
Submitted:
24 January 2026
Posted:
26 January 2026
You are already at the latest version
Abstract
Most falls occur while walking making gait quality a logical therapeutic target. Many tempo-ro-spatial variables have been implicated in increasing fall risk, but these are dependent upon kinematic parameters of the joints involved in the gait cycle. The widespread availability of wearable sensors has made the acquisition of kinematic data feasible and those related to the an-kle are most relevant as they relate most closely to causes of falls, trips, slips, and missteps. The purpose of this study is to estimate the extent to which measures of ankle angular velocity (AV) during walking are associated with falls. This is a comparative study of ankle AV metrics between people who have or have not experienced a fall in the past year. Data came from experimental use of the Heel2Toe™ sensor in a variety of settings including demonstrations and clinical research studies. The sample comprised 387 participants of whom 68 (17.6%) self-reported falling in the past year. Logistic regression with a natural cubic spline with 3 degrees of freedom identified AV of the angle at heel-strike to be the best discriminator between fallers and non fallers and the re-gression parameters were used to propose an algorithm to estimate fall risk. Applying the algo-rithm to the existing data yielded a range of probabilities from 0.0480 to 0.7245 depending on age of the person assessed. Further testing of this algorithm in different samples is warranted.
Keywords:
gait
; kinematics
; falls
; wearable
; sensor
; digital
1. Introduction
There is considerable clinical and research interest in risk factors for falls [1,2]) and fall risk assessment. Based on these risk factors, a number of fall risk algorithms have been developed, put into use, and systematicallyx summarized. [3,4,5]
The methods to identify risk factors and develop these algorithms have varied. One method has been to identify fallers, usually through self-reports of falls in the past, and estimate the extent to which current values on a set of candidate variables discriminate between fallers and non-fallers. [6,7,8,9,10] This method assumes participant recall is accurate and that the fall itself did not change the values on the variables of interest, the chicken-egg phenomenon.
A second and by far the strongest method is to assemble a representative sample of the target population, assess all at study entry, and follow participants into the future to ascertain the fall episodes for all and then link variables at study entry to fall occurrence or occurrences. A cohort study provides the most accurate estimates to develop an algorithm when there is complete follow-up of the cohort. [11,12,13,14,15]
A third method is, within a representative cohort, to identify those who fall (cases) and match these cases to one or more controls who have not fallen and look at historical data to identify factors predicting fall status, a case-control study [16,17]
The candidate variables fall into two groups: intrinsic (related to the person), and extrinsic, (related to the environment). [18,19] Within the intrinsic group, a further distinction is made between modifiable and non-modifiable variables and within the non-modifiable there are factors that pre-dispose someone to fall like medications which might alter blood pressure or vigilance and factors related to the circumstances of the fall. In a 2022 systematic review of 31 studies involving 70,868 community seniors the strongest intrinsic risk factors for falls were mainly non-modifiable factors including dementia (2.01, 95% CI: 1.41-2.86), age (1.15, 95% CI: 1.09-1.22), female gender (1.52, 95% CI: 1.27-1.81), fear of falling (2.82, 95% CI: 1.68-4.74), history of falls (3.22, 95% CI: 1.98-5.23), and vision unclear (1.56, 95% CI: 1.29-1.89). The strongest modifiable factors were depression (1.23, 95% CI: 1.10-1.37), and balance disorder (3.00, 95% CI: 2.05-4.39). [1]
Of the modifiable factors contributing to falls, the greatest interest is in those related to gait pattern as most falls occur when someone is upright and walking, [7,20,21,22,23,24] and balance and gait are amenable to intervention. [25,26,27,28]
Many features of gait, which is the manner of walking, have been implicated in falls and these are classified as temporo-spatial, kinetic, and kinematic gait parameters. Temporo-spatial gait parameters refer to measures of distance, time, or distance by time such as step and stride length, cadence, gait speed, step and stride time, time and duration of swing and stance phases of gait. [29] Kinematic parameters relate to range of motion at different joints and body segments during walking, and kinetic parameters relate to ground reaction forces generated during walking. [30,31] Kinematic and kinetic data are generated from technologically advanced systems such as motion capture systems, instrumented walkways, and force plates. [32] However, with the increasing number and sophistication of wearable sensors, it is now possible to measure these gait quality parameters outside of the laboratory without the expertise, cost, and infrastructure associated with these complex systems and then relate these data to health events, such as falls.
Several temporo-spatial variables have been related to falls including gait speed, stride length, and single leg stance [11] and these metrics are readily available from wearable sensors. Kinematic parameters are less easily obtained but the widespread availabiity of wearable sensors had made the acquistion of kinematic data feasible. [33] The kinematic parameters that have been linked to falls have been measured during the different phases of the gait cycle (heel-strike, foot-flat, push-off, swing). These include metrics related to variability in time spent in the different phases of gait, leg velocities, ankle angle velocities, and ankle angles. [34,35,36,37,38,39]
These studies, and others deriving metrics or non-linear dynamic measures from sensor outputs from different body segments, [40] provide a list of potential kinematic variables that discriminate between non fallers but do not provide an algorithm to predict an individual’s risk of falling. This is an important parameter because reducing fall risk can be a targeted outcome similarily to cardiovascular risk. [41,42,43]
Angular velocites of the ankle during the gait cycle are highly relevant metrics as they relate most closely to causes of falls, trips, slips, and mis-steps. [8,44] A new sensor, the Heel2Toe™ sensor, developed by PhysioBiometrics Inc., was developed specifically to measure ankle angular velocities during walking as human bipedal gait is characterized by a heel-to-toe pattern [45] and losing that pattern has been associated with falls. [46,47] The Heel2Toe sensor, shown in Figure 1, is one of a new generation of smart wearables that, in addition to providing rich data to accurately measure gait, also provides feedback for an optimal gait pattern, providing therapy in every step. [48]
The purpose of this study is to estimate the extent to which measures of ankle angular velocity during walking are associated with falls. This information would be used to quantify fall risk among gait vulnerable people and assess the extent to which interventions to improve gait quality would reduce this risk.
