
Submitted:
19 January 2026
Posted:
20 January 2026
You are already at the latest version
Abstract
Introduction: Gymnastic exercises exert positive effects on chronic neck pain. Growing evidence suggests that combining cervical spine exercises with temporomandibular joint (TMJ) relax pads, may enhance outcomes on pain, discomfort and functional limitations. Objective: To evaluate the additive effect of silicone TMJ relax pads worn in the molar region during cervical spine exercises on reducing neck pain and improving function. Methods: 52 sedentary middle-aged to older adults working on video display unit (VDU) workstations were randomly assigned to two groups. Both groups performed a specific cervical spine exercise program (3x 3min/day) for three months. One group used bilateral TMJ relax pads during the sessions (EX-RP); the control group exercised without pads (EX). Neck pain intensity was assessed using a one-week pain protocol prior and after a six-week intervention. Functional assessments included cervical/thoracic spine and shoulder mobility tests, and thoracic kyphosis angle measurement. Intention-to-treat analysis with multiple imputation was performed. Results: Data from 25 EX-RP and 22 EX participants were analysed. Both groups showed reduced neck pain, but only EX-RP achieved a statistically significant reduction (p=.001). Pain reduction was greater in EX-RP than in EX (p=.046). Neck Disability Index (NDI) scores improved in both groups (p <.001), with no significant difference between groups (p =.514). EX-RP showed greater improvements in cervical extension (p=.044) and trunk rotation (p=.019). Conclusion: Combining cervical exercises with TMJ relax pads may enhance pain reduction and functional outcomes in individuals with chronic neck pain.
Keywords:
chronic neck pain
; exercise therapy
; TMJ relax pads
; VDU work
Introduction
Chronic non-specific neck pain is a common orthopaedic condition. According to the Global Burden of Disease study, neck pain ranks fourth among the leading causes of years lived with disability (Hoy et al. 2014). Neck and lower back pain are also the fourth most prevalent causes of Disability-Adjusted Life Years (DALYs) worldwide, following ischaemic heart disease, cerebrovascular disease, and respiratory infections (Hurwitz et al. 2018). Over the past 25 years, the prevalence of neck and lower back pain – and the associated limitations in daily life – has increased significantly (Hurwitz et al. 2018). A representative German study found that, at the time of the survey, 18% of the population had experienced neck pain and 25% had suffered from lower back pain within the previous three months (Häuser et al. 2013). The high incidence of neck pain is largely attributed to modern lifestyles, which are often characterised by physical inactivity and prolonged static postures, especially at work. Sedentary work at video display unit (VDU) workstations is a significant risk factor in the development of chronic non-specific neck pain (Johnston et al. 2008). In contrast, physical activity and exercise are of major importance in both the prevention and treatment of neck pain. For example, a meta-analysis has clearly demonstrated that targeted exercise programs can improve pain and function in people with chronic non-specific neck pain (Höppchen et al.).
The close bidirectional relationship between cervical and orofacial disorders has been discussed in several studies (Ciancaglini et al. 1999; De Laat et al. 1998), based on mechanical-functional and neuroanatomical correlations (Walczyńska-Dragon & Baron 2011). There is strong evidence for a high correlation between neck pain and temporomandibular joint (TMJ) dysfunction (Olivo et al. 2010). Studies have shown that acute occlusal interventions using occlusal splints can positively influence posture, balance, and postural alignment, as well as postural control, gait and running biomechanics, and physical performance (Bracco et al.; 1998; Maurer et al.; 2018; Maurer et al. 2015). Since research has indicated that the dynamic interaction between the upper and lower jaw can affect muscle strength in other regions of the body, occlusal splints have also been used in recent years to enhance athletic performance (Arent et al. 2010; Herzog et al. 2022; Lee et al. 2014). Sedentary work is frequently associated with complaints in both the cervical spine and the TMJ region, with 42% of women working at VDUs with cervical spine complaints also presenting with TMJ dysfunction (Bragatto et al. 2016). Given these craniocervical and orofacial interconnections, integrating the orofacial region into the management of neck pain may offer a promising therapeutic approach. This study explored an innovative method using silicone TMJ relax pads placed in the molar region during specific therapeutic exercises. It was hypothesised that combining TMJ relax pads with exercises would enhance their effect on neck pain and related symptoms. As this is a novel approach, no clinical trials have been conducted so far.
The exact effects and mechanisms of TMJ relax pads have not yet been scientifically studied. In contrast to conventional occlusal splints, TMJ relax pads are designed to induce a slight jaw-stretching posture and promote relaxation of the masticatory muscles. This pragmatic effectiveness study aims to fill this gap by evaluating whether the use of TMJ relax pads during cervical-targeted gymnastic exercises enhances their therapeutic impact on neck pain and associated functional limitations.
Material and Methods
Study Objectives
By designing and evaluating a training program that is easy to implement in everyday life and by investigating a possible additive effect of a TMJ relax pads, the study aims to contribute to the optimization of care for patients with neck pain.
Hypotheses
Primary Hypothesis
The use of TMJ relax pads during specific gymnastics exercises significantly reduces neck pain compared to identical gymnastics exercises without the use of TMJ relax pads.
Secondary Hypothesis
The use of TMJ relax pads during gymnastics exercises leads to a significant (1) reduction in neck pain-related impairment in everyday life (Neck Disability Index (NDI), (2) improvement in mobility of the cervical spine, (3) increase in the rotational ability of the trunk , (4) increase in mobility (elevation ability) in the shoulder joint area, (5) reduction in the kyphosis angle of the thoracic spine in an upright position.
Study Design and Ethical Approval
This is a monocentric, partially blinded, randomized clinical intervention study (RCT) with a parallel group design, involving participants from the Erlangen-Nuremberg area. The study was conducted at the Institute of Medical Physics at Friedrich-Alexander-Universität Erlangen-Nürnberg. Ethical approval for the study was granted by the ethics committee (number 130-21b) and the data protection officer of the FAU. The study adheres to the ethical standards outlined in the Declaration of Helsinki by the World Medical Association (World Medical Association 2013) and is fully registered at ClinicalTrials.gov (NCT05302466). All participants provided written informed consent prior to their involvement in the study. Figure 1. illustrates the chronological sequence of the study.
Study Population
Based on the a priori power analysis (see biometrics), a total of 52 participants, were recruited according to the following eligibility criteria. Inclusion criteria: (a) men and women aged between 30-65 years, (b) chronic non-specific neck pain (at least for 3 months on 50% of the days, with a pain intensity of ≥2 on the Nominal Rating Scale NRS (Höppchen et al.)), and (c) sedentary activity and VDU workstation use. Exclusion criteria: (a) specific neck pain (e.g., herniated disc, spinal stenosis, etc.), (b) cervical spine-related neuronal symptoms (e.g., paresthesia, brachial plexus pain, etc.). (c) the use of long-term pain medication, (d) the concurrent administration of other therapies with the potential to influence neck pain, (e) an absence exceeding two weeks during the intervention period, and (f) the performance of regular specific exercises or training focusing on the cervical spine within the previous six months. After receiving comprehensive information during individual interviews and having time for reflection, all participants provided written consent to participate in the study (Figure 1).
