Submitted:
10 January 2026
Posted:
12 January 2026
You are already at the latest version
Abstract
Rationale: Urban–rural inequities in primary healthcare (PHC) service delivery remain a major barrier to achieving Sustainable Development Goal 3 (SDG 3) in low- and middle-income countries. In Nigeria, limited empirical evidence exists on how structural capacity, governance, and utilisation pathways jointly shape these disparities at the frontline health system level, particularly in underserved riverine states such as Bayelsa. Objectives: This study assessed urban–rural disparities in PHC service delivery in Bayelsa State, southern Nigeria, with a focus on service readiness, governance and performance management, utilisation pathways, and prospects for strengthening PHC systems to advance SDG 3. Methods: A cross-sectional facility-based assessment was conducted across 34 government-owned PHC facilities (17 rural and 17 urban). Standardised indicators were used to evaluate human resources, infrastructure and utilities, equipment readiness, infection prevention and control, medicine availability, health information systems, governance practices, and service utilisation pathways. Urban–rural differences were analysed using chi-square or Fisher’s exact tests, with statistical significance set at p<0.05. Results: Rural PHC facilities exhibited significantly greater weaknesses in infrastructure, electricity and water supply, basic medical equipment, infection prevention and control, waste management, essential medicine availability, and referral system functionality. Rural facilities were more likely to experience frequent medicine stock-outs (64.7% vs. 11.8%, p=0.001), lack electricity (64.7% vs. 0.0%, p<0.001), and report non-functional referral systems (58.8% vs. 11.8%, p=0.004). Despite these deficits, rural PHCs demonstrated high service utilisation and stronger routine data reporting. Governance indicators—including planning, target setting, and community engagement—were largely comparable across settings, although urban facilities achieved a higher proportion of planned service targets. Urban PHCs showed relatively stronger infrastructure and equipment readiness but notable weaknesses in essential drug availability and health information reporting. Conclusion: Urban–rural disparities in PHC delivery in Bayelsa State are driven primarily by unequal distribution of foundational health system inputs rather than deficiencies in governance structures. Persistent rural infrastructure, supply chain, and referral gaps undermine equitable progress toward SDG 3 despite high service demand and community engagement. Recommendation: Context-specific, equity-oriented PHC reforms are required, prioritising rural infrastructure, utilities, equipment, supply chain reliability, and referral integration, alongside targeted improvements in urban system management and data use. Significant Statement: Addressing spatial inequities in PHC capacity is essential to reducing preventable morbidity and mortality, strengthening universal health coverage, and achieving SDG 3 in resource-constrained and hard-to-reach populations.
Keywords:
primary healthcare
; urban–rural disparities
; health system capacity
; service readiness
; referral systems
; universal health coverage
; sustainable development goal 3
; nigeria
; health equity
; service utilization
1. Introduction
Primary healthcare (PHC) systems are universally recognised as the foundation of resilient health systems and a critical driver for achieving Sustainable Development Goal 3 (SDG 3), which seeks to ensure healthy lives and promote well-being for all across the life course [1,2,3,4,5,6,7,8,9]. Globally, evidence demonstrates that strong PHC systems are associated with improved population health outcomes, reduced health inequalities, and enhanced system efficiency, particularly in low and middle-income countries (LMICs) [10]. However, despite global consensus on the centrality of PHC, substantial disparities persist in the availability, accessibility, and quality of services between urban and rural settings. Rural populations frequently experience shortages of skilled health personnel, inadequate infrastructure, limited-service readiness, and weak referral systems, resulting in poorer health outcomes compared with their urban counterparts [11,12,13,14,15,16,17,18,19,20,21,22,23,24]. These inequities are further compounded by demographic transitions, spatial development patterns, and resource concentration in urban centres, which systematically marginalise rural communities [25]. International experiences from both high and middle-income contexts illustrate that addressing urban-rural PHC gaps requires context-specific strategies that integrate community participation, workforce development, and health system innovation [26,27,28,29,30,31,32]. Digital health technologies, including mobile health and electronic decision-support tools, have also been shown to enhance service delivery efficiency and reach underserved populations when appropriately implemented [26,27,28,29,30,31,32]. Despite these advances, translating global PHC principles into equitable, locally responsive service delivery remains a persistent challenge, particularly in fragile health systems where governance, financing, and workforce constraints intersect. Consequently, understanding how structural and contextual factors shape PHC performance across urban and rural settings is essential for informing policies aimed at accelerating progress toward SDG 3 and Universal Health Coverage [1,2,3,4,5,6,7,8,9]. In Nigeria, the challenges confronting PHC service delivery are particularly pronounced, reflecting longstanding structural weaknesses within the health system. Nigeria operates a three-tier health system in which PHC is primarily the responsibility of local governments; however, chronic underfunding, fragmented governance, and weak accountability mechanisms have undermined effective service delivery [20,21,22,23,24,25,26,27,28]. Empirical assessments of PHC facilities across the country reveal widespread deficiencies in service readiness, including inadequate staffing, limited essential medicines, unreliable power supply, and poor infrastructure, with rural facilities disproportionately affected [33,34,35,36,37,38]. These weaknesses translate into low utilisation rates, even where facilities are geographically accessible, as communities often perceive PHC services as ineffective or unresponsive to their needs [39]. High out-of-pocket expenditures further exacerbate inequities, pushing vulnerable households into financial hardship and discouraging timely care-seeking [10]. Studies from southern Nigeria consistently demonstrate significant urban-rural differentials in maternal, child, and reproductive health service utilisation, with rural women facing compounded barriers related to transportation, education, and socio-cultural norms [11,12,13,14,15,16,17,18,19]. In the Niger Delta region, including Bayelsa State, geographic isolation, difficult terrain, and environmental degradation intensify these disparities, limiting both physical access and continuity of care. While national reforms such as the Primary Health Care Under One Roof initiative sought to address governance fragmentation, evidence suggests that implementation gaps persist, particularly in rural local government areas [40,41]. As a result, Nigeria’s PHC system remains insufficiently equipped to serve as an effective platform for achieving SDG 3, especially for populations residing outside urban centres. Beyond structural deficiencies, socio-cultural and community-level factors play a critical role in shaping PHC utilisation and outcomes. Community trust, health literacy, and perceived quality of care strongly influence service uptake, particularly for preventive and promotive services such as immunisation, antenatal care, and skilled birth attendance [42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57]. Evidence from Nigeria and comparable LMIC settings indicates that weak community engagement mechanisms contribute to underutilisation of PHC services, even where services are nominally available [44,45,46,47,48,49,50,51,52]. Collaborative care models that actively involve communities in service design and delivery have demonstrated potential to strengthen rural health workforce retention, enhance service acceptability, and improve health outcomes [58].
Similarly, digital health interventions, when aligned with local contexts, can mitigate workforce shortages and improve service continuity across dispersed rural populations [60]. However, digital divides related to infrastructure, digital literacy, and network coverage risk reinforcing existing inequities if not carefully addressed. Empirical work from China highlights that people-centred PHC reforms can reduce urban–rural inequities when equity considerations are explicitly integrated into service design and financing models [61]. In Nigeria, emerging evidence from immunisation, disease surveillance, and maternal health studies underscores the importance of community-based approaches, integrated data systems, and decentralised decision-making in strengthening PHC performance [13,23,24,54,55,56,57]. Nevertheless, systematic comparative analyses examining how these factors manifest differently across urban and rural PHC facilities remain limited, particularly at subnational levels such as Bayelsa State. Theoretical and conceptual frameworks further underscore the importance of examining PHC through an equity-oriented, systems lens. Service quality theory emphasises responsiveness, reliability, and patient-centredness as core determinants of healthcare utilisation and satisfaction, while health systems frameworks highlight the interdependence of governance, financing, workforce, service delivery, information systems, and community engagement [10,49,58]. Regular performance assessment has been identified as essential for identifying system bottlenecks and informing evidence-based reforms [40]. In rural contexts, transportation barriers, workforce maldistribution, and fiscal constraints often interact to produce cumulative disadvantage, reinforcing health inequities across the life course [62,63]. Despite recognition of these dynamics, much of the existing Nigerian literature remains either nationally aggregated or sector-specific, limiting its utility for targeted subnational policy interventions. Furthermore, while SDG 3 provides a unifying global framework, empirical studies explicitly linking PHC service delivery performance to SDG 3 outcomes at the community level remain scarce. This gap constrains the ability of policymakers to translate global commitments into locally actionable strategies, particularly in resource-constrained settings such as Bayelsa State. Against this backdrop, there remains a critical need for empirically grounded, context-specific analyses that systematically compare PHC service delivery across urban and rural settings and assess their implications for SDG 3 attainment. Bayelsa State provides a compelling case study due to its predominantly rural population, challenging geography, and persistent health inequities despite ongoing reforms. This study is timely given renewed global and national emphasis on strengthening PHC as a pathway to Universal Health Coverage and sustainable development [10]. By integrating facility-level assessment with an urban-rural comparative lens, the study seeks to advance understanding of how structural, operational, and contextual factors shape PHC performance in southern Nigeria. Specifically, the objectives of this study are: (1) to assess the level of weakness in primary healthcare service delivery in urban and rural PHC facilities in Bayelsa State; (2) to identify and compare key areas of service delivery weakness across urban and rural settings; (3) to examine the prospects of strengthening primary healthcare service delivery for advancing the achievement of Sustainable Development Goal 3 in urban and rural communities of Bayelsa State; (4) to examine facility planning, performance management, and target achievement (5) to examine barriers, facilitators, and utilisation pathways influencing access to primary healthcare services in urban and rural communities of Bayelsa State.
2. Materials and Methods
2.1. Study Setting and Context
This study was conducted in Bayelsa State, located in the Niger Delta region of southern Nigeria, a predominantly riverine and rural environment characterised by dispersed settlements, difficult terrain, and limited transport infrastructure. Bayelsa State was created in 1996 and currently has an estimated population exceeding 2.3 million people, with a substantial proportion residing in rural communities that depend almost exclusively on public primary healthcare (PHC) facilities for essential health services [25,40,62]. The state operates a three-tier health system in which PHC is administered by local government authorities under the coordination of the Bayelsa State Primary Healthcare Board, following national PHC governance frameworks [10,40]. At the time of the study, Bayelsa State had approximately 225 public PHC facilities distributed across eight Local Government Areas (LGAs) within three senatorial zones (Central, West, and East). Despite this apparent coverage, service delivery remains constrained by workforce shortages, infrastructure deficits, and weak health information systems, particularly in rural settings [3,40,63]. Evidence from Nigeria and comparable LMIC contexts indicates that such constraints disproportionately affect maternal, child, and preventive health services, undermining progress toward SDG 3 [10,11,12,13,14,15,23,24]. Bayelsa State therefore provides a critical subnational context for examining urban–rural disparities in PHC service delivery and their implications for equitable health outcomes [58,61].
2.2. Study Design
A facility-based comparative descriptive cross-sectional study design was employed to assess differences in primary healthcare service delivery between urban and rural PHC facilities in Bayelsa State. This design is well suited for health systems evaluations where the objective is to compare structural, process, and service delivery characteristics across defined settings at a single point in time [40,63]. Comparative designs are widely used in PHC research to identify inequities in service readiness, utilisation patterns, and system performance across geographic contexts [61,62]. The study was guided conceptually by the Donabedian structure–process-outcome framework, which provides a robust theoretical basis for assessing healthcare quality and performance [3,26,42]. In addition, elements of the WHO health systems performance framework informed the selection of domains related to workforce, service availability, governance, and community engagement [10,13]. This integrated approach allowed for systematic comparison of PHC service delivery strengths and weaknesses across urban and rural facilities, while situating findings within broader health system and SDG 3 performance discussions [58,61].
2.3. Study Population
The study population comprised all public primary healthcare facilities operating within Bayelsa State at the time of data collection. These facilities constitute the frontline of healthcare delivery for preventive, promotive, and basic curative services, particularly for underserved populations [40,62]. The unit of analysis was the PHC facility, with data obtained from facility records, infrastructure assessments, and healthcare workers employed within the facilities. Inclusion of facilities across diverse geographic and socio-demographic contexts enabled comprehensive assessment of service delivery variations [26,42,63]. Consistent with prior Nigerian PHC studies, focusing on public facilities allowed for standardized comparison within the same governance and financing framework [3,40]. The study also considered facility staff as key informants for operational and service delivery data, recognising their central role in PHC performance [18,23,24,58]. This population definition aligns with global PHC evaluation practices and supports generalisability of findings within similar subnational contexts [10,61].
2.4. Sampling Technique and Sample Size Determination
A stratified cluster sampling technique was employed to ensure balanced representation of PHC facilities across Bayelsa State’s three senatorial zones (Central, West, and East) and across urban and rural settings. Stratification by senatorial zone accounted for administrative, demographic, and ecological heterogeneity, while urban–rural stratification reflected known disparities in service delivery and access [25,63]. From the official master list of 225 public PHC facilities obtained from the Bayelsa State Primary Healthcare Board, facilities were first grouped by senatorial zone and then classified as urban or rural based on Federal Ministry of Health criteria, including population density, infrastructure availability, and proximity to urban centres [10,40]. Within each stratum, facilities were selected using simple random sampling with unique identification numbers to ensure transparency and minimise selection bias [13,26,42]. A total of 34 PHC facilities were sampled, comprising 17 urban and 17 rural facilities, distributed proportionately across senatorial zones. This sample size is consistent with facility-based PHC assessments conducted in Nigeria and comparable LMIC settings and provides sufficient power for comparative descriptive and inferential analyses [61,62,64].
