Submitted:
23 January 2026
Posted:
26 January 2026
You are already at the latest version
Abstract
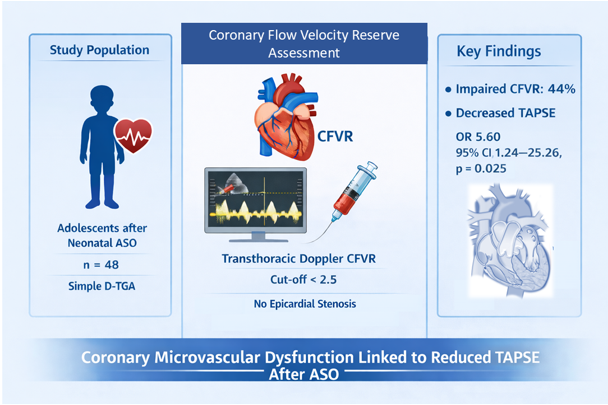
Background/Objectives: We assessed the prevalence of impaired coronary flow veloc-ity reserve (CFVR) and aimed to identify echocardiographic and clinical predictors of coronary microvascular dysfunction in adolescents after neonatal arterial switch op-eration (ASO). Methods: This single-center, cross-sectional study included patients that underwent neonatal ASO for simple D-transposition of the great arteries (D-TGA) during 1998-2013. All patients were evaluated by echocardiography with global left ventricu-lar strain measurement (GLS) and cardiac catheterization, including coronary angi-ography. Coronary flow velocity reserve was assessed by transthoracic Doppler echo-cardiography in the left anterior descending artery (LAD) using adenosine induced hyperemia. Patients were stratified into two groups according to CFVR: group with impaired CFVR (< 2.5) and group with normal CFVR (≥2.5). Spearman correlation was used to assess relationship between CFVR and echocardiographic variables. Binary lo-gistic regression was used to determine independent predictors of impaired CFVR. Results: Out of 48 patients included (median age 16 years, age range 13 to 23 years, 71% male), impaired CFVR was found in 21 patients (44%). These patients had de-creased longitudinal tricuspid annular plane systolic excursion (TAPSE), greater Z-scores for left ventricular end-systolic dimensions and higher mean pulmonary ar-tery pressures (mPAP). CFVR showed modest but significant positive correlations with tricuspid annular plane systolic excursion (TAPSE). Left pulmonary artery branch ste-nosis, reduced TAPSE and mPAP≥ 20 mmHg, were significantly associated with im-paired CFVR, while decreased TAPSE remained independent predictor in multivaria-ble analysis (odds ratio 5.6, 95% confidence interval 1.24-25.26, p=0.025). Conclusions: Impaired CFVR is highly prevalent in adolescents after neonatal ASO. Importantly, impaired CFVR is associated with right ventricular dysfunction.
Keywords:
coronary flow velocity reserve
; D- transposition of the great arteries
; arterial switch operation
; adolescents
; long-term follow-up
1. Introduction
Dextro-transposition of the great arteries (D-TGA) is the most common cyanotic congenital heart disease in the neonatal period, accounting for 5–7% of all congenital heart defects and about one-third of conotruncal anomalies [1,2]. The arterial switch operation, since its introduction in 1976. by Adib Jatene, has become the standard surgical approach for D-TGA in most developed countries, offering excellent long-term outcomes, with survival rates of 93-97%, and operative mortality of 3-5% [3,4,5]. Consequently, an increasing number of patients are reaching adolescence and adulthood, shifting the focus from survival to long-term follow-up, identification and management of late sequalae.
Among the most relevant concerns during long-term follow-up after ASO are coronary complications [6,7,8,9]. Although coronary arteries transfer can be successfully performed in all anatomical variants, somatic growth along with remodeling of the great arteries may predispose coronary arteries to kinking, compression, or scarring at reimplantation sites [7]. The incidence of late coronary obstruction is estimated at 3-8%. Furthermore, substantial number of cases remains clinically silent, due to inevitable myocardial denervation and consequential masking of the ischemic symptoms [4,6,7,8,9].
Contemporary guidelines recommend both multi-slice computed tomography (MSCT) coronary angiography as well as selective coronary angiography as a standard diagnostic tools for evaluation of coronary artery stenosis in presence of electrocardiographic (ECG) or echocardiographic signs of myocardial ischemia, or in the presence of complex coronary anatomy [6]. While both methods demonstrate high sensitivity and specificity for detecting lesions in the large epicardial vessels, they provide little information on the coronary microcirculation and microvascular function. Cardiac magnetic resonance (CMR) perfusion imaging has been utilized as a non-invasive tool with good results in pediatric and young adult populations, though its use remains limited by restricted availability [10,11].
Given these limitations, there is a growing need for reliable functional assessment of coronary circulation beyond the epicardial vessels. Coronary arterioles and capillary vessels comprise nearly 75% of entire coronary circulatory bed [12]. Coronary flow velocity reserve (CFVR), measured non-invasively by transthoracic Doppler echocardiography in the left anterior descending artery during pharmacologic hyperemia, provides valuable insight into coronary microvascular function [12,13]. Unlike MSCT or conventional angiography, which primarily evaluate large-vessel anatomy, CFVR reflects the integrity of the microcirculatory bed and has emerged as a sensitive marker of early coronary dysfunction. However, data on CFVR in patients after ASO remain scarce, particularly in adolescents and young adults, despite their increasing clinical relevance [14].
Therefore, we sought to evaluate the prevalence of impaired coronary flow velocity reserve in adolescents after ASO and to identify clinical and echocardiographic predictors of coronary microvascular dysfunction in this population.
2. Materials and Methods
2.1. Study design and population
This was a single-center, cross-sectional, observational cohort study, which included cohort of patients who previously underwent neonatal ASO for simple D-TGA in Cardiac surgery department at University Children’s Hospital in Belgrade, Serbia, between 1998. and 2013. The patient data regarding ASO were retrieved from electronic database of Cardiac surgery department.
2.2. Exclusion and inclusion criteria
Patients selected have met the following criteria: 1) neonatal ASO for simple D-TGA, 2) Age at follow-up ≥12 years, 3) asymptomatic at the time of inclusion. Exclusion criteria were as follows: 1) complex D-TGA, 2) surgical technique other than ASO for treatment of D-TGA, 3) previous catheter and/or surgical reintervention after neonatal ASO, 4) known coronary artery complications in the follow-up. Complex D-TGA was defined as D-TGA associated with ventricular septal defect (VSD), left ventricular outflow tract obstruction (LVOTO), coarctation of the aorta (CoAo), interrupted aortic arch, or other significant intracardiac anomalies. This study has been conducted in concordance with the Declaration of the Helsinki. Prior to initiation of the study, University Children’s Hospital Ethics Committee provided approval (reference no. 017/02, approval date: 02.12.2019.).
2.3. Baseline clinical assessment
All patients have been operated by ASO for simple D-TGA at neonatal age. At the time of evaluation, demographic characteristics, detailed previous medical history and physical examination including anthropometrics has been recorded. N-terminal pro-B-type natriuretic peptide (NTproBNP) levels were measured at admission (ECLIA, Roche diagnostics, Basel, Switzerland), and Zlog value was calculated according to age [15]. Standard 12-lead electrocardiogram (ECG) and chest X-ray were performed for every patient at admission. Additionally, prior to or after hospitalization, all patients underwent a 24-hour ECG Holter monitoring and standardized exercise stress test following modified Bruce protocol in order to exclude arrhythmia or exercise induced myocardial ischemia [16].
