Submitted:
23 January 2026
Posted:
26 January 2026
You are already at the latest version
Abstract
Background: One in four US adults aged ≥65 years experiences a fall annually, leading to substantial injury and morbidity. Functional limitations may serve as early markers of vulnerability to fall injury. We aimed to estimate temporal trends and the association between functional limitation and fall injuries among community-dwelling older adults. Methods: For this retrospective cohort analysis, we pooled 2006–2017 National Health Interview Survey data and identified older adult survey respondents. Functional limitation, defined as any reported difficulty performing daily activities, and fall injury, defined as occurring within three months prior to the interview, were measured as binary variables. We controlled for sociodemographic, self-rated health, healthcare access, and physical activity factors. We reported the yearly trend in fall injury and functional limitations and performed survey-weighted univariable and multivariable logistic regression analyses, accounting for the potential confounders. Results: Our sample comprised 79,891 older adults, of whom 66% reported functional limitations and 2.3% reported a fall injury within 3 months of their interview. The prevalence of functional limitation increased from 61.8% in 2007 to 68.4% in 2017 (p<0.001). Also, the fall injury rates ranged from 1.8% to 2.6% during the same period. Older adults with functional limitations were more likely to report fall injuries (3.2% vs. 1.1%, p<0.001). After adjustment, functional limitation was associated with a two-fold higher odds of fall injury (OR = 2.03, 95% CI 1.71–2.40). Conclusion: Functional limitations are highly prevalent and increasing among older U.S. adults, doubling the likelihood of fall injury occurrence.
Keywords:
functional limitation
; fall injury
; older adults
; national health interview survey
1. Introduction
One in four older adults (65 years and older) experiences at least one fall event each year in the United States [1,2]. About a third of these falls result in injuries, including fractures, head trauma, and lacerations (3-5). In the U.S., falls account for nearly 3 million emergency department visits and 1 million hospital admissions annually, and cost approximately $50 billion in direct medical costs (2, 6, 7). Falls are often multifactorial in origin, and there is evidence that underlying functional limitations play a critical role in predisposing older adults to these events (8-10).
Functional limitations refer to difficulties in performing basic physical tasks required for independent daily living, such as walking, climbing stairs, carrying objects, or bathing, as well as the ability to perform daily life activities such as shopping and participating in leisure activities [11,12]. These limitations often stem from chronic health conditions, frailty, degenerative decline, neurological impairments, or a combination of these factors [10]. Among older adults, functional limitations can significantly compromise mobility, increasing reliance on assistive devices, caregivers, or environmental modifications [13,14]. Impaired mobility, in turn, reduces an individual's ability to safely navigate their surroundings, maintain balance, or recover from a loss of footing—all of which are critical for preventing falls [9,15]. While a fall in an older adult is a sentinel event for adverse outcome, functional limitation may be seen as a marker of vulnerability and a manifestation of the physical phenotype of frailty [16,17]. Earlier studies have reported that functional limitation is associated with a two-fold increased likelihood of hospitalization and a two-fold increased likelihood of mortality [9,18,19] Efforts to address functional limitations have included rehabilitation programs, community-based mobility interventions, and multifactorial fall-prevention initiatives that integrate physical therapy, home safety assessments, and assistive technologies [10,20]. However, continued monitoring of the population-level burden of functional limitation remains essential for informing prevention strategies [11,21].
As the older age proportion of the U.S. population increases, accurately identifying functional limitations becomes increasingly important for prioritizing interventions, such as physical and occupational therapy, assistive technologies, or environmental modifications [22,23]. This study aims to estimate the prevalence of fall injury and functional limitation among community-dwelling US older adults, examine their temporal trends, and examine the association between functional limitation and fall injury. While prior studies have reported an association between functional limitations and fall injuries [24,25,26,27], there is a lack of nationally representative data to assess the prevalence and strength of this association. Understanding the prevalence of functional limitations may provide critical insights into population vulnerability, guide resource allocation, and inform targeted strategies to reduce fall-related injuries.
2. Materials and Methods
Study Population
For this retrospective cohort analysis, we pooled data from the National Health Interview Survey (NHIS) between 2006 to 2017. The NHIS is a yearly cross-sectional survey of the non-institutionalized U.S. population that uses a multistage probability sampling method to collect data from households across all U.S. states and the District of Columbia [28]. Each year, more than 86,000 individuals within 35,000 households are surveyed, with intentional oversampling of Blacks, Hispanics, and Asians to ensure adequate subgroup representation [28]. Household data captured include basic family demographics and health characteristics, and one adult and one child per household are sampled. Sampled adults are further asked about specific health conditions, health-related behaviors, functional limitations, and healthcare access and utilization. To account for temporal changes in coding and variable definitions, and to ensure accurate survey data combination across years, we extracted NHIS data from the publicly available Integrated Public Use Microdata Series (IPUMS) platform [29]. The IPUMS NHIS dataset contains harmonized NHIS survey data, and each data extract includes pre-specified sampling weights, strata, and clusters.
Inclusion and Exclusion Criteria
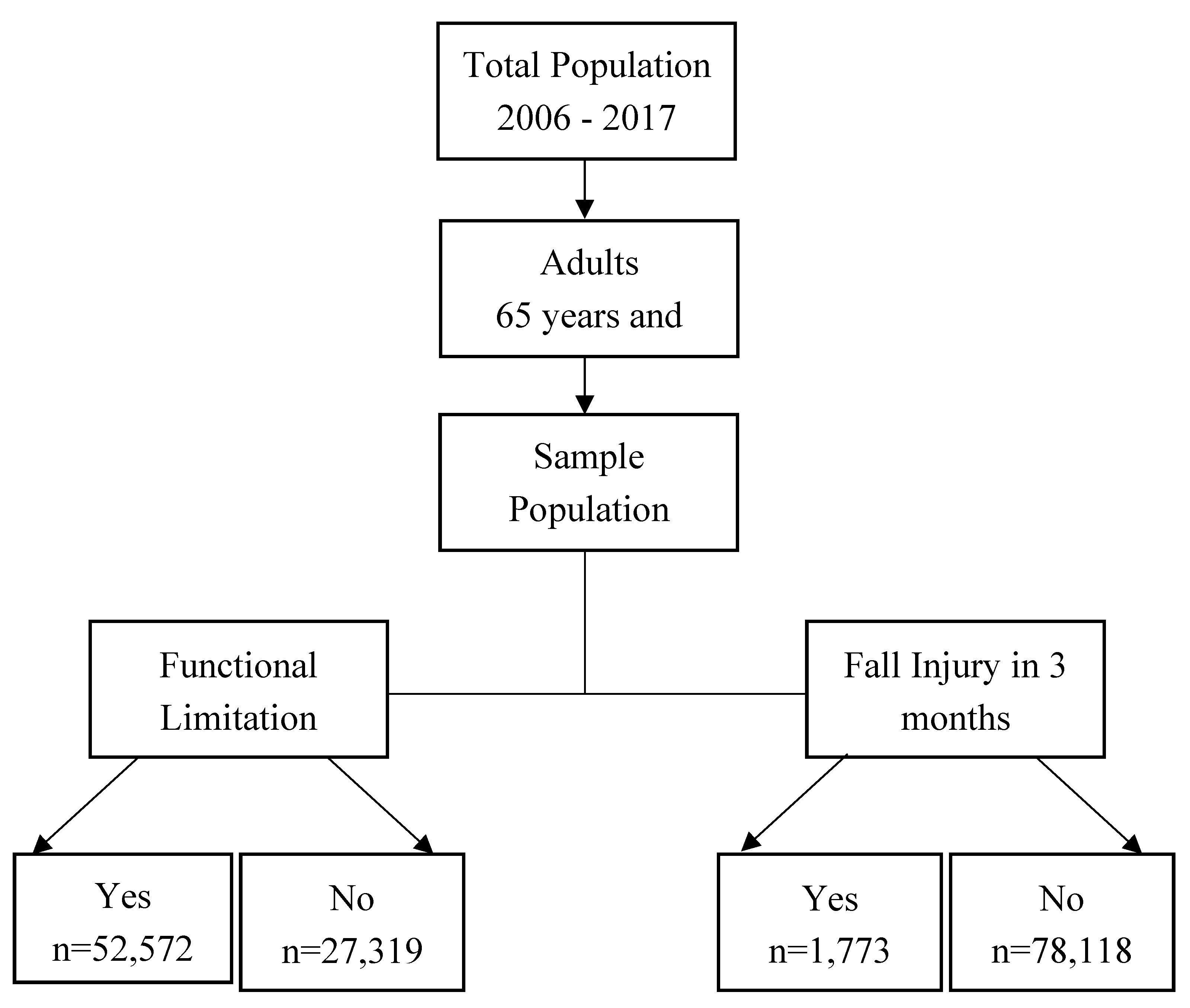
Between 2006 and 2017, 1,109,807 survey respondents participated (Figure 1). We selected individuals aged 65 years and older (n = 146,448) and further restricted the data to sampled adults, excluding household members whose data were captured as part of the household survey (n = 79,891). Our final sample, therefore, was 79,891 older adults.