2. Materials and Methods
This is a comparative study of ankle angular velocity measures between people who have or have not experienced a fall in the past year.
2.1. Source of the Data
The data available for this study came from experimental use of the Heel2Toe sensor in a variety of settings including demonstrations and clinical research studies. Data collected during demonstrations of the sensor were not originally acquired for research purposes and therefore permission to use these data for research was granted by the Institutional Review Board of McGill University (A09-M51-23B) as no personal data was collected that could be used to identify the individual. All the clinical research studies using the sensor had ethical approval from their local research review boards and no identifying information was available to the research team associated with this project.
2.2. Sample
Only participants where it was possible to identify their age, disability status, and fall status were included. Excluded were participants with less than 10 steps during a walking session.
2.3. Measurement
Age was classified as 75 years and older or not; disability status was a binary variable based on diagnosis or use of a walking aid, and fall status (yes or no in the past year) was ascertained as part of the clinical research studies and also queried during demonstrations for people with disabilities. Data on sex was not consistently available. From the available descriptive information, 5 strata were formed. One stratum comprised people <75, without a disabilty, and a non-faller. This stratum served as a reference group. Another stratum comprised the fallers. The other three strata were comprised of non-fallers who were either older, with a disability, or both.
The Heel2Toe sensor attaches to the side of shoe and detects motion of the ankle during the gait cycle. The hardware for the Heel2Toe sensor consists of a microprocessor (MCU) running at 150 million instructions per second, an accelerometer, gyroscope, and magnetometer (collectively called an Inertial Measurement Unit (IMU)), each with 3 degrees of freedom running at 100 Hertz, or samples per second.
Metrics available from the Heel2Toe sensor for each step in a walking session are: angular velocity (AV) during heel strike, push off, and foot swing. These metrics are averaged over steps taken during each walking session and coefficient of variation (CV) is also calculated. Also available from the sensor is the time for each part of the gait cycle that can be used to calculate cadence and single leg stance.
Angular velocity of ankle rotation is extracted from the gyroscope (Z axis), clockwise movement is recorded as negative values (the more negative indicates higher velocity), movement anti-clockwise is recorded as positive values. Movement of the foot from initial heelstrike to footflat is a clockwise movement as is foot flat to push-off so both heel strike AV and push-off AV have negative values. To clear the foot during swing phase, the foot must rotate counter-clockwise and hence AV for foot clearance has a positive value.
2.4. Statistical Analysis
Each walking session comprises multiple steps, therefore, each gait metric was presented as the mean and standard deviation (SD) over all steps which was used to derive the CV over the steps of the walking session. The sample was described using the mean and the SD of the mean, and the mean and SD of the CV (presented as absolute value) as well as the range. Spearman correlations were conducted for all pairs of kinematic variables. A linear model was used to regress temporo-spatial and kinematic variable on the variable representing the 5 strata with the stratum representing non-fallers, <75 years, and without disability as the referent group
Logistic regression was used to identify the temporo-spatial and kinematic variables associated with the binary variable, fall status. A full model was tested first comprising all nine variables: three for each of AV of heel strike, push-off, and foot swing; ;three for the CV of these variables; and cadence, step time (proxy for stride length) and single leg stance. As all of these explanatory variables were continuous a natural cubic spline function with 3 degrees of freedom was used to model any potential non-linear effects.
All possible subsets analysis was used to choose the most parsimonous model. This modeling strategy yields a series of nested models which were tested using a likelihood ratio test. From the first model of nine variables all possible 8-variable models were tested against the full model and the variable with the least contribution to the model eliminated. This process was repeated with all nvar-1 models until all non-contrtibuting variables were eliminated. To this model, age category was added . Disability status was also considered but was strongly concordant with age. Once the shape of the function was known, ORs (95% CI) were produced for each part of the curve. All analyses were conducted using SAS version 9.4 and R version 4.3.1.
2.5. Power
As this study took advantage of existing data, power for a fixed sample size is the relevant estimate to consider. There were 68 fallers and 319 non-fallers, even with the conservative rule-of-thumb of 10 events per variable, this study has adequate power for testing 6 to 7 predictors. [49]
3. Results
3.1. Characteristics of the Sample
The sample comprised data on 387 participants who were assessed using the Heel2toe sensor, 68 (17.6%) of the participants self-reported falling in the past year. Of the sample, 240 (62.0%) were <75 years of age and 147 (38.0%) were 75+ years; 148 (39.2%) were classified as having a disability: 29 with Parkinson’s Disease, 12 with Multiple Sclerosis, 33 with orthopaedic conditions, 18 with soft tissue sarcoma; 53 needed a walking aid; and 2 had other disability situations. Table 1 presents temporo-spatial and kinematic characteristics of the sample according to five strata. In comparison to the reference strata (n=205) of non-fallers, <75 years, and without disability, the other samples all had less optimal values. The variables that differed between the strata and the reference sample are bolded and indicated by the inclusion of a p-value when it was <0.05. The variables that consistently distinguished all other strata from the referent strata were metrics related to AV.
Table 2 presents Spearman correlation coefficients among the 9 kinematic gait parameters tested in this study for their relationship with fall status. As these variables a part of the same construct, correlations of 0.8 or more are considered strong, and 0.5 to 0.8 are considered moderate. These are highlighted in the deepest blue. In lighter shades of blue are correlations of 0.4 and correlations of 0.3. The strongest correlations are among the measures of AV.
The results of the all-possible-subsets regression are not presented because the non-linear relationships required a model with a 3-df spline rendering the regression co-efficents uninterpretable. Three variables emerged from the regression model: Heel strike AV, age category, and cadence.
