGate, and PubMed. The search focused on publications on clinical manifestations and symptoms, epidemiology, and diagnostic techniques for toxoplasmosis in pregnant women, from January 2000 to December 2025. Key phrase combinations included “Toxoplasma gondii,” “toxoplasmosis,” “early warning signs,” “pregnant women,” “clinical signs,” “symptoms,” “risk factors,” and “diagnosis, using Boolean operators (AND/OR). To find more papers, the reference lists of journal articles and qualified studies were manually screened after eliminating duplicate records and those without references.
2.2. Eligibility Criteria
Studies were included if they:
a) Reported early clinicals or subclinical signs and symptoms, risk factors, or diagnostic indicators of T. gondii infection in pregnant women;
b) Presented original research (cross-sectional, cohort, case–control, experimental, outbreak/case reports, or surveillance studies);
c) Were published in English from January 2000 to December 2025;
d) Provided sufficient methodological and outcome details for data extraction.
Studies were excluded if they:
a) Did not focus on toxoplasmosis in pregnant women;
b) Were reviews, editorials, conference abstracts, or commentaries;
c) Had missing key information (e.g., title, abstract, or authors);
d) Were inaccessible despite reasonable retrieval efforts.
2.3. Study Selection
The titles and abstracts were screened, followed by full-text assessment to select the relevant studies. The study selection process was conducted in accordance with the PRISMA guidelines, and the final number of included studies is presented in a PRISMA flow diagram.
2.4. Data Extraction
Data were extracted using a structured extraction form in Microsoft Word 2019 and later transferred to Excel for organization. Extracted information included:
- Study characteristics (author, year, location, design)
- Early symptoms, clinical or subclinical signs reported
- Behavioral and host-related risk factors
- Diagnostic tools used (e.g., ELISA, MAT, PCR)
The extracted data were cross-checked for accuracy and completeness.
2.5. Data Synthesis and Analysis
Due to variation in study designs, diagnostic methods, and outcome measures, meta-analysis was not feasible. Instead, a narrative synthesis approach was adopted, organizing data based on early warning signs, risk factors, and diagnostic indicators. Microsoft Excel was used to tabulate and visualize quantitative results such as prevalence figures and frequency distributions. The findings were summarized using descriptive statistics, where graphs and tables were used to illustrate clinical presentations, risk factor patterns, and diagnostic indicators.
2.6. Ethical Considerations and Data Availability
Only publicly available studies were used; ethical approval for this review was not required. All materials, data, and extraction forms will be made available upon request.
3. Results
A total of 407 studies were initially identified through database searches. After removing duplicates and screening titles and abstracts, 31 studies met the inclusion criteria (Figure 1). Studies were excluded if they did not focus on toxoplasmosis in pregnant women, lacked accessible full texts, or lacked essential bibliographic details. The remaining articles provided additional relevant evidence on early signs, risk factors, or diagnostic indicators of Toxoplasma gondii infection. Findings were synthesized narratively and summarized in Table 1, with the studies arranged alphabetically by study location. The 31 studies were from 18 countries, including 28 from Africa, 1 from France in Europe, 1 from Palestine in the Middle East, and 1 from El Salvador in Latin America. Most countries had only one or two studies, except for Nigeria, which had 5 studies, and Cameroon and Ethiopia, which each had 4 studies (Table 1). The 28 studies from Africa were distributed across the five African Union regions, with 10 from Eastern Africa, 9 from Western Africa, 5 from Central Africa, and 2 each from Northern and Southern Africa.
3.1. Early Warning Signs / Clinical Manifestations and Outcomes
Congenital anomalies were the most frequently reported outcome of the infection, appearing in 25.8% of the studies (Figure 2), reflecting the well-documented risk of fetal structural damage following maternal toxoplasmosis. Miscarriage followed at 22.6%, highlighting its substantial contribution to adverse pregnancy outcomes. Lymphadenopathy and flu-like manifestations each occurred in 19.4% of studies, consistent with the nonspecific systemic presentation of acute infection. Neurological involvement and stillbirth were reported less often (both 16.1%), yet remain clinically significant due to their severity. Ocular manifestations and asymptomatic infections were the least frequent (6.5% each), underscoring the heterogeneous clinical spectrum observed across studies.
3.2. Key Risk Factors for Toxoplasmosis in Pregnancy
Exposure to cats was the most frequently reported risk factor, appearing in the greatest proportion of the included studies (51.6%) (Figure 3), followed by consumption of undercooked meat (41.9%), which remained a major contributor to Toxoplasma gondii transmission. Consumption of contaminated water (25.8%) was identified less often, yet still represented a relevant environmental source of infection. Contact with contaminated soil (22.6%) and consumption of raw vegetables (19.4%) were the least frequently documented exposures.
3.3. Diagnostic Indicators and Methods
The enzyme-linked immunosorbent assay (ELISA) was the diagnostic test used in the highest proportion of studies (65.5%) (Figure 4). Other tests were used in only one study (3.4%), except for the Latent Agglutination Test (LAT) and ELISA combined with polymerase chain reaction (PCR), which were used in 3 (103%) and 2 (6.9%) of the studies (Figure 4).
The seroprevalence of T. gondii infections varied widely across studies within countries and regions, even when the same test was used. For instance, of the 10 studies conducted in eastern Africa, 5 used ELISA and 3 used LAT. The median and range of seroprevalence based on ELISA were 23.9% (12.2% – 67.8%). Similarly, in western Africa, 8 of the 9 studies used ELISA to determine seroprevalence, and the observed median and range were 42.09% (29.60% - 55.90%). Four of the 5 studies in central Africa also used ELISA, and the median and range were 52.3% (34.6% - 80.30%).
4. Discussion
In this systematic review, the most commonly reported signs and symptoms of toxoplasmosis during pregnancy are swollen lymph nodes and flu-like symptoms. These are mild symptoms that are often missed as they are disregarded and confused with the flu or other infections, as previously observed by Nguemaïm et al [14]. Signs of toxoplasmosis during pregnancy can be asymptomatic, as reported by Daweet et al (26). Lack of specific clinical signs and its asymptomatic nature complicates early detection using clinical signs without laboratory confirmation [16,26]. This is therefore of particular concern because it carries significant risks for vertical transmission, potentially resulting in congenital toxoplasmosis [36].
