Submitted:
15 January 2026
Posted:
16 January 2026
You are already at the latest version
Abstract
Severe malaria in pregnancy remains a major contributor to maternal and perinatal morbidity in sub-Saharan Africa. When complicated by thrombocytopenia and fetal distress, management is particularly challenging in resource-limited settings, creating an ethical and clinical dilemma: whether to proceed with urgent delivery or delay for maternal stabilization. We report a 31-year-old multiparous Ghanaian woman at 37 weeks and 2 days of gestation, referred with suspected pre-eclampsia and fetal distress following a recent malaria episode treated with oral Artemether-Lumefantrine. She had received five doses of intermittent preventive treatment with sulfadoxine–pyrimethamine and an insecticide-treated net, but she did not use it. Investigations revealed severe Plasmodium falciparum malaria (parasite density 22,268/μL), moderate anemia (Hb 8.9 g/dL), marked thrombocytopenia (37 × 10⁹/L), and persistent fetal tachycardia (162–187 bpm). Emergency cesarean section was deferred due to unavailable blood products. She received intravenous Artesunate and supportive care, resulting in maternal stabilization and resolution of fetal tachycardia. One week later, induction of labor led to spontaneous vaginal delivery of a healthy infant. This case underscores overlapping malaria and hypertensive disorders, declining preventive efficacy, and health-system challenges, highlighting the importance of vigilant maternal stabilization and adaptive management to improve outcomes.
Keywords:
malaria in pregnancy
; fetal distress
; thrombocytopenia
; maternal stabilization
; term pregnancy
; resource-limited setting
; Ghana
1. Introduction
Severe malaria remains a major cause of maternal and perinatal morbidity in sub-Saharan Africa [1]. It can precipitate anemia, thrombocytopenia, and placental insufficiency, often resulting in fetal distress and maternal instability [2]. Thrombocytopenia in malaria is primarily attributed to immune-mediated destruction of platelets, splenic sequestration, and dysregulation of thrombopoiesis within the bone marrow [3]. Studies have consistently demonstrated a strong correlation between severe malaria during pregnancy and adverse fetal outcomes, including intrauterine growth restriction, preterm birth, and stillbirth, often precipitated by placental dysfunction and subsequent fetal hypoxia [4].
Malaria in pregnancy (MiP) may present with fever, chills, headache, anemia, hypoglycemia, jaundice, respiratory distress, thrombocytopenia, altered consciousness, and signs of placental insufficiency such as decreased fetal movement or non-reassuring fetal heart rate patterns [5]. The presentation of severe thrombocytopenia further compounds the surgical risks, increasing the likelihood of intraoperative and postoperative hemorrhagic complications, which are already elevated in emergency obstetric procedures [6]. The particular confluence of severe malaria, thrombocytopenia, and fetal distress at term pregnancy, therefore, presents a formidable challenge for obstetricians, demanding rapid assessment and judicious decision-making under high-stakes conditions [7].
The World Health Organization (WHO) recommends a three-pronged approach for MiP: intermittent preventive treatment with sulfadoxine–pyrimethamine (IPTp-SP), insecticide-treated net (ITN) use, and prompt diagnosis and effective treatment of clinical malaria during antenatal care (ANC) [8]. Historically, MiP was a significant cause of maternal and fetal mortality in Ghana, particularly before the introduction of sustained WHO-recommended control interventions. Over the past decade, the country has seen a notable decline in malaria transmission due to the widespread implementation of WHO-recommended strategies [9]. As malaria transmission declines, however, the naturally acquired immunity that previously helped regulate parasite densities may wane, potentially leading to higher parasite densities and attendant complications [10]. Thus, health workers must be vigilant to make prompt decisions and manage patients effectively, thereby preventing adverse outcomes.
In resource-limited settings, the decision to proceed with immediate delivery or delay for maternal stabilization in an obstetric emergency presents a difficult ethical and clinical dilemma. This report highlights a real-life scenario in which a surgeon faced a dilemma when managing a pregnant woman with severe malaria and thrombocytopenia who presented with fetal distress at term. This case report further highlights the challenges posed by MiP, a condition whose prevalence in Ghana has shown a decreasing trend, yet still contributes significantly to adverse pregnancy outcomes [10]. Early diagnosis may be challenging because malaria symptoms such as nausea, vomiting, fatigue, and anemia closely resemble normal pregnancy symptoms [11]. In addition, MiP may clinically overlap with pre-eclampsia, as both conditions can present with anemia, thrombocytopenia, and adverse maternal and fetal outcomes, further complicating timely diagnosis [12]. Diagnosis of MiP is further complicated because infected erythrocytes tend to sequester in the placenta and may not appear in peripheral blood smears [13].
2. Case Presentation
A 31-year-old Ghanaian woman, gravida 5 para 3+1 spontaneous abortion, at 37 weeks and 2 days of gestation, presented to the maternity unit of Tetteh Quarshie Memorial Hospital (TQMH) at 10 pm on 2nd October 2025. She was referred from a peripheral facility as a case of suspected preeclampsia and fetal distress with a two-day history of worsening lower abdominal pain, suspected uterine contractions, and reduced fetal movement. Two weeks earlier, she had experienced fever, chills, and vomiting, diagnosed as malaria and treated with oral Artemether-Lumefantrine (AL) by the peripheral health facility.
