Submitted:
04 January 2026
Posted:
07 January 2026
You are already at the latest version
Abstract
Background: Neuropathic pain is increasingly recognized as a significant con-tributor to chronic pain and reduced quality of life in patients with rheumatoid arthritis (RA). However, its clinical correlates and relationship with disease ac-tivity and patient-reported outcomes in RA remain incompletely understood.
Objective: To evaluate the prevalence of likely neuropathic pain features in RA patients and to investigate their associations with disease activity, pain intensity, fatigue, sleep quality, and health-related quality of life.
Methods: In this cross-sectional study, 160 RA patients were enrolled. Neuro-pathic pain features were assessed using the PainDETECT questionnaire. Dis-ease activity was evaluated with the Disease Activity Score in 28 joints (DAS28). Pain intensity, fatigue, sleep quality, and health-related quality of life were as-sessed using the visual analog scale (VAS), Functional Assessment of Chronic Illness Therapy–Fatigue (FACIT-F), Pittsburgh Sleep Quality Index (PSQI), and Short Form-36 (SF-36), respectively. Group comparisons, correlation analyses, and multivariate linear regression models were performed to identify factors associated with neuropathic pain.
Results: Likely neuropathic pain was identified in 22.5% of patients. Patients with neuropathic pain had significantly higher pain intensity, greater fatigue, poorer sleep quality, and lower SF-36 scores across all domains compared with patients without neuropathic pain (all p < 0.001). Although DAS28 scores were higher in patients with neuropathic pain, PainDETECT scores correlated more strongly with VAS pain in-tensity (ρ = 0.679, p < 0.001) than with DAS28 (ρ = 0.536, p < 0.001). PainDETECT scores were negative-ly correlated with FACIT-F (ρ = −0.512, p < 0.001) and multiple SF-36 domains, indicating substantial quality-of-life impairment. In multivariate regression analysis, only pain intensity independently predicted neuropathic pain features.
Conclusions: Neuropathic pain is common in RA and is more closely associated with pain intensity and patient-reported outcomes than with inflammatory activ-ity alone. Routine assessment of neuropathic pain features may facilitate more personalized and effective pain management strategies in RA, highlighting the clinical relevance of targeting neuropathic mechanisms alongside inflammation.
Keywords:
rheumatoid arthritis
; neuropathic pain
; PainDETECT
; pain intensity
; quality of life
; disease activity
1. Introduction
Rheumatoid arthritis (RA) is a chronic systemic autoimmune disease characterized by persistent synovial inflammation, leading to progressive joint damage, functional disability, and reduced quality of life [1,2]. Pain is one of the most common and disabling symptoms in RA and profoundly affects physical functioning, psychological well-being, and social participation [1,3]. Traditionally, RA-related pain has been attributed primarily to synovial inflammation; however, accumulating evidence suggests that RA pain involves multilocal mechanisms, with both nociceptive and non-nociceptive pain processes contributing to symptom persistence [2,4,5]. Notably, a substantial proportion of patients continue to experience moderate to severe pain despite having low disease activity or being in clinical remission, indicating that mechanisms beyond inflammation play a critical role in the maintenance of chronic pain in RA [1,2,6].
Chronic inflammatory input from affected joints can induce peripheral sensitization and, over time, promote central sensitization, resulting in amplified pain perception, allodynia, and hyperalgesia, which may persist independently of active inflammation [1,7]. Peripheral and central sensitization processes lower pain thresholds and enhance nociceptive signaling, contributing to chronic pain in RA even when synovial inflammation is clinically controlled [1,7]. Neuropathic-like pain features have been reported in a substantial subset of patients with RA; screening studies using tools such as the painDETECT questionnaire have found that roughly 15–25% of RA patients exhibit symptoms suggestive of neuropathic pain components [8]. Neuroimaging and quantitative sensory testing investigations demonstrate alterations in central pain processing pathways in RA, including widespread hyperalgesia and changes in pain thresholds consistent with central sensitization [9,10]. Proinflammatory cytokines, including tumor necrosis factor-α (TNF-α), interleukin-1β (IL-1β), and interleukin-6 (IL-6), modulate nociceptive transmission by increasing peripheral nociceptor excitability and disrupting central pain inhibitory controls, acting directly on sensory neurons as well as through immune-neural interactions [1,7]. Notably, Janus kinase (JAK) inhibitors exert rapid analgesic effects that often precede measurable reductions in traditional inflammatory markers, and preclinical and clinical evidence suggests these agents may diminish both inflammatory and neuropathic-like pain by modulating cytokine signaling and neural sensitization pathways [11,12]. Collectively, these findings underscore RA pain as a complex, multidimensional phenomenon arising from the interplay of inflammatory, neuropathic-like, and centrally mediated mechanisms that extend beyond synovial inflammation alone [11,17].