2.4. Echocardiographic assessment
Standard two-dimensional (2D) and Doppler transthoracic echocardiography was performed in all patients at admission, using a standardized imaging protocol in accordance with contemporary pediatric and adult congenital echocardiography guidelines [10,16]. All studies were conducted by experienced pediatric cardiologist using Vivid E95 ultrasound system (GE Healthcare). All measurements represent the average of three consecutive cardiac cycles. Images were acquired by standard two-dimensional, M-mode, Doppler techniques in subcostal, apical, parasternal and suprasternal views with ECG gating. Measurements included left ventricular end-diastolic (LVEDD), end-systolic diameters (LVESD), interventricular septal and posterior wall thickness, left atrial end-systolic diameter. Atrioventricular valves were measured from 4-chamber apical view and were assessed by color Doppler techniques. Morphometric analysis of the neoaorta and neopulmonary artery was performed from parasternal long-axis view [17]. Acquired dimensions were standardized using the corresponding Z-scores. Neoartic and neopulmonary stenosis or dilation was determined as a Z score ≥2, respectively [18]. Left ventricular systolic function was assessed by linear measurement of shortening fraction (SF) in parasternal short-axis M-mode, mitral annular plane systolic excursion (MAPSE) and volumetric measurement of ejection fraction (LVEF) via modified biplane Simpson method. Right ventricular function was assessed by tricuspid annular plane systolic excursion (TAPSE), measured by M-mode at the tricuspid valve free wall annulus from 4-chamber, apical view [17,19]. Right ventricular systolic pressure was assessed from the peak tricuspid valve regurgitation velocity, calculated by modified Bernoulli equation, with addition of estimated right atrial pressure. Elevated right ventricular systolic pressure (RVSP) was defined as > 35 mmHg [19,20,21,22]. Early (E) and late (A) diastolic mitral and tricuspid inflow velocities were measured using pulsed-wave Doppler at the level of the mitral and tricuspid leaflet tips, respectively, in accordance with published pediatric normative data [23,24].
2.5. Left ventricular global longitudinal strain (GLS) analysis
In addition to standard 2D echocardiographic assessment, all patient underwent left ventricular global longitudinal strain (GLS) assessment in concordance with contemporary guidelines [17,25,26,27]. Two-dimensional speckle tracking echocardiography (2D-STE) was used for left ventricular deformation analysis. Minimum three consecutive cardiac cycles, with ECG gating were recorded and stored in cine-loop format, with frame rates of 70 to 90 Hz [25]. The acquisitions were performed in apical 3-chamber (or long-axis), 4- chamber and 2-chamber views, with clear visualization and manual tracing of endocardial borders in the end-systolic frame. Aortic valve closure timing was automated and verified manually by experienced echocardiographer. Then, GLS was calculated offline using vendor specific software (EchoPAC, version 201, GE Healthcare); endocardial borders were manually traced at end-systole, after which automated speckle-tracking was performed with manual adjustments when needed to optimize segmental tracking. Left ventricle was divided into six segments in each view, and GLS was obtained as the average longitudinal strain from all segments and reported as an absolute value (%) [25,27]. Normal GLS was determined according to contemporary pediatric normative values [26,28].
2.6. Coronary flow velocity reserve assessment
Coronary flow velocity reserve was assessed non-invasively, by transthoracic Doppler echocardiography. A special preset for coronary flow velocity assessment was provided by the vendor, on a 4 MHz transducer. Color Doppler flow map was optimized, by setting the Nyquist limit to 16-24 cm/s. The distal segment of left anterior descending coronary artery (LAD) was visualized in a modified apical 4-chamber view, and rotated until coronary artery flow was identified by color Doppler. Pulsed wave Doppler imaging was then applied with a 3 to 5 mm sample volume, ensuring the ultrasound beam was aligned as parallel as possible to coronary flow, and as stable as possible during measurements. Peak diastolic flow velocity was measured at baseline and during pharmacologically induced hyperemia. Maximum hyperemia was achieved by intravenous adenosine infusion at 140 µg/kg/min for 2 minutes, with continuous ECG and blood pressure monitoring. CFVR was calculated as the ratio of hyperemic to resting peak diastolic flow velocity [29,30,31]. Patients with CFVR <2.5 were defined as those with impaired coronary flow reserve [31,32].
2.7. Cardiac catheterization
All patients in the cohort underwent diagnostic cardiac catheterization, according to the standardized protocol for adolescent patients after ASO during long-term follow-up at our institution [6]. The procedure was performed in accordance with contemporary international expert consensus recommendations for cardiac catheterization in congenital heart disease, including standards for anatomic imaging, hemodynamic assessment, and radiation-safety practice [34]. Catheterizations were performed via transfemoral arterial and venous approach, respectively. After vascular access was obtained, a left sided cardiac catheterization was performed. Aortography was carried out to visualize supravalvular stenosis or dilation of the aorta. Coronary angiography was done in all patients to exclude significant epicardial coronary artery stenosis, which was defined as ≥50% of luminal narrowing in any major epicardial artery [35]. Subsequently, right-sided catheterization, with right ventriculography and pulmonary angiography was performed to assess the position and potential stenosis of the pulmonary artery branches after LeCompte maneuver. Direct hemodynamic pressures were recorded as the mean of three consecutive measurement in the aorta, left ventricle, right atrium, right ventricle, pulmonary artery and pulmonary artery branches. Pulmonary artery branch stenosis was defined as ≥30% luminal diameter reduction on angiography and/or a systolic pressure gradient ≥20 mmHg across the stenotic segment, according to contemporary guidelines [36].
2.8. Statistical analysis
Statistical analysis was performed using SPSS Statistics version 23 (SPSS, Chicago, IL, USA). A two-sided p value <0.05 was considered statistically significant. Descriptive data were expressed as means with standard deviation for continuous variables, and as count with percentage for categorical variables. The normality of the data was assessed by Shapiro Wilk test. Differences between continuous variables were compared using Student’s T-test or Mann-Whitney U test, according to data distribution, while χ2 test was used for categorical variables. Associations between coronary flow velocity reserve (CFVR) and clinical, echocardiographic, and invasive hemodynamic parameters were explored using Spearman rank correlation analysis. To identify predictors of impaired CFVR, binary logistic regression analysis was performed. In the univariable model, impaired CFVR was entered as the dependent variable and tested against individual explanatory variables, including demographic characteristics, perioperative parameters, long-term postoperative sequelae, echocardiographic measures, NT-proBNP levels, and catheterization findings. Variables demonstrating statistical significance in univariable analysis (p < 0.05) were subsequently entered into a multivariable logistic regression model to identify independent predictors of impaired CFVR.
3. Results
3.1. Study population and baseline characteristics
During period from 1998. to 2013. a total of 93 patients were treated for D-TGA at University Children’s Hospital. After exclusion, 48 patients who underwent ASO for simple D-TGA at neonatal age were included in the study (Figure 1). Baseline characteristics of the cohort is presented in Table 1. The mean age was 16.0±2.8 and patients were predominantly male (71%). Mean age at the time of surgery was 19±10 days, and D-TGA was prenatally recognized in 15% of patients. The majority of patients received continous intravenous prostaglandin E1 (PGE1) infusion prior to surgery, and balloon atrial septostomy (the Rahskind procedure) has been performed in 85% of the patients prior to surgery. There was no statistically significant differences between groups with preserved and impaired CFVR in regard to sex, age, NTproBNP levels, and pre-,intraoperative and postoperative parameters.
3.2. Echocardiographic parameters and coronary flow velocity reserve
Echocardiographic findings for the entire cohort, as well as groups with preserved and impaired CFVR are summarized in Table 2. All patients underwent successful CFVR measurement. Impaired CFVR was identified in 21 patients (44%), while 27 patients (56%) demonstrated preserved CFVR.
All patients had preserved LVEF. However, reduced longitudinal systolic indices were frequently observed: MAPSE and TAPSE were reduced in almost 30% and 44% of patients, respectively. Left ventricular GLS values were below age-adjusted reference limits in approximately one third of the cohort. Neoaortic root dilation was present in 79% of patients.
When comparing patients with impaired and preserved CFVR, those with preserved CFVR showed significantly higher left ventricular end-systolic Z scores; conversely, the group with impaired CFVR had significantly lower values of TAPSE (p<0.05). There was no statistically significant difference between groups regarding LVEF, SF, cardiac dimensions with corresponding Z-scores, and GLS values.
3.3. Catheterization findings
Invasive hemodynamic assessment and cardiac catheterization findings are presented in Table 3. No patients had significant epicardial coronary stenosis. Mean pulmonary artery pressure was significantly higher in patients with impaired CFVR compared to those with preserved CFVR (p<0.05). Furthermore, left pulmonary artery branch stenosis was more frequent in the impaired CFVR group (p=0.051). There were no statistically significant differences between in other pressure measurements between groups.