Randomisation and Blinding
The 52 participants were randomly assigned to either an experimental group (EX-RP, n=26) or a control group (EX, n=26) stratified by the “pain intensity” (Figure 1). In detail, the participants were allocated to the two groups by drawing lots from a bowl. The tickets were individually contained in small opaque capsules (“Kinder-Ei”, Ferrero, Italy). A researcher not involved in this project prepared the lots and supervised the randomization procedure. Thus, neither the researcher nor the participants were aware of the allocation in advance, thus ensuring the blinding of the study (“allocation concealment”). Following randomization, the principal investigator provided the participants with detailed information of the procedures. Due to the nature of the study, blinding at the participant level was not feasible. Additionally, the study director was aware of the participants’ group status (EX-RP or EX). However, all individuals involved in the testing and analysis were blinded to the group status and were prohibited from inquiring about the final grouping.
Interventions
Gymnastics Program (EX-RP and EX)
The two groups were subjected to an identical exercise program of “usual care” comprising of three distinct three-minute sequences to be performed daily. At the beginning of the study, each participant received individualized instructions and guidance on the correct execution of the exercises. As the study progressed, the participants were required to perform the exercise programs independently, using video animations and their own personal devices (mobile phone, tablet, notebook, PC). The relevant film sequences were made available to the participants for download. If participants had any questions or concerns, they could seek individual guidance or to engage in a video consultation via the “FAU Zoom” platform. Compliance was recorded daily in the training diary. Telephone contact was maintained with the participants at two-week intervals for three purposes: (a) to document the implementation of the protocol, (b) to identify and address any protocol deviations or implementation issues, and (c) to encourage consistent adherence to the program.
The specific physical training consisted of three different exercise programs, each to be performed daily. Each program comprised of three exercises, each lasting one minute (approximately 10-15 Repetitions), resulting in a total duration of three minutes per program. The programs included low-intensity gymnastic exercises from functional and therapeutic gymnastics aimed at activating, loosening, and stretching the muscles, with a focus on the shoulder-neck region and the cervical spine.
The morning program, performed standing, focused on full spine and upper body mobility through active exercises. The first exercise involved rotating the head to one side while performing a retrograde shoulder circle. The second exercise extended the arms backward and downward while engaging the glutes, lowering the head to the occiput. The third exercise involved extending the arms to shoulder height, contracting the glutes, and sequentially moving one arm to the side while orienting the head towards the hand.
The noon program, performed seated, focused on stretching and stabilizing the shoulder, neck, and cervical spine. The first exercise involved rounding the back, allowing the head to hang, then extending the upper body and protracting the chest. The second exercise involved bending to one side while keeping one hand on the chair. The third exercise involved rotating the arms outwards, extending the elbows to 90°, and rotating the upper body with the head directed posteriorly.
The evening program, performed supine, aimed to enhance spinal and shoulder mobility. The first exercise involved bending the knees to one side, elevating the contralateral arm, and orienting the head toward the hand. The second exercise focused on pressing the glutes upwards while rolling down the spine. The third exercise, performed prone, involved alternating lateral leg movements while resting the arms and head on the floor.
TMJ Relax Pads
The TMJ relax pads TJ Motion (TJ Motion GmbH & Co. KG, Weisendorf, Germany) are manufactured using medical silicone (Figure 2). The splints are placed on the back molars of the lower jaw (area between tooth 34 and approximately 36 or between tooth 44 and 46). Once positioned, the mouth should be closed loosely. In the event of a gag reflex becoming apparent, the TMJ relax pads should be placed slightly further forward (33 to approximately 35 or between teeth 43 and 45). These pads are to be maintained in this position throughout the exercise, which is to be performed for a period of three minutes.
Confounders: Medication Supply with Painkillers
If necessary, medication with oral painkillers (NSAIDs) was administered as prescribed by the attending physician. The use of NSAIDs was recorded daily in the training diary and was also discussed during the biweekly telephone contacts.
Outcomes Measures and Assessment Schedule
Primary Study Endpoint
Change in neck pain on the “Numeric Rating Scale” (NRS) between basal assessment and control measurement after the 12-week intervention
Secondary Study Endpoints
- Change in the Neck Disability Index (NDI) between basal assessment and control measurement after the 12-week intervention
- Change in mobility (lateral flexion, flexion, extension, rotation) of the cervical spine between basal assessment and control measurement after the 12-week intervention
- Change in mean trunk rotation between basal assessment and control measurement after the 12-week intervention
- Change in elevation ability of the shoulder joints (degree) between basal assessment and control measurement after the 12-week intervention
- Change in kyphosis angle between basal assessment and control measurement after the 12-week intervention
Neck Pain (NRS)
Pain intensity was recorded daily using the Numeric Rating Scale (NRS, 0-10) in a pain diary, for one week prior to commencing the intervention and during the 12th week of the intervention. Pain intensity as the primary endpoint is defined as the mean value over one week in each case.
Limitations Due to Neck Complaints
The German version of the Neck Disability Index (NDI) was used to record neck complaints (Cramer et al. 2014; MacDermid et al. 2009; Trouli et al. 2008; Vernon & Mior 1991). The NDI questionnaire is utilized to document complaints and problems during everyday activities caused by the cervical spine.
Flexibility, Mobility and Posture
The mobility analysis of the cervical spine (range of motion (ROM)) (Fletcher & Bandy 2008; Howell 2011) was performed via sensor-based digital recording of the maximum range of motion of flexion, extension, lateral flexion and rotation (in degrees), during active performance in a seated position (Mobeefit SportMed A.G. SA, Echternach, Luxembourg). For flexion and lateral flexion, the mean value of both directions of movement (right, left) was calculated. The position sensor was attached to the head resembling a headlamp using an elastic strap. The mean rotational mobility of the torso was determined in a similar sensor-based manner in a seated position, with the sensor placed on the sternum (breastbone).
Shoulder mobility was determined by ROM (Riddle et al. 1987; Sabari et al. 1998; Shin et al. 2017) by means of end-range active flexion in a seated position (bilateral synchronized exercise with a gymnastic rod) employing a goniometer. The goniometer measurement was performed on the right shoulder.
Kyphosis
The kyphosis angle was evaluated in an upright position using a Debrunner kyphometer (Protek, Bern, Switzerland), in accordance with the method proposed by Ohlen et al. (Ohlen et al. 1988).
Craniomandibular Dysfunction
The prevalence of CMD (Craniomandibular Dysfunction) was determined using a CMD short report according to Ahlers and Jakstat (Ahlers & Jakstat 2008), which includes the following criteria: (1) asymmetrical opening of the mouth, (2) restricted opening of the mouth, (3) joint noises, (4) occlusal noises, (5) painful muscle palpation, and (6) traumatic eccentricity.
Biometrics and Statistical Analysis
The biometric and statistical analysis was conducted by an independent statistician. The number of participants was planned through an a priori case number analysis based on the primary endpoint, “pain intensity of neck complaints”. It was hypothesized that there would be an overall reduction in pain intensity of at least 20% (standard deviation ±25%), which was considered to be a clinically relevant minimum. The statistical analysis indicated that, assuming the standard statistical parameters (α: 5%, 1-β: 80%), a sample size of 26 participants per group was deemed sufficient to address the primary endpoint.
It was applied the intention to treat principle that included all participants randomly assigned to the study arms regardless of their loss to follow-up. R statistics software (R Development Core Team Vienna, Austria) were applied in combination with Amelia II (Honaker et al. 2011) for multiple imputation (ITT). The full data set was used for multiple imputation, with imputation repeated 100 times. The primary analysis focus on differences between the intragroup changes in EX-RP versus EX, using analysis of covariance (ANCOVA) adjusted for differences in baseline data. Further, after checking the normal distribution of the data (gg-plots, residual plots), all study results presented here were analyzed by dependent t-tests with pooled SD. The chi-square test was utilized for categorical variables (see Table 1). All tests were two-sided and a significance level of p < 0.05 was accepted.