Congenital anomalies and miscarriage were the most common outcomes in the studies reviewed, but this does not necessarily mean that they are the most common consequences of toxoplasmosis. Their severe manifestation increases the likelihood of investigating and reporting them. Congenital anomalies are characterized by fetal complications such as hydrocephalus, chorioretinitis, or intracranial calcifications [40]. Miscarriages and abortion, on the other hand, are consequences of acute toxoplasmosis during pregnancy [33,38]. However, toxoplasmosis is one of the causes of these congenital anomalies and miscarriage among many diseases and conditions. Early diagnosis of Toxoplasma gondii infections in pregnant women is therefore crucial to prevent the serious complications. In this review, many studies combined maternal symptoms with fetal outcomes. However, lymphadenopathy and flu-like symptoms are early warning signs in the mother, while miscarriage and congenital defects are the results of vertical transmission of the infection to the foetus.
The significant risk factor reported in the review is exposure to cat faeces. It is the major transmission route, emphasizing the importance of preventive practices such as safe litter handling, regular handwashing, and avoiding contact with stray cats during pregnancy [24]. Other risk factors include: consumption of undercooked or raw meat, poor food hygiene, contact with contaminated soil, and exposure to unsafe water sources. The differences in the reported risk factors could be explained by the diversity of geographical regions where the included studies were conducted [23,37]. Regional diversity influences cultural food habits, human and animal interactions, farming practices, sanitation levels, access to clean water, and awareness of toxoplasmosis [42]. However, most of the studies reviewed were cross-sectional, so the results indicate only the frequency with which these factors were mentioned, rather than their actual association with infection. These risk factors highlight the need for awareness campaigns targeting pregnant women to reduce infection rates by promoting simple preventive measures, such as proper meat cooking, hand hygiene, and avoidance of direct contact with cat feces [41].
Most of the studies included in this review primarily use the enzyme-linked immunosorbent assay (ELISA) to detect anti-Toxoplasma gondii antibodies in sera of pregnant women, but it cannot detect recent infections. IgG avidity was rarely used in the studies reviewed, yet it is essential for differentiating acute and chronic toxoplasmosis. The IgG avidity test can detect acute toxoplasmosis during early pregnancy and is important for controlling vertical transmission, which can cause congenital infection [39]. Limited studies reviewed, used PCR to detect T. gondii DNA, and the underutilization of these advanced diagnostic tools across the reviewed studies leads to inaccuracy of case classification and underreporting of the prevalence of acute toxoplasmosis. The underuse of PCR across the reviewed studies in varied regions could be explained by the fact that, despite it being highly sensitive, its utilization is often limited by cost and the need for specialized laboratory facilities and trained personnel [40]. However, polymerase chain reaction (PCR) can enhance the specificity of toxoplasmosis diagnosis in pregnancy as it detects T. gondii DNA in maternal blood, amniotic fluid, or placental tissues, providing direct evidence of active infection and complementing serological findings [33,40]. Future studies should integrate IgG avidity assays and molecular diagnostics alongside serology to improve the detection of recent infections and strengthen early warning systems to prevent congenital toxoplasmosis. These tests enable clinicians to identify pregnant women at the highest risk and to implement preventive or therapeutic measures, such as spiramycin treatment or close fetal monitoring [40].
5. Conclusion and Recommendation
In conclusion, this review highlights that early detection of toxoplasmosis in pregnant women requires an integrated diagnostic strategy combining the history of the pregnant woman to capture possible risk factors, clinical examination for signs/symptoms, serology, and, where possible use of molecular diagnostic methods.
It is therefore recommended that improving education, strengthening laboratory diagnosis, and promoting early screening during pregnancy are essential to reduce congenital toxoplasmosis.
Limitation of this Review
A formal risk-of-bias assessment was not conducted, meaning the methodological quality of individual studies was not systematically evaluated, and the likelihood of biases related to study design, sampling methods, and diagnostic accuracy may not have been clearly addressed.
The studies reviewed differed significantly in their design, diagnostic methods, reporting format, and outcome definitions. The cross-sectional nature of the studies limits conclusions about symptoms and their effects. Some studies used only IgG or IgM tests, while others used IgG avidity or PCR, leading to misclassification of infections. In addition, outcomes such as “toxoplasmosis infection” or “pregnancy complications” were defined differently across studies. These differences reduce comparability and may partly explain the wide variation in reported results. A meta-analysis could not be performed, and the findings are based on narrative synthesis, which may be more susceptible to subjective interpretation than pooled statistical analysis.
Despite these limitations, the review provides valuable insight into current diagnostic practices, reported clinical features, and research gaps, and highlights the need for more robust, standardized study designs in future toxoplasmosis research.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, C.J.T., N.EM., J.C.N, K.N., D.K.N.; methodology, C.J.T. and B.E.L.; validation, C.J.T. and B.E.L.; formal and data analysis, C.J.T. and B.E.L.; data curation, C.J.T.; writing original draft preparation, C.J.T.; writing review and editing, C.J.T.; supervision, N. M., J.C.N, K.N., D.K.N. A. P. N.N; funding acquisition, K.K.A., G.I.M. and B.B. All authors have read and agreed to the published version of the manuscript.
Funding
This study was funded in whole by Science for Africa Foundation [Afrique One-ASPIRE, Del-15-008 and Afrique One-REACH, Del-22-011] with support from Wellcome Trust and the UK Foreign, Commonwealth & Development Office, and is part of the EDCTP2 program supported by the European Union.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author on request. No publicly archived datasets were created or analyzed in this study.
