
Submitted:
23 January 2026
Posted:
26 January 2026
You are already at the latest version
Abstract
Background: Xanthogranulomatous endometritis (XGE) is a rare, chronic inflammatory disease that could mimic endometrial malignancy. While ultrasound is a primary imaging tool in gynecology, a comprehensive synthesis of its features in XGE is lacking. Objective: This study aimed to systematically review and summarize the sonographic characteristics of XGE. Methods: A systematic review was conducted following PRISMA guidelines, searching PubMed, Web of Science, and EMBASE for case reports describing ultrasound findings in pathologically confirmed XGE. A novel scoring system was developed and applied to evaluate reporting completeness of the ultrasound descriptions of XGE. Results: Eighteen case reports were included. The mean quality score was 3.2 out of 8 (range: 1-6). The most frequently reported sonographic features were intrauterine fluid collection or mass (88.9%) and endometrial thickening or irregularity (61.1%). Uterine enlargement was reported in 38.9% of cases. Assessment of vascular features was notably limited, with only three reports (16.7%) documenting the use of Color Doppler; among these, two confirmed the presence of intralesional blood flow, and both of the reports that provided spectral Doppler parameters described a low resistive index (RI < 0.7). Conclusion: This study reveals the common sonographic features of XGE, which center on intrauterine abnormalities and endometrial changes. The application of our novel scoring table revealed that the ultrasound descriptions in existing case reports are often incomplete, with doppler assessment being a notable gap. Future reports would benefit from more detailed doppler and morphological descriptions, which could help build a more reliable evidence base for the preoperative diagnosis of this rare condition.
Keywords:
xanthogranulomatous endometritis
; ultrasonography
; systematic review
; scoring system
; case reports
1. Introduction
Xanthogranulomatous inflammation is a rare chronic inflammation and a mixture of foam lipid loaded tissue cells and inflammatory cells [1,2], which may affect the kidney and gallbladder, and rarely involve endometrium. Xanthogranulomatous endometritis (XGE), an extraordinary disease, may be associated with endometrial carcinoma [3]. If not properly treated, this disease can have fatal consequences [4]. Therefore, it is important to make a correct diagnosis.
Ultrasound plays an important role in the examination of gynecological diseases because of non-invasive nature, real-time capability, safety, and accuracy [5,6,7].
The first case of XGE was reported by Barua et al. in 1978 [8], however, there is currently few English literature describing the ultrasonographic features of XGE till date [9,10].
This study aims to conduct a systematic review to integrate the ultrasonographic characteristics of XGE. Notably, I introduce a pioneering scoring system—the first of its kind—specifically designed to evaluate the methodological quality and reporting completeness of case reports on sonographic findings. This novel tool was developed to enable a structured assessment of the available evidence, hoping to explore the sonographic features of XGE and inform future studies.
2. Materials and Methods
2.1. Search Strategy
A systematic literature review on neonates with SPH was performed on PubMed, Web of Science and EMBASE according to the PRISMA guidelines by two independent researchers (Ji X and He WT). The search terms were: (“Xanthogranulomatous Endometritis” OR “XGE”). The search was conducted for published papers up to October 2025.
2.2. Inclusion and Exclusion Criteria
Case reports written in English describing female patients with a pathological confirmation of XGE who underwent ultrasound examination were included. Studies were excluded if they were irrelevant, non-English, not case reports, involved non-human subjects, or lacked any description of the ultrasound findings.
2.3. Study Selection and Data Extraction
Two reviewers (Ji X and He WT) independently screened the titles, abstracts, and full texts against the inclusion and exclusion criteria.
A standardized data extraction form was used in Microsoft Excel 2010 to collect the following information from each included study: first author, year of publication, patient age, and ultrasonographic findings. The process of study screening and selection is detailed in the PRISMA flow diagram (Figure 1).
2.4. Development of the Ultrasound Reporting Completeness Score
To systematically evaluate the methodological quality and reporting completeness of the ultrasound descriptions in the included case reports, we developed an 8-point scoring system based on the essential components of routine sonographic assessment and IETA consensus [11], the system assesses six key elements. The assessment items and scoring criteria are detailed in Table 1.