According to her antenatal records, she had been tested for malaria twice with the malaria rapid diagnostic test: the first test at 18 weeks (Figure 1), which was negative, and the second at 35 weeks of gestation, which was positive and treated with oral antimalarial medication, the episode that led to her subsequent referral (Figure 2). She had also received five doses of IPTp-SP, with the first dose at 16 weeks and the following four doses given at four-weekly intervals (Figure 3). Her final dose was administered at 33 weeks of gestation. Additionally, she was given an insecticide-treated net (ITN) at booking, but she reported not using it during her pregnancy.
She was referred with a blood pressure (BP) of 144/96 mmHg, a pulse of 125 beats per minute (bpm), and positive urine proteins. Fetal heart rate was 165 bpm, indicating fetal distress. Measurements upon her arrival at TQMH showed BP of 135/68 mmHg, pulse of 60 bpm, and negative urine proteins. On examination, she was pale, afebrile, with a gravid uterus measuring 37 cm, cephalic presentation, and lower abdominal tenderness. Fetal heart rate ranged between 179–186 bpm with minimal variability. Vaginal speculum examination revealed a closed cervix and intact membranes.
Laboratory investigations conducted at the TQMH on day 1 of admission revealed hemoglobin 8.9 g/dL, white cell count of 3.2 × 109/L, and platelets 37 × 109/L. Blood film showed a high Plasmodium falciparum trophozoite density (22,268 parasites/μL). Urine routine examination- Clear and light amber, protein (-), ketones (+++), nitrite (-), pus cells were 3/high power field (hpf), epithelial cells were 7/hpf. Blood urea and creatinine- Unremarkable. Obstetric ultrasound confirmed a live intrauterine pregnancy with an estimated age of 39 weeks + 5 days, a fetal weight of 2.9 kg, and a normal amniotic fluid index. Cardiotocography showed fetal tachycardia of 180 bpm (Figure 4). A definitive diagnosis of severe malaria in a term pregnancy complicated by thrombocytopenia, anemia, and fetal distress was made. “Pre-eclampsia was ruled out”. The initial decision was to do an emergency cesarean section to deliver the baby. However, at that point, no fresh frozen plasma or platelet products were available. The whole blood available was about a week old, sampled with platelet depletion, and couldn’t have replaced the platelet deficit. At midnight, it was also difficult to find a donor. The attending surgeon faced a dilemma: to perform an immediate cesarean section to save the baby or delay to stabilize the mother medically and hope for a positive outcome. Given the high hemorrhagic risk, the surgeon opted to delay surgery and commenced intravenous Artesunate per WHO protocol (204 mg at 0, 12, and 24 hours), alongside oxygen therapy and intravenous fluids. Fetal heart rate was monitored every 30 minutes (Figure 5). Remarkably, within four hours, the fetal heart rate was normalizing. It was observed that the patient felt better, uterine contractions had ceased, and fetal heart rate had normalized by 24 hours of initiating IV Artesunate administration. Also, maternal temperature, blood pressure, and pulse returned to values within normal ranges. The patient received two units of blood transfusions: the first unit of B+ blood was administered on admission day 2, and the second unit was given on day 3 of admission.
She completed a three-day course of oral Artemether-Lumefantrine after the first 24 hours of IV artesunate and was discharged home after 4 days of admission. A week later, she was observed with a follow-up review and was readmitted. An induction of labor was done, which led to spontaneous vaginal delivery of a healthy baby weighing 3.6 kg. Both mother and baby were discharged on day 2 after the second admission in good condition. At the post-delivery review, the mother and baby were in good health with no symptoms.
3. Discussion
In this case, a 31-year-old woman at 37 weeks of gestation presented with suspected preeclampsia, accompanied by fetal distress, anemia, and thrombocytopenia. However, her laboratory results confirmed severe malaria with high Plasmodium falciparum infection. A definitive diagnosis of MiP is essential before initiating management for pre-eclampsia, particularly in endemic regions where the two conditions share overlapping symptoms. Features such as headache, vomiting, thrombocytopenia, liver dysfunction, and misclassification can delay life-saving antimalarial therapy [12].
It was documented that this client received approximately five doses of IPTp at four-week intervals under direct observation, with the final dose administered at 33 weeks. Despite receiving five doses of IPTp-SP at monthly intervals, this client developed malaria at 35 weeks, two weeks after the last dose. Recent evidence indicates that the efficacy of SP for preventing malaria is reduced in regions with high SP resistance [14]. Thus IPTp-SP could be offering less protection against malaria infection even when guideline-recommended doses are administered, although it may still confer some benefits for birth outcomes such as improved birth weight [14,15]. Although she was provided with an ITN at her booking ANC contact, she did not use it during her pregnancy. Sleeping consistently under ITNs reduces maternal malaria infection, which in turn lowers the risk of complications such as anemia and preterm birth [16]. Combining IPTp-SP with regular use of ITNs is more effective in reducing maternal malaria infection than IPTp-SP alone, as ITNs provide continuous protection against malaria transmission, particularly at night when mosquitoes are most active, thereby enhancing the effectiveness of IPTp [17]. Pregnant women need to be encouraged to consistently use the ITN during pregnancy in addition to receiving IPTp-SP during their ANC contacts.