In this context, neuropathic pain—defined as pain arising from a lesion or dysfunction of the somatosensory nervous system—is commonly characterized by burning, tingling, electric shock–like, or shooting sensations [13]. Recent evidence indicates that a substantial proportion of patients with rheumatoid arthritis (RA) experience neuropathic-like pain features in addition to inflammatory nociceptive pain [8]. These pain mechanisms are clinically relevant, as they are associated with greater pain intensity, increased fatigue, sleep disturbances, mood impairment, and markedly reduced quality of life [4,15]. Importantly, neuropathic pain in RA may persist despite adequate control of synovial inflammation and often shows limited responsiveness to conventional anti-inflammatory or disease-modifying therapies [13]. This underscores the clinical importance of identifying neuropathic pain components in RA and supports the adoption of mechanism-based, multidimensional treatment strategies targeting both inflammatory and non-inflammatory pain pathways to optimize patient outcomes [13,16].
Despite increasing recognition of neuropathic pain in rheumatoid arthritis (RA), the complex interrelationships among neuropathic pain features, inflammatory activity, and patient-reported outcomes remain incompletely understood [1,16]. While some studies have reported associations between systemic inflammatory markers and neuropathic pain [17], others emphasize the predominant role of central sensitization and non-inflammatory mechanisms in sustaining pain, even during periods of low disease activity or clinical remission [18]. Furthermore, prior research has frequently examined these factors in isolation or relied on limited assessment tools, resulting in an incomplete understanding of the multidimensional impact of neuropathic pain on patients’ daily functioning [18]. Consequently, a comprehensive approach integrating clinical, biochemical, and patient-reported measures—including fatigue, sleep quality, and health-related quality of life—is needed to clarify these complex interactions and to inform the development of targeted, mechanism-based interventions aimed at improving pain control and overall well-being in RA [17,18].
The aim of this study was to determine the prevalence and clinical characteristics of neuropathic pain in patients with rheumatoid arthritis (RA) and to investigate its associations with pain intensity, disease activity, inflammatory markers, fatigue, sleep quality, and health-related quality of life. We hypothesized that neuropathic pain represents a substantial and distinct contributor to the overall disease burden in RA, partially independent of systemic inflammatory activity, and that its presence is associated with worse patient-reported outcomes. By integrating multidimensional assessments—including the PainDETECT questionnaire, Visual Analogue Scale (VAS), 36-Item Short Form Health Survey (SF-36), Functional Assessment of Chronic Illness Therapy–Fatigue (FACIT-F), and Pittsburgh Sleep Quality Index (PSQI)—this study aimed to provide a comprehensive characterization of neuropathic pain in RA and to support more targeted, mechanism-based pain management strategies.
2. Materials and Methods
Study Design and Ethics
This cross-sectional study was conducted at Dicle University. The study protocol was approved by the Dicle University Ethics Committee (Approval No. 2025-355), and all participants provided written informed consent in accordance with the principles of the Declaration of Helsinki. The primary objective of the study was to determine the prevalence and clinical characteristics of neuropathic pain in patients with rheumatoid arthritis (RA) and to investigate its associations with disease activity, inflammatory markers, fatigue, sleep quality, and health-related quality of life.