2.5. Statistical Analysis
Data analysis was performed using SPSS 28. Continuous variables are expressed as mean±standard deviation, frequency data is given as number and percent.
3. Results
3.1. Patient Baseline Characteristics
Among the 18 included patients, 16 reported exact age. The mean age of these patients was 68.7 ± 10.9 years (mean ± standard deviation), with an age range of 45 to 87 years. The remaining two patients were described as being in their “70s” and “late 70s”, respectively.
3.2. Ultrasound Reporting Completeness Score Results
The novel standardized scoring scheme was applied to the 18 included studies. The total scores of the included reports yielded a mean of 3.2 out of a maximum of 8 points, with a range from 1 to 6. The detailed scores for each paper are presented in Table 2.
Analysis of individual score items revealed the following: Basic lesion description: At least one descriptor of lesion nature was included in 18 reports (100%). Lesion Measurement: A specific measurement was provided in 13 reports (72.2%). Endometrium-myometrium relationship: This was described in 12 reports (66.7%). Color doppler assessment: Its use was mentioned and applied in only 3 reports (16.7%). Spectral doppler parameters: RI or PI values were provided in 2 reports (11.1%). Provision of ultrasound images: Images were provided in 5 reports (27.8%).
3.3. Summary of Sonographic Features
The frequency of described sonographic features across the 18 reports is summarized as follows: Uterus and Endometrium: Uterine enlargement was reported in 38.9% and endometrial thickening or irregularity in 61.1% of cases. Intracavitary Lesions: Intrauterine fluid collection or a mass was the most common finding (88.9%). Among reports providing specific descriptions, cystic texture was most frequent (68.8%). Vascular Features: Of the three reports that documented the use of Doppler techniques, two described rich intralesional vascularity with a low resistive index (RI < 0.7). The frequency of described sonographic features across the 18 reports is summarized in Table 3.
4. Discussion
This study, utilizing a novel quality assessment table alongside systematic review methodology, conducted the first comprehensive evaluation of the quality of ultrasound descriptions in case reports on XGE and summarized its characteristic sonographic findings. To our knowledge, this is also the first attempt to systematically assess reporting quality of ultrasound descriptions in case reports, using the scoring table as an initial tool for such analysis.
The kidneys and the gallbladder are the most common sites affected by xanthogranulomatous inflammation [26]. XGE is extremely rare [22], and it typically occurs in postmenopausal women, with a median age of 72 years and an age range of 45–88 years. Common clinical presentations include lower abdominal pain, irregular vaginal bleeding, and increased discharge, often secondary to conditions such as cervical stenosis, pyometra, endometrial hyperplasia, or malignancy. Infection is considered the most likely etiology, with other contributing factors including intrauterine hemorrhage and endometriosis. It may also occur after radiotherapy-induced endometrial or cervical tumor necrosis [3]. The pathogenesis of XGE is still subject to debate. The pathogenesis may involve chronic inflammation associated with pyometra caused by cervical stenosis or cervical cancer, where obstruction, inflammation, lipid sources, free radical generation, and lipid peroxidation could collectively contribute to the development of XGE [20].
The patients in the included reports were all postmenopausal, with a median age of 70.5 years, consistent with the commonly reported high-risk age group. Frequently observed sonographic features of XGE included intrauterine fluid collection or pyometra and endometrial thickening or irregularity. These findings are likely attributable to secretory retention from cervical stenosis or obstruction, chronic suppurative inflammation, and the subsequent histiocytic infiltration—including characteristic foam cells—mucosal disruption, and microabscess formation. Regarding the uniformity of echogenicity, while detailed description was lacking in many reports, heterogeneity was the most common finding (6 out of 9 reports that described the uniformity of echogenicity, 66.7%), which may reflect the underlying process of inflammatory attack and tissue repair.