2.5. Study Instrument and Data Collection
Data were collected using a structured health facility assessment questionnaire adapted from the WHO Service Availability and Readiness Assessment (SARA) tool, which is widely validated for evaluating PHC service delivery in LMICs [10,40]. The instrument comprised four sections: Section A captured facility demographics and operational characteristics; Section B assessed service availability, target population coverage, and utilisation patterns; Section C examined strengths and weaknesses related to access, quality, workforce, infrastructure, and referral systems; and Section D evaluated PHC contributions to SDG 3, including community engagement and sustainability of health initiatives [58,61]. Facility records were reviewed to corroborate self-reported information, enhancing data accuracy [3,18,23,24]. The instrument was pretested in non-sampled PHC facilities to ensure clarity, contextual relevance, and feasibility [13,63]. Data collection was conducted by trained researchers following standardized protocols to minimise interviewer bias and ensure consistency across facilities [10,60].
2.6. Inclusion and Exclusion Criteria
Public PHC facilities located in urban and rural communities within Bayelsa State and operational at the time of the study were included. Eligible respondents included healthcare workers employed at the selected facilities and directly involved in service delivery or facility management [40,58]. Private healthcare facilities were excluded to maintain comparability within the public PHC governance framework [3,62]. Non-functional public PHC facilities were also excluded, as they could not provide valid data on service delivery processes or utilisation patterns [26,42,63]. These criteria ensured methodological consistency and enhanced the validity of comparisons across facilities [10,61].
2.7. Data Analysis
Data were entered and analysed using IBM SPSS version 21.0. Descriptive statistics were used to summarise facility characteristics and service delivery indicators [40,64]. Binary variables were coded as “Yes” (1) and “No” (0), and composite domain scores were generated by summing affirmative responses within each assessment section [3,61]. Independent t-tests and chi-square tests were employed to compare urban and rural facilities, while Mann–Whitney U tests were used for non-parametric variables. Binary logistic regression models were constructed to identify predictors of service delivery performance and acceptability, with results interpreted within the Donabedian framework. Statistical significance was set at p < 0.05.
2.8. Validity and Reliability
Instrument validity was ensured through expert review by public health specialists and supervisors, establishing face and content validity [3,63]. Pretesting enhanced clarity and contextual appropriateness [18,23,24,40]. Reliability was supported through standardized administration procedures and internal consistency checks across domains [61,64]. These measures collectively strengthened the robustness of the study findings.
2.9. Ethical Considerations
Ethical approval was obtained from the University of Port Harcourt Postgraduate Ethical Review Committee. Administrative permissions were secured from the Bayelsa State Primary Healthcare Board and relevant local authorities. Participation was voluntary, informed consent was obtained, and confidentiality was maintained by excluding personal identifiers from data collection instruments. Ethical approval was granted by the University of Port Harcourt Postgraduate Ethical Review Committee (UP/HEC/IRB/2025/075). Administrative approval was obtained from the Bayelsa State Primary Healthcare Board to conduct the study in primary healthcare facilities, as documented in the attached approval letter. All participants provided written informed consent; participation was voluntary, and confidentiality was ensured by anonymizing data and excluding personal identifiers.
2.10. Confidentiality
3. Results
Table 1 and Figure 1 present marked urban-rural differentials in the level of weakness across multiple primary healthcare (PHC) service delivery domains in government-owned facilities in Bayelsa State. Human resource constraints were evident in both settings but were more pronounced in rural PHCs, where nearly half of the facilities (47.1%) had one or fewer trained staff for key PHC services, compared with 23.5% of urban facilities. Infrastructure and utility deficits were substantially higher in rural facilities, with over three-quarters reporting inadequate infrastructure scores (76.5%) and lack of functional water supply (76.5%), alongside a high prevalence of absent electricity supply (64.7%); none of the urban PHCs lacked electricity. Deficiencies in basic medical equipment were also concentrated in rural areas, where 70.6% of facilities lacked essential equipment, compared with 5.9% in urban facilities. Similarly, weaknesses in infection prevention and control (58.8% vs. 23.5%) and waste management systems (52.9% vs. 5.9%) were considerably more common in rural PHCs. In contrast, weaknesses in health information systems followed a different pattern, with incomplete monthly NHMIS reporting observed exclusively among urban facilities (29.4%), while no rural facility reported this indicator. Composite service readiness measures showed low readiness for basic amenities, essential medicines, and diagnostic capacity in a minority of facilities overall, but these weaknesses remained more frequent in rural PHCs (17.6%) than in urban PHCs (5.9%). The key takeaway from Table 1 and Figure 1 is the clear concentration of structural and operational weaknesses in rural PHC facilities relative to their urban counterparts, highlighting a pronounced spatial inequity in frontline health system capacity within Bayelsa State. These disparities are central to the study’s objective of assessing urban-rural differences in primary healthcare delivery and directly underscore barriers to achieving Sustainable Development Goal 3, particularly targets related to universal health coverage, quality essential services, and health system strengthening. In real-world terms, the observed rural deficits in infrastructure, utilities, equipment, and infection control have direct implications for service availability, quality of care, and patient safety, potentially reinforcing avoidable morbidity and mortality in underserved communities. Conversely, the identification of urban-specific weaknesses in health information reporting points to the need for context-sensitive interventions rather than uniform policy responses. Collectively, these findings provide empirical evidence to inform targeted resource allocation, rural health system investments, and equity-oriented PHC reforms aimed at closing urban-rural gaps in healthcare delivery in southern Nigeria.
Table 2 and Figure 2 compare key service delivery weaknesses between rural and urban primary healthcare (PHC) facilities in Bayelsa State and highlight statistically significant urban-rural differences across several service domains. No rural facilities reported the absence of maternal and child health services or outpatient care, whereas one urban facility (5.9%) reported weaknesses in each of these core clinical services; however, these differences were not statistically significant (p = 0.310). Preventive services related to disease surveillance and control were more frequently weak in rural PHCs (29.4%) than in urban PHCs (5.9%), approaching but not reaching statistical significance (p = 0.072). Diagnostic capacity weaknesses, measured by the absence of laboratory services, were observed in both settings, affecting 35.3% of rural and 52.9% of urban facilities, with no significant urban-rural difference (p = 0.300). In contrast, essential drug availability showed a significant disparity, with weaknesses more prevalent in urban PHCs (76.5%) compared with rural PHCs (35.3%) (χ² = 5.846, p = 0.016). Marked and highly significant disparities were observed in infrastructure, equipment readiness, infection control, and health information systems. Rural PHCs were substantially more likely to lack electricity (64.7% vs. 0.0%) and functional water supply (76.5% vs. 11.8%), with both differences highly significant (p < 0.001). Similarly, deficiencies in basic medical equipment were overwhelmingly concentrated in rural facilities (70.6% vs. 5.9%; p < 0.001), as were weaknesses in waste disposal systems (52.9% vs. 5.9%; p = 0.003). Conversely, weaknesses in monthly health data reporting were observed exclusively in urban PHCs (29.4%), representing a statistically significant difference relative to rural facilities (p = 0.015). Overall, the findings from Table 2 and Figure 2 reinforce the study’s central conclusion that rural PHCs in Bayelsa State face disproportionately greater structural and operational constraints, particularly in utilities, equipment, and infection control, which are foundational to safe and effective service delivery. These statistically robust disparities underscore critical barriers to equitable progress toward Sustainable Development Goal 3, highlighting the need for differentiated, context-specific health system strengthening strategies that address both rural infrastructure deficits and urban system management challenges.
Table 3 and Figure 3 present indicators of existing capacity and prospects for strengthening primary healthcare (PHC) service delivery relevant to the advancement of Sustainable Development Goal 3 (SDG 3) across urban and rural communities in Bayelsa State. Human resource capacity was relatively comparable between settings, with at least one trained staff member available for key PHC services in 82.4% of rural and 76.5% of urban facilities, showing no statistically significant difference (p = 0.691). Marked urban–rural disparities were observed in infrastructure and essential utilities, with adequate infrastructure scores reported by only 23.5% of rural PHCs compared with 70.6% of urban facilities (p = 0.017). Availability of electricity and water supply was substantially higher in urban PHCs (100.0% and 88.2%, respectively) than in rural PHCs (35.3% and 23.5%), with both differences highly significant (p < 0.001). Equipment readiness followed a similar pattern, as basic medical equipment was available in 94.1% of urban facilities but only 29.4% of rural facilities (p < 0.001). Urban PHCs also demonstrated stronger infection prevention and control practices (76.5% vs. 41.2%; p = 0.037) and more functional waste management systems (94.1% vs. 47.1%; p = 0.003). In contrast, rural facilities showed higher proportions of moderate-to-high patient attendance (100.0% vs. 76.5%) and routine monthly data reporting (100.0% vs. 70.6%), with the latter difference reaching statistical significance (p = 0.015). No statistically significant urban–rural differences were observed in the conduct of performance review meetings (p = 0.203). The key takeaway from Table 3 and Figure 3 is that while both urban and rural PHCs demonstrate important foundational capacities for advancing SDG 3, the nature of these strengths differs substantially by setting. Urban facilities exhibit significantly greater readiness in infrastructure, utilities, equipment, and infection control, core inputs for delivering safe and high-quality health services, whereas rural PHCs display comparatively stronger service utilisation and health information reporting capacities. This divergence is highly significant to the overall study, as it suggests that urban–rural disparities in PHC delivery are not solely defined by deficits but also by unevenly distributed strengths that can be strategically leveraged. In practical terms, the findings indicate that accelerating progress toward SDG 3 in Bayelsa State will require differentiated system-strengthening approaches: targeted investments in rural infrastructure, utilities, and equipment to address critical bottlenecks, alongside efforts to sustain and optimise urban service management while reinforcing data use and community engagement. By identifying context-specific opportunities for strengthening PHC systems, these results provide actionable evidence for policymakers and health system managers seeking to implement equity-oriented and efficiency-driven reforms in southern Nigeria.
Table 4 and Figure 4 summarises key indicators of facility planning, performance management, and target achievement across rural and urban primary healthcare (PHC) facilities in Bayelsa State. The availability of annual work plans was uniformly high in both rural and urban settings, with 94.1% of facilities in each group reporting the presence of a documented plan (p = 1.000). Similarly, nearly all facilities demonstrated population accountability through the definition of a catchment population, reported by all rural PHCs (100.0%) and the majority of urban PHCs (94.1%), with no statistically significant difference between locations (p = 0.310). Target-setting practices were also widely adopted, as 94.1% of rural and 88.2% of urban facilities reported setting monthly or quarterly service targets (p = 0.545). In contrast, differences emerged in performance achievement, with a higher proportion of urban PHCs achieving at least 75% of their planned service targets (88.2%) compared with rural PHCs (58.8%), approaching statistical significance (χ² = 3.778, p = 0.052). Routine performance review meetings were more frequently conducted in urban facilities (88.2%) than in rural facilities (70.6%), although this difference was not statistically significant (p = 0.203). The key takeaway from Table 4 and Figure 4 is that foundational governance and planning structures are largely in place across both urban and rural PHCs in Bayelsa State, but there is a notable divergence in the translation of plans into achieved service outputs. This finding is significant to the overall study, as it suggests that urban-rural disparities in PHC performance are not primarily driven by the absence of planning or target-setting mechanisms, but rather by differences in operational capacity and execution. In real-world terms, the lower rate of target achievement observed in rural facilities, despite comparable planning frameworks, points to underlying structural constraints, such as infrastructure deficits, limited utilities, and equipment shortages identified elsewhere in the study, that may hinder effective service delivery. These results underscore the importance of complementing governance and performance management reforms with sustained investments in rural health system inputs to ensure that planning translates into measurable progress toward SDG 3 at the community level.
Table 5 and Figure 5 presents a comparative analysis of barriers, facilitators, and utilisation pathway indicators influencing access to primary healthcare (PHC) services across rural and urban communities in Bayelsa State. Shortages of qualified healthcare staff were widely reported in both settings, affecting 76.5% of rural and 52.9% of urban respondents, although this difference was not statistically significant (p = 0.151). Infrastructure-related barriers, including deficits in water, electricity, and physical space, were more frequently reported in rural communities (41.2%) than in urban communities (17.6%), but the difference did not reach statistical significance (p = 0.132). Delayed or avoided care-seeking was reported more often in urban settings (23.5%) than rural settings (5.9%), though this variation was also not statistically significant (p = 0.146). In contrast, supply chain constraints showed pronounced and statistically significant disparities, with frequent essential medicine stock-outs reported by 64.7% of rural communities compared with 11.8% of urban communities (χ² = 10.088, p = 0.001). Service access mechanisms differed markedly by location, as reliance on outreach services for care was substantially higher in rural areas (70.6%) than in urban areas (17.6%), with this difference reaching statistical significance (p = 0.018). Similarly, referral pathway weaknesses were significantly more prevalent in rural communities, where non-functional referral systems (58.8% vs. 11.8%; p = 0.004) and absence of patient referrals in the preceding month (76.5% vs. 11.8%; p < 0.001) were commonly reported. The key takeaway from Table 5 and Figure 5 is that rural communities in Bayelsa State experience significantly greater constraints along the primary healthcare utilisation pathway, particularly in relation to medicine availability, service continuity, and referral linkages, despite comparable levels of community engagement and access to service information across settings. This finding is central to the overall study, as it highlights that urban–rural disparities in PHC access extend beyond facility readiness to encompass systemic bottlenecks that shape how individuals navigate and utilise services. In practical terms, the heavy reliance on outreach services and the high prevalence of non-functional referral pathways in rural areas underscore vulnerabilities in service integration and continuity of care, with potential consequences for timely diagnosis, treatment, and follow-up, key components of SDG 3. These results point to the need for health system interventions that strengthen rural supply chains, formalise referral networks, and reduce dependence on episodic outreach, thereby improving equitable access to comprehensive and continuous primary healthcare services in southern Nigeria.
