Submitted:
22 January 2026
Posted:
26 January 2026
You are already at the latest version
Abstract
Background: Anti–double-stranded DNA (anti-dsDNA) antibodies are a key serological marker for Systemic Lupus Erythematosus (SLE) and are commonly assessed in con-junction with antinuclear antibody (ANA) testing by indirect immunofluorescence (IIF) on HEp-2 cells. However, their detection is influenced both by the heterogeneity of auto-immune response and by the characteristics of the analytical methods employed, com-plicating the diagnostic interpretation. Methods: In this retrospective single-center study, 3,090 patients undergoing anti-dsDNA analysis were screened, and 138 positive indi-viduals, with anti-dsDNA levels ≥15 IU/mL by fluoroenzyme immunoassay (FEIA), were included in the study. A control group of 29 anti-dsDNA–negative patients was also analyzed. Anti-dsDNA–positive patients were stratified by antibody levels (low, mild, high), and results were correlated with HEp-2 IIF titers and fluorescence patterns. In a subset of 30 positive patients, the anti-dsDNA antibodies had also been evaluated using immunoblot (IB) and Crithidia Luciliae indirect Immunofluorescence Test (CLIFT). Sta-tistical analyses assessed associations and concordance among methods. Results: Higher anti-dsDNA levels were generally associated with higher Hep-2 IIF titers. However, a considerable percentage (35%) of patients with positive anti-dsDNA were negative by HEp-2 IIF. Notably, high anti-dsDNA levels were detected in 19% of Hep-2 IIF–negative patients (titer 1:320). In the subset of 30 positive patients, FEIA analysis showed high concordance with immunoblot in both IIF positive (81%) and negative (100%) patients while CLIFT demonstrated lower agreement with both FEIA and IB independently from the IIF. Conclusions: Our findings indicate that anti-dsDNA an-tibody detection may occur independently of HEp-2 IIF positivity and that FEIA, par-ticularly when confirmed by immunoblot, represents a reliable approach for anti-dsDNA assessment. The observed results in this study likely reflect differences in epitope recognition and assay sensitivity among methods, suggesting the use of a multi-step diagnostic strategy in the serological evaluation of SLE.
Keywords:
anti-dsDNA antibody
; systemic lupus erythematous
; FEIA
; immunoblot
; CLIFT
; indirect immunoflorescence
1. Introduction
The detection of antinuclear antibodies (ANA) is one of the immunological parameters included in the classification criteria for systemic lupus erythematosus (SLE), according to both the American College of Rheumatology (ACR) and the Systemic Lupus International Collaborating Clinics (SLICC) [1,2]. Among the various ANA specificities, anti-Sm, anti-Rib-P, and anti-dsDNA antibodies are considered highly specific for SLE. Several studies have investigated the potential of high-avidity anti-dsDNA antibodies in predicting disease onset [3] assessing disease activity and organ damage—particularly renal involvement [4]and monitoring treatment response [5] However, anti-dsDNA antibodies exhibit significant heterogeneity due to the polyclonal and diverse nature of the autoimmune response to native DNA in affected patients [6] a factor that may affect the reliability of the assays used for their detection. Moreover, the presence of anti-dsDNA antibodies is not exclusive to SLE: they may also be detected in other unrelated autoimmune diseases, during infections, after treatment with biologic agents for inflammatory arthritis, and, albeit rarely, in healthy individuals [7]. Therefore, it is essential to confirm a positive anti-dsDNA result with a highly specific test, especially when these antibodies are being used for diagnostic purposes in SLE. Although the Farr assay is still considered the reference method for identifying high-avidity anti-dsDNA antibodies [8], issues related to the use of radioactive substrates have prompted the adoption of alternative non-radioactive methods, such as CLIFT, CLIA, EIA, FEIA, and MFI. In particular, FEIA and CLIA employ antigen-antibody interactions in liquid phase using paramagnetic particles (microbeads), which optimally preserve the conformational structure of epitopes and improve binding affinity [9] Nevertheless, existing methods for anti-dsDNA antibody detection differ in avidity, affinity, antigenic specificity, and substrate type. For this reason, a multi-step approach has been proposed: starting with a highly sensitive screening assay capable of detecting both low- and high-affinity antibodies, followed by a more specific confirmatory test [7]. CLIFT, with a specificity greater than 90% compared to pathological controls, is widely recommended internationally and often used to confirm a positive result obtained through other assays. However, its low diagnostic sensitivity limits its use in primary SLE diagnosis. The present study evaluated the concordance among different analytical methods for anti-dsDNA antibodies measurement and their correlation with the immunofluorescence pattern in Hep-2 cells in order to establish a standardized reporting procedure, especially in cases where there is no concordance of results between the analytical methods and/or the positivity of anti-dsDNA antibodies does not correlate with the expected fluoroscopic pattern.