Notably, vascular assessment with Doppler ultrasound was infrequently reported (16.7%). However, in this small subset of cases, detectable blood flow was reported in two of the three studies that performed Color Doppler, and both of the two studies that provided spectral Doppler indices reported low-resistance values (RI < 0.7). This emerges as a noteworthy, though not yet generalizable, finding. The chronic inflammatory milieu characteristic of XGE could theoretically promote angiogenesis and localized vasodilation, which offers a plausible explanation for these observed Doppler features. While obstruction, inflammation, and lipid peroxidation might collectively foster a hypervascular environment, our current data are insufficient to confirm this as a hallmark. Recognizing this potential is crucial for differential diagnosis, as these vascular features could otherwise heighten the suspicion for malignancy, potentially leading to misdiagnosis.
Histopathology still remains the gold standard for diagnosing XGE. The primary value of ultrasound lies in identifying abnormalities, suggesting diagnostic directions, and guiding biopsy. Since XGE may present with intrauterine fluid, endometrial thickening or irregularity, or even hypervascular masses, its imaging features overlap with those of endometrial carcinoma, making differential diagnosis based solely on ultrasound particularly challenging. However, this overlap underscores the importance of maintaining diagnostic awareness. When ultrasound reveals unexplained pyometra or other intrauterine fluid collection, especially when accompanied by a thickened or irregular endometrium in postmenopausal women, XGE should be considered in the differential diagnosis. The value of ultrasound in this context lies in highlighting the imaging similarities between this benign condition and malignant lesions. This could remind clinicians to actively seek evidence supporting XGE during pathological sampling, thereby avoiding misdiagnosis.
An analysis of the sonographic descriptions in the included case reports revealed that they primarily focused on basic morphological changes. For instance, hemodynamic information was missing in the vast majority of reports. Incorporating such information could complement existing descriptions and contribute to a more comprehensive understanding of the sonographic presentation of XGE.
This study systematically reviewed the sonographic features of XGE and, as a novel initiative, introduced a quality scoring table to evaluate the completeness of ultrasound descriptions in published case reports. It is important to note that this scoring system was developed specifically for this review, with its primary aim being to provide a structured, preliminary assessment of the current literature. The application of this tool revealed a considerable heterogeneity in reporting practices, with the majority of cases providing only fundamental morphological details while hemodynamic information from Doppler ultrasound was missing in most reports. By highlighting these variations, our scoring approach offers a practical tool to facilitate more objective and quantifiable assessments of ultrasound descriptions in future studies on XGE.
The main limitation of this work was that the analysis relied on the descriptions of sonographic findings as reported in the published literature rather than original images, which may have introduced bias in feature interpretation.
5. Conclusions
This study reveals the common sonographic features of XGE, which center on intrauterine abnormalities and endometrial changes. Frequently observed sonographic features of XGE included intrauterine fluid collection or pyometra and endometrial thickening or irregularity. The application of our novel scoring table revealed that the ultrasound descriptions in existing case reports are often incomplete, with doppler assessment being a notable gap. Future reports would benefit from more detailed doppler and morphological descriptions, which could help build a more reliable evidence base for the preoperative diagnosis of this rare disease. We hope that the scoring approach introduced here may also serve as a starting point for evaluating ultrasound description quality in future systematic reviews of case reports.
Disclosure of conflict of interest
None.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
- Goodman M, Curry T and Russel T. Xanthogranulomatous pyelonephritis (XGP): a local disease with systemic manifestations. Report of 23 patients and review of the literature. Medicine (Baltimore) 1979; 58:171-81.
- Dogan-Ekici AI, Usubütün A, Küçükali T and Ayhan A. Xanthogranulomatous endometritis: a challenging imitator of endometrial carcinoma. Infect Dis ObstetGynecol. 2007; 2007: 34763. [CrossRef]
- Russack V and Lammers RJ. Xanthogranulomatous endometritis. Report of six cases and a proposed mechanism of development. Arch Pathol Lab Med. 1990; 114: 929-32.