Outcome Variable
The outcome measure was fall injury, defined as a self-reported injury resulting from a fall in the three months preceding the interview. This variable was extracted from the IPUMS NHIS’s injury module, designed to capture multiple injury events per respondent [30]. We reshaped the fall injury data to person-level, excluded duplicate entries, and linked it to the remaining core demographic and health-related data. For each respondent, we defined fall injury as a binary variable (yes/no).
Predictor Variables
The principal exposure variable was functional limitation, a recoded variable from the NHIS survey responses and defined as any self-reported difficulty or inability to carry out routine activities due to physical, mental, or emotional problems. NHIS survey respondents were asked about the degree of difficulty performing common activities such as walking a quarter mile, climbing ten steps, standing or sitting for two hours, stooping, reaching overhead, grasping small objects, carrying ten pounds, pushing large objects, shopping, or participating in social or leisure activities—without the use of special equipment [31]. Individuals reporting any level of difficulty (“only a little,” “somewhat,” “very,” or “can’t do at all”) on one or more items were classified as having a functional limitation.
Potential Confounders
We controlled for sociodemographic, health care access, self-reported health, and physical activity measures. The sociodemographic variables included age, sex, race/ethnicity, place of birth (US-born—yes/no), educational attainment, marital status, smoking status (never smoked, past smoker, current smoker), and poverty level, defined as either poor or not poor using a family income-to-poverty threshold ratio of 1.0 as the poverty benchmark [32]. Measures of health care access included available, accessible, and affordable care, as well as healthcare insurance. Respondents were asked if they had a usual place for medical care (available care), experienced delayed care because they could not get an appointment soon (accessible care), if they needed but could not afford medical care in the past 12 months (affordable care), and whether they had health insurance (health coverage). All measures of healthcare access were consistent with prior studies and measured as binary variables (33-35). Self-reported health measures included the chronic disease index and self-rated health. We created an index of chronic conditions from ten self-reported diagnoses: Chronic Obstructive Pulmonary Disease, Asthma, Angina, Chronic Arthritis, Cancer, Coronary Heart Disease, Liver Disease, Peptic Ulcer Disease, Diabetes, and Hypertension. We defined the index of chronic disease as 0 (none), 1, 2, or 3 or more. We defined self-rated health using the response to the survey item: “Would you say your health in general is excellent, very good, good, fair, or poor?” We defined self-rated health as a three-level variable: poor, fair, and good to excellent. Physical activity was assessed using self-reported weekly activity intensity, defined using weekly metabolic equivalent of task (MET) minutes. Respondents were asked, "How often do you engage in [1] moderate-intensity and [2] vigorous-intensity leisure-time physical activities” [36]? Following prior studies (37-39), weekly MET-minutes were calculated as: 4 × frequency of moderate activity per week × duration (in minutes) + 8 × frequency of vigorous activity per week × duration (in minutes). We reported activity intensity as none (0 MET-minutes), low (1 – 500 MET-minutes), moderate to high (>500 MET-minutes), similar to prior studies (37-39).
Handling of Missing Data
We encountered missingness in five variables: educational attainment (0.81%), marital status (0.28%), available care (0.14%), healthcare coverage (0.14%), and smoking status (0.78%). We imputed the missing values using the Multiple Imputation by Chained Equations (MICE) approach, generating 100 complete datasets through 100 iterations [40]. Final values were aggregated across imputations consistent with Rubin’s rules [41,42].
Data Analysis
We computed descriptive statistics to characterize the overall sample and reported differences between those with and without fall injuries, as well as between those with and without functional limitations. We reported trends in fall injuries and functional limitations over time and assessed change using a simple linear regression. We computed the unadjusted and adjusted associations between functional limitation and fall injury using univariate and multivariate logistic regression and reported the odds ratios and 95% confidence intervals (CIs). All regression models accounted for the complex NHIS survey design, including stratification, clustering, and weighting. Since we pooled 12 years of data, the original weight was divided by 12, consistent with the NHIS documentation [43,44]. All statistical analyses were performed using STATA version 16 [45].
3. Results
Our study included 79,891 persons, representing 22,642,863 non-institutionalized U.S. older adults. More than half (54%) of the population was between 65 and 74 years old, and the population was predominantly female (60%), non-Hispanic White (80%), US-born (89%), and with high school or less education (52%). Approximately 42% were married, and 39% were current smokers. Approximately 3% did not have a usual place of care, 4% experienced delayed care, 3% could not afford care, and less than one percent did not have healthcare coverage. Although only 87% reported having chronic diseases, 77% described their health as either good, very good, or excellent. Approximately 47% did not engage in any moderate or vigorous activity, and 66% reported having functional limitations.
A total of 1,773 (2.3%) older adults reported sustaining a fall injury within 3 months prior to their interview. The proportion of those having fall injury was higher with increasing age (p<0.001), among females (p<0.001), non-Hispanic White (p<0.001), US-born (p=0.040), with lower education attainment (p<0.001), and among those widowed, divorced, or separated (p<0.001). Additionally, the proportion of fall injury was higher among those who experienced delayed care (p<0.001) and could not afford care (p<0.001). Also, the proportion of fall injuries was higher among those with two or more chronic diseases (p<0.001), who self-reported poor or fair health (p<0.001), and who did not engage in at least moderate activity (p<0.001). Furthermore, 86% of those with functional limitations reported a fall injury, compared with 65% among those without functional limitations (p<0.001).