Acknowledgments
The authors acknowledge their support in the preparation of this review. The authors reviewed and edited all outputs and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| ELISA | Enzyme-Linked Immunosorbent Assay |
| IgG | Immunoglobulin G |
| IgM | Immunoglobulin M |
| MAT | Modified Agglutination Test |
| PCR | Polymerase Chain Reaction |
| EIA- | Enzyme Immunoassay |
| T. gondii | Toxoplasma gondii |
References
- Tenter, A. M., Heckeroth, A. R., & Weiss, L. M. (2000). Toxoplasma gondii: From animals to humans. International Journal for Parasitology, 30(12–13), 1217–1258. [CrossRef]
- Roy, A., Gaucher, L., Dupont, D., Menotti, J., Atallah, A., De La Fournière, B., Massoud, M., Lina, B., Tirard-Collet, P., & Wallon, M. (2025). Epidemiological changes in Toxoplasma infection: A 7-year longitudinal study in pregnant women in Lyon, France, 2017–2023. Parasite, 32, 31. [CrossRef]
- Dubey J. P. (2021). Outbreaks of clinical toxoplasmosis in humans: five decades of personal experience, perspectives and lessons learned. Parasites & vectors, 14(1), 263. [CrossRef]
- Rukamba, J. D. D., Hakizimana, T., Ishimwe, M. P. S., Adoch, C. O., Pius, T., Baluku, A., & Musiime, J. N. (2024). Seroprevalence and factors associated with toxoplasmosis among pregnant women attending antenatal care clinic at a tertiary teaching hospital in Uganda: A cross-sectional study. International Journal of Reproduction, Contraception, Obstetrics and Gynecology, 13(2), 234–240. [CrossRef]
- Allam, A. F., Shehab, A. Y., Ahmed, N. A., Elshereedy, A. G., Farag, H. F., Abdo, S. M., & Ibrahim, H. S. (2025). IgG avidity and placenta real-time PCR in detection of active maternal toxoplasmosis: Relation to pregnancy outcomes. Experimental Parasitology, 279, 109065. [CrossRef]
- Akpan, N. G., Ekanem, E. N., Umoyen, A. J., Etang, U. E., Tuemi, R. D., & Moses, A. E. (2023). Seroprevalence and Risk Factors of Toxoplasmosis Among Pregnant Women Attending Antenatal Clinic in Uyo, Nigeria. Research Journal of Microbiology, 18(1), 80–92. [CrossRef]
- Sebaa, S., Behnke, J. M., Labed, A., & Abu-Madi, M. A. (2024). Seroprevalence of Toxoplasma gondii and Associated Risk Factors among Pregnant Women in Algeria. The American Journal of Tropical Medicine and Hygiene, 110(6), 1137–1144. [CrossRef]
- Agmas, B., Tesfaye, R., & Koye, D. N. (2015). Seroprevalence of Toxoplasma gondii infection and associated risk factors among pregnant women in Debre Tabor, Northwest Ethiopia. BMC Research Notes, 8(1), 107. [CrossRef]
- Lushina, M., Mushi, V., Tarimo, D., & Babafemi, E. O. (2022). Seroprevalence of Toxoplasma gondii and associated risk factors among pregnant women attending antenatal care in Ilala Municipality, Dar es Salaam, Tanzania. In Review. [CrossRef]
- Assoah, E., Yar, D. D., Amissah-Reynolds, P. K., Balali, G. I., Addy, R., & Zineyele, J. K. (2024). The Burden and Transmission Dynamics of Toxoplasmosis in Relation to Congenital Diseases among Pregnant Women in Ghana. Epidemiology. [CrossRef]
- Paul, E., Kiwelu, I., Mmbaga, B., Nazareth, R., Sabuni, E., Maro, A., Ndaro, A., Halliday, J. E. B., & Chilongola, J. (2018). Toxoplasma gondii seroprevalence among pregnant women attending an antenatal clinic in Northern Tanzania. Tropical Medicine and Health, 46(1), 39. [CrossRef]
- Page MJ, et al. BMJ 2021;372:n71. [CrossRef]
- Dambrun, M., Dechavanne, C., Guigue, N., Briand, V., Candau, T., Fievet, N., Lohezic, M., Manoharan, S., Sare, N., Viwami, F., Simon, F., Houzé, S., & Migot-Nabias, F. (2022). Retrospective study of toxoplasmosis prevalence in pregnant women in Benin and its relation with malaria. PloS one, 17(1), e0262018. [CrossRef]
- Nguemaïm, N. F., Takang, W. A., Dobgima, W. P., Guebidiang, B. M., Foumane, P.(2020). Seroprevalence of Toxoplasma gondii infection and associated risk factors among pregnant women attending antenatal clinic at the Bamenda Regional Hospital, Cameroon. African Journal of Clinical and Experimental Microbiology 21 (2), 123-131. 10.4314/ajcem.v21i2.
- Gebremedhin, E. Z., Abebe, A. H., Tessema, T. S., Tullu, K. D., Medhin, G., Vitale, M., Di Marco, V., Cox, E., & Dorny, P. (2013). Seroepidemiology of Toxoplasma gondii infection in women of child-bearing age in central Ethiopia. BMC Infectious Diseases, 13, 101. [CrossRef]
- Mabeku, L. B. K., Tchakounte, C., Bonsi, S. T., & Etoa, F.-X. (2018). Prevalence of Toxoplasma gondii and Associated Risk Factors among Pregnant Women Attending Hospital Centers in Penka-Michel, Cameroon. Journal of Scientific Research and Reports, 21(2), 1–11. [CrossRef]
- Cedric Y, Nadia NAC, Ambe NF, Guy-Armand GN, Payne VK (2022) Seroprevalence of Toxoplasma gondii IgG and IgM Antibodies and Associated Risk Factors among Pregnant Women Consulted at the Bamenda Regional Hospital, Cameroon. J Infect Dis Epidemiol 8:288. doi.org/10.23937/2474-3658/1510288.