Figure 2 shows the shape of the relationship between heel strike AV on the x-axis and probability of a fall expressed as a percent on the y-axis using a logistic model with a natural cubic spline with 3 df and adjusting for cadence and age category. The dots at the bottom of the graph indicate the values of non-fallers along the x-axis, and those at the top of graph indicate the locations of the fallers. The graph clearly shows the non-linear relationship between heel strike AV and probability of falls. The shaded areas around the line show the 95% CI. As can be seen there is more confidence when values of heel strike AV are more than -450o/sec. Also evident is that the relationship changes considerably when values of heel strike AV approach -200 o/sec. To illustrate, the distribution of heel strike AV was divided into two segments, -450 to -200 and -200 to -50. There was a non-significant relationship between faller status and heel strike AV with values at the lower end, the more optimal values (OR per 1 o/sec: 1.003; 95% CI: 0.997 – 1.009). At less optimal values between -200 and -50 o/sec, there was a strong association (OR per 1o/sec: 1.026; 95% CI: 1.01 – 1.04). These values appear small because the units are per 1o/sec. If the regression parameters are estimatead per 50o/sec. the OR are 1.17 and 3.45 for the two segments, respectively. For the less optimal segment (-200 to -50 o/sec), for every 50 degrees that heel strike is less optimal, the odds of being a faller is increased by a factor of 3.45. Both models showed good predictive strength c-statistics >0.728 for people with strong heel strike and 0.768 for people with weak heel strike.
Table 3 presents the predicted probability of a fall for people with heel strike AV stronger (more negative) than 200o/sec and for people with with heel strike AV weaker (closter to 0) than 200o/sec, according to age category. The regression equations for each of these four strata are also presented. Fall risk decreased with stronger heel strike and increased with weaker heel strike; people aged 75 or older had a greater risk of falls at any degree of heel strike.
While cadence was associated with faller status overall, its effect when the data set was stratified by magnitude of heel strike AV, it was not significant and its effect on the predicted probability estimates was neglible. The lowest risk of falling was observed for cadences between 80 and 100 steps per minute, nadir 90 steps per minute.
Figure 3a and Figure 3b show the gait pattern of two individuals extracted from the data from the z-axis of the gyroscope of the Heel2Toe™ sensor positioned on the outside of the right shoe just under the lateral malleolus; 3a shows a person with an optimal gait pattern and a very low risk of fall and 3b shows a person with a very poor gait pattern and a high risk of falls.
4. Discussion
The results of this analysis indicate that starting the gait cycle with a strong heel strike has the potential to reduce fall risk. One reason for this is that a strong heel strike sets up the other phases of the gait, in particular optimal foot clearance. [44] Foot scuffing has been implicated in falls but the strategy to increase foot clearance is to emphasize a heel-to- gait pattern. [46,50]
AV at push off has previously been found to be associated with falls in a small sample of 163 seniors of mean age 82.6 years. [36] But few other studies have measured AV at the ankle. Some studies measured the degree of dorsi-flexion at the ankle during initial contact. One study measured AV but the sensor was placed mid shank representing leg movement rather than ankle movement. [37,39] A number of systematic reviews describe the potential utility of sensor derived kinematic data from sensors placed on the lower limb or on the lower back for the assessment of fall risk, but no current fall risk prediction algorithms have bee proposed. [40,51,52]
Our values on gait parameters are somewhat different than those reported by Beauchet at al. for a healthy sample of people 65+ years from two consortiums (n=954). Using the GAITrite® system, mean stride time for people 75+ was 1.15 seconds compared with >1.30 seconds in our samples (see Table 1). Similarly, Beauchet et al. reported single leg stance values of 0.41 seconds whereas in our sample with the value over the full sample was lower, approximately 0.31 seconds. This likely reflects that 50% of our sample had a disabling health condition or a history of falls.
This study is limited in that fall status was modeled and not fall incidence. Thus, this algorithm needs to undergo further testing. In addition, the data came from data accumulated from research projects where the sensor was used and hence the amount of data available was varied. Future studies, could also consider testing the algorithm for different walking durations or distances.
This study is limited in that fall status was modeled and not fall incidence. This our algorithm needs to undergo further testing. In addition, the data came from data accumulated from research projects where the sensor was used and hence the amount of data available was varied. The sample was also not selected to be representative of any particular segment of the population.
The results presented here open up additional avenues of scientific enquiry and implementation. The Heel2Toe™ sensor was developed primarily as a gait training device as its main functionality is to provide auditory feedback for a good step, one in which the AV at heel strike surpasses a specific threshold. This reward-feedback loop promotes neuroplasticity likely through the dopamine system. [48] While there are many effective exercise programs targeting balance [53], few target the elements needed for an optimal gait pattern: knowledge, strength and mobility of muscles and joints of the lower limb, core strength, all facets of balance (static, dynamic, anticipatory, and reactive), and coached training. [54,55] Paradoxically, indoor or outdoor walking programs have low evidence for efficacy and could even be harmful [55] and we hypothesize this negative effect could be because a sub-optimal gait pattern can increase scuffing, tripping, or mis-stepping, particularly as the person fatigues. [56] In addition, the role of sarcopenia in gait failure could be mediated through optimization of macro- and micronutrients known to be needed for muscle power and coordination. [57] Preventing falls is a complex goal and needs a multi-modal approach as each element is likely to increase the effectiveness of the other elements.
5. Conclusions
Average angular velocity at heel strike over a walking session of a minimum of 10 steps was the key kinematic variable discriminating between fallers and non-fallers and together with age (≥75 vs. <75 years) was used to propose an algorithm to estimate individual fall risk. Further validation of this risk model is needed.
Author Contributions
Conceptualization, NM; methodology, NM, HD, EH; software, EH; formal analysis, NM.; investigation, AA, HD, SD, CG, KG, KM, YT.; resources, HD, SD, CG, KG, YT; writing—original draft preparation, NM; writing—review and editing, HD, SD, CG, KG, KM, YT; project administration, NM; funding acquisition, NM, HD, SD, CG, KG, YT. All authors have read and agreed to the published version of the manuscript.
