Submitted:
07 January 2026
Posted:
08 January 2026
You are already at the latest version
Abstract
Tyrosine kinase inhibitors (TKIs) added to chemotherapy have improved outcomes ofadult patients with Philadelphia-positive B-cell acute lymphoblastic leukemia (Ph+ B-ALL). These improvements initially led to a larger proportion of patients realizing allogeneic stem cell transplantation (alloSCT), long considered essential for cure, but there has been a re-evaluation of alloSCT. At Princess Margaret Hospital (PM), adult patients with Ph+ B-ALL have been treated with a pediatric-inspired chemotherapy protocol with mostly imatinib. In the last two decades, we have witnessed many iterative changes in our approach. Here we examine the outcomes of all Ph+ B-ALL patients treated at our institution from 2001 to 2019. During this time, there were two major protocol changes – omission of asparaginase in 2009, and discontinuation of routine referral for first complete remission (CR1) alloSCT from the early 2010s. Median follow-up was 41.13 months (range, 0.46-228.79). 141 patients (91.56%) achieved CR1. Patient outcomes improved iteratively, with best results seen in the final (2016-2019) cohort: no asparaginase, no routine alloSCT referral in CR1; 4-year OS and RFS were 87.0% and 69.3%, respectively. The long-term OS in this patient group retained statistical significance in the multivariable analysis (p=0.0176) when BCR::ABL1 molecular residual disease (MRD) were considered.
Keywords:
Philadelphia-positive B-cell acute lymphoblastic leukemia
; adult
; pediatric-inspired chemotherapy
Introduction
The treatment landscape of adult Ph+ B-ALL has changed considerably since the addition of TKIs to chemotherapy. At PM, our approach has been to use a pediatric-inspired chemotherapy protocol, PM-DFCI (originally derived from DFCI 10-175/NCIC CTG AL.4), combined with a TKI (usually imatinib), and with modifications for ages <60 (PM-DFCI-3.n) and ≥60 (PM-DFCI-4.n) years (Martell et al, 2013; Thyagu et al, 2014; Kanfar et al, 2016). Our approach (Supplement – Figure S1) has been adopted by many other institutions in Canada. Increased toxicity observed early on when imatinib was added led to the subsequent omission of asparaginase in 2009. This approach was subsequently adopted by other groups due to toxicity seen in their patients (Bassan et al, 2010; Patel et al, 2017).
In the early 2010s, there was evidence for better safety and efficacy of chemotherapy/TKI combinations. Further, we observed that many patients for whom we were unable to find an alloSCT donor, were nevertheless achieving good long-term outcomes without consolidative alloSCT, we started to question the value of obligatory transplantation. Our approach evolved further such that only patients with an inadequate MRD response were referred for CR1 alloSCT. This contrasts with some centres where alloSCT remains the mainstay consolidative treatment. The European Society for Blood and Marrow Transplantation (EBMT) recommends CR1 alloSCT as standard of care, regardless of MRD results (Snowden et al, 2022). However, our approach has been adopted by many other centres, and consistent with this, the National Comprehensive Cancer Network (NCCN) now recommends consolidative alloSCT only for patients with persistent or rising MRD after minimizing MRD with additional treatment (Shah et al, 2024). While NCCN 2024 explicitly states that there is no CR1 alloSCT advantage for those ≤21 years if they have achieved MRD negativity, for patients >21 years, the transplant recommendation remains less clear (Shah et al, 2024). Additionally, while the American Society for Transplantation and Cellular Therapy recommends CR1 alloSCT for patients receiving TKIs, it remains unclear whether this recommendation should apply to patients achieving complete molecular remission (CMR) (DeFilipp et al, 2019).
Given the evolution, this retrospective review aims to examine the effectiveness of our approach, with a particular focus on the roles of asparaginase, CR1 alloSCT, and MRD monitoring, on overall survival (OS) and relapse free survival (RFS), and to compare our outcomes with those reported in the literature.
Methods
Patients
Between March 2001 and March 2019, 157 patients (≥18 years) with newly diagnosed Ph+ B-ALL were treated at PM. Patients were last followed up in May 2022. Three patients were excluded due to initial treatment with imatinib/steroid, single agent imatinib, and amsacrine/vincristine, respectively. 152 patients were treated with our pediatric-inspired multiagent regimen in combination with imatinib and 12 intrathecal chemotherapy. 2 additional patients treated with the original NCIC CTG AL.4 or HyperCVAD protocols were included. All patients except one, who received an unknown TKI, received imatinib upfront, while 2 patients received dasatinib after intolerance to imatinib early in their treatment course. After completion of chemotherapy, the TKI was continued indefinitely as maintenance therapy. 141 of the 154 (91.56%) patients achieved CR1. Prior to 2015-2016, patients were universally referred for consolidative alloSCT, regardless of MRD response, if they were appropriate transplant candidates and matched related or unrelated donors were identified. Between 2016 and 2019, however, only eight patients underwent alloSCT in CR1 – two due to therapy-related disease, four due to flow cytometric MRD positivity post-induction or at 3 months, one due to a very slow reduction in BCR::ABL1 levels, and another due to patient choice after discussion with the transplant team (in the first year after the decision to shift away from CR1 alloSCT, patient referrals were still being made to facilitate patient informed consent). This treatment review was approved by the University Health Network Ethics Board.
Response Definitions
BCR::ABL1 molecular response criteria used in this analysis is BCR::ABL1:ABL1 ratio ≤0.1% on the International Scale for the p210 transcripts, or ≥3-log reduction in p190 transcripts. Relapse was defined by the recurrence of ≥5% blasts in a bone marrow aspirate/biopsy, or by the new presence of extramedullary disease. Time to RFS was calculated in months from the date of CR1 until relapse or death. Time to OS was calculated in months from the date of CR1 until death.
Statistical Analysis
Patient characteristics were summarized using median (range) for continuous variables, and frequencies (percentages) for categorical variables of interest. Comparisons of baseline characteristics of the two groups (those who undergo CR1 alloSCT vs. those who did not undergo CR1 alloSCT) were made using chi-square or Fisher’s exact tests (as appropriate) for categoric variables, and with the student’s t-test for continuous variables. RFS and OS rates were calculated using the Kaplan-Meier estimates, and the impact of covariates of interest was assessed using the log-rank test. Multivariable Cox proportional hazards models were used to assess the joint impact of covariates on RFS and OS. All p-values were 2-sided. For the statistical analyses, p<0.05 was considered statistically significant. Statistical analysis was performed using version 9.4 of the SAS system for Windows, Copyright © 2023 by SAS Institute, Inc., Cary, NC, USA.
