
Submitted:
16 January 2026
Posted:
19 January 2026
You are already at the latest version
Abstract
Polysubstance use, particularly the combination of opioids with stimulants such as cocaine and methamphetamine, is increasingly prevalent and contributes to severe morbidity and mortality. It results in complex clinical consequences, with an expanded spectrum of complications and reduced efficacy of standard emergency interventions. Co-occurring psychiatric disorders and under-recognized systemic injuries beyond primary target organs further complicate patient assessment and management.
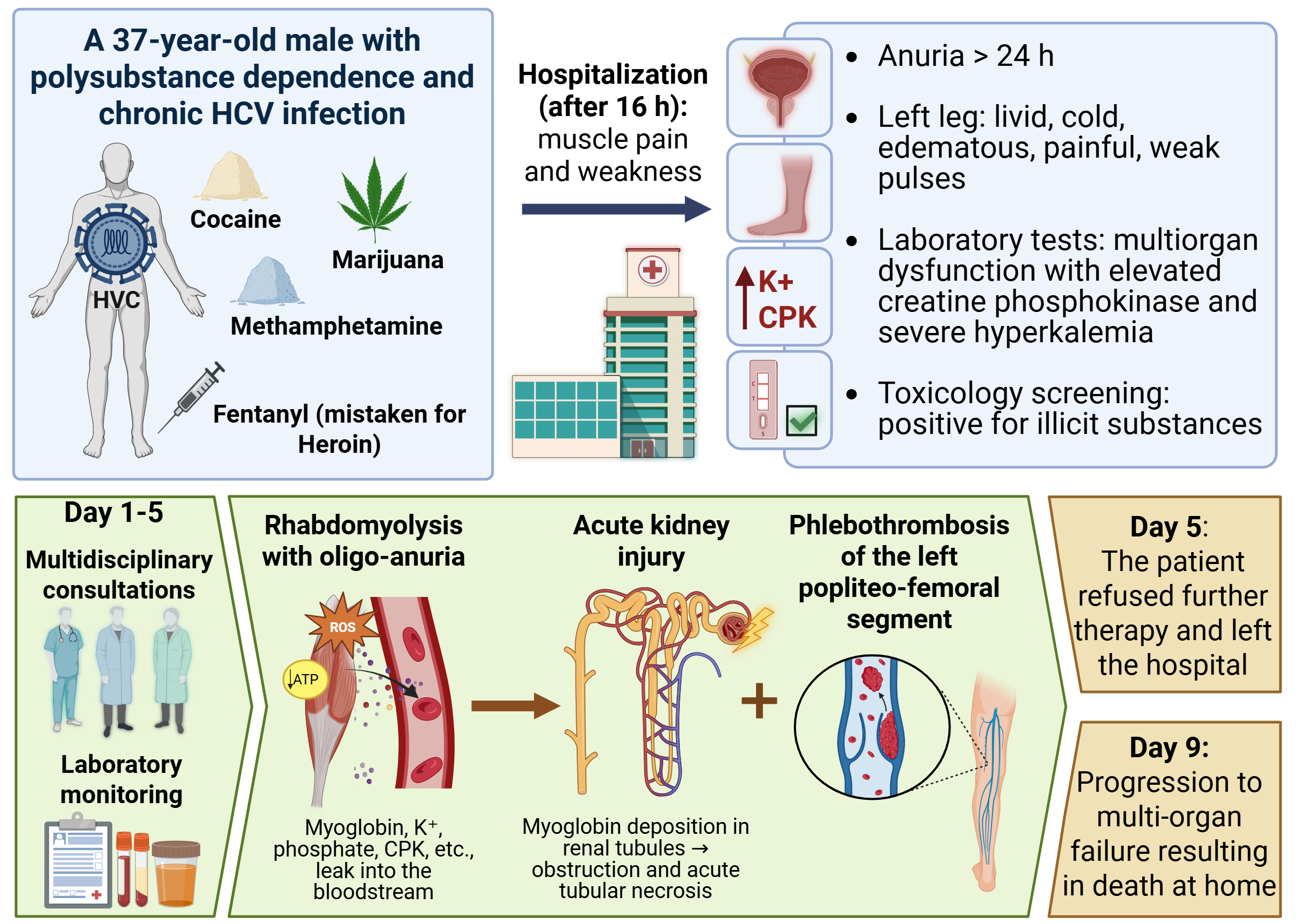
We report a clinical case of a 37-year-old male with chronic Hepatitis C Virus in-fection and documented polysubstance abuse, including fentanyl, cocaine, metham-phetamine, and cannabis, resulting in fatal complications. The patient developed mas-sive rhabdomyolysis, acute kidney injury with anuria, generalized edema, and left-sided deep vein thrombosis. The clinical course demonstrated rapid progression of multisystem dysfunction, severe electrolyte disturbances, and high-risk metabolic de-rangements. Management included intensive intravenous hydration, diuretic therapy, urinary alkalinization, electrolyte correction, anticoagulation, hemodialysis, and com-prehensive supportive care.
This case illustrates the complex pathophysiology of polysubstance toxicity, in which additive and potentially synergistic interactions exacerbate organ damage. Acute rhabdomyolysis emerged as a central mechanism, driven by both sympathomi-metic-induced hypermetabolism and opioid-related immobilization, ultimately precip-itating fatal renal and systemic complications. Despite intensive medical interventions, including hemodialysis, and active family support, the patient’s refusal to continue treatment proved a critical determinant of the fatal outcome. The case underscores the urgent need for effective strategies to manage patients with substance use disorders in acutely life-threatening conditions. It raises the importance of early psychiatric in-volvement, assessment of decision-making capacity, and, where legally justified, tem-porary measures to prevent self-harm resulting from treatment refusal.
Keywords:
polysubstance abuse
; fentanyl
; cocaine
; methamphetamine
; cannabis
; rhabdomyolysis
; acute kidney injury
; thrombosis
; hemodialysis
; clinical toxicology
1. Introduction
“Everywhere, everything, everyone” — with this deliberately polysemous message, the European Drug Report 2024 encapsulates the escalating scale of illicit drug misuse and the constrained effectiveness of institutional control mechanisms in curbing their ever-expanding availability [1]. According to data from the World Health Organization, approximately 275 million people worldwide have used psychoactive substances, with a projected increase of around 11%. In 2019, an estimated 583,000 deaths were directly or indirectly attributable to drug use. Notably, the COVID-19 pandemic further compromised the accessibility and functioning of addiction treatment services, underscoring the critical need for resilient and adaptive healthcare systems, capable of maintaining continuity of care even under conditions of global health crises [2]. According to the 2025 report of the European Union Drugs Agency (EUDA), the number of drug-related deaths shows a slight increase in several Member States of the European Union. Preliminary estimates indicate nearly 7,500 cases, while acknowledging that these figures are substantially underestimated due to incomplete registration practices and limited availability of toxicological data [3]. Concurrently, the United Nations Office on Drugs and Crime offers a sobering reminder that the morbidity and mortality associated with substance abuse are not attributable solely to acute overdose, but rather arise from a complex interplay of acute and chronic toxic effects, compounded by adverse behavioral determinants (Table 1) [4].
Against this backdrop, the available data delineate a concerning emerging trend — the progressive normalization of polysubstance use. According to the EUDA, opioids are implicated in approximately 70% of overdose-related fatalities, most often in combination with other psychoactive substances. Cocaine is detected in roughly 26% of cases, with its use increasing even in regions where it has traditionally been limited, and increasingly in conjunction with opioids. Other stimulants, including amphetamines and methamphetamines, also contribute to a substantial number of fatal outcomes, again predominantly in the context of combined use with opioids [3]. The presented epidemiological data align with what the National Institutes of Health have termed the “fourth wave of the opioid crisis”, first identified in the United States. Unlike the preceding three phases, which were respectively associated with prescription opioids, heroin, and synthetic opioids such as fentanyl, the current wave is characterized by widespread polysubstance use, wherein opioids are frequently combined with stimulants such as methamphetamine and cocaine. The clinical consequences are multifaceted and highly complex: there is a marked increase in mortality, an expansion of the spectrum of complications, and a diminished effectiveness of standard interventions in emergency toxicology. Concurrently, there is a rising co-morbidity with psychiatric disorders, rendering the fourth wave a challenge not only from a pharmacological standpoint but also from a behavioral perspective [5,6].
Our clinical observations over recent years corroborate the rising trend of polysubstance use. Within the context of emergency toxicology, where life-saving interventions are traditionally focused on critical organs and systems such as the central nervous system, cardiovascular system, and lungs, systemic injuries beyond these primary targets are frequently underestimated, despite their potentially fatal nature [7,8]. To illustrate this issue, we present a clinical case with a fatal outcome, resulting from a complex of complications, including rhabdomyolysis, acute renal failure, and deep vein thrombosis (DVT), in a patient with concurrent use of fentanyl, cocaine, methamphetamine, and cannabis.
2. Case Presentation
2.1. Medical History
A 37-year-old male with a documented history of polysubstance use disorder and chronic Hepatitis C Virus (HCV) infection was admitted to the Emergency Consultative Unit of the Military Medical Academy–Varna. The reason for admission was self-injection of “ten heroin units” (later identified as illicit fentanyl) into the vein of the left foot approximately 16 hours prior to hospitalization. The patient also reported concurrent use of methamphetamine and cocaine via inhalation, as well as cannabis via smoking. Following a period of sleep, he experienced pronounced generalized weakness, which was followed by a fall when attempting to rise from bed, accompanied by pain and a sense of stiffness in the left lower leg.
2.2. Physical Examination and Clinical Course
The patient was admitted to the Clinical Toxicology Department, Naval Hospital—Varna, Bulgaria Medical Academy, in an acute condition, with inaccessible peripheral venous access; a central venous catheter was therefore established. Upon admission, he was awake and oriented, exhibiting a dysphoric mood and mildly clouded consciousness, with limited insight into his substance use disorder. He reported anuria for more than 24 hours. Vital signs were stable, and the patient was able to maintain an active position in bed.
Examination of the skin revealed multiple puncture marks on the left foot, lower legs, and forearms. Bilateral swelling of the hands and fingers was noted. The left lower limb demonstrated pronounced tense edema, with a 3 cm increase in circumference compared to the contralateral limb, accompanied by mild cyanosis and signs of venous congestion. Peripheral pulses were preserved.
An extended panel of laboratory tests was ordered, including muscle and cardiac enzymes, coagulation parameters, arterial blood gas analysis, and electrolyte profiling. The patient’s daily clinical course is summarized in Table 2.