- Noack F, Briese J, Stellmacher F, Hornung D and Horny HP. Lethal outcome in xanthogranulomatous endometritis. APMIS. 2006; 114: 386-8. [CrossRef]
- Guerriero S, Condous G, Rolla M, Pedrassani M, Leonardi M, Hudelist G, Ferrero S, Alcazar JL, Ajossa S, Bafort C, Van Schoubroeck D, Bourne T, Van den Bosch T, Singh SS, Abrao MS, Di Giovanni A, Tomassetti C, Timmerman D. Addendum to consensus opinion from the International Deep Endometriosis Analysis (IDEA) group: sonographic evaluation of superficial endometriosis. Ultrasound Obstet Gynecol. 2025; 66: 541-547. [CrossRef]
- Qiu Y, Xie Z, Jiang Y, Ma J. Segment anything with inception module for automated segmentation of endometrium in ultrasound images. J Med Imaging (Bellingham). 2024; 11: 034504. [CrossRef]
- Kim MJ, Lee Y, Lee C, Chun S, Kim A, Kim HY, Lee JY. Accuracy of three dimensional ultrasound and treatment outcomes of intrauterine adhesion in infertile women. Taiwan J Obstet Gynecol. 2015; 54(6):737-41. [CrossRef]
- Barua R, Kirkland JA and Petrucco OM. Xanthogranulomatous endometritis: case report. Pathology. 1978; 10: 161-4. [CrossRef]
- Zhang XS, Dong HY, Zhang LL, Desouki MM and Zhao C. Xanthogranulomatous inflammation of the female genital tract: report of three cases. J Cancer. 2012; 3: 100-106. [CrossRef]
- Wader JV, Jain A, Kumbhar SS and Vhawal V. Histiocytic endometritis. Am J Case Rep. 2013; 14: 329-32. [CrossRef]
- Leone FP, Timmerman D, Bourne T, Valentin L, Epstein E, Goldstein SR, Marret H, Parsons AK, Gull B, Istre O, Sepulveda W, Ferrazzi E, Van den Bosch T. Terms, definitions and measurements to describe the sonographic features of the endometrium and intrauterine lesions: a consensus opinion from the International Endometrial Tumor Analysis (IETA) group. Ultrasound Obstet Gynecol. 2010; 35: 103-12.
- Wu H, Liu J, Chen L, Peng J. Contrast-enhanced Ultrasound of Xanthogranulomatous Endometritis: A Case Report and Literature Review. Curr Med Imaging. 2023 May 11. [CrossRef]
- Shraim S, Al-Ettewi W, Mahfouz IA, Al-Attar M, Al-Masri A. Rare histopathological diagnosis of malakoplakia and Rosai-Dorfman disease in the same uterus mimicking malignancy: A case report. Exp Ther Med. 2025; 29: 44. [CrossRef]
- Batool R, Abdul Wahab NA, Selvamani S, Hennessy G. Recurrent pyometra coupled with xanthogranulomatous endometritis mimicking pyelonephritis and malignancy: unravelling clinical complexities. BMJ Case Rep. 2025;18: e259441. [CrossRef]
- Malik V, Chatterjee D, Goel B, Takkar N. Xanthogranulomatous Endometritis: A Benign Uncommon Masquerader of Malignancy. J Midlife Health. 2019; 10: 206-208. [CrossRef]
- Merviel P, James P, Carlier M, Thomas-Kergastel I, Guilloique M, Conan-Charlet V, Bastard C, Marcorelles P, Jobic Y, Dupré PF. Xanthogranulomatous endometritis: A case report and literature review. Clin Case Rep. 2021; 9: e04299. [CrossRef]
- Burston K, Lim W. Xanthogranulomatous endometritis: A rare histopathological finding. Australian and New Zealand Journal of Obstetrics and Gynaecology. 2021; 61: SUPPL 1 (47-).