Study Population
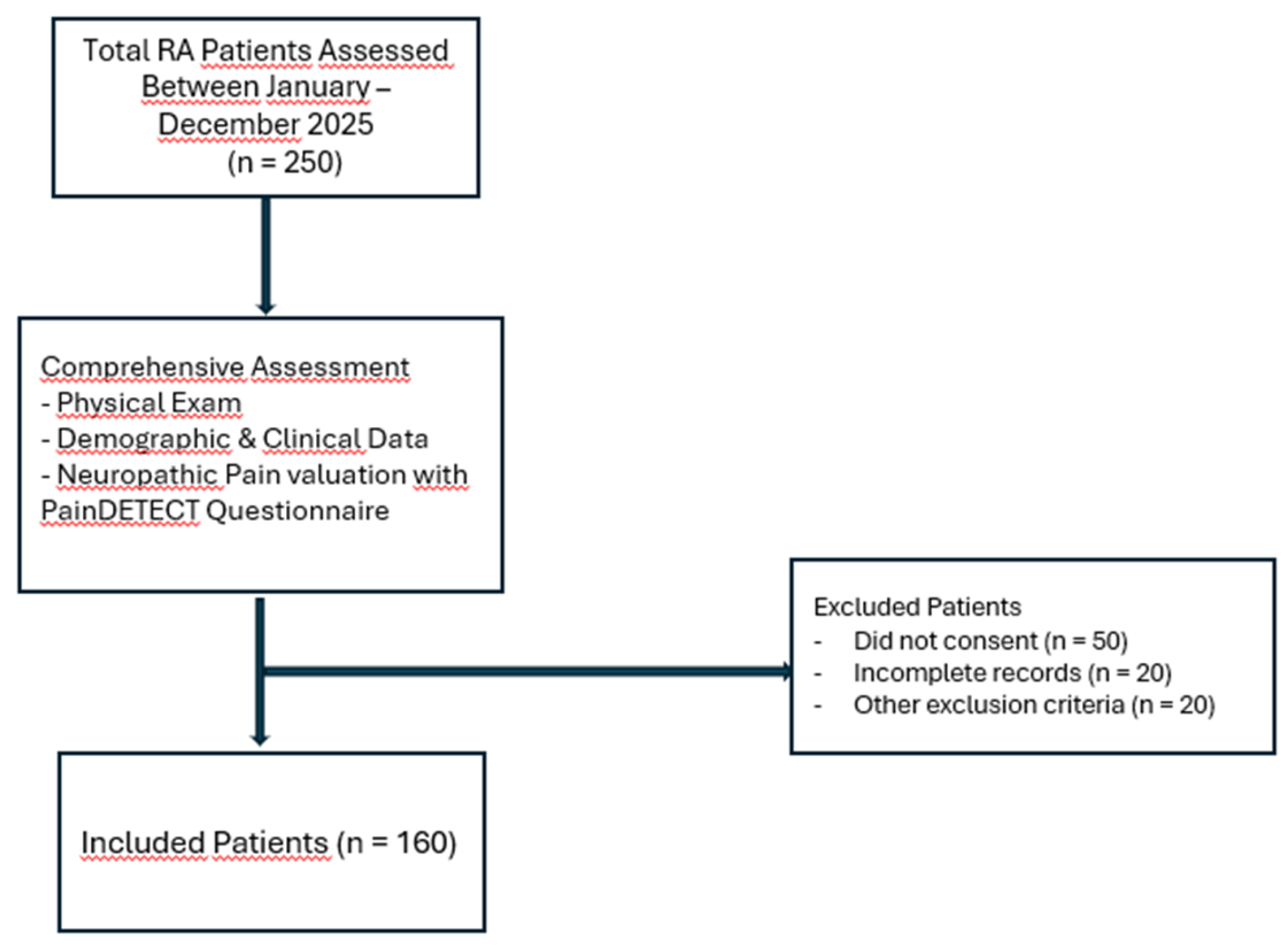
A total of 160 patients diagnosed with rheumatoid arthritis (RA) according to the 2010 American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) classification criteria were included in the final analysis. Between January and December 2025, a total of 250 consecutive RA patients were assessed at the Rheumatology Outpatient Clinic of Dicle University. All patients underwent an initial comprehensive clinical evaluation.
Inclusion criteria were age ≥18 years, a confirmed diagnosis of rheumatoid arthritis according to the 2010 ACR/EULAR classification criteria, ability to complete clinical assessments and self-reported questionnaires, and provision of written informed consent. Exclusion criteria included diabetes mellitus, peripheral neuropathy, fibromyalgia, chronic kidney or liver disease, malignancy, psychiatric disorders, and the use of medications known to affect the nervous system (e.g., antidepressants or anticonvulsants).
Of the initially assessed patients, 90 were excluded due to lack of informed consent (n = 50), incomplete clinical records (n = 20), or other exclusion criteria (n = 20). Consequently, 160 patients were eligible and included in the study. Disease duration and current antirheumatic treatments, including conventional synthetic disease-modifying antirheumatic drugs (csDMARDs), biologic agents, and glucocorticoids, were recorded at the time of assessment.
All participants underwent a comprehensive clinical evaluation and completed standardized questionnaires under the supervision of trained researchers. The study population selection and assessment process are illustrated in Figure 1.
Clinical and Laboratory Assessment
Disease activity was assessed using the Disease Activity Score in 28 joints (DAS28), which incorporates tender and swollen joint counts, erythrocyte sedimentation rate (ESR), and the patient’s global assessment of disease activity measured on a visual analogue scale (VAS). Pain intensity was evaluated using a 100-mm VAS, with higher scores indicating greater pain severity.
Blood samples were obtained after overnight fasting to measure C-reactive protein (CRP) and ESR using standardized laboratory methods. Demographic and clinical characteristics, including age, sex, body mass index (BMI), and disease duration, were recorded for all patients at the time of assessment.