Results
Table 1 presents the baseline characteristics of the study participants. The baseline characteristics did not significantly differ between the groups. Specifically, there were no statistically significant differences observed in terms of prevalent illnesses or medication regimens.
A total of five participants (EX-RP: n=1 vs. EX: n=4) were unable to participate in the follow-up study. Specifically, two EX participants reported that they had lost interest in the study, primarily due to randomization into the non-preferred (control) group. One EX participant cited a road accident as the reason for their withdrawal. Another participant cited pain during or due to the gymnastic exercises as the reason for withdrawing. In the EX-RP, one person was no longer able or willing to carry out the intervention or FU measurement due to a death in the close surrounding.
The rate of physical training was found to be 68.4 ± 28.5% in the control group and 75.8 ± 19.0% in the EX-RP group. The training frequency of the groups did not differ significantly (p = 0.314). Subsequent analyses of the participants’ records and telephone interviews revealed that the exercise of the EX-RP-Group were consistently performed with the TMJ Relax Pads.
Study Endpoints
Primary Study Endpoint: Intensity of Neck Pain
ITT analysis demonstrated a reduction in the average pain intensity in both groups. However, this reduction was only found to be significant (p=.001) for the EX-RP. Even after adjustment to the basal values via ANCOVA, the reduction in pain intensity was significantly more stated in the EX-RP (p=.046) than in the EX.

Table 2.
Basal values and changes in neck pain intensity (primary outcome) with statistical parameters: TMJ relax pads group (EX-RP) versus control group (EX). MV: mean value; SD: standard deviation; 95% CI: 95%: Confidence interval; * via ANCOVA adjusted for basal differences between the groups.
Table 2.
Basal values and changes in neck pain intensity (primary outcome) with statistical parameters: TMJ relax pads group (EX-RP) versus control group (EX). MV: mean value; SD: standard deviation; 95% CI: 95%: Confidence interval; * via ANCOVA adjusted for basal differences between the groups.
| EX-RP (n=26) MV ± SD |
EX (n=26) MV ± SD |
Difference MV (95% CI) |
p-value | |
|---|---|---|---|---|
| Neck pain intensity [Index] | ||||
| Basal value | 2.93± 1.72 | 2.66± 1.79 | ------------- | .661 |
| Change | -1.46± 1.90 | -0.45± 1.82 | 0.98 (0.02 to 1.95)* | .046* |
In this respect, it verifies the primary hypothesis that “the use of TMJ relax pads during gymnastics exercises significantly reduces neck pain compared to identical gymnastics exercises without the use of TMJ relax pads”.
Secondary Study Endpoints
The Neck Disability Index (NDI) exhibited a significant positive change during the intervention period in both groups (p<.001 each) (see Table 3). The difference between the groups was not significant (p=.514), thereby rejecting the secondary hypothesis 1.
Range of motion in flexion exhibited a significant positive change in both groups (EX-RP: p=.002 vs. EX: p=.016). No significant differences were observed between the groups (p=.581). In contrast, the analysis of mobility during extension of the cervical spine revealed significant positive changes in the EX-RP (p=.002) but not in the EX (p=.35). This finding was reflected in significant effects (p=.044) in favor of the EX-RP group. For the rotation of the cervical spine (see Table 3), significant improvements in mobility were recorded in both groups (EX-RP: p<.001 vs EX: p=.020). Although the changes within the EX-RP were more pronounced, a between-group comparison (ANCOVA) showed no significant effects for the EX-RP group (p=.405). Thus, secondary hypothesis 2 can only partially be confirmed.
Trunk rotation (see Table 3) exhibited a substantial enhancement in rotational performance in both groups (EX-RP: p<.001 vs EX: p=.006). A significant between-group difference was observed in favor of the TJ group (p=.019). This outcome serves to confirm the secondary hypothesis 3.
Both groups demonstrated a significant enhancement in shoulder mobility (p < .001 each). A significant difference between the groups was not recorded (p=.667). Consequently, we can reject hypothesis 4.
Following the 12-week period of intervention, a reduction in kyphosis angle was observed in both groups. However, this change was only found to be statistically significant in the EX-RP group (p<.005 vs. EX: p=.074). The differences between the groups for the changes from the basal measurement to the 12-week control measurement (12-week FU) were not significant (p=.634). Consequently, hypothesis 5 was rejected.
A sub-analysis was conducted within the TMJ relax pads group to ascertain whether the prevalence of CMD had an influence on the treatment effects. A comparison was made between subjects with and without CMD, and no significant differences were observed in the effect of the intervention on pain (p = .523) or NDI (p = .730). A further analysis of the pure gymnastics group revealed no significant differences in the effects on pain and NDI in subjects without CMD compared to those with CMD.
Adverse Effects
None of the EX-RP participants reported any undesirable side effects. Some participants reported increased saliva production during application. One participant in the control group reported pain when performing the gymnastic exercises, otherwise no difficulties or particularities were reported during or after the exercises.
Potential Confounding Variables
No relevant changes in lifestyle, physical activity, illness or medication (especially analgesics) were reported by the participants that could have influenced our results. However, one participant in the EX-RP had an accident in intervention week 7 and suffered whiplash, which, according to the participant, prevented her from continuing with the intervention (though not from completing the final measurement).
Discussion
This study investigated the additive effect of TMJ relax pads when performing a high-frequency exercise program with short, three times daily exercise sequences that can be easily integrated into everyday life. The exercise program demonstrated a substantial positive effect on pain, cervical spine-related restrictions in everyday life, spinal and shoulder mobility and posture. These were significantly increased using TMJ relax pads regarding the primary endpoint “neck pain intensity” and the secondary endpoints “cervical spine extension flexibility” and “trunk mid-rotation flexibility”.
The approach applied in this study represents an innovative and previously unique method for the treatment of neck pain. The management of neck pain is supported by combining gymnastic exercises with the use of a dental splint worn during exercise. The TMJ relax pads utilized in the study are also not directly comparable with the occlusal splints that are generally applied. Despite the limited comparability, the TMJ relax pads will be differentiated from the occlusal splints below, and the results of this study will be discussed against the background of the results of other studies (Incorvati et al. 2020).
The utilization of occlusal splints is endorsed by the guideline of the German Society of Dentistry, Oral and Maxillofacial Medicine (DGZMK) (DGZMK 2024) particularly in the treatment of CMD. Meta-analyses have demonstrated that corresponding splints have a significant effect on pain reduction when used for muscular and atherogenic complaints, in comparison with no therapy (Al-Moraissi et al. 2020; Zhang et al. 2020).
The DGZMK guideline classifies occlusal splints into four categories. The first group comprises of relaxation splints or stabilizing splints, with the Michigan splint (Badel et al. 2013) serving as a prime example. These splints which are worn in both the upper and lower jaw, generally have a flat contact and are particularly indicated for chewing muscle and/or temporomandibular joint pain and bruxism (Wassell et al. 2006)
The second group consists of reflex splints, which are characterized by the presence of point or linear contacts on specific teeth. These contacts have been shown to inhibit masticatory muscle activity (Hannam et al. 1981). Their utilization in the initial treatment of myogenic dysfunctions, along with their application in the elimination of occlusal instability, has been documented (Stapelmann & Türp 2008).
The third group comprises of positioning splints. The function of this type of splint is to modify the position of the condyle-discus complex with the aim to provide relief to the temporomandibular joint structures. These splints are used for the management of painful disc displacements and inflammatory atherogenic dysfunctions (Eberhard et al. 2002; Guo et al. 2021; Lakshmi et al. 2016).