- Silva-Rengifo C, Asencio A, Salirrosas O. Xanthogranulomatous Endometritis: A Report of Two Cases. Cureus. 2023; 15: e38226. [CrossRef]
- Na JM, Kim MH, Ko GH, Shin JK. Xanthogranulomatous endometritis: a report of two Korean cases with cytologic findings. J Pathol Transl Med. 2020; 54: 513-516. [CrossRef]
- Makkar M, Gill M, Singh D. Xanthogranulomatous endometritis: an unusual pathological entity mimicking endometrial carcinoma. Ann Med Health Sci Res. 2013; 3(Suppl 1): S48-9. [CrossRef]
- Altanis S, Raweily E, Katesmark M. Xanthogranulomatous endometritis and oophoritis secondary to diverticulitis. A rare cause of postmenopausal bleeding. J Obstet Gynaecol. 2007; 27: 746-7. [CrossRef]
- Du XZ, Lu M, Safneck J, Baker P, Dean E, Mottola J. Xanthogranulomatous endometritis mimicking endometrial carcinoma: A case report and review of literature. Radiol Case Rep. 2018; 14: 121-125. [CrossRef]
- Malik CA, Dudani S, Mani BN. Xanthogranulomatous endometritis presenting as pyometra and mimicking carcinoma on imaging. J Midlife Health. 2016; 7: 88-90. [CrossRef]
- Kumar N, Lakra PS, Sinha RK, Roy AD, Saha D, Sinha JK. Xanthogranulomatous Endometritis with calculus formation in setting of prolapsed uterus. Autops Case Rep. 2023; 13: e2023439. [CrossRef]
- Anandathirtha K, Shabnam Z, Manjeera L, Ramesh N. Xanthogranulomatous endometritis with unilateral salpingo-oophoritis in a postmenopausal woman masquerading as a malignancy. BMJ Case Rep. 2023; 16: e247341. [CrossRef]
- Morales Vicente A, García Sánchez Y, Santonja López N, Gilabert Estellés J. Xanthogranulomatous endometritis. Facts Views Vis Obgyn. 2023; 15: 351-353.
Figure 1.
PRISMA flow diagram for the study.
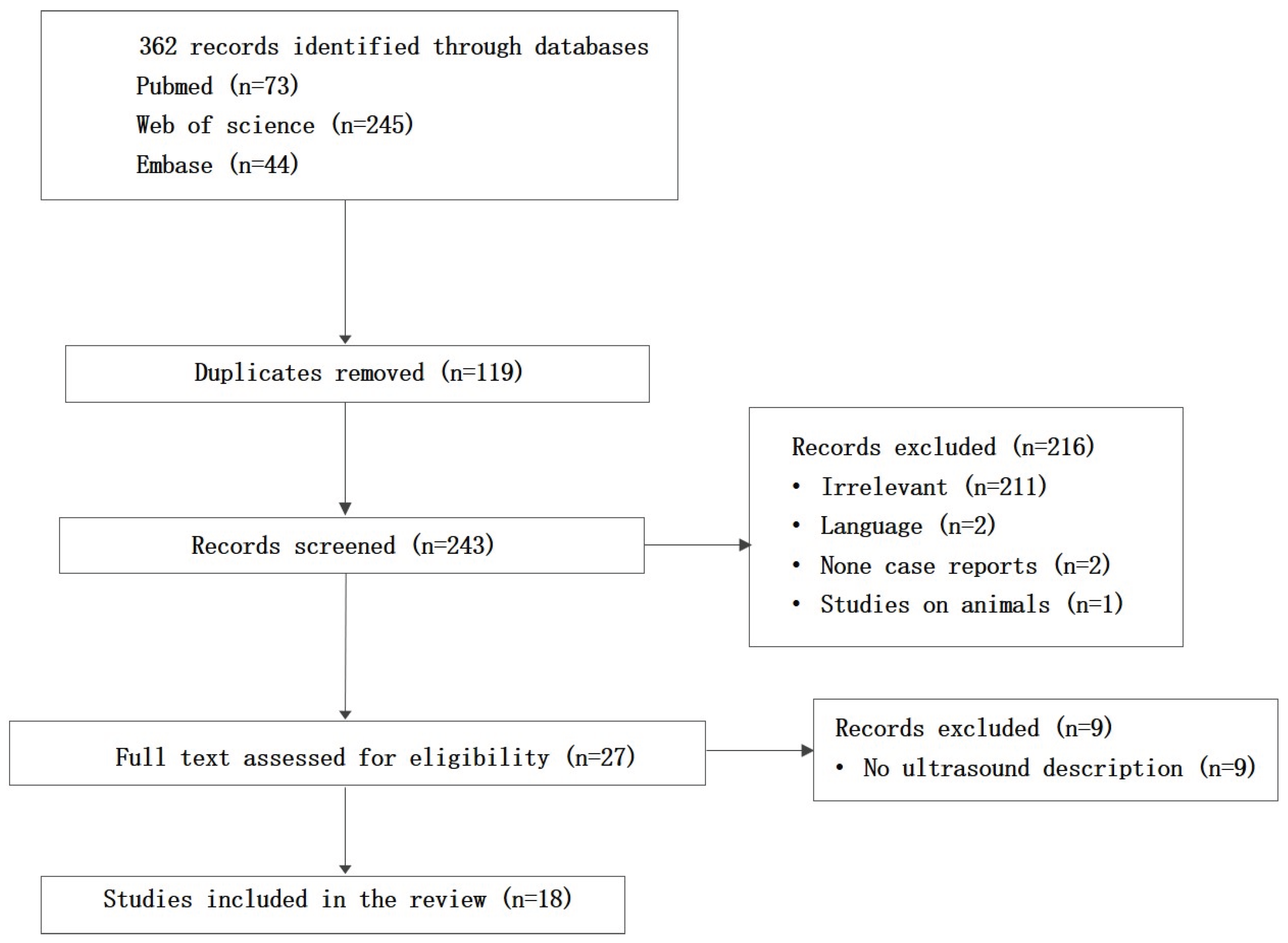

Table 1.
The assessment items and scoring criteria.
| Assessment Item | Scoring Criteria and Explanations | Score Range |