Results
Patient clinical and demographic characteristics are summarized in Table 1. 141 patients achieved CR1. There were five induction deaths. One patient who did not receive asparaginase died from bacteremia, viremia, electrolyte disturbance, and subdural hemorrhages/infarcts in the context of CNS disease. The other four deaths had received asparaginase – two from liver failure, pneumonia and upper gastrointestinal bleeding (one also with methotrexate toxicity), one from liver and renal failure in the context of septicemia from Aspergillus, and another of cardiac and renal failure, and pneumonia.
Median follow-up was 41.13 months (range, 0.46-228.79). Fifty-three (37.59%) patients underwent CR1 alloSCT. These patients, and those who did not undergo CR1 alloSCT, had similar baseline characteristics with regards to median white blood cell (WBC) count, prior cancer diagnosis, extramedullary disease, and central nervous system (CNS) involvement. The only difference between these two groups was patient age, with the transplanted cohort being significantly younger (median, 46 vs 55 years; p<0.001). Median time from diagnosis to CR1 alloSCT was 1.18 months (range, 0.66-2.89). Twenty-five patients had matched sibling donors, 39 had matched unrelated donors, and one patient had a cord blood donor, while information on donor was missing for one patient. Only 12 patients received TKI maintenance post-alloSCT, as its role was unclear at the time when these transplants were performed.
From 2001 to 2019, thirty five (24.8%) patients received asparaginase. In 2001-2009, all 35 of patients received. After 2009, no patients received asparaginase.
Post-Induction Status and Survival
For the entire cohort, 4-year OS was 54.9% (95% CI, 46.1-62.9%) and 4-year RFS 47.8% (95% CI, 39.2-56.0%). 4-year OS for patients who underwent CR1 alloSCT was 42.7% (95% CI 29.2-55.6%), compared to 62.6% (95% CI, 51.2-72.1%) for those who received chemotherapy and imatinib alone (Figure 1a). There was a trend towards improved OS but overall no statistical difference (p=0.0661). RFS (Figure 1b) though, did not differ significantly between the two groups – 4-year RFS 43.1% (95% CI, 29.6-55.9%) and 50.9% (95% CI, 39.6-61.0%) (p=0.5272) with and without alloSCT, respectively.
The first protocol amendment was the removal of asparaginase after 2009. From 2015, another significant modification was a shift away from CR1 alloSCT. To assess how these changes may have influenced outcomes over time, we grouped patients into 3 cohorts according to induction treatment time period: 2001-2009, 2010-2015, and 2016-2019. There were 50, 58 and 31 patients, respectively. Unsurprisingly, patients who were treated in the most recent years, 2016-2019, demonstrated a significantly improved OS (HR 0.394 [95% CI, 0.180-0.864]), while patients treated in 2010-2015 were no significant different to patients treated in 2001-2009 (HR 0.873 [95% CI, 0.528-1.443]), p=0.0201 and p=0.5970, respectively (Figure 2). These results were not influenced by the length of follow up – median follow up 47.84 months (range, 5.06-73.35), 50.45 months (range, 3.65-141.83), and 35.56 months (range, 0.46-228.20), respectively. Although there appears to be a trend towards longer RFS in the more recent groups, this did not reach statistical significance – HR 0.571 (95% CI, 0.292-1.116, p=0.1012) and HR 1.008 (95% CI 0.623-1.630, p=0.9747), respectively.
When alloSCT in CR1 and year of induction were considered together, the 23 patients diagnosed between 2016 and 2019 who did not undergo CR1 alloSCT, had the best outcomes – 4-year OS 87.0% (95% CI, 64.8-95.6) (p=0.0143) and 4-year RFS 69.3% (95% CI, 46.1-84.0) (p=0.1888) (Figure 3). Patients who underwent induction in 2001-2009, whether they were (22 patients) or were not (28 patients) transplanted, had similarly unfavorable outcomes – 4-year OS 50.0% (95% CI, 28.2-58.4) versus 39.4% (95% CI, 21.1-57.3), and 4-year RFS 50.0% (95% CI, 28.2-58.4) versus 35.8% (95% CI, 18.3-53.7), respectively. Intermediate outcomes were observed in the 35 patients who commenced therapy in 2010-2015, and did not undergo consolidative alloSCT – 4-year OS 66.5% (95% CI, 47.6-79.9) and 4-year RFS 52.3% (95 CI, 34.3-67.5). These results underscore that omitting asparaginase did not have a detrimental impact on RFS. See Supplemental Table S1 for full analysis according to year of induction stratified by alloSCT in CR1.
Univariate and Multivariable Analyses
Age <60 and ≥60 years, sex, WBC at presentation, extramedullary disease and CNS involvement, prior cancer, asparaginase use, alloSCT as time varying variable, years of induction and BCR::ABL1 MRD results at 3/6 months and 9/12months (<3-log reduction and ≥3-log reduction in transcripts) were identified as important factors for univariate analysis (Table 2). Patients with ≥3-log reduction in BCR::ABL1 transcripts at 9/12 months had significantly longer OS and RFS than patients with <3-log reduction (HR 0.35 [95% CI, 0.16-0.79]; p=0.0115 and HR 0.38 [95% CI, 0.18-0.81]; p=0.0120), respectively. ≥3-log reduction in BCR::ABL1 transcripts at earlier timepoints (3/6 months) were not statistically significant for both OS and RFS. Interestingly, alloSCT as a time variable was demonstrated to result in statistically inferior OS and RFS (HR 2.19 [95% CI, 1.35-3.57]; p=0.0016) and (HR 1.73 [95% CI, 1.09-2.74]; p=0.0204), respectively. Asparaginase use was not significantly associated with inferior outcomes, though this could be due to small patient numbers.
In the multivariable model (Table 3), ≥3-log reduction in BCR::ABL1 transcripts at 9/12 months and alloSCT as a time variable retained statistical significance for OS and RFS. BCR::ABL1 transcript at 9/12 months had HR 0.37 [95% CI, 0.15-0.94]; p=0.0368) for OS and HR 0.36 [95% CI, 0.15-0.86]; p=0.0220) for RFS, respectively, while alloSCT as a time varying variable had HR 2.26 [95% CI, 1.18-4.33]; p=0.0139) for OS and HR 1.88 [95% CI, 1.01-3.48]; p=0.0452) for RFS, respectively. When examining the different cohorts according to induction year, there was no statistical difference among patients treated during any of these separate timepoints.