Patient-Reported Outcome Measures
Neuropathic pain symptoms were assessed using the PainDETECT questionnaire, a validated self-reported instrument designed to identify neuropathic pain components in chronic pain conditions. Total scores range from −1 to 38, with scores ≤12 indicating unlikely neuropathic pain, 13–18 suggesting possible neuropathic pain, and ≥19 indicating likely neuropathic pain [19].
Fatigue was evaluated using the Functional Assessment of Chronic Illness Therapy–Fatigue (FACIT-F) scale, with lower scores indicating greater fatigue severity [20]. Sleep quality was assessed using the Pittsburgh Sleep Quality Index (PSQI), which measures subjective sleep quality and disturbances over the past month, with higher scores indicating poorer sleep [21].
Health-related quality of life was measured using the 36-Item Short Form Health Survey (SF-36), which includes eight subscales representing physical and mental health domains [22].
All questionnaires have validated Turkish versions and were completed under the supervision of trained researchers to ensure accuracy and consistency.
Statistical Analysis
All statistical analyses were performed using IBM SPSS Statistics for Windows, version 27 (IBM Corp., Armonk, NY, USA). Continuous variables were assessed for normality using the Kolmogorov–Smirnov and Shapiro–Wilk tests. Normally distributed variables are presented as mean ± standard deviation (SD), whereas non-normally distributed variables are reported as median (interquartile range, IQR). Categorical variables are expressed as frequencies and percentages.
Comparisons between patients with and without neuropathic pain features were performed using independent-samples t-tests for normally distributed continuous variables and Mann–Whitney U tests for non-normally distributed variables. Chi-square tests or Fisher’s exact tests (where appropriate) were used to compare categorical variables. Effect sizes (Cohen’s d for t-tests and r for nonparametric tests) were calculated to quantify the magnitude of differences.
Correlations between PainDETECT scores and continuous clinical, laboratory, and patient-reported outcome measures were assessed using Spearman’s rank correlation coefficients, given the non-normal distribution of some variables. Correlation strength was interpreted as very weak (ρ = 0.00–0.19), weak (0.20–0.39), moderate (0.40–0.59), strong (0.60–0.79), or very strong (0.80–1.0).
To identify independent predictors of neuropathic pain, a multiple linear regression model was constructed with PainDETECT score as the dependent variable. Candidate predictors included demographic factors (age, sex, BMI), disease-related variables (disease duration, DAS28, CRP, ESR), and patient-reported outcomes (VAS pain, FACIT-F, PSQI, SF-36 subscales). Multicollinearity was assessed using variance inflation factors (VIF), with VIF > 5 indicating potential collinearity. Model assumptions, including linearity, normality of residuals, homoscedasticity, and independence of errors, were evaluated using residual plots and the Durbin–Watson statistic.
All statistical tests were two-tailed, and p-values < 0.05 were considered statistically significant. Where appropriate, 95% confidence intervals (CIs) are reported. A post hoc power analysis confirmed that the study had sufficient power to detect moderate effect sizes.
3. Results
A total of 160 patients with rheumatoid arthritis (RA) were included in the study. The mean age was 51.41 ± 13.48 years, and the majority were female (81.8%). The mean body mass index (BMI) was 27.56 ± 5.20 kg/m². Regarding education, 30.6% were illiterate, 34.4% had primary education, 8.1% middle school, 16.9% high school, and 10% university. Most patients were married (76.9%), 11.3% were single, and 11.9% were widowed. In terms of smoking status, 75.6% were non-smokers. Median disease duration was 8.00 years (IQR 0.75–40.00). Neuropathic pain, evaluated using the PainDETECT questionnaire, revealed a mean score of 6.41 ± 2.45.
Regarding treatment, 31.2% of patients were receiving csDMARDs, 28.1% TNF inhibitors, 25% JAK inhibitors, 3.1% rituximab, 7.5% tocilizumab, and 5% abatacept. Disease activity measured by DAS28 averaged 2.73, with 45% of patients in remission (<2.6), 20% with low disease activity (2.6–3.2), 28.1% moderate (3.2–5.1), and 6.9% high (>5.1). Regarding pain phenotype, 22.5% were classified as having likely neuropathic pain, 15% had unclear pain type, and 62.5% were likely non-neuropathic (Table 1).