2.3. Toxicological Screening and Laboratory Results
Blood and urine samples from the patient were analyzed at the Laboratory of Analytical Toxicology using rapid immunoassay tests (ALL TEST™, MedNet GmbH, Germany). Negative results in the routine opiate screening prompted additional testing for fentanyl using dedicated mononarcotic immunoassays from the same manufacturer, which yielded a positive result in the urine sample. This finding is fully consistent with the known pharmacokinetic profile of fentanyl: the compound exhibits a short plasma half-life (≈3–8 hours), leading to rapid decline of blood concentrations below the detection threshold of routine assays. In contrast, fentanyl and its metabolites are primarily excreted via the kidneys, permitting prolonged detectability in urine, typically up to 24–48 hours post-administration [9,10,11]. Furthermore, this case highlights a broader concern: opioid users are sometimes unaware that they are consuming fentanyl, a far more potent opioid, which substantially increases the risk of overdose [12]. Analytical results, together with the corresponding cut-off values for urine and plasma, are summarized in Table 3.
The patient’s laboratory parameters reflect both the severity and dynamic progression of the clinical course and are pathophysiologically consistent with the described case evolution (Table 4). A massive rhabdomyolysis was observed, evidenced by marked elevations in muscle enzymes and related proteins, with progressive increases in biochemical markers of muscle injury. Concurrently, acute kidney injury (AKI) progressed, reflected by rising indicators of renal function corresponding to impaired excretory capacity. Severe hyperkalemia and metabolic acidosis were also documented, indicative of electrolyte imbalance and systemic disruption of acid–base homeostasis, both characteristic of this condition.
Systemic inflammatory markers demonstrated an active inflammatory response, correlating with the clinical presentation of systemic inflammatory syndrome. Coagulation and vascular assessments identified a DVT, likely precipitated by the combination of inflammation, stasis, and coagulopathy. Due to the absence of arterial access, blood gas analysis was performed on capillary blood obtained from the fingertip. This approach allowed rapid evaluation of acid–base status and metabolic parameters. Capillary pH, pCO₂, and HCO₃⁻ were used for trend monitoring, whereas pO₂ and oxygen saturation cannot be considered fully arterial. Base excess and lactate provided approximate information regarding metabolic acidosis. Despite these limitations, the analysis clearly demonstrated developing metabolic acidosis associated with AKI and massive rhabdomyolysis.
2.4. Diagnosis
The patient was diagnosed with polysubstance use disorder (fentanyl, cocaine, methamphetamine, cannabis) and chronic HCV infection. Hospitalization followed intravenous exposure to illicit fentanyl, resulting in severe rhabdomyolysis, AKI with oligo-anuria, generalized edema, and left-sided DVT, complicated by multisystem dysfunction. Despite the reported fall, clinical findings and the temporal association with intoxication indicate toxin-induced rhabdomyolysis as the primary cause of muscle pain and edema. Acute arterial thrombosis or arterial dissection were excluded as causes of oligo-anuria and muscular injury; Doppler imaging confirmed venous involvement (phlebothrombosis). Sepsis or bacterial infection were also excluded (afebrile status, normal CRP, absence of fever), with antibiotic therapy administered empirically for prophylactic purposes. The impact of all administered medications and infusion solutions was considered minimal relative to the effect of the drug intoxication. Observed hyperkalemia, oligo-anuria, and generalized edema were deemed secondary to rhabdomyolysis and renal dysfunction.
Muscle biopsy was considered as a potentially informative diagnostic tool in rhabdomyolysis, particularly in cases of unclear etiology or suspected primary myopathies. In the present case of toxin-induced rhabdomyolysis, muscle biopsy was deemed unnecessary. Given the patient’s critical condition, the invasive procedure would have posed an unjustified risk without providing significant diagnostic or prognostic benefit [13,14,15].
2.5. Therapeutic Course
The therapeutic course during the patient’s clinical hospitalization is summarized in Table 5 by day. It reflects a multifaceted, multidisciplinary approach, specifically tailored to address the established complex pathophysiology.
3. Discussion
The present clinical case illustrates an exceptionally severe polysubstance intoxication involving fentanyl, methamphetamine, cocaine, and cannabis, resulting in a rare and high-risk toxicological profile. It raises a pivotal question as to whether the combined effects of these substances are merely additive or represent true toxicological synergy with accelerated progression of organ injury. Intranasally administered methamphetamine and cocaine are potent sympathomimetic agents, inducing massive catecholamine release, pronounced peripheral vasoconstriction, and a marked increase in skeletal muscle metabolic demand. Consequently, a critical imbalance develops between oxygen delivery and metabolic requirements within skeletal muscle tissue, leading to localized ischemia, mitochondrial dysfunction, and sarcolemmal instability. The clinical manifestation of this cascading pathophysiological process is fulminant rhabdomyolysis [16,17,18,19,20]. In this context, sympathomimetic agents may induce rhabdomyolysis both directly through toxic effects on myocytes and indirectly via immobilization, mechanical compression, and excessive muscular activity [21]. The involvement of opioids, including fentanyl, in the pathogenesis of rhabdomyolysis has also been described and is typically multifactorial, encompassing prolonged immobilization, muscle compression, localized ischemia, and metabolic disturbances [17,22,23,24,25,26,27,28,29,30]. In the present case, injection of fentanyl into the left foot further complicated the clinical course through the development of a locally induced compartment syndrome. The central depressant effects of fentanyl resulted in reduced motor activity and prolonged compression ischemia, in conjunction with vascular and soft tissue injury at the site of administration. This was clinically corroborated by the development of subfascial edema, neurological deficits, and venous thrombosis, all of which further potentiated the rhabdomyolytic process. Although cannabis is the most commonly used illicit substance worldwide, it has not been convincingly associated with rhabdomyolysis when used in its herbal forms. Available literature suggests that such an association is more characteristic of synthetic cannabinoids, for which cases of rhabdomyolysis and AKI have been reported, albeit rarely as isolated primary etiological factors [31,32,33]. Therefore, in the present case, the role of cannabis is considered likely secondary and modulatory rather than causative or primary.
The toxicologically induced rhabdomyolysis observed in this patient follows a unified pathophysiological model based on sarcolemmal injury and progressive depletion of adenosine triphosphate (ATP) [14,34,35,36,37]. Although ATP depletion is not invariably the initiating event, it almost universally represents the final common pathogenic pathway, culminating in intracellular calcium overload, activation of calcium-dependent proteases, and myocyte necrosis (Figure 1) [15,16,37,38]. Destruction of muscle cells results in massive release of potassium, myoglobin, creatine phosphokinase, and other intracellular constituents into the systemic circulation [34,38,39,40,41,42]. Given that skeletal muscle accounts for approximately 40% of total body mass, the destruction of as little as 100 g of muscle tissue is sufficient to produce the clinical manifestation of rhabdomyolysis. Circulating myoglobin rapidly exceeds plasma binding capacity and, under acidic pH conditions, may precipitate within the glomerular filtrate, leading to tubular obstruction and necrosis, accompanied by pronounced renal vasoconstriction [37,43]. Moreover, it induces the release of free iron via heme and catalyzes the generation of reactive oxygen species, further exacerbating ischemic tubular injury [15,34,36,40,44]. A frequent complication of rhabdomyolysis is the development of compartment syndrome, characterized by the accumulation of substantial fluid volumes (up to 10–12 L) within muscle compartments, resulting in increased tissue pressure and compromised local perfusion. In more severe cases, hepatic injury and disseminated intravascular coagulation may also occur [15,36,39].
The classic triad of rhabdomyolysis—muscle pain, muscle weakness, and dark-colored urine—was observed in the presented patient. However, it is well established that this combination occurs in only approximately 10% of cases, which, together with etiological heterogeneity, concomitant comorbidities, and behavioral factors, necessitated the application of a more comprehensive diagnostic approach [15]. Serum creatine phosphokinase (CK), established as the most sensitive biochemical marker for skeletal muscle injury, was measured in the patient [14,15,33,41]. Rhabdomyolysis is typically defined by CK levels exceeding 1000 U/L or ≥5 times the upper limit of normal, with concentrations ≥5000 U/L being associated with an increased risk of AKI [14,15,35,39,40,45,46]. In this context, the extreme elevation of CK in our patient (up to 161,050 U/L) reflected massive skeletal muscle injury. Concurrently, the elevated CK-MB values in this setting are considered analytically unreliable for diagnosing acute myocardial infarction in the presence of severe rhabdomyolysis. Myocardial involvement was primarily assessed via troponin, which was markedly elevated and most likely indicative of type 2 myocardial injury—uremic and/or toxin-induced cardiomyocyte necrosis. Simultaneously, rapidly progressive AKI developed, evidenced by rising serum creatinine and urea levels, decreased eGFR, and transition from oliguria to anuria. Urinalysis revealed proteinuria, hematuria, and leukocyturia, consistent with tubular injury and myoglobinuria.
The clinical manifestations of rhabdomyolysis can range from subclinical elevations of serum enzymes to severe, life-threatening complications, as observed in our patient. These complications include metabolic acidosis, marked electrolyte disturbances (hyperkalemia, hyperphosphatemia, hypocalcemia), and AKI—the most severe and prognostically significant complication of the condition. AKI develops in over 50% of affected patients and accounts for 5–15% of all cases of acute renal failure. Among these patients, the requirement for renal replacement therapy reaches 5–26%, while mortality may be as high as 80% [36,47,48,49]. According to Cabral et al. (2020), dialysis is required in approximately 85% of patients with oliguric AKI and around 30% of those with non-oliguric AKI. Although randomized controlled trials are lacking, available clinical evidence indicates that early and aggressive intervention is associated with a more favorable outcome [14]. In this context, the McMahon score represents a clinically validated tool for the early assessment of the risk of AKI, the need for renal replacement therapy, and mortality upon admission. Despite the absence of serum phosphate data, the McMahon score in our patient remained critically high (≥11 points), reflecting the severity of muscle injury and the elevated risk of dialysis-requiring AKI [14,33,50]. The primary determinants of the high score were extreme elevation of creatine phosphokinase (>160,000 U/L), hyperkalemia, hypocalcemia, and marked increase in serum creatinine. This underscores that even in the context of incomplete data, the patient’s elevated McMahon score correlated with persistent oligo-anuria, severe hyperkalemia, and multi-organ dysfunction, confirming its reliability as a prognostic tool and highlighting the necessity for early, aggressive interventions. Unfortunately, the patient’s categorical refusal of dialysis in the setting of progressive AKI proved life-threatening and ultimately fatal.