4. Discussion
4.1. Urban-Rural Inequities in Primary Healthcare Readiness
The marked concentration of human resource, infrastructure, utilities, equipment, infection prevention, and waste management weaknesses in rural PHC facilities observed in this study is consistent with a substantial body of evidence from Nigeria and comparable low and middle-income country settings. Human resource constraints, particularly the limited availability of trained personnel in rural facilities, align with earlier findings from Bayelsa State and other parts of Nigeria, which document persistent maldistribution of the health workforce favouring urban centres [40,66,67]. Agarwal et al. [68] similarly emphasised that staffing presence alone does not equate to functional workforce capacity, particularly where skill mix and supervision are inadequate. The pronounced rural deficits in infrastructure, electricity, and water supply corroborate national and subnational assessments showing that basic amenities remain a critical bottleneck to PHC readiness in rural Nigeria [69,70,71,72,73,74,75,76]. Comparable patterns have also been reported in rural health systems globally, where infrastructure gaps directly undermine service quality and safety [37,38,62,77]. The high prevalence of inadequate infection prevention, waste management, and lack of essential equipment in rural facilities further mirrors findings from studies linking poor WaSH conditions to elevated infection risks and reduced service utilisation [37,38,72,73,74,75,76], reinforcing the structural nature of rural PHC vulnerability. Conversely, the finding that weaknesses in routine health information system reporting were observed exclusively among urban facilities introduces an important nuance that both supports and extends existing literature. While rural facilities are often portrayed as weaker across all system dimensions, several studies have documented that smaller, less complex rural facilities may demonstrate stronger compliance with routine reporting due to lower service volume and simpler administrative structures [60,78,79]. This pattern aligns with evidence from Nigeria showing that urban PHCs, despite better infrastructure, often face challenges related to data completeness, workload pressures, and fragmented accountability mechanisms [13,51,80]. Similar urban-rural contrasts in health information performance have been reported in China and Europe, where urban complexity rather than resource scarcity undermines reporting efficiency [61,81]. Importantly, the composite service readiness findings, showing that rural facilities consistently lag behind urban facilities even when weaknesses appear numerically modest, echo broader global health systems analyses that emphasise cumulative disadvantage rather than isolated deficits [77,82]. Taken together, these converging lines of evidence suggest that the urban-rural disparities observed in Bayelsa State are neither anomalous nor transient but reflect entrenched structural inequities that continue to shape PHC performance across diverse contexts [11,12,13,14,15,58,83].
4.2. Infrastructure, Medicines, and Infection Control as System Constraints
The observed lack of statistically significant urban-rural differences in the availability of core clinical services, such as maternal and child health services and outpatient care, suggests that basic service presence has been largely achieved across PHC facilities in Bayelsa State. This finding aligns with national policy aspirations articulated in Nigeria’s National Strategic Health Development Plan II and NPHCDA minimum standards, which emphasise universal availability of essential PHC services regardless of location [69,84]. Similar patterns have been reported in other Nigerian and sub-Saharan African studies, where service availability masks deeper challenges related to service quality and functional capacity [40,71,80]. The near-significant rural disadvantage in disease surveillance and control is consistent with evidence highlighting weak integration of surveillance functions within rural PHCs, often due to limited training, supervision, and digital infrastructure [13,14,18,19,20,21,22,23,24]. Furthermore, the lack of significant difference in laboratory service availability across settings reflects broader systemic constraints in PHC diagnostic capacity in Nigeria, where laboratory services remain underdeveloped even in urban facilities [3,61,82]. Collectively, these findings reinforce the notion that nominal service coverage does not equate to effective service delivery, echoing global health system critiques that emphasise functionality over mere presence [77,83]. In contrast, the statistically significant disparities observed in utilities, equipment readiness, infection control, waste management, and essential drug availability underscore the structural roots of urban–rural inequities in PHC performance. The concentration of electricity and water supply deficits in rural facilities mirrors extensive Nigerian and global literature identifying basic utilities as persistent barriers to safe healthcare delivery in rural settings [37,38,62,70,71,72,73,74,75,76]. The severe lack of basic medical equipment and functional waste disposal systems in rural PHCs corroborates findings from earlier assessments in the Niger Delta and other LMIC contexts, which link inadequate equipment and poor IPC practices to increased occupational and patient safety risks [46,53,58]. Conversely, the higher prevalence of essential drug stock-outs and incomplete routine data reporting in urban facilities challenges conventional assumptions that urban PHCs are uniformly better resourced, aligning with studies that document urban supply chain inefficiencies, higher service volumes, and administrative overload [60,78,79,80]. Similar urban-specific system management challenges have been reported in China and European settings, where complexity rather than scarcity constrains performance [61,81]. Together, these findings reinforce calls in the literature for differentiated, context-sensitive PHC strengthening strategies that address rural infrastructure deficits while simultaneously improving urban system management to advance equitable progress toward Sustainable Development Goal 3 [1,4,77].
4.3. Contrasting Capacity and Utilisation Patterns Across Settings
The relatively comparable human resource capacity observed across rural and urban PHC facilities, as reflected by the availability of at least one trained staff member for key services, suggests that workforce presence alone may not be the primary limiting factor to PHC strengthening in Bayelsa State. This finding aligns with growing evidence from Nigeria and other LMICs indicating that the mere availability of health workers does not guarantee functional service delivery, particularly in contexts characterised by inadequate infrastructure, limited supervision, and constrained working conditions [40,67,68]. Similar observations have been reported in sub-Saharan Africa, where health worker productivity and retention are strongly mediated by enabling environments rather than absolute staffing levels [62,66,77]. The pronounced urban advantage in infrastructure readiness, electricity, water supply, and equipment availability corroborates national facility assessments and WHO service readiness studies that consistently identify these domains as critical prerequisites for effective PHC and progress toward SDG 3 [69,71,83,84]. Evidence from the Niger Delta and other fragile geographies further highlights how infrastructural deficits disproportionately constrain rural PHCs, limiting their capacity to deliver safe maternal, child, and infectious disease services [37,38,53,70]. Collectively, these findings underscore that prospects for PHC strengthening in rural Bayelsa are structurally bounded by deficits in foundational system inputs rather than workforce availability per se. Conversely, the higher levels of patient attendance and routine monthly data reporting observed in rural facilities reveal latent system strengths that are often overlooked in dominant deficit-oriented narratives of rural health systems. High rural service utilisation aligns with evidence suggesting that PHCs in underserved communities remain the primary and often only, point of care, resulting in sustained demand despite infrastructural limitations [1,4,11,12,13,14,15,58]. Stronger routine data reporting in rural facilities also supports findings from health systems research indicating that smaller facility size and simpler administrative structures may enhance compliance with reporting requirements [60,78,79]. In contrast, urban facilities, while better equipped, often face challenges related to higher patient volumes, fragmented accountability, and administrative overload, which can undermine data quality and utilisation [61,80,81]. The absence of significant urban–rural differences in governance indicators such as performance review meetings further suggests that managerial processes are not inherently weaker in rural settings, echoing broader evidence that governance capacity can exist independently of material resources [77,82]. Taken together, these findings indicate that advancing SDG 3 in Bayelsa State requires dual strategies that simultaneously address rural infrastructural inequities while leveraging existing rural strengths in service utilisation and data reporting to build resilient, people-centred PHC systems [11,12,13,14,15,67,83].
4.4. From Planning to Performance: Gaps in PHC Accountability
The uniformly high levels of facility planning, population accountability, and target-setting practices observed across both rural and urban PHC facilities indicate that foundational governance structures are largely in place throughout Bayelsa State. This finding aligns with national PHC reforms in Nigeria, particularly the “PHC Under One Roof” initiative, which emphasises standardised planning frameworks, defined catchment populations, and routine target setting across all facilities irrespective of location [69,84]. Similar patterns have been documented in other Nigerian states and sub-Saharan African contexts, where formal governance instruments are widely adopted even in resource-constrained rural settings [40,80,82]. The presence of annual work plans and clearly defined service populations further reflects alignment with WHO health system building blocks, particularly governance and accountability, which are considered prerequisites for effective PHC and SDG 3 implementation [67,83,85]. Evidence from LMICs also suggests that such governance artefacts often diffuse more rapidly than material resources, creating a scenario in which “policy readiness” outpaces “operational readiness” [58,71,77]. The absence of statistically significant urban–rural differences in these indicators therefore underscores the success of top-down governance harmonisation efforts, while simultaneously raising questions about their translation into measurable performance outcomes. Despite comparable planning and target-setting structures, the higher proportion of urban PHCs achieving at least 75% of planned service targets highlights an emerging performance gap that favours urban facilities. This finding is consistent with health systems research demonstrating that performance achievement is strongly conditioned by infrastructural adequacy, staffing mix, and service readiness rather than planning processes alone [62,68,77]. Studies from Nigeria and comparable LMICs have shown that rural facilities often struggle to meet service targets due to constraints such as unreliable utilities, limited equipment, and disrupted supply chains, factors that were prominently identified in earlier tables of this study [37,38,53,70,71,72,73,74,75,76]. The more frequent conduct of performance review meetings in urban facilities, although not statistically significant, aligns with evidence suggesting that urban settings benefit from closer managerial oversight, easier access to supervisory structures, and stronger feedback loops [60,78,80]. Conversely, rural facilities may experience performance review as a procedural requirement rather than a continuous improvement mechanism, particularly where actionable resources are lacking [79,82]. Taken together, these findings reinforce the argument that governance parity does not automatically translate into performance equity and that closing the urban-rural performance gap will require aligning planning and accountability mechanisms with sustained investments in service readiness and operational capacity to advance equitable progress toward SDG 3 [67,77,83].
4.5. Supply Chains and Referral Pathways as Barriers to Access
The widespread reporting of healthcare workforce shortages across both rural and urban communities underscores a systemic human resource challenge that transcends spatial location, consistent with national and regional assessments of PHC service readiness in Nigeria [3,40,62]. Similar findings have been reported across sub-Saharan Africa, where staffing gaps persist even in urban settings due to maldistribution, attrition, and limited incentives for frontline service delivery [61,67,68]. The higher prevalence of infrastructure-related barriers in rural communities aligns strongly with earlier Nigerian and Niger Delta-focused studies documenting chronic deficits in water, electricity, and facility space as key deterrents to service utilisation [37,38,53,70,73,74,75,76]. However, the lack of statistically significant differences in delayed or avoided care-seeking, despite poorer rural infrastructure, reflects a nuanced utilisation dynamic previously observed in Bayelsa and Rivers States, where geographic isolation and limited alternatives compel rural populations to rely on PHCs regardless of service quality [11,12,13,14,15,17,63]. Conversely, the relatively higher reporting of delayed care-seeking in urban settings is consistent with studies linking urban congestion, indirect costs, and perceived quality differentials to deferred utilisation [25,39,61], highlighting that access barriers in urban contexts may be more behavioural and system-complexity driven rather than purely infrastructural [60,78]. In contrast, the statistically significant rural disadvantage in supply chain reliability, outreach dependence, and referral system functionality represents a critical access bottleneck with direct implications for continuity of care and SDG 3 attainment. The high prevalence of essential medicine stock-outs in rural communities corroborates extensive Nigerian evidence linking weak last-mile distribution, cold-chain disruptions, and limited logistics oversight to poor medicine availability in hard-to-reach settings [3,22,40,45,48]. Similar rural-skewed supply chain vulnerabilities have been documented across immunisation, maternal health, and infectious disease control programmes in Nigeria and East Africa [45,54,55,56,57,59]. The heavy reliance on outreach services among rural communities strongly aligns with evidence from Bayelsa State demonstrating the effectiveness, but also the fragility of outreach-dependent service delivery models in contexts of poor facility readiness [11,12,13,14,15,23,24,45]. While outreach strategies have been shown to improve coverage for vaccination and maternal services, multiple studies caution that they are not substitutes for functional facility-based care, particularly where referral systems are weak or non-existent [4,60,61]. The high proportion of rural facilities reporting non-functional referral pathways and absence of referrals mirrors findings from disease surveillance and outbreak response studies in Nigeria, which identify referral breakdowns as a major contributor to preventable morbidity and delayed emergency care [13,14,28,46]. Collectively, these findings reinforce global calls for integrated, people-centred PHC systems that strengthen supply chains, referral networks, and digital coordination to ensure equitable access across the urban–rural continuum [10,60,61,77].