The proportion of respondents with functional limitations increased with increasing age (p<0.001). Also, the population with functional limitations was disproportionately female (p<0.001), non-Hispanic White and non-Hispanic Black (p<0.001), US-born (p<0.001), with lower educational attainment (p<0.001). Additionally, the proportion of functional limitations was higher among those who were either widowed, divorced, or separated (p<0.001), current and past smokers (p<0.001), without a usual place for care (p<0.001), or who reported that healthcare was unaffordable (p<0.001). Also, the proportion of functional limitations was higher among those with 2 or more chronic diseases (p<0.001), those who reported their health as either poor or fair (p<0.001), and those who did not engage in at least moderate activity (p<0.001)
Between 2006 and 2017, the fall injury rate ranged from 1.8% to 2.6%, with rates consistently higher among females. Also, the proportion of functional limitations significantly increased from 61.8% in 2007 to 68.4% in 2017 (p<0.001), representing a 0.3% increase for each year. Similarly, the rates were significantly and consistently higher among females during the period of study. In the unadjusted model, older adults with functional limitations were 3.2 times (OR: 3.22; 95% CI: 2.78–3.73) more likely to sustain a fall injury. After adjusting for sociodemographic, health, and healthcare access factors, functional limitation was associated with a two-fold increase in the odds of fall injury (OR: 2.03; 95% CI: 1.71 – 2.40).

Table 1.
Sociodemographic, injury, healthcare access, and health characteristics among older adults with and without fall injuries.
Table 1.
Sociodemographic, injury, healthcare access, and health characteristics among older adults with and without fall injuries.
| Variable | All Population (N=79,891) |
Fall Injury (n=1,773; 2.3%) |
No Fall Injury (n=78,118; 97.7%) |
p-value |
| Age Category | ||||
| 65 – 74 years | 43,811 (53.6) | 723 (39.6) | 43,088 (53.9) | <0.001 |
| 75 – 84 years | 25,735 (33.0) | 611 (34.9) | 25,124 (33.0) | |
| 85 years and older | 10,345 (13.4) | 439 (25.5) | 9,906 (13.1) | |
| Sex | ||||
| Male | 32,376 (39.9) | 522 (29.2) | 31,854 (40.1) | <0.001 |
| Female | 47,515 (60.1) | 1,251 (70.8) | 46,264 (59.9) | |
| Race/Ethnicity | ||||
| Non-Hispanic White | 58,413 (79.6) | 1,420 (85.1) | 56,993 (79.5) | <0.001 |
| Non-Hispanic Black | 9,944 (9.5) | 149 (6.8) | 9,795 (9.5) | |
| Hispanic | 7,038 (6.8) | 121 (5.0) | 6,917 (6.8) | |
| Other Races | 4,496 (4.1) | 83 (3.1) | 4,413 (4.2) | |
| Born in the US | ||||
| No | 9,935 (10.9) | 180 (9.3) | 9,755 (10.9) | 0.040 |
| Yes | 69,956 (89.1) | 1,593 (90.7) | 68,363 (89.1) | |
| Education | ||||
| High school or less | 42,000 (51.7) | 939 (51.7) | 41,061 (51.7) | <0.001 |
| Some college or AA | 19,640 (24.7) | 458 (26.1) | 19,182 (24.7) | |
| Bachelor’s degree | 10,324 (13.4) | 216 (12.7) | 10,108 (13.4) | |
| Postgraduate | 7,927 (10.3) | 160 (9.5) | 7,767 (10.3) | |
| Marital Status | ||||
| Married | 33,680 (42.3) | 548 (31.3) | 33,132 (42.5) | <0.001 |
| Single | 4,776 (5.8) | 96 (5.8) | 4,680 (5.8) | |
| WDS | 41,435 (51.9) | 1,129 (62.9) | 40,306 (51.6) | |
| Poverty Level | ||||
| Not Poor | 71,160 (90.3) | 1,545 (89.0) | 69,615 (90.4) | 0.078 |
| Poor | 8,731 (9.7) | 228 (11.0) | 8,503 (9.6) | |
| Smoking Status | ||||
| Never Smoked | 41,975 (52.0) | 926 (52.3) | 41,049 (52.0) | 0.433 |
| Past Smoker | 7,531 (9.3) | 153 (8.3) | 7,378 (9.4) | |
| Current Smoker | 30,385 (38.7) | 694 (39.4) | 29,691 (38.7) | |
| Available Care | ||||
| No place | 2,846 (3.4) | 27 (1.5) | 2,819 (3.5) | <0.001 |
| Has a place | 77,045 (96.6) | 1,746 (98.5) | 75,299 (96.5) | |
| Accessible Care | ||||
| Delayed | 3,249 (4.1) | 126 (7.2) | 3,123 (4.0) | <0.001 |
| Not Delayed | 76,642 (95.9) | 1,647 (92.8) | 74,995 (96.0) | |
| Affordable Care | ||||
| Cannot Afford | 2,487 (3.0) | 81 (4.5) | 2,406 (2.9) | <0.001 |
| Can Afford | 77,404 (97.0) | 1,692(95.5) | 75,712 (97.1) | |
| Health Insurance | ||||
| No Coverage | 605 (0.6) | 3 (0.2) | 602 (0.6) | 0.064 |
| Has Coverage | 79,286 (99.4) | 1,770 (99.8) | 77,516 (99.4) | |
| Chronic Disease Index | ||||
| None | 10,610 (13.4) | 112 (6.8) | 10,498 (13.6) | <0.001 |
| 1 | 41,264 (51.5) | 779 (44.3) | 40,485 (51.7) | |
| 2 | 23,564 (29.6) | 671 (37.3) | 22,893 (29.4) | |
| 3 or more | 4,453 (5.5) | 211 (11.7) | 4,242 (5.3) | |
| Self-rated health | ||||
| Poor | 4,732 (5.7) | 257 (14.3) | 4,475 (5.5) | <0.001 |
| Fair | 14,142 (17.0) | 448 (25.4) | 13,694 (16.8) | |
| Good/Excellent | 61,017 (77.3) | 1,068 (60.3) | 59,949 (77.7) | |
| Activity Intensity | ||||
| None | 37,356 (46.7) | 1,039 (58.0) | 36,317 (46.5) | <0.001 |
| Low | 12,696 (15.8) | 264 (15.0) | 12,432 (15.8) | |
| Moderate to High | 29,839 (37.5) | 470 (27.0) | 29,369 (37.7) | |
| Functional Limitations | ||||
| No | 27,319 (34.5) | 262 (14.3) | 27,057 (35.0) | <0.001 |
| Yes | 52,572 (65.5) | 1,511 (85.7) | 51,061 (65.0) |
WDS: Widowed, Divorced, and Separated.
Table 2.
Sociodemographic, injury, healthcare access, and health characteristics among older adults with and without functional limitations.
Table 2.
Sociodemographic, injury, healthcare access, and health characteristics among older adults with and without functional limitations.