Although xenobiotic agents—most commonly opioids, alcohol, and stimulants—represent a leading cause of rhabdomyolysis, according to our data, clinical studies attempting to elucidate the correlation between rhabdomyolysis manifestation and illicit drug use remain limited (Table 6) [37,41,47,51,52,53,54,55].
Clearly, several studies lack stratification by specific psychoactive substances. More importantly, a general limitation across all these investigations is the absence of statistical data on the risk of rhabdomyolysis associated with concurrent use of multiple xenobiotics—a scenario directly relevant to the clinical problem we encountered. In clinical practice, additional factors, such as viral infections—as present in our patient—may further modulate organ vulnerability, complicating the isolation of the individual substance effect on renal function [21,34,56]. In this context, it is important to note that chronic HCV infection is associated with extrahepatic manifestations, including myalgia and inflammatory myopathies, which may predispose patients to muscle injury and, rarely, to rhabdomyolysis in the presence of additional risk factors such as substance abuse or drug interactions [57]. Cases of acute rhabdomyolysis have been reported in patients with chronic HCV infection, either following the initiation of antiviral therapy (e.g., direct-acting antivirals) or in combination with concomitant medications such as statins, where pharmacokinetic interactions can precipitate severe muscle toxicity [58,59]. Moreover, some reported cases among intravenous drug users with HCV indicate that the viral infection may lower the threshold for muscle lysis, thereby facilitating the development of rhabdomyolysis in the context of substance abuse [60]. However, the available evidence is limited and predominantly derived from case reports and observational studies, necessitating cautious interpretation and further investigation.
The massive rhabdomyolysis observed in the patient reflected severe skeletal muscle injury and created conditions conducive to venous thrombosis. The release of myoglobin and muscle proteins increases blood viscosity and activates the coagulation cascade, while local edema and immobility contribute to venous stasis. The combination of systemic and local factors underscores the link between muscle necrosis and vascular complications. Intravenous self-injection into distal veins of the lower limb is a well-known high-risk practice among individuals who use drugs. Superficial veins are initially accessed; when these become thrombosed, patients resort to deeper veins (inguinal, axillary, subclavian, jugular, or even dorsal penile veins), with the femoral vein often preferred due to accessibility and discretion. Peripheral veins, particularly in the foot and ankle region, are highly susceptible to endothelial injury, local thrombophlebitis, and proximal thrombus propagation [61,62,63]. The presence of thrombosis involving the popliteal–femoral venous segment was confirmed, supporting the hypothesis of ascending progression of the thrombotic process. Clinically, subfascial edema, limb tension, and cyanotic discoloration were observed, which are typical signs of acute venous obstruction [64]. Although arterial compromise was initially suspected, Doppler imaging revealed no evidence of arterial occlusion, allowing acute arterial thrombosis or embolism to be excluded. The transient attenuation of peripheral pulses was most likely due to extravascular compression from massive edema. The pathogenesis of the thrombosis can be explained via Virchow’s triad: endothelial injury resulted from chemical and mechanical irritation during injection; venous stasis arose from edema and immobilization; and hypercoagulability was driven by systemic inflammation, dehydration, acute renal dysfunction, and a potential hereditary thrombophilia suggested by a family history of DVT [65,66,67]. A diagnostic challenge in this population is the frequent coexistence of chronic venous damage with acute thrombotic episodes, which renders clinical assessment unreliable. In this context, duplex ultrasonography remains the method of choice for differentiating acute DVT from chronic post-thrombotic changes and for excluding arterial pathology [68,69].
Due to the patient’s critical condition, intensive intravenous hydration with isotonic and balanced solutions (0.9% NaCl, Ringer’s lactate, 5% Glucose) was initiated on the first day to stabilize hemodynamics and correct electrolyte imbalances. The therapeutic approach was guided by the current lack of high-quality randomized controlled trials defining clear early management algorithms for rhabdomyolysis, as existing recommendations are primarily based on retrospective analyses, clinical case series, and experimental models. At present, early intravenous hydration remains the cornerstone of therapy, although the optimal type, volume, and infusion rate are still subjects of debate [15,35,40]. Additionally, comprehensive supportive therapy was implemented, including parenteral nutrition with a lipid emulsion, neurometabolic and vitamin supplementation (Piracetam, Thiamine, Pyridoxine, Cyanocobalamin), and targeted electrolyte correction. Psychomotor agitation and psychotropic symptoms were managed with Diazepam and Haloperidol. Due to severe hyperkalemia and progressive oligo-anuria, diuretic and renal support with Furosemide was initiated under strict laboratory and hemodynamic monitoring. Another potential diuretic option in rhabdomyolysis management is Mannitol, an osmotic diuretic with theoretical advantages such as increased urinary flow, improved renal perfusion, and reduction of tubular obstruction. However, clinical data have not convincingly demonstrated improvements in renal outcomes or overall survival. Moreover, its use carries significant risks in oligo-anuric patients, including volume overload, osmotic nephropathy, and electrolyte disturbances [34,35,70,71]. Therefore, based on this rationale and our own clinical experience, Furosemide was selected. As a potent loop diuretic, it allows more precise control of volume status and may aid in correcting hyperkalemia and reducing the risk of tubular obstruction by myoglobin casts. In the presented case, the choice of Furosemide over Mannitol was dictated by the presence of progressive oligo-anuria, severe hyperkalemia, generalized edema, and a high risk of hypervolemia, conditions under which the osmotic effect of Mannitol could have further compromised hemodynamic stability and renal function [33,36]. It is important to emphasize that neither Furosemide nor Mannitol has been proven to prevent rhabdomyolysis-induced AKI when used in isolation. The role of both diuretics remains a topic of active debate, with the primary therapeutic principle continuing to be early and adequate intravenous hydration, aimed at maintaining renal perfusion and reducing tubular myoglobin concentration [21,34,39,72].
Given the high thrombotic risk, standard protocols dictated the initiation of prophylactic anticoagulation with low-molecular-weight heparin (Enoxaparin), followed by continued anticoagulant therapy. The left lower limb was maintained in an elevated position to reduce venous stasis and improve tissue perfusion. Since edema control is critical, compression stockings with a pressure of 30–40 mmHg were also applied. Although recent randomized studies have not demonstrated a reduction in post-thrombotic syndrome incidence, there is consensus that such measures can alleviate patient symptoms [73,74,75,76]. Thrombolytic therapy is generally not recommended in this patient population. These patients often provide unreliable histories, and acute DVT frequently occurs as a new episode superimposed on chronic DVT, rendering thrombolysis largely ineffective. Moreover, thrombolytic treatment carries a significant risk of bleeding from arteries or veins that may have been compromised by prior intravenous drug use. Similarly, thrombectomy is not advised due to the high procedural risk and limited expected benefit [75,76,77,78,79].
In the subsequent days, supportive therapy for renal function and correction of metabolic disturbances was continued through the administration of insulin–glucose solutions, sodium bicarbonate, and calcium preparations as clinically indicated. It should be noted that the use of sodium bicarbonate for the prevention of AKI remains a controversial issue, with limited and inconsistent evidence regarding its efficacy [37,72]. This approach is based on the concept that an acidic environment potentiates myoglobin toxicity; consequently, alkalinization of the urine may reduce redox cycling, lipid peroxidation, and the formation of myoglobin casts. It is therefore reasonable to assume that increasing urine pH above 6.5 through intravenous administration of sodium bicarbonate could help prevent the development of AKI [36]. Furthermore, some authors recommend the use of sodium bicarbonate for the correction of metabolic acidosis. On the other hand, its administration may result in paradoxical intracellular acidosis and volume overload, particularly in patients with respiratory or circulatory insufficiency, as the bicarbonate buffering system leads to increased carbon dioxide production [40,49].
Despite intensive therapy, persistent oligo-anuria and generalized edema were observed, with no significant improvement in renal function. Therefore, on the fifth day of hospitalization, urgent intermittent hemodialysis was initiated due to overtly progressive AKI. This modality was chosen as it balances rapid correction of metabolic disturbances with the patient’s clinical tolerance [80,81,82]. Despite timely and aggressive therapeutic interventions, including an individualized multidisciplinary approach, the clinical course was further complicated by the patient’s categorical refusal to continue treatment immediately thereafter. This refusal should be considered not only an ethical and legal issue but also a critical clinical factor that contributed to the fatal outcome. In patients with substance use disorders, impaired illness insight, limited recognition of disease severity, and impulsive behavior are common and can substantially compromise adherence to life-saving therapeutic regimens [83]. In this particular case, despite the patient maintaining formal contact and orientation, the likely influence of ongoing intoxication, uremic encephalopathy, and the psychiatric sequelae of chronic polysubstance use called into question the patient’s actual capacity to adequately assess risk and make an informed decision. Consequently, the patient left the medical facility with persistent anuria and metabolic derangements, despite clear indications for continued renal replacement therapy. This led to progression of multiorgan dysfunction and a fatal outcome on the ninth day after hospitalization at home. Despite extraordinary efforts by the patient’s family to provide support and care, this case clearly illustrates that urgent and professional medical intervention remains indispensable and potentially life-saving in such scenarios. In this context, various sources emphasize that the so-called “family burden” can result in emotional stress and physical exhaustion not only for the individual with substance use disorder but also for family members, highlighting the limited capacity for care among non-medical persons involved in the treatment process of patients with addiction [84,85,86,87]. Thus, the present case underscores the critical need to develop more effective management strategies for patients with substance use disorders in acutely life-threatening conditions. These strategies should include early involvement of a psychiatrist, formal assessment of decision-making capacity, and, where legally justified, temporary protective measures to prevent self-harm through refusal of treatment. More broadly, the case highlights the complex interplay between toxicology, nephrology, and medical ethics, which can prove decisive for patient outcomes even under optimal medical management [4].
4. Conslusion
The present clinical case demonstrates that the synergistic toxic effects of polysubstance abuse can lead to unpredictable and fatal outcomes, including rhabdomyolysis, AKI, and DVT. Although these complications are less common than central nervous system, cardiac, or pulmonary damage, they are life-threatening and require early recognition and timely therapeutic intervention.
Publishing detailed clinical cases is of critical importance for medical practice and public health, as it provides in-depth toxicological data, an assessment of polysubstance use, and specific mechanisms of toxicity often absent from national registries and official statistics. Such information facilitates the early identification of novel substances, emerging patterns of use, and risk factors, while also enhancing patient prevention and management strategies.