The fourth group encompasses a range of splints, including customized soft splints. One such example is the Aqualizer - a hydrostatic mouth splint that automatically eliminates the distorting influence of the maxillomandibular relationship, thus harmonizing the muscles, bite and body (Srivastava et al. 2013). These splints are inserted in the acute treatment of CMD complaints; however, they are not utilized in the long term.
In addition to the splints mentioned by the DGZMK, sport splints can be mentioned, which generally does not pursue a therapeutic approach, but is intended to improve athletic performance by changing posture when wearing the splint (Herzog et al. 2022).
The TMJ relax pads (TJ-Motion) employed in this study differ from the previously mentioned splints regarding design, shape and material. The majority of the commonly used splints cover the entire row of teeth of the upper and lower jaw, have a thinner layer thickness than the TJ-Motion and are usually made of plastics such as PMMA (Benli et al. 2023) or polycarbonate. They are often customized for the respective patient. In contrast, the TJ-Motion typically covers a smaller area, limited to 2-3 premolars or molars, and does not involve connection of the two pads. It has a layer thickness of 8.5 mm, is made of medical silicone and is not customized to the individual patient.
The duration over which conventional splints are worn varies significantly across studies; however, most of the research indicates that they are used either nocturnally or during the day. The present study proposes the utilization of TMJ relax pads with significantly reduced wearing intervals, consisting of three sessions of three minutes per day. The TMJ Relax Pads can be worn during exercises and in everyday activities, such as desk work.
The scope of application of TMJ relax pads differs from that of conventional dental splints. Occlusal splints, aside from sports splints, are primarily used for the treatment of bruxism and temporomandibular disorders (TMD). According to clinical guidelines, a key objective of occlusal splint therapy for TMD is to modify the functional patterns of the masticatory muscles and optimize the condylar position within the temporomandibular joint. This approach aims to relieve structures subjected to excessive or improper loading, even in the absence of a splint (Albagieh et al. 2023).
The TJ-Motion does not induce a targeted and individual correction of the jaw position. Rather, it is intended to stretch and relax hypertonic jaw muscles through increased layer thickness. Hypertonicity in these muscles can negatively affect adjacent regions, particularly the cervical spine, by contributing to increased muscular tension and impaired function. The correlation between the jaw and the cervical spine has been thoroughly documented in the existing literature, with studies indicating the potential to influence the musculoskeletal system and its associated complaints by altering the position of the temporomandibular joint (Grondin et al. 2017). Weber et al. (Weber et al. 2012) found that women with TMD also have more frequent signs of cervical dysfunction and neck pain. In the study by Walczyńska-Dragon et al. (Walczyńska-Dragon et al. 2014) it is reported that following a period of three months during which patients were treated for TMD with the use of splints, a significant improvement in the mobility of the cervical spine and a reduction in spinal pain was achieved in the treatment group. Odzimek and Brola (Odzimek & Brola 2024) found that neck pain is significantly more prevalent and more intense in patients diagnosed with temporomandibular joint (TMJ) disorder. Furthermore, they described that the mobility of the cervical spine is more restricted in TMD patients than in healthy individuals.
It should be noted that CMD was not an inclusion criterion in this study. The incidence of CMD was found to be equally distributed across both groups, with a notable prevalence of approximately 75% observed. However, a sub-analysis revealed no significant difference in treatment outcomes between individuals with and without CMD. Thus, regardless of the prevalence of CMD, the use of the TMJ Relax Pads has the potential to positively influence cervical spine dysfunctions. In the present study, a reduction in the intensity of neck pain was observed in both study groups; however, only the pain reduction of the EX-RP group was significant (p.001). It should be noted that the existing literature has focused on either gymnastic exercises or isolated splint therapy, thus limiting the scope for direct comparison (Kang 2020). In the study by Shousha et al. (Shousha et al. 2018), a direct comparison was made between conservative physiotherapy, predominantly hands-on in nature, and occlusal splinting, with the former achieving greater pain relief and improvement in movement. However, it should be noted that the study by Shousha et al. refers to patients diagnosed with TMD, and the intervention group of that study used isolated splint therapy. This is not the case in the present study.
Regarding the NDI, a significant improvement was observed in both study groups; however, the difference between the EX and EX-RP was not significant. A meta-analysis by Bertozzi et al. (Bertozzi et al. 2013) shows, in line with the present results, that therapeutic exercises cause significant improvements in the NDI. However, a comparison is only possible to a limited extent, as only the results of isolated exercises were analyzed. The literature review found no study that directly measured the NDI in relation to splints. As other parameters of pain and function were measured, the search on the effects of splint therapy yielded only indirect correlations between the effects of a dental splint and the NDI. An enhancement in cervical spine mobility regarding flexion was observed in both groups, with no significant difference between them. However, a more notable enhancement was evident in the EX-RP group with respect to cervical spine extension. No improvement was observed in the EX-group. A significant improvement was recorded in the rotation of the cervical spine in both groups without significant difference between the groups. Tereshchuk’s study (Tereshchuk 2024) concluded that the utilization of relaxation splints can achieve both an enhancement in mobility and a reduction in pain for patients suffering from chronic neck pain. The improvement in mobility of the cervical spine through splint therapy or other adjustment of the occlusion was also found in several other studies (Karppinen et al. 1999; Walczyńska-Dragon et al. 2014). Nevertheless, the examination in these studies was limited to splint therapy or occlusion adjustment, excluding the combination with gymnastic exercises, which consequently restricts the comparability of the findings.
Regarding shoulder mobility and mid-torso rotation, no studies were identified in the current literature search that would permit comparability.
The EX-RP group demonstrated a marked improvement in the kyphosis angle, although this difference was not statistically significant. In some studies, positive effects on posture (Ohlendorf et al. 2014; Sakaguchi et al. 2007) and also on the kyphosis angle (De Giorgi Dds et al. 2020; März et al. 2017) have been achieved by changing the position of the lower jaw, using splints. However, the study results are largely inconsistent, and the influence of splint therapy is generally discussed controversially (Giannakopoulos et al. 2018; Hampe et al. 2024; Kang 2020; Lippold et al. 2006; Maurer-Grubinger et al. 2020; Sofyanti et al. 2021).
The significant limitations that result in the poor comparability of individual studies are the absence of methodological standardization, the inability to differentiate between muscular, articular, or combined TMD, and the failure to distinguish between physio pathological conditions and risk factors (Sofyanti et al. 2021).
The present study’s design precludes the drawing of any conclusions regarding the mechanism of action. It is hypothesized that the stretching stimulus of the temporomandibular joint (TMJ) associated with the positioning of TMJ relax pads in the molar region could lead to a reduction in tension in hypertonic muscles in the entire jaw and shoulder-neck area via myofascial and neuronal pathways. This reduction in tension could, in turn, have a positive influence on the symptoms of chronic cervical spine syndrome. The craniocervical-orofacial connections that could underpin this effect have been described in numerous publications (Ciancaglini et al. 1999; De Laat et al. 1998). Nevertheless, it is important to emphasize that the discussion of potential underlying mechanisms remains speculative.
Finally, the gymnastics program will be discussed, which demonstrated significant effects on pain intensity, NDI and function even without TMJ relax pads. Apart from the extension of the cervical spine and the kyphosis angle of the thoracic spine, all values of the functional examinations also improved significantly on the EX-group.