Discussion
Adult patients with newly diagnosed Ph+ B-ALL have long been treated with chemotherapy and TKI. Recent reports have demonstrated that frontline immunotherapy, in particular using blinatumomab, can lead to better outcomes (Foà et al, 2024; Jabbour et al, 2023). Nevertheless, chemotherapy backbones remain standard of care in most centres. We, and several other Canadian institutions, use pediatric-inspired multiagent chemotherapy protocols, in combination with imatinib. Though consolidative alloSCT continues to be performed routinely in many centres and is still recommended in some guidelines such as those by EBMT (Snowden et al, 2022), we have shifted away from CR1 alloSCT. The evolution of our practice – omission of asparaginase and alloSCT in CR1 – was based on excess toxicity and inferior outcomes observed in earlier years. This study examined if our protocol changes addressed these concerns.
The efficacy of our approach appears to be at least comparable to the literature. The EBMT Registry reported that patients with Ph+ B-ALL transplanted in CR1 between 2016 and 2020 had 3-year OS of 73% and 77% if MRD-positive or MRD-negative, respectively, pre-transplant (Bazarbachi et al, 2025). Our patients who received induction in 2016–2019, and did not undergo CR1 alloSCT, demonstrated a superior 4-year OS of 87.0% (95% CI, 64.8.1-95.6). In fact, the multivariable analysis here revealed that alloSCT in CR1 as a time dependent variable negatively affected both OS and RFS. This supports the notion that universal CR1 alloSCT is not indicated even when the TKI used is imatinib, in contrast to prior suggestions that CR1 alloSCT improves long term survival rates when first or second generation TKIs are used (Badar et al, 2023a; Ribera et al, 2018; Saleh et al, 2022).
Stratifying our patients by time period helped to address potentially confounding issues such as improvements in supportive care and facilitated the comparison with time-matched cohorts from the literature. Focussing first on our initial approach that incorporated asparaginase and alloSCT, only the UKALLXII protocol reported by Fielding et al (2014) used a pediatric-inspired multiagent chemotherapy protocol that also incorporated L-asparaginase. Other contemporaneous adult studies utilizing chemotherapy and imatinib largely used conventional adult-type protocols (Lee et al, 2005; Yanada et al, 2006; Bassan et al, 2010; Daver et al, 2015; Ribera et al, 2015). The former delivered more intensive chemotherapy followed by prolonged maintenance chemotherapy. The UKALLXII trial transplanted a substantial number (72%) of patients, resulting in 4-year OS and RFS of 38% and 50%, respectively (Fielding et al, 2014). Our patients induced in 2001-2009, of whom 44.0% received consolidative alloSCT, 4-year OS and RFS were 44.4% (95% CI, 30.2-57.7%) and 42.5% (28.4-55.8%), respectively.
Asparaginase toxicity in our cohort is also comparable to that observed in UKALLXII and later studies. A retrospective analysis of our patients when asparaginase was part of the protocol found that most toxicities occurred during induction or intensification phases, with asparaginase being held or discontinued largely due to liver function abnormalities (Thyagu et al, 2012). Due to toxicities, only six of 28 patients (21%) who entered the intensification phase received ≥80% of the intended cumulative dose of asparaginase (Thyagu et al, 2012). In this report, 4 of 5 patients who died during induction had received asparaginase. While this observation does not necessarily indicate causality, it is consistent with results of the UKALL14 trial that recruited patients between 2010 and 2012, which added pegylated-asparaginase and imatinib to their pediatric-inspired intensive induction regimen. Ph+ patients had >8-fold increase in induction deaths as compared to Ph- disease, which remained significant in the multivariable analysis (Patel et al, 2017). Consequently, pegylated-asparaginase was removed from the UKALL14 induction protocol for patients with Ph+ B-ALL (Patel et al, 2017).
Univariate and multivariable analyses here demonstrate that OS and RFS can be predicted more precisely by BCR::ABL1 MRD monitoring. Achieving ≥3-log reduction at 9 and 12 months correlated with significantly better OS (HR 0.351 [95% CI, 0.156-0.791], p=0.0115) and RFS (HR 0.381 [95% CI, 0.180-0.809], p=0.0120). 3-log reduction was chosen as the benchmark response because this was previously adopted by different groups including Ravandi et al (2013) and Chalandon et al (2015) as an appropriate molecular response criterion. Notably many of our patients have been observed to have longstanding detectable BCR::ABL1 transcripts, at levels ≥3-log reduction, with no signs of relapse. Ravandi et al (2013) furthermore found no difference in OS when comparing patients attaining MMR and CMR at 3, 6, 9 and 12 months, who were treated with hyperCVAD and imatinib or dasatinib, and no consolidative alloSCT. Ravandi et al (2013), however, did not report RFS that would have corroborated our findings.
The literature is clear that newer generation TKIs can achieve deeper molecular responses faster, with ponatinib having the highest 3-month CMR rate (Badar et al, 2023b; Short et al, 2016). A meta-analysis by Jabbour et al (2018) comparing one study using HyperCVAD and ponatinib with pooled results from 25 studies using first and second generation TKI/chemotherapy combinations, reported greater CMR and 3-year OS rates of 79% and 79%, versus 34%, and 50%, respectively, favoring ponatinib. Jabbour et al (2018) further suggested that using ponatinib may eliminate the need for consolidative alloSCT. Nevertheless, the results from this meta-analysis need to be interpreted with caution, due to significant heterogeneity among studies, and because the comparison was made to a single ponatinib study. Although ponatinib was associated with the highest 3-month CMR rate, Badar et al (2023b) did not find any difference in RFS among non-transplanted patients reaching CMR at 3 months with various TKIs, compared to those who did not achieve CMR, although OS was statistically superior in the former group. Short et al (2016) also demonstrated that while ponatinib and HyperCVAD without consolidative alloSCT induced deep molecular responses in a greater number of patients, outcomes did not differ if similarly deep responses were achieved using imatinib or dasatinib. Among their patients, 4-year OS and RFS for patients achieving CMR by 3 months were 66% and 63%, respectively (Short et al, 2016), which are inferior to results reported here, possibly reflecting different chemotherapy backbones.
Not achieving ≥3-log reduction at 9 and 12 months may indicate poor risk disease biology, as reflected by IKZF1 deletion alone or additional genetic aberrations including CDKN2A, CDKN2B, PAX5 or both (IKZFplus). Conventional chemotherapy and imatinib may be inadequate in such patients (Badar et al, 2023a; Foà et al, 2020; Martinelli et al, 2009). Alternative approaches for patients who do not achieve desirable MRD responses are needed, including pre-emptive or targeted (if ABL kinase domain mutations are found) switches to newer generation TKIs, use of targeted chemotherapy i.e., inotuzumab, and immunotherapy i.e., blinatumomab or chimeric antigen receptor T-cell therapy. If alloSCT is considered, it makes sense to deepen MRD prior to the procedure. In a Phase 2 study, the adverse disease biology of IKZF1/IKZF1plus could be overcome with blinatumomab consolidation post pre-phase glucocorticoids and dasatinib induction (Foà et al, 2020).