3.4. Correlation analysis and binary logistic regression
Spearman correlation demonstrated modest, but statistically significant positive correlation between TAPSE and CFVR (r=0.35, p=0.016). Correlation scatter plot is presented in Figure 2. When analyzing other variables, there was no statistically significant correlation with CFVR.
To identify independent predictors of reduced CFVR, binary logistic regression was performed. In univariable analysis, left pulmonary artery branch stenosis (odds ratio (OR) 5.92, 95% confidence interval (CI) 1.06-32.89, p= 0.042), reduced TAPSE (OR 3.86, 95% CI 1.15-12.91, p=0.028) and mPAP≥ 20 mmHg (OR 3.64, 95% CI 1.04-12.78, p=0.043), were significantly associated with impaired CFVR. In multivariable analysis, reduced TAPSE emerged as an independent predictor of impaired CFVR (OR 5.60, 95% CI 1.24–25.26, p = 0.025). Mean pulmonary artery pressure ≥20 mmHg and left pulmonary artery branch stenosis were associated with impaired CFVR in univariable analysis but did not retain independent significance after adjustment.
4. Discussion
In the present study, there are two main findings. The first finding reveals significant portion of patients with impaired coronary flow velocity reserve (44%), in a well characterized, contemporary cohort of adolescent patients after neonatal arterial switch operation for simple D-TGA, despite preserved epicardial coronary anatomy and global systolic function. Secondly, reduced CFVR was associated with indices of right ventricular dysfunction, and elevated pulmonary artery pressures, suggesting a potential link between right ventricular function and microvascular dysfunction in this group of patients.
Majority of previous studies have focused on anatomical epicardial coronary artery stenosis as a late sequalae after neonatal ASO, while functional microvascular impairment has received less attention [4,5,7,9]. To our knowledge, this is the largest cohort of patients with simple D-TGA treated with ASO at neonatal age assessed for coronary flow velocity reserve [14,37,38]. The observed prevalence of impaired CFVR in our cohort is notably higher, than in previous invasive Doppler and angiographic study by Oscarsson et al. [37]. This might be attributed to differences between invasive and non-invasive CFVR assessment. Likewise, studies by Gagliardi and Hauser, have confirmed significantly reduced CFVR in patients after coronary artery transfer, respectively [14,38]. These findings are similar to our results, and support the concept of abnormal coronary vasomotor response in D-TGA patients in the long-term follow-up after ASO, even in the absence of fixed epicardial coronary stenosis. Moreover, all patients in the present study were clinically asymptomatic, had preserved left ventricular ejection fraction and normal coronary angiograms. This underscores the limited sensitivity of conventional clinical and anatomical assessments in early detection of microvascular dysfunction in the post-ASO cohort.
There are several factors contributing to impaired CFVR after ASO. Of note, during ASO, surgical coronary transfer inevitably damages cardiac autonomic plexus, resulting in partial or complete coronary denervation. This leads to impaired vasomotor response and changes in coronary flow regulation [9,39]. Additionally, progressive somatic growth and spatial remodeling of the great vessels, may result in alterations in coronary geometry, as well as in stretching or kinking. These changes might not result in hemodynamically significant coronary stenosis, but may alter coronary flow dynamics [8]. Lastly, endothelial dysfunction as a part of innate disease might be involved, unlike in populations with history of complete heart denervation, such as in heart transplant patients [40,41]. Combined, these mechanisms may provide a possible explanation for the discrepancy between preserved epicardial coronary anatomy and impaired coronary microvascular function in significant portion of our cohort.
An important and novel observation in our study is the association between impaired CFVR and markers of right ventricular dysfunction, particularly reduced TAPSE, higher mean pulmonary artery pressures and higher frequency of left pulmonary artery branch stenosis. Although these variables did not all maintain independent significance in multivariable analysis, their association with impaired CFVR suggests a pathophysiological interplay between right ventricular performance, pulmonary artery pressure and coronary microvascular function.
Ventricular interdependence may present an important mechanistic link between right ventricular dysfunction and coronary microvascular function [42,43]. Increase in the right ventricular afterload leads to septal displacement and changes in left ventricular geometry, resulting in impaired diastolic filling and increased myocardial wall stress [44]. These factors may adversely affect coronary microvascular reserve, even in the absence of significant epicardial coronary stenosis. Furthermore, association of the right ventricular pressure overload and coronary microvascular dysfunction was demonstrated in previous studies, supporting this link [21,42,45].
In patients after ASO, a common sequela, occurring in up to 42% of patients in the long-term follow-up is pulmonary artery branch stenosis, following LeCompte maneuver [4,10,46]. Therefore, despite ASO restoring normal ventriculo-arterial connection, subtle changes of the right ventricular function and pulmonary circulation may persist. Although pulmonary artery branch stenosis did not remain an independent predictor in multivariable analysis, its association with impaired CFVR in univariable analysis suggests that chronic right ventricular pressure overload may contribute to coronary microvascular dysfunction. Importantly, right ventricular systolic function, assessed by TAPSE, emerged as the only independent predictor of impaired CFVR in multivariable analysis. This finding suggests that right ventricular performance may serve as an integrative marker of cardiopulmonary interaction and coronary microvascular function in this population.
Interestingly, although left ventricular GLS was reduced in approximately one third of the cohort, GLS values did not differ significantly between groups with impaired and preserved CFVR. Furthermore, we did not find statistically significant association between CFVR and GLS in our group of patients. Several adult studies have demonstrated a significant association between impaired coronary flow reserve and reduced left ventricular global longitudinal strain, suggesting that microvascular dysfunction may precede or accompany subtle systolic impairment detectable by deformation imaging. In contrast, other investigations have failed to identify a meaningful correlation between CFR and GLS, particularly in cohorts with preserved left ventricular ejection fraction and absence of overt ischemic heart disease [47,48,49]. Our findings indicate that subclinical left ventricular dysfunction may be present in adolescents after ASO, but it does not appear to be primary determinant of microvascular impairment at this stage of follow-up. In contrast, TAPSE demonstrated a closer relationship with CFVR, highlighting the dominant role of right-sided cardiopulmonary interactions in the pathophysiology of microvascular dysfunction in this population. Furthermore, these findings indicate that coronary microvascular dysfunction may precede or occur independently of overt left ventricular deformation abnormalities.
There are several limitations to our study. First of all, this is a single-center, cross-sectional study, with a relatively small number of patients, reducing the statistical power of the study and resulting in wide CIs, particularly for multivariable analysis. Second, coronary flow velocity reserve was assessed non-invasively by transthoracic Doppler echocardiography, rather than by invasive coronary flow measurements or positron emission tomography. Although transthoracic CFVR is a well-validated and widely used method, it remains operator-dependent and limited to assessment of the left anterior descending artery. Third, myocardial deformation analysis was limited to left ventricular global longitudinal strain, while advanced indices such as myocardial work were not assessed. Similarly, right ventricular strain parameters were not systematically analyzed and may have provided additional insights in this cohort.
In conclusion, in a contemporary cohort of adolescents after neonatal ASO for simple D-TGA, impaired coronary flow velocity reserve is highly prevalent, despite preserved epicardial coronary anatomy and global left ventricular systolic function. Importantly, impaired CFVR was associated with markers of right ventricular dysfunction and elevated pulmonary artery pressures, highlighting a potential interaction between pulmonary circulation, right ventricular performance, and coronary microvascular function. These findings suggest that coronary microvascular dysfunction represents an underrecognized component of late sequelae after ASO and may not be adequately detected by conventional anatomical or functional assessments. Comprehensive long-term follow-up strategies in post-ASO patients should therefore extend beyond epicardial coronary evaluation and include functional assessment of coronary microcirculation and right ventricular performance.