Patients with likely neuropathic pain had significantly higher pain intensity (VAS: 60.89 ± 17.94 vs. 38.73 ± 18.58), greater fatigue (FACIT-F: 23.13 ± 11.89 vs. 38.19 ± 12.61), and poorer sleep quality (PSQI: 10.80 ± 3.35 vs. 7.08 ± 3.79) compared with patients without neuropathic pain (all p < 0.001). Disease activity (DAS28: 2.87 ± 0.68 vs. 2.26 ± 0.86) and tender joint count were also higher in the neuropathic pain group. Health-related quality of life was markedly impaired, with lower scores across all SF-36 domains, including PF, RP, RE, VT, SF, MH, BP, and GH (all p < 0.001). No significant differences were observed for age, BMI, CRP, ESR, or swollen joint count, suggesting that neuropathic pain may be partially independent of systemic inflammation and demographic factors. Table 2 presents the comparison of clinical, laboratory, fatigue, sleep quality, and quality of life parameters between RA patients with and without neuropathic pain.
The relationship between neuropathic pain status and sex was examined, and a statistically significant association was observed (Chi-square test, p < 0.001). In contrast, no significant association was found between smoking status and neuropathic pain (p = 0.593). Similarly, no statistically significant relationship was observed between treatment groups (JAK inhibitors, TNF inhibitors, and DMARDs) and neuropathic pain status (Pearson Chi-square test, p = 0.707) (Table 3).
Spearman correlation analyses (Table 4, Figure 2) demonstrated significant associations between PainDETECT scores and both clinical and patient-reported outcome measures. PainDETECT scores were strongly positively correlated with VAS pain intensity (ρ = 0.650, p < 0.01) and DAS28 (ρ = 0.527, p < 0.01), while weaker positive correlations were observed with inflammatory markers ESR (ρ = 0.235, p < 0.01) and CRP (ρ = 0.150, p < 0.01). Fatigue, as assessed by FACIT-F, was negatively correlated with PainDETECT scores (ρ = −0.456, p < 0.01), indicating that higher neuropathic pain was associated with greater fatigue. Similarly, poorer sleep quality was associated with higher PainDETECT scores (PSQI: ρ = 0.318, p < 0.01).
Health-related quality of life, measured by SF-36 subscales, showed significant negative correlations with PainDETECT scores, particularly for Bodily Pain (ρ = −0.689), Social Functioning (ρ = −0.703), Role Physical (ρ = −0.706), Vitality (ρ = −0.634), and Physical Functioning (ρ = −0.690) (all p < 0.01). These findings indicate that neuropathic pain substantially impairs physical, emotional, and social functioning in patients with rheumatoid arthritis (Table 4, Figure 2).
A multiple linear regression analysis was performed to identify independent predictors of PainDETECT scores within the RA cohort. The model was statistically significant (F(16, 177) = 19.77; p < 0.001) and explained 64% of the variance in PainDETECT scores (R² = 0.64). Among the candidate predictors—including age, BMI, CRP, ESR, DAS28, FACIT-F, VAS, and SF-36 subscales—only pain intensity (VAS) remained an independent predictor (β = −0.039; p = 0.006). Collinearity diagnostics indicated moderate to high multicollinearity among SF-36 subscales; however, residual analyses confirmed an adequate model fit (Table 5).
4. Discussion
The primary finding of the present study is that perceived pain intensity (VAS) serves as the sole independent predictor of neuropathic pain in patients with rheumatoid arthritis, distinct from systemic inflammation markers (CRP, ESR) or disease activity scores (DAS28) [23]. This dissociation suggests that central sensitization and non-inflammatory mechanisms may contribute more significantly to the RA pain experience than previously appreciated [24]. Furthermore, our multidimensional assessment reveals that patients with neuropathic pain features carry a heavier burden of disease, characterized by exacerbated fatigue, poorer sleep quality, and significantly impaired health-related quality of life [25]. These results underscore the limitations of solely targeting inflammatory pathways and highlight the necessity of addressing central pain mechanisms to improve functional outcomes.
The prevalence of neuropathic pain components observed in our cohort 22.5% is consistent with the growing body of evidence suggesting that 20–40% of RA patients experience neuropathic-like symptoms, even when inflammation is clinically controlled [26]. While earlier investigations using PainDETECT classified approximately 5–28% of patients as having 'likely' or 'possible' neuropathic pain, more recent data indicate an even higher burden [8]. A 2023 systematic review and meta-analysis corroborated these findings, reporting pooled prevalence estimates ranging from 31% to 40% across various screening tools (PainDETECT, DN4, LANSS) [26]. This upward trend in reported prevalence is further supported by recent cross-sectional evidence demonstrating that nearly half of RA patients exhibit features of central sensitization [27]. Collectively, these studies, alongside our findings, reinforce the hypothesis that persistent pain in RA is frequently driven by central mechanisms rather than peripheral inflammation alone.