The case further highlights that patient behavior can compromise medical efforts; refusal of therapy led to a fatal outcome despite optimal medical management. This underscores the complex interplay between medical, social, psychological, and legal factors, necessitating an integrated, multidisciplinary approach and specialized care strategies.
In conclusion, this case not only supplements statistical data but also provides critical insight into the risks and dynamics of polysubstance abuse, with direct implications for clinical management, public health, future research, and the development of effective preventive policies.
Author Contributions
Conceptualization, S.S.-G., I.Y., G.B, S.Z., and P.M.; methodology, S.S.-G., I.Y., I.P., M.R.-I., G.B., M.T., D.I., S.M., P.M, and S.Z.; software, S.S.-G. and I.Y.; validation, S.S.-G. and I.Y.; formal analysis, S.S.-G., I.Y., I.P., G.B., M.T., and S.M.; investigation, S.S.-G., I.Y., I.P., G.B., M.T., D.I., and S.M.; resources, D.I., M.M., P.M, and S.Z.; data curation, S.S.-G. and I.Y; writing—original draft preparation, S.S.-G.; writing—review and editing, S.S.-G. and S.Z.; visualization, S.S.-G. and I.Y; supervision, G.B., M.T., D.I., P.M, and S.Z.; project administration, S.S.-G., D.I., M.M., and P.M.; funding acquisition, D.I., M.M., P.M, and S.Z. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the European Union–NextGenerationEU through the National Recovery and Resilience Plan of the Republic of Bulgaria [project No. BG-RRP-2.004-0009-C02/2023], which is part of the MUVE-TEAM.
Institutional Review Board Statement
This study is retrospective and relies solely on medical data that had already been collected for other clinical purposes. Therefore, no approval was required from an ethics committee or an institutional review board, as no new interventions were performed on patients and all data were obtained from existing medical records.
Informed Consent Statement
Informed consent was obtained from the patients for their clinical history.
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AKI | Acute kidney injury |
| ATP | Adenosine triphosphate |
| CK | Creatine phosphokinase |
| DVT | Deep vein thrombosis |
| EUDA | European Union Drugs Agency |
| HCV | Hepatitis C Virus |
References
- European Monitoring Centre for Drugs and Drug Addiction. European Drug Report 2024: Trends and Developments – The Drug Situation in Europe up to 2024; European Monitoring Centre for Drugs and Drug Addiction: Lisbon, Portugal, 2024; ISBN 978-92-9497-975-9. https://www.emcdda.europa.eu/publications/european-drug-report/2024/drug-situation-in-europe-up-to-2024_en.
- World Health Organization. Strengthening Clinical Trials to Provide High-Quality Evidence on Health Interventions and to Improve Research Quality and Coordination: Report by the Director-General; World Health Organization: Geneva, Switzerland, 2022; Document No. A75/43. https://apps.who.int/gb/ebwha/pdf_files/WHA75/A75_43-en.pdf (accessed on 13 November 2025).
- European Union Drugs Agency (EUDA). Drug Induced Deaths – The Current Situation in Europe (European Drug Report 2025); EUDA: Lisbon, Portugal, 2025. https://www.euda.europa.eu/publications/european-drug-report/2025/drug%20induced%20deaths_en (accessed on 13 November 2025).
- United Nations Office on Drugs and Crime. Contemporary Issues on Drugs. Booklet 2, World Drug Report 2025; United Nations Office on Drugs and Crime: Vienna, Austria, 2025. https://www.unodc.org/documents/data-and-analysis/WDR_2025/WDR25_B2_Contemporary_drug_issues.pdf (accessed on 13 November 2025).
- National Institutes of Health, HEAL Initiative. Opioid Crisis. National Institutes of Health, 2024. Available online: https://heal.nih.gov/about/opioid-crisis (accessed on 22 December 2025).
- Rawy, M.; Abdalla, G.; Look, K. Polysubstance mortality trends in White and Black Americans during the opioid epidemic, 1999–2018. BMC Public Health 2024, 24, 112. [CrossRef]
- Shannon, M.W.; Borron, S.W.; Burns, M.J. Emergency management of poisoning. In Haddad and Winchester’s Clinical Management of Poisoning and Drug Overdose, 4th ed.; Shannon, M.W., Borron, S.W., Burns, M.J., Eds.; W.B. Saunders: Philadelphia, PA, USA, 2007; pp. 13–61. [CrossRef]
- Manjón-Prado, H.; Serrano Santos, E.; Osuna, E. Patterns of polydrug use in patients presenting at the emergency department with acute intoxication. Toxics 2025, 13, 380. [CrossRef]
- Uljon, S. Advances in fentanyl testing. Adv. Clin. Chem. 2023, 116, 1–30. [CrossRef]
- Stoeva-Grigorova, S.; Radeva-Ilieva, M.; Karkkeselyan, N.; Dragomanova, S.; Kehayova, G.; Dimitrova, S.; Petrova, M.; Zlateva, S.; Marinov, P. Historical perspectives and emerging trends in fentanyl use: Part 1—Pharmacological profile. Pharmacia 2025, 72, 1–9. [CrossRef]
- Stoeva-Grigorova, S.; Hvarchanova, N.; Gancheva, S.; Eftimov, M.; Georgiev, K.D.; Radeva-Ilieva, M. Differentiation of therapeutic and illicit drug use via metabolite profiling. Metabolites 2025, 15, 745. [CrossRef]
- Griswold, M.K.; Chai, P.R.; Krotulski, A.J.; Friscia, M.; Chapman, B.; Boyer, E.W.; Logan, B.K.; Babu, K.M. Self-identification of nonpharmaceutical fentanyl exposure following heroin overdose. Clin. Toxicol. 2018, 56, 37–42. [CrossRef]
- Vanholder, R.; Sever, M.S.; Erek, E.; Lameire, N. Rhabdomyolysis. J. Am. Soc. Nephrol. 2000, 11, 1553–1561. [CrossRef]
- Cabral, B.M.I.; Edding, S.N.; Portocarrero, J.P.; Lerma, E.V. Rhabdomyolysis. Dis. Mon. 2020, 66, 101015. [CrossRef]
- Yang, B.-F.; Li, D.; Liu, C.-L.; Luo, Y.; Shi, J.; Guo, X.-Q.; Fan, H.-J.; Lv, Q. Advances in rhabdomyolysis: A review of pathogenesis, diagnosis, and treatment. Chin. J. Traumatol. 2025, S1008-1275(25)00010-0. [CrossRef]
- Richards, J.R. Rhabdomyolysis and drugs of abuse. J. Emerg. Med. 2000, 19, 51–56. [CrossRef]
- Wurcel, A.G.; Merchant, E.A.; Clark, R.P.; Stone, D.R. Emerging and underrecognized complications of illicit drug use. Clin. Infect. Dis. 2015, 61, 1840–1849. [CrossRef]
- Alessi, M.R.; Ribas, T.M.; Campelo, V.S.; Mauer, S. Acute cocaine intoxication leading to multisystem dysfunction: A case report. Cureus 2024, 16, e72128. [CrossRef]
- Hong, Z.M.; Kromm, J.A. Neurological and systemic effects of cocaine toxicity: A case report and review of the literature. Med. Int. (Lond.) 2024, 8, 196. [CrossRef]
- Mirza, S.A.; Mohammed, N.S.; Ali, Z.Q.; Mohamed, A.S. The effects of methamphetamine intoxication on acute kidney injury in Iraqi male addicts. Toxicol. Rep. 2025, 102065. [CrossRef]
- Mitaritonno, M.; Lupo, M.; Greco, I.; Mazza, A.; Cervellin, G. Severe rhabdomyolysis induced by co-administration of cocaine and heroin in a 45 years old man treated with rosuvastatin: A case report. Acta Biomed. 2021, 92(S1), e2021089. [CrossRef]
- Sahni, V.; Garg, D.; Garg, S.; Agarwal, S.K.; Singh, N.P. Unusual complications of heroin abuse: Transverse myelitis, rhabdomyolysis, compartment syndrome, and ARF. Clin. Toxicol. 2008, 46, 153–155. [CrossRef]
- Kosmadakis, G.; Michail, O.; Filiopoulos, V.; Papadopoulou, P.; Michail, S. Acute kidney injury due to rhabdomyolysis in narcotic drug users. Int. J. Artif. Organs 2011, 34, 584–588. [CrossRef]
- Alinejad, S.; Ghaemi, K.; Abdollahi, M.; Mehrpour, O. Nephrotoxicity of methadone: A systematic review. SpringerPlus 2016, 5, 2087. [CrossRef]
- Babak, K.; Mohammad, A.; Mazaher, G.; Samaneh, A.; Fatemeh, T. Clinical and laboratory findings of rhabdomyolysis in opioid overdose patients in the intensive care unit of a poisoning center in 2014 in Iran. Epidemiol. Health 2017, 39, e2017050. [CrossRef]
- Dobrie, L.; Handa, T.; Sirotkin, I.; Cruz, A.; Konstas, D.; Baldinger, E. Rhabdomyolysis occurring after use of cocaine contaminated with fentanyl causing bilateral brachial plexopathy. Fed. Pract. 2022, 39, 261–265. [CrossRef]
- Pi, M.; Nie, S.; Su, L.; Li, Y.; Cao, Y.; Gao, P.; Lin, Y.; Zha, Y.; Shi, Y.; Li, H.; Zhao, J.; Kong, Y.; Li, G.; Hu, Y.; Liu, H.; Wan, Q.; Chen, C.; Liu, B.; Yang, Q.; Su, G.; Zhou, Y.; Weng, J.; Xu, G.; Xu, H.; Tang, Y.; Gong, M.; Hou, F.F.; Xu, X. Risk of Hospital-Acquired Acute Kidney Injury among Adult Opioid Analgesic Users: A Multicenter Real-World Data Analysis. Kidney Dis. 2023, 9, 517–528. [CrossRef]
- Tom, K.; Bzdusek, J. Heroin overdose complicated by compartment syndrome, rhabdomyolysis, and acute renal failure. Cureus 2024, 16, e61144. [CrossRef]
- Gokul, K.; Hoque, F. Rhabdomyolysis with severe creatine phosphokinase elevation and acute kidney injury: A case report and review of rare causes. APIK J. Intern. Med. 2025, 13, 300–302. [CrossRef]
- Keenum, O.D.; Patel, S.; Balasubramaniam, A.; Bates, W.; Smallwood, D. An unusual presentation of fentanyl-induced rhabdomyolysis. Cureus 2025, 17, e83426. [CrossRef]
- Jullian-Desayes, I.; Roselli, A.; Lamy, C.; Alberto-Gondouin, M.C.; Janvier, N.; Venturi-Maestri, G. Rhabdomyolysis with acute renal failure and deep vein thrombosis induced by antipsychotic drugs: A case report. Pharmacopsychiatry 2015, 48, 265–267. [CrossRef]
- Zhao, A.; Tan, M.; Aung, M.; Salifu, M.; Mallappallil, M. Rhabdomyolysis and acute kidney injury requiring dialysis as a result of concomitant use of atypical neuroleptics and synthetic cannabinoids. Case Rep. Nephrol. 2015, 2015, 235982. [CrossRef]
- Upadrista, P.K.; Peketi, S.H.; Sudireddy, N.; Cadet, B.; Kim, Z. Rhabdomyolysis and acute kidney injury: Exploring the potential causes in a hospitalized patient. Cureus 2025, 17, e80535. [CrossRef]
- Huerta-Alardín, A.L.; Varon, J.; Marik, P.E. Bench-to-bedside review: Rhabdomyolysis—An overview for clinicians. Crit. Care 2005, 9, 158–169. [CrossRef]
- Bagley, W.H.; Yang, H.; Shah, K.H. Rhabdomyolysis. Intern. Emerg. Med. 2007, 2, 210–218. [CrossRef]
- Bosch, X.; Poch, E.; Grau, J.M. Rhabdomyolysis and acute kidney injury. N. Engl. J. Med. 2009, 361, 62–72. [CrossRef]
- Zimmerman, J.L.; Shen, M.C. Rhabdomyolysis. Chest 2013, 144, 1058–1065. [CrossRef]
- Giannoglou, G.D.; Chatzizisis, Y.S.; Misirli, G. The syndrome of rhabdomyolysis: Pathophysiology and diagnosis. Eur. J. Intern. Med. 2007, 18, 90–100. [CrossRef]
- Torres, P. A.; Helmstetter, J. A.; Kaye, A. M.; Kaye, A. D. Rhabdomyolysis: Pathogenesis, diagnosis, and treatment. Ochsner J. 2015, 15, 58–69.