Funding
THIS NEEDS TO BE COMPLETED BY ALL IF RELEVANT. NM: data donation was made possible from funding by Health Brains for Health Lives, Rossy Cancer Network, and AGEWELL. HD: data donated was made possible from funding and support by the National Institute for Health and Care Research (NIHR) Exeter Biomedical Research Centre (BRC) and Healthtechnology Research Centre (HRC). The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care. SJD: data donated was made possible through funding from the Royal University Hospital Foundation and the College of Medicine, University of Saskatchewan. CG: data donated owing to funding as a Tier 2 Canada Research Chair in Perioperative Nutrition. KG: data donation made possible through funding from the Mayo Clinic, Arizona
Institutional Review Board Statement
The project --- Using existing data from Heel2Toe sensor to develop algorithms to detect gait anomalies that increases the risk of falls (23-07-020) --- was approved by the McGill University Research Ethics Board as a project making use of deidentified data not collected specifically for this specific research purpose.
Informed Consent Statement
Patient consent for this analysis was waived as no personal data was collected. However, each research project donating data to this study had an informed consent process approved by their local REB.
Data Availability Statement
These data are not available but the algorithm is given in the paper. We did not seek ethical approval for data sharing as the data have been donated from other projects.
Conflicts of Interest
NM, AA, HD, KM, EH are co-founders of PhysioBiometrics Inc., the company that developed and manufactures the Heel2Toe™ sensor. However, the algorithm given in this paper can populated with estimates from any sensor with the relevant IMUs. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results”.
References
- Li, Y., et al., Risk factors for falls among community-dwelling older adults: A systematic review and meta-analysis. Front Med (Lausanne), 2022. 9: p. 1019094. [CrossRef]
- Huang, A.R., et al., Medication-related falls in the elderly. Drugs & aging, 2012. 29(5): p. 359-376.
- Ong, M.F., et al., Falls risk screening tools intended to reduce fall risk among independent community-dwelling older adults: A systematic review. Int J Nurs Pract, 2023. 29(4): p. e13083. [CrossRef]
- Strini, V., R. Schiavolin, and A. Prendin, Fall Risk Assessment Scales: A Systematic Literature Review. Nurs Rep, 2021. 11(2): p. 430-443. [CrossRef]
- Hu, Z., et al., Diagnostic Accuracy of Fall Risk Screening Tools in Older Individuals: A Systematic Review With Bivariate Random-Effects Meta-Analysis. J Am Med Dir Assoc, 2025. 26(12): p. 105943. [CrossRef]
- Cesari, M., et al., Prevalence and risk factors for falls in an older community-dwelling population. J.Gerontol.A Biol.Sci.Med Sci., 2002. 57(11): p. M722-M726. [CrossRef]
- Boyé, N.D., et al., Circumstances leading to injurious falls in older men and women in the Netherlands. Injury, 2014. 45(8): p. 1224-30. [CrossRef]
- Lord, S.R., et al., An epidemiological study of falls in older community-dwelling women: the Randwick falls and fractures study. Aust.J.Public Health, 1993. 17(3): p. 240-245. [CrossRef]
- Brymer, C.D., et al., Do geriatric programs decrease long-term use of acute care beds? Journal of the American Geriatrics Society, 1995. 43(8): p. 885-889. [CrossRef]
- Lajoie, Y. and S.P. Gallagher, Predicting falls within the elderly community: comparison of postural sway, reaction time, the Berg balance scale and the Activities-specific Balance Confidence (ABC) scale for comparing fallers and non-fallers. Archives of Gerontology and Geriatrics, 2004. 38(1): p. 11-26. [CrossRef]
- Verghese, J., et al., Quantitative gait markers and incident fall risk in older adults. J Gerontol A Biol Sci Med Sci, 2009. 64(8): p. 896-901. [CrossRef]
- Tinetti, M.E., et al., Risk factors for serious injury during falls by older persons in the community. J Am Geriatr.Soc., 1995. 43(11): p. 1214-1221. [CrossRef]
- Tinetti, M.E., M. Speechley, and S.F. Ginter, Risk factors for falls among elderly persons living in the community. New England.Journal.of.Medicine, 1988. 319: p. 1701-1707. [CrossRef]
- Maki, B.E., P.J. Holliday, and A.K. Topper, A prospective study of postural balance and risk of falling in an ambulatory and independent elderly population. J Gerontol, 1994. 49(2): p. M72-84. [CrossRef]
- Graafmans, W.C., et al., Falls in the elderly: a prospective study of risk factors and risk profiles. American Journal of Epidemiology.143(11):1129-36, 1996. [CrossRef]
- Mayo, N.E., et al., Predicting falls among patients in a rehabilitation hospital. American Journal of Physical Medicine & Rehabilitation, 1989. 68(3): p. 139-146. [CrossRef]
- Grisso, J.A., et al., Risk factors for falls as a cause of hip fracture in women. The Northeast Hip Fracture Study Group. New England.Journal.of.Medicine, 1991. 324: p. 1326-1331. [CrossRef]
- Lach, H.W., et al., Falls in the elderly: reliability of a classification system. J Am Geriatr Soc, 1991. 39(2): p. 197-202. [CrossRef]
- Duque, G., Age-Related Physical and Physiologic Changes and Comorbidities in Older People: Association with Falls, in Medicaiton-Related Falls in Older People: Causitive Factors and Management Strategies, L.M. Allen R. Huang, Editor. 2016, Adis: Switzerland.