2. Materials and Methods
2.1. Patient Population Characteristics
This retrospective study was conducted at the Clinical Pathology Unit of the University Hospital “Policlinico Riuniti” of Foggia (Foggia, Italy) between May 2024 and April 2025. The laboratory information system (WEBLAB - Tesi Group - Milan, Italy) was queried to identified all patients for whom anti–double-stranded DNA (anti-dsDNA) antibody testing had been ordered during the study period. Overall, 3,090 consecutive patients were identified, of whom 138 had anti-dsDNA antibody concentrations ≥15 IU/mL, as determined by fluoroenzyme immunoassay (FEIA). A comparison group consisting of 29 patients with anti-dsDNA levels ≤ 14 IU/mL was selected and classified as the negative control cohort. For all patients included in the analysis, indirect immunofluorescence (IIF) patternsonHep-2 cells were collected, based on independent evaluation by two experienced pathologists. Furthermore, anti-dsDNA antibodies were reassessed in a subset of 30 patients using orthogonal methodologies complementary to FEIA, specifically Crithidia Luciliae indirect Immunofluorescence Test (CLIFT) and immunoblotting (IB).
2.2. Fluoroenzyme Immunoassay (FEIA)
Quantitative serum measurement of anti-double stranded DNA (anti-dsDNA) antibodies was performed using the EliA™ dsDNA assay on the fully automated Phadia™ 250 platform (ThermoFisher Scientific), which standardizes and automates all analytical steps. Serum samples were diluted as required and dispensed into microplate wells coated with plasmidic double-stranded DNA, enabling specific capture of anti-dsDNA antibodies. Following several wash steps to remove unbound antibodies, a human anti-IgG secondary antibody conjugated with a fluorescent label was added, along with the appropriate substrate. The resulting fluorescence signal, directly proportional to the concentration of anti-dsDNA antibodies, was then recorded. Each analytical run included calibration curves and/or internal quality control materials. Results were reported as international units per milliliter (IU/mL), and anti-dsDNA levels ≤ 14 IU/mL were considered negative and≥15 IU/mL as positive.
2.3. Indirect Immunofluorescence (IIF)
Anti-Nuclear Antibodies (ANA) and anti-dsDNA antibodies were assessed using indirect immunofluorescence (IIF) on HEp-2 cells and Crithidia Luciliae substrates, respectively. Sample preparation and analysis were performed using the HELIOS automated system (AESKU Diagnostics, Wendelsheim, Germany). HEp-2 pre-coated slides were used to assess nuclear and cytoplasmic fluorescence patterns, whereas Crithidia Luciliae slides were used to detect anti-dsDNA antibodies through visualization kinetoplast fluorescence. Serum samples dilution, incubation, washing, FITC-conjugated anti-human IgG addition, and slide mounting were performed automatically by the HELIOS system in accordance with the manufacturer’s instructions. Fluorescence images were acquired using an integrated high-resolution microscope. Data were analyzed using the HELIOS software, which captured three distinct fields per well and determined sample positivity based on laboratory-validated cut-off values. For Hep-2 IIF, samples exhibiting positive screening fluorescence at ≥1:80 were further titrated in serial dilution (up to 1:1280) to determine endpoint titers. For Crithidia Luciliae IIF, anti-dsDNA positivity was defined by specific fluorescence of the kinetoplast, a structure rich in double-stranded DNA. All results were independently reviewed by two experienced pathologists.
2.4. Immunoblot (IB) Analysis
Serum samples from 30 patients were analyzed using the AESKUBLOTS® ANA-17 PRO system (AESKU Diagnostics, Wendelsheim, Germany), which employs purified or recombinant antigens immobilized on nitrocellulose membrane strips, each placed in a defined and reproducible position. Analyzed autoantigens included: anti-dsDNA, anti-nucleosome, anti-histone, anti-Sm, anti-U1-snRNP, anti-Ro/SSA (60 kDa and 52 kDa), anti-La/SSB, anti-Scl-70, anti-CENP-B, anti-PM-Scl, anti-Jo-1, anti-Mi-2, anti-Ku, anti-ribosomal P0, anti-PCNA, and anti-AMA-M2.The immunoblot procedure was performed using the HELIA instrument (AESKU SYSTEMS, Wendelsheim, Germany). Samples were diluted and processed according to the manufacturer’s instructions. Antigen-specific colorimetric band intensities were evaluated by the HELIA system using its integrated camera and software. Results were classified semi-quantitatively based on signal intensity as either negative (< 0.8) or positive (≥ 0.8). Positive results were further graded by intensity in 3 groups: 0.8–1.5 (score 1), 1.5–2.5 (score 2), and ≥ 2.5 (score 3).
2.5. Data Processing and Statistical Analysis
Data processing and statistical analysis were conducted using R (v.4.2) and IBM SPSS Statistics (v.26). Continuous variables were summarized as mean ± standard deviation (SD).Group comparisons for continuous variables were performed using one-way analysis of variance (ANOVA). Categorical variables were compared using contingency tables and Pearson’s Chi-square test. Analytical concordance between methods was assessed by calculating the percentage agreement. Statistical significance was set at p < 0.05.