5. Implications for Policy and Interventions
The findings demonstrate that urban-rural disparities in primary healthcare (PHC) service delivery in Bayelsa State are driven primarily by unequal distribution of foundational system inputs rather than by the absence of governance structures or community engagement mechanisms. Rural PHC facilities consistently exhibited severe deficits in infrastructure, essential utilities, basic medical equipment, infection prevention and control, supply chain reliability, and referral system functionality, despite demonstrating comparable levels of service planning, community accountability, and in some domains, stronger service utilisation and health information reporting. These patterns indicate that existing policy frameworks and planning instruments are insufficient to overcome structural constraints that limit effective service delivery in rural settings. Policy responses should therefore prioritise input-intensive system strengthening in rural PHCs, focusing on reliable electricity and water supply, facility rehabilitation, equipment provision, and functional waste management systems as prerequisites for quality and safety of care. Targeted human resource policies are also required to translate staffing presence into service capacity. Although the availability of at least one trained staff member was relatively high across both settings, rural facilities were disproportionately affected by limited staffing depth and a skewed skill mix, which constrained service continuity and performance achievement. Policies that incentivise rural deployment, retention, and continuous professional development, combined with task-shifting where appropriate, are essential to improve operational efficiency in underserved areas. In parallel, the persistence of essential medicine stock-outs and non-functional referral pathways in rural communities points to systemic weaknesses beyond the facility level, necessitating supply chain reforms, strengthened logistics management, and integrated referral networks linking PHCs with higher-level facilities. Urban-specific interventions should focus on improving health information system performance and medicine availability, ensuring that relatively stronger infrastructure is matched by effective system management. Collectively, the evidence supports the need for context-differentiated, equity-oriented PHC policies to accelerate progress toward Sustainable Development Goal 3, rather than uniform interventions that risk reinforcing existing spatial inequalities.
6. Summary of the Findings
This study provides comprehensive empirical evidence of pronounced urban-rural disparities in primary healthcare service delivery across government-owned PHC facilities in Bayelsa State, southern Nigeria. Rural facilities were disproportionately affected by structural weaknesses, including inadequate infrastructure, unreliable electricity and water supply, lack of basic medical equipment, suboptimal infection prevention and waste management practices, frequent essential medicine stock-outs, and poorly functioning referral systems. These deficits were statistically significant across multiple service delivery and utilisation pathway domains and were strongly aligned with lower levels of service readiness and performance achievement. In contrast, urban PHCs demonstrated relatively stronger infrastructure and equipment readiness but exhibited notable weaknesses in essential drug availability and routine health information reporting. Despite these disparities, governance and planning mechanisms such as annual work plans, target setting, defined catchment populations, and community engagement were widely present across both rural and urban settings, indicating that performance gaps are less attributable to the absence of managerial frameworks than to differential access to critical system inputs. Importantly, rural PHCs showed high levels of patient utilisation and stronger routine data reporting, underscoring both unmet demand and latent system potential. Taken together, the findings reveal a health system characterised by uneven capacity rather than uniform dysfunction, with rural communities bearing a disproportionate burden of service delivery constraints. Addressing these inequities is essential for achieving universal health coverage and advancing SDG 3 in southern Nigeria, and will require strategic, location-specific investments that strengthen the foundations of primary healthcare where needs are greatest.
7. Conclusion
This study demonstrates that urban-rural disparities in primary healthcare (PHC) service delivery in Bayelsa State are primarily rooted in unequal distribution of essential system inputs rather than differences in governance structures or service planning frameworks. Rural PHC facilities were consistently disadvantaged across multiple domains, including infrastructure, utilities, equipment availability, infection prevention and control, medicine supply, and referral functionality, all of which are foundational to the delivery of safe, effective, and continuous care. These structural weaknesses persisted despite comparable levels of facility planning, community engagement, and, in some cases, stronger service utilisation and health information reporting in rural settings. In contrast, urban PHCs benefited from greater infrastructure and equipment readiness but exhibited notable gaps in essential drug availability and routine data reporting, underscoring the multidimensional nature of service delivery challenges across settings. Collectively, the findings indicate that progress toward Sustainable Development Goal 3 in southern Nigeria is constrained less by the absence of policy intent or management structures than by persistent spatial inequities in health system capacity. Without targeted investments to address rural deficits in basic amenities, equipment, supply chains, and referral networks, existing planning and performance management mechanisms are unlikely to translate into equitable health outcomes. By quantifying these disparities across service delivery, utilisation pathways, and governance domains, this study provides robust evidence to support context-sensitive primary healthcare strengthening strategies aimed at closing urban–rural gaps and advancing universal health coverage in resource-constrained settings.
8. Study Limitations
Several limitations should be considered when interpreting the findings of this study. First, the cross-sectional design captures service delivery conditions at a single point in time and does not account for seasonal or temporal variations in infrastructure availability, medicine supply, or service utilisation, which may influence observed urban–rural differences. Second, the analysis was limited to government-owned primary healthcare facilities in Bayelsa State, and the findings may not be generalisable to private facilities, faith-based providers, or other states in Nigeria with different health system contexts or levels of resource allocation. The relatively small sample size of facilities, while appropriate for the study setting, may also have reduced statistical power for detecting differences in some indicators that approached but did not reach conventional levels of significance. Third, several indicators relied on facility-level reporting and administrative records, which may be subject to reporting bias or inconsistencies, particularly in domains such as health information systems and performance achievement. Although efforts were made to use objective measures and standardised tools, the possibility of misclassification cannot be fully excluded. Finally, the study focused on service readiness, access pathways, and governance indicators, and did not directly assess health outcomes or patient-level experiences, limiting the ability to draw causal inferences between observed service delivery weaknesses and population health outcomes. Future research incorporating longitudinal designs, larger geographic coverage, and mixed-methods approaches would be valuable for deepening understanding of how urban-rural PHC disparities translate into differential health outcomes and for evaluating the impact of targeted system-strengthening interventions.
9. Recommendations
9.1. Short-Term Actions (0-12 Months)
Address Critical Service Delivery Bottlenecks
Immediate interventions should prioritise restoring basic functionality in rural primary healthcare (PHC) facilities where service delivery is most constrained. Emergency investments are required to ensure an uninterrupted electricity and water supply through interim solutions such as solar power systems, boreholes, and water storage facilities, particularly in rural PHCs where utility deficits were pervasive. Rapid provision of essential basic medical equipment, infection prevention materials, and waste disposal tools should be implemented using standardised equipment kits to address critical safety and quality gaps. In parallel, urgent measures to stabilise essential medicine availability such as buffer stock deployment, emergency procurement, and redistribution of medicines from overstocked urban facilities, are necessary to mitigate frequent rural stock-outs. Short-term administrative actions should also include reactivation of referral linkages through clear referral protocols and designated focal persons to address the high prevalence of non-functional referral systems in rural communities.
9.2. Mid-Term Actions (1-3 Years)
Strengthen System Capacity and Operational Efficiency
Over the medium term, policy efforts should focus on consolidating gains through sustainable system strengthening. Infrastructure rehabilitation and expansion should be prioritised for rural PHCs, guided by minimum service readiness standards and equity-based resource allocation frameworks. Human resource strategies should move beyond staff presence to improving staffing depth, skill mix, and retention through rural posting incentives, continuous professional development, and task-shifting policies where appropriate. Supply chain reforms are essential, including strengthening last-mile distribution systems, improving logistics management information systems, and integrating PHCs more effectively into state-level procurement and distribution platforms. Additionally, formalisation and digitisation of referral networks linking PHCs with secondary facilities should be pursued to improve continuity of care. In urban PHCs, targeted interventions should focus on improving essential drug availability and strengthening routine health information reporting to address observed management and system performance gaps.
9.3. Long-Term Actions (3-10 Years)
Institutionalise Equity-Oriented Primary Healthcare Reform
Long-term strategies should aim to institutionalise resilient, equitable primary healthcare systems aligned with Sustainable Development Goal 3. This includes embedding rural infrastructure financing within state and national health budgets, expanding renewable energy solutions for PHCs, and integrating PHC facility upgrading into broader rural development policies. Workforce planning should be aligned with population health needs through data-driven deployment, career progression pathways for rural health workers, and strengthened pre-service training linked to community-based practice. Health information systems should be fully integrated and interoperable, enabling real-time monitoring of service readiness, utilisation, and performance across urban and rural settings. Finally, governance reforms should emphasise accountability for equity outcomes, with routine performance monitoring explicitly disaggregated by location and linked to corrective financing and management actions. These long-term investments are critical for translating planning frameworks into sustained service delivery improvements and for ensuring that progress toward universal health coverage and SDG 3 is inclusive and spatially equitable in southern Nigeria.
10. Health Significance
The findings of this study have substantial health significance, as they reveal systemic urban-rural inequities in primary healthcare (PHC) service delivery that directly influence access to essential health services, quality of care, and continuity across communities in Bayelsa State. The concentration of infrastructure deficits, unreliable electricity and water supply, inadequate equipment, weak infection prevention practices, and frequent essential medicine stock-outs in rural PHCs represents a critical threat to safe and effective healthcare delivery. These foundational gaps compromise the management of common conditions, increase the risk of healthcare-associated infections, and limit the capacity of frontline facilities to deliver timely maternal, child, and preventive services, key determinants of morbidity and mortality in low-resource settings. Beyond service readiness, the study demonstrates that rural populations face constrained care pathways, characterised by heavy reliance on outreach services and non-functional referral systems, which undermine early diagnosis, treatment escalation, and follow-up care. These utilisation barriers heighten the risk of delayed care, disease progression, and avoidable complications, particularly for vulnerable populations such as pregnant women, children, and individuals with chronic conditions. At the same time, the high levels of service utilisation and community engagement observed in rural settings indicate substantial unmet health needs and latent demand for care, suggesting that strengthening PHC capacity could yield immediate population health gains. Collectively, the evidence underscores that achieving Sustainable Development Goal 3, particularly universal health coverage and equitable access to quality essential services, depends not only on expanding service availability but also on rectifying spatial inequities in health system capacity that disproportionately affect rural communities. Addressing these gaps is therefore central to reducing preventable illness and death and to improving health equity in southern Nigeria. Thus, graphically it is represented (Figure 6 below) as:
Author Contributions
Macaulay Tinimoye, Morufu Olalekan Raimi and Anyandi Daberechi contributed equally to this work. All authors conceptualized the study, curated data on urban-rural primary healthcare disparities in southern Nigeria, conducted the formal analysis, wrote the original draft, reviewed and edited subsequent versions, and approved the final manuscript. All authors had full access to all data and accept responsibility for submission.
Competing Interests
The authors declare no competing interests.
Dual-Use Research of Concern
This study did not involve dual-use research in the life sciences.
Acknowledgments
We thank the anonymous reviewers for their constructive feedback, which improved the manuscript.
References
- Oweibia M, Elemuwa UG, Akpan E et al (2024). Analyzing Nigeria’s Journey Towards Sustainable Development Goals: A Comprehensive Review From Inception To Present [version 1; peer review: awaiting peer review]. F1000Research 2024, 13:984. [CrossRef]
- Raimi MO, Ihuoma BA, Esther OU, Abdulraheem AF, Opufou T, Deinkuro NS, Adebayo PA and Adeniji AO (2020) “Health Impact Assessment: Expanding Public Policy Tools for Promoting Sustainable Development Goals (SDGs) in Nigeria”. EC Emergency Medicine and Critical Care 4.9 (2020).
- Christopher OE, Muyi A, Teddy CA, Rotifa SU, Oyeyemi AS, Uchenna GE, Ansa H, Oyindiepreye LA, Akinloye BO, Morufu OR (2024) Transforming Primary Healthcare in Nigeria: Enhancing Universal Health Coverage through Strong and Sustainable Primary Healthcare Laboratories. Qeios. [CrossRef]
- Mordecai O, Uchenna GE, Emma A, Elemuwa TD; Gabriel JO; Egberipou T; Etim EO; Christopher OE; Morufu OR; Anuoluwapo B (2024). Analyzing Nigeria’s Journey Towards Sustainable Development Goals: A Comprehensive Review From Inception to Present. Qeios. [CrossRef]
- Olalekan RM, Oluwatoyin OA, Olawale SH, Emmanuel OO, Olalekan AZ (2020) A Critical Review of Health Impact Assessment: Towards Strengthening the Knowledge of Decision Makers Understand Sustainable Development Goals in the Twenty-First Century: Necessity Today; Essentiality Tomorrow. Research and Advances: Environmental Sciences. 2020(1): 72-84. https://ospopac.com/journal/environmental-sciences/early-online. [CrossRef]
- Raimi MO, Odubo TR, Ogah A (2022) Women, Water and Development in the Global South. Oral Presentation Presented at the Multidisciplinary International Conference on Water in Africa (ICWA 2022) on the theme: Towards Successful Delivery of SDGs 3 & 6, which held February 09 – 11, 2022.
- Olalekan RM, Oluwatoyin O and Olalekan A (2020) Health Impact Assessment: A tool to Advance the Knowledge of Policy Makers Understand Sustainable Development Goals: A Review. ES Journal of Public Health; 1(1); 1002. https://escientificlibrary.com/public-health/in-press.php.