- Pitchai, P., et al., Prevalence, risk factors, circumstances for falls and level of functional independence among geriatric population - A descriptive study. Indian J Public Health, 2019. 63(1): p. 21-26. [CrossRef]
- Berg, W.P., et al., Circumstances and consequences of falls in independent community-dwelling older adults. Age Ageing, 1997. 26(4): p. 261-8. [CrossRef]
- Duckham, R.L., et al., Sex differences in circumstances and consequences of outdoor and indoor falls in older adults in the MOBILIZE Boston cohort study. BMC Geriatr, 2013. 13: p. 133. [CrossRef]
- Nachreiner, N.M., et al., Circumstances and consequences of falls in community-dwelling older women. J Womens Health (Larchmt), 2007. 16(10): p. 1437-46. [CrossRef]
- Talbot, L.A., et al., Falls in young, middle-aged and older community dwelling adults: perceived cause, environmental factors and injury. BMC Public Health, 2005. 5: p. 86. [CrossRef]
- Cadore, E.L., et al., Effects of different exercise interventions on risk of falls, gait ability, and balance in physically frail older adults: a systematic review. Rejuvenation.Res., 2013. 16(2): p. 105-114. [CrossRef]
- El-Khoury, F., et al., The effect of fall prevention exercise programmes on fall induced injuries in community dwelling older adults: systematic review and meta-analysis of randomised controlled trials. BMJ, 2013. 347: p. f6234. [PubMed]
- Goodwin, V.A., et al., Multiple component interventions for preventing falls and fall-related injuries among older people: systematic review and meta-analysis. BMC Geriatr., 2014. 14: p. 15. [CrossRef] [PubMed]
- Martin, J.T., et al., The effectiveness of physical therapist-administered group-based exercise on fall prevention: a systematic review of randomized controlled trials. J Geriatr.Phys.Ther., 2013. 36(4): p. 182-193. [CrossRef]
- Whittle, M., Applications of gait analysis. Gait Anal, 1991: p. 174-200.
- Sutherland, D.H., The evolution of clinical gait analysis part III--kinetics and energy assessment. Gait Posture, 2005. 21(4): p. 447-61. [CrossRef]
- Sutherland, D.H., The evolution of clinical gait analysis. Part II kinematics. Gait Posture, 2002. 16(2): p. 159-79. [CrossRef]
- Zahradka, N., et al., An Evaluation of Three Kinematic Methods for Gait Event Detection Compared to the Kinetic-Based ‘Gold Standard’. Sensors, 2020. 20(18): p. 5272. [CrossRef] [PubMed]
- Tao, W., et al., Gait analysis using wearable sensors. Sensors (Basel), 2012. 12(2): p. 2255-83. [CrossRef]
- Marques, N.R., et al., Is it possible to predict falls in older adults using gait kinematics? Clin Biomech (Bristol), 2018. 59: p. 15-18. [CrossRef]
- Callisaya, M.L., et al., Gait, gait variability and the risk of multiple incident falls in older people: a population-based study. Age Ageing, 2011. 40(4): p. 481-7. [CrossRef] [PubMed]
- García-de-Villa, S., et al., Validation of an IMU-Based Gait Analysis Method for Assessment of Fall Risk Against Traditional Methods. IEEE Journal of Biomedical and Health Informatics, 2025. 29(1): p. 107-117. [CrossRef]
- Álvarez, M.N., et al., Predictors of fall risk in older adults using the G-STRIDE inertial sensor: an observational multicenter case–control study. BMC Geriatrics, 2023. 23(1): p. 737. [CrossRef]
- Ullrich, M., et al., Fall Risk Prediction in Parkinson's Disease Using Real-World Inertial Sensor Gait Data. IEEE J Biomed Health Inform, 2023. 27(1): p. 319-328.
- Greene, B.R., et al., Digital assessment of falls risk, frailty, and mobility impairment using wearable sensors. npj Digital Medicine, 2019. 2(1): p. 125.
- Bonanno, M., et al., Use of Wearable Sensors to Assess Fall Risk in Neurological Disorders: Systematic Review. JMIR Mhealth Uhealth, 2025. 13: p. e67265.
- James, S., et al., A Systematic Review of Interventions to Improve Guideline Directed Secondary Cardiovascular Risk Reduction in Patients with Peripheral Arterial Disease. Eur J Vasc Endovasc Surg, 2025.
- Widmer, R.J., et al., Digital health interventions for the prevention of cardiovascular disease: a systematic review and meta-analysis. Mayo Clin Proc, 2015. 90(4): p. 469-80.
- Heneghan, H.M., et al., Effect of bariatric surgery on cardiovascular risk profile. Am J Cardiol, 2011. 108(10): p. 1499-507.
- Lai, D.T., S.B. Taylor, and R.K. Begg, Prediction of foot clearance parameters as a precursor to forecasting the risk of tripping and falling. Hum Mov Sci, 2012. 31(2): p. 271-83.
- Lovejoy, O., Evolution of Human Walking. Scientific American, 1988. 259: p. 118-25.
- Ginis, P., et al., Focusing on heel strike improves toe clearance in people with Parkinson's disease: an observational pilot study. Physiotherapy, 2017. 103(4): p. 485-490.
- Tinetti, M.E., Performance-oriented assessment of mobility problems in elderly patients. J Am Geriatr Soc, 1986. 34(2): p. 119-26.
- Mate K.V.K; Abou-Sharkh, A.M., M; Alosaimi, A; Dawes, N; Wright, M; Stanwood, O; Gorenkob, D; Mayo, N.E, Evidence for efficacy of commercially available wearable biofeedback gait devices: a consumer-centered review. Journal of Medical Informatics Research (JMIR) Rehabilitation and Assistive Technologies. In press.
- Vittinghoff, E. and C.E. McCulloch, Relaxing the rule of ten events per variable in logistic and Cox regression. Am J Epidemiol, 2007. 165(6): p. 710-8.
- Hughes, J.R., et al., Parkinsonian abnormality of foot strike: a phenomenon of ageing and/or one responsive to levodopa therapy? Br J Clin Pharmacol, 1990. 29(2): p. 179-86.
- Teixeira, E., et al., Wearable Devices for Physical Activity and Healthcare Monitoring in Elderly People: A Critical Review. Geriatrics (Basel), 2021. 6(2).