Regarding demographic factors, our analysis revealed a significant female predominance in the prevalence of neuropathic pain. This aligns with established literature describing sex-based disparities in pain processing, where hormonal, neurobiological, and psychosocial factors likely contribute to a lower pain threshold and higher symptom burden in female RA patients [28,29]. Interestingly, while sex appeared as a determinant, neither smoking status nor the specific class of anti-rheumatic treatment (conventional DMARDs, TNF inhibitors, or JAK inhibitors) showed a significant association with neuropathic pain features [8]. The lack of correlation with treatment modalities is particularly clinically relevant; it suggests that current biological and targeted synthetic therapies, while effective for suppressing inflammation, may fail to address established central sensitization [30]. This observation corroborates emerging evidence that neuropathic pain in RA is largely refractory to standard anti-inflammatory regimens, necessitating adjuvant pain management strategies independent of disease-modifying protocols.
Although PainDETECT scores showed moderate correlations with inflammatory markers (CRP, ESR) and disease activity indices (DAS28), these associations were significantly weaker than the correlation observed with self-reported pain intensity (VAS). This crucial discrepancy highlights that while inflammation contributes to pain, it is not the sole driver of neuropathic components [31]. Our finding that VAS was the only independent predictor of PainDETECT scores strongly supports the predominant influence of non-inflammatory, central mechanisms. This interpretation is consistent with recent literature showing neuropathic features persisting even in patients with well-controlled RA [32]. The co-existence of inflammatory and non-inflammatory inputs suggests a progression where persistent peripheral nociceptive signaling leads to maladaptive neuroplastic changes and subsequent central sensitization, amplifying pain responses that are resistant to conventional anti-inflammatory therapies [33].
Collectively, these data confirm that neuropathic pain represents a distinct and clinically significant phenotype in RA, which is strongly associated with an increased functional burden—specifically, exacerbated fatigue, sleep disturbance (PSQI), and reduced health-related quality of life (SF-36) [26]. These profound functional impairments underscore the inadequacy of traditional, inflammation-centric pain management. Accordingly, effective therapeutic strategies must extend beyond controlling synovitis and integrate approaches that specifically target central sensitization and neuropathic mechanisms [34]. Such mechanism-based interventions include tailored neuromodulatory pharmacologic agents, cognitive-behavioral techniques, and physical activity programs [35,36]. Routine assessment of neuropathic features is thus essential to guide individualized care and improve long-term outcomes in RA patients.
In our study, RA patients classified as having likely neuropathic pain reported significantly greater fatigue (FACIT-F), poorer sleep quality (PSQI), and lower scores across most SF-36 subscales, consistent with previous findings [8,26]. Notably, the moderate-to-strong negative correlations between PainDETECT scores and SF-36 domains—particularly Bodily Pain, Social Functioning, and Role Physical—highlight that neuropathic pain contributes substantially to overall disease burden, independent of joint inflammation [26]. This association emphasizes that a significant portion of functional impairment experienced by RA patients is linked to non-nociceptive mechanisms.
This functional burden is likely mediated by a self-perpetuating neurophysiological cycle: chronic pain exacerbates central sensitization, which in turn disrupts restorative sleep, leading to amplified fatigue and reduced psychological resilience [37,38]. This complex interplay underscores the necessity of moving beyond a purely inflammatory model [37]. Our findings strongly advocate for routine and comprehensive pain assessment that captures both nociceptive and neuropathic dimensions. Consequently, effective management strategies in RA must be multidimensional and mechanism-based, incorporating pharmacological agents (e.g., neuromodulators), behavioral interventions, and rehabilitative therapies specifically tailored to address sleep quality, central sensitization, and psychological resilience. This integrated approach is essential to achieving true well-being, rather than simply suppressing disease activity, in RA patients with neuropathic features [1,30].
Our study possesses several notable strengths. We included a relatively large cohort of RA patients, which enabled a robust evaluation of neuropathic pain prevalence and its relationship with disease activity and quality of life. The use of comprehensive, patient-reported assessments—including PainDETECT, SF-36, VAS, FACIT-F, and PSQI—integrated with objective inflammatory markers, provided a strong multidimensional perspective on the pain experience. Additionally, the application of multiple linear regression analysis allowed for the identification of independent factors contributing to neuropathic pain features.
Despite these strengths, several limitations should be considered. First, the cross-sectional nature of this study prevents us from drawing conclusions about causal relationships between neuropathic pain, disease activity, and quality of life; it remains unclear whether neuropathic pain exacerbates disease activity or if higher disease activity contributes to neuropathic pain. Second, although we employed validated self-reported measures, these assessments are inherently subject to individual perception and recall bias, which may have influenced the reported outcomes. Finally, our recruitment from a single tertiary care center may limit the generalizability of these findings, as patient demographics and clinical characteristics might differ across other settings or populations.