Decline in malaria transmission erodes naturally acquired immunity, potentially leading to higher parasite densities and increased risk of complications [10]. This is consistent with our patient’s presentation, as she had high parasite densities. She resided in an urban area, where malaria prevalence is generally lower, and opportunities to develop and sustain the naturally acquired immunity are reduced. The 2022 Ghana Demographic and Health Survey (DHS) reported a three times lower malaria prevalence in children under five in urban areas (4.3%) compared to those in rural areas (12.8%), underscoring the substantially lower transmission intensity in urban settings and hence the potential for more severe disease when infection does occur [18].
This woman received a full dose of oral AL when she was diagnosed with malaria at 35 weeks of gestation; however, she went on to develop severe malaria by 37 weeks of gestation. There is the possibility of non-adherence to treatment on the woman’s side [19]; however, a closer look at the management of confirmed malaria infection in pregnancy, especially at peripheral health facilities in this era of reduced malaria transmission, may need to be taken. Oral artemisinin-based combination therapy (ACT) remains guideline-recommended; however, systemic and practical challenges such as drug stock-outs, inconsistent service delivery, and poor adherence can undermine its effectiveness and influence treatment outcomes [9,19,20]. Health workers in malaria-endemic settings may require re-orientation on the management of MiP in the context of reducing malaria transmission patterns. Enhanced clinical vigilance is needed, including consideration of short-term observation of pregnant women to assess symptom resolution, timely escalation to parenteral therapy where indicated, and increased awareness of atypical presentations, particularly in rural facilities with limited access to laboratory diagnostics and parasite density testing [19,20]. Should the woman have been detained and offered a 24-hour IV Artesunate and followed with the oral ACT when she was first diagnosed, she probably would not have ended up with the complications she developed.
The successful management of this patient, without recourse to immediate cesarean section despite indications of fetal distress, highlights the potential for conservative, yet intensive, medical management to achieve positive maternal and neonatal outcomes [21]. This approach effectively mitigated the significant maternal risks associated with emergency surgery in the presence of severe thrombocytopenia, such as hemorrhage and coagulopathy, without compromising fetal viability [22]. The decision to delay surgical intervention, despite fetal distress, was further justified by the resolution of the tachycardia following maternal stabilization, demonstrating the interconnectedness of maternal systemic health and fetal well-being [23].
4. Conclusions
This case illustrates the clinical dilemma faced when managing life-threatening emergencies in pregnancy, where overlapping features of MiP and pre-eclampsia can complicate diagnosis and decision-making. Prompt recognition of malaria and prioritization of maternal stabilization over immediate surgical intervention were pivotal to achieving favorable maternal and neonatal outcomes, underscoring the importance of accurate diagnosis in endemic settings [2]. Beyond the individual case, it highlights emerging challenges in malaria control, including declining transmission with erosion of naturally acquired immunity, possible increasing parasite resistance to established interventions, and inadequacy of current management guidelines for the treatment of MiP at the periphery that may limit the effectiveness of current prevention and treatment strategies [9,10,19,20]. In this evolving epidemiological context, heightened clinical vigilance and a high index of suspicion for malaria remain essential across all levels of maternal healthcare.
Funding
This work was self-funded.
Institutional Review Board Statement
The authors were granted permission by the Head of Obstetric and Gynecology Department, Tetteh Quarshie Memorial Hospital, to conduct this study, using information from the medical records of the hospitalized patient, with the provision that no personal data of the patient would be used.
Informed Consent Statement
Written Informed consent was obtained from the patient involved in the study.
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author(s).
Conflicts of Interest
The authors declare no conflicts of interest.
Acknowledgments
Special Appreciation to Dr Joseph Opare and Dr Victor Loglo for their immense contributions.
References
- World Health Organization. (2024). World Malaria Report 2024. Available online: https://www.who.int/teams/global-malaria-programme/reports/world-malaria-report-2024.