| Variable | Functional Limitations (n=52,572; 65.5% |
No Functional Limitations (n=27,319; 34.5%) |
p-value |
| Age Category | |||
| 65 – 74 years | 25,855 (47.6) | 17,956 (65.0) | <0.001 |
| 75 – 84 years | 18,088 (35.4) | 7,647 (28.5) | |
| 85 years and older | 8,629 (17.0) | 1,716 (6.5) | |
| Sex | |||
| Male | 19,275 (35.8) | 13,101 (47.6) | <0.001 |
| Female | 33,297 (64.2) | 14,218 (52.4) | |
| Race/Ethnicity | |||
| Non-Hispanic White | 38,832 (80.2) | 19,581 (78.6) | <0.001 |
| Non-Hispanic Black | 6,713 (9.7) | 3,231 (9.0) | |
| Hispanic | 4,435 (6.5) | 2,603 (7.3) | |
| Other Races | 2,592 (3.6) | 1,904 (5.1) | |
| Born in the US | |||
| No | 5,882 (9.8) | 4,053 (13.0) | <0.001 |
| Yes | 46,690 (90.2) | 23,266 (87.0) | |
| Education | |||
| High school or less | 29,417 (55.2) | 12,583 (45.0) | <0.001 |
| Some college or AA | 12,884 (24.8) | 6,756 (24.5) | |
| Bachelor’s degree | 5,997 (11.7) | 4,327 (16.5) | |
| Postgraduate | 4,274 (8.3) | 3,653 (14.0) | |
| Marital Status | |||
| Married | 20,173 (38.6) | 13,507 (49.3) | <0.001 |
| Single | 3,078 (5.6) | 1,698 (6.2) | |
| WDS | 29,321 (55.8) | 12,114 (44.5) | |
| Poverty Level | |||
| Not Poor | 45,853 (88.6) | 25,307 (93.5) | <0.001 |
| Poor | 6,719 (11.4) | 2,012 (6.5) | |
| Smoking Status | |||
| Never Smoked | 27,039 (50.8) | 14,936 (54.2) | <0.001 |
| Past Smoker | 5,107 (9.6) | 2,424 (8.8) | |
| Current Smoker | 20,426 (39.6) | 9,959 (37.0) | |
| Available Care | |||
| No place | 1,412 (2.6) | 1,434 (5.0) | <0.001 |
| Has a place | 51,160 (97.4) | 25,885 (95.0) | |
| Accessible Care | |||
| Delayed | 2,675 (5.2) | 574 (2.0) | <0.001 |
| Not Delayed | 49,897 (94.8) | 26,745 (98.0) | |
| Affordable Care | |||
| Cannot Afford | 2,087 (3.8) | 400 (1.4) | <0.001 |
| Can Afford | 50,485 (96.2) | 26,919 (98.6) | |
| Health Insurance | |||
| Has Coverage | 52,289 (99.5) | 26,997 (99.1) | <0.001 |
| No Coverage | 283 (0.5) | 322 (0.9) | |
| Chronic Disease Index | |||
| None | 3,768 (7.3) | 6,842 (25.1) | <0.001 |
| 1 | 25,325 (48.1) | 15,939 (58.1) | |
| 2 | 19,366 (37.0) | 4,198 (15.5) | |
| 3 or more | 4,113 (7.7) | 340 (1.3) | |
| Self-rated health | |||
| Poor | 4,445 (8.1) | 287 (1.0) | <0.001 |
| Fair | 12,390 (22.8) | 1,752 (5.9) | |
| Good/Excellent | 35,737 (69.1) | 25,280 (93.1) | |
| Activity Intensity | |||
| None | 27,933 (53.2) | 9,423 (34.2) | |
| Low | 8,920 (16.9) | 3,776 (13.9) | <0.001 |
| Moderate-to-high | 15,719 (29.9) | 14,120 (51.9) |
WDS: Widowed, Divorced, and Separated.
Table 3.
Unadjusted and adjusted likelihood of fall injury among older adults by functional limitations, sociodemographic, injury, health, and healthcare access factors.
Table 3.
Unadjusted and adjusted likelihood of fall injury among older adults by functional limitations, sociodemographic, injury, health, and healthcare access factors.
| Variable | Unadjusted Odds Ratio (95% CI) | Adjusted Odds Ratio (95% CI) |
| Functional Limitations | ||
| Yes | 3.22 (2.78 – 3.73) | 2.03 (1.71 – 2.40) |
| No | Ref | Ref |
| Age Category | ||
| 65 – 74 years | Ref | Ref |
| 75 – 84 years | 1.44 (1.27 – 1.63) | 1.25 (1.10 – 1.42) |
| 85 years and older | 2.66 (2.32 – 3.04) | 2.01 (1.72 – 2.34) |
| Sex | ||
| Male | 0.62 (0.54 – 0.70) | 0.70 (0.61 – 0.80) |
| Female | Ref | Ref |
| Race/Ethnicity | ||
| Non-Hispanic White | Ref | Ref |
| Non-Hispanic Black | 0.66 (0.54 – 0.81) | 0.60 (0.49 – 0.74) |
| Hispanic | 0.69 (0.56 – 0.84) | 0.72 (0.57 – 0.91) |
| Other Races | 0.70 (0.55 – 0.90) | 0.77 (0.57 – 1.03) |
| Born in the US | ||
| Yes | 1.20 (1.01 – 1.43) | 1.02 (0.82 – 1.27) |
| No | Ref | Ref |
| Education | ||
| High school or less | Ref | Ref |
| Some college or AA | 1.06 (0.93 – 1.21) | 1.22 (1.06 – 1.39) |
| Bachelor’s degree | 0.95 (0.80 – 1.14) | 1.30 (1.09 – 1.56) |
| Postgraduate | 0.92 (0.75 -1.14) | 1.42 (1.15 – 1.77) |
| Marital Status | ||
| Married | Ref | Ref |
| Single | 1.35 (1.04 – 1.75) | 1.33 (1.02 – 1.72) |
| WDS | 1.65 (1.47 – 1.86) | 1.25 (1.09 – 1.43) |
| Poverty Level | ||
| Poor | 1.16 (0.98 – 1.37) | 0.96 (0.80 – 1.15) |
| Not Poor | Ref | Ref |
| Smoking Status | ||
| Never Smoked | Ref | Ref |
| Past Smoker | 0.88 (0.71 – 1.09) | 0.96 (0.77 – 1.19) |
| Current Smoker | 1.01 (0.90 – 1.13) | 1.04 (0.93 – 1.17) |
| Available Care | ||
| No place | 0.43 (0.27 – 0.67) | 0.58 (0.37 – 0.91) |
| Has a place | Ref | Ref |
| Accessible Care | ||
| Delayed | 1.86 (1.51 – 2.30) | 1.50 (1.21 – 1.85) |
| Not Delayed | Re | Ref |
| Affordable Care | ||
| Cannot Afford | 1.55 (1.20 – 2.01) | 1.19 (0.90 – 1.57) |
| Can Afford | Ref | Ref |
| Health Insurance | ||
| Has Coverage | 0.34 (0.11 – 1.12) | 0.57 (0.17 – 1.90) |
| No Coverage | Ref | Ref |
| Chronic disease Index | ||
| None | Ref | Ref |
| 1 | 1.72 (1.36 – 2.18) | 1.27 (0.99 – 1.62) |
| 2 | 2.55 (2.00 – 3.24) | 1.47 (1.14 – 1.89) |
| 3 | 4.43 (3.38 – 5. 81) | 2.04 (1.53 – 2.71) |
| Self-rated health | ||
| Poor | 3.38 (2.87 -3.99) | 2.43 (2.02 – 2.92) |
| Fair | 1.95 (1.71 – 2.21) | 1.54 (1.34 – 1.77) |
| Good/Excellent | Ref | Ref |
| Activity Intensity | ||
| None | 1.75 (1.54 – 1.99) | 1.15 (0.99 – 1.33) |
| Low | 1.32 (1.11 – 1.57) | 1.04 (0.87 – 1.23) |
| Moderate-to-high | Ref | Ref |
WDS: Widowed, Divorced, and Separated.