Our study’s main limitation is the bias inherent to retrospective analyses. By stratifying patients according to the time periods during which asparaginase and CR1 alloSCT were omitted from our protocol, and by analyzing the specific impact of these changes using univariate and multivariable analyses, potential selection bias and unknown confounders were minimized.
Conclusions
Our analysis is instructive in several regards. While the treatment paradigm is evolving with the incorporation of newer therapeutic agents at earlier timepoints, our data indicate that our pediatric-inspired multiagent chemotherapy backbone results in excellent outcomes, even if imatinib is used. Our data further support the notion that omission of asparaginase in Ph+ B-ALL is associated with better outcomes, and CR1 alloSCT is not obligatory, as long as MRD targets are met.
Supplementary Materials
The following supporting information can be downloaded at website of this paper posted on Preprints.org.
Author Contributions
Donna Zhe Sian Eng, Fatima Khadadah, Maria Agustina Perusini and Eshrak Al Shaibani performed the research. Marta Davidson, Guillaume Richard-Carpentier, Dawn Maze, Karen Yee, Aaron Schimmer, Vikas Gupta, Steven Chan, Dennis Dong Hwan Kim, Andre Schuh and Hassan Sibai designed the research study. Eshetu G. Atenafu wrote statistical sections, analysed the data and reviewed the manuscript for proper interpretation. Donna Zhe Sian Eng, Andre Schuh and Hassan Sibai wrote the paper.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was approved by research ethics board (REB) and waiver of consent was granted.
Informed Consent Statement
Waiver of consent was granted by the REB.
Data Availability Statement
Not applicable.
Conflicts of Interest
All other authors report no conflicts of interest.
References
- Badar, T.; Alkhateeb, H.; Aljurf, M.; Kharfan-Dabaja, M.A. Management of Philadelphia chromosome positive acute lymphoblastic leukemia in the current era. Curr Res Transl Med. 2023a, 71(2), 103392. [Google Scholar] [CrossRef]
- Badar, T.; Narra, R.; Mims, A.; Shallis, R.M.; De Camargo Correia, G.S.; Hunter, C.; Kota, V.K.; Desai, S.; Patel, A.A.; Duvall, A.S.; Palmisiano, N.; Curran, E.K.; Zulfa, O.; Advani, A.S.; Atallah, E.L.; Litzow, M.R. Achievement of Undetectable BCR::ABL1 (uBCR::ABL1) Is Predictive of Improved Survival in Philadelphia Chromosome Positive (Ph+ve) Acute Lymphoblastic Leukemia (ALL) Patients Not Receiving Allogeneic Stem Cell Transplantation. Blood 2023b, 142 Supplement 1, 1464. [Google Scholar] [CrossRef]
- Bassan, R.; Rossi, G.; Pogliani, E.M.; Di Bona, E.; Angelucci, E.; Cavattoni, I.; Lambertenghi-Deliliers, G.; Mannelli, F.; Levis, A.; Ciceri, F.; Mattei, D.; Borlenghi, E.; Terruzzi, E.; Borghero, C.; Romani, C.; Spinelli, O.; Tosi, M.; Oldani, E.; Intermesoli, T; Rambaldi, A. Chemotherapy-phased imatinib pulses improve long-term outcome of adult patients with Philadelphia chromosome-positive acute lymphoblastic leukemia: Northern Italy Leukemia Group protocol 09/00. J Clin Oncol 2010, 28(22), 3644–52. [Google Scholar] [CrossRef]
- Bazarbachi, A.; Labopin, M.; Dalle, I.A.; Yakoub-Agha, I.; Socié, G.; Schroeder, T.; Blaise, D.; Poiré, X.; Balsat, M.; Salmenniemi, U.; Kröger, N.; Kulagin, A.; Wagner-Drouet, E.M.; Wu, D.; Brissot, E.; Nagler, A.; Giebel, S.; Ciceri, F.; Mohty, M. Improved post-transplant outcomes since 2000 for Ph-positive acute lymphoblastic leukemia in first remission: A study from the EBMT Acute Leukemia Working Party. Hemasphere 2025, 9(4), e70117. [Google Scholar] [CrossRef] [PubMed]
- Chalandon, Y.; Thomas, X.; Hayette, S.; Cayuela, J.M.; Abbal, C.; Huguet, F.; Raffoux, E.; Leguay, T.; Rousselot, P.; Lepretre, S.; Escoffre-Barbe, M.; Maury, S.; Berthon, C.; Tavernier, E.; Lambert, J.F.; Lafage-Pochitaloff, M.; Lhéritier, V.; Chevret, S.; Ifrah, N.; Dombret, H.; Group for Research on Adult Acute Lymphoblastic Leukemia (GRAALL). Randomized study of reduced-intensity chemotherapy combined with imatinib in adults with Ph-positive acute lymphoblastic leukemia. Blood 2015, 125(24), 3711–9. [Google Scholar] [CrossRef]