- Rogerson, S.J.; Hviid, L.; Duffy, P.E.; Leke, R.F.G.; Taylor, D.W. Malaria in pregnancy: Pathogenesis and immunity. The Lancet Infectious Diseases 2007, 7, 105–117. [Google Scholar] [CrossRef] [PubMed]
- Mayala, A.M.M.; Diama, D.N.; Diama, A.A.M.; Lubaki, J.-P.F.; Lukanu, P.N. Prevalence of Coinfection Malaria-Covid-19 at the International Hospital Center of Kinshasa during the 3<sup>rd</sup> Wave of the Pandemic. Advances in Infectious Diseases 2023, 13, 468. [Google Scholar] [CrossRef]
- Mwin, P.K.; Kuffuor, A.; Nuhu, K.; Okine, R.; Kubio, C.; Wurapa, F.; Osei, F.; Afari, E. Predictors of placental malaria in Upper West Regional Hospital-Ghana. BMC Pregnancy and Childbirth 2021, 21. [Google Scholar] [CrossRef] [PubMed]
- Takem, E.N.; D’Alessandro, U. Malaria in pregnancy. Mediterranean Journal of Hematology and Infectious Diseases 2013, 5, e2013010. [Google Scholar] [CrossRef] [PubMed]
- Olajumoke, T.O.; Babatunde, O.P.; Adelekan, A.A.; Ola, B.N. Emergency Cesarean Section in a COVID-19 Patient with Antepartum Hemorrhage: A Case Report. Open Journal of Anesthesiology 2022, 12, 249. [Google Scholar] [CrossRef]
- Tsikouras, P.; Tempelhoff GFvon Rath, W.; Nikos, N. New Aspects in Cesarean Sections. In IntechOpen eBooks; IntechOpen; 2022. [Google Scholar] [CrossRef]
- World Health Organization. Intermittent preventative treatment to reduce the risk of malaria during pregnancy (ELENA intervention). World Health Organization. 2024. Available online: https://www.who.int/tools/elena/interventions/iptp-pregnancy.
- Osarfo, J.; Ampofo, G.D.; Tagbor, H. Trends of malaria infection in pregnancy in Ghana over the past two decades: a review. Malaria Journal 2022, 21, 3. [Google Scholar] [CrossRef] [PubMed]
- Ampofo, G.D.; Osarfo, J.; Aberese-Ako, M.; Asem, L.; Komey, M.; Mohammed, W.; Ofosu, A.; Tagbor, H. Malaria in pregnancy control and pregnancy outcomes: a decade’s overview using Ghana’s DHIMS II data [Review of Malaria in pregnancy control and pregnancy outcomes: a decade’s overview using Ghana’s DHIMS II data]. Malaria Journal 2022, 21. [Google Scholar] [CrossRef] [PubMed]
- Desai, M.; ter Kuile, F.O.; Nosten, F.; McGready, R.; Asamoa, K.; Brabin, B.; Newman, R.D. Epidemiology and burden of malaria in pregnancy. The Lancet Infectious Diseases 2007, 7, 93–104. [Google Scholar] [CrossRef] [PubMed]
- Steketee, R.W.; Nahlen, B.L.; Parise, M.E.; Menendez, C. The burden of malaria in pregnancy in malaria-endemic areas. American Journal of Tropical Medicine and Hygiene 2001, 64, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Chua, C.L.L.; Khoo, S.K.M.; Ong, J.L.E.; Ramireddi, G.K.; Yeo, T.W.; Teo, A. Malaria in pregnancy: From placental infection to its abnormal development and damage. Frontiers in Microbiology 2021, 12, 777343. [Google Scholar] [CrossRef] [PubMed]
- Odom John. (2022). Prevention of malaria in pregnancy: The threat of sulfadoxine-pyrimethamine resistance. Frontiers in Pediatrics. Available online: https://www.frontiersin.org/journals/pediatrics/articles/10.3389/fped.2022.966402/fullFrontiers.
- van Eijk, A.M.; et al. The impact of sulfadoxine–pyrimethamine resistance on the effectiveness of intermittent preventive treatment for the prevention of malaria in pregnancy in Africa: An updated systematic review and meta-analysis. The Lancet Infectious Diseases 2025. [Google Scholar] [CrossRef] [PubMed]
- Gamble, C.; Ekwaru, J.P.; Garner, P.; ter Kuile, F.O. Insecticide-treated nets for preventing malaria in pregnancy. Cochrane Database of Systematic Reviews 2006, (2), CD003755. [Google Scholar] [CrossRef] [PubMed]
- Madukwe, J.C.; Ahaneku, E.B.; Onukafor, O.S.; et al. Do women attending antenatal clinics who use only intermittent preventive treatment (IPTp) have higher Plasmodium falciparum prevalence compared to those who used both IPTp and slept under insecticide-treated nets? Malar J 2025, 24, 275. [Google Scholar] [CrossRef] [PubMed]
- Ghana Statistical Service (GSS) & ICF. (2023). 2022 Ghana Demographic and Health Survey: Summary report. Ghana Statistical Service & ICF. Available online: https://ghana.unfpa.org/sites/default/files/pub-pdf/ghana_dhs_2022_summary_report.pdf.