Author Contributions
Conceptualization: Andrija Pavlovic, Milorad Tesic and Vojislav Parezanovic; methodology: Andrija Pavlovic, Milorad Tesic, Milan Djukic, Igor Stefanovic, Jasna Kalanj; validation: Milorad Tesic, Milan Djukic and Vojislav Parezanovic; formal analysis Andrija Pavlovic, Milorad Tesic, Milica Kuzmanovic, Maja Bijelic, Dusan Andric, Dejan Bisenic; investigation: Andrija Pavlovic, Igor Stefanovic, Maja Trkulja, Vladimir Milovanovic, Dejan Bisenic, Irena Ostric Pavlovic.; resources: Andrija Pavlovic, Jasna Kalanj, Igor Stefanovic, Milica Kuzmanovic, Marko Pavlovic, Maja Bijelic, Maja Trkulja, Irena Ostric Pavlovic; data curation: Andrija Pavlovic, Milica Kuzmanovic, Dusan Andric, Maja Trkulja, Maja Bijelic, Dejan Bisenic, Irena Ostric Pavlovic; writing—original draft preparation, Andrija Pavlovic, Milorad Tesic, Dusan Andric, Milica Kuzmanovic; writing—review and editing Andrija Pavlovic, Milorad Tesic, Igor Stefanovic, Vojislav Parezanovic, Milan Djukic .; supervision: Milorad Tesic, Milan Djukic, Vladimir Milovanovic, Vojislav Parezanovic; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of University Children’s Hospital (protocol code reference no. 017/02, approval date: 02.12.2019.).
Informed Consent Statement
Informed consent was obtained from all subjects and/or parents/legal guardians involved in the study.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Acknowledgments
During the preparation of this manuscript, the authors used ChatGPT version 5.2 for the purposes of creating a graphical abstract. The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ASO | Arterial Switch Operation |
| BMI | Body Mass Index |
| BSA | Body Surface Area |
| CFVR | Coronary Flow Velocity Reserve |
| CI | Confidence Interval |
| CMR | Cardiac Magnetic Resonance |
| CoAo | Coarctation of the Aorta |
| D-TGA | Dextro-Transposition of the Great Arteries |
| ECG | Electrocardiogram |
| GLS | Global Longitudinal Strain |
| LAD | Left Anterior Descending (coronary artery) |
| LV | Left Ventricle/Left Ventricular |
| LVEDD | Left Ventricular End-Diastolic Diameter |
| LVESD | Left Ventricular End-Systolic Diameter |
| LVEF | Left Ventricular Ejection Fraction |
| LVOTO | Left Ventricular Outflow Tract Obstruction |
| MAP | Mean Arterial Pressure |
| MAPSE | Mitral Annular Plane Systolic Excursion |
| mPAP | Mean Pulmonary Artery Pressure |
| MSCT | Multislice Computed Tomography |
| NTproBNP | N-terminal pro-B-type Natriuretic Peptide |
| OR | Odds Ratio |
| PGE1 | Prostaglandin E1 |
| RA | Right Atrium |
| RV | Right Ventricle/Right Ventricular |
| RVSP | Right Ventricular Systolic Pressure |
| SF | Shortening Fraction |
| STE | Speckle Tracking Echocardiography |
| TAPSE | Tricuspid Annular Plane Systolic Excursion |
| TV | Tricuspid Valve |
| VSD | Ventricular Septal Defect |
References
- Martins, P; Castela, E. Transposition of the great arteries. Orphanet J Rare Dis 2008, 3, 27. [Google Scholar] [CrossRef]
- Walter, CC; Escobar-Diaz, MC; Cesar, S; Garrido, BAM; Sanchez-de-Toledo, J. Functional and morphometric changes in children after neonatal arterial switch operation for transposition of the great arteries. Ann Pediatr Cardiol 2022, 15(5-6), 447–452. [Google Scholar] [CrossRef] [PubMed]
- Jatene, AD; Fontes, VF; Paulista, PP; Souza, LC; Neger, F; Galantier, M; Sousa, JE. Anatomic correction of transposition of the great vessels. J Thorac Cardiovasc Surg. 1976, 72(3), 364–70. [Google Scholar] [CrossRef] [PubMed]
- Dorobantu, DM; Espuny Pujol, F; Kostolny, M; Brown, KL; Franklin, RC; Crowe, S; Pagel, C; Stoica, SC. Arterial Switch for Transposition of the Great Arteries: Treatment Timing, Late Outcomes, and Risk Factors. JACC Adv. 2023, 2(5), 100407. [Google Scholar] [CrossRef]
- Morfaw, F; Leenus, A; Mbuagbaw, L; Anderson, LN; Dillenburg, R; Thabane, L. Outcomes after corrective surgery for congenital dextro-transposition of the arteries using the arterial switch technique: a scoping systematic review. Syst Rev. 2020, 9(1), 231. [Google Scholar] [CrossRef]
- Sarris, GE; Balmer, C; Bonou, P; Comas, JV; da Cruz, E; Chiara, LD; Di Donato, RM; Fragata, J; Jokinen, TE; Kirvassilis, G; Lytrivi, I; Milojevic, M; Sharland, G; Siepe, M; Stein, J; Büchel, EV; Vouhé, PR. Clinical guidelines for the management of patients with transposition of the great arteries with intact ventricular septum. Eur J Cardiothorac Surg 2017, 51(1), e1–e32. [Google Scholar] [CrossRef]
- Linglart, L; Malekzadeh-Milani, S; Gaudin, R; Raisky, O; Bonnet, D. Outcomes of coronary artery obstructions after the arterial switch operation for transposition of the great arteries. J Thorac Cardiovasc Surg. 2024, 168(2), 331–341.e4. [Google Scholar] [CrossRef] [PubMed]
- Ou, P; Khraiche, D; Celermajer, DS; Agnoletti, G; Le Quan Sang, KH; Thalabard, JC; Quintin, M; Raisky, O; Vouhe, P; Sidi, D; Bonnet, D. Mechanisms of coronary complications after the arterial switch for transposition of the great arteries. J Thorac Cardiovasc Surg. 2013, 145(5), 1263–9. [Google Scholar] [CrossRef]
- Lim, RS; Lefkovits, J; Menahem, S. Long-Term Coronary Artery Complications Following the Arterial Switch Operation for Transposition of the Great Arteries-A Scoping Review. World J Pediatr Congenit Heart Surg 2025, 16(3), 402–408. [Google Scholar] [CrossRef]
- Cohen, MS; Eidem, BW; Cetta, F; Fogel, MA; Frommelt, PC; Ganame, J; Han, BK; Kimball, TR; Johnson, RK; Mertens, L; Paridon, SM; Powell, AJ; Lopez, L. Multimodality Imaging Guidelines of Patients with Transposition of the Great Arteries: A Report from the American Society of Echocardiography Developed in Collaboration with the Society for Cardiovascular Magnetic Resonance and the Society of Cardiovascular Computed Tomography. J Am Soc Echocardiogr. 2016, 29(7), 571–621. [Google Scholar] [CrossRef]
- Noel, CV; Krishnamurthy, R; Masand, P; Moffett, B; Schlingmann, T; Cheong, BY; Krishnamurthy, R. Myocardial Stress Perfusion MRI: Experience in Pediatric and Young-Adult Patients Following Arterial Switch Operation Utilizing Regadenoson. Pediatr Cardiol 2018, 39(6), 1249–1257. [Google Scholar] [CrossRef] [PubMed]
- Del Buono, MG; Montone, RA; Camilli, M; Carbone, S; Narula, J; Lavie, CJ; Niccoli, G; Crea, F. Coronary Microvascular Dysfunction Across the Spectrum of Cardiovascular Diseases: JACC State-of-the-Art Review. J Am Coll Cardiol. 2021, 78(13), 1352–1371. [Google Scholar] [CrossRef]