In light of these limitations, future longitudinal studies are warranted to rigorously examine the temporal relationships between the development of neuropathic pain and RA progression. Such investigations should also evaluate the long-term efficacy of targeted pharmacologic and non-pharmacologic interventions aimed at central sensitization, and further elucidate the underlying neurobiological mechanisms. These future steps will be critical for refining clinical guidelines, advancing patient-centered pain management strategies, and ultimately reducing the long-term burden of chronic pain in RA.
5. Conclusions
This study significantly advances the existing literature by offering a comprehensive, multidimensional assessment of neuropathic pain in rheumatoid arthritis (RA). Our central finding identifies perceived pain intensity (VAS) as the primary independent predictor of neuropathic pain, demonstrating that central pain processing mechanisms are key drivers of the symptom profile, distinct from systemic inflammation. Furthermore, we demonstrated that neuropathic pain features exert a substantial negative impact on fatigue, sleep disturbance, and overall quality of life. Collectively, these results underscore the clinical necessity of routinely evaluating neuropathic pain in RA patients and strongly support the implementation of personalized, mechanism-based management strategies that extend beyond conventional anti-inflammatory and disease-modifying therapies.
Author Contributions
ZAA, DY, ÖK, KK, MÇ, PO, and RÇ contributed to the conceptualization of the study. DY, MÇ, were responsible for data collection and analysis. ÖK contributed to the methodology and statistical analysis. KK and RÇ assisted with the review and editing of the manuscript. ZAA, RÇ, PO and ÖK supervised the study and contributed to the preparation of the final manuscript. All authors have read and approved the final version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Dicle University Faculty of Medicine (protocol code 355 and 22/10/2025).
Informed Consent Statement
Data are available from the corresponding author upon reasonable request, and will be shared in a manner that ensures the confidentiality of the data..
Acknowledgments
The authors would like to thank all the patients who participated in this study. We also appreciate the support of the clinical and research staff involved in data collection and management.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| SD: | Standard Deviation |
| BMI: | Body Mass Index |
| IQR: | Interquartile Range |
| csDMARDs: | Conventional Synthetic Disease-Modifying Antirheumatic Drugs |
| DMARD: | Disease-Modifying Antirheumatic Drug |
| TNFi / TNF: | Tumor Necrosis Factor Inhibitors |
| JAKi / JAK: | Janus Kinase Inhibitors |
| DAS28: | Disease Activity Score in 28 Joints |
| CRP: | C-Reactive Protein |
| ESR: | Erythrocyte Sedimentation Rate |
| VAS: | Visual Analogue Scale |
| FACIT-F: | Functional Assessment of Chronic Illness Therapy–Fatigue |
| PSQI: | Pittsburgh Sleep Quality Index |
| SF-36: | 36-Item Short Form Health Survey |
| PF: | Physical Functioning |
| RP: | Role Physical |
| RE: | Role Emotional |
| VT: | Vitality |
| SF: | Social Functioning |
| MH: | Mental Health |
| BP: | Bodily Pain |
| GH: | General Health |
References
- Zhang A, Lee YC. Mechanisms for Joint Pain in Rheumatoid Arthritis (RA): from Cytokines to Central Sensitization. Curr Osteoporos Rep. 2018 Oct;16(5):603-610. [CrossRef]
- Perniola S, Bruno D, Di Mario C, Campobasso D, Calabretta M, Gessi M, Petricca L, Tolusso B, Alivernini S, Gremese E. Residual pain and fatigue are affected by disease perception in rheumatoid arthritis in sustained clinical and ultrasound remission. Clin Rheumatol. 2025 Mar;44(3):1019-1029. [CrossRef]
- Walsh DA, McWilliams DF. Pain in rheumatoid arthritis. Curr Pain Headache Rep. 2012 Dec;16(6):509-17. [CrossRef]
- Das D, Choy E. Non-inflammatory pain in inflammatory arthritis. Rheumatology (Oxford). 2023 Jul 5;62(7):2360-2365. [CrossRef]