- Aberese-Ako, M.; Magnussen, P.; Ampofo, G.D.; Tagbor, H. Managing intermittent preventive treatment of malaria in pregnancy challenges: An ethnographic study of two Ghanaian administrative regions. Malaria Journal 2020, 19, 407. [Google Scholar] [CrossRef] [PubMed]
- Aberese-Ako, M.; Magnussen, P.; Tagbor, H. Motivators and demotivators to accessing malaria in pregnancy interventions in sub-Saharan Africa: A meta-ethnographic review. Malaria Journal 2022, 21, 263. [Google Scholar] [CrossRef] [PubMed]
- Drummond, W.K.; Rees, K.; Ladd-Wilson, S.; Mace, K.E.; Blackall, D.P.; Sutton, M. Delayed Plasmodium falciparum Malaria in Pregnant Patient with Sickle Cell Trait 11 Years after Exposure, Oregon, USA. Emerging Infectious Diseases 2023, 30. [Google Scholar] [CrossRef] [PubMed]
- Abadi, K.; Jama, A.H.; Addi, H.; Yemane, A.; Gebremichael, A. Spontaneous Rupture of Uterine Vessels in the Third Trimester of Pregnancy Resulting in Severe Hemoperitoneum and Fetal Death: A Case Report and Literature Review. International Medical Case Reports Journal 2023, 561. [Google Scholar] [CrossRef] [PubMed]
- Sooknarine, C.; Çetin, E.; Pyatt, D.W.; Saçıntı, K.G.; Akinpeloye, A. Second-trimester spontaneous uterine rupture: a rare case of diagnostic nuances and multidisciplinary management. Journal of the Turkish-German Gynecological Association 2024. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
First Malaria test at 18weeks of gestation.
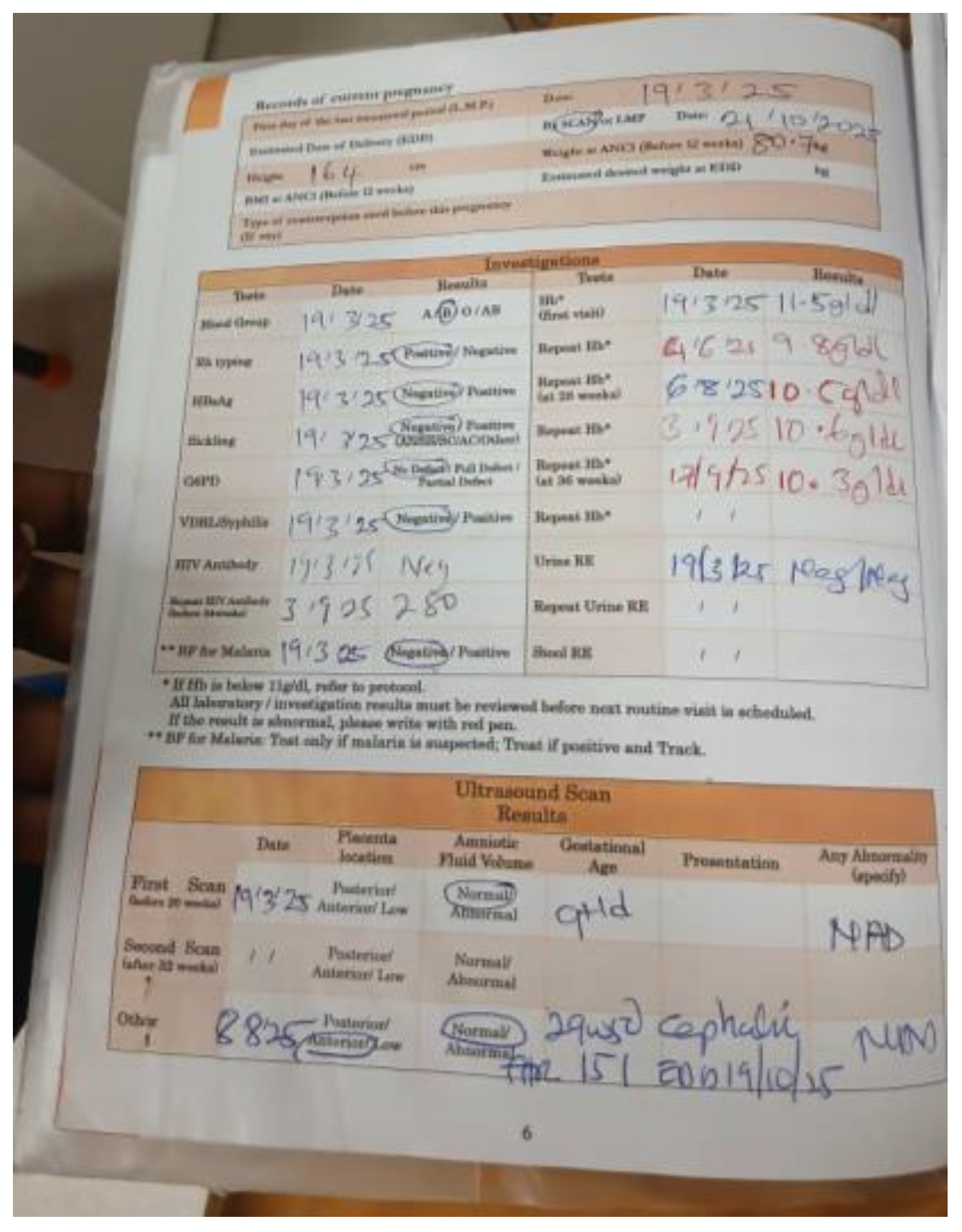
Figure 2.