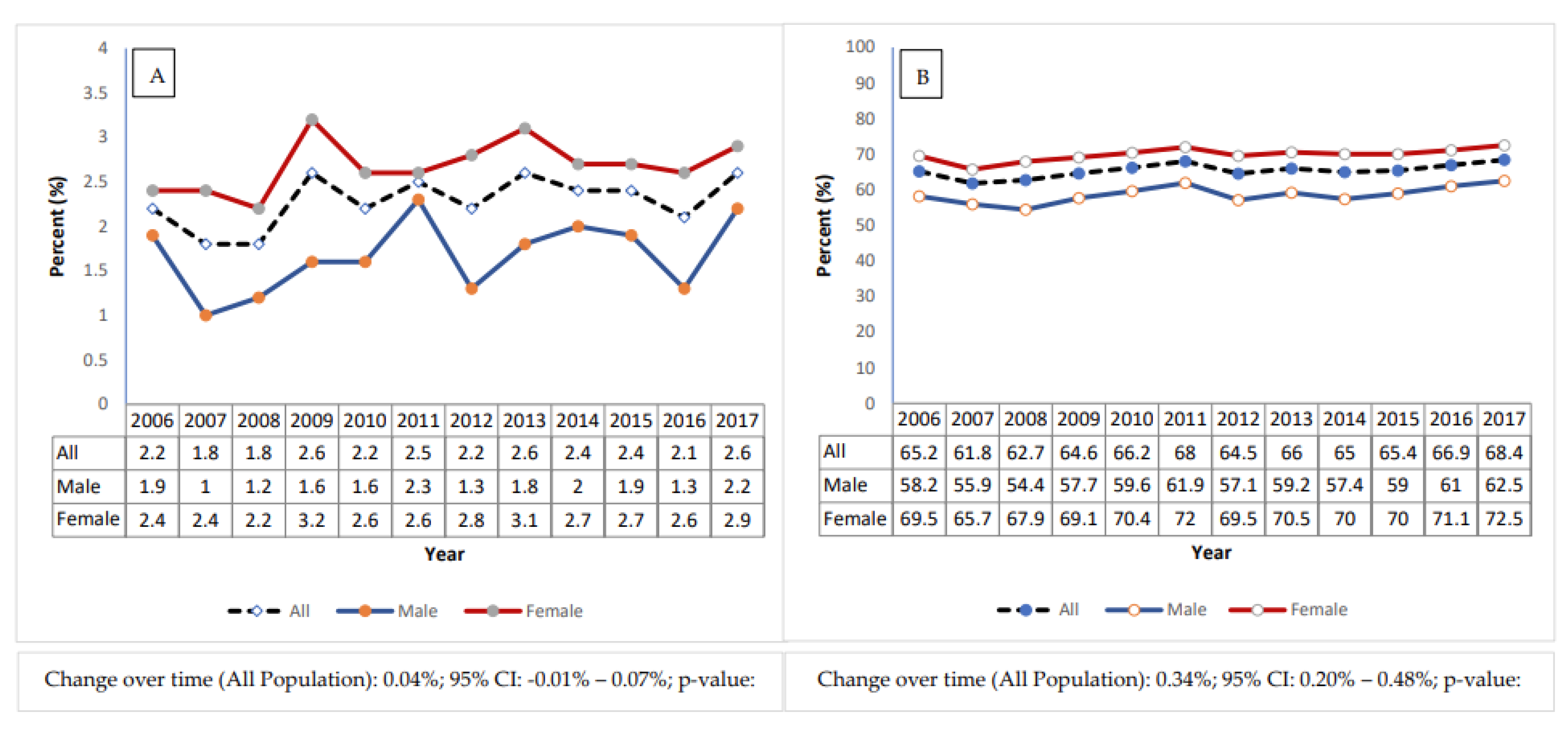
Figure 2.
Trend in (A.) Proportion of Fall Injuries, and (B.) Functional Limitations among the study population, stratified by sex, between 2006 and 2017.
Figure 2.
Trend in (A.) Proportion of Fall Injuries, and (B.) Functional Limitations among the study population, stratified by sex, between 2006 and 2017.
4. Discussion
In this nationally representative analysis of older U.S. adults conducted between 2002 and 2017, we observed a slow upward trend in the proportion of persons with functional limitations, affecting two-thirds of the population. While the 3-month incidence of fall injuries ranged between 2–3% among both sexes, females consistently demonstrated higher rates of both functional limitations and fall injuries than males. Also, older adults with functional limitations were two times more likely to sustain a fall-related injury compared with those without functional limitations.
Consistent with earlier studies [46,47], the 3-month incidence of fall injuries among US community-dwelling older adults ranged between 2% and 3%. When extrapolated, our 3-month fall injury rate is closely aligned with national annual fall injury rates of 8% to 10% (46, 48, 49). While intrinsic and extrinsic factors such as age-related physiologic decline, vision, hearing, and other causes of imbalance, polypharmacy and fall risk-inducing drugs, and environmental hazards primarily increase the likelihood of falling [50], the occurrence of injury after a fall depends on additional clinical, biomechanical, and environmental factors [50]. Lower bone mineral density, sarcopenia, slower protective responses, and anticoagulant use increase the risk that a fall will result in fracture rather than a minor event [51]. Injury mechanisms, such as height, speed, and protective responses and reflexes that interrupt the progression of a fall, may affect the occurrence and severity of a fall injury [52,53]. Comorbidities such as osteoporosis, frailty, and cognitive impairment further compound this risk by reducing postural control and the ability to mitigate impact during a fall [50]. Environmental factors, such as hard flooring or a lack of cushioning, also influence the severity of fall injuries (54-56).
Among our study population, functional limitation was associated with a two-fold increased likelihood of fall injury. Several studies have reported that functional limitations predict the risk of fall injuries (57-59). For example, Stevens et al. [57] reported that older adults with functional limitations were three times more likely to sustain fall-related fractures. Yet, other studies have reported that fall injuries predict functional limitations [60,61]. On one hand, functional limitations, such as impaired balance, slowed gait, reduced muscle strength, and poor coordination [62], compromise an individual’s ability to recover from perturbations, navigate environmental hazards, or stabilize after a slip, thereby increasing the risk of sustaining a fall-related injury [58]. On the other hand, prior falls, a strong predictor of future falls [63], can lead to injuries such as fractures and soft-tissue injuries, which can exacerbate or precipitate new functional limitations, manifesting as reduced mobility, deconditioning, and loss of independence [64]. Over time, this cyclical interplay between functional decline and fall injury may contribute to the gradual increase in functional limitation, which may explain the increasing prevalence we report in this study.
Consistent with prior research, our study found that females exhibited higher rates of both functional limitations and fall injuries than males across all study years [65,66]. Several biological, behavioral, and social factors may explain this disparity. Women are more likely to experience musculoskeletal disorders such as osteoporosis and sarcopenia and have lower muscle mass and strength [67,68], all of which contribute to heightened fracture risk and fall injuries [69,70]. The consistently higher rates of functional limitations and fall injuries we report lend credence to this underlying vulnerability.
Our findings have important implications for clinical care and public health. Given the strong association between functional limitations and fall injuries, there should be continued emphasis on screening for functional limitations using instruments such as the Activities of Daily Living and Instrumental Activities of Daily Living scales [71] or as part of the Comprehensive Geriatric Assessment [72]. Fall risk assessment tools such as the Centers for Disease Control and Prevention’s Stopping Elderly Accidents, Deaths, and Injuries (STEADI) [73] can further identify individuals whose functional impairments may predispose them to falls [74,75]. Early intervention, such as tailored exercise programs such as Tai Chi, physical and occupational therapy, and environmental assessments, may help reduce falls and extend functional independence [76,77,78]. From a policy perspective, consistent integration of fall prevention and functional assessment into community-based aging programs, such as naturally occurring retirement community social service programs and Medicare wellness visits, could yield significant downstream benefits. Identifying and preventing functional limitations early, such as preclinical mobility limitations [79], may represent one of the most effective strategies for preventing fall-related injuries and promoting healthy aging.