3. Results
3.1. Anti-dsDNA Antibody Level
The 138 patients who tested positive for anti-dsDNA antibodies were stratified into three subgroups accordingly to the antibody levels as follow: Low (15–25 IU/mL), Mild (26–49 IU/mL), and High positive (>50 IU/mL). Sixty-three patients (45.6%) exhibited low anti-dsDNA levels, while 46 (33%) and 29 (21%) showed mild and high levels, respectively. Twenty-nine patients testing negative for anti-dsDNA antibodies (≤ 14 IU/mL) were selected as control group. The mean age was 59.7 ± 14.4 years and 54.8 ± 16.6 years in the negative and positive anti-dsDNA groups, respectively. When stratified into subgroups (Table 1), patients with higher anti-dsDNA antibodies levels tended to be younger, although the differences with the other groups were not statistically significant (Anova p= 0.105). Overall, a high female-to-male ratio was observed across all groups, except the high-positive group, which had a more balanced ratio (1.07:1).
3.2. Correlation Between Hep-2 Fluorescence Titers and Plasma Levels of Anti-dsDNA Antibodies
To better understand the relationship between fluorescence patterns in Hep-2 cells and anti-dsDNA antibody levels, we analyzed the HEp-2 IIF titers on the 138 anti-dsDNA positive patients by FEIA. Correlation analysis was performed, regardless of pattern type. Based on HEp-2 IIF results, patients were divided into 3 groups: Negative (titer <1:80), Weakly Positive (titer from 1:80 to 1:160), and Positive (titer from 1:320 to 1:1280). Anti-dsDNA levels increased progressively across subgroups, with mean values of 31.46 ± 18.56 IU/mL in the IIF negative group, 33.59 ± 18.46 IU/mL in the weakly positive group, and 42.29 ± 30.96 IU/mL in the positive group (Figure 1). Moreover, we cross-stratified the 138 patients by Hep-2 IIF titers (negative, weakly positive and positive) and by anti-dsDNA levels (low, mild, and high positive groups). Data reported Table 2 shows that among the Hep-2 IIF negative group, 24 patients (50%) had low anti-dsDNA levels, 15 (31%) had mild levels, and 9 (19%) had high levels. This indicates that even among patients with a negative IIF Hep-2 titer, a notable proportion still had positive anti-dsDNA antibodies, including 19% with high levels. In the IIF Hep-2 weak-positive group, 13 patients (38%) showed low anti-dsDNA levels, 15 (44%) mild levels, and 6 (18%) had high levels. In the IIF Hep-2 positive group, 26 patients (46%) had low levels, 16 (29%) mild levels, and 14 (25%) high levels of anti-dsDNA antibodies. Chi-square analysis indicated no statistically significant association between IIF Hep-2 titers groups and anti-dsDNA levels (Pearson χ² = 2.97, p = 0.563).
3.3. Correlation Between Anti-dsDNA Antibodies and HEp-2 IIF Patterns
In order to explore potential correlations between anti-dsDNA antibodies and HEp-2 IIF patterns, the antibody results were compared with the fluoroscopic profiles. Forty-eight anti-dsDNA-positive patients (35%) were negative by Hep-2 IIF while 65% were IIF-positive. Among positive patients, the following main patterns were observed: homogeneous (22%), fine speckled (13%), coarse speckled (9%), nucleolar (9%), and speckled with positive mitoses (4%). Less frequent patterns, recognized in 8% of cases, were classified as other patterns. They included AC3-Centromeric (N.= 3), AC29-DNA Topoisomerase I-like (N.= 2), AC8-10- Nuclear Dots (N.= 2), AC27-Intracellular Bridges (N.= 1), AC18-Cytoplasmic GW bodies (N.= 1), AC22-Cytoplasmic Golgi-like (N.= 1) and AC21-AMA-like mitochondrial staining (N.= 1) according to the International Consensus on ANA Patterns (ICAP) (Figure 2).
3.4. Comparison of Positivity Rates Across Different Anti-dsDNA Detection Methods
To compare how well different methods may detect anti-dsDNA antibodies, we analyzed a panel of 30 serum samples using several complementary assays. Not all methods were applied to the full set of samples, depending on sample availability (Table 3 and Table S1). Since patients were selected based on the result of FEIA analysis (28 positive and 2 negative), the other methods were tested for their ability to confirm positive or negative cases detected by FEIA. Seventy-three % of FEIA positive patients had positive nuclear patterns on Hep2 cells while 21% were Hep-2 negative. Furthermore 79% and 24% of FEIA positive patients showed positive anti-dsDNA antibodies when measured by immunoblot and CLIFT, respectively. Finally, antibodies against related nuclear antigens were less common, with 10% positivity rate for the nucleosome and none for the histone (Table 3 and S1). When compared with each other FEIA and immunoblot showed consistent results in 86% of cases while CLIFT agreed with the other methods in 32% of cases. Comparative analysis, in patients divided according to nuclear pattern, showed an 81% and 100% agreement between FEIA and immunoblot in patients with positive and negative Hep-2 IIF pattern, respectively. Finally, the agreement between CLIFT and the other two methods was 40% in IIF negative patients and 30% in IIF positive patients (Table 3B and S1).