- Subramaniam, S., A.I. Faisal, and M.J. Deen, Wearable Sensor Systems for Fall Risk Assessment: A Review. Front Digit Health, 2022. 4: p. 921506.
- Sherrington, C., et al., Exercise to prevent falls in older adults: an updated systematic review and meta-analysis. British journal of sports medicine, 2017. 51(24): p. 1750-1758.
- Pollock, A.S., et al., What is balance? Clin Rehabil, 2000. 14(4): p. 402-6.
- Pillay, J., et al., Falls prevention interventions for community-dwelling older adults: systematic review and meta-analysis of benefits, harms, and patient values and preferences. Syst Rev, 2024. 13(1): p. 289.
- Morrison, S., et al., Walking-Induced Fatigue Leads to Increased Falls Risk in Older Adults. J Am Med Dir Assoc, 2016. 17(5): p. 402-9.
- Granic, A., et al., Nutrition in the prevention and treatment of skeletal muscle ageing and sarcopenia: a single nutrient, a whole food and a whole diet approach. Proc Nutr Soc, 2025. 84(4): p. 340-355.
Figure 1.
Heel2Toe™ sensor on the right shoe.

Figure 2.
Relationship of heel strike AV to faller status adjusted for average cadence and age.
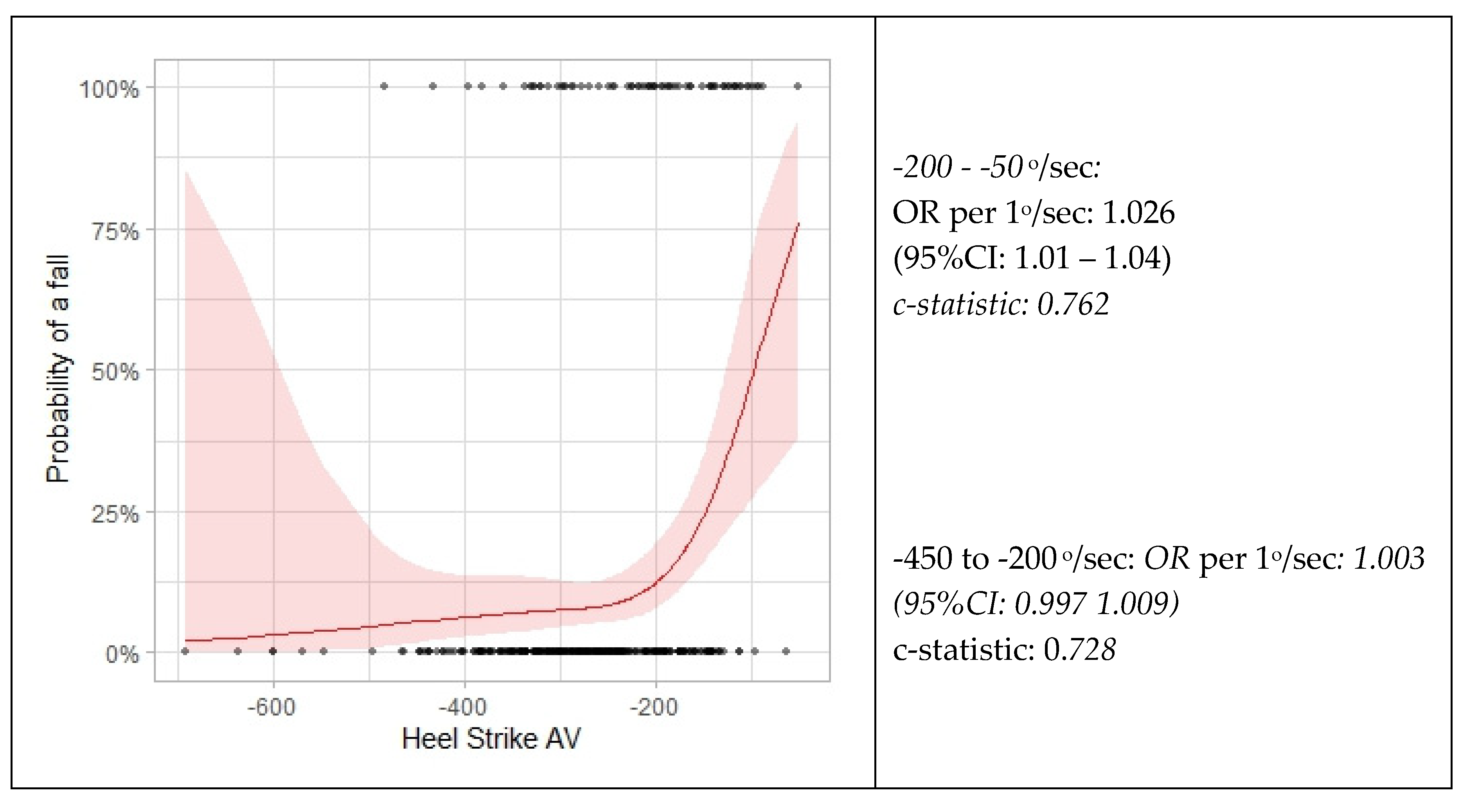
Figure 3.
a) Optimal Gait Pattern b) Poor Gait Pattern.