- Taqueti, VR; Di Carli, MF. Coronary Microvascular Disease Pathogenic Mechanisms and Therapeutic Options: JACC State-of-the-Art Review. J Am Coll Cardiol. 2018, 72(21), 2625–2641. [Google Scholar] [CrossRef]
- Gagliardi, MG; Adorisio, R; Crea, F; Versacci, P; Di Donato, R; Sanders, SP. Abnormal vasomotor function of the epicardial coronary arteries in children five to eight years after arterial switch operation: an angiographic and intracoronary Doppler flow wire study. J Am Coll Cardiol. 2005, 46(8), 1565–72. [Google Scholar] [CrossRef]
- Palm, J; Hoffmann, G; Klawonn, F; Tutarel, O; Palm, H; Holdenrieder, S; Ewert, P. Continuous, complete and comparable NT-proBNP reference ranges in healthy children. Clin Chem Lab Med. 2020, 58(9), 1509–1516. [Google Scholar] [CrossRef] [PubMed]
- Paridon, SM; Alpert, BS; Boas, SR; Cabrera, ME; Caldarera, LL; Daniels, SR; Kimball, TR; Knilans, TK; Nixon, PA; Rhodes, J; Yetman, AT. American Heart Association Council on Cardiovascular Disease in the Young, Committee on Atherosclerosis, Hypertension, and Obesity in Youth. Clinical stress testing in the pediatric age group: a statement from the American Heart Association Council on Cardiovascular Disease in the Young, Committee on Atherosclerosis, Hypertension, and Obesity in Youth. Circulation 2006, 113(15), 1905–20. [Google Scholar] [CrossRef] [PubMed]
- Lopez, L; Saurers, DL; Barker, PCA; Cohen, MS; Colan, SD; Dwyer, J; Forsha, D; Friedberg, MK; Lai, WW; Printz, BF; Sachdeva, R; Soni-Patel, NR; Truong, DT; Young, LT; Altman, CA. Guidelines for Performing a Comprehensive Pediatric Transthoracic Echocardiogram: Recommendations From the American Society of Echocardiography. J Am Soc Echocardiogr. 2024, 37(2), 119–170. [Google Scholar] [CrossRef]
- Pettersen, MD; Du, W; Skeens, ME; Humes, RA. Regression equations for calculation of z scores of cardiac structures in a large cohort of healthy infants, children, and adolescents: an echocardiographic study. J Am Soc Echocardiogr. 2008, 21(8), 922–34. [Google Scholar] [CrossRef]
- Mah, K; Mertens, L. Echocardiographic Assessment of Right Ventricular Function in Paediatric Heart Disease: A Practical Clinical Approach. CJC Pediatr Congenit Heart Dis 2022, 1(3), 136–157. [Google Scholar] [CrossRef]
- Lammers, AE; Apitz, C; Michel-Behnke, I; Koestenberger, M. A guide to echocardiographic assessment in children and adolescents with pulmonary hypertension. Cardiovasc Diagn Ther 2021, 11(4), 1160–1177. [Google Scholar] [CrossRef]
- Huston, JH; Maron, BA; French, J; Huang, S; Thayer, T; Farber-Eger, EH; Wells, QS; Choudhary, G; Hemnes, AR; Brittain, EL. Association of Mild Echocardiographic Pulmonary Hypertension With Mortality and Right Ventricular Function. JAMA Cardiol 2019, 4(11), 1112–1121. [Google Scholar] [CrossRef]
- Wu, VC; Takeuchi, M. Echocardiographic assessment of right ventricular systolic function. Cardiovasc Diagn Ther. 2018, 8(1), 70–79. [Google Scholar] [CrossRef]
- Cantinotti, M; Marchese, P; Scalese, M; Franchi, E; Assanta, N; Koestenberger, M; Van den Eynde, J; Kutty, S; Giordano, R. Normal Values and Patterns of Normality and Physiological Variability of Mitral and Tricuspid Inflow Pulsed Doppler in Healthy Children. Healthcare (Basel) 2022, 10(2), 355. [Google Scholar] [CrossRef]
- Cantinotti, M; Giordano, R; Scalese, M; Murzi, B; Assanta, N; Spadoni, I; Crocetti, M; Marotta, M; Molinaro, S; Kutty, S; Iervasi, G. Nomograms for mitral inflow Doppler and tissue Doppler velocities in Caucasian children. J Cardiol. 2016, 68(4), 288–99. [Google Scholar] [CrossRef] [PubMed]
- Voigt, JU; Pedrizzetti, G; Lysyansky, P; Marwick, TH; Houle, H; Baumann, R; Pedri, S; Ito, Y; Abe, Y; Metz, S; Song, JH; Hamilton, J; Sengupta, PP; Kolias, TJ; d'Hooge, J; Aurigemma, GP; Thomas, JD; Badano, LP. Definitions for a common standard for 2D speckle tracking echocardiography: consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur Heart J Cardiovasc Imaging 2015, 16(1), 1–11. [Google Scholar] [CrossRef] [PubMed]
- Marcus, KA; Mavinkurve-Groothuis, AM; Barends, M; van Dijk, A; Feuth, T; de Korte, C; Kapusta, L. Reference values for myocardial two-dimensional strain echocardiography in a healthy pediatric and young adult cohort. J Am Soc Echocardiogr. 2011, 24(6), 625–36. [Google Scholar] [CrossRef]
- Mihos, CG; Liu, JE; Anderson, KM; Pernetz, MA; O'Driscoll, JM; Aurigemma, GP; Ujueta, F; Wessly, P. American Heart Association Council on Peripheral Vascular Disease; Council on Cardiovascular and Stroke Nursing; and Council on Clinical Cardiology. Speckle-Tracking Strain Echocardiography for the Assessment of Left Ventricular Structure and Function: A Scientific Statement From the American Heart Association. Circulation 2025, 152(10), e96–e109. [Google Scholar] [CrossRef] [PubMed]
- Cantinotti, M; Scalese, M; Giordano, R; Franchi, E; Assanta, N; Marotta, M; Viacava, C; Molinaro, S; Iervasi, G; Santoro, G; Koestenberger, M. Normative Data for Left and Right Ventricular Systolic Strain in Healthy Caucasian Italian Children by Two-Dimensional Speckle-Tracking Echocardiography. J Am Soc Echocardiogr. 2018, 31(6), 712–720.e6. [Google Scholar] [CrossRef]
- Tesic, M; Beleslin, B; Giga, V; Jovanovic, I; Marinkovic, J; Trifunovic, D; Petrovic, O; Dobric, M; Aleksandric, S; Juricic, S; Boskovic, N; Tomasevic, M; Ristic, A; Orlic, D; Stojkovic, S; Vukcevic, V; Stankovic, G; Ostojic, M; Djordjevic Dikic, A. Prognostic Value of Transthoracic Doppler Echocardiography Coronary Flow Velocity Reserve in Patients With Asymmetric Hypertrophic Cardiomyopathy. J Am Heart Assoc. 2021, 10(20), e021936. [Google Scholar] [CrossRef]
- Tesic, M; Djordjevic-Dikic, A; Giga, V; Stepanovic, J; Dobric, M; Jovanovic, I; Petrovic, M; Mehmedbegovic, Z; Milasinovic, D; Dedovic, V; Zivkovic, M; Juricic, S; Orlic, D; Stojkovic, S; Vukcevic, V; Stankovic, G; Nedeljkovic, M; Ostojic, M; Beleslin, B. Prognostic Value of Transthoracic Doppler Echocardiography Coronary Flow Velocity Reserve in Patients with Nonculprit Stenosis of Intermediate Severity Early after Primary Percutaneous Coronary Intervention. J Am Soc Echocardiogr. 2018, 31(8), 880–887. [Google Scholar] [CrossRef]