- Doudou, Y., Renaud, P., Coralie, L., Jacqueline, F., Hypolite, S., Hypolite, M., Patrick, M., Andreia, I.daL., Van Sprundel, M., Marleen, B., Van Geertruyden, J. P., & Pascal, L. (2014). Toxoplasmosis among pregnant women: high seroprevalence and risk factors in Kinshasa, Democratic Republic of Congo. Asian Pacific journal of tropical biomedicine, 4(1), 69–74. [CrossRef]
- Mulugeta, S., Munshea, A., & Nibret, E. (2020). Seroprevalence of Anti–Toxoplasma gondii Antibodies and Associated Factors Among Pregnant Women Attending Antenatal Care at Debre Markos Referral Hospital, Northwest Ethiopia. Infectious Diseases: Research and Treatment, 13, 1178633720948872. [CrossRef]
- Wodage, M. , Asrade, B. , Teshome, Y. , Mengistu, A. and Bueso-Rodenas, J. (2023). Seroprevalence and Associated Risk Factors of Toxoplasma gondii Infections in Pregnant Women and Sheep in Meket District, North East Ethiopia. Journal of Zoonotic Diseases, 7(3), 333-344. [CrossRef]
- Jula, J., Girones, G., Edao, B., Deme, C., Cebrian, J., Butrón, L., Reyes, F., & Ramos, J. M. (2018). Seroprevalence of Toxoplasma gondii infection in pregnant women attending antenatal care in southern Ethiopia. Revista española de quimioterapia : publicación oficial de la Sociedad Española de Quimioterapia, 31(4), 363–366.
- Addo, S. O., Asare, T. O., Arthur, C., Amoateng, K., Addo, K., & Larbi, J. A. (2023). Toxoplasma gondii among pregnant women attending antenatal care in a district hospital in Ghana. Public Health Challenges, 2(2), e82. [CrossRef]
- Atif, I., Touloun, O., & Boussaa, S. (2025). Seroprevalence and Risk Factors of Toxoplasmosis Among Pregnant Women in Morocco: A Cross-sectional Study. Innovative Journal of Pediatrics, 35(4). [CrossRef]
- Zakari, M. (2020). Serological survey and risk factors associated with Toxoplasma gondii infection among HIV-infected pregnant women attending Abuja Tertiary Hospital, Nigeria. Malawi Medical Journal, 32(3), 169–176. [CrossRef]
- Bello, H., Umar, Y., Abdulsalami, M., & Amusan, V. (2017). Seroprevalence and Risk Factors of Toxoplasmosis among Pregnant Women Attending Antenatal Clinic in Kaduna Metropolis and Environs. International Journal of TROPICAL DISEASE & Health, 23(3), 1–11. [CrossRef]
- Dawet, A., Yusuf, K., Golnaan, C., Lengnen, E., Buhari, M., & Yakubu, D. (2022). Sero-Prevalence of Toxoplasma gondii in Pregnant Women Attending Antenatal Care in Jos University Teaching Hospital (JUTH). Journal of Infectious Diseases and Epidemiology, 8(11). [CrossRef]
- Adeniyi, O. T., Adekola, S. S., & Oladipo, O. M. (2023). Seroprevalence and risk factors associated with Toxoplasma gondii infection among pregnant women in Ile-Ife, Southwestern Nigeria. Journal of Infectious Diseases and Immunity, 15(2), 33-40.
- Nijem, K. I., & Al-Amleh, S. (2009). Seroprevalence and associated risk factors of toxoplasmosis in pregnant women in Hebron district, Palestine. Eastern Mediterranean health journal = La revue de santé de la Méditerranée orientale = al-Majallah al-sihhiyah li-sharq al-mutawassit, 15(5), 1278–1284.
- Murebwayire, E., Njanaake, K., Ngabonziza, J. C. S., Jaoko, W., & Njunwa, K. J. (2017). Seroprevalence and risk factors of Toxoplasma gondii infection among pregnant women attending antenatal care in Kigali, Rwanda. Tanzania Journal of Health Research, 19(1). [CrossRef]
- Ndiaye, J. L. A., Faye, B., Idarousse, N., Sow, D., Lo, A. C., Coulibaly, F., Manga, I. A., Ndiaye, M., Sylla, K., Tine, R. C., & Gaye, O. (2019). Toxoplasmosis Seroprevalence in pregnant women and in sheep and goats intended for human consumption in Dakar, using Direct Agglutination High-sensitivity techniques. African Journal of Parasitology Research.6(5), 001–008.