- Chavez, L.O.; Leon, M.; Einav, S.; Varon, J. Beyond muscle destruction: a systematic review of rhabdomyolysis for clinical practice. Crit. Care 2016, 20, 135. [CrossRef]
- Waldman, W.; Kabata, P.M.; Dines, A.M.; Wood, D.M.; Yates, C.; Heyerdahl, F.; Hovda, K.E.; Giraudon, I.; Euro-DEN Research Group; Dargan, P.I.; Sein, J.A. Rhabdomyolysis related to acute recreational drug toxicity—A Euro-DEN study. PLoS ONE 2021, 16, e0246297. [CrossRef]
- Rixey, A.B.; Glazebrook, K.N.; Powell, G.M.; Baffour, F.I.; Collins, M.S.; Takahashi, E.A.; Tiegs-Heiden, C.A. Rhabdomyolysis: a review of imaging features across modalities. Skeletal Radiol. 2024, 53, 19–27. [CrossRef]
- Petejova, N.; Martinek, A. Acute kidney injury due to rhabdomyolysis and renal replacement therapy: a critical review. Crit. Care 2014, 18, 224. [CrossRef]
- Shimada, M.; Dass, B.; Ejaz, A. A. Paradigm shift in the role of uric acid in acute kidney injury. Semin. Nephrol. 2011, 31, 453–458. [CrossRef]
- Thompson, P. D.; Clarkson, P.; Karas, R. H. Statin-associated myopathy. JAMA 2003, 289, 1681–1690. [CrossRef]
- Gupta, A.; Thorson, P.; Penmatsa, K.; Gupta, P. Rhabdomyolysis: Revisited. Ulster Med. J. 2021, 90, 61–69.
- Lau Hing Yim, C.; Wong, E. W. W.; Jellie, L. J.; Lim, A. K. H. Illicit drug use and acute kidney injury in patients admitted to hospital with rhabdomyolysis. Intern. Med. J. 2019, 49, 1285–1292. [CrossRef]
- Kodadek, L.; Carmichael II, S. P.; Seshadri, A.; Pathak, A.; Hoth, J.; Appelbaum, R.; Michetti, C. P.; Gonzalez, R. P. Rhabdomyolysis: an American Association for the Surgery of Trauma Critical Care Committee Clinical Consensus Document. Trauma Surg. Acute Care Open 2022, 7, e000836. [CrossRef]
- Neves Pinto, G.; Campelo Fraga, Y.; De Francesco Daher, E.; Bezerra da Silva Junior, G. Acute Kidney Injury Due to Rhabdomyolysis: A Review of Pathophysiology, Causes, and Cases Reported in the Literature, 2011–2021. Rev. Colomb. Nefrol. 2023, 10, e619. [CrossRef]
- Wilhelm-Leen, E. R.; Winkelmayer, W. C. Predicting the outcomes of rhabdomyolysis: a good starting point. JAMA Intern. Med. 2013, 173, 1828–1829. [CrossRef]
- Welte, T.; Bohnert, M.; Pollak, S. Prevalence of rhabdomyolysis in drug deaths. Forensic Sci. Int. 2004, 139, 21–25. [CrossRef]
- Larbi, E. B. Drug induced rhabdomyolysis: case report. East Afr. Med. J. 1997, 74, 829–831.
- Rodríguez, E.; Soler, M.J.; Rap, O.; Barrios, C.; Orfila, M.A.; Pascual, J. Risk factors for acute kidney injury in severe rhabdomyolysis. PLoS ONE 2013, 8, e82992. [CrossRef]
- Amanollahi, A.; Babeveynezhad, T.; Sedighi, M.; Shadnia, S.; Akbari, S.; Taheri, M.; Besharatpour, M.; Jorjani, G.; Salehian, E.; Etemad, K.; Mehrabi, Y. Incidence of rhabdomyolysis occurrence in psychoactive substances intoxication: a systematic review and meta-analysis. Sci. Rep. 2023, 13, 17693. [CrossRef]
- Eghbali, F.; Owliaey, H.; Shirani, S.; Fatahi Asl, F.; Hosseinzadeh, R.; Deravi, N.; Ghasemirad, H.; Shariatpanahi, M.; Farajidana, H. Rhabdomyolysis in patients with drug or chemical poisoning: clinical investigation and implications. Int. J. Mol. Sci. 2025, 50, 455–463. [CrossRef]
- Mansoor, K.; Kheetan, M.; Shahnawaz, S.; Shapiro, A.P.; Patton-Tackett, E.; Dial, L.; Rankin, G.; Santhanam, P.; Tzamaloukas, A.H.; Nadasdy, T.; Shapiro, J.I.; Khitan, Z.J. Systematic review of nephrotoxicity of drugs of abuse, 2005–2016. BMC Nephrol. 2017, 18, 379. [CrossRef]
- Flores-Chávez, A.; Carrion, J.A.; Forns, X.; Ramos-Casals, M. Extrahepatic manifestations associated with chronic hepatitis C virus infection. Rev. Esp. Sanid. Penit. 2017, 19, 87–97. [CrossRef]
- Kanters, C.T.M.M.; van Luin, M.; Solas, C.; Burger, D.M.; Vrolijk, J.M. Rhabdomyolysis in a hepatitis C virus-infected patient treated with telaprevir and simvastatin. Ann. Hepatol. 2014, 13, 452–455. [CrossRef]
- Qatomah, A.; Bukhari, M.; Cupler, E.; Alardati, H.; Mawardi, M. Acute reversible rhabdomyolysis during direct-acting antiviral hepatitis C virus treatment: a case report. J. Med. Case Rep. 2021, 15, 627. [CrossRef]
- Bansal, R.; Goel, A.; Mishra, N. Rhabdomyolysis: Heroin induced or HCV related. Indian J. Med. Specialties 2016, 7(4), 174–176. [CrossRef]
- Jensenius, M.; Holm, B.; Calisch, T.E.; Haugen, K.; Sandset, P.M. Dyp venetrombose hos intravenøse stoffmisbrukere [Deep venous thrombosis in intravenous drug addicts]. Tidsskr. Nor. Lægeforen. 1996, 116(21), 2556–2558. Iellin, A.E.; Frankhouse, J.H.; Weaver, F.A. Vascular injury secondary to drug abuse. In Current Therapy in Vascular Surgery, 3rd ed.; Ernst, C.B., Stanley, J.C., Eds.; Mosby: St Louis, MO, USA, 1995; pp. 637–644.
- Pieper, B.; Kirsner, R.S.; Templin, T.N.; Birk, T.J. Injection drug use: an understudied cause of venous disease. Arch. Dermatol. 2007, 143(10), 1305–1309. [CrossRef]
- Pieper, B. Nonviral Injection-Related Injuries in Persons Who Inject Drugs: Skin and Soft Tissue Infection, Vascular Damage, and Wounds. Adv. Skin Wound Care 2019, 32(7), 301–310. [CrossRef]
- Mayo Clinic Staff. Deep vein thrombosis (DVT) – Symptoms & causes. Mayo Clinic, 11 June 2022. Available online: https://www.mayoclinic.org/diseases-conditions/deep-vein-thrombosis/symptoms-causes/syc-20352557 (accessed on 6 January 2026).
- Stark, K.; Massberg, S. Interplay between inflammation and thrombosis in cardiovascular pathology. Nat. Rev. Cardiol. 2021, 18, 666–682. [CrossRef]
- Murillo Solera, A.; Diaz, J.A. The Critical Role of Inflammation in Deep Vein Thrombosis. Endovasc. Today 2024, July Issue. Available online: https://evtoday.com/articles/2024-july/the-critical-role-of-inflammation-in-deep-vein-thrombosis (accessed on 6 January 2026).
- Schulman, S.; Makatsariya, A.; Khizroeva, J.; Bitsadze, V.; Kapanadze, D. The Basic Principles of Pathophysiology of Venous Thrombosis. Int. J. Mol. Sci. 2024, 25, 11447. [CrossRef]
- Baker, M.; Anjum, F.; dela Cruz, J. Deep Venous Thrombosis Ultrasound Evaluation. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2025. Updated 8 August 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK470453/ (accessed on 6 January 2026).
- Arnoldussen, C.W.K.P. Imaging of Deep Venous Pathology. Cardiovasc. Interv. Radiol. 2024, 47(12), 1580–1594. [CrossRef]
- Sorrentino, S.A.; Kielstein, J.T.; Lukasz, A.; Sorrentino, J.N.; Gohrbandt, B.; Haller, H.; Schmidt, B.M. High permeability dialysis membrane allows effective removal of myoglobin in acute kidney injury resulting from rhabdomyolysis. Crit. Care Med. 2011, 39, 184–186.