A multitude of studies have been conducted regarding the impact of exercise programs on chronic non-specific neck pain. These studies have been summarized in a meta-analysis. The exercise programs of the included studies vary considerably in terms of frequency (once a week to two times a day), duration (7-60 minutes), intervention period (4 weeks to 12 months) and content (stretching vs. strengthening exercises, whole-body vs. local neck exercises, as well as endurance exercises). The majority of these programs, despite their marked differences, demonstrated a significant improvement in neck pain intensity (Louw et al. 2017).
In contrast to the majority of the studies included in the meta-analysis, which worked less frequently and with a longer training duration, a high-frequency program with a very short training duration was designed. This program can be easily integrated into everyday life and is conducive to the development of habits. The relatively high compliance rate (68.4 ± 28.5% and 75.8 ± 19.0% in the EX-RP group in the control group) and low drop-out rate (EX-RP: n=1 vs. EX: n=4) demonstrate the program’s success in terms of feasibility. Given the investigation’s focus on the additional effect of the TMJ Relax Pads, it was imperative that the exercises were standardized and identical for all patients. The utilization of video instruction in this context was found to be an effective approach.
It is important to acknowledge the distinctive characteristics and limitations inherent to the study. Primarily, the absence of a comparison group for the gymnastics program, in the form of a zero group, diminishes the informative value. Secondly, despite a comparatively low and moderate drop-out rate (less than 10%), ‘lost-to-follow-up’ data had to be imputed via the intention-to-treat (ITT) approach of the study. Experience has shown (Mostazir et al. 2021) that the results are in some cases significantly more cautious (i.e., tend to be less positive) than in per-protocol analyses. This was demonstrated in an additional analysis for the primary study endpoint, ‘neck pain intensity’, where the per-protocol analysis revealed a significantly higher significance level (p=.006) for the between-group effect. Thirdly, the possibility exists that discrepancies in the implementation rate between the groups (EX: 68.4 ± 28.5% vs. TJR 75.8 ± 19.0%, p = .157) may be a contributing factor to the observed positive effect of the TMJ relax pads. However, statistical adjustment for this factor (ANCOVA) did not demonstrate any significant changes in the results.
As there is an absence of any comparable data in the extant literature, this study can be regarded as a pilot study. The results obtained appear to be promising, and it is therefore recommended that further research be conducted in this area.
Furthermore, additional research is needed to determine whether the effects of the TMJ relax pads are more pronounced in certain groups of participants compared to others. The efficacy of the pads may also be influenced by modifications to the application protocol, with respect to duration or timing of use. An interesting question to explore would be whether the potential of the pads to alleviate neck pain exists even without the inclusion of gymnastic exercises. In summary, TMJ relax pads enhanced the effect of a short, thrice-daily exercise program specifically designed for neck problems. In conclusion, TMJ relax pads could contribute to the optimization of care for patients suffering from chronic neck pain.
Clinical Relevance
- Combining TMJ relax pads with cervical exercises improved the functional outcomes in office workers with chronic non-specific neck pain.
- The combined intervention led to greater reductions in neck discomfort and disability than exercise alone
- It is non-evasive, easy to integrate into therapy sessions and requires no additional setup or expertise
Author Contributions
Conceptualization, NK, WK, SvS; methodology, NK, MK, WK, SvS; software, MK; validation, NK, RL, WK, SvS; formal analysis, MK, WK.; investigation, NK, RL; resources, WK, SvS.; data curation, NK, RL, SvS; writing—original draft preparation, NK, RL, MK, WK, SvS; writing— NK, RL, MK, WK, SvS; funding acquisition, WK, SvS. All authors have read and agreed to the published version of the manuscript.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial or non-profit-sectors.
Institutional Review Board Statement
Ethical approval for the study was granted by the FAU Erlangen-Nürnberg ethics committee (number 130-21b).
Informed Consent Statement
All participants were fully informed about the risks of the study and gave written informed consent.
Data Availability Statement
The datasets generated and/or analysed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
We would like to thank all participants who took part in the study and dedicated their time and effort to complete the intervention period. This work was conducted in partial fulfillment of the requirements for obtaining the degree “Dr. med. dent” at the Friedrich-Alexander-Universität Erlangen-Nürnberg (FAU), Germany, by the first author.
Use of Artificial Intelligence
During the preparation of this work the authors used Chat GPT (Open AI) for language refinement and grammar correction. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Conflicts of Interest
The authors declare no conflicts of interest related to this study.
References
- 2013 World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. Jama 310, 2191-2194. [CrossRef]
- Ahlers MO, Jakstat HA 2008 Identifikation funktionsgestörter Patienten. Zahnmedizin up2date 2, 143-155. [CrossRef]
- Al-Moraissi, EA; Farea, R; Qasem, KA; Al-Wadeai, MS; Al-Sabahi, ME; Al-Iryani, GM. Effectiveness of occlusal splint therapy in the management of temporomandibular disorders: network meta-analysis of randomized controlled trials. Int J Oral Maxillofac Surg 2020, 49, 1042–1056. [Google Scholar] [CrossRef] [PubMed]
- Albagieh, H; Alomran, I; Binakresh, A; Alhatarisha, N; Almeteb, M; Khalaf, Y; Alqublan, A; Alqahatany, M. Occlusal splints-types and effectiveness in temporomandibular disorder management. The Saudi Dental Journal 2023, 35, 70–79. [Google Scholar] [CrossRef] [PubMed]
- Arent, S; McKenna, J; Golem, D. Effects of a neuromuscular dentistry-designed mouthguard on muscular endurance and anaerobic power. 2010, 7, 73–79. [Google Scholar] [CrossRef]
- Badel, T; Simonić-Kocijan, S; Lajnert, V; Dulčić, N; Zdravec, D. Michigan splint and treatment of temporomandibular joint. Medicina fluminensis 2013, 49, 112–120. [Google Scholar]
- Benli, M; Al-Haj Husain, N; Ozcan, M. Mechanical and chemical characterization of contemporary occlusal splint materials fabricated with different methods: a systematic review. Clinical Oral Investigations 2023, 27, 7115–7141. [Google Scholar] [CrossRef]
- Bertozzi, L; Gardenghi, I; Turoni, F; Villafañe, JH; Capra, F; Guccione, AA; Pillastrini, P. Effect of Therapeutic Exercise on Pain and Disability in the Management of Chronic Nonspecific Neck Pain: Systematic Review and Meta-Analysis of Randomized Trials. Physical Therapy 2013, 93, 1026–1036. [Google Scholar] [CrossRef]
- Bracco, P; Deregibus, A; Piscetta, R; Ferrario, G. Observations on the correlation between posture and jaw position: a pilot study. Cranio 1998, 16, 252–258. [Google Scholar] [CrossRef]
- Bragatto, MM; Bevilaqua-Grossi, D; Regalo, SC; Sousa, JD; Chaves, TC. Associations among temporomandibular disorders, chronic neck pain and neck pain disability in computer office workers: a pilot study. J Oral Rehabil 2016, 43, 321–332. [Google Scholar] [CrossRef]
- Ciancaglini, R; Gherlone, EF; Radaelli, G. Association between loss of occlusal support and symptoms of functional disturbances of the masticatory system. J Oral Rehabil 1999, 26, 248–253. [Google Scholar] [CrossRef]
- Cramer, H; Lauche, R; Langhorst, J; Dobos, GJ; Michalsen, A. Validation of the German version of the Neck Disability Index (NDI). BMC Musculoskelet Disord 2014, 15, 91. [Google Scholar] [CrossRef]
- De Giorgi Dds, I; Castroflorio Dds, PT; Cugliari Msc, G. Deregibus Md DDSPA 2020 Does occlusal splint affect posture? A randomized controlled trial. CRANIO® 38, 264–272.