- Adedoyin OO, Olalekan RM, Olawale SH, et al (2020). A review of environmental, social and health impact assessment (Eshia) practice in Nigeria: a panacea for sustainable development and decision making. MOJ Public Health. 2020;9(3):81–87. https://medcraveonline.com/MOJPH/MOJPH-09-00328.pdf. [CrossRef]
- Raimi MO, Odubo TR, Odubo TV, Omidiji AO (2022) Gender and Sustainability in the Niger Delta. Oral Presentation Presented at the Multidisciplinary International Conference on Water in Africa (ICWA 2022) on the theme: Towards Successful Delivery of SDGs 3 & 6, which held February 09 – 11, 2022.
- World Health Organization (2023) Global Health Expenditure data base, retrieved April 7, 2023. (apps.who.int/nha/database). https://data.worldbank.org/indicator.
- Abdulraheem AF, Ononokpono DN, Raimi MO (2025a) Breaking Barriers: How Socio-Demographic, Cultural, and Geographic Factors Shape Skilled Birth Attendance in Nigeria – A Call for Equity and Empowerment. JMIR Preprints. 25/05/2025:78050.
- Abdulraheem AF, Raimi MO, Ononokpono DN (2025b) Who Delivers Safely? The Hidden Role of Transport and Education in Nigeria’s Maternal Health Crisis. JMIR Preprints. 21/06/2025:79460. [CrossRef]
- Oginifolunnia OC, Elemuwa CO, Adias TC, Raimi MO, Angalabiri C (2025) Bridging the Gaps: Unveiling Weaknesses in Disease Surveillance During Mass Immunization Campaigns in Nigeria JMIR Preprints. 04/07/2025:80148. [CrossRef]
- Abaya ST, Ogoina D, Stow J, Abaye BB, Emeka C, Raimi MO (2024) Beyond the Epidemic: Effective Public Health Strategies in Response to Nigeria’s First Lassa Fever Outbreak in a Non-Endemic Region. JMIR Preprints. 19/08/2024:65539. [CrossRef]
- Abdulraheem AF, Ononokpono DN, Raimi MO (2025c). Breaking barriers to safe motherhood: how social, cultural, and geographic inequalities shape skilled birth attendance in Nigeria. Sociol Int J.;9(5):188–200. [CrossRef]
- Morufu OR, Ebikapaye O, Tuebi M, Aziba-anyam GR, Adedoyin OO, Aishat FA, Mariam OR, Beatrice OJ (2021) Do Weak Institutions Prolong Crises? [#ENDSARs] in the Light of the Challenges and opportunities beyond COVID-19 Pandemic and the Next Normal in Nigeria. Communication, Society and Media. ISSN 2576-5388 (Print) ISSN 2576-5396 (Online) Vol. 4, No. 2, http://www.scholink.org/ojs/index.php/csm/article/view/3790. [CrossRef]
- Tuebi M; Franco, A; Raimi, MO; Chidubem, O; Sampou, WD (2021). The Quality and Acceptance of Family Planning Services in Improving Bayelsa State: Lessons Learnt From a Review of Global Family Planning Programs. Greener Journal of Medical Sciences, 11(2): 212-225.
- Raimi, MO., Mcfubara, KG., Abisoye, OS., Ifeanyichukwu EC., Henry SO., & Raimi, GA (2021) Responding to the call through Translating Science into Impact: Building an Evidence-Based Approaches to Effectively Curb Public Health Emergencies [COVID-19 Crisis]. Global Journal of Epidemiology and Infectious Disease, 1(1). https://www.scipublications.com/journal/index.php/gjeid/article/view/72. [CrossRef]
- Raimi MO & Raimi AG (2020). The Toughest Triage in Decision Impacts: Rethinking Scientific Evidence for Environmental and Human Health Action in the Times of Concomitant Global Crises. CPQ Medicine, 11(1), 01-05.
- Raimi MO, Moses T, Okoyen E, Sawyerr HO, Joseph BO, Oyinlola BO (2020) “A Beacon for Dark Times: Rethinking Scientific Evidence for Environmental and Public Health Action in the Coronavirus Diseases 2019 Era” Medical and Research Microbiology, Vol. 1, Issues 3.
- Samson TK, Ogunlaran OM, Raimi OM (2020); A Predictive Model for Confirmed Cases of COVID-19 in Nigeria. European Journal of Applied Sciences, Volume 8, No 4, Aug 2020;pp:1-10. [CrossRef]
- Raimi MO, Omidiji AO, Ebikapaye O, Moses T, Adeolu TA, Makanjuola Bosede C (2019), Situational Analysis of National Immunization Programme in Nigeria, Journal of Immunology and Inflammation Diseases Therapy. [CrossRef]
- Raimi OM, Lucky EC, Okoyen E, Clement A, Ogbointuwei C, et al. (2021) Making Better Informed, More Confident COVID-19 Decisions: Vaccine Hesitancy, Its Barriers and Impact Studies: Taking Bayelsa State as an Example. Int J Vaccine Immunizat 5(1). https://sciforschenonline.org/journals/vaccines/IJVI126.php. [CrossRef]
- Raimi MO, Emeka CL, Ebikapaye O, Angalabiri C, Christopher O, Atoyebi B (2021) COVID-19 Decision Impacts: Vaccine Hesitancy, its Barriers and Impact Studies: Taking Bayelsa State as an Example., 27 May 2021, PREPRINT (Version 1) available at Research Square. [CrossRef]
- Salvia, R., Halbac-Cotoara-Zamfir, R., Cividino, S., Salvati, L., & Quaranta, G. (2020). From Rural Spaces to Peri-Urban Districts: Metropolitan Growth, Sparse Settlements and Demographic Dynamics in a Mediterranean Region. Land, 9(6), 200. [CrossRef]
- Morufu Olalekan Raimi, Teddy Charles Adias, Christopher Ononiwu Elemuwa (2025) Leveraging Artificial Intelligence to Develop a Nigerian Vaccine Impact Vulnerability Index (NVIVI) for Sustainable Public Health and Environmental Safety. Oral Presentation Presented at the ACS-FUO Conference of the Faculty of Science, Federal University Otuoke, Bayelsa State on the theme: Harnessing Green Chemistry & Artificial Intelligence for Sustainable Development, which held Tuesday, 4th - Thursday 7th November, 2025. Pg. 33.
- Uchenna Geraldine Elemuwa, Christopher Ononiwu Elemuwa, Morufu Olalekan Raimi (2025) Leveraging Artificial Intelligence for Proactive Pharmacovigilance: A National Security Imperative for HPV Vaccine Deployment in Nigeria. Oral Presentation Presented at the ACS-FUO Conference of the Faculty of Science, Federal University Otuoke, Bayelsa State on the theme: Harnessing Green Chemistry & Artificial Intelligence for Sustainable Development, which held Tuesday, 4th - Thursday 7th November, 2025. Pg. 123.
- Raimi Aziba-anyam Gift, Raimi Morufu Olalekan (2025) AI-Driven Synthesis of Personalized ECG Signals for Privacy-Preserving Healthcare Innovation in Nigeria: Toward Sustainable and Ethical Medical Data Generation. Oral Presentation Presented at the ACS-FUO Conference of the Faculty of Science, Federal University Otuoke, Bayelsa State on the theme: Harnessing Green Chemistry & Artificial Intelligence for Sustainable Development, which held Tuesday, 4th - Thursday 7th November, 2025. Pg. 139.
- Aziba-anyam Gift Raimi, Morufu Olalekan Raimi (2025) Leveraging Digital Platforms for Community-Driven Public Health Surveillance in the Niger Delta: A Feasibility Study from Bayelsa State, Nigeria. Oral Presentation Presented at the ACS-FUO Conference of the Faculty of Science, Federal University Otuoke, Bayelsa State on the theme: Harnessing Green Chemistry & Artificial Intelligence for Sustainable Development, which held Tuesday, 4th - Thursday 7th November, 2025. Pg. 124.
- Yusuf Babatunde Adiama; Morufu Olalekan Raimi; Agbebaku Henry Usiobaifo (2025) Echoes of Outbreaks Past: Rethinking Public Health Preparedness in Sub-Saharan Africa in the Age of Emerging Pandemics. Oral Presentation Presented at the 3rd Ku8+International Conference, Kwara State University, Malete with the theme “Innovation and Sustainability of Higher Education in a Changing World.”, which held on Wednesday, 6th – Friday 8th August, 2025.
- Olaniyi Afolabi Opasola; Morufu Olalekan Raimi (2025) From Crisis to Catalyst: Leveraging Public Health Emergencies to Redesign Urban Health Policy in Nigerian Megacities. Oral Presentation Presented at the 3rd Ku8+International Conference, Kwara State University, Malete with the theme “Innovation and Sustainability of Higher Education in a Changing World.”, which held on Wednesday, 6th – Friday 8th August, 2025.
- Henry Olawale Sawyerr; Morufu Olalekan Raimi (2025) Surveillance in the Shadows: Reinventing Community-Based Disease Monitoring Systems in Rural Nigeria. Oral Presentation Presented at the 3rd Ku8+International Conference, Kwara State University, Malete with the theme “Innovation and Sustainability of Higher Education in a Changing World.”, which held on Wednesday, 6th – Friday 8th August, 2025.
- Gift RA, Olalekan RM, Owobi OE, Oluwakemi RM, Anu B, Funmilayo AA (2020). Nigerians crying for availability of electricity and water: a key driver to life coping measures for deepening stay at home inclusion to slow covid-19 spread. Open Access Journal of Science. 2020;4(3):69–80. [CrossRef]
- Gift RA, Olalekan RM (2020). Access to electricity and water in Nigeria: a panacea to slow the spread of Covid-19. Open Access J Sci. 2020;4(2):34. https://medcrave.com/index.php?/articles/det/21409/. [CrossRef]
- Michael-Olomu, Oyintonyo, Raimi Aziba-anyam Gift, Raimi Morufu Olalekan (2025) Strengthening Green Health System Sustainability through Enrollee-Centered Policy Reform: Insights from the National Health Insurance Scheme (NHIS) in Nigeria. Oral Presentation Presented at the ACS-FUO Conference of the Faculty of Science, Federal University Otuoke, Bayelsa State on the theme: Harnessing Green Chemistry & Artificial Intelligence for Sustainable Development, which held Tuesday, 4th - Thursday 7th November, 2025. Pg. 137.
- Babbo D, Raimi MO, Samson TK, Adesina AD, Adaka OA, Jatau SS (2025) Understanding HPV Vaccine Awareness and Knowledge through Sociodemographic Profiling and Multivariable Predictive Modelling in Port Harcourt Local Government Area, Nigeria. JMIR Preprints. 08/12/2025:89196. [CrossRef]
- Iyoha OW, Omotoso AJ, Usiobaifo BE, Raimi MO, Ofor TN (2025) Beyond the Tap: Water Insecurity, Environmental Contamination, and Health Inequities in Uselu, Benin City. JMIR Preprints. 01/11/2025:86938. [CrossRef]
- Omotoso AJ, Ojile MO, Morufu OR (2025). Uncovering the Hidden Burden: Water, Sanitation, and Hygiene (WaSH) Gaps and Their Impact on Health and Learning Outcomes in Secondary Schools, Ede South LGA, Nigeria. Authorea. October 13, 2025. [CrossRef]
- Pambid, R. C. (2015). Factors influencing mothers’ utilization of maternal and child care (MCC) services. Asia Pacific Journal of Multidisciplinary Research, 3(5), 16-28.
- Oyekale, A. S. (2017). Assessment of primary health care facilities’ service readiness in Nigeria. BMC Health Services Research, 17(1), 1-12. [CrossRef]
- Okoyen E, Raimi MO, Omidiji AO, Ebuete AW (2020). Governing the Environmental Impact of Dredging: Consequences for Marine Biodiversity in the Niger Delta Region of Nigeria. Insights Mining Science and technology 2020; 2(3): 555586. https://juniperpublishers.com/imst/pdf/IMST.MS.ID.555586.pdf. [CrossRef]
- Morufu Olalekan Raimi, Elemuwa Uchenna Geraldine, Sarah Samson Jatau (2025) Bridging Gaps in Childhood Immunization Timeliness: Global Evidence from JRF Data with a Spotlight on Nigeria. Oral Presentation Presented at the ACS-FUO Conference of the Faculty of Science, Federal University Otuoke, Bayelsa State on the theme: Harnessing Green Chemistry & Artificial Intelligence for Sustainable Development, which held Tuesday, 4th - Thursday 7th November, 2025. Pg. 97.