- Sever, M.S.; Vanholder, R.; RDRTF of ISN Work Group on Recommendations for the Management of Crush Victims in Mass Disasters. Recommendation for the management of crush victims in mass disasters. Nephrol. Dial. Transplant. 2012, 27 Suppl 1, i1–i67. [CrossRef]
- Brown, C.V.; Rhee, P.; Chan, L.; Evans, K.; Demetriades, D.; Velmahos, G.C. Preventing renal failure in patients with rhabdomyolysis: do bicarbonate and mannitol make a difference? J. Trauma 2004, 56, 1191–1196. [CrossRef]
- Kahn, S.R.; Shapiro, S.; Wells, P.S.; Rodger, M.A.; Kovacs, M.J.; Anderson, D.R.; Tagalakis, V.; Houweling, A.H.; Ducruet, T.; Holcroft, C.; Johri, M.; Solymoss, S.; Miron, M.-J.; Yeo, E.; Smith, R.; Schulman, S.; Kassis, J.; Kearon, C.; Chagnon, I.; Wong, T.; Demers, C.; Hanmiah, R.; Kaatz, S.; Selby, R.; Rathbun, S.; Desmarais, S.; Opatrny, L.; Ortel, T.L.; Ginsberg, J.S.; SOX Trial Investigators. Compression stockings to prevent post-thrombotic syndrome: a randomised placebo-controlled trial. Lancet 2014, 383, 880–888. [CrossRef]
- Appelen, D.; van Loo, E.; Prins, M.H.; Neumann, M.H.; Kolbach, D.N. Compression therapy for prevention of post-thrombotic syndrome. Cochrane Database Syst. Rev. 2017, 9, CD004174. [CrossRef]
- Ortel, T.L.; Neumann, I.; Ageno, W.; Beyth, R.; Clark, N.P.; Cuker, A.; Hutten, B.A.; Jaff, M.R.; Manja, V.; Schulman, S.; et al. American Society of Hematology 2020 Guidelines for Management of Venous Thromboembolism: Treatment of Deep Vein Thrombosis and Pulmonary Embolism. Blood Adv. 2020, 4, 4693–4738. [CrossRef]
- Palareti, G.; Santagata, D.; De Ponti, C.; Ageno, W.; Prandoni, P. Anticoagulation and compression therapy for proximal acute deep vein thrombosis. VASA. Zeitschrift für Gefasskrankheiten 2024, 53, 289–297. [CrossRef]
- Stevens, S.M.; Woller, S.C.; Baumann Kreuziger, L.; Doerschug, K.; Geersing, G.J.; Klok, F.A.; King, C.S.; Murin, S.; Vintch, J.R.E.; Wells, P.S.; et al. Antithrombotic Therapy for VTE Disease: Compendium and Review of CHEST Guidelines 2012–2021. Chest 2024, S0012-3692(24)00292-7. [CrossRef]
- Ziyadeh, F.; Mauer, Y. Management of Lower Extremity Venous Thromboembolism: An Updated Review. Cleveland Clin. J. Med. 2024, 91, 229–235. [CrossRef]
- Patel, P.; Varacallo, M.A. Low-Molecular-Weight Heparin (LMWH) [Updated 2025 Mar 28]. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2025. Available online: https://www.ncbi.nlm.nih.gov/books/NBK525957/.
- Gaudry, S.; Grolleau, F.; Barbar, S.; Martin-Lefevre, L.; Pons, B.; Boulet, É.; Boyer, A.; Chevrel, G.; Montini, F.; Bohe, J.; et al. Continuous renal replacement therapy versus intermittent hemodialysis as first modality for renal replacement therapy in severe acute kidney injury: a secondary analysis of AKIKI and IDEAL-ICU studies. Crit. Care 2022, 26, 93. [CrossRef]
- Yılmaz Aydın, F.; Aydın, E.; Kadiroglu, A.K. Comparison of the Treatment Efficacy of Continuous Renal Replacement Therapy and Intermittent Hemodialysis in Patients With Acute Kidney Injury Admitted to the Intensive Care Unit. Cureus 2022, 14, e21707. [CrossRef]
- Chander, S.; Luhana, S.; Sadarat, F.; et al. Mortality and mode of dialysis: meta-analysis and systematic review. BMC Nephrol. 2024, 25, 1. [CrossRef]
- Racheva, R. Attention as a Factor Related to Addictions to Psychoactive Substances. Bulgarian J. Public Health 2025, 17, 30–39.
- Maina, G.; Ogenchuk, M.; Phaneuf, T.; Kwame, A. “I can’t live like that”: the experience of caregiver stress of caring for a relative with substance use disorder. Subst. Abuse Treat. Prev. Policy 2021, 16, 11. [CrossRef]
- Mikulić, M.; Ćavar, I.; Jurišić, D.; Jelinčić, I.; Degmečić, D. Burden and Psychological Distress in Caregivers of Persons with Addictions. Challenges 2023, 14, 24. [CrossRef]
- Tyo, M.B.; McCurry, M.K.; Horowitz, J.A.; Elliott, K. Perceived Stressors and Support in Family Caregivers of Individuals With Opioid Use Disorder. J. Addict. Nurs. 2023, 34, E136–E144. [CrossRef]
- Soellner, R.; Hofheinz, C. Burden and satisfaction with social support in families with a history of problematic substance use or dementia – a comparison. BMC Psychol. 2024, 12, 448. [CrossRef]
Figure 1.
Integrated model of non-traumatic rhabdomyolysis: 1) ATP depletion inhibits Na⁺/K⁺-ATPase activity, resulting in intracellular sodium accumulation. 2) Activation of the Na⁺/Ca²⁺ exchanger increases intracellular calcium levels. 3) Energy deficiency impairs Ca²⁺-ATPase–mediated calcium extrusion; 4) Elevated intracellular Ca²⁺ activates proteases that disrupt plasma and mitochondrial membranes, promoting further Ca²⁺ influx and inducing apoptosis and cell necrosis. 5) Damaged muscle cells subsequently release myoglobin, potassium, phosphate, creatine phosphokinase, and other intracellular constituents into the circulation, causing systemic biochemical disturbances.
Figure 1.
Integrated model of non-traumatic rhabdomyolysis: 1) ATP depletion inhibits Na⁺/K⁺-ATPase activity, resulting in intracellular sodium accumulation. 2) Activation of the Na⁺/Ca²⁺ exchanger increases intracellular calcium levels. 3) Energy deficiency impairs Ca²⁺-ATPase–mediated calcium extrusion; 4) Elevated intracellular Ca²⁺ activates proteases that disrupt plasma and mitochondrial membranes, promoting further Ca²⁺ influx and inducing apoptosis and cell necrosis. 5) Damaged muscle cells subsequently release myoglobin, potassium, phosphate, creatine phosphokinase, and other intracellular constituents into the circulation, causing systemic biochemical disturbances.
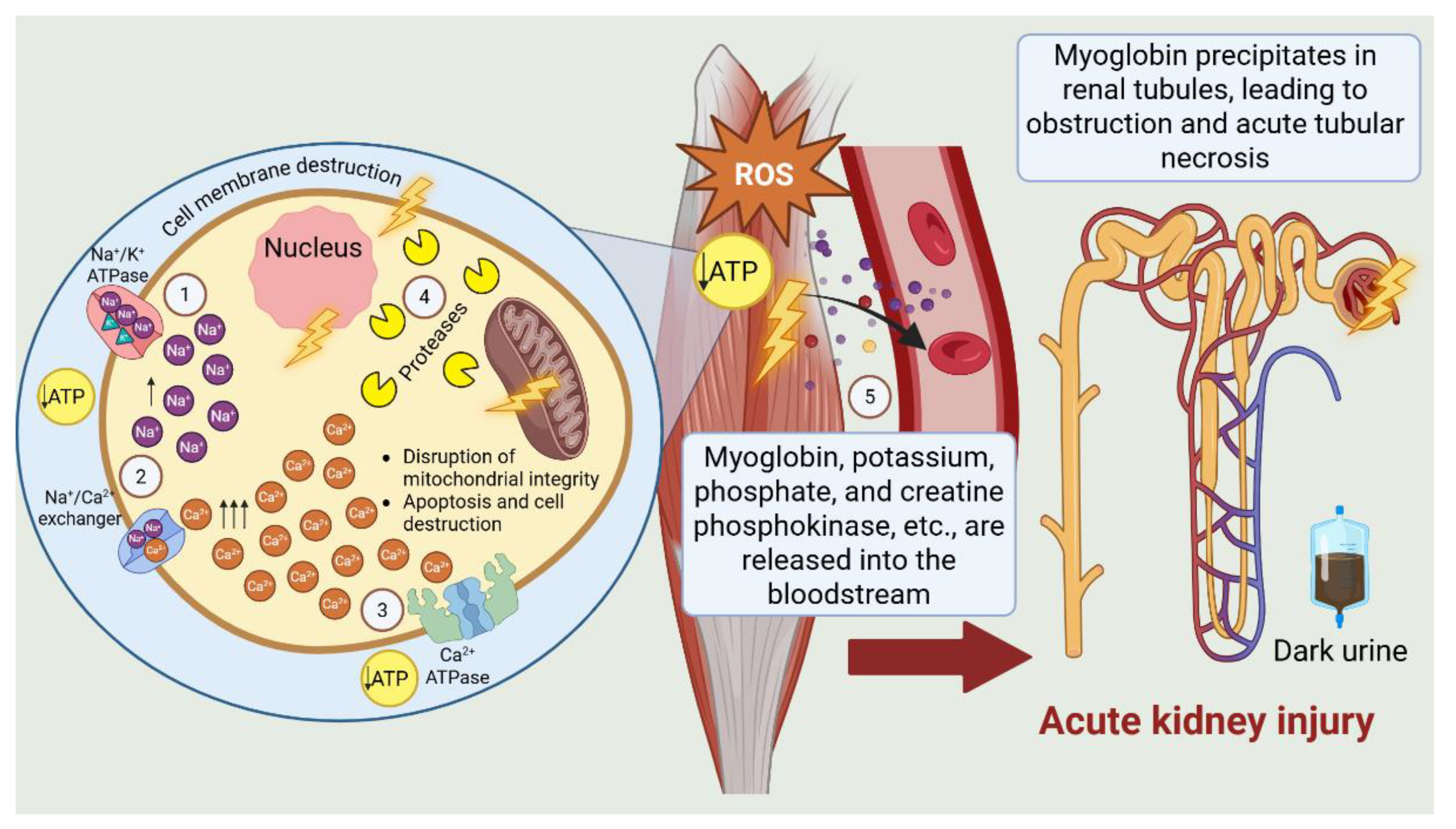

Table 1.