- De Laat, A; Meuleman, H; Stevens, A; Verbeke, G. Correlation between cervical spine and temporomandibular disorders. Clin Oral Investig 1998, 2, 54–57. [Google Scholar] [CrossRef]
- Deutsche Gesellschaft für Zahn- M-uKD 2024 Okklusionsschienen zur Behandlung craniomandibulärer Dysfunktionen und zur präprothetischen Therapie; Berlin.
- Eberhard, D; Bantleon, HP; Steger, W. The efficacy of anterior repositioning splint therapy studied by magnetic resonance imaging. European Journal of Orthodontics 2002, 24, 343–352. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, JP; Bandy, WD. Intrarater reliability of CROM measurement of cervical spine active range of motion in persons with and without neck pain. J Orthop Sports Phys Ther 2008, 38, 640–645. [Google Scholar] [CrossRef]
- Giannakopoulos, NN; Schindler, HJ; Hellmann, D. Co-contraction behaviour of masticatory and neck muscles during tooth grinding. J Oral Rehabil 2018, 45, 504–511. [Google Scholar] [CrossRef] [PubMed]
- Grondin, F; Hall, T; von Piekartz, H. Does altered mandibular position and dental occlusion influence upper cervical movement: A cross–sectional study in asymptomatic people. Musculoskeletal Science and Practice 2017, 27, 85–90. [Google Scholar] [CrossRef]
- Guo, Y-n; Cui, S-j; Zhou, Y-h; Wang, X-d. An Overview of Anterior Repositioning Splint Therapy for Disc Displacement-related Temporomandibular Disorders. Current Medical Science 2021, 41, 626–634. [Google Scholar] [CrossRef]
- Hampe, T; Fürstberger, L; Kordsmeyer, TL; Penke, L; Mahler, AM; Mäder, CM; Bürgers, R; Krohn, S. Impact of occlusal stabilization splints on global body posture: a prospective clinical trial. Clinical Oral Investigations 2024, 28, 505. [Google Scholar] [CrossRef] [PubMed]
- Hannam, AG; Wood, WW; De Cou, RE; Scott, JD. The effects of working-side occlusal interferences on muscle activity and associated jaw movements in man. Archives of Oral Biology 1981, 26, 387–392. [Google Scholar] [CrossRef]
- Häuser, W; Schmutzer, G; Hinz, A; Hilbert, A; Brähler, E. Prevalence of chronic pain in Germany. A representative survey of the general population. Schmerz 2013, 27, 46–55. [Google Scholar] [CrossRef]
- Herzog, J; Göttfert, F; Maurer-Grubinger, C; Holzgreve, F; Oremek, G; Groneberg, DA; Ohlendorf, D. Improvement of cervical spine mobility and stance stability by wearing a custom-made mandibular splint in male recreational athletes. PLoS One 2022, 17, e0278063. [Google Scholar] [CrossRef]
- Honaker, J; King, G; Blackwell, M. Amelia II: A Program for Missing Data. Journal of Statistical Software 2011, 45, 1–47. [Google Scholar] [CrossRef]
- Hopewell, S; Chan, A-W; Collins, GS; Hróbjartsson, A; Moher, D; Schulz, KF; Tunn, R; Aggarwal, R; Berkwits, M; Berlin, JA; Bhandari, N; Butcher, NJ; Campbell, MK; Chidebe, RCW; Elbourne, D; Farmer, A; Fergusson, DA; Golub, RM; Goodman, SN; Hoffmann, TC; Ioannidis, JPA; Kahan, BC; Knowles, RL; Lamb, SE; Lewis, S; Loder, E; Offringa, M; Ravaud, P; Richards, DP; Rockhold, FW; Schriger, DL; Siegfried, NL; Staniszewska, S; Taylor, RS; Thabane, L; Torgerson, D; Vohra, S; White, IR. Boutron I 2025 CONSORT 2025 statement: updated guideline for reporting randomised trials. The Lancet 405, 1633–1640. [CrossRef]
- Höppchen, I; Wittek, M; Szecsenyi, J. Diagnostik bei Nackenschmerzen.
- Howell, E. The association between neck pain, the Neck Disability Index and cervical ranges of motion: a narrative review. The Journal of the Canadian Chiropractic Association 2011, 55, 211–221. [Google Scholar]
- Hoy, D; March, L; Woolf, A; Blyth, F; Brooks, P; Smith, E; Vos, T; Barendregt, J; Blore, J; Murray, C; Burstein, R; Buchbinder, R. The global burden of neck pain: estimates from the Global Burden of Disease 2010 study. Annals of the Rheumatic Diseases 2014, 73, 1309–1315. [Google Scholar] [CrossRef] [PubMed]
- Hurwitz, EL; Randhawa, K; Yu, H; Côté, P; Haldeman, S. The Global Spine Care Initiative: a summary of the global burden of low back and neck pain studies. Eur Spine J 2018, 27, 796–801. [Google Scholar] [CrossRef]
- Incorvati, C; Romeo, A; Fabrizi, A; Defila, L; Vanti, C; Gatto, MRA; Marchetti, C; Pillastrini, P. Effectiveness of physical therapy in addition to occlusal splint in myogenic temporomandibular disorders: protocol of a randomised controlled trial. BMJ Open 2020, 10, e038438. [Google Scholar] [CrossRef]
- Johnston, V; Jull, G; Souvlis, T; Jimmieson, NL. Neck movement and muscle activity characteristics in female office workers with neck pain. Spine (Phila Pa 1976) 2008, 33, 555–563. [Google Scholar] [CrossRef] [PubMed]
- Kang, J-H. Effects on migraine, neck pain, and head and neck posture, of temporomandibular disorder treatment: Study of a retrospective cohort. Archives of Oral Biology 2020, 114, 104718. [Google Scholar] [CrossRef] [PubMed]
- Karppinen, K; Eklund, S; Suoninen, E; Eskelin, M; Kirveskari, P. Adjustment of dental occlusion in treatment of chronic cervicobrachial pain and headache. Journal of Oral Rehabilitation 1999, 26, 715–721. [Google Scholar] [CrossRef]
- Lakshmi, MS; Kalekhan, SM; Mehta, R; Bhangdia, M; Rathore, K; Lalwani, V. Occlusal Splint Therapy in Temporomandibular Joint Disorders: An Update Review. Journal of International Oral Health 2016, 8, 639–645. [Google Scholar] [CrossRef]
- Lee, SY; Park, YJ; Park, HM; Bae, HJ; Yu, MJ; Choi, HW; Hwang, NY. Effect of the Mandibular Orthopedic Repositioning Appliance (MORA) on Forearm Muscle Activation and Grasping Power during Pinch and Hook Grip. J Phys Ther Sci 2014, 26, 195–197. [Google Scholar] [CrossRef] [PubMed]
- Lippold, C; Danesh, G; Schilgen, M; Drerup, B; Hackenberg, L. Sagittal jaw position in relation to body posture in adult humans – a rasterstereographic study. BMC Musculoskeletal Disorders 2006, 7, 8. [Google Scholar] [CrossRef]
- Louw, S; Makwela, S; Manas, L; Meyer, L; Terblanche, D; Brink, Y. Effectiveness of exercise in office workers with neck pain: A systematic review and meta-analysis. S Afr J Physiother 2017, 73, 392. [Google Scholar] [CrossRef]