- Toya, T; Corban, MT; Park, JY; Ahmad, A; Ӧzcan, I; Sebaali, F; Sara, JDS; Gulati, R; Lerman, LO; Lerman, A. Prognostic impact and clinical outcomes of coronary flow reserve and hyperaemic microvascular resistance. EuroIntervention 2021, 17(7), 569–575. [Google Scholar] [CrossRef]
- Kawata, T; Daimon, M; Hasegawa, R; Toyoda, T; Sekine, T; Himi, T; Uchida, D; Miyazaki, S; Hirose, K; Ichikawa, R; Maruyama, M; Suzuki, H; Daida, H. Prognostic value of coronary flow reserve assessed by transthoracic Doppler echocardiography on long-term outcome in asymptomatic patients with type 2 diabetes without overt coronary artery disease. Cardiovasc Diabetol 2013, 12, 121. [Google Scholar] [CrossRef]
- Moscatelli, S; Bianco, F; Cimini, A; Panebianco, M; Leo, I; Bucciarelli-Ducci, C; Perrone, MA. The Use of Stress Cardiovascular Imaging in Pediatric Population. Children (Basel) 2023, 10(2), 218. [Google Scholar] [CrossRef]
- Holzer, RJ; Bergersen, L; Thomson, J; Aboulhosn, J; Aggarwal, V; Akagi, T; Alwi, M; Armstrong, AK; Bacha, E; Benson, L; Bökenkamp, R; Carminati, M; Dalvi, B; DiNardo, J; Fagan, T; Fetterly, K; Ing, FF; Kenny, D; Kim, D; Kish, E; O'Byrne, M; O'Donnell, C; Pan, X; Paolillo, J; Pedra, C; Peirone, A; Singh, HS; Søndergaard, L; Hijazi, ZM. PICS/AEPC/APPCS/CSANZ/SCAI/SOLACI: Expert Consensus Statement on Cardiac Catheterization for Pediatric Patients and Adults With Congenital Heart Disease. JACC Cardiovasc Interv. 2024, 17(2), 115–216. [Google Scholar] [CrossRef] [PubMed]
- Vrints, C; Andreotti, F; Koskinas, KC; Rossello, X; Adamo, M; Ainslie, J; Banning, AP; Budaj, A; Buechel, RR; Chiariello, GA; Chieffo, A; Christodorescu, RM; Deaton, C; Doenst, T; Jones, HW; Kunadian, V; Mehilli, J; Milojevic, M; Piek, JJ; Pugliese, F; Rubboli, A; Semb, AG; Senior, R; Ten Berg, JM; Van Belle, E; Van Craenenbroeck, EM; Vidal-Perez, R; Winther, S; ESC Scientific Document Group. 2024 ESC Guidelines for the management of chronic coronary syndromes. Eur Heart J 2024, 45(36), 3415–3537. [Google Scholar] [CrossRef]
- Villafañe, J; Lantin-Hermoso, MR; Bhatt, AB; Tweddell, JS; Geva, T; Nathan, M; Elliott, MJ; Vetter, VL; Paridon, SM; Kochilas, L; Jenkins, KJ; Beekman, RH, 3rd; Wernovsky, G; Towbin, JA; American College of Cardiology’s Adult Congenital and Pediatric Cardiology Council. D-transposition of the great arteries: the current era of the arterial switch operation. J Am Coll Cardiol. 2014, 64(5), 498–511. [Google Scholar] [CrossRef] [PubMed]
- Oskarsson, G; Pesonen, E; Munkhammar, P; Sandström, S; Jögi, P. Normal coronary flow reserve after arterial switch operation for transposition of the great arteries: an intracoronary Doppler guidewire study. Circulation 2002, 106(13), 1696–702. [Google Scholar] [CrossRef]
- Hauser, M; Bengel, FM; Kühn, A; Sauer, U; Zylla, S; Braun, SL; Nekolla, SG; Oberhoffer, R; Lange, R; Schwaiger, M; Hess, J. Myocardial blood flow and flow reserve after coronary reimplantation in patients after arterial switch and ross operation. Circulation 2001, 103(14), 1875–80. [Google Scholar] [CrossRef]
- Engele, LJ; van der Palen, RLF; Egorova, AD; Bartelings, MM; Wisse, LJ; Glashan, CA; Kiès, P; Vliegen, HW; Hazekamp, MG; Mulder, BJM; Ruiter, MC; Bouma, BJ; Jongbloed, MRM. Cardiac Fibrosis and Innervation State in Uncorrected and Corrected Transposition of the Great Arteries: A Postmortem Histological Analysis and Systematic Review. J Cardiovasc Dev Dis. 2023, 10(4), 180. [Google Scholar] [CrossRef]
- Possner, M; Buechel, RR; Vontobel, J; Mikulicic, F; Gräni, C; Benz, DC; Clerc, OF; Fuchs, TA; Tobler, D; Stambach, D; Greutmann, M; Kaufmann, PA. Myocardial blood flow and cardiac sympathetic innervation in young adults late after arterial switch.
- operation for transposition of the great arteries. Int J Cardiol 2020, 299, 110–115. [CrossRef]
- Di Carli, MF; Tobes, MC; Mangner, T; Levine, AB; Muzik, O; Chakroborty, P; Levine, TB. Effects of cardiac sympathetic innervation on coronary blood flow. N Engl J Med 1997, 336(17), 1208–15. [Google Scholar] [CrossRef]
- Mahfouz, RA; Gouda, M; Arab, M. Right ventricular mechanics and exercise capacity in patients with microvascular angina: The impact of microvascular function. Echocardiography 2020, 37(1), 71–76. [Google Scholar] [CrossRef]
- Friedberg, MK. Imaging Right-Left Ventricular Interactions. JACC Cardiovasc Imaging 2018, 11(5), 755–771. [Google Scholar] [CrossRef]
- Yang, F; Ren, W; Wang, D; Yan, Y; Deng, YL; Yang, ZW; Yu, TL; Li, D; Zhang, Z. The Variation in the Diastolic Period with Interventricular Septal Displacement and Its Relation to the Right Ventricular Function in Pulmonary Hypertension: A Preliminary Cardiac Magnetic Resonance Study. Diagnostics (Basel) 2022, 12(8), 1970. [Google Scholar] [CrossRef]
- Essafri, I; Ichimura, K; Ivy, D; Stenmark, KR; Turton, HA; Pyle, LL; Spiekerkoetter, E; Kheyfets, VO. The effect of microvascular remodeling on fluid dynamics in the pressure-overloaded right ventricle. Am J Physiol Heart Circ Physiol. 2025, 329(5), H1379–H1390. [Google Scholar] [CrossRef]
- Luo, S; Haranal, M; Deng, MX; Varenbut, J; Runeckles, K; Steve Fan, CP; Van Arsdell, GS; Haller, C; Honjo, O. Branch pulmonary artery stenosis after arterial switch operation: The effect of preoperative anatomic factors on reintervention. J Thorac Cardiovasc Surg. 2022, 164(2), 317–327.e8. [Google Scholar] [CrossRef]
- Jovanovic, I; Tesic, M; Giga, V; Dobric, M; Boskovic, N; Vratonjic, J; Orlic, D; Gudelj, O; Tomasevic, M; Dikic, M; Nedeljkovic, I; Trifunovic, D; Nedeljkovic, MA; Dedic, S; Beleslin, B; Djordjevic-Dikic, A. Impairment of coronary flow velocity reserve and global longitudinal strain in women with cardiac syndrome X and slow coronary flow. J Cardiol. 2020, 76(1), 1–8. [Google Scholar] [CrossRef]
- Clemmensen, TS; Løgstrup, BB; Eiskjaer, H; Poulsen, SH. Coronary Flow Reserve Predicts Longitudinal Myocardial Deformation Capacity in Heart-Transplanted Patients. Echocardiography 2016, 33(4), 562–71. [Google Scholar] [CrossRef]
- Li, Y; Sun, D; Zhao, H; Qin, Z; Ji, W; Zhang, H; Jiao, N; Luan, B; Ding, M; Zhu, F. Incremental value of non-invasive myocardial work for the evaluation and prediction of coronary microvascular dysfunction in angina with no obstructive coronary artery disease. Front Cardiovasc Med. 2023, 10, 1209122. [Google Scholar] [CrossRef]
Figure 1.
Study flow-chart.