4. Discussion
The present study investigates, in a cohort of 138 patients testing positive for anti–double-stranded DNA (anti-dsDNA) antibodies, the relationship between this biomarker and the results of indirect immunofluorescence (IIF) analysis on HEp-2 cells, as well as the concordance of results across different analytical technique for anti-dsDNA antibody detection. Given the well-established association between anti-dsDNA antibody titers and disease activity or flares, patients were stratified into three subgroups based on antibody levels—low (15–25 IU/mL), medium (26–49 IU/mL), and high (>50 IU/mL)—to allow a more refined evaluation of the relationships between anti-dsDNA levels and the other parameters examined. In this cohort, 79% of patients exhibited low or medium anti-dsDNA titers, whereas the remaining 21% showed high titers. Although Systemic Lupus Erythematosus (SLE) is known to be more prevalent in females [11], the patients with higher antibody levels displayed a more balanced male-to-female ratio. These findings may suggest that disease activity and severity—often associated with elevated anti-dsDNA titers [12,13,14]—may not be strongly influenced by sex. Furthermore, in Hep-2 IIF–positive patients, anti–dsDNA antibody levels tended to correlate with fluorescence titers, and, in accordance with the literature, the main observed patterns were homogeneous, speckled, and nucleolar. Notably, a substantial proportion of anti–dsDNA–positive patients were surprisingly negative by Hep-2 IIF. Recent studies reported this pattern in both SLE [15] e non SLE cohorts [16] although other ones [17] consider it a rare and uncommon event. In our cohort a considerable number of Hep-2 IIF negative patients displayed medium to high anti-dsDNA antibody levels which could paradoxically indicate a more severe phenotype of the disease. In a subgroup of 30 patients, anti-dsDNA antibody testing was repeated using immunoblot and immunofluorescence on Crithidia Luciliae (CLIFT) for confirmation. An higher concordance was observed between FEIA and immunoblot (86%), whereas concordance between CLIFT and the other methods was lower (32%), as previously reported [18]. Overall, these findings support the notion that anti-dsDNA antibodies may be detected independently of Hep-2 IIF positivity. This observation reinforces the hypothesis that different assays recognize distinct epitopes [15,19,20], some of which may not be adequately represented or accessible in the Hep-2 IIF substrate despite being present in patients’ sera. Importantly, HEp-2 IIF–negative patients retested using alternative methods showed complete concordance between FEIA and immunoblot. Moreover, two IIF negative patients also were positive for anti-nucleosome antibodies, which have been reported to be a more sensitive diagnostic marker for SLE than anti-dsDNA antibodies [21]. These results further support the diagnostic reliability of anti-dsDNA antibody positivity in SLE, even in the absence of Hep-2 IIF reactivity.
Several limitations of this study should be acknowledged, including its single-center design and the relatively limited sample size. Moreover, the lack of detailed clinical information prevented correlation of laboratory findings with patients’ clinical status, such as newly diagnosed disease versus disease flare as well as with the ongoing therapies. While it is evident that future studies including larger and well-characterized cohorts will be necessary to address these issues, the present findings highlight that, in the absence of general guidelines, each case should be carefully evaluated by the clinician to ensure an interpretation that is more consistent with the patient’s clinical condition.
5. Conclusions
This study provides practical laboratory guidance for the management of anti-dsDNA antibody positivity, particularly in patients with negative Hep-2 IIF results. In this cohort, FEIA-positive anti-dsDNA findings warrant re-evaluation using alternative methods, and laboratory reports should include a comment on the concordance or discordance among the different assays. Such an approach may be especially valuable in cases of discrepant results, allowing clinicians to consider longitudinal re-testing when a false-positive result is suspected.
Supplementary Materials
The following supporting information can be downloaded at: Preprints.org, Table S1: Results of anti-dsDNA antibody analysis by FEIA, CLIFT and IB;.
Author Contributions
MP: Conceptualization, Methodology, Data curation, Formal analysis, Validation and investigation, Writing – original draft, Writing – review & editing, CP: Methodology, Data analysis, Writing – review & editing, TT: Data curation , Writing – review & editing, GSN: , Formal analysis , Writing – review & editing, ER: Formal analysis , Writing – review & editing, GC: Conceptualization, Methodology, Formal analysis, Supervision, Writing – review & editing. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the Polyclinic Riuniti of Foggia (prot. n. 106/CE/2025 – June 30th 2025).
Data Availability Statement
No new data were created for this study. Patients data unavailable due to patient’s privacy.