Our study has its limitations. This study’s retrospective cohort design precludes establishing causal relationships between functional limitation and fall injury. Responses to the NHIS questions are self-reported and may be subject to recall and social desirability biases [80,81]. Although we controlled for comorbidity, self-reported health, and physical activity, we did not account for prior functional limitations or the number of prior falls due to the unavailability of such data. Despite these limitations, our large, nationally representative data set enables reliable estimation of population-level trends among U.S. older adults. The 16-year trend enables temporal assessment of changes in both fall injury incidence and functional limitation prevalence. Additionally, our robust control for potential confounders, survey design, clustering, and weights provides reliable estimates for epidemiological assessment, policy recommendations, and intervention design.
Author Contributions
Conceptualization, O.A; Methodology, O.A.; Software, O.A., J.C.; Formal Analysis, O.A.; Data Curation, O.A.; Writing – Original Draft Preparation, O.A.; Writing – Review & Editing, O.A., T.C., G.O., D.B, J.C.; Visualization, O.A.; Supervision, J.C.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study. Based on guidance from the New York University Institutional Review Board, secondary data analysis of publicly available dataset does not require IRB approval.
Informed Consent Statement
Not applicable since this study used de-identified publicly available data.
Data Availability Statement
The original data presented in the study are openly available in FigShare at 10.6084/m9.figshare.30739685.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| MET | Metabolic Equivalent of Task |
| IPUMS | Integrated Public Use Microdata Series |
| NHIS | National Health Interview Survey |
| AOR | Adjusted Odds Ratio |
| CI | Confidence Interval |
| US | United States |
| WDS | Widowed, Divorced, Separated |
References
- Centers for Disease Control and Prevention. Older Adult Falls Data 2024. Available online: https://www.cdc.gov/falls/data-research/?CDC_AAref_Val=https://www.cdc.gov/falls/data/index.html.
- National Council on Aging. Get the Facts on Falls Prevention 2025. Available online: https://www.ncoa.org/article/get-the-facts-on-falls-prevention/.
- Grundstrom, A.C.; Guse, C.E.; Layde, P.M. Risk factors for falls and fall-related injuries in adults 85 years of age and older. Arch. Gerontol. Geriatr. 2011, 54, 421–428. [Google Scholar] [CrossRef]
- Richard, G. Stefanacci JRW. Reviewed/Revised Aug 2025. Available online: https://www.msdmanuals.com/home/older-people-s-health-issues/falls-in-older-adults/falls-in-older-adults.
- Centers for Disease Control and Prevention. Disease Severity of Respiratory Syncytial Virus Compared with COVID-19 and Influenza Among Hospitalized Adults Aged ≥60 Years — IVY Network, 20 U.S. States. February 2022–May 2023 2023. Available online: https://www.cdc.gov/mmwr/volumes/72/wr/mm7240a2.htm.
- National Center for Injury Prevention and Control. Cost of older adult falls Atlanta, GA2020. Available online: https://stacks.cdc.gov/view/cdc/122747.
- Shankar, K.N.; Liu, S.W.; Ganz, D.A. Trends and Characteristics of Emergency Department Visits for Fall-Related Injuries in Older Adults, 2003–2010. West J. Emerg. Med. 2017, 18, 785–793. [Google Scholar] [CrossRef]
- A Soriano, T.; DeCherrie, L.V.; Thomas, D.C. Falls in the community-dwelling older adult: A review for primary-care providers. Clin. Interv. Aging 2007, 2, 545–553. [Google Scholar] [CrossRef]
- Smee, D.J.; Anson, J.M.; Waddington, G.S.; Berry, H.L. Association between Physical Functionality and Falls Risk in Community-Living Older Adults. Curr. Gerontol. Geriatr. Res. 2012, 2012, 864516. [Google Scholar] [CrossRef]
- Colón-Emeric, C.S.; Whitson, H.E.; Pavon, J.; Hoenig, H. Functional decline in older adults. Am Fam Physician 2013, 88, 388–394. [Google Scholar]
- Centers for Disease Control and Prevention. Functional Limitation: National Center for Health Statistics. 2024. Available online: https://www.cdc.gov/nchs/hus/topics/functional-limitation.htm.
- Institute of Medicine Committee on Assessing Rehabilitation Science and Engineering. Functional Limitations Research in Rehabilitation Science and Engineering; Brandt EN Jr., PA, Ed.; National Academies Press (US): Washington (DC), 1997. [Google Scholar]
- Lin, I.-F.; Wu, H.-S. Activity Limitations, Use of Assistive Devices or Personal Help, and Well-Being: Variation by Education. Journals Gerontol. Ser. B 2014, 69, S16–S25. [Google Scholar] [CrossRef] [PubMed]
- Prajapati, G.; Sharmila, K. Difficulties experienced by older adults when not using assistive devices. Discov. Soc. Sci. Heal. 2023, 3, 1–10. [Google Scholar] [CrossRef]
- Wagner, M. Impaired Physical Mobility Nursing Diagnosis & Care Plans Updated in 2025. Available online: https://www.nursetogether.com/impaired-physical-mobility-nursing-diagnosis-care-plan/.
- Wisdom, L. Significance of Physical frailty. Available online: https://www.wisdomlib.org/concept/physical-frailty.
- Fingerman, K.L.; Ng, Y.T.; Huo, M.; Birditt, K.S.; Charles, S.T.; Zarit, S. Functional Limitations, Social Integration, and Daily Activities in Late Life. J Gerontol B Psychol Sci Soc Sci. 2021, 76, 1937–1947. [Google Scholar] [CrossRef]
- A Garvin, D.; A Roberto, M. Change through persuasion. 2005, 83, 104–112. [Google Scholar] [PubMed]
- Isaia, G.; Maero, B.; Gatti, A.; Neirotti, M.; Ricauda, N.A.; Bo, M.; Ruatta, C.; Gariglio, F.; Miceli, C.; Corsinovi, L.; et al. Risk factors of functional decline during hospitalization in the oldest old. Aging Clin. Exp. Res. 2009, 21, 453–457. [Google Scholar] [CrossRef] [PubMed]
- Gillespie, L.D.; Robertson, M.C.; Gillespie, W.J.; Sherrington, C.; Gates, S.; Clemson, L.M.; et al. Interventions for preventing falls in older people living in the community. Cochrane Database Syst Rev. 2012, 2012, Cd007146. [Google Scholar]
- Keyes, D TH; Das, JM. Prevention Strategies; StatPearls Publishing: StatPearls [Internet] Treasure Island (FL), 14 Sep 2025; Available online: https://www.ncbi.nlm.nih.gov/books/NBK537222/.
- Newman, A.B. The Epidemiology and Societal Impact of Aging-Related Functional Limitations: A Looming Public Health Crisis. Journals Gerontol. Ser. A 2023, 78, 4–7. [Google Scholar] [CrossRef]
- Fotteler, M.L.; Mühlbauer, V.; Brefka, S.; Mayer, S.; Kohn, B.; Holl, F.; Swoboda, W.; Gaugisch, P.; Risch, B.; Denkinger, M.; et al. The Effectiveness of Assistive Technologies for Older Adults and the Influence of Frailty: Systematic Literature Review of Randomized Controlled Trials. JMIR Aging 2022, 5, e31916. [Google Scholar] [CrossRef] [PubMed]
- Büchele, G.; Rapp, K.; König, H.-H.; Jaensch, A.; Rothenbacher, D.; Becker, C.; Benzinger, P. The Risk of Hospital Admission Due to Traumatic Brain Injury Is Increased in Older Persons With Severe Functional Limitations. J. Am. Med Dir. Assoc. 2016, 17, 609–612. [Google Scholar] [CrossRef] [PubMed]
- Gill, T.M.; Murphy, T.E.; Gahbauer, E.A.; Allore, H.G. The Course of Disability Before and After a Serious Fall Injury. JAMA Intern. Med. 2013, 173, 1780–1786. [Google Scholar] [CrossRef]
- Ward, R.E.; Leveille, S.G.; Beauchamp, M.K.; Travison, T.; Alexander, N.; Jette, A.M.; Bean, J.F. Functional Performance as a Predictor of Injurious Falls in Older Adults. J. Am. Geriatr. Soc. 2015, 63, 315–320. [Google Scholar] [CrossRef]
- \ Welmer, A.-K.; Rizzuto, D.; Laukka, E.J.; Johnell, K.; Fratiglioni, L. Cognitive and Physical Function in Relation to the Risk of Injurious Falls in Older Adults: A Population-Based Study. J. Gerontol. A Biol. Sci. Med. Sci. 2017, 72, 669–675. [Google Scholar] [PubMed]
- Centers for Disease Control and Prevention. About the National Health Interview Survey 2018. Available online: https://www.cdc.gov/nchs/nhis/about_nhis.htm.