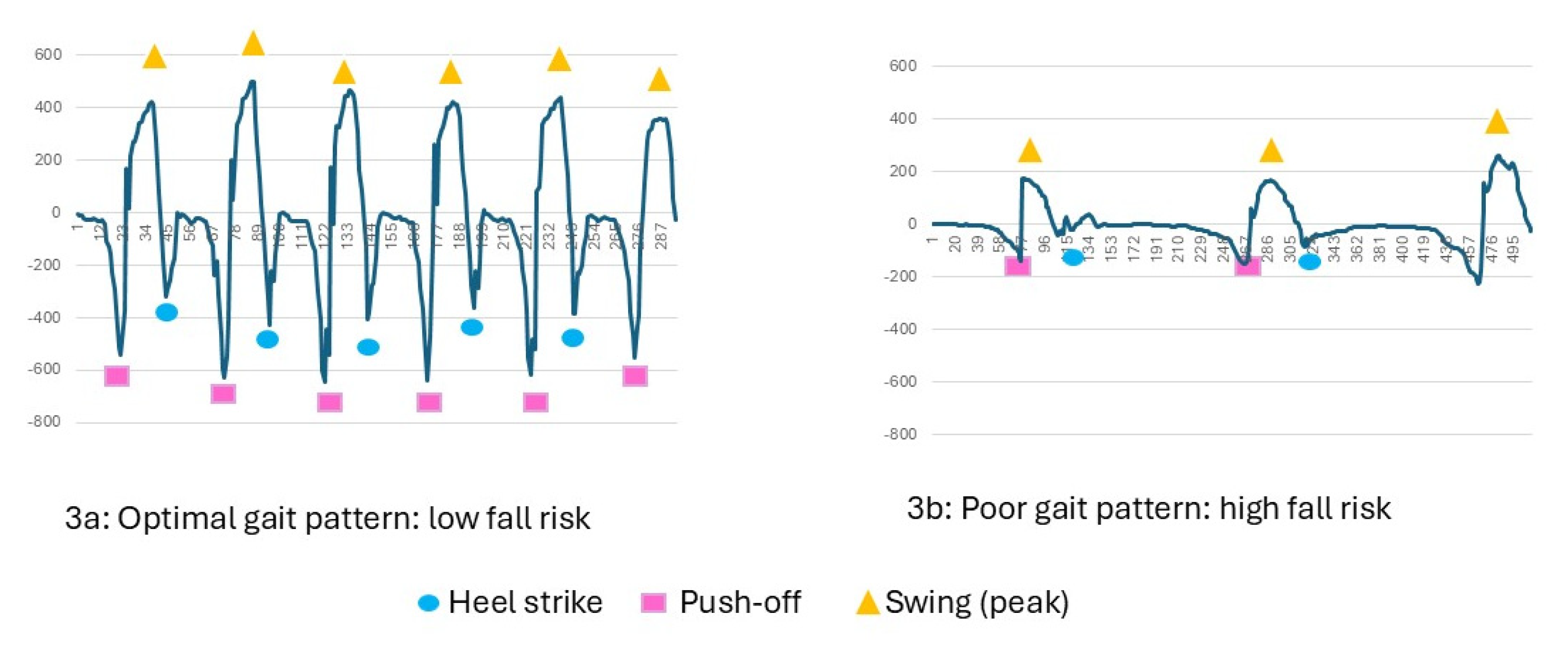

Table 1.
Average values for temporo-spatial and kinematic parameters calculated over a walking session according to strata defined by fall status, age, and disability.
Table 1.
Average values for temporo-spatial and kinematic parameters calculated over a walking session according to strata defined by fall status, age, and disability.
| Variable | Mean (SD) | Range | p-value (<0.05) vs. Referent |
| Stratum 1: Reference sample of non-fallers, <75 years, no disability (n=205) | |||
| Number of steps | 68.7 (132.3) | 10.0 - 1724.0 | Referent |
| Stride time (seconds) | 1.27 (0.28) | 0.62 - 2.44 | Referent |
| Cadence (steps/min) | 98.0 (19.2) | 49.3 - 193.3 | Referent |
| Single leg stance (seconds) | 0.31 (0.03) | 0.16 - 0.47 | Referent |
| Heel strike AV (-o/sec) | -289.12 (88.4) | -692.89 - -130.78 | Referent |
| |Heel strike CV | | 0.31 (0.15) | 0.05 - 0.88 | Referent |
| Push-off AV ( o/sec) | -393.2 (134.4) | -911.9 - -55.3 | Referent |
| |Push-off CV| | 0.29 (0.23) | 0.02 -1.44 | Referent |
| Foot swing AV (o/sec) | 362.9 (85.7) | 175.5 - 719.2 | Referent |
| |Foot swing CV| | 0.16 (0.11) | 0.03 - 0.61 | Referent |
| Stratum 2: Non-faller, <75, with disability (n=35) | |||
| Number of steps | 171.7 (130.5) | 17.0 - 562.0 | |
| Stride time (seconds) | 1.33 (0.39) | 0.87 - 2.59 | |
| Cadence (steps/min) | 96.3 (22.0) | 46.4 - 137.2 | |
| Single leg stance (seconds) | 0.32 (0.03) | 0.25 - 0.36 | |
| Heel strike AV (-o/sec) | -297.3 (84.6) | -436.8 - -147.0 | |
| |Heel strike CV| | 0.28 (0.12) | 0.10 - 0.61 | |
| Push-off AV (-o/sec) | -360.8 (153.4) | -629.4 - -4.7 | |
| |Push-off CV| | 0.47 (1.38) | 0.05 - 8.37 | 0.0460 |
| Foot swing AV (o/sec) | 344.5 (109.6) | 165.9 - 588.2 | <.0001 |
| |Foot swing CV| | 0.14 (0.06) | 0.06 - 0.31 | |
| Stratum 3: Non-faller, 75+, no disability (n-9) | |||
| Number of steps | 95.0 (80.2) | 18.0 - 254.0 | |
| Stride time (seconds) | 1.45 (0.39) | 1.05 - 2.26 | |
| Cadence (steps/min) | 87.2 (19.6) | 53.1 - 114.4 | |
| Single leg stance (seconds) | 0.31 (0.05) | 0.20 - 0.39 | |
| Heel strike AV | -255.5 (122.6) | -496.4 - -133.8 | |
| |Heelstrike CV| | 0.39 (0.14) | 0.19 - 0.64 | |
| Push-off AV | -267.7 (124.6) | -507.7 - -97.2 | 0.0110 |
| |Push-off CV| | 0.48 (0.33) | 0.10 -1.19 | |
| Foot swing AV | 293.1 (115.4) | 156.6 - 549.6 | 0.0256 |
| |Foot swing CV| | 0.21 (0.12) | 0.11 - 0.51 | |
| Stratum 4: Non-faller, 75+, with disability (n=70) | |||
| Number of steps | 95.9 (85.0 | 13.0 - 502.0 | |
| Stride time (seconds) | 1.32 (0.35 | 0.92 - 2.62 | |
| Cadence (steps/min) | 95.4 (18.9 | 45.8 - 130.5 | |
| Single leg stance (seconds) | 0.30 (0.03 | 0.21 - 0.39 | 0.0488 |
| Heel strike AV | -241.6 (82.0 | -463.7 - -62.3 | 0.0001 |
| |Heel strike CV| | 0.32 (0.16 | 0.09 -1.00 | |
| Push-off AV | -311.2 (148.1 | -721.6 - -64.6 | <.0001 |
| |Push-off CV| | 0.29 (0.28 | 0.05 -1.77 | |
| Foot swing AV | 313.2 (93.0 | 136.7 - 657.2 | 0.0001 |
| |Foot swing CV| | 0.16 (0.09 | 0.04 - 0.56 | |
| Stratum: Faller (n=68) | |||
| Age 75+ | 29 (63.2%) | ||