- Kakwi JD, Yakasai KM, Kakwi JD, Raimi MO (2025). Promotion over pixels: a mixed-methods analysis of vaccine communication strategies in Plateau State, Nigeria. BMJ Open 2025;0:e094029. [CrossRef]
- Elemuwa CO, Ainu M, Adias TC, Sunday OA, Ufuoma RS, Elemuwa UG, Christopher O, Raimi MO, Oginifolunnia OC, Oweibia M, Ozoemena OV, Daniel ET (2024) Boosting community engagement: Leveraging the ward health system approach for enhanced HPV vaccination acceptance in Nigeria. [version 1; peer review: awaiting peer review]. F1000Research 2024, 13:1392. [CrossRef]
- Promise VI, Alabere I, Abdulraheem I, Raimi MO (2025) The Effect of Mobile Phone and Home Visit on Childhood Vaccination Uptake in Rural Communities of Bayelsa State Nigeria. A Pragmatic Cluster Randomized Control Trial. JMIR Preprints. 01/04/2025:75332. [CrossRef]
- Ibrahim ML, Sawyerr HO, Opasola OA, Adiama YB, Raimi MO (2025) Bridging Knowledge and Practice Gaps in Lassa Fever Prevention: Awareness, Attitudes, and Infection Control Measures Among Healthcare Workers and Residents in Edo, Ondo, and Kwara States. JMIR Preprints. 30/03/2025:75233. [CrossRef]
- Kakwi JD, Yakasai KM, Raimi MO, Kakwi JD (2024) Understanding the Dynamics of COVID-19 Vaccine Uptake in Plateau State, Nigeria: Analyzing Socioeconomic, Cultural, and Communication Influences. JMIR Preprints. 30/12/2024:70702. [CrossRef]
- Promise VI, Macauley T, Alabere I, Abdulraheem I, Raimi MO (2024) Closing the Gap: Assessment of Vaccination Coverage Among Under Two Children in Bayelsa State, Nigeria. JMIR Preprints. 29/12/2024:70671. [CrossRef]
- Elemuwa CO, Raimi MO, Ainu M, Adias TC, Ufuoma RS, Elemuwa UG, Oginifolunnia OC, Rath BA, Obermeier PE (2024) Conquering Mpox: A Comprehensive Public Health Strategy for Addressing Mpox and Poxvirus Infections in Nigeria – Understanding Global Trends, Transmission Dynamics, and Effective Prevention and Control Measures in Nigeria. JMIR Preprints. 14/10/2024:67534. [CrossRef]
- Kakwi JD, Yakasai KM, Kakwi JD, Raimi MO (2024) Campaigning Against Vaccine Hesitancy: Evaluating the Effectiveness of Health Communication on COVID-19 Vaccination Uptake in Plateau State, Nigeria. JMIR Preprints. 22/09/2024:66755. [CrossRef]
- Okechukwu CO, Ainu M, Adias TC, Elemuwa CO, Rotifa SU, Ogbointuwei C, Raimi MO, Oweibia M, Alabo AF, Okoyen E, Appah WW (2024) Evaluating the Impact of Rotavirus Vaccination on Childhood Diarrhea Incidence in Bayelsa State, Nigeria: Achievements, Challenges, and Future Directions. JMIR Preprints. 27/07/2024:64822. [CrossRef]
- Uchenna GE, Enato E, Christopher OE, Tochukwu DE, Morufu OR (2024) Pentavalent Vaccine: How Safe Is It Among Infants Accessing Immunization In Nigerian Health Facilities. medRxiv 2024.05.28.24307998. [CrossRef]
- Morufu OR, Aziba-anyam GR and Teddy CA (2021) ‘Silent Pandemic’: Evidence-Based Environmental and Public Health Practices to Respond to the Covid-19 Crisis. IntechOpen. ISBN 978-1-83969-144-7. https://www.intechopen.com/online-first/silent-pandemic-evidence-based-environmental-and-public-health-practices-to-respond-to-the-covid-19-Published: December 1st 2021; ISBN: 978-1-83969-144-7; Print ISBN: 978-1-83969-143-0; eBook (PDF) ISBN: 978-1-83969-145-4. Copyright year: 2021. [CrossRef]
- Raimi MO (2025a). Peer Review Report For: Zero-Dose Childhood Immunization in Conflict-Affected Productive Safety Net Program Districts of Ethiopia: A Comparative Cross-Sectional Study [version 2; peer review: 2 approved with reservations, 1 not approved]. VeriXiv 2025, 2:140. [CrossRef]
- Raimi MO (2025b). Peer Review Report For: Zero-Dose Childhood Immunization in Conflict-Affected PSNP Districts of Ethiopia: A Comparative Cross-Sectional Study [version 3; peer review: 1 approved, 1 approved with reservations, 1 not approved]. VeriXiv 2025, 2:140. [CrossRef]
- Raimi MO (2025c). Peer Review Report For: Mapping Community Vulnerability to reduced Vaccine Impact in Uganda and Kenya: A spatial Data-driven Approach [version 2; peer review: 1 approved with reservations]. NIHR Open Res 2025, 5:24. [CrossRef]
- Raimi MO (2025d). Peer Review Report For: Mapping Community Vulnerability to reduced Vaccine Impact in Uganda and Kenya: A spatial Data-driven Approach [version 3; peer review: 2 approved]. NIHR Open Res 2025, 5:24. [CrossRef]
- Nott, S., Colbran, R., & Edwards, M. A. (2023). Collaborative care: Empowering community in the development of rural primary health workforce and service delivery models. International Journal of Integrated Care, 23(S3), 20. [CrossRef]
- Christopher OE; Teddy CA; Uchenna GE; Aziba-anyam GR; Morufu OR (2025) Digital Science Observatory (DSO) Web Application: Advancing Data Science for Sustainability. Oral Presentation Presented at the 1st International Conference of the Faculty of Science, Federal University Otuoke, Bayelsa State on the theme: Revolutionizing a Sustainable Tomorrow: Harnessing Science, Innovation and Community Power to Drive Circular Economy Solutions, Climate Resilience, and a Thriving Green Economy, which held Tuesday, 4th – Friday 7th March, 2025. Pp. 21.
- Orton, M., Agarwal, S., Muhoza, P., Vasudevan, L., & Vu, A. (2018). Strengthening delivery of health services using digital devices. Global Health: Science and Practice, 6(Supplement 1), S61-S71. https://StrengtheningDeliveryofHealthServicesUsingDigitalDevices&btnG=#. [CrossRef]
- Peng, Y., Zhai, S., Zhang, Z., Zhang, R., Zhang, J., Jin, Q., ... & Chen, J. (2024). People-centered primary care measures in health equity: a perspective of urban–rural comparison in Beijing, China. International Journal for Quality in Health Care, 36(3), mzae067. [CrossRef]
- Peterson, K. (2020). Meeting healthcare needs in rural America. Nursing2023, 50(8), 16-18. [CrossRef]
- Peter-Kio, O. B., & Oweredaba, S. (2023). Comparative analysis of reproductive healthcare services utilization among women of childbearing age in rural and urban areas of Rivers West Senatorial District, Nigeria. Current Journal of Applied Science and Technology, 35(22), 262-272. [CrossRef]
- Shahzad, F., Abid, F., Obaid, A. J., Kumar Rai, B., Ashraf, M., & Abdulbaqi, A. S. (2021). Forward stepwise logistic regression approach for determinants of hepatitis B & C among Hiv/Aids patients. International Journal of Nonlinear Analysis and Applications, 12(Special Issue), 1367-1396.
- Novoa, P. C. R. (2014). What changes in research ethics in Brazil: Resolution no. 466/12 of the National Health Council. Einstein (São Paulo), 12, vii-xiv. [CrossRef]
- Mcfubara, K. G., & Eragbhe, E. (2012). Health manpower development in Bayelsa State, Nigeria. Annals of African Medicine, 11(4), 259–266. [CrossRef]
- Cometto, G., Boniol, M., Mahat, A., Diallo, K., & Campbell, J. (2023). Understanding the WHO health workforce support and safeguards list 2023. Bulletin of the World Health Organization, 101(6), 362. [CrossRef]
- Agarwal, S., Sripad, P., Johnson, C., Kirk, K., Bellows, B., Ana, J., ... & Warren, C. E. (2019). A conceptual framework for measuring community health workforce performance within primary health care systems. Human resources for health, 17, 1-20. [CrossRef]
- National Primary Health Care Development Agency (NPHCDA): Minimum Standards for Primary Health Care in Nigeria (NPHCDA) Plot 681/682 Port-Harcourt Crescent, Off Gimbiya Street, Garki II, Abuja Department of Planning, Research and Statistics.
- Dipeolu, I. O. (2022). New approaches for improved service delivery in rural settings. In U. Bacha (Ed.), Rural Health. IntechOpen. [CrossRef]
- Kumar, R. (2014). Rural health care services of PHC and its impact on marginalized and minority communities. Journal of Health Management, 16(2), 215-229. [CrossRef]
- Raimi MO. (2024). Structured PREreview of “Development and Content Validity of the Handwashing Index (HWI)”. Zenodo. [CrossRef]
- Raimi MO, Omidiji AO, Abdulraheem AF, Ochayi EO (2018) A Survey of Hand Washing Behaviour and Awareness among Health Care Workers in Health Care Facilities in Kubwa District of Bwari Area Council, F.C.T. Abuja, Nigeria. Annals of Ecology and Environmental Science Volume 2, Issue 2, 2018, PP 1-18.
- Raimi, MO, Pigha, Tarilayun K and Ochayi, E. O (2017). Water-Related Problems and Health Conditions in the Oil-Producing Communities in Central Senatorial District of Bayelsa State. Imperial Journal of Interdisciplinary Research (IJIR) Vol-3, Issue-6, ISSN: 2454-1362.
- Olalekan RM, Vivien O. T, Adedoyin O. O, et al. (2018). The sources of water supply, sanitation facilities and hygiene practices in oil producing communities in central senatorial district of Bayelsa state, Nigeria. MOJ Public Health. 2018;7(6):337–345. [CrossRef]
- Raimi MO, Abdulraheem AF, Major I, Odipe OE, Isa HM, Onyeche C (2019). The Sources of Water Supply, Sanitation Facilities and Hygiene Practices in an Island Community: Amassoma, Bayelsa State, Nigeria. Public Health Open Access 2019, 3(1): 000134. ISSN: 2578-5001. [CrossRef]
- Kubica, G. (2022). Impacts of Sustainable Development Goal 3 and health systems. International Journal of Environmental Research and Public Health, 19(23), 15700. [CrossRef]
- Andrews, K., & Sharma, J. (2023). Unlocking SDG 3 success: The power of data collection on health service delivery. World Bank Publications. [CrossRef]
- Friedman C. P., Wyatt J.C. Evaluation methods in biomedical informatics. 2nd ed. New York: Springer Science + Business Media, Inc; 2006. https://www.ncbi.nlm.nih.gov/books/NBK481584/#references.c10.r7.Federal Republic of Nigeria, National Strategic Health Development Plan II 2018-2022.
- Ajisegiri WS, Abimbola S, Tesema AG, Odusanya OO, Peiris D, Joshi R (2022) The organisation of primary health care service delivery for non-communicable diseases in Nigeria: A case-study analysis. PLOS Glob Public Health 2(7): e0000566. [CrossRef]
- Cattivelli, V. (2024). Where is the city? Where is the countryside? Assessing the methods for the classification of urban, rural, and intermediate areas in Europe. Journal of Rural Studies, 109, 103288. [CrossRef]
- Mahdiyan, S., Dehghani, A., Tafti, A. D., Pakdaman, M., & Askari, R. (2019). Hospitals’ efficiency in Iran: A systematic review and meta-analysis. Journal of Education and Health Promotion, 8. [CrossRef]
- Haldane, V., H. Chuah, F. L., Srivastava, A., Singh, S. R., H. Koh, G. C., Seng, C. K., & Legido-Quigley, H. (2019). Community participation in health services development, implementation, and evaluation: A systematic review of empowerment, health, community, and process outcomes. PLOS ONE, 14(5), e0216112. [CrossRef]
- Federal Republic of Nigeria. (2018). Second National Strategic Health Development Plan II (2018–2022). Federal Ministry of Health. https://extranet.who.int/countryplanningcycles/sites/default/files/public_file_rep/NGA_Nigeria_Second-National-Strategic-Health-Development-Plan-II-2018-22.pdf.
- World Health Organization. (2016). National Health Policy. Federal Ministry of Health, Nigeria.https://extranet.who.int/countryplanningcycles/sites/default/files/planning_cycle_repository/nigeria/draft_nigeria_national_health_policy_final_1_feb_2016.pdf.
Figure 1.
Urban-rural disparities in primary healthcare service delivery weaknesses across government-owned facilities in Bayelsa State, Nigeria.
Figure 1.
Urban-rural disparities in primary healthcare service delivery weaknesses across government-owned facilities in Bayelsa State, Nigeria.