Second Malaria test at 35weeks of gestation.
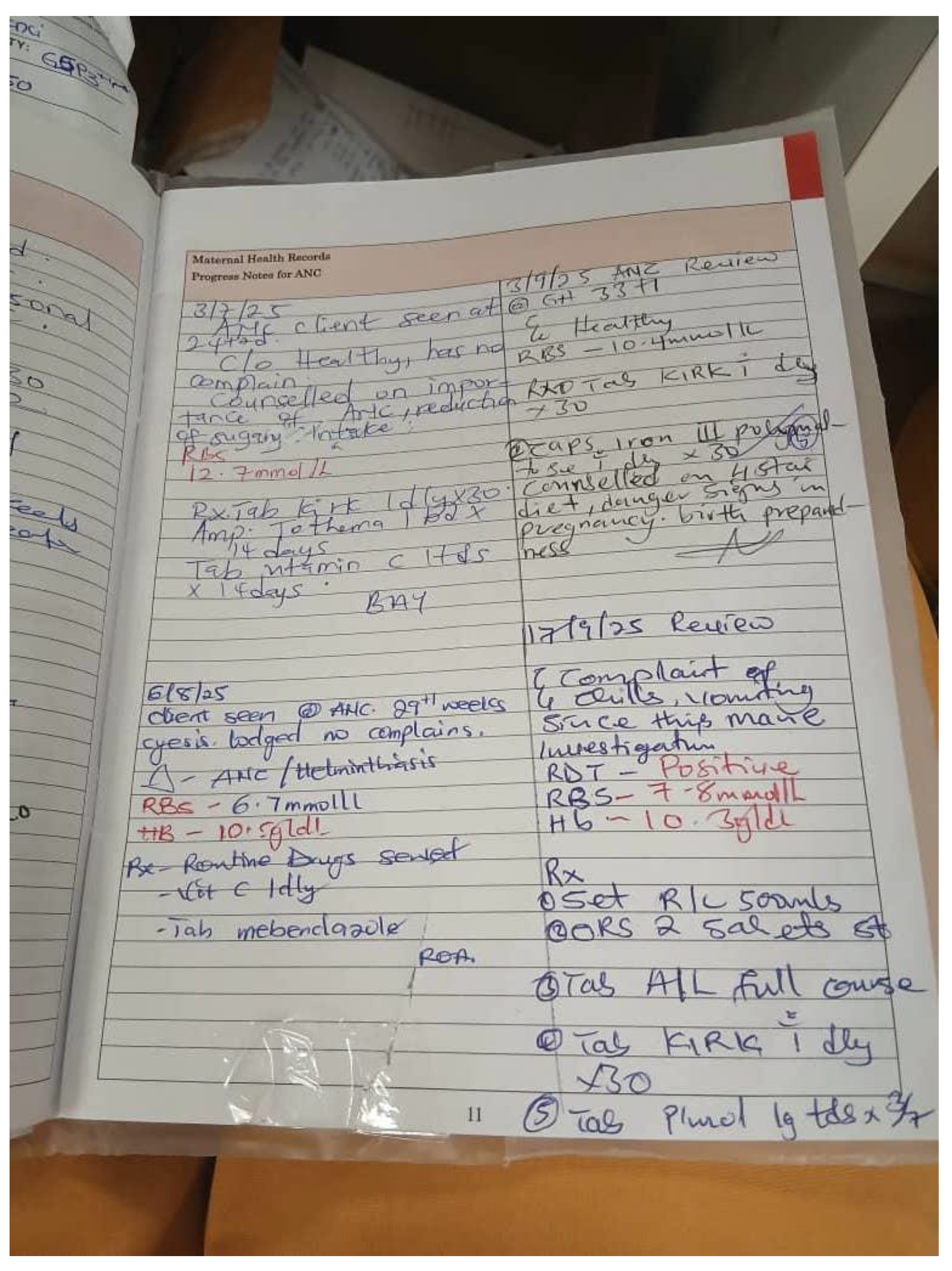
Figure 3.
Five doses of IPTp-SP.