- Yusuf, A. A., Hassan-Kadle, A. A., Ibrahim, A. M., Hassan-Kadle, M. A., Yasin, A. M., Khojaly, M., Garcia, J. L., & Vieira, R. F. C. (2021). Prevalence of Anti-Toxoplasma gondii and Anti-Brucella Spp. Antibodies in Pregnant Women From Mogadishu, Somalia. Frontiers in reproductive health, 3, 672885. [CrossRef]
- Mustafa, M., Fathy, F., Mirghani, A., Mohamed, M. A., Muneer, M. S., Ahmed, A. E., Ali, M. S., Omer, R. A., Siddig, E. E., Mohamed, N. S., & Abd Elkareem, A. M. (2019). Prevalence and risk factors profile of seropositive Toxoplasmosis gondii infection among apparently immunocompetent Sudanese women. BMC research notes, 12(1), 279. [CrossRef]
- Lynn, M. K., Rodriguez Aquino, M. S., Cornejo Rivas, P. M., Miranda, X., Torres-Romero, D. F., Cowan, H., Meyer, M. M., Castro-Godoy, W. D., Kanyangarara, M., Self, S. C. W., Campbell, B. A., & Nolan, M. S. (2024). Employing digital PCR for enhanced detection of perinatal Toxoplasma gondii infection: A cross-sectional surveillance and maternal-infant outcomes study in El Salvador. PLOS Neglected Tropical Diseases, 18(5), e0012153. [CrossRef]
- Daka V, Mukosha M, Zimba SD, Phiri, A. M. (2024). Cross-sectional study to investigate the seroprevalence and risk factors of Toxoplasma gondii among women attending the antenatal clinic in Namwala, Zambia. BMJ Open;14:e084582. [CrossRef]
- Frimpong, C., Makasa, M., Sitali, L., & Michelo, C. (2017). Seroprevalence and determinants of toxoplasmosis in pregnant women attending antenatal clinic at the university teaching hospital, Lusaka, Zambia. BMC infectious diseases, 17(1), 10. [CrossRef]
- Damar Çakırca, T., Can, İ. N., Deniz, M., Torun, A., Akçabay, Ç., & Güzelçiçek, A. (2023). Toxoplasmosis: A Timeless Challenge for Pregnancy. Tropical Medicine and Infectious Disease, 8(1), 63. [CrossRef]
- Bobić, B., Villena, I., & Stillwaggon, E. (2019). Prevention and mitigation of congenital toxoplasmosis. Economic costs and benefits in diverse settings. Food and waterborne parasitology, 16, e00058. [CrossRef]
- Lima, M. L. F., Sousa, A. M. A. F. L. S. D., Marques, L. L., Ferreira, I. B., Giuffrida, R., Kmetiuk, L. B., Biondo, A. W., & Santarém, V. A. (2024). Household Location (Urban, Peri-Urban and Rural Settlements) as an Associated Risk Factor for Toxoplasmosis during Pregnancy in Southeastern Brazil. Tropical Medicine and Infectious Disease, 9(8), 173. [CrossRef]
- Teimouri, A., Mohtasebi, S., Kazemirad, E., & Keshavarz, H. (2020). Role of Toxoplasma gondii IgG Avidity Testing in Discriminating between Acute and Chronic Toxoplasmosis in Pregnancy. Journal of Clinical Microbiology, 58(9), e00505-20. [CrossRef]
- Teimouri, A., Mahmoudi, S., Behkar, A., Sahebi, K., Foroozand, H., Hassanpour, G., & Keshavarz, H. (2024). Current and Emerging Techniques for Diagnosis of Toxoplasmosis in Pregnancy: A Narrative Review. Iranian Journal of Parasitology. [CrossRef]
- Deganich, M., Boudreaux, C., & Benmerzouga, I. (2022). Toxoplasmosis Infection during Pregnancy. Tropical medicine and infectious disease, 8(1), 3. [CrossRef]
- Kurere, M., Mwandawiro, C., Kagira, J. M., & Karanja, S. (2024). Seroprevalence and Associated Risk Factors for Toxoplasma Gondii Among HIV Positive Pregnant Women Attending Antenatal Clinics in Uasin Gishu County, Kenya. In Review. [CrossRef]
Figure 1.
PRISMA 2020 Flow Diagrams modified from: [12].
Figure 1.
PRISMA 2020 Flow Diagrams modified from: [12].
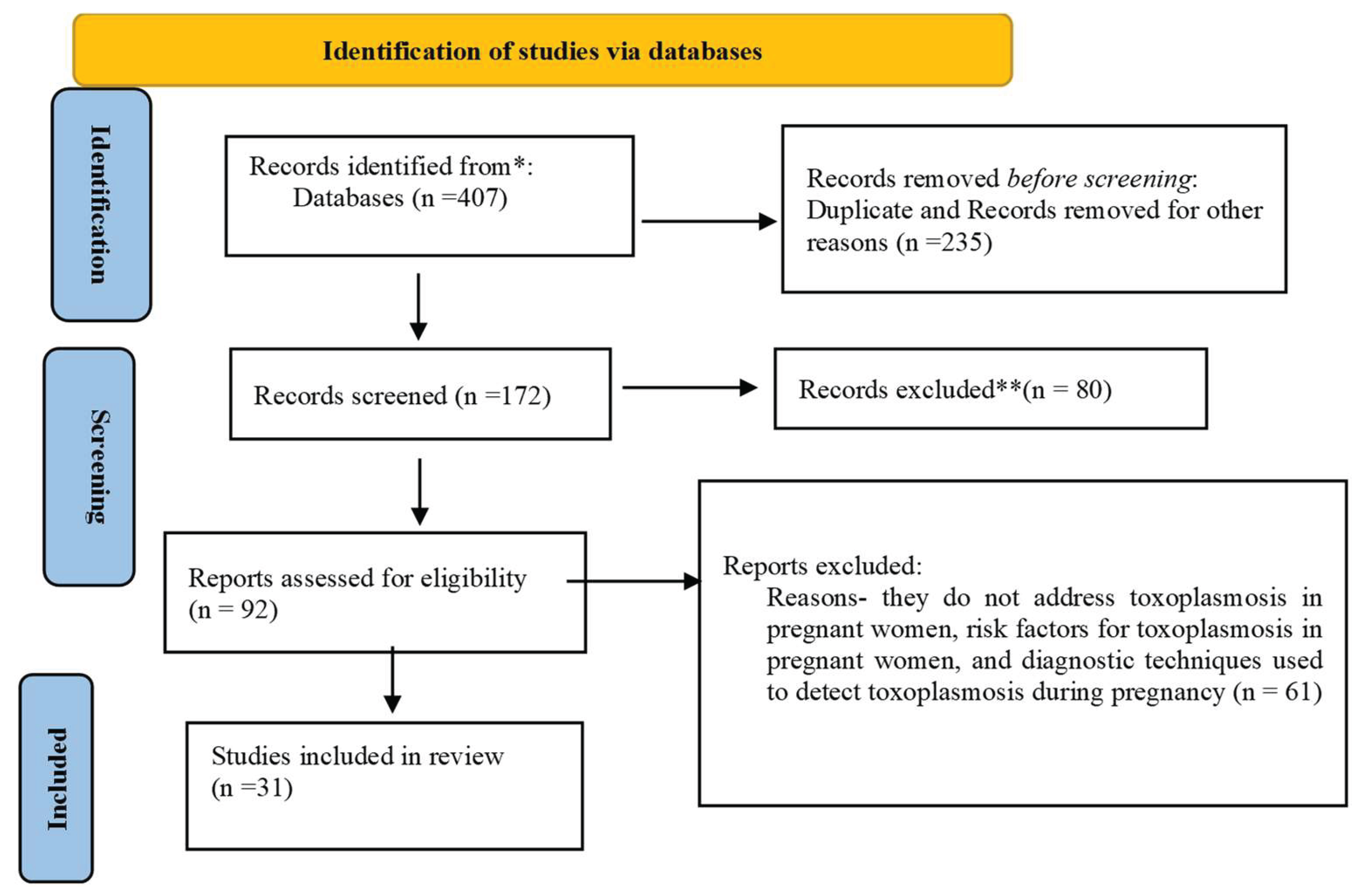
Figure 2.