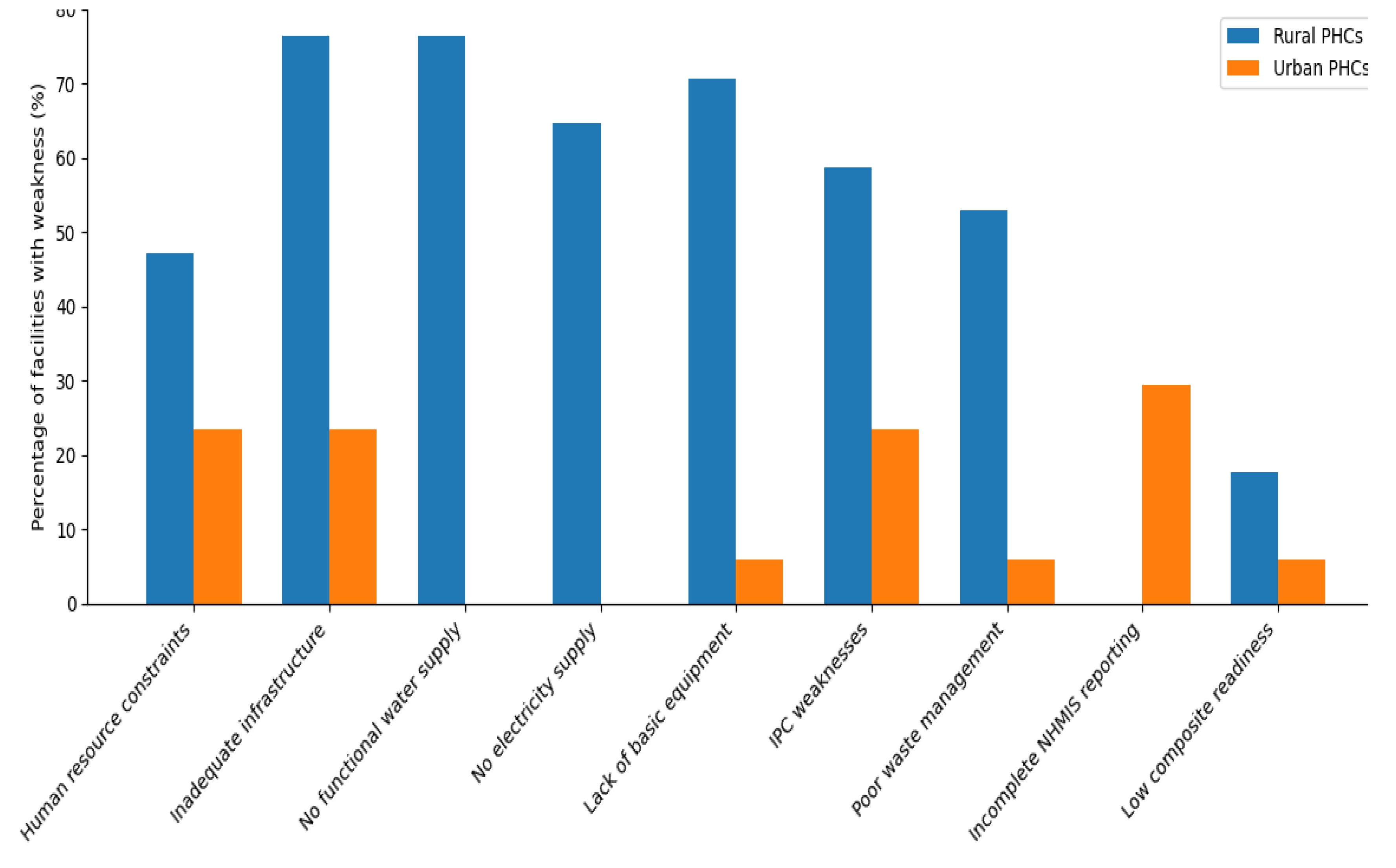
Figure 2.
Forest plot of urban-rural differences in primary healthcare service delivery weaknesses across key service domains in Bayelsa State, Nigeria.
Figure 2.
Forest plot of urban-rural differences in primary healthcare service delivery weaknesses across key service domains in Bayelsa State, Nigeria.
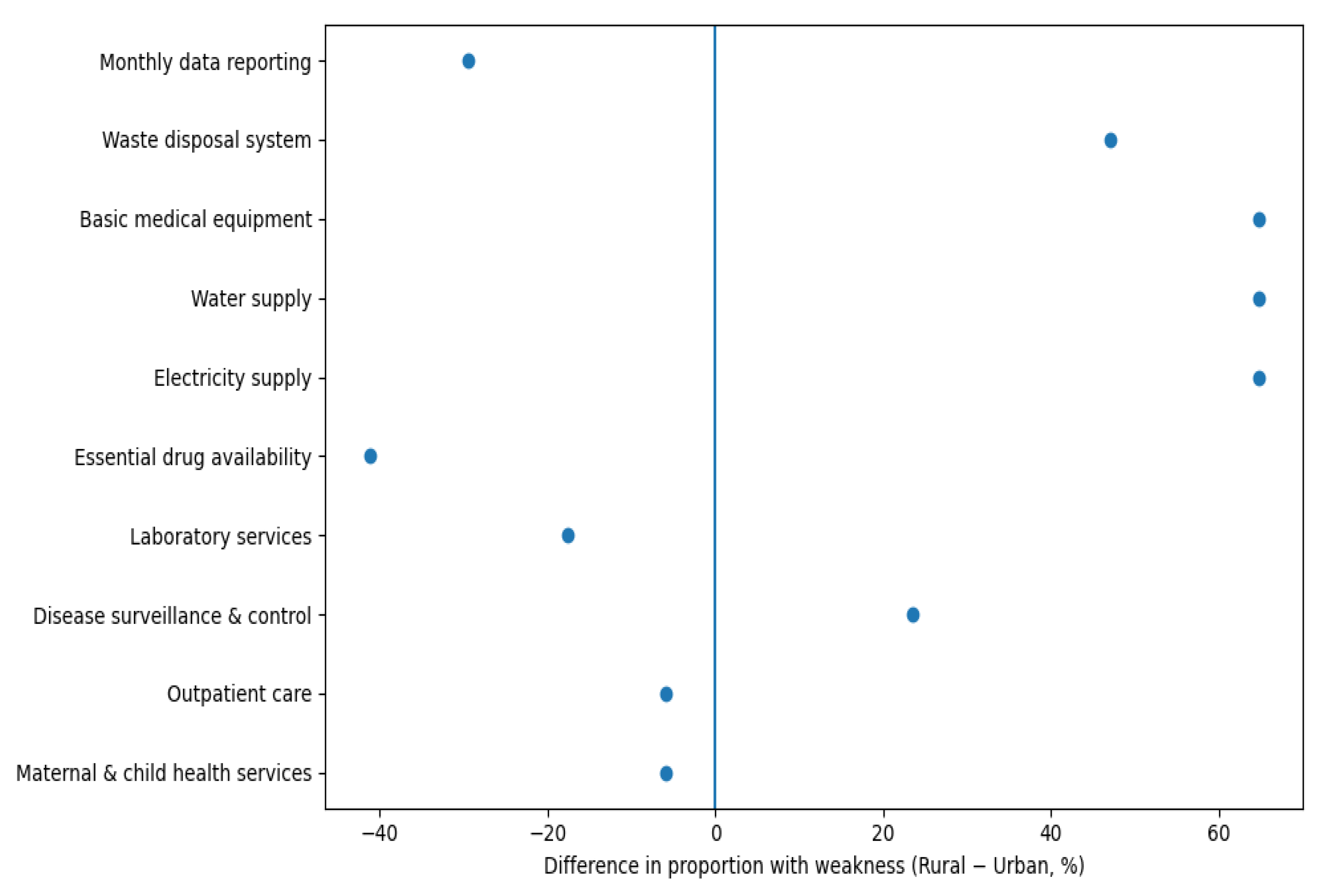
Figure 3.
Prospects for strengthening primary healthcare service delivery across rural and urban communities in Bayelsa State. The figure illustrates pronounced urban–rural disparities in infrastructure readiness, essential utilities, equipment availability, infection prevention and control practices, and health information systems, with comparatively stronger service utilisation indicators in rural facilities.
Figure 3.
Prospects for strengthening primary healthcare service delivery across rural and urban communities in Bayelsa State. The figure illustrates pronounced urban–rural disparities in infrastructure readiness, essential utilities, equipment availability, infection prevention and control practices, and health information systems, with comparatively stronger service utilisation indicators in rural facilities.
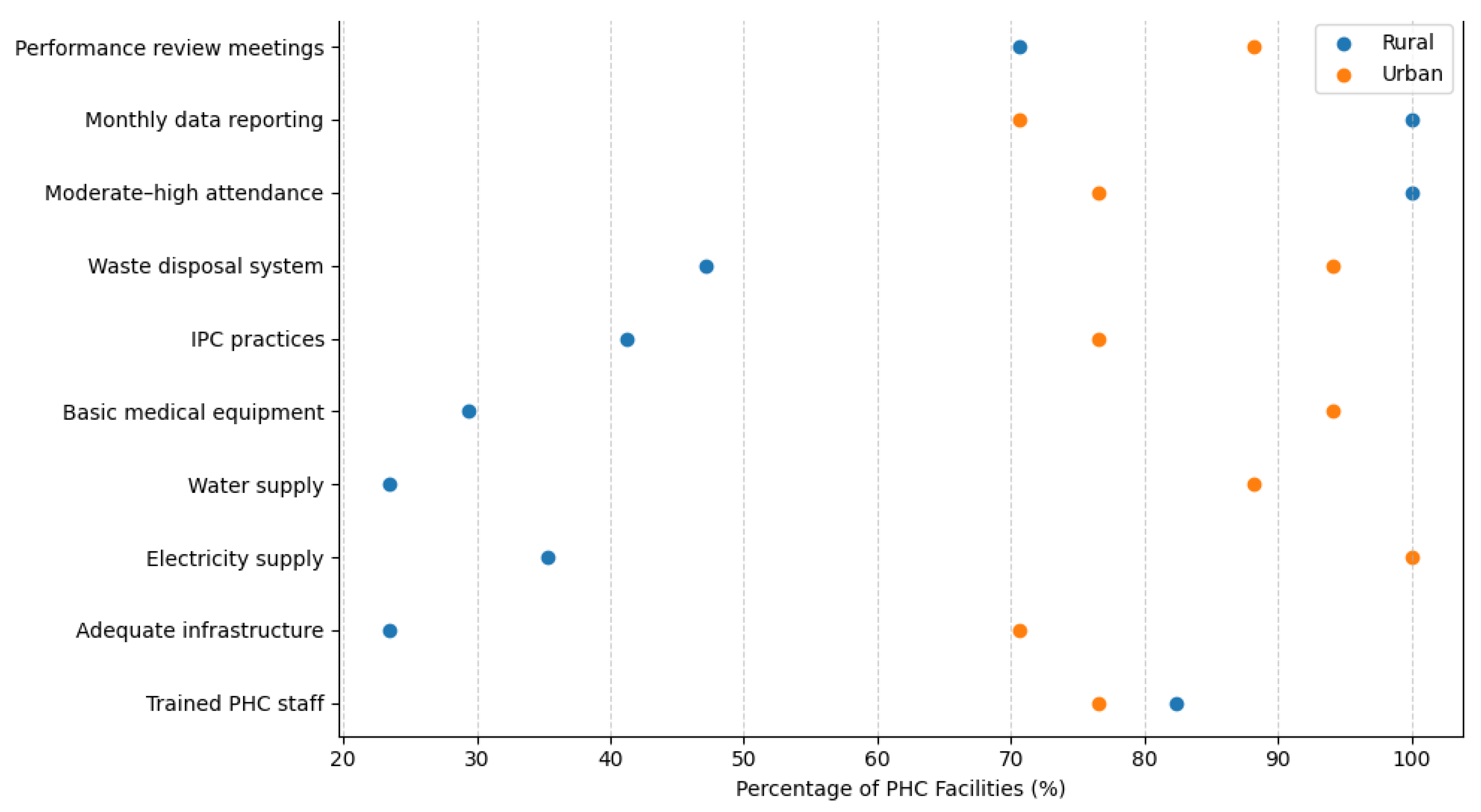
Figure 4.
Facility planning, performance management, and target achievement by location of primary healthcare facilities in Bayelsa State.
Figure 4.
Facility planning, performance management, and target achievement by location of primary healthcare facilities in Bayelsa State.
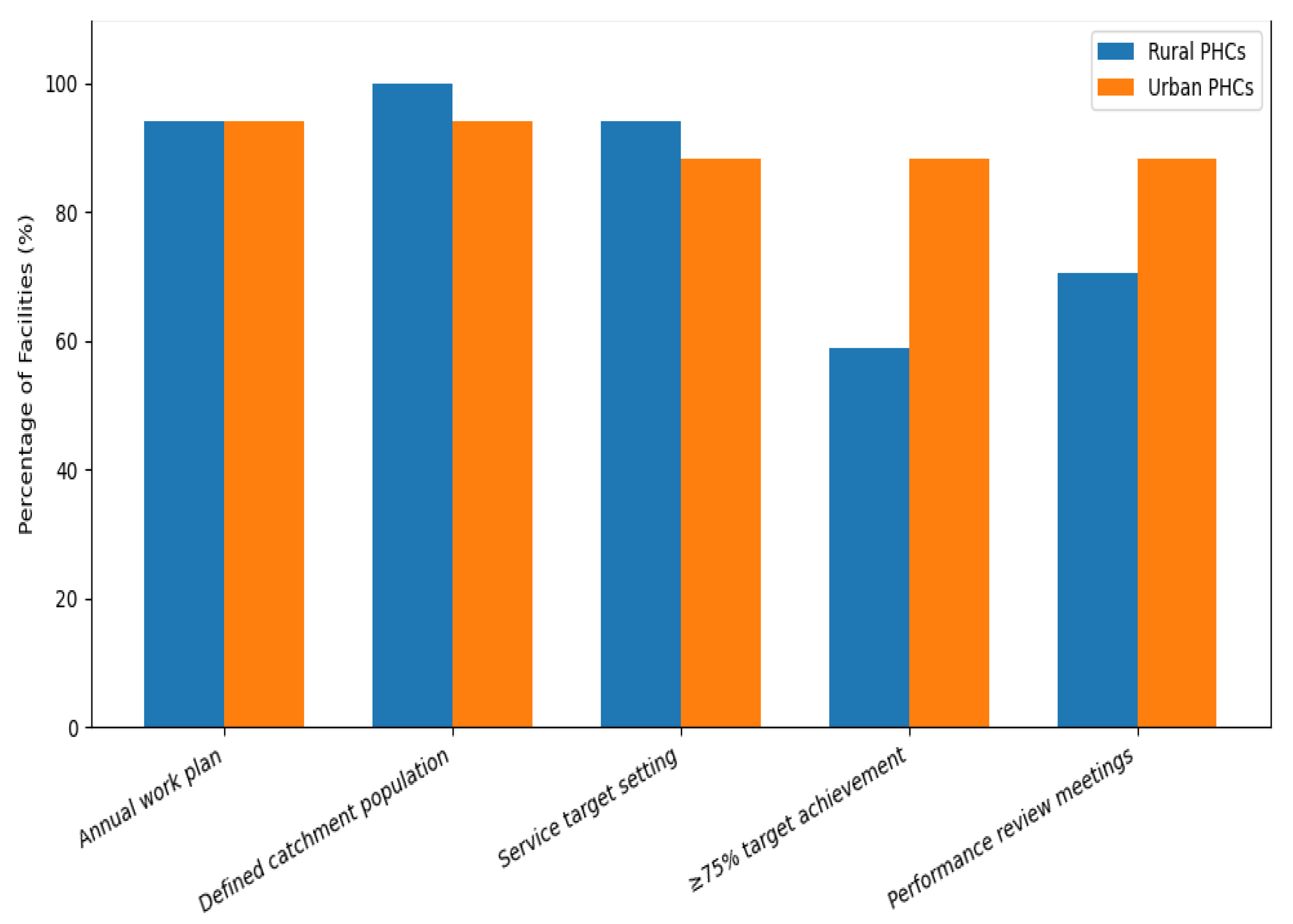
Figure 5.
| Barriers, facilitators, and utilisation pathways influencing access to primary healthcare services in rural and urban communities of Bayelsa State.