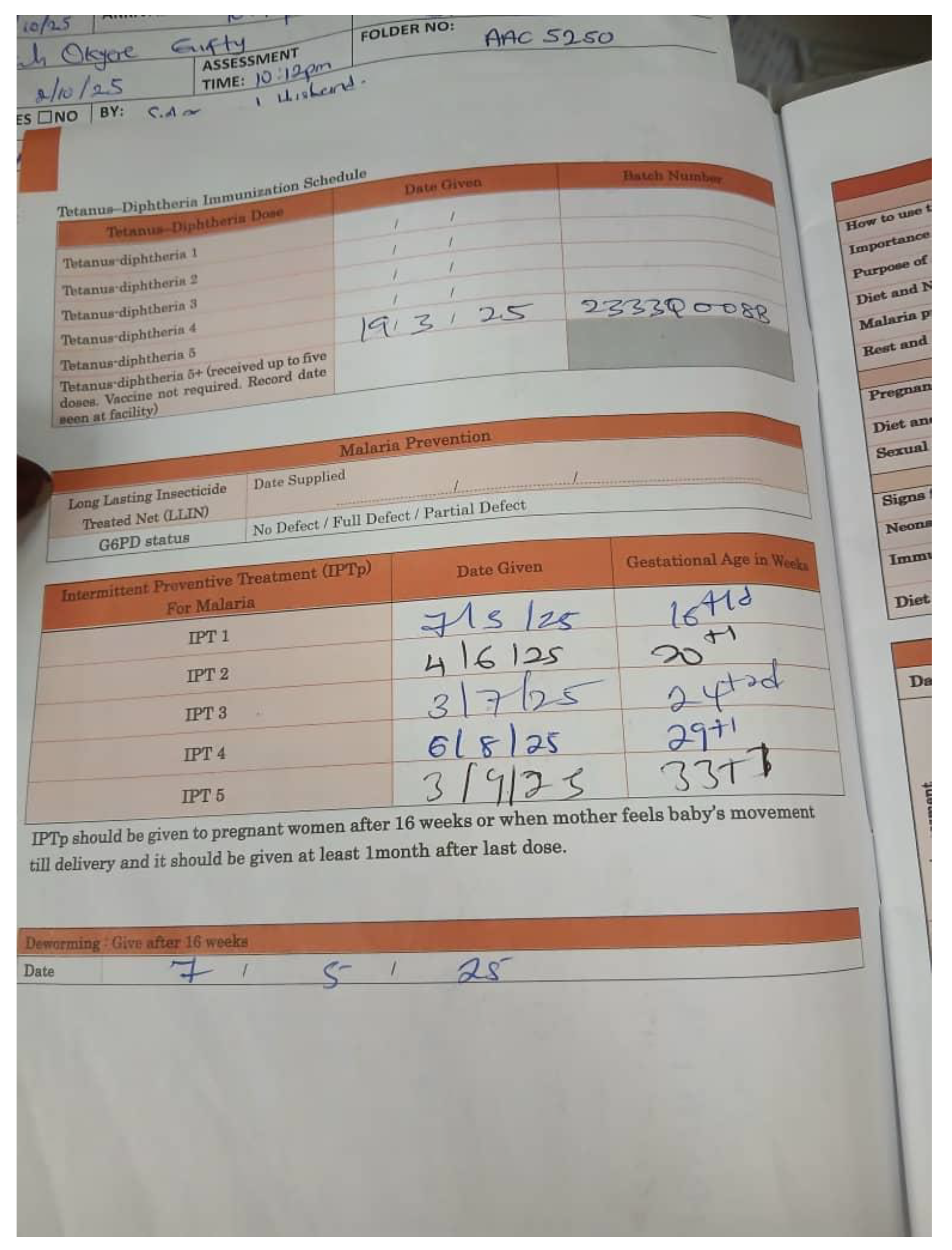
Figure 4.
Cardiotocography findings on day 1 of admission.
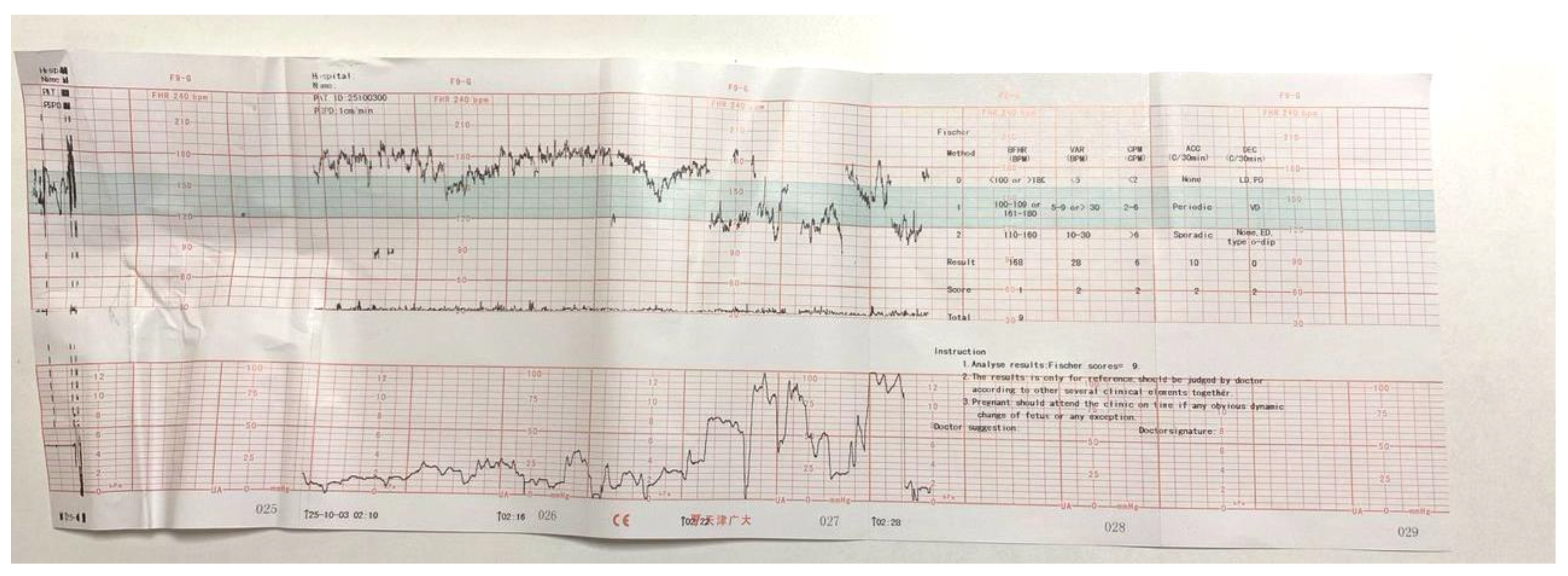