The percentage of the 31 studies included in the review that reported specific clinical symptoms or outcomes among pregnant women with toxoplasmosis.
Figure 2.
The percentage of the 31 studies included in the review that reported specific clinical symptoms or outcomes among pregnant women with toxoplasmosis.
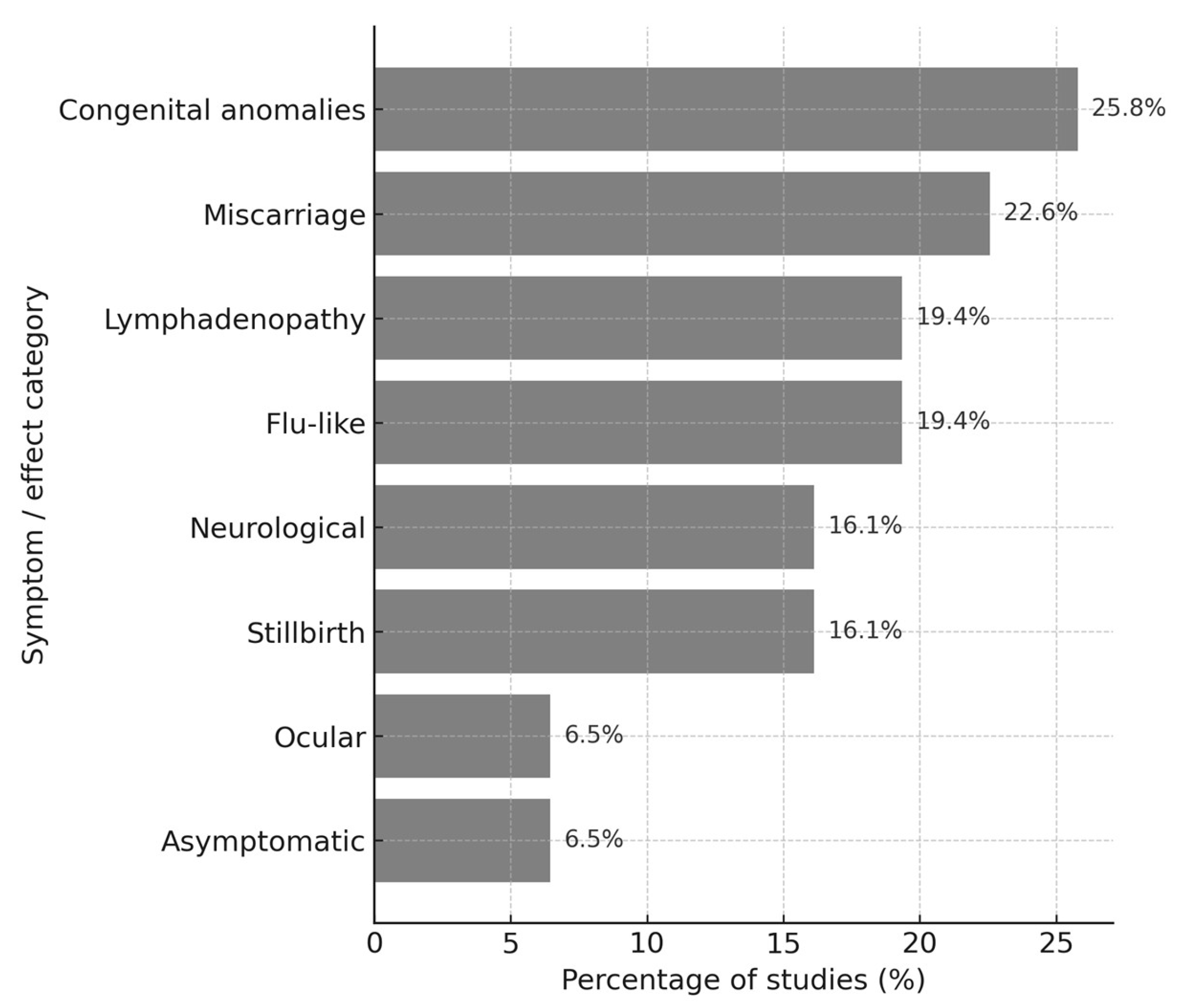
Figure 3.
Percentageof major risk factors reported across 31 studies included in the review.