- Daver, N.; Thomas, D.; Ravandi, F.; Cortes, J.; Garris, R.; Jabbour, E.; Garcia-Manero, G.; Borthakur, G.; Kadia, T.; Rytting, M.; Konopleva, M.; Kantarjian, H.; O’Brien, S. Final report of a phase II study of imatinib mesylate with hyper-CVAD for the front-line treatment of adult patients with Philadelphia chromosome-positive acute lymphoblastic leukemia. Haematologica 2015, 100(5), 653–61. [Google Scholar] [CrossRef] [PubMed]
- DeFilipp, Z.; Advani, A.S.; Bachanova, V.; Cassaday, R.D.; Deangelo, D.J.; Kebriaei, P.; Rowe, J.M.; Seftel, M.D.; Stock, W.; Tallman, M.S.; Fanning, S.; Inamoto, Y.; Kansagra, A.; Johnston, L.; Nagler, A.; Sauter, C.S.; Savani, B.N.; Perales, M.A.; Carpenter, P.A.; Larson, R.A.; Weisdorf, D. Hematopoietic Cell Transplantation in the Treatment of Adult Acute Lymphoblastic Leukemia: Updated 2019 Evidence-Based Review from the American Society for Transplantation and Cellular Therapy. Biol Blood Marrow Transplant 2019, 25(11), 2113–2123. [Google Scholar] [CrossRef]
- Fielding, A.K.; Rowe, J.M.; Buck, G.; Foroni, L.; Gerrard, G.; Litzow, M.R.; Lazarus, H.; Luger, S.M.; Marks, D.I.; McMillan, A.K.; Moorman, A.V.; Patel, B.; Paietta, E.; Tallman, M.S.; Goldstone, A.H. UKALLXII/ECOG2993: addition of imatinib to a standard treatment regimen enhances long-term outcomes in Philadelphia positive acute lymphoblastic leukemia. Blood 2014, 123(6), 843–50. [Google Scholar] [CrossRef]
- Foà, R.; Bassan, R.; Vitale, A.; Elia, L.; Piciocchi, A.; Puzzolo, M.C.; Canichella, M.; Viero, P.; Ferrara, F.; Lunghi, M.; Fabbiano, F.; Bonifacio, M.; Fracchiolla, N.; Di Bartolomeo, P.; Mancino, A.; De Propris, M.S.; Vignetti, M.; Guarini, A.; Rambaldi, A.; Chiaretti, S. GIMEMA Investigators. Dasatinib-Blinatumomab for Ph-Positive Acute Lymphoblastic Leukemia in Adults. N Engl J Med. 2020, 383(17), 1613–1623. [Google Scholar] [CrossRef]
- Foà, R.; Bassan, R.; Elia, L.; Piciocchi, A.; Soddu, S.; Messina, M.; Ferrara, F.; Lunghi, M.; Mulè, A.; Bonifacio, M.; Fracchiolla, N.; Salutari, P.; Fazi, P.; Guarini, A.; Rambaldi, A.; Chiaretti, S. Long-Term Results of the Dasatinib-Blinatumomab Protocol for Adult Philadelphia-Positive ALL. J Clin Oncol 2024, 42(8), 881–885. [Google Scholar] [CrossRef]
- Jabbour, E.; DerSarkissian, M.; Duh, M.S.; McCormick, N.; Cheng, W.Y.; McGarry, L.J.; Souroutzidis, A.; Huang, H.; O’Brien, S.; Ravandi, F.; Kantarjian, H.M. Efficacy of Ponatinib Versus Earlier Generation Tyrosine Kinase Inhibitors for Front-line Treatment of Newly Diagnosed Philadelphia-positive Acute Lymphoblastic Leukemia. Clin Lymphoma Myeloma Leuk 2018, 18(4), 257–265. [Google Scholar] [CrossRef] [PubMed]
- Jabbour, E.; Short, N.J.; Jain, N.; Huang, X.; Montalban-Bravo, G.; Banerjee, P.; Rezvani, K.; Jiang, X.; Kim, K.H.; Kanagal-Shamanna, R.; Khoury, J.D.; Patel, K.; Kadia, T.M.; Daver, N.; Chien, K.; Alvarado, Y.; Garcia-Manero, G.; Issa, G.C.; Haddad, F.G.; Kwari, M.; Thankachan, J.; Delumpa, R.; Macaron, W.; Garris, R.; Konopleva, M.; Ravandi, F.; Kantarjian, H. Ponatinib and blinatumomab for Philadelphia chromosome-positive acute lymphoblastic leukaemia: a US, single-centre, single-arm, phase 2 trial. Lancet Haematol 2023, 10(1), e24–e34. [Google Scholar] [CrossRef] [PubMed]
- Kanfar, S.S.; Chan, S.M.; Gupta, V.; Schimmer, A.D.; Schuh, A.C.; Sibai, H.; Yee, K.W.L.; Minden, M.D. Outcomes of Adult Philadelphia Positive Acute Lymphoblastic Leukemia Patients Treated with Pediatric Multi-Agent Chemotherapy and Imatinib and the Impact of Residual Disease Monitoring on Survival. Blood 2016, 128(22), 3976. [Google Scholar] [CrossRef]
- Lee, K.H.; Lee, J.H.; Choi, S.J.; Lee, J.H.; Seol, M.; Lee, Y.S.; Kim, W.K.; Lee, J.S.; Seo, E.J.; Jang, S.; Park, C.J.; Chi, H.S. Clinical effect of imatinib added to intensive combination chemotherapy for newly diagnosed Philadelphia chromosome-positive acute lymphoblastic leukemia. Leukemia 2005, 19(9), 1509–16. [Google Scholar] [CrossRef]
- Martell, M.P.; Atenafu, E.G.; Minden, M.D.; Schuh, A.C.; Yee, K.W.; Schimmer, A.D.; Gupta, V.; Brandwein, J.M. Treatment of elderly patients with acute lymphoblastic leukaemia using a paediatric-based protocol. Br J Haematol 2013, 163(4), 458–64. [Google Scholar] [CrossRef]