| Disability | 43 (91.2%) | ||
| Number of steps | 111.7 (102.4) | 10.0 -395.0 | |
| Stride time (seconds) | 1.41 (0.42) | 0.63 -2.60 | 0.0052 |
| Cadence (steps/min) | 92.7 (26.8) | 46.1 - 192.0 | |
| Single leg stance (seconds) | 0.30 (0.04) | 0.20 - 0.44 | |
| Heel strike AV | -213.0 (92.9) | -483.2 - -49.0 | <.0001 |
| |Heel strike CV| | 0.35 (0.16) | 0.10 - 0.80 | 0.0333 |
| Push-off AV | -286.7 (165.2) | -652.5 - -20.7 | <.0001 |
| |Push-off CV| | 0.40 (0.45) | 0.05 - 2.83 | |
| Foot swing AV | 283.2 (93.7) | 116.4 - 500.2 | <.0001 |
| |Foot swing CV| | 0.14 (0.08) | 0.04 - 0.42 | |
|absolute value|; (-o/sec) higher values are closer to 0 and a less optimal value for heel strike and push-off; (o/sec) higher values indicate more optimal foot swing.
Table 2.
Spearman Correlations among Kinematic Gait Parameters.
| Cadence | Single leg stance | Heel strike AV | Heel strike CV | Push-off AV | Push-off CV | Foot swing AV | Foot swing CV | ||
|---|---|---|---|---|---|---|---|---|---|
| Step time (sec) | -1.000 | -0.154 | 0.319 | -0.069 | 0.441 | -0.502 | -0.332 | 0.203 | |
| Cadence | 0.154 | -0.319 | 0.068 | -0.441 | 0.502 | 0.332 | -0.203 | ||
| Single leg stance | -0.348 | 0.228 | -0.459 | 0.225 | 0.416 | -0.271 | |||
| Heel strike AV | -0.297 | 0.570 | -0.263 | -0.784 | 0.063 | ||||
| Heel strike CV | -0.256 | 0.447 | 0.274 | -0.458 | |||||
| Push-off AV | -0.574 | -0.720 | 0.423 | ||||||
| Push-off CV | 0.335 | -0.671 | |||||||
| Foot swing AV | -0.186 | ||||||||
Table 3.
Probability of fall for people with Heel Strike AV stronger and weaker than -200o/sec according to category of age.
Table 3.
Probability of fall for people with Heel Strike AV stronger and weaker than -200o/sec according to category of age.
| Age (years) | Heel Strike AV (o/sec) | Predicted probability of a fall |
| Heel strike AV stronger than -200 o/sec | ||
| Predicted probability =1/(1+EXP(-(-1.7441 + 0.00311*HeelStrikeAV + 0*Age))) | ||
| <75 | -201 | 0.0858 |
| <75 | -225 | 0.0799 |
| <75 | -250 | 0.0744 |
| <75 | -275 | 0.0692 |
| <75 | -300 | 0.0643 |
| <75 | -325 | 0.0598 |
| <75 | -350 | 0.0556 |
| <75 | -375 | 0.0516 |
| <75 | -400 | 0.0480 |
| Predicted probability =1/(1+EXP(-(-1.7441 + 0.00311*HeelStrikeAV + 1.7339*Age))) | ||
| ≥75 | -200 | 0.0858 |
| ≥75 | -225 | 0.3296 |
| ≥75 | -250 | 0.3127 |
| ≥75 | -275 | 0.2962 |
| ≥75 | -300 | 0.2803 |
| ≥75 | -325 | 0.2648 |
| ≥75 | -350 | 0.2500 |
| ≥75 | -375 | 0.2357 |
| ≥75 | -400 | 0.2220 |
| Heel strike AV weaker than -200 o/sec | ||
| Predicted probability =1/(1+EXP(-(2.7323+0.0253*Heelstrike AV+0*Age))) | ||
| <75 | -200 | 0.0889 |
| <75 | -175 | 0.1551 |
| <75 | -150 | 0.2568 |
| <75 | -125 | 0.3941 |
| <75 | -100 | 0.5504 |
| <75 | -200 | 0.1739 |
| <75 | -175 | 0.2838 |
| <75 | -150 | 0.4272 |
| <75 | -125 | 0.5840 |
| Predicted probability =1/(1+EXP(-(2.7323+0.0253*Heelstrike AV+0.7693*Age))) | ||
| ≥75 | -100 | 0.7254 |
| ≥75 | -200 | 0.1739 |
| ≥75 | -175 | 0.2838 |
| ≥75 | -150 | 0.4272 |
| ≥75 | -125 | 0.5840 |
| ≥75 | -100 | 0.7254 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