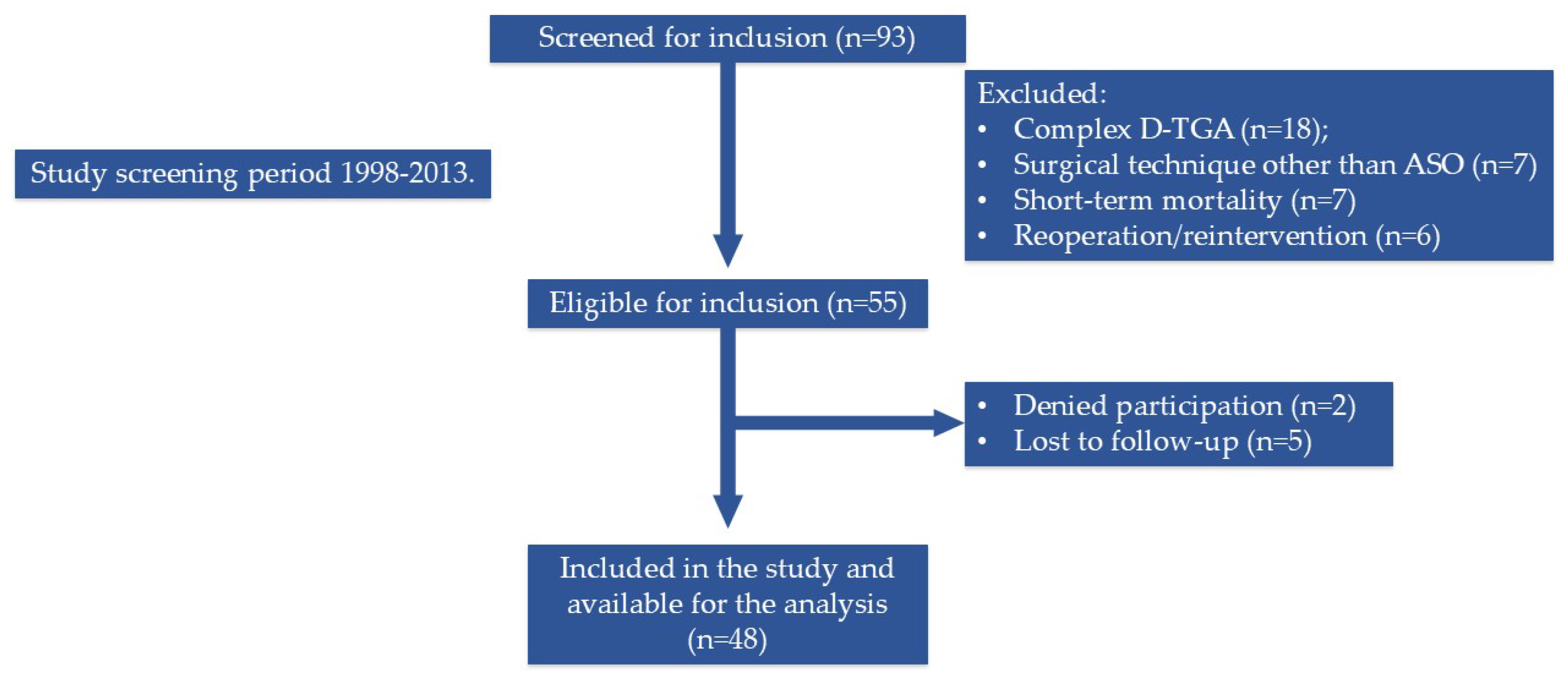
Figure 2.
Scatter plot demonstrating the relationship between TAPSE and CFVR in the study cohort (r=0.35, p=0.016).
Figure 2.
Scatter plot demonstrating the relationship between TAPSE and CFVR in the study cohort (r=0.35, p=0.016).
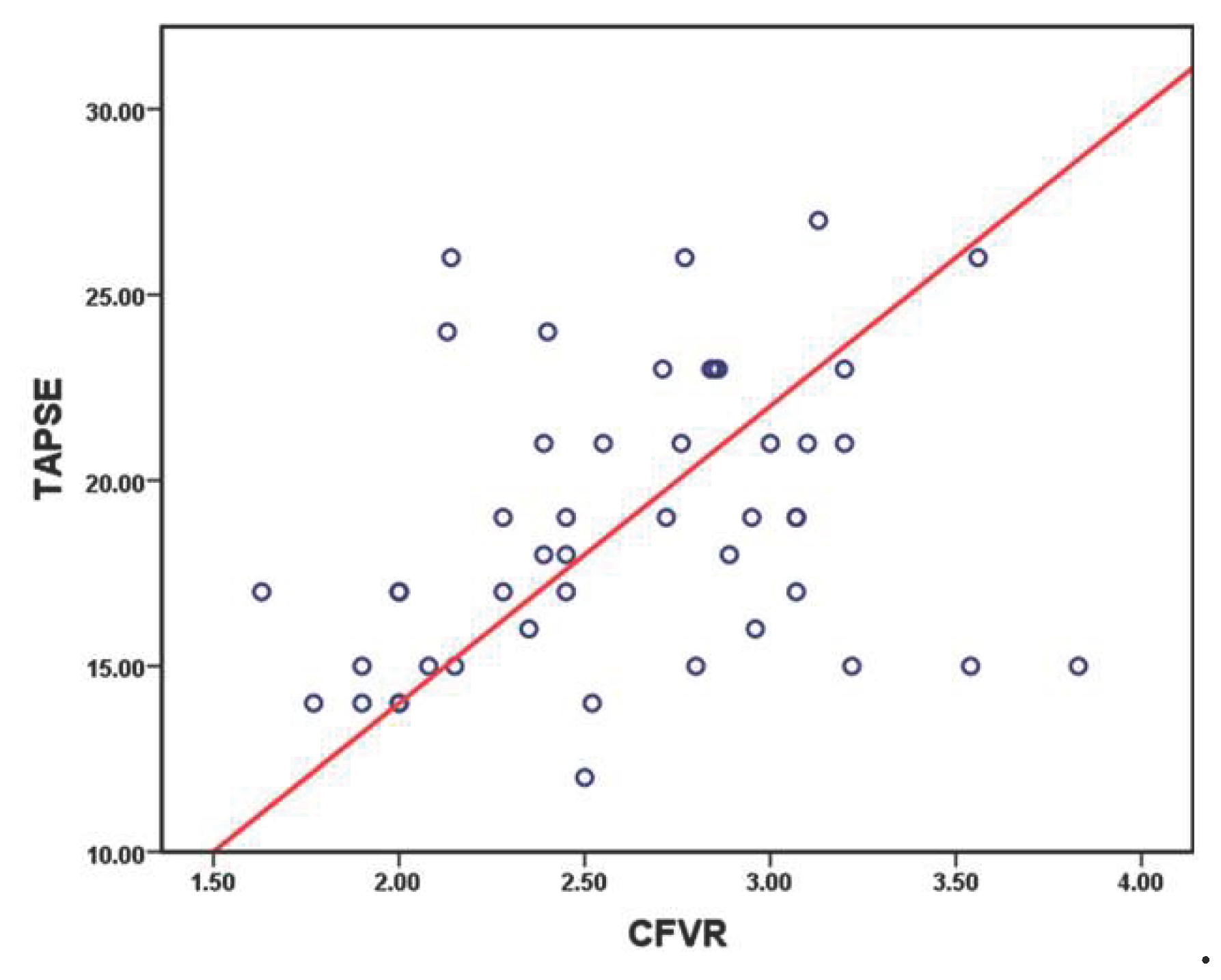

Table 1.
Baseline clinical and ASO characteristics in all patients, and in groups with impaired and preserved CFVR, respectively.
Table 1.
Baseline clinical and ASO characteristics in all patients, and in groups with impaired and preserved CFVR, respectively.