- Blewett, L.A.; Rivera, JADrew; King, M.L.; Williams, K. IPUMS Health Surveys: National Health Interview Survey, Version 6.4 [NHIS]. Version 6.4 [NHIS] ed.; Minneapolis, 2019. [Google Scholar]
- Integrated Public Use Microdata Series. IRCAUSE. 2022. Available online: https://nhis.ipums.org/nhis-action/variables/IRCAUSE#description_section.
- IPUMS Health Surveys. FLANY: Has any functional limitation 2019. Available online: https://nhis.ipums.org/nhis-action/variables/FLANY#description_section.
- IPUMS Health Surveys. Pooryn. 2018. Available online: https://nhis.ipums.org/nhis-action/variables/POORYN#description_section.
- Adeyemi, O.J.; Gill, T.L.; Paul, R.; Huber, L.B. Evaluating the association of self-reported psychological distress and self-rated health on survival times among women with breast cancer in the U.S. PLOS ONE 2021, 16, e0260481. [Google Scholar] [CrossRef]
- Adeyemi, O.J.; Paul, R.; Akinsola, O.O.; Bouillon-Minois, J.-B.; Arinxe, G.R.; Arif, A.A. Poverty, Health Care Access Barriers, and Functional Limitations among Individuals with Chronic Obstructive Pulmonary Disease: An 11-Year Cross-sectional Analysis, 2008–2018. J. Heal. Care Poor Underserved 2023, 34, 652–672. [Google Scholar] [CrossRef]
- Ayodele, T.; Fletcher, C.; Beredjiklian, K.B.; Valenzuela, M.; Mazur, Z.; Adoyele, T. Disparities in Health Insurance and Delayed Care Among Hispanic Immigrants in the United States. Cureus 2025, 17. [Google Scholar] [CrossRef]
- IPUMS Health Surveys. LANY: Has any activity limitation 2019. Available online: https://nhis.ipums.org/nhis-action/variables/LANY#codes_section.
- Adeyemi, O.; Chippendale, T.; Ogedegbe, O.; Boatright, D.; Chodosh, J. Activity Intensity and All-Cause Mortality Following Fall Injury Among Older Adults: Results from a 12-Year National Survey. Healthcare 2025, 13, 2530. [Google Scholar] [CrossRef]
- Jeong, S.-W.; Kim, S.-H.; Kang, S.-H.; Kim, H.-J.; Yoon, C.-H.; Youn, T.-J.; Chae, I.-H. Mortality reduction with physical activity in patients with and without cardiovascular disease. Eur. Heart J. 2019, 40, 3547–3555. [Google Scholar] [CrossRef]
- Jetté, M.; Sidney, K.; Blümchen, G. Metabolic equivalents (METS) in exercise testing, exercise prescription, and evaluation of functional capacity. Clin. Cardiol. 1990, 13, 555–565. [Google Scholar] [CrossRef]
- Azur, M.J.; Stuart, E.A.; Frangakis, C.; Leaf, P.J. Multiple imputation by chained equations: What is it and how does it work? Int. J. Methods Psychiatr. Res. 2011, 20, 40–49. [Google Scholar] [CrossRef] [PubMed]
- McNeish, D. Exploratory Factor Analysis With Small Samples and Missing Data. J. Pers. Assess. 2017, 99, 637–652. [Google Scholar] [CrossRef] [PubMed]
- Dray, S.; Josse, J. Principal component analysis with missing values: a comparative survey of methods. Plant Ecol. 2015, 216, 657–667. [Google Scholar] [CrossRef]
- Blewett, LA; Drew, JAR; King, ML; Williams, CWK. User Note - Sampling Weights 2020. Available online: https://nhis.ipums.org/nhis/userNotes_weights.shtml.
- IPUMS Health Surveys. User Note - Sampling Weights: Minnesota Population Center, University of Minnesota. 2017. Available online: https://nhis.ipums.org/nhis/userNotes_weights.shtml.
- StataCorp. Stata Statistical Software: Release 16; StataCorp LLC: College Station, TX, 2017. [Google Scholar]
- Verma, S.K.; Willetts, J.L.; Corns, H.L.; Marucci-Wellman, H.R.; Lombardi, D.A.; Courtney, T.K. Falls and Fall-Related Injuries among Community-Dwelling Adults in the United States. PLoS ONE 2016, 11, e0150939. [Google Scholar] [CrossRef]
- Kenis, C.; Decoster, L.; Flamaing, J.; Debruyne, P.R.; De Groof, I.; Focan, C.; Cornélis, F.; Verschaeve, V.; Bachmann, C.; Bron, D.; et al. Incidence of falls and fall-related injuries and their predictive factors in frail older persons with cancer: a multicenter study. BMC Geriatr. 2022, 22, 1–14. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Facts About Falls 2021. Available online: https://www.cdc.gov/falls/data-research/facts-stats/index.html?
- Bergen, G.; Stevens, M.R.; Burns, E.R. Falls and Fall Injuries Among Adults Aged ≥65 Years — United States, 2014. Mmwr-Morbidity Mortal. Wkly. Rep. 2016, 65, 993–998. [Google Scholar] [CrossRef]
- Appeadu, M.K.; Bordoni, B. Falls and Fall Prevention In The Elderly2022 01/13/2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK560761/.