Acknowledgments
We would like to thank laboratory technicians Maria Adele Rinaldi, Giuseppina De Laurentiis, and Loredana Iacuzio for their precise and professional routine analyses, Dr. Loredana Iafelice for her contribution to data collection, and Dr. Oceania D’Apolito for her valuable input in interpreting part of the results.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Aringer M, Costenbader K, Daikh D, Brinks R, Mosca M, Ramsey-Goldman R, et al. 2019 European League AgainstRheumatism/American College of Rheumatologyclassificationcriteria for systemic lupus erythematosus. AnnRheumDis.2019 Sep;78(9):1151-1159. Epub 2019 Aug 5. PMID: 31383717. [CrossRef]
- Petri M, Orbai AM, Alarcón GS, Gordon C, Merrill JT, Fortin PR, et al. Derivation and validation of the Systemic Lupus International Collaborating Clinics classification criteria for systemic lupus erythematosus. ArthritisRheum. 2012 Aug;64(8):2677-86. PMID: 22553077; PMCID: PMC3409311. [CrossRef]
- Arbuckle MR, McClain MT, Rubertone MV, Scofield RH, Dennis GJ, James JA, Harley JB. Development of autoantibodies before the clinical onset of systemic lupus erythematosus. N Engl J Med. 2003 Oct 16;349(16):1526-33. PMID: 14561795. [CrossRef]
- Andrejevic S, Jeremic I, Sefik-Bukilica M, Nikolic M, Stojimirovic B, Bonaci-Nikolic B. Immunoserological parameters in SLE: high-avidity anti-dsDNA detected by ELISA are the most closely associated with the disease activity. ClinRheumatol. 2013 Nov;32(11):1619-26. Epub 2013 Jul 16. PMID: 23857662. [CrossRef]
- Swaak T, Smeenk R. Clinical significance of antibodies to double stranded DNA (dsDNA) for systemic lupus erythematosus (SLE). ClinRheumatol. 1987 Jun;6 Suppl 1:56-73. PMID: 3304800. [CrossRef]
- Fillatreau S, Manfroi B, Dörner T. Toll-like receptor signalling in B cells during systemic lupus erythematosus. Nat Rev Rheumatol.2021 Feb;17(2):98-108. Epub 2020 Dec 18. PMID: 33339987; PMCID: PMC7747191. [CrossRef]
- Compagno M, Jacobsen S, Rekvig OP, Truedsson L, Heegaard NH, Nossent J, Jönsen A, Jacobsen RS, Eilertsen GØ, Sturfelt G, Bengtsson AA. Low diagnostic and predictive value of anti-dsDNA antibodies in unselected patients with recent onset of rheumatic symptoms: results from a long-term follow-up Scandinavian multicentre study. Scand J Rheumatol. 2013;42(4):311-6. Epub 2013 Mar 16. PMID: 23496224. [CrossRef]
- Agmon-Levin N, Damoiseaux J, Kallenberg C, Sack U, Witte T, Herold M, et al. International recommendations for the assessment of autoantibodies to cellular antigens referred to as anti-nuclear antibodies. Ann Rheum Dis. 2014 Jan;73(1):17-23. Epub 2013 Oct 14. PMID: 24126457. [CrossRef]