Figure 5.
| Barriers, facilitators, and utilisation pathways influencing access to primary healthcare services in rural and urban communities of Bayelsa State.
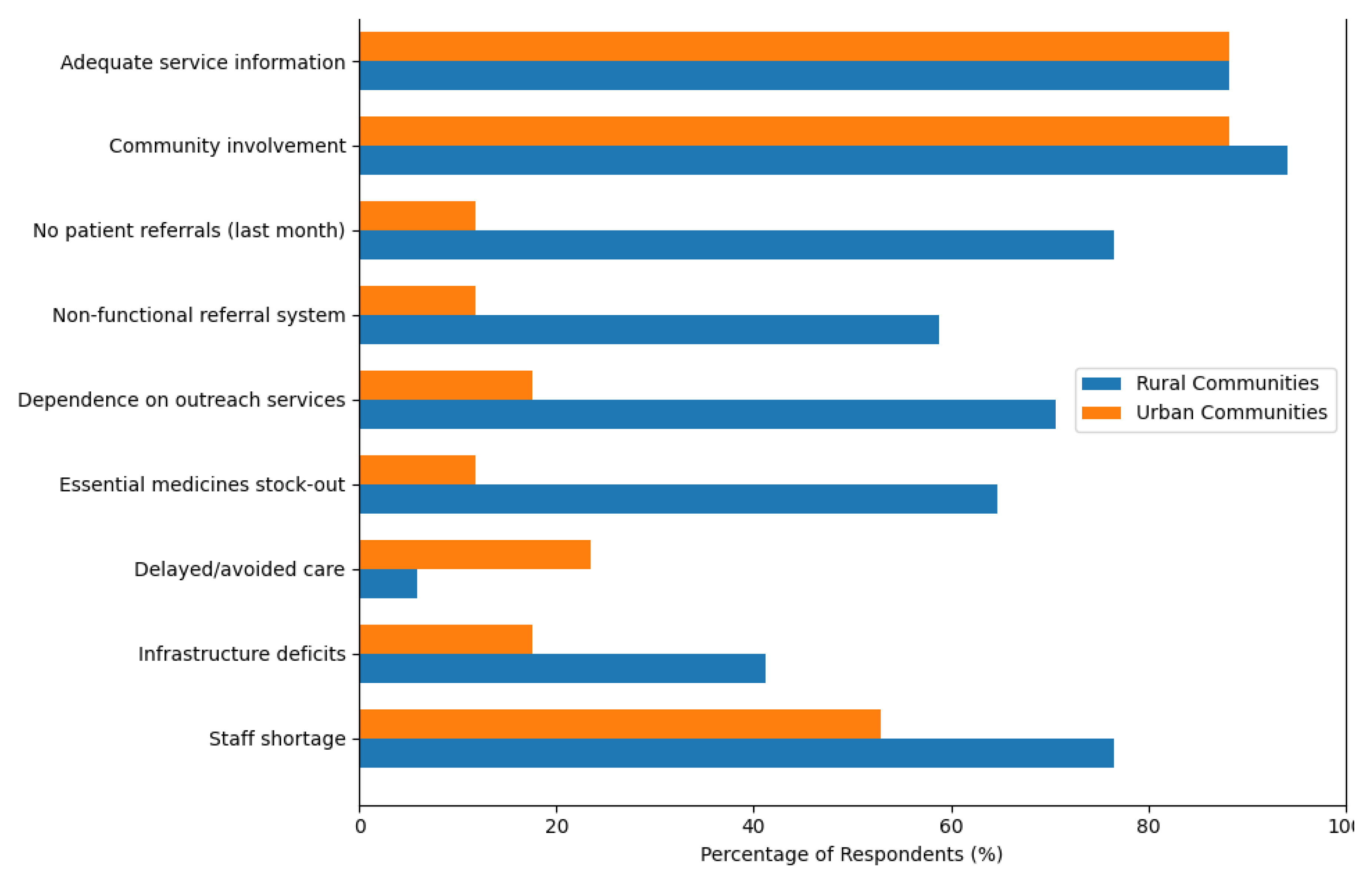
Figure 6.
Urban-Rural Health Inequities in Bayelsa State.


Table 1.
Level of Weakness in Primary Healthcare Service Delivery in Urban and Rural PHC Facilities in Bayelsa State.
Table 1.
Level of Weakness in Primary Healthcare Service Delivery in Urban and Rural PHC Facilities in Bayelsa State.
| Service delivery domain | Weakness indicator | Rural PHCs n (%) | Urban PHCs n (%) |
|---|---|---|---|
| Human resources | No trained staff for key PHC services | 3 (17.6) | 4 (23.5) |
| ≤1 trained staff available | 8 (47.1) | 4 (23.5) | |
| Infrastructure & utilities | Inadequate infrastructure score | 13 (76.5) | 5 (29.4) |
| No electricity supply | 11 (64.7) | 0 (0.0) | |
| No functional water supply | 13 (76.5) | 2 (11.8) | |
| Basic medical equipment | Lacking essential basic equipment | 12 (70.6) | 1 (5.9) |
| Infection prevention & control | Inadequate IPC measures | 10 (58.8) | 4 (23.5) |
| Waste management | No functional waste disposal process | 9 (52.9) | 1 (5.9) |
| Health information systems | Incomplete monthly NHMIS reporting | 0 (0.0) | 5 (29.4) |
| Service readiness (composite) | Low readiness for basic amenities | 3 (17.6) | 1 (5.9) |
| Low readiness for essential medicines | 3 (17.6) | 1 (5.9) | |
| Low diagnostic capacity readiness | 3 (17.6) | 1 (5.9) |
Table 1: Distribution of indicators reflecting human resource, infrastructure, equipment, infection control, information system, and composite service readiness weaknesses across urban and rural government-owned primary healthcare facilities in Bayelsa State. Data are presented as frequencies and percentages to quantify the level of service delivery weakness within each setting.
Table 2.
Comparison of Key Service Delivery Weaknesses Across Urban and Rural Primary Healthcare Facilities, Bayelsa State.
Table 2.
Comparison of Key Service Delivery Weaknesses Across Urban and Rural Primary Healthcare Facilities, Bayelsa State.
| Service delivery domain | Indicator (weakness defined as “No”) | Rural (n = 17) n (%) | Urban (n = 17) n (%) | χ² | p-value |
|---|---|---|---|---|---|
| Core clinical services | Maternal & child health services | 0 (0.0) | 1 (5.9) | 1.030 | 0.310 |
| Outpatient care | 0 (0.0) | 1 (5.9) | 1.030 | 0.310 | |
| Preventive services | Disease surveillance & control | 5 (29.4) | 1 (5.9) | 3.238 | 0.072 |
| Diagnostic capacity | Laboratory services | 6 (35.3) | 9 (52.9) | 1.074 | 0.300 |
| Medicines & supplies | Essential drug availability | 6 (35.3) | 13 (76.5) | 5.846 | 0.016 |
| Utilities | Electricity supply | 11 (64.7) | 0 (0.0) | 16.261 | <0.001 |
| Water supply | 13 (76.5) | 2 (11.8) | 14.435 | <0.001 | |
| Equipment readiness | Basic medical equipment | 12 (70.6) | 1 (5.9) | 15.070 | <0.001 |
| Infection control | Waste disposal system | 9 (52.9) | 1 (5.9) | 9.067 | 0.003 |
| Health information systems | Monthly data reporting | 0 (0.0) | 5 (29.4) | 5.862 | 0.015 |
Table 3.
Indicators of Prospects for Strengthening Primary Healthcare Service Delivery for Advancing SDG 3 in Urban and Rural Communities of Bayelsa State.
Table 3.
Indicators of Prospects for Strengthening Primary Healthcare Service Delivery for Advancing SDG 3 in Urban and Rural Communities of Bayelsa State.
| SDG-3-relevant service domain | Strengthening indicator | Rural (n = 17) n (%) |
Urban (n = 17) n (%) |
χ² | p-value |
|---|---|---|---|---|---|
| Human resources capacity | ≥1 trained staff for key PHC services | 14 (82.4) | 13 (76.5) | 0.158 | 0.691 |
| Infrastructure readiness | Adequate infrastructure score | 4 (23.5) | 12 (70.6) | 8.127 | 0.017 |
| Essential utilities | Electricity supply available | 6 (35.3) | 17 (100.0) | 16.261 | <0.001 |
| Water supply available | 4 (23.5) | 15 (88.2) | 14.435 | <0.001 | |
| Equipment readiness | Basic medical equipment available | 5 (29.4) | 16 (94.1) | 15.070 | <0.001 |
| Infection prevention & control | Adequate IPC practices | 7 (41.2) | 13 (76.5) | 4.371 | 0.037 |
| Waste management systems | Functional waste disposal system | 8 (47.1) | 16 (94.1) | 9.067 | 0.003 |
| Service utilisation capacity | Moderate–high patient attendance | 17 (100.0) | 13 (76.5) | 7.040 | 0.218 |
| Health information systems | Routine monthly data reporting | 17 (100.0) | 12 (70.6) | 5.862 | 0.015 |
| Governance & monitoring | Performance review meetings held | 12 (70.6) | 15 (88.2) | 1.619 | 0.203 |
Table 4.
Facility Planning, Performance Management, and Target Achievement by Location of Primary Healthcare Facilities in Bayelsa State.
Table 4.
Facility Planning, Performance Management, and Target Achievement by Location of Primary Healthcare Facilities in Bayelsa State.
| Health system governance domain | Indicator | Rural (n = 17) n (%) | Urban (n = 17) n (%) | χ² | p-value |
|---|---|---|---|---|---|
| Facility planning | Availability of annual work plan | 16 (94.1) | 16 (94.1) | 0.000 | 1.000 |
| Population accountability | Defined catchment population | 17 (100.0) | 16 (94.1) | 1.030 | 0.310 |
| Target setting | Sets monthly or quarterly service targets | 16 (94.1) | 15 (88.2) | 0.366 | 0.545 |
| Performance achievement | Achieves ≥75% of planned service targets | 10 (58.8) | 15 (88.2) | 3.778 | 0.052 |
| Performance monitoring | Conducts routine performance review meetings | 12 (70.6) | 15 (88.2) | 1.619 | 0.203 |
Table 5.
Distribution of barriers, facilitators, and utilisation pathway indicators influencing access to primary healthcare services across urban and rural communities in Bayelsa State.
Table 5.
Distribution of barriers, facilitators, and utilisation pathway indicators influencing access to primary healthcare services across urban and rural communities in Bayelsa State.
| Utilisation pathway domain | Indicator | Rural n (%) | Urban n (%) | χ² | p-value |
|---|---|---|---|---|---|
| Access barriers | Shortage of qualified healthcare staff | 13 (76.5) | 9 (52.9) | 2.061 | 0.151 |
| Infrastructure deficits (water, electricity, space) | 7 (41.2) | 3 (17.6) | 2.267 | 0.132 | |
| Delayed or avoided seeking care | 1 (5.9) | 4 (23.5) | 2.110 | 0.146 | |
| Supply chain constraints | Essential medicines frequently out of stock | 11 (64.7) | 2 (11.8) | 10.088 | 0.001 |
| Service access mechanisms | Dependence on outreach services for care | 12 (70.6) | 3 (17.6) | 20.000 | 0.018 |
| Referral pathways | Non-functional referral system | 10 (58.8) | 2 (11.8) | 8.242 | 0.004 |
| No patient referrals in previous month | 13 (76.5) | 2 (11.8) | 22.400 | <0.001 | |
| Community engagement | Community involvement in health planning | 16 (94.1) | 15 (88.2) | 0.366 | 0.545 |
| Information access | Adequate information on available services | 15 (88.2) | 15 (88.2) | 0.000 | 1.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