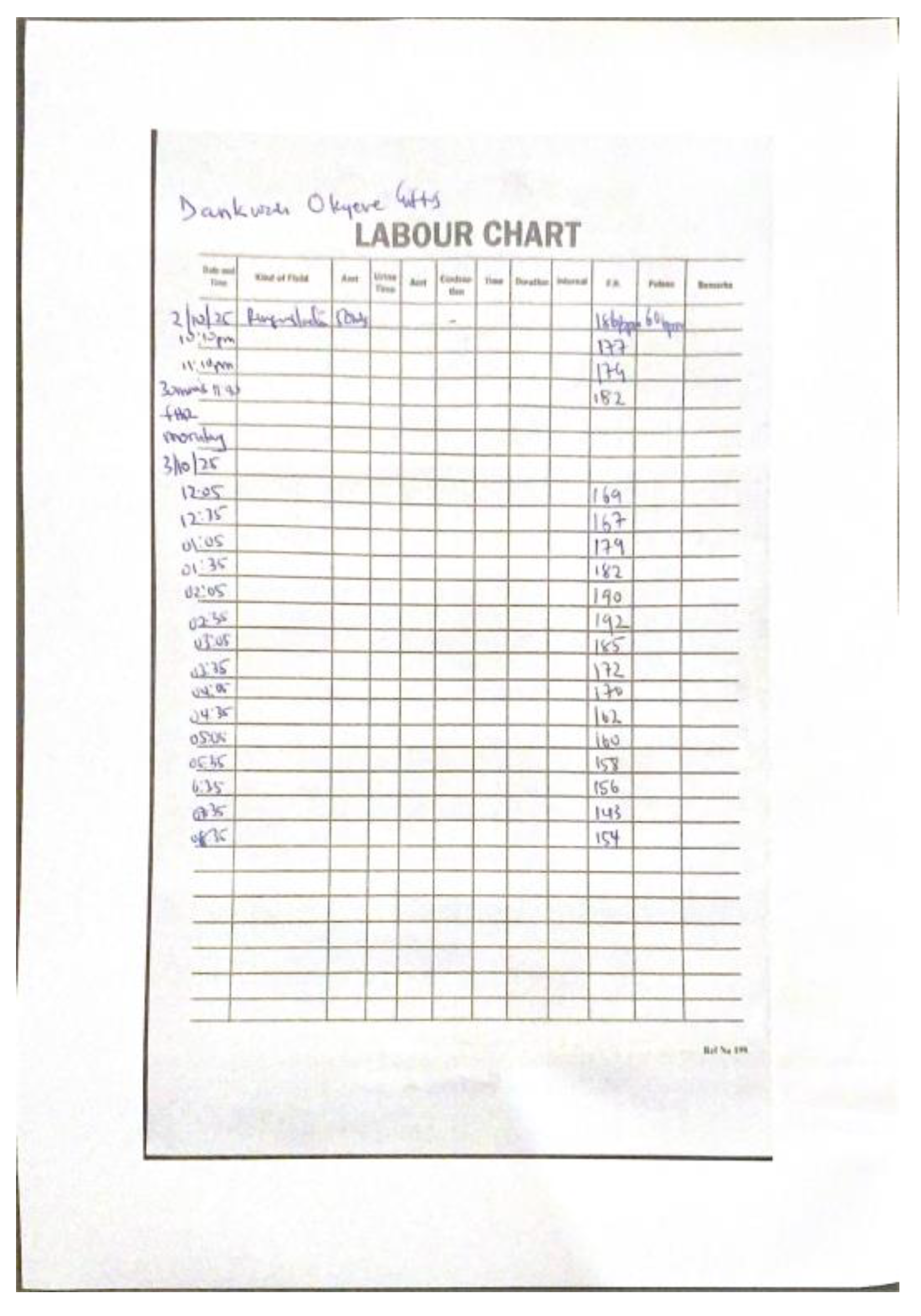
Figure 5.
Fetal Heart Monitoring Chart on day one of admission.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