- Martinelli, G.; Iacobucci, I.; Storlazzi, C.T.; Vignetti, M.; Paoloni, F.; Cilloni, D.; Soverini, S.; Vitale, A.; Chiaretti, S.; Cimino, G.; Papayannidis, C.; Paolini, S.; Elia, L.; Fazi, P.; Meloni, G.; Amadori, S.; Saglio, G.; Pane, F.; Baccarani, M.; Foà, R. IKZF1 (Ikaros) deletions in BCR-ABL1-positive acute lymphoblastic leukemia are associated with short disease-free survival and high rate of cumulative incidence of relapse: a GIMEMA AL WP report. J Clin Oncol 2009, 27(31), 5202–7. [Google Scholar] [CrossRef]
- Patel, B.; Kirkwood, A.A.; Dey, A.; Marks, D.I.; McMillan, A.K.; Menne, T.F.; Micklewright, L.; Patrick, P.; Purnell, S.; Rowntree, C.J.; Smith, P.; Fielding, A.K. Pegylated-asparaginase during induction therapy for adult acute lymphoblastic leukaemia: toxicity data from the UKALL14 trial. Leukemia 2017, 31(1), 58–64. [Google Scholar] [CrossRef]
- Ravandi, F.; Jorgensen, J.L.; Thomas, D.A.; O’Brien, S.; Garris, R.; Faderl, S.; Huang, X.; Wen, S.; Burger, J.A.; Ferrajoli, A.; Kebriaei, P.; Champlin, R.E.; Estrov, Z.; Challagundla, P.; Wang, S.A.; Luthra, R.; Cortes, J.E.; Kantarjian, H.M. Detection of MRD may predict the outcome of patients with Philadelphia chromosome-positive ALL treated with tyrosine kinase inhibitors plus chemotherapy. Blood 2013, 122(7), 1214–21. [Google Scholar] [CrossRef]
- Ribera, J.M.; Ribera, J.; Genescà, E. The role of stem cell transplantation in the management of Philadelphia chromosome-positive acute lymphoblastic leukemia. Ther Adv Hematol 2018, 9(12), 357–368. [Google Scholar] [CrossRef]
- Saleh, K.; Fernandez, A.; Pasquier, F. Treatment of Philadelphia Chromosome-Positive Acute Lymphoblastic Leukemia in Adults. Cancers (Basel) 2022, 14(7), 1805. [Google Scholar] [CrossRef]
- Shah, B.; Mattison, R.J.; Abboud, R.; Abdelmessieh, P.; Aldoss, I.; Burke, P.W.; DeAngelo, D.J.; Dinner, S.; Fathi, A.T.; Gauthier, J.; Haddadin, M.; Jain, N.; Jonas, B.; Kirby, S.; Liedtke, M.; Litzow, M.; Logan, A.; Long, M.; Luger, S.; Mangan, J.K.; Massaro, S.; May, W.; Oluwole, O.; Park, J.; Przespolewski, A.; Rangaraju, S.; Saygin, C.; Schwartz, M.; Shami, P.; Tomlinson, B.; Webster, J.; Awotiwon, A.; Stehman, K. Acute Lymphoblastic Leukemia, Version 2.2024, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw 2024, 22(8), 563–576. [Google Scholar] [CrossRef] [PubMed]
- Short, N.J.; Jabbour, E.; Sasaki, K.; Patel, K.; O’Brien, S.M.; Cortes, J.E.; Garris, R.; Issa, G.C.; Garcia-Manero, G.; Luthra, R.; Thomas, D.; Kantarjian, H.; Ravandi, F. Impact of complete molecular response on survival in patients with Philadelphia chromosome-positive acute lymphoblastic leukemia. Blood 2016, 128(4), 504–7. [Google Scholar] [CrossRef]
- Snowden, J.A.; Sánchez-Ortega, I.; Corbacioglu, S.; Basak, G.W.; Chabannon, C.; de la Camara, R.; Dolstra, H.; Duarte, R.F.; Glass, B.; Greco, R.; Lankester, A.C.; Mohty, M.; Neven, B.; de Latour, R.P.; Pedrazzoli, P.; Peric, Z.; Yakoub-Agha, I.; Sureda, A.; Kröger, N.; European Society for Blood and Marrow Transplantation (EBMT). Indications for haematopoietic cell transplantation for haematological diseases, solid tumours and immune disorders: current practice in Europe, 2022. Bone Marrow Transplant 2022, 57(8), 1217–1239. [Google Scholar] [CrossRef]
- Thyagu, S.; Minden, M.D.; Gupta, V.; Yee, K.W.; Schimmer, A.D.; Schuh, A.C.; Lipton, J.H.; Messner, H.A.; Xu, W.; Brandwein, J.M. Treatment of Philadelphia chromosome-positive acute lymphoblastic leukaemia with imatinib combined with a paediatric-based protocol. Br J Haematol 2012, 158(4), 506–14. [Google Scholar] [CrossRef] [PubMed]
- Yanada, M.; Takeuchi, J.; Sugiura, I.; Akiyama, H.; Usui, N.; Yagasaki, F.; Kobayashi, T.; Ueda, Y.; Takeuchi, M.; Miyawaki, S.; Maruta, A.; Emi, N.; Miyazaki, Y.; Ohtake, S.; Jinnai, I.; Matsuo, K.; Naoe, T.; Ohno, R. Japan Adult Leukemia Study Group. High complete remission rate and promising outcome by combination of imatinib and chemotherapy for newly diagnosed BCR-ABL-positive acute lymphoblastic leukemia: a phase II study by the Japan Adult Leukemia Study Group. J Clin Oncol 2006, 24(3), 460–6. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
(a). Overall Survival stratified by alloHSCT in CR1, (b). RFS stratified by alloHSCT in CR1.
Figure 1.
(a). Overall Survival stratified by alloHSCT in CR1, (b). RFS stratified by alloHSCT in CR1.
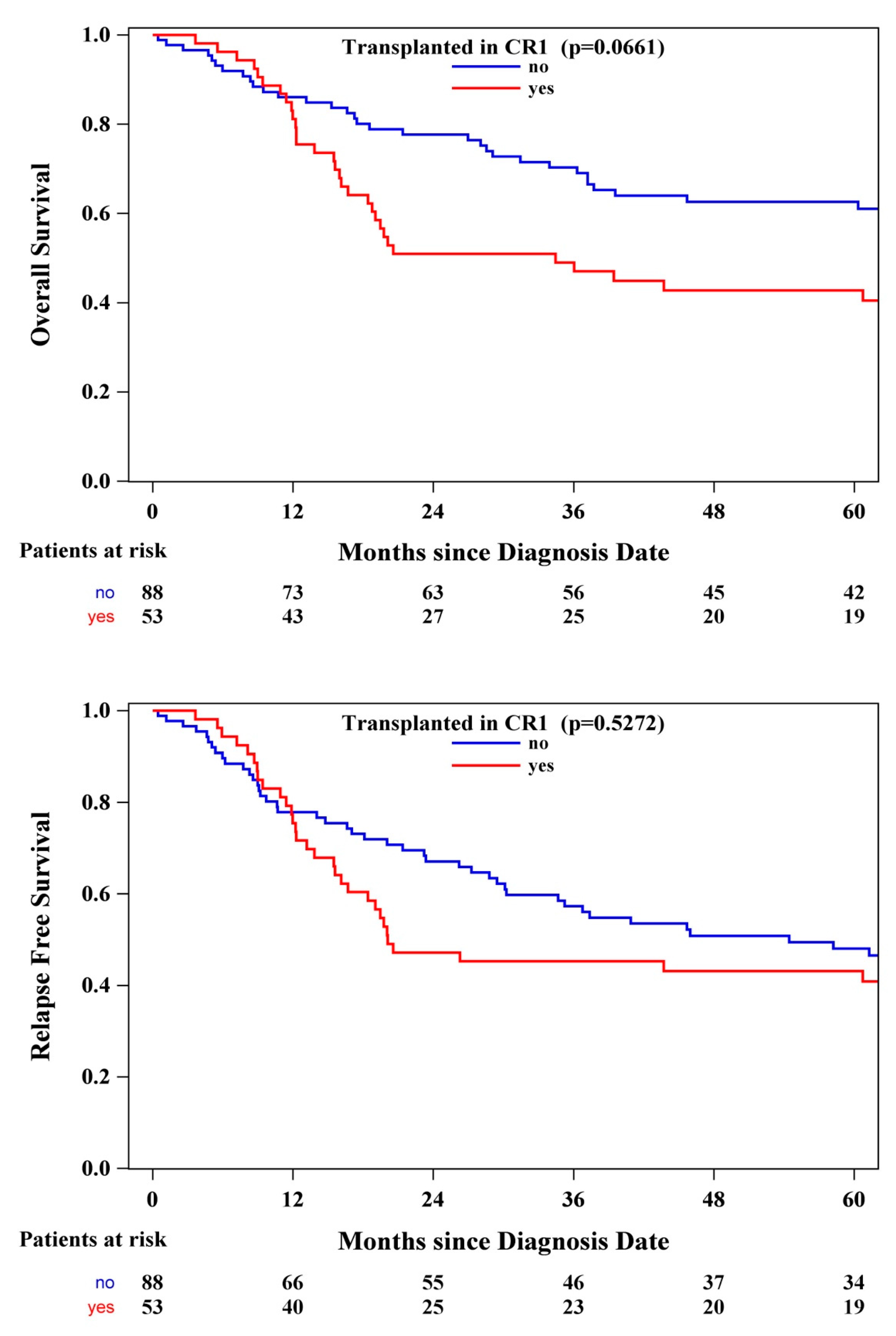
Figure 2.