- Ghirardello A, Villalta D, Morozzi G, Afeltra A, Galeazzi M, Gerli R, et al. Forum Interdisciplinare per la Ricerca sulle Malattie Autoimmuni(FIRMA) study group. Diagnostic accuracy of currently available anti-double-stranded DNA antibody assays. An Italian multicentre study. ClinExpRheumatol. 2011 Jan-Feb;29(1):50-6. Epub 2011 Feb 23. PMID: 21345292.
- Albrecht K, Troll W, Callhoff J, Strangfeld A, Ohrndorf S, Mucke J. Sex- and gender-related differences in systemic lupus erythematosus: a scoping review. Rheumatol Int. 2025 Jun 27;45(7):160. PMID: 40576834; PMCID: PMC12204902. [CrossRef]
- Somers EC, Marder W, Cagnoli P, Lewis EE, et al. Population-based incidence and prevalence of systemic lupus erythematosus: the Michigan Lupus Epidemiology and Surveillance program. Arthritis Rheumatol. 2014 Feb;66(2):369-78. PMID: 24504809; PMCID: PMC4198147. [CrossRef]
- Pan N, Amigues I, Lyman S, Duculan R, Aziz F, Crow MK, Kirou KA. A surge in anti-dsDNA titer predicts a severe lupus flare within six months. Lupus. 2014 Mar;23(3):293-8. Epub 2013 Dec 6. PMID: 24316605. [CrossRef]
- Narayanan K, Marwaha V, Shanmuganandan K, Shankar S. Correlation between Systemic Lupus Erythematosus Disease Activity Index, C3, C4 and Anti-dsDNA Antibodies. Med J Armed Forces India. 2010 Apr;66(2):102-7. Epub 2011 Jul 21. PMID: 27365721; PMCID: PMC4920905. [CrossRef]
- Olson SW, Lee JJ, Prince LK, Baker TP, Papadopoulos P, Edison J, Abbott KC. Elevated subclinical double-stranded DNA antibodies and future proliferative lupus nephritis. Clin J Am SocNephrol. 2013 Oct;8(10):1702-8. Epub 2013 Jul 5. PMID: 23833315; PMCID: PMC3789337. [CrossRef]
- Abozaid HSM, Hefny HM, Abualfadl EM, Ismail MA, Noreldin AK, Eldin ANN, Goda AM, Ali AH. Negative ANA-IIF in SLE patients: what is beyond? Clin Rheumatol. 2023 Jul;42(7):1819-1826. Epub 2023 Apr 4. PMID: 37016193; PMCID: PMC10267001. [CrossRef]
- Uzun GS, Apsley E, Isenberg D. Identification of patients with ANA-negative and double-stranded DNA positive: what is the significance in daily rheumatology practice? Clin Rheumatol. 2025 Feb;44(2):863-865. Epub 2024 Dec 24. PMID: 39718671. [CrossRef]
- Robier C, Haas M, Quehenberger F. The clinical relevance of anti-dsDNA antibodies determined by the Elia™ dsDNA assay in patients with negative indirect immunofluorescence on the HEp-2 cell. ClinChem Lab Med. 2020 Oct 16;59(3):541-546. PMID: 33064668. [CrossRef]
- Trujillo Aguilera A, Bernardo Serrano R, Navas A, Alcaide Molina J, Alvarez Romero P, Jurado Roger A. Longitudinal study of patients with discrepant results in CLIFT and a solid-phase dsDNA antibody assay: does a gold standard dsDNA assay exist? Lupus Sci Med. 2023 Oct;10(2):e000984. PMID: 37903589; PMCID: PMC10618974. [CrossRef]