| All patients (n=48) | Impaired CFVR (n=21) | Preserved CFVR (n=27) |
p value | |
|---|---|---|---|---|
| Age (years, mean, SD) | 16.0±2.8 | 16.3±2.8 | 15.7±2.8 | 0.47 |
| Sex (male, %) | 71.0 | 71.0 | 70 | 0.99 |
| Weight (kg, mean, SD) | 64.16±23.54 | 66.18±30.1 | 62.58±17.27 | 0.34 |
| BMI (kg/m2, mean, SD) | 20.84±3.27 | 20.49±3.24 | 21.11±3.33 | 0.52 |
| BSA (m2, mean, SD) | 1.70±0.26 | 1.68±0.24 | 1.71±0.29 | 0.73 |
| NTproBNP (pg/ml, mean, SD) | 61.7±60.2 | 48.2±26.0 | 71.7±68.2 | 0.27 |
| Zlog NTproBNP (mean, SD) | 0.45±0.74 | 0.28±0.64 | 0.57±0.79 | 0.23 |
| Preoperative parameters | ||||
| Age at surgery (days, mean, SD) | 19±10 | 17±8 | 20±11 | 0.28 |
| Prenatal diagnosis (%) | 15.0 | 18.0 | 9.0 | 0.44 |
| Birth BW (kg, mean, SD) | 3.32±0.4 | 3.23±0.4 | 3.36±0.4 | 0.24 |
| BW less than 3 kg (%) | 13.0 | 19.0 | 7.0 | 0.38 |
| Preoperative PGE1 infusion (%) | 79.0 | 71.0 | 85.0 | 0.29 |
| Rashkind procedure (%) | 85.0 | 81.0 | 89.0 | 0.68 |
| Aorta/Pulmonary artery ratio (mean, SD) | 1.03±0.35 | 1.11±0.51 | 0.98±0.13 | 0.22 |
| Intraoperative and immediate postoperative characteristics | ||||
| Single coronary artery (%) | 12.0 | 9.0 | 15.0 | 0.68 |
| Left atrial pressure (mmHg, mean, SD) |
10.6±3.5 | 10.4±2.8 | 10.8±4.2 | 0.72 |
| Central venous pressure (mmHg, mean, SD) |
8.3±2.6 | 7.8±2.4 | 8.7±2.8 | 0.37 |
| MAP (mmHg, mean, SD) | 47±7.6 | 46.4±5.3 | 47.7±9.4 | 0.64 |
| Time from operation to extubating (days, mean, SD) | 4.0±2.3 | 4.4±2.1 | 4.7±2.5 | 0.62 |
| Low cardiac output syndrome (%) | 22.0 | 16.0 | 27.0 | 0.48 |
| Junctional ectopic tachycardia (%) | 26.0 | 20.0 | 31.0 | 0.51 |
| Peritoneal dialysis (%) | 26.0 | 15.0 | 35.0 | 0.18 |
| Diaphragm paresis (%) | 4.0 | 3.0 | 5.0 | 0.99 |
| Bleeding (%) | 11.0 | 5.0 | 15.0 | 0.37 |
| Myocardial ischemia (%) | 13.0 | 5.0 | 18.0 | 0.22 |
| Atelectasis (%) | 9.0 | 8.0 | 10.0 | 0.99 |
| Pneumothorax (%) | 11.0 | 15.0 | 8.0 | 0.64 |
| Any postoperative complication (%) | 50.0 | 40.0 | 58.0 | 0.37 |
Table 2.
Echocardiographic findings in all patients, and in groups with impaired and preserved CFVR, respectively.
Table 2.
Echocardiographic findings in all patients, and in groups with impaired and preserved CFVR, respectively.
| All patients (n=48) | Impaired CFVR (n=21) | Preserved CFVR (n=27) |
p value | |
|---|---|---|---|---|
| Left atrium (mm, mean, SD) | 26.5±3.0 | 26.6±3.0 | 26.4±3.0 | 0.88 |
| Left atrium Z score (mean, SD) | -0.16±0.89 | -0.13±0.87 | -0.19±0.91 | 0.81 |
| MV annulus (mm, mean, SD) | 27.8±3.8 | 27.4±3.1 | 28.2±4.4 | 0.46 |
| MV annulus Z score (mean, SD) | -0.51±0.90 | -0.53±0.84 | -0.49±0.96 | 0.87 |
| TV annulus (mm, mean, SD) | 27.5±3.7 | 26.7±4.0 | 28.1±3.4 | 0.18 |
| TV annulus Z score (mean, SD) | -0.58±0.71 | -0.60±0.85 | -0.56±0.60 | 0.84 |
| LVEDD (mm, mean, SD) | 48.5±5.2 | 48.0±5.4 | 48.9±5.0 | 0.54 |
| LVEDD Z score (mean, SD) | -0.20±1.00 | -0.20±1.03 | -0.20±1.00 | 0.99 |
| LVESD (mm, mean, SD) | 28.5±5.6 | 28.6±7.2 | 28.4±4.1 | 0.86 |
| LVESD Z score (mean, SD) | -0.47±1.07 | -0.13±1.06 | -0.74±1.02 | 0.050 |
| Shortening fraction (%, mean, SD) | 40.0±0.0 | 38.5±0.4 | 42.2±0.5 | 0.10 |
| LV ejection fraction (%, mean, SD) | 59.0±4.5 | 58.7±4.7 | 59.3±4.5 | 0.65 |
| Mitral valve E/A ratio (mean, SD) | 1.71±0.26 | 1.67±0.22 | 1.74±0.29 | 0.36 |
| MAPSE (mm, mean, SD) | 16.9±2.5 | 17.4±2.5 | 16.6±2.5 | 0.28 |
| Reduced MAPSE (%) | 29.0 | 28.0 | 29.0 | 0.99 |
| Tricuspid valve E/A ratio (mean, SD) | 1.57±0.31 | 1.53±0.27 | 1.60±0.34 | 0.39 |
| TAPSE (mm, mean, SD) | 18.8±3.8 | 17.6±3.5 | 19.7±3.9 | 0.064 |
| Reduced TAPSE (%) | 44.0 | 62.0 | 30.0 | 0.040 |
| Aorta (mm, mean, SD) | 24.4±3.0 | 24.2±2.9 | 24.7±3.1 | 0.59 |
| Aorta Z score (mean, SD) | 2.26±1.06 | 2.29±1.05 | 2.24±1.09 | 0.87 |
| Aortic dilation (%) | 79.0 | 80.0 | 78.0 | 0.99 |
| Pulmonary artery (mm, mean, SD) | 22.0±2.4 | 21.9±2.3 | 22.2±2.6 | 0.69 |
| Pulmonary artery Z score (mean, SD) | -0.70±0.74 | -0.69±0.81 | -0.71±0.70 | 0.93 |
| Global longitudinal LV strain (%, mean, SD) | -19.3±2.7 | -18.9±2.9 | -19.5±2.5 | 0.43 |
| Reduced GLS (%) | 29.0 | 29.0 | 30.0 | 0.99 |
Table 3.
Invasive hemodynamic measurements and cardiac catheterization findings in all patients, and groups with impaired and preserved CFVR, respectively.
Table 3.
Invasive hemodynamic measurements and cardiac catheterization findings in all patients, and groups with impaired and preserved CFVR, respectively.
| All patients (n=48) | Impaired CFVR (n=21) | Preserved CFVR (n=27) |
p value | |
|---|---|---|---|---|
| Aortic regurgitation> +1/4 (%) | 20.0 | 15.0 | 24.0 | 0.71 |
| Aorta, systolic pressure (mmHg, mean, SD) | 110±13 | 108±13 | 111±13 | 0.37 |
| Aorta, diastolic pressure (mmHg, mean, SD) | 68±10 | 65±8 | 70±10 | 0.082 |
| Aorta, mean pressure (mmHg, mean, SD) | 85±10 | 84±10 | 86±11 | 0.46 |
| Left ventricular systolic pressure (mmHg, mean, SD) | 114±16 | 111±17 | 115±15 | 0.36 |
| LV end-diastolic pressure (mmHg, mean, SD) | 13±5 | 12±6 | 13±5 | 0.52 |
| Right atrial a wave (mmHg, mean, SD) | 11±4 | 11±4 | 12±4 | 0.77 |
| Right atrial x wave (mmHg, mean, SD) | 8±3 | 8±3 | 8±4 | 0.77 |
| Right atrial mean pressure (mmHg, mean, SD) | 10±4 | 10±4 | 10±4 | 0.87 |
| Right ventricular systolic pressure (mmHg, mean, SD) | 42±9 | 44±7 | 40±10 | 0.26 |
| Right ventricular end-diastolic pressure (mmHg, mean, SD) | 10±4 | 10±5 | 9±3 | 0.39 |
| Left pulmonary artery branch stenosis (%) | 21.0 | 35.0 | 8.3 | 0.051 |
| Right pulmonary artery branch stenosis (%) | 21.0 | 25.0 | 17.0 | 0.71 |
| Pulmonary artery systolic pressure (mmHg, mean, SD) | 33±9 | 35±7 | 30±10 | 0.071 |
| Pulmonary artery diastolic pressure (mmHg, mean, SD) | 12±5 | 12±3 | 11±5 | 0.33 |
| Pulmonary artery mean pressure (mmHg, mean, SD) | 19±5 | 21±5 | 18±4 | 0.030 |
| Pulmonary artery mean pressure>20 mm Hg (%) | 43.0 | 60.0 | 29.0 | 0.041 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