(a). Overall Survival according to Year of Induction, (b). Relapse Free Survival according to Year of Induction.
Figure 2.
(a). Overall Survival according to Year of Induction, (b). Relapse Free Survival according to Year of Induction.
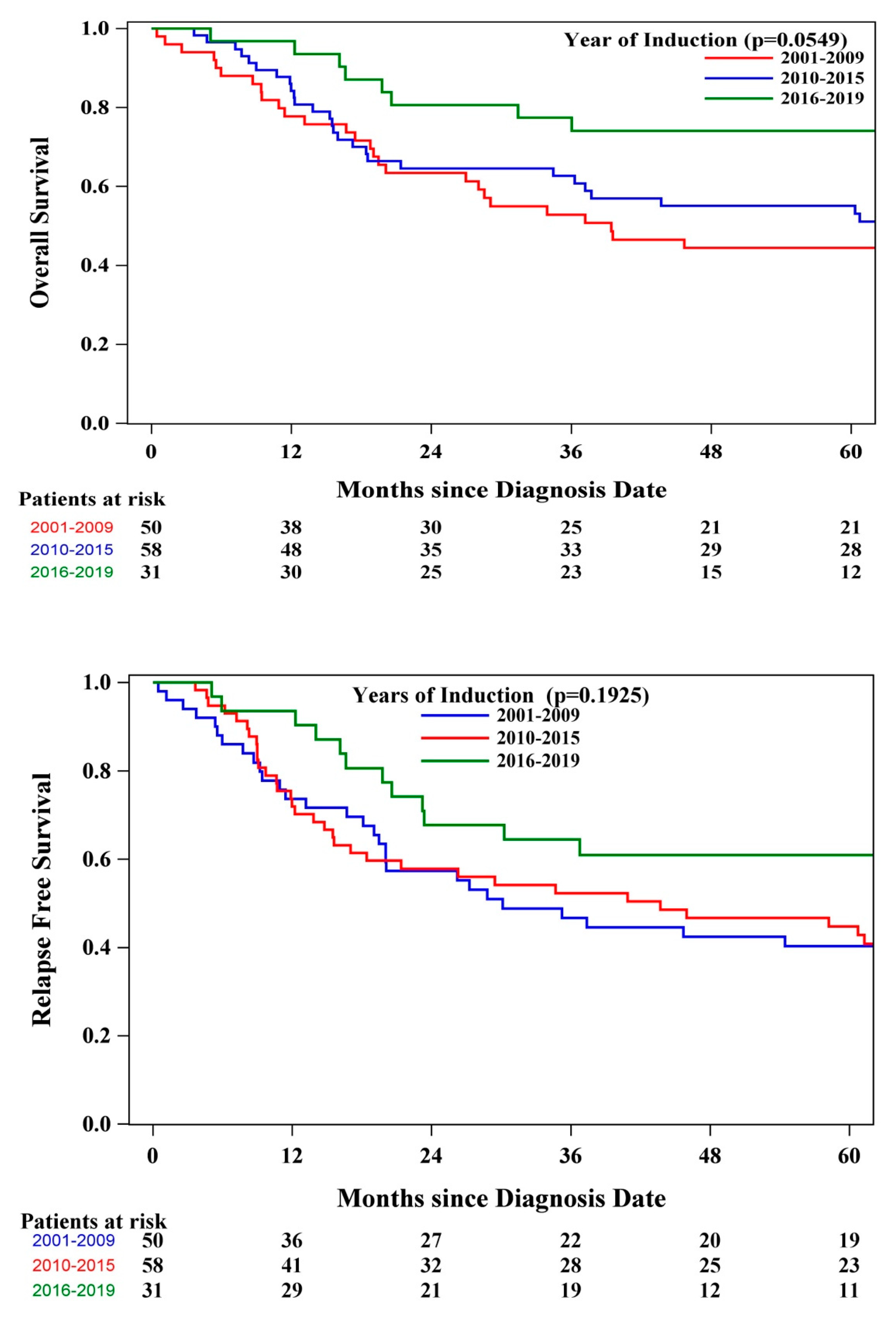
Figure 3.
(a). Overall Survival according to Year of Induction and alloSCT in CR1, (b). RFS according to Year of Induction and alloSCT in CR1.
Figure 3.
(a). Overall Survival according to Year of Induction and alloSCT in CR1, (b). RFS according to Year of Induction and alloSCT in CR1.