- MacDermid, JC; Walton, DM; Avery, S; Blanchard, A; Etruw, E; McAlpine, C; Goldsmith, CH. Measurement properties of the neck disability index: a systematic review. J Orthop Sports Phys Ther 2009, 39, 400–417. [Google Scholar] [CrossRef]
- März, K; Adler, W; Matta, R-E; Wolf, L; Wichmann, M; Bergauer, B. Can different occlusal positions instantaneously impact spine and body posture? Journal of Orofacial Orthopedics/Fortschritte der Kieferorthopadie 2017, 78. [Google Scholar] [CrossRef] [PubMed]
- Maurer, C; Heller, S; Sure, JJ; Fuchs, D; Mickel, C; Wanke, EM; Groneberg, DA; Ohlendorf, D. Strength improvements through occlusal splints? The effects of different lower jaw positions on maximal isometric force production and performance in different jumping types. PLoS One 2018, 13, e0193540. [Google Scholar] [CrossRef]
- Maurer, C; Stief, F; Jonas, A; Kovac, A; Groneberg, DA; Meurer, A; Ohlendorf, D. Influence of the Lower Jaw Position on the Running Pattern. PLoS One 2015, 10, e0135712. [Google Scholar] [CrossRef]
- Maurer-Grubinger, C; Avaniadi, I; Adjami, F; Christian, W; Doerry, C; Fay, V; Fisch, V; Gerez, A; Goecke, J; Kaya, U; Keller, J; Krüger, D; Pflaum, J; Porsch, L; Wischnewski, C; Scharnweber, B; Sosnov, P; Oremek, G; Groneberg, DA; Ohlendorf, D. Systematic changes of the static upper body posture with a symmetric occlusion condition. BMC Musculoskeletal Disorders 2020, 21, 636. [Google Scholar] [CrossRef]
- Mostazir, M; Taylor, G; Henley, WE; Watkins, ER; Taylor, RS. Per-Protocol analyses produced larger treatment effect sizes than intention to treat: a meta-epidemiological study. Journal of Clinical Epidemiology 2021, 138, 12–21. [Google Scholar] [CrossRef]
- Odzimek, M; Brola, W. Occurrence of Cervical Spine Pain and Its Intensity in Young People with Temporomandibular Disorders. Journal of Clinical Medicine 2024, 13, 1941. [Google Scholar] [CrossRef] [PubMed]
- Ohlen, G; Aaro, S; Bylund, P. The sagittal configuration and mobility of the spine in idiopathic scoliosis. Spine (Phila Pa 1976) 1988, 13, 413–416. [Google Scholar] [CrossRef]
- Ohlendorf, D; Seebach, K; Hoerzer, S; Nigg, S; Kopp, S. The effects of a temporarily manipulated dental occlusion on the position of the spine: a comparison during standing and walking. The Spine Journal 2014, 14, 2384–2391. [Google Scholar] [CrossRef] [PubMed]
- Olivo, SA; Fuentes, J; Major, PW; Warren, S; Thie, NM; Magee, DJ. The association between neck disability and jaw disability. J Oral Rehabil 2010, 37, 670–679. [Google Scholar] [CrossRef]
- Riddle, DL; Rothstein, JM; Lamb, RL. Goniometric reliability in a clinical setting. Shoulder measurements. Phys Ther 1987, 67, 668–673. [Google Scholar] [CrossRef] [PubMed]
- Sabari, JS; Maltzev, I; Lubarsky, D; Liszkay, E; Homel, P. Goniometric assessment of shoulder range of motion: comparison of testing in supine and sitting positions. Arch Phys Med Rehabil 1998, 79, 647–651. [Google Scholar] [CrossRef]
- Sakaguchi, K; Mehta, NR; Abdallah, EF; Forgione, AG; Hirayama, H; Kawasaki, T; Yokoyama, A. Examination of the Relationship Between Mandibular Position and Body Posture. CRANIO® 2007, 25, 237–249. [Google Scholar] [CrossRef]
- Shin, YJ; Kim, WH; Kim, SG. Correlations among visual analogue scale, neck disability index, shoulder joint range of motion, and muscle strength in young women with forward head posture. J Exerc Rehabil 2017, 13, 413–417. [Google Scholar] [CrossRef]
- Shousha, TM; Soliman, ES; Behiry, MA. The effect of a short term conservative physiotherapy versus occlusive splinting on pain and range of motion in cases of myogenic temporomandibular joint dysfunction: a randomized controlled trial. J Phys Ther Sci 2018, 30, 1156–1160. [Google Scholar] [CrossRef]
- Sofyanti, E; Boel, T; Sihombing, ARN. The correlation between back posture and sagittal jaw position in adult orthodontic patients. Journal of Taibah University Medical Sciences 2021, 16, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, R; Jyoti, B; Devi, P. Oral splint for temporomandibular joint disorders with revolutionary fluid system. Dent Res J (Isfahan) 2013, 10, 307–313. [Google Scholar]
- Stapelmann, H; Türp, JC. The NTI-tss device for the therapy of bruxism, temporomandibular disorders, and headache – Where do we stand? A qualitative systematic review of the literature. BMC Oral Health 2008, 8, 22. [Google Scholar] [CrossRef]
- Tereshchuk. EFFECT OF USING A RELAXATION SPLINT ON REDUCING CHRONIC NECK PAIN. Ukrainian Dental Almanac 2024, 61–65. [Google Scholar] [CrossRef]
- Trouli, MN; Vernon, HT; Kakavelakis, KN; Antonopoulou, MD; Paganas, AN; Lionis, CD. Translation of the Neck Disability Index and validation of the Greek version in a sample of neck pain patients. BMC Musculoskelet Disord 2008, 9, 106. [Google Scholar] [CrossRef]
- Vernon, H; Mior, S. The Neck Disability Index: a study of reliability and validity. J Manipulative Physiol Ther 1991, 14, 409–415. [Google Scholar]
- Walczyńska-Dragon, K; Baron, S. The biomechanical and functional relationship between temporomandibular dysfunction and cervical spine pain. Acta Bioeng Biomech 2011, 13, 93–98. [Google Scholar] [PubMed]
- Walczyńska-Dragon, K; Baron, S; Nitecka-Buchta, A; Tkacz, E. 2014 Correlation between TMD and Cervical Spine Pain and Mobility: Is the Whole Body Balance TMJ Related? BioMed Research International 2014, 582414. [Google Scholar] [CrossRef]
- Wassell, RW; Adams, N; Kelly, PJ. The treatment of temporomandibular disorders with stabilizing splints in general dental practice: one-year follow-up. J Am Dent Assoc 2006, 137, 1089-1098; quiz 1168-1089. [Google Scholar] [CrossRef]
- Weber, P; Corrêa, EC; Ferreira Fdos, S; Soares, JC; Bolzan Gde, P; Silva, AM. Cervical spine dysfunction signs and symptoms in individuals with temporomandibular disorder. J Soc Bras Fonoaudiol 2012, 24, 134–139. [Google Scholar] [CrossRef]
- Zhang, S-H; He, K-X; Lin, C-J; Liu, X-D; Wu, L; Chen, J; Rausch-Fan, X. Efficacy of occlusal splints in the treatment of temporomandibular disorders: a systematic review of randomized controlled trials. Acta Odontologica Scandinavica 2020, 78, 580–589. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Participant flow through the study (Hopewell et al., 2025).