Acute and chronic health consequences arising from substance abuse.
| Category of Effects | Types |
|---|---|
| Acute Effects | ⋅ Intoxication, accidental poisoning, and overdose leading to hospitalization ⋅ Psychiatric manifestations: anxiety, psychosis, paranoia, acute cognitive impairment ⋅ Accidents, injuries, or traffic incidents secondary to psychomotor impairment |
| Chronic Effects | ⋅ Medical (somatic) morbidity: infectious, pulmonary, metabolic, cardiovascular, and oncological diseases ⋅ Poor nutrition and hygiene associated with chaotic lifestyle, increasing risk for somatic health problems ⋅ Psychiatric comorbidity resulting from or exacerbated by substance use |
Table 2.
Clinical timeline.
| Day | Clinical Course |
| Day 1 | ⋅ The patient remained hemodynamically stable, afebrile, alert, and oriented, with persistent pain and edema of the left lower limb. ⋅ Following urethral catheterization, approximately 200 mL of dark-colored urine, resembling tea, was produced. ⋅ Urine toxicology screening was positive for psychoactive substances. ⋅ Serial examinations revealed a livid, markedly edematous, tense, and cool left lower limb with diminished to absent peripheral pulses (+3 cm circumference increase compared to the contralateral limb). ⋅ Electrocardiogram demonstrated sinus tachycardia with nonspecific repolarization changes. ⋅ Laboratory findings indicated massive enzymatic release and early signs of multiorgan dysfunction. ⋅ Cardiological, internal medicine, and surgical consultations were obtained, recommending Doppler ultrasonography and additional vascular assessment. Anticoagulant and symptomatic therapy were initiated. ⋅ Severe hyperkalemia (K⁺ 8.4 mmol/L) was corrected emergently with pharmacological intervention, diuretics, analgesics, and intensive laboratory monitoring. ⋅ Pain and edema persisted without significant change in vascular status by the end of the day. |
| Day 2 | ⋅ No substantial change in overall condition was noted. The patient remained afebrile, alert, and oriented, with persistent pain and cold edema of the left lower leg, along with generalized edema of the limbs and face. ⋅ Urine output remained severely reduced (oligo-anuria), totaling approximately 200–400 mL in 24 hours despite a markedly positive fluid balance. Intensive diuretic and vasoactive therapy was administered without significant effect. ⋅ Hemodynamics were relatively stable with a tendency toward hypertension. ⋅ Respiratory status was stable, with no clinical or laboratory evidence of respiratory failure. ⋅ Laboratory results indicated severe renal impairment (eGFR ≈ 24 mL/min/1.73 m²) in the context of ongoing multisystem dysfunction. ⋅ Extended laboratory tests and consultations with cardiology, nephrology, and vascular surgery were planned for diagnostic clarification and therapeutic planning. |
| Day 3 | ⋅ The patient spent the night relatively calmly, remaining alert, oriented, and afebrile, with persistent left lower limb pain and generalized edema. ⋅ Severe oligo-anuria persisted (≈200 mL of dark urine in 24 hours) despite intensive diuretic and pharmacologic stimulation. Nephrology assessment confirmed acute kidney injury in the context of acute renal failure. ⋅ Hemodynamic and respiratory status remained stable, with a tendency toward hypertension. ⋅ Vascular surgery consultation revealed tense subfascial edema of the entire left lower limb, neurological deficits in the toes, and reduced active movements. Doppler imaging demonstrated thrombosis of the left popliteo-femoral segment without signs of acute arterial occlusion. ⋅ Progression to complete anuria was noted. Infusion therapy with vasoactive and diuretic agents was continued without significant clinical effect. ⋅ Overall condition remained stable, with persistent renal dysfunction, edema, and local vascular complications. ⋅ Extended laboratory monitoring and multidisciplinary consultations were planned. |
| Day 4 | ⋅ The patient remained calm, alert, and oriented, with persistent generalized edema of the face, hands, and feet. ⋅ Severe anuria persisted (≈100 mL/24 h with 900 mL fluid infusion). Renal stimulation therapy with dopamine, furosemide, and novofilin was continued. ⋅ Despite persistent edema, the patient reported reduced pain, allowing ambulation, without new subjective complaints. ⋅ Hemodynamically, the patient remained relatively stable (BP 125–140/68–100 mmHg, HR 76–90 bpm). Spontaneous breathing and oxygen saturation (95–96%) were normal. Pulmonary and abdominal examinations revealed no pathological findings. ⋅ In the evening, the patient remained alert, with mild agitation, reporting urethral pain and hematochezia. |
| Day 5 | ⋅ The patient remained afebrile, with persistent pain in the leg and generalized body pain. The patient was alert, oriented, and cooperative; however, despite institutional restrictions, smoking was observed in the intensive care unit. ⋅ Urine output was markedly reduced (≈100 mL/24 h). ⋅ Vesicular breathing was clear. Generalized edema persisted, most pronounced in the left lower limb. Blood pressure remained elevated (up to 175/110 mmHg); symptomatic antihypertensive therapy (chlofazoline) was administered. ⋅ The patient underwent hemodialysis without complications. ⋅ Later in the day, he decisively refused continued hospital treatment. He was informed of health and life risks and discharged with accompaniment by his mother. |
| Day 6 | ⋅ The patient returned to the clinic, accompanied by family insistence. He was informed in detail of the necessity for urgent dialysis and potential complications of treatment refusal. Despite this, he again refused therapy, demonstrating verbal aggression and demanding removal of venous access and urethral catheter. In the presence of on-duty staff and the head of the clinic, he signed a written refusal of treatment. Immediate life-threatening risks were repeatedly explained. The patient was discharged per his insistence with a medical report including recommendations for follow-up and monitoring. |
| Day 9 | ⋅ The patient died at home following a continued refusal of urgent therapy and hospital treatment. |
Table 3.
Toxicological screening results
| Substance | Cut-Off (Urine, ng/mL) |
Cut-Off (Plasma, ng/mL) |
Result from the analysis | |
|---|---|---|---|---|
| Urine | Plasma | |||
| Amphetamine | 1000 | 80 | – | – |
| Cocaine (Benzoylecgonine) | 300 | 50 | + | + |
| Δ9-Tetrahydrocannabinol metabolite (Marijuana) | 50 | 35 | + | + |
| Benzodiazepines | 300 | 100 | – | – |
| Tricyclic Antidepressants | 1000 | 100 | – | – |
| Barbiturates | 300 | 100 | – | – |
| Morphine (Opiates) | 300 | 40 | – | – |
| Methadone | 300 | 40 | – | – |
| Methamphetamine | 1000 | 70 | + | + |
| 3,4-Methylenedioxymethamphetamine | 500 | 50 | – | – |
| Fentanyl | 20 | 15 | + | – |
Table 4.
Monitoring of Laboratory Parameters.
| Parameter | Reference Range | Day 01 | Day 02 | Day 03 | Day 04 | Day 05 |
|---|---|---|---|---|---|---|
| Complete Blood Count | ||||||
| ESR [mm/h] | <20 | 27.0 | – | – | – | – |
| Hemoglobin [g/L] | 130–180 | 164.0 | – | – | 126.0 | 106.0 |
| Erythrocytes [x10¹²/L] | 4.8–6.2 | 5.53 | – | – | 4.2 | 3.51 |
| Hematocrit [L/L] | 0.35–0.55 | 0.50 | – | – | 0.37 | 0.308 |
| Leukocytes [x10⁹/L] | 3.5–10.5 | 22.21 | – | – | 14.31 | 11.1 |
| St [%] | 1–6 | 87.9 | – | – | 85.8 | 81.1 |
| Eosinophils [%] | 1.5–8 | 0.0 | – | – | 0.1 | 0.0 |
| Basophils [%] | <1 | 0.01 | – | – | 0.01 | 0.0 |
| Lymphocytes [%] | 22–50 | 6.3 | – | – | 7.2 | 12.2 |
| Monocytes [%] | 2–10 | 5.7 | – | – | 5.8 | 5.7 |
| MCV [fL] | 82–100 | 90.4 | – | – | 88.1 | 87.7 |
| MCH [pg] | 28–32 | 29.7 | – | – | 30.0 | 30.2 |
| MCHC [g/L] | 300–360 | 328.0 | – | – | 341.0 | 344.0 |
| RDW [%] | 11.5–14.9 | 14.2 | – | – | 14.3 | 14.4 |
| Platelets [x10⁹/L] | 140–440 | 316.0 | – | – | 170.0 | 136.0 |
| MPV [fL] | 8.8–12.5 | 10.8 | – | – | 10.9 | 11.3 |
| NRBC [x10⁹/L] | <0.01 | 0.01 | – | – | 0.01 | 0.01 |
| NRBC [%] | 0 | 0.0 | – | – | 0.1 | 0.1 |
| Immature Granulocytes [x10⁹/L] | <0.3 | 0.18 | – | – | 0.07 | 0.07 |
| IG [%] | <4 | 0.8 | – | – | 0.5 | 0.6 |
| Neutrophils [x10⁹/L] | 2.4–6.9 | 19.52 | – | – | 12.27 | 9.01 |