- Cuomo L, Vitillo M, Della Rocca M, Trivedi P. Comparative analysis of three methods in anti-dsDNA antibodies detection: implications for Systemic Lupus Erythematosus diagnosis. Scand J Immunol. 2022 Feb;95(2):e13123. Epub 2021 Dec 12. PMID: 34865261. [CrossRef]
- Infantino M, Palterer B, Previtali G, Alessio MG, Villalta D, Carbone T, et al. Comparison of current methods for anti-dsDNA antibody detection and reshaping diagnostic strategies. Scand J Immunol. 2022 Dec;96(6):e13220. Epub 2022 Oct 10. PMID: 36373656. [CrossRef]
- Bizzaro N, Villalta D, Giavarina D, Tozzoli R. Are anti-nucleosome antibodies a better diagnostic marker than anti-dsDNA antibodies for systemic lupus erythematosus? A systematic review and a study of metanalysis. Autoimmun Rev. 2012 Dec;12(2):97-106. Epub 2012 Jul 15. PMID: 22810055. [CrossRef]
Figure 1.
Anti-dsDNA level stratified by Hep-2 IIF positivity. (A) Anti-dsDNA groups: Low= 15-25 IU/ml (white dots); Mild= 26-49 IU/ml (grey dots); High= over 50 IU/ml (red dots). Hep-2 IIF groups: Negative= <1:80; Weak positive= 1:80-1:160; Positive=1:320-1:1280. (B) Anti-dsDNA mean levels distribution across Hep-2 IIF groups. The differences did not reach statistical significance (ANOVA, p = 0.061), although a trend toward higher anti-dsDNA levels with increasing HEp-2 IIF titers was observed.
Figure 1.
Anti-dsDNA level stratified by Hep-2 IIF positivity. (A) Anti-dsDNA groups: Low= 15-25 IU/ml (white dots); Mild= 26-49 IU/ml (grey dots); High= over 50 IU/ml (red dots). Hep-2 IIF groups: Negative= <1:80; Weak positive= 1:80-1:160; Positive=1:320-1:1280. (B) Anti-dsDNA mean levels distribution across Hep-2 IIF groups. The differences did not reach statistical significance (ANOVA, p = 0.061), although a trend toward higher anti-dsDNA levels with increasing HEp-2 IIF titers was observed.
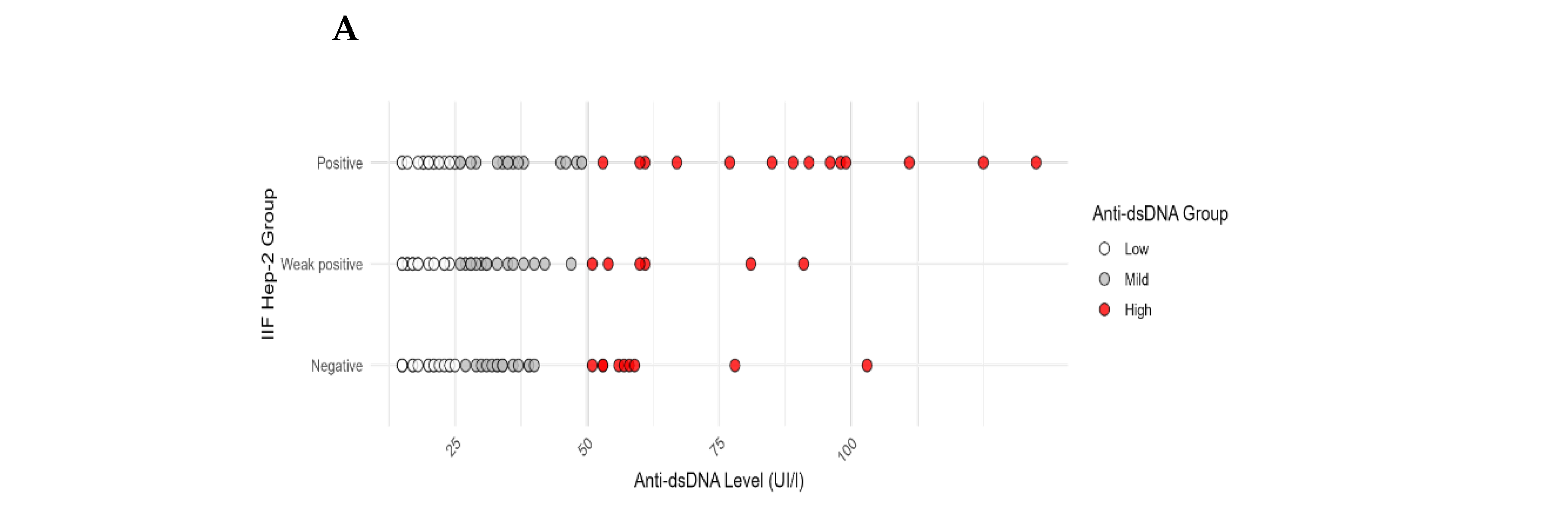
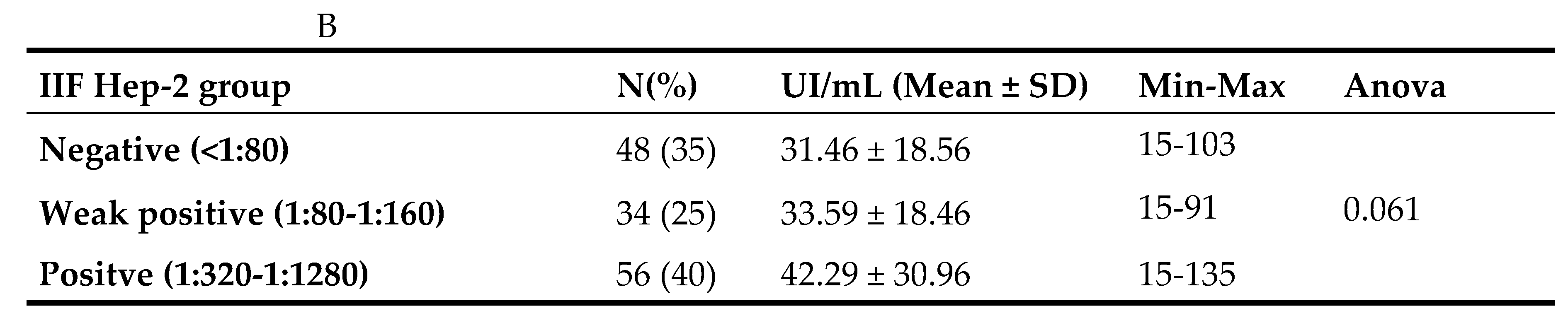
Figure 2.
Hep-2 IIF pattern across anti-dsDNA positive patients. Distribution of Hep-2 IIF pattern within the selected patients. The percentage of cases found for each type of IIF pattern is shown in the pie chart while the number of samples is shown in brackets.
Figure 2.
Hep-2 IIF pattern across anti-dsDNA positive patients. Distribution of Hep-2 IIF pattern within the selected patients. The percentage of cases found for each type of IIF pattern is shown in the pie chart while the number of samples is shown in brackets.
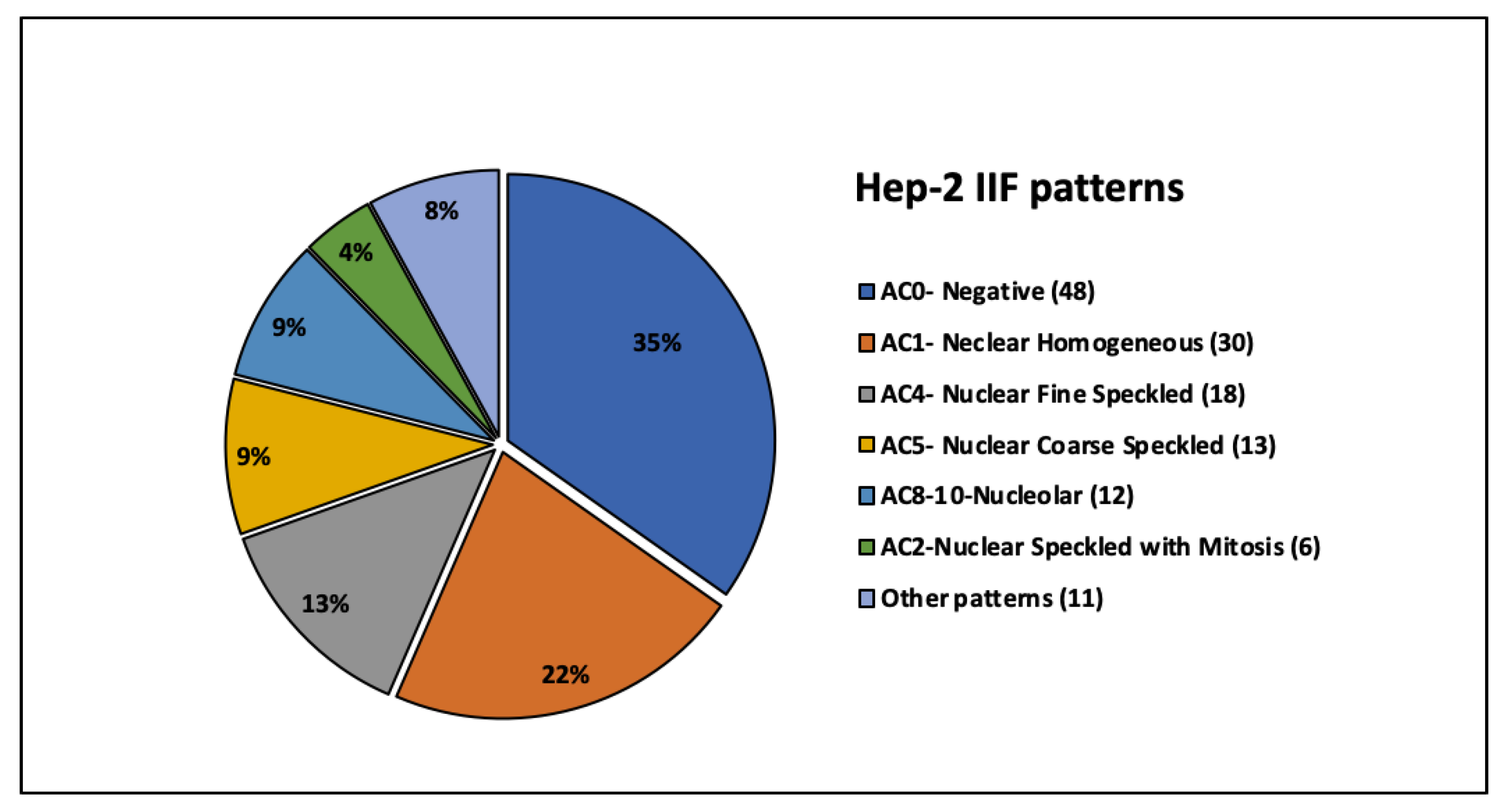

Table 1.