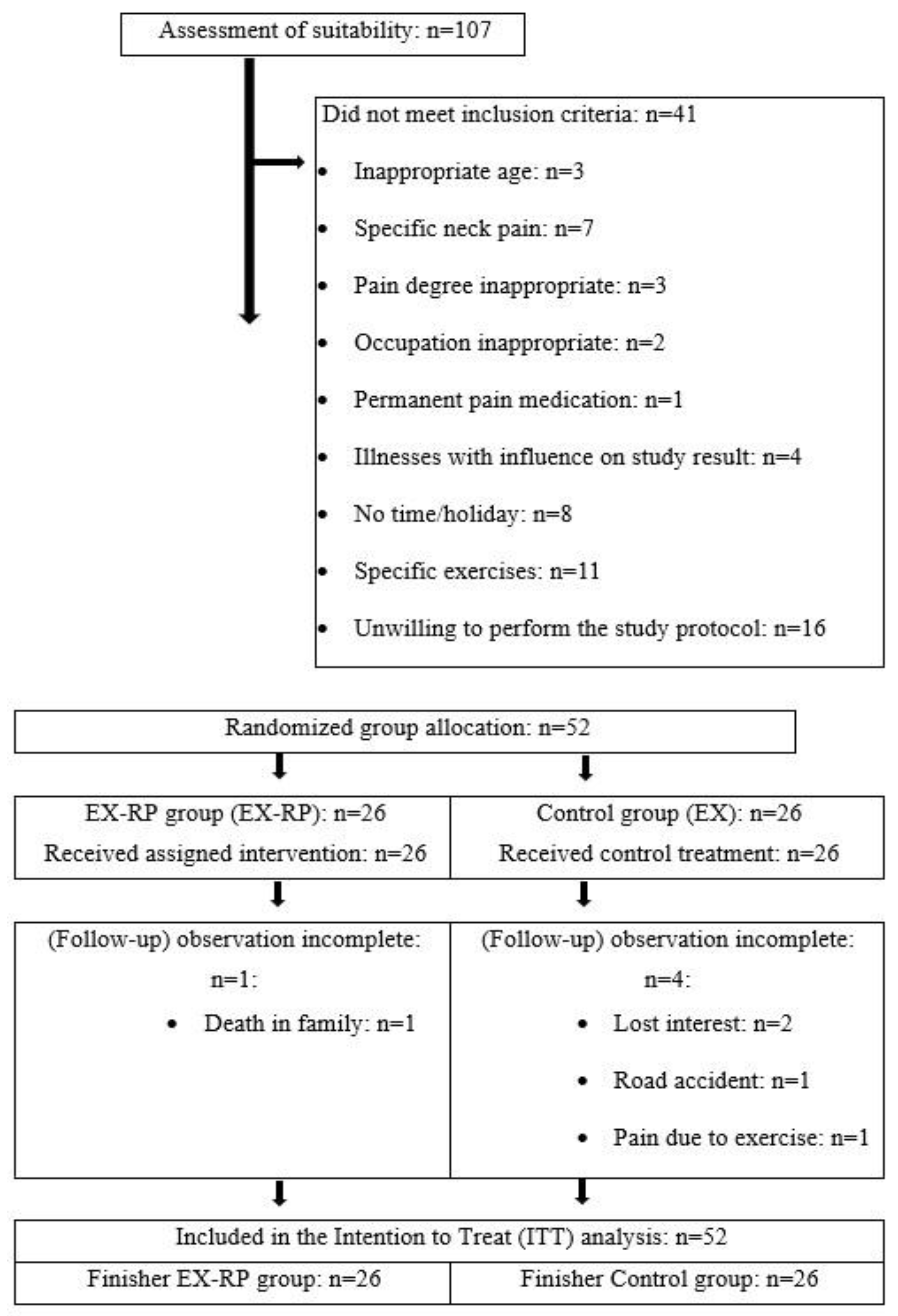
Figure 2.
Silicone TMJ-Relax-Pads.

Table 1.
Basal characteristics of the experimental group (EX-RP) and control group (EX). MW: mean value; SD: standard deviation.
Table 1.
Basal characteristics of the experimental group (EX-RP) and control group (EX). MW: mean value; SD: standard deviation.
| Variable | EX-RP (n=26) MW ± SD |
EX (n=26) MW ± SD |
p |
|---|---|---|---|
| Female/male/diverse [n] | 20/6/0 | 19/7/0 | .749 |
| Age [years] | 48.5 ± 9.3 | 47.3 ± 9.3 | .922 |
| Height [cm] | 169 ± 9 | 171 ± 7 | .306 |
| Body mass [kg] | 70.5 ± 11.9 | 71.0 ± 13.2 | .553 |
| Craniomandibular dysfunction (CMD) [n] | 16 | 15 | .777 |
| Pain medication [n]a | 4 | 3 | .692 |
| Osteoporosis medication [n] | 19 | 17 | .653 |
| Physical training [min/week] | 45.5 ± 38.5 | 56.5 ± 50.0 | .271 |
| Physical activity [Index] | 4.2 ± 1.2 | 4.1 ± 1.2 | .783 |
| Prevalence of CMD | 16/10 | 15/11 | .783 |
Table 3.
Basal values and changes in secondary study endpoints with statistical parameters: TMJ relax pads (EX-RP) versus control group (EX). MV: mean values; SD: standard deviation; 95% CI: 95%: Confidence interval; * via ANCOVA adjusted for basal differences between the groups.
Table 3.
Basal values and changes in secondary study endpoints with statistical parameters: TMJ relax pads (EX-RP) versus control group (EX). MV: mean values; SD: standard deviation; 95% CI: 95%: Confidence interval; * via ANCOVA adjusted for basal differences between the groups.
| EX-RP (n=26) MV± SD |
EX (n=26) MV± SD |
Difference MV (95% CI) |
p-value | |
|---|---|---|---|---|
| Neck Disability Index (NDI) [%] | ||||
| Basal | 36.7± 6.7 | 37.8± 8.5 | ------------- | .611 |
| Change | -6.6± 8.0 | -8.2± 8.8 | 1.44 (-2.9 to 5.8)* | .514* |
| Lateral flexion cervical spine [°] | ||||
| Basal | 34.9± 7.2 | 37.8± 8.3 | ------------- | .188 |
| Change | 5.9± 6.6 | 4.6± 7.0 | 0.38 (-3.1 to 3.9)* | .825* |
| Flexion cervical spine [°] | ||||
| Basal | 50.5± 13.6 | 49.5± 11.1 | ------------- | .773 |
| Change | 6.6± 9.8 | 5.4± 10.2 | 1.35 (-4.1 to 6.9)* | .581* |
| Extension cervical spine [°] | ||||
| Basal | 75.7± 14.9 | 74.9± 17.2 | ------------- | .871 |
| Change | 7.4± 10.9 | 2.2± 11.4 | 5.48 (0.2 to 10.8)* | .044* |
| Mean rotation cervical spine [°] | ||||
| Basal | 71.1± 10.6 | 73.4± 12.2 | ------------- | .468 |
| Change | 6.3± 8.1 | 3.9± 8.5 | 1.69 (-2.4 to 5.8)* | .405* |
| Average torso rotation [°] | ||||
| Basal | 50.1± 9.2 | 51.8± 11.3 | ------------- | .534 |
| Change | 5.9± 10.9 | 13.1± 10.1 | 6.62 (1.1 to 12.1)* | .019* |
| Elevation shoulder [°] | ||||
| Basal | 165.5± 15.6 | 160.2± 13.7 | ------------- | .192 |
| Change | 10.6± 10.5 | 12.1± 11.2 | 1.09 (-4.0 to 6.1)* | .667* |
| Kyphosis angle [°] | ||||
| Basal | 42.2± 8.2 | 41.3± 8.8 | ------------- | .710 |
| Change | -3.6± 6.9 | -2.5± 7.2 | 0.85 (-4.4 to 2.7)* | .634* |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