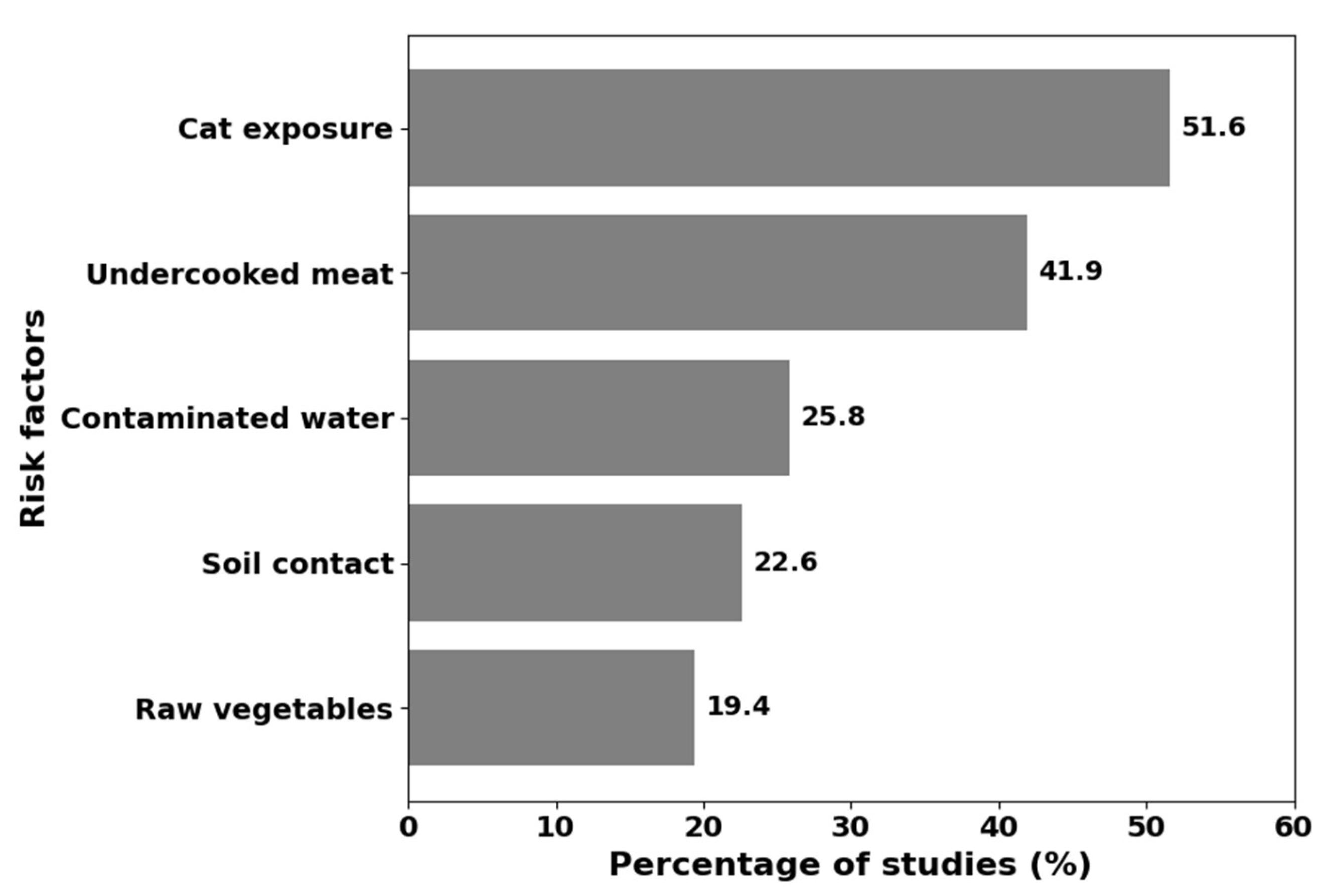
Figure 4.
Percentage of the 31 studies included in the review where specific diagnostic methods were used to estimate the prevalence of toxoplasmosis in pregnant women.
Figure 4.
Percentage of the 31 studies included in the review where specific diagnostic methods were used to estimate the prevalence of toxoplasmosis in pregnant women.
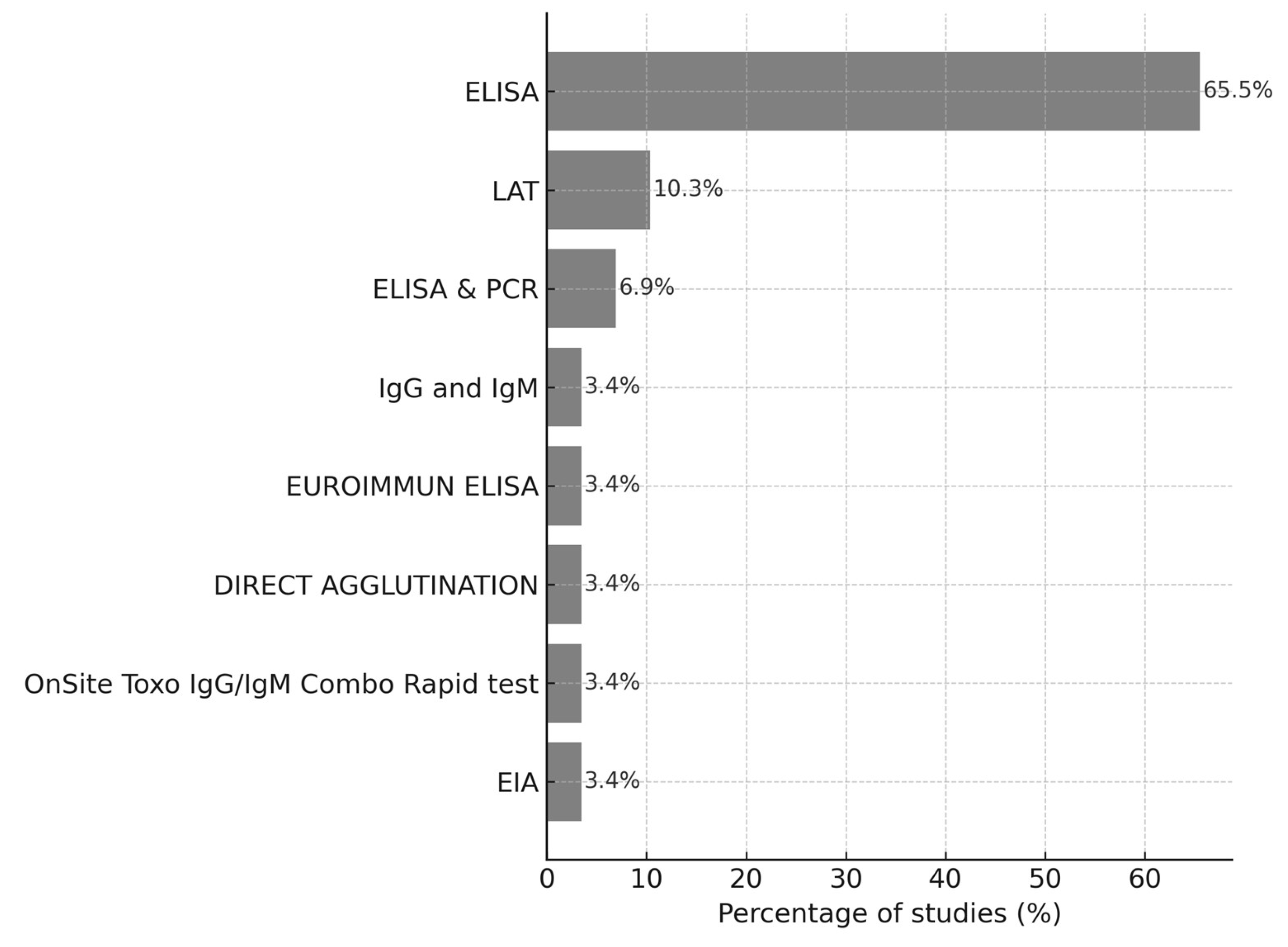

Table 1.