Cross-comparison of anti-dsDNA levels and patient age.
| Anti-dsDNAgroup | N | Anti-dsDNA (IU/mL) | Age Mean ± SD |
| Negative (≤14 IU/mL) | 29 | 8.6 ± 2.7 | 59.4 ± 14.9 |
| Low (15–25 IU/mL) | 63 | 19.1 ± 3.4 | 57.8 ± 17.4 |
| Mild (26–49 IU/mL) | 46 | 34.8 ± 6.4 | 53.3 ± 16.4 |
| High (≥50 IU/mL) | 29 | 76.3 ± 23.7 | 50.8 ± 14.1 |
| Anova | p=0.105 |
Table 2.
Distribution of numbers (N) of patients accordingly to Hep-2 IIF and Anti-dsDNA groups. No statistically significant differences were observed across subgroups. (Chi-square Pearson =2.9695 p=0.5629);.
Table 2.
Distribution of numbers (N) of patients accordingly to Hep-2 IIF and Anti-dsDNA groups. No statistically significant differences were observed across subgroups. (Chi-square Pearson =2.9695 p=0.5629);.
| Hep-2 IIF group | Tot | Anti-dsDNA Low | Anti-dsDNA Mild | Anti-dsDNA High |
| (15-25 UI/mL) | (26-49 UI/mL) | (over 50 UI/mL) | ||
| N (%) | N (%) | N (%) | ||
| Negative <1:80 | 48 | 24 (50) | 15 (31) | 9 (19) |
| Weak positive (1:80-1:160) | 34 | 13 (38) | 15 (44) | 6 (18) |
| Positive (1:320-1:1280) | 56 | 26 (46) | 16 (29) | 14 (25) |
| Tot | 138 | 63 (46) | 46 (33) | 29 (21) |
Table 3.
Cross-comparison among complementary methods. (A) Prevalence of positive nuclear pattern and anti-dsDNA antibodies tested by FEIA, Immunoblot, and CLIFT in an independent set of 30 samples. Immunoblot results for anti-dsDNA associated antibodies (nucleosome and histones) are also reported. (B) Percentage of agreement across different anti-dsDNA detection methods in Hep2- positive and negative groups.
Table 3.
Cross-comparison among complementary methods. (A) Prevalence of positive nuclear pattern and anti-dsDNA antibodies tested by FEIA, Immunoblot, and CLIFT in an independent set of 30 samples. Immunoblot results for anti-dsDNA associated antibodies (nucleosome and histones) are also reported. (B) Percentage of agreement across different anti-dsDNA detection methods in Hep2- positive and negative groups.
| A | ||||
| Marker | N | Positive (%) | Negative (%) | NA |
| Cell pattern (IIF-Hep2) | 30 | 22 (73) | 8 (27) | -- |
| dsDNA (FEIA) | 30 | 28 (93) | 2 (7) | -- |
| dsDNA (Immunoblot) | 29 | 23 (79) | 6 (21) | 1 |
| dsDNA (CLIFT) | 25 | 6 (24) | 19 (76) | 5 |
| Nucleosome (Immunoblot) | 29 | 3 (10.3) | 26 (89.7) | 1 |
| Histone (Immunoblot) | 29 | 0 (0) | 100 (100) | 1 |
| B | ||||
| Anti-dsDNApositivity concordance (%) | ||||
| FEIA vs IB (agreement %) | FEIA vs CLIFT (agreement %) |
IB vs CLIFT (agreement %) |
||
| IIF-Hep2 negative | 100 | 40 | 40 | |
| IIF-Hep2 positive | 81 | 30 | 30 | |
| IIF-Hep2 (all) | 86 | 32 | 32 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