- Yeung, S.S.Y.; Reijnierse, E.M.; Pham, V.K.; Trappenburg, M.C.; Lim, W.K.; Meskers, C.G.M.; Maier, A.B. Sarcopenia and its association with falls and fractures in older adults: A systematic review and meta-analysis. J. Cachexia Sarcopenia Muscle 2019, 10, 485–500. [Google Scholar] [CrossRef]
- Hsieh, T.-M.; Tsai, C.-H.; Liu, H.-T.; Huang, C.-Y.; Chou, S.-E.; Su, W.-T.; Hsu, S.-Y.; Hsieh, C.-H. Effect of Height of Fall on Mortality in Patients with Fall Accidents: A Retrospective Cross-Sectional Study. Int. J. Environ. Res. Public Heal. 2020, 17, 4163. [Google Scholar] [CrossRef] [PubMed]
- Borrelli, J.; Creath, R.; Rogers, M.W. Protective arm movements are modulated with fall height. J. Biomech. 2020, 99, 109569. [Google Scholar] [CrossRef]
- Drahota, A.; Felix, L.M.; Raftery, J.; Keenan, B.E.; Lachance, C.C.; Mackey, D.C.; Markham, C.; Laing, A.C. The SAFEST review: a mixed methods systematic review of shock-absorbing flooring for fall-related injury prevention. BMC Geriatr. 2022, 22, 1–28. [Google Scholar] [CrossRef]
- Gustavsson, J.; Bonander, C.; Andersson, R.; Nilson, F. Investigating the fall-injury reducing effect of impact absorbing flooring among female nursing home residents: initial results. Inj. Prev. 2015, 21, 320–324. [Google Scholar] [CrossRef]
- Lachance, C.C.; Jurkowski, M.P.; Dymarz, A.C.; Robinovitch, S.N.; Feldman, F.; Laing, A.C.; Mackey, D.C. Compliant flooring to prevent fall-related injuries in older adults: A scoping review of biomechanical efficacy, clinical effectiveness, cost-effectiveness, and workplace safety. PLOS ONE 2017, 12, e0171652. [Google Scholar] [CrossRef]
- Stevens, J.A.; Powell, K.E.; Smith, S.M.; Wingo, P.A.; Sattin, R.W. Physical activity, functional limitations, and the risk of fall-related fractures in community-dwelling elderly. Ann. Epidemiology 1997, 7, 54–61. [Google Scholar] [CrossRef]
- Yip, W.; Ge, L.; Heng, B.H.; Tan, W.S. Association between patient-reported functional measures and incident falls. Sci. Rep. 2021, 11, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Adeyemi, O.; Grudzen, C.; DiMaggio, C.; Wittman, I.; Velez-Rosborough, A.; Arcila-Mesa, M.; Cuthel, A.; Poracky, H.; Meyman, P.; Chodosh, J. Pre-injury frailty and clinical care trajectory of older adults with trauma injuries: A retrospective cohort analysis of A large level I US trauma center. PLOS ONE 2025, 20, e0317305. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.; Peng, W.; Ge, S.; Li, C.; Zheng, Y.; Huang, X.; Liu, M. Longitudinal associations of concurrent falls and fear of falling with functional limitations differ by living alone or not. Front. Public Heal. 2023, 11. [Google Scholar] [CrossRef]
- Yang, R.; Wang, H.; Tracy, E.L.; Jo, Y.J.; Sward, K.A.; Edelman, L.S.; Demiris, G. What is the relationship between falls, functional limitations, and depressive symptoms among Chinese older adults? The role of living alone. Maturitas 2023, 168, 78–83. [Google Scholar] [CrossRef]
- Institute of Medicine (US) Division of Health Promotion and Disease Prevention. Falls in Older Persons: Risk Factors and Prevention. The Second Fifty Years: Promoting Health and Preventing Disability [Internet]. 1992. Available online: https://www.ncbi.nlm.nih.gov/books/NBK235613/.
- Barrett-Connor, E.; Weiss, T.W.; McHorney, C.A.; Miller, P.D.; Siris, E.S. Predictors of falls among postmenopausal women: results from the National Osteoporosis Risk Assessment (NORA). Osteoporos. Int. 2009, 20, 715–722. [Google Scholar] [CrossRef]
- Belete, Y.; Belay, G.J.; Dugo, T.; Gashaw, M. Assessment of Functional Limitation and Associated Factors in Adults with Following Lower Limb Fractures, Gondar, Ethiopia in 2020: Prospective Cross-Sectional Study. Orthop. Res. Rev. 2021, 13, 35–45. [Google Scholar] [CrossRef]
- Li, S.; Surineni, K. Falls in Hospitalized Patients and Preventive Strategies: A Narrative Review. Am. J. Geriatr. Psychiatry: Open Sci. Educ. Pr. 2024, 5, 1–9. [Google Scholar] [CrossRef]
- A Stevens, J.; Sogolow, E.D. Gender differences for non-fatal unintentional fall related injuries among older adults. Inj. Prev. 2005, 11, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Greco, E.A.; Pietschmann, P.; Migliaccio, S. Osteoporosis and Sarcopenia Increase Frailty Syndrome in the Elderly. Front. Endocrinol. 2019, 10, 255. [Google Scholar] [CrossRef] [PubMed]
- Wright, V.J.; Schwartzman, J.D.; Itinoche, R.; Wittstein, J. The musculoskeletal syndrome of menopause. Climacteric 2024, 27, 466–472. [Google Scholar] [CrossRef] [PubMed]
- Gielen, E.; Dupont, J.; Dejaeger, M.; Laurent, M.R. Sarcopenia, osteoporosis and frailty. Metabolism 2023, 145, 155638. [Google Scholar] [CrossRef]
- Huo, Y.R.; Suriyaarachchi, P.; Gomez, F.; Curcio, C.L.; Boersma, D.; Muir, S.W.; Montero-Odasso, M.; Gunawardene, P.; Demontiero, O.; Duque, G. Phenotype of Osteosarcopenia in Older Individuals With a History of Falling. J. Am. Med Dir. Assoc. 2015, 16, 290–295. [Google Scholar] [CrossRef]
- Katz, S; Ford, AB; Moskowitz, RW; Jackson, BA; Jaffe, MW. Studies of Illness in the Aged: The Index of ADL: A Standardized Measure of Biological and Psychosocial Function. JAMA 1963, 185, 914–919. [Google Scholar]
- Welsh, T.J.; Gordon, A.L.; Gladman, J.R. Comprehensive geriatric assessment – a guide for the non-specialist. Int. J. Clin. Pr. 2014, 68, 290–293. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. STEADI—Older Adult Fall Prevention 2021. Available online: https://www.cdc.gov/steadi/index.html.
- Eckstrom, E.; Parker, E.M.; Lambert, G.H.; Winkler, G.; Dowler, D.; Casey, C.M. Implementing STEADI in Academic Primary Care to Address Older Adult Fall Risk. Innov. Aging 2017, 1, igx028. [Google Scholar] [CrossRef]
- Ritchey, K.; Olney, A.; Chen, S.; Phelan, E.A. STEADI Self-Report Measures Independently Predict Fall Risk. Gerontol. Geriatr. Med. 2022, 8, 23337214221079222. [Google Scholar] [CrossRef]
- Kirk-Sanchez, N.; McDonough, C.; Avin, K.G.; Blackwood, J.; Hanke, T.A. Physical Therapy Management of Fall Risk in Community-Dwelling Older Adults: An Evidence-Based Clinical Practice Guideline From the American Physical Therapy Association – Geriatrics. J. Geriatr. Phys. Ther. 2025, 48, 62–87. [Google Scholar] [CrossRef]
- Li, G.; Li, X.; Chen, L. Personally tailored exercises for improving physical outcomes for older adults in the community: A systematic review. Arch. Gerontol. Geriatr. 2022, 101, 104707. [Google Scholar] [CrossRef] [PubMed]
- Sadaqa, M.; Németh, Z.; Makai, A.; Prémusz, V.; Hock, M. Effectiveness of exercise interventions on fall prevention in ambulatory community-dwelling older adults: a systematic review with narrative synthesis. Front. Public Heal. 2023, 11, 1209319. [Google Scholar] [CrossRef]
- Richardson, J.; Beauchamp, M.; Bean, J.; Brach, J.; Chaves, P.H.M.; Guralnik, J.M.; Jette, A.M.; Leveille, S.G.; Hoenig, H.; Manini, T.; et al. Defining and Measuring Preclinical Mobility Limitation: An Expert Consensus Exercise Informed by a Scoping Review. Journals Gerontol. Ser. A 2023, 78, 1641–1650. [Google Scholar] [CrossRef] [PubMed]
- Althubaiti, A. Information bias in health research: definition, pitfalls, and adjustment methods. J. Multidiscip. Healthc. 2016, 9, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Van de Mortel, T.F. Faking it: social desirability response bias in self-report research. Aust. J. Adv. Nurs. 2008, 25, 40. [Google Scholar]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