| Lymphocytes [x10⁹/L] | 0.8–3.4 | 1.39 | – | – | 1.03 | 1.35 |
| Monocytes [x10⁹/L] | 0.4–1.0 | 1.27 | – | – | 0.98 | 0.74 |
| Biochemistry | ||||||
| Total Bilirubin [μmol/L] | 5–21 | 7.17 | – | – | 5.31 | 7.8 |
| Direct Bilirubin [μmol/L] | <5.13 | – | – | – | 2.36 | 1.77 |
| AST [U/L] | <35 | 2501.8 | – | – | 2588.8 | 2876.68 |
| ALT [U/L] | <50 | 619.4 | – | – | 826.6 | 887.66 |
| GGT [U/L] | <55 | 32.0 | – | – | 16.3 | 21.68 |
| α-Amylase [U/L] | 28–100 | 1472.7 | – | – | 440.6 | 267.66 |
| Albumin [g/L] | 35–53 | – | – | – | 29.5 | 28.92 |
| CRP [mg/L] | <5 | 14.41 | – | – | 53.08 | 31.02 |
| Creatine Kinase [U/L] | 24–180 | 63,444.0 | – | – | 55,050.0 | 161,050.0 |
| Blood Glucose [mmol/L] | 4.1–5.9 | 5.18 | – | – | 5.66 | 5.27 |
| Urea [mmol/L] | 2.8–7.2 | 10.66 | – | – | 24.05 | 33.35 |
| Creatinine [μmol/L] | 64–104 | 260.1 | – | – | 605.2 | 737.0 |
| Sodium [mmol/L] | 135–150 | 133.0 | 130.0 | 128.0 | 127.0 | 126.0 |
| Potassium [mmol/L] | 3.5–5.5 | 8.4 | 6.7 | 6.2 | 6.2 | 6.0 |
| Chloride [mmol/L] | 96–106 | 100.4 | 98.9 | 99.0 | 98.0 | 97.0 |
| Total Protein [g/L] | 60–83 | – | – | – | 53.9 | 53.12 |
| CK-MB [U/L] | <24 | 8576.8 | – | – | 2188.9 | 2360.0 |
| Urinalysis | ||||||
| pH | 4.5–8.0 | – | – | – | 5.5 | – |
| Specific Gravity | 1.010–1.030 | – | – | – | 1.030 | – |
| Protein [g/L] | 0 | – | – | – | 3+ | – |
| Bilirubin | Negative | – | – | – | Negative | – |
| Urobilinogen [μmol/L] | 0–17 | – | – | – | Normal | – |
| Sediment [/μL] | RBC 0–3; WBC 0–5 | – | – | – | RBC 34; WBC 32; BACT 13; SQEP 5; UNCC 3 | – |
| Glucose (urine dipstick) | Negative | – | – | – | 1+ | – |
| Ketones (urine dipstick) [mmol/L] | Negative | – | – | – | Negative | – |
| Nitrites [μmol/L] | Negative | – | – | – | Negative | – |
| Leukocytes (urine dipstick) | 0–5 | – | – | – | 1+ | – |
| Blood in urine | Negative | – | – | – | 1+ | – |
| Immunology | ||||||
| Troponin I [ng/L] | <14 | 10,375.3 | – | – | – | 2,094.66 |
| Arterial Blood Gas – Capillary | ||||||
| BE (ecf) [mmol/L] | ±3 | 1.2 | – | – | –12.8 | –11.6 |
| HCO₃ act [mmol/L] | 22–26 | 22.1 | – | – | 12.9 | 14.1 |
| HCO₃ stat [mmol/L] | 22–26 | 19.8 | – | – | 17.0 | 17.6 |
| O₂ Sat [%] | 95–100 | 94.6 | – | – | 84.7 | 83.8 |
| pCO₂ [kPa] | 4.7–6.0 | 5.6 | – | – | 3.3 | 3.6 |
| pH | 7.35–7.45 | 7.354 | – | – | 7.34 | 7.34 |
| pO₂ [kPa] | 10–13 | 11.2 | – | – | 6.7 | 6.6 |
| tCO₂ [mmol/L] | 22–29 | 24.5 | – | – | 13.5 | 14.8 |
| Lactate [mmol/L] | 0.5–2.2 | – | – | – | 1.4315 | 0.4666 |
| Hemostasis | ||||||
| Prothrombin Time [sec] | 11.8–15 | 21.45 | – | 16.12 | – | 15.89 |
| Prothrombin Activity [%] | 80–120 | 49.22 | – | – | 73.92 | 68.94 |
| aPTT [sec] | 26–38.4 | – | – | – | – | 36.37 |
| INR | 0.7–1.1 | 1.73 | – | – | 1.26 | 1.33 |
| D-dimer [μg/mL] | <0.5 | – | – | – | 2.97 | 2.13 |
| Coagulation Screening | ||||||
| Bleeding Time [sec] | 60–180 | 90 | – | – | – | – |
| Clotting Time [sec] | 130–300 | 210 | – | – | – | – |
Table 5.
Implemented therapeutic courses and interventions by day
| Day | Therapeutic Goal | Treatment | Dose and Route |
|---|---|---|---|
| 1 | IV hydration & electrolyte balance | Sodium chloride 0.9% Ringer lactate Glucose 5% |
500 mL i.v., 2–4×/day 500 mL i.v., 2–4×/day 500 mL i.v., 4×/day |
| Parenteral nutrition | Lipid emulsion | 500 mL i.v., 1 bag over 6 h, as needed | |
| Neurometabolic & vitamin therapy | Piracetam Thiamine Pyridoxine Cyanocobalamin |
1 g i.v., 2×/day 3×/day i.v. 3×/day i.v. 1 mg i.m., 1×/day |
|
| Electrolyte correction | Magnesium / Calcium aspartate | 1 amp i.v., 1×/day | |
| Anxiolytic/psychotropic therapy | Diazepam Haloperidol |
As needed i.v. | |
| Anticonvulsant therapy | Carbamazepine | 200 mg p.o., 3×/day | |
| Anticoagulant prophylaxis | Enoxaparin | 0.4 mL s.c., 2×/day | |
| Antibacterial therapy | Ceftriaxone | 2 g i.v. | |
| Metabolic & antioxidant therapy | S-adenosylmethionine | 2×1 amp i.v. | |
| Diuretic therapy | Furosemide | 1 amp i.v., as needed | |
| Anti-inflammatory therapy | Dexamethasone | 4 mg i.v., 2×/day | |
| 2 | Diuretic & renal support | Furosemide | 2 amp i.v., bolus |
| Metabolic/electrolyte correction | Insulin Actrapid + Glucose 10% + Sodium bicarbonate + Calcium gluconate | 8E Insulin Actrapid in Glucose 10% 500 mL + 1 amp Sodium bicarbonate + 1 amp Calcium gluconate, 2–3 h i.v. infusion | |
| Hemodynamic & renal support | Dopamine + Theophylline + Furosemide | Continuous infusion via perfusor | |
| Anticoagulant therapy | Enoxaparin | 0.6 mL s.c., 1×/day | |
| Venous circulation | Diosmin / Hesperidin | 2×/day orally | |
| Local thrombosis prophylaxis | Heparinoid ointment | 100 IU/mg, topical | |
| Analgesia | Paracetamol | 1 fl. i.v. | |
| 3 | Diuretic & renal support | Furosemide | 5–15 amp i.v. + continuous infusion 15 mL/h |
| Hemodynamic & renal support | Dopamine + Theophylline | Continuous infusion via perfusor | |
| Neurometabolic & vitamin therapy | Piracetam Thiamine Pyridoxine |
1 g i.v., 2×/day 2×/day i.v. 2×/day i.v. |
|
| Gastroprotection | Pantoprazole | 2×/day i.v. | |
| Antibacterial therapy | Ceftriaxone | 2 g i.v. | |
| Analgesia | Analgin | As needed i.v. | |
| Anticoagulant prophylaxis | Enoxaparin | 0.4 mL s.c., 2×/day | |
| Venous circulation | Diosmin/Hesperidin | 2×2 tablets/day | |
| 4 | Diuretic & renal support | Furosemide | i.v., 10× |
| Hemodynamic & renal support | Dopamine Theophylline |
1×/day i.v. 1/2 amp i.v., 5×/day |
|
| Correction of metabolic acidosis | Sodium bicarbonate | i.v., 2×/day | |
| 5 | IV hydration & electrolytes | Sodium chloride 0.9% | 100 mL i.v., 2×/day |
| Metabolic & renal support | Insulin Actrapid + Glucose 10% + Sodium bicarbonate + Calcium gluconate | 8E Insulin Actrapid in Glucose 10% 500 mL + 1 amp Sodium bicarbonate + 1 amp Calcium gluconate, 2–3 h i.v. infusion | |
| Hemodynamic & renal support | Dopamine + Theophylline + Furosemide | Continuous infusion via perfusor | |
| Neurometabolic & vitamin therapy | Piracetam Thiamine Pyridoxine |
1 g i.v., 2×/day 2×/day i.v. 2×/day i.v. |
|
| Gastroprotection | Pantoprazole | 2×/day i.v. | |
| Antibacterial therapy | Ceftriaxone | 2 g i.v. | |
| Anticoagulant prophylaxis | Enoxaparin | 0.4 mL s.c., 2×/day | |
| Hypertension control | Clonidine | 0.15 mg, tablets | |
| Renal support | Hemodialysis | – |
Table 6.
Incidence of rhabdomyolysis and fatal outcomes associated with individual psychoactive substances and alcohol in clinical and epidemiological studies, presented chronologically.
Table 6.
Incidence of rhabdomyolysis and fatal outcomes associated with individual psychoactive substances and alcohol in clinical and epidemiological studies, presented chronologically.
| Source | Study design | Number of patients with rhabdomyolysis due to substance use | Rhabdomyolysis (%) by substance | Fatality (%) by substance |
| Welte T. (2004) [51] | Retrospective forensic study | 103 (drug deaths) | Heroin/other opioids – NR Methadone – NR Cocaine – NR Alcohol – NR Benzodiazepines – NR |
50.5% of fatal drug abuse cases showed confirmed or probable rhabdomyolysis based on the presence of myoglobin in renal tissue (no stratification by substance) |
| Rodríguez E. (2013) [53] | Retrospective cohort | 35 (of 126) | Heroin – 24% Cocaine – 22.4% Other substances – 19.8% Alcohol – 13.5% “Smart drugs” – 5.6% |
NR |
| Lau Hing Yim C. (2019) [47] | Retrospective cohort | 77 (of 643) | NR | NR |
| Waldman W. (2021) [41] | Observational (Euro-DEN) | 468 (of 1,015) | Cocaine – 22.9% Amphetamine – 16.2% Cannabis – 15.8% GHB/GBL – 15.4% Heroin – 14.3% |
NR |
| Amanollahi A. (2023) [54] | Systematic review & meta-analysis | NR | Heroin – 57.2%† Amphetamines – 30.5%† Methamphetamine – 40.3%† MDMA – 19.9%† Cocaine – 26.6%† Tramadol – 17.1%† Methadone – 16.1%† Synthetic cannabinoids – 10.3%† Opioids overall – 8.8%† Ethanol – 3.0%† Methanol – 2.0%† |
NR |
| Eghbali F. (2025) [55] | Cross-sectional clinical | 455 (of 788) | Methadone – 41.5% Benzodiazepines – 10.1% Opium – 6.1% |
Methadone – 5.2% Benzodiazepines – 0.8% Others – NR |
| NR = Not reported; †Substance-specific incidence proportions across studies. | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