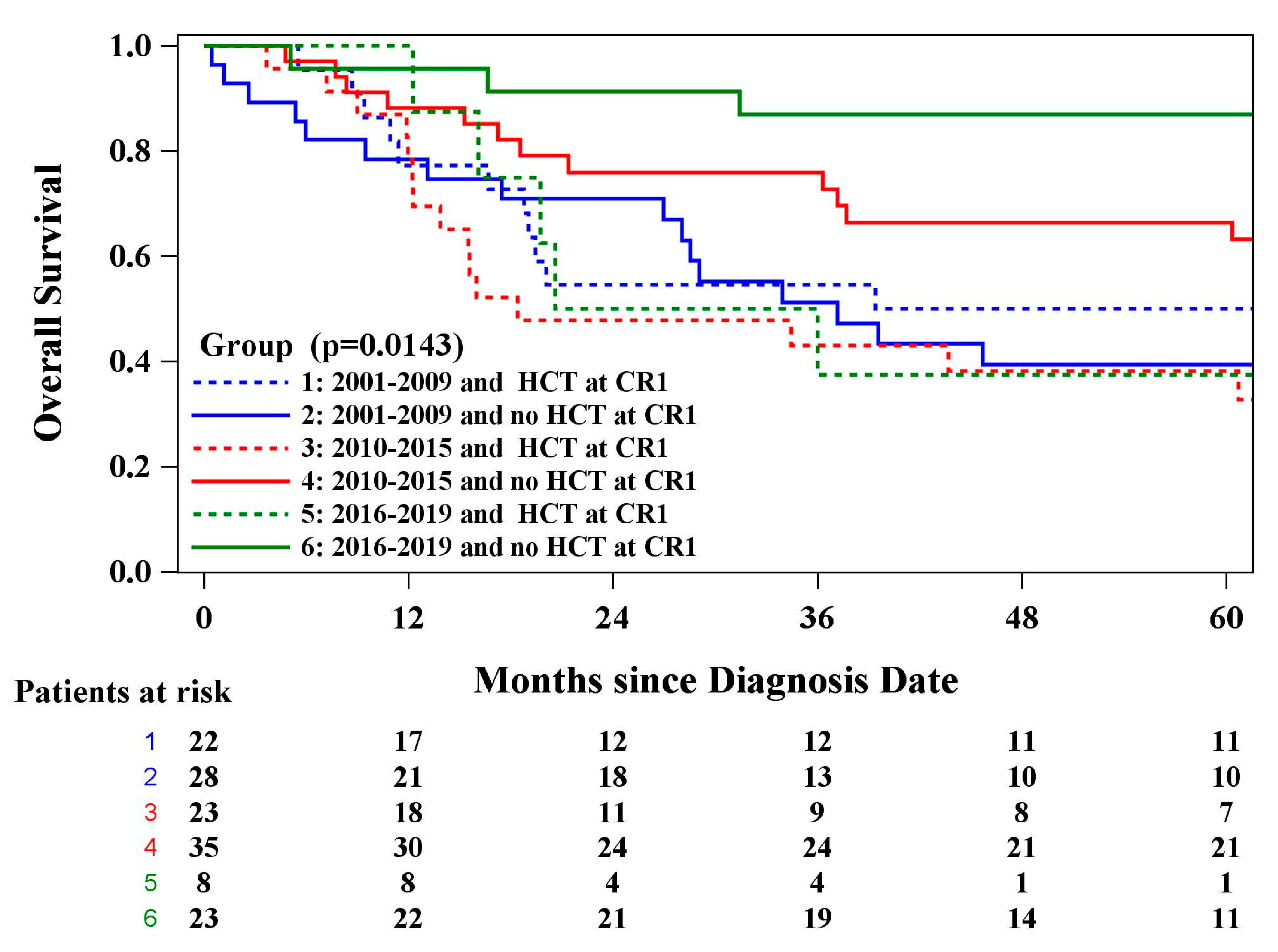

Table 1.
Patient characteristics and treatment regimens.
| Parameter | All Patients N=141 |
|---|---|
| Median age, year (range) | 50.00 (18.0-79.1) |
| Age ≥60, n (%) | 39 (27.66) |
| Male, n (%) | 77 (54.61) |
| Female, n (%) | 64 (45.39) |
| Median WBC count, x109/L (range) | 19.20 (0.80-272.0) |
| Extramedullary disease, n (%) | 14 (9.93) |
| CNS involvement at diagnosis, n (%) | 15 (10.64) |
| Prior cancer history, n (%) | 13 (9.63) |
| Chemotherapy, n (%) | |
| Pediatric-inspired multiagent protocol | 140 (99.29) |
| Other | 1 (0.71) |
| Asparaginase, n (%) | 35 (24.82) |
| TKI, n (%) | |
| Imatinib | 138 (98.57) |
| Dasatinib | 2 (1.43) |
| Transplant in CR1, n (%) | 53 (37.59) |
Table 2.
Results from Univariate Analysis.
|
Variable |
OS | RFS | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-value | HR | 95% CI | p-value | |
| Age (>60 years) | 0.91 | (0.54, 1.54) | 0.7255 | 1.06 | (0.65, 1.72) | 0.8198 |
| Sex (female) | 1.52 | (0.95, 2.43) | 0.0824 | 1.42 | (0.92, 2.20) | 0.1162 |
| WBC (>30 x109/L) | 1.27 | (0.78, 2.10) | 0.3389 | 1.24 | (0.78, 1.97 | 0.3696 |
| Extramedullary disease + CNS involvement (present) | 1.20 | (0.67, 2.17) | 0.5434 | 0.95 | (0.53, 1.70) | 0.8690 |
| Prior cancer (present) | 1.51 | (0.72, 3.18) | 0.2720 | 1.69 | (0.84, 3.41) | 0.1384 |
| Asparaginase (yes) | 1.10 | (0.65, 1.87) | 0.7245 | 0.99 | (0.60, 1.65) | 0.9824 |
| Year of induction (ref=2001-2009) |
0.87 |
(0.53, 1.44) |
0.0651 0.5970 |
1.01 |
(0.62, 1.63) |
0.2008 0.9747 |
| 2010-2015 | ||||||
| 2016-2019 | 0.39 | (0.18, 0.86) | 0.0201 | 0.57 | (0.29, 1.12) | 0.1012 |
| HCTCR1t (time varying) | 2.19 | (1.35, 3.57) | 0.0016 | 1.73 | (1.09, 2.74) | 0.0204 |
| BCR::ABL1 3/6 months (>3-log reduction) | 1.09 | (0.51, 2.32) | 0.8329 | 1.02 | (0.51, 2.03) | 0.9557 |
| BCR::ABL1 9/12 months (>3-log reduction) | 0.35 | (0.16, 0.79) | 0.0115 | 0.38 | (0.18, 0.81) | 0.0120 |
Table 3.
Results from Multivariable Analysis.
|
Variable |
OS | RFS | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-value | HR | 95% CI | p-value | |
| Sex (female) | 1.66 | (0.90, 3.06) | 0.1016 | 1.53 | (0.87, 2.69) | 0.1371 |
| Prior cancer (present) | 1.35 | (0.52, 3.56) | 0.5385 | 1.56 | (0.65, 3.74) | 0.3215 |
| BCR::ABL1 9/12 months (>3-log reduction) | 0.37 | (0.15, 0.94) | 0.0368 | 0.36 | (0.15, 0.86) | 0.0220 |
| Year of induction (ref=2001-2009) | 0.2876 | 0.2870 | ||||
| 2010-2015 | 1.24 | (0.63, 2.45) | 0.5350 | 1.39 | (0.74, 2.62) | 0.3021 |
| 2016-2019 | 0.47 | (0.13, 1.73) | 0.2583 | 0.71 | (0.25, 2.03) | 0.5211 |
| HCTCR1t (time varying) | 2.26 | (1.18, 4.33) | 0.0139 | 1.88 | (1.01, 3.48) | 0.0452 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