| Basic Lesion Description | Scoring Rule: Based on the number of the following three information categories described. • A. Uterine Size Abnormality: (e.g., “enlarged uterus” or “bulky uterus”). • B. Lesion Nature (IETA criteria): Mention of any of the following: - Basic Presence (e.g., intrauterine fluid collection/effusion” or “intrauterine mass/occupying lesion”). - Echogenicity Uniformity (e.g., uniform” or “non-uniform/heterogeneous”). - Lesion Texture (e.g., “cystic”, “solid”, or “mixed”). - Echogenicity Level (e.g., “hyperechoic/strong echo”, “isoechoic”, or “hypoechoic/weak echo”. • C. Precise Morphology (IETA criteria): Mention of specific morphological terms (e.g., “nodular”, “mass-like”, “polypoidal”, or “cauliflower like”). 1 point: Contains any 1 of categories A, B, or C. 2 points: Contains any 2 of categories A, B, or C. 3 points: Contains all 3 categories (A, B, and C). |
0-3 |
| Lesion Measurement | Provides specific dimensions of the lesion or uterus (e.g., length, width, thickness, endometrial thickness). 0 points: No specific measurement values provided. 1 point: At least one specific measurement value provided. |
0-1 |
| Endometrium-Myometrium Relationship | Describes the state of the endometrium or the relationship of the lesion to the myometrium/endometrium. 0 points: Not mentioned. 1 point: Explicitly describes relevant features (e.g., “endometrial thickening/irregularity” or “lesion with clear/unclear demarcation from the myometrium”, “lesion involving the myometrium”). |
0-1 |
| Color Doppler Assessment | Mentions the use of Color Doppler and describes blood flow. 0 points: Use of Doppler not mentioned. 1 point: Explicitly mentions the use of CDFI and describes blood flow signals (e.g., “rich vascularity” or “no internal flow”). |
0-1 |
| Spectral Doppler Parameters | Provides hemodynamic parameters. 0 points: No parameters provided. 1 point: Provides RI (Resistive Index) or PI (Pulsatility Index) values. |
0-1 |
| Provision of Ultrasound Images | Whether ultrasound images are provided in the paper for reference. 0 points: No ultrasound images provided. 1 point: At least one ultrasound image provided. |
0-1 |
| Total Score | 0-8 |
Table 2.