Characteristics of 31 cross-sectional studies included in the systematic review on toxoplasmosis in pregnant women.
Table 1.
Characteristics of 31 cross-sectional studies included in the systematic review on toxoplasmosis in pregnant women.
| Authors and year of publication | Study location | Geographical region | Potential symptoms and effects | Risks factors |
| Sebaa et al., 2024, | Algeria | Northern Africa | Miscarriages, stillbirths, complications in newborns | consumption of undercooked meat, contact with cats, and previous spontaneous abortions. |
| Dambrun et al.,2022, | Benin | Western Africa | neurological and ophthalmic disorders, or abortion | immune and genetic host factors, and characteristics of the T. gondii strain |
| Nguemaïm et al., 2020, | Cameroon | Central Africa | malaise, low-grade fever, and lymphadenopathy | pet ownership and handling of their litters |
| Gebremedhin et al., 2013, | Cameroon | Central Africa | mental retardation in congenitally infected children | raw vegetable consumption and poor drinking water quality. |
| Mabeku et al.,2018 | Cameroon | Central Africa | mild febrile illness, lymphadenopathy, and fatigue in some patients | lower educational levels, soil-related occupations, and consumption of raw or unwashed vegetables |
| Cedric et al., 2022 | Cameroon | Central Africa | malaise, low-grade fever, and lymphadenopathy | pet ownership and handling of their litters |
| Doudou et al., 2014, | Congo | Central Africa | severe malformations and spontaneous abortion. | Contact with soil, presence of a domestic cat, raw meat consumption, and poor hygiene. |
| Mulugeta et al., 2020, | Ethiopia | Eastern Africa | Causes mild symptoms | contact with cat feces, consumption of undercooked meat, raw vegetables, and blood transfusion |
| Wadage et al., 2023 | Ethiopia | Eastern Africa | abortion, stillbirth, and neonatal mortality | cat ownership, contact with soil, and lack of knowledge about food-borne diseases |
| Juja et al., 2018, | Ethiopia | Eastern Africa | miscarriage and cerebral calcification | Drinking unsafe water |
| Agma et al., 2015, | Ethiopia | Eastern Africa | flu-like illness, abortion, stillbirth, and severe neurological disorders | age, educational status, and cat ownership |
| Roy et al, 2025, | France | Europe | fetal loss, neonatal death, and neurological complications | Age, parity, population density, region |
| Addo et al., 2023, | Ghana | Western Africa | seizures, jaundice, loss of vision, and developmental delay | education level, contact with cats, soil exposure, and consumption of raw fruits and vegetables |
| Assoah et al., 2024 | Ghana | Western Africa | Miscarriage | level of education, residence, backyard animal farms, hygiene practices, water sources, and quality |
| Atif et al., 2025, | Morocco | Northern Africa | Miscarriage and congenital malformation | Contact with cats and a lack of awareness |
| Zakari et al., 2020. | Nigeria | Western Africa | blindness and neurological impairment in children | HIV-positive, older age, and urban settlement |
| Bello et al. 2017 | Nigeria | Western Africa | Cold and flu, cervical lymphadenopathy, and mononucleosis-like syndrome | Contact with cats and their litter |
| Dawet et al., 2022, | Nigeria | Western Africa | asymptomatic | Ingestion of undercooked meat, unpasteurized milk, and contact with cat litter |
| Akpan et al., 2023, | Nigeria | Western Africa | Abortion, stillbirth, hydrocephaly, mental retardation, and chorioretinitis in infants | educational level, outdoor gardening, blood transfusion, consumption of uncooked meat, and cat ownership |
| Adeniyi et al., 2023, | Nigeria | Western Africa | lymphadenopathy and flu-like illness | marital status, tasting raw meat, and the presence of rodents or cockroaches |
| Nijem, & Al-Amleh et al.,2009 | Palestine | Middle East | abortions and fetal anomalies | contact with contaminated soil, water, and vegetables, rather than just undercooked meat |
| Murebwayire et al., 2017 | Rwanda | Eastern Africa | spontaneous abortions and congenital deformities | drinking untreated water and consuming undercooked meat |
| Ndiaye et al, 2019, | Senegal | Western Africa | Severe complication during pregnancy | Consuming raw or undercooked contaminated meat and ingesting oocysts from contaminated water or food |
| Yusuf et al., 2021, | Somalia | Eastern Africa | abortion and congenital defects | at contact and consumption of raw or undercooked meat |
| Mustafa et al., 2019 | Sudan | Eastern Africa | severe fetal consequences in congenital transmission | Contact with cats, ingestion of raw meat |
| Lushina et al. (2023) | Tanzania | Eastern Africa | Asymptomatic but causes Miscarriage. Others: Swollen glands, Diarrhoea, Leg swelling, Nausea, Blindness, Eclampsia, Anaemia, Gestational diabetes | Increasing maternal age, consumption of undercooked meat, and lack of handwashing after meat preparation |
| Paul et al., (2018), | Tanzania | Eastern Africa | No clear sign, but it causes congenital problems | eating undercooked meat, raw vegetables, soil contact, and drinking contaminated water |
| Rukamba et al., (2024), | Uganda | Eastern Africa | Chronic: intrauterine growth retardation, post-term pregnancies, slow development of postnatal motor skills. Acute: miscarriages and congenital infections, | contact with cats, drinking untreated water, and HIV status |
| Lynn et al., 2024, | El Salvador. Western Region | Latin America | acute infection- labor and delivery complication, | presence of a cat pet |
| Daka et al., (2024), | Zambia | Southern Africa | Missed carriage and stillbirth | No significant risk factors |
| Frimpong et al., 2017, | Zambia | Southern Africa | ocular disease, lymphadenopathy, and encephalitis | Contact with cats |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