Completeness of sonographic descriptions in included case reports.
| Author (Year) | Basic Lesion Description | Lesion Measurement | Endometrium-Myometrium Relationship | Color Doppler Assessment | Spectral Doppler Parameters | Provision of Ultrasound Images | Total Score |
| Wu et al. (2023) [12] | 2 | 1 | 0 | 1 | 1 | 1 | 6 |
| Noack et al. (2006) [4] | 1 | 0 | 0 | 0 | 0 | 0 | 1 |
| Shraim et al. (2025) [13] | 1 | 1 | 1 | 0 | 0 | 0 | 3 |
| Batool et al. (2025) [14] | 1 | 0 | 0 | 0 | 0 | 0 | 1 |
| Malik et al. (2019) [15] | 1 | 1 | 1 | 0 | 0 | 1 | 4 |
| Merviel et al. (2021) [16] | 1 | 1 | 1 | 0 | 0 | 1 | 4 |
| Doğan-Ekici et al. (2007) [2] | 1 | 1 | 1 | 0 | 0 | 0 | 3 |
| BURSTON et al. (2021) [17] | 1 | 1 | 1 | 0 | 0 | 0 | 3 |
| Silva-Rengifo et al. (2023) [18] | 1 | 1 | 1 | 1 | 1 | 1 | 6 |
| Na et al. (2020) [19] | 2 | 0 | 0 | 0 | 0 | 0 | 2 |
| Makkar et al. (2013) [20] | 1 | 1 | 1 | 0 | 0 | 0 | 3 |
| Altanis et al. (2007) [21] | 1 | 1 | 1 | 0 | 0 | 0 | 3 |
| Du et al. (2018) [22] | 1 | 0 | 0 | 1 | 0 | 1 | 3 |
| Malik et al. (2016) [23] | 2 | 1 | 1 | 0 | 0 | 0 | 4 |
| Kumar et al. (2023) [24] | 2 | 0 | 1 | 0 | 0 | 0 | 3 |
| Anandathirtha et al. (2023) [25] | 1 | 1 | 0 | 0 | 0 | 0 | 2 |
| Morales et al. (2023) [26] | 1 | 1 | 1 | 0 | 0 | 0 | 3 |
| Zhang et al. (2012) [9] | 1 | 1 | 1 | 0 | 0 | 0 | 3 |
Table 3.
The frequency of described sonographic features across the reports.
| Sonographic Feature (based on direct description or inferable findings) | Frequency (Based on Total N=18) | Subgroup Distribution Analysis (Within Reports Describing the Category) |
| Uterus Uterine Enlargement |
7 (38.9%) |
|
| Endometrium Endometrial Thickening or Irregularity |
11 (61.1%) |
|
| Intracavitary Lesion – Presence Fluid Collection or Mass |
16 (88.9%) |
|
| Intracavitary Lesion - Characteristics (when specified) Echogenicity Level (n=4) Hyperechoic Hypoechoic Lesion Texture (n=16) Solid Cystic Mixed Uniformity of Echogenicity (n=9) Uniform Heterogeneous |
2 (11.1%) 2 (11.1%) 4 (22.2%) 11 (68.8%) 1 (5.6%) 3 (16.7%) 6 (33.3%) |
(Denominator = reports with specific description) (Denominator = 4) 2 / 4 (50.0%) 2 / 4 (50.0%) (Denominator = 16) 4 / 16 (25.0%) 11 / 16 (68.8%) 1 / 16 (6.3%) (Denominator = 9) 3 / 9 (33.3%) 6 / 9 (66.7%) |
| Intracavitary Lesion - Morphology (when specified) Polypoidal |
1 (5.6%) |
|
| Lesion Measurement Any Measurement Provided |
13 (72.2%) |
|
| Endometrium-Myometrium Relationship |
12 (66.7%) |
|
| Any Color Doppler Assessment Provided Blood Flow Detected No Blood Flow Detected |
3 (16.7%) 2 (11.1%) 1 (5.6%) |
(Denominator = 3) 2 / 3 (66.7%) 1 / 3 (33.3%) |
| Resistive Index Provided Low Resistive Index (RI < 0.7) |
2 (11.1%) 2 (11.1%) |
(Denominator = 2) 2 / 2 (100%) |
| Ultrasound Image Provided | 5 (27.8%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