- Minhas D, Murphy A, Clauw DJ. Fibromyalgia and centralized pain in the rheumatoid arthritis patient. Curr Opin Rheumatol. 2023 May 1;35(3):170-174. [CrossRef]
- Lee YC, Cui J, Lu B, Frits ML, Iannaccone CK, Shadick NA, Weinblatt ME, Solomon DH. Pain persists in DAS28 rheumatoid arthritis remission but not in ACR/EULAR remission: a longitudinal observational study. Arthritis Res Ther. 2011 Jun 8;13(3):R83. [CrossRef]
- Trouvin AP, Attal N, Perrot S. Assessing central sensitization with quantitative sensory testing in inflammatory rheumatic diseases: A systematic review. Joint Bone Spine. 2022 Oct;89(5):105399. [CrossRef]
- Koop SM, ten Klooster PM, Vonkeman HE, Steunebrink LM, van de Laar MA. Neuropathic-like pain features and cross-sectional associations in rheumatoid arthritis. Arthritis Res Ther. 2015 Sep 3;17(1):237. [CrossRef]
- Kelleher EM, Meouchi R, Irani A. Beyond Inflammation: Why Understanding the Brain Matters in Inflammatory Arthritis. Arthritis Care Res (Hoboken). 2025 Nov 14. [CrossRef]
- Georgopoulos V, Smith S, McWilliams DF, Ferguson E, Wakefield R, Platts D, Ledbury S, Wilson D, Walsh DA. Contribution of inflammation markers and quantitative sensory testing (QST) indices of central sensitisation to rheumatoid arthritis pain. Arthritis Res Ther. 2024 Oct 8;26(1):175. [CrossRef]
- Belančić A, Sener S, Sener YZ, Fajkić A, Vučković M, Markotić A, Benić MS, Potočnjak I, Pavlović MR, Radić J, Radić M. Effects of Janus Kinase Inhibitors on Rheumatoid Arthritis Pain: Clinical Evidence and Mechanistic Pathways. Biomedicines. 2025 Oct 5;13(10):2429. [CrossRef]
- Taylor PC, Lee YC, Fleischmann R, Takeuchi T, Perkins EL, Fautrel B, Zhu B, Quebe AK, Gaich CL, Zhang X, Dickson CL, Schlichting DE, Patel H, Durand F, Emery P. Achieving Pain Control in Rheumatoid Arthritis with Baricitinib or Adalimumab Plus Methotrexate: Results from the RA-BEAM Trial. J Clin Med. 2019 Jun 12;8(6):831. [CrossRef]
- McWilliams DF, Walsh DA. Pain mechanisms in rheumatoid arthritis. Clin Exp Rheumatol. 2017 Sep-Oct;35 Suppl 107(5):94-101. Epub 2017 Sep 29. PMID: 28967354.
- Tański W, Szalonka A, Tomasiewicz B. Quality of Life and Depression in Rheumatoid Arthritis Patients Treated with Biologics - A Single Centre Experience. Psychol Res Behav Manag. 2022 Mar 3;15:491-501. [CrossRef]
- Vergne-Salle P, Pouplin S, Trouvin AP, Bera-Louville A, Soubrier M, Richez C, Javier RM, Perrot S, Bertin P. The burden of pain in rheumatoid arthritis: Impact of disease activity and psychological factors. Eur J Pain. 2020 Nov;24(10):1979-1989. [CrossRef]
- Fitzcharles MA, Shir Y. Management of chronic pain in the rheumatic diseases with insights for the clinician. Ther Adv Musculoskelet Dis. 2011 Aug;3(4):179-90. [CrossRef]
- Sebba A. Pain: A Review of Interleukin-6 and Its Roles in the Pain of Rheumatoid Arthritis. Open Access Rheumatol. 2021 Mar 5;13:31-43. [CrossRef]
- Baerwald C, Stemmler E, Gnüchtel S, Jeromin K, Fritz B, Bernateck M, Adolf D, Taylor PC, Baron R. Predictors for severe persisting pain in rheumatoid arthritis are associated with pain origin and appraisal of pain. Ann Rheum Dis. 2024 Sep 30;83(10):1381-1388. [CrossRef]
- Alkan H, Ardic F, Erdogan C, Sahin F, Sarsan A, Findikoglu G. Turkish version of the painDETECT questionnaire in the assessment of neuropathic pain: a validity and reliability study. Pain Med. 2013 Dec;14(12):1933-43. [CrossRef]
- Webster K, Cella D, Yost K. The Functional Assessment of Chronic Illness Therapy (FACIT) Measurement System: properties, applications, and interpretation. Health Qual Life Outcomes. 2003 Dec 16;1:79. [CrossRef]
- Akman T, Yavuzsen T, Sevgen Z, Ellidokuz H, Yilmaz AU. Evaluation of sleep disorders in cancer patients based on Pittsburgh Sleep Quality Index. Eur J Cancer Care (Engl). 2015 Jul;24(4):553-9. [CrossRef]
- Çelik D, Çoban Ö. Short Form Health Survey version-2.0 Turkish (SF-36v2) is an efficient outcome parameter in musculoskeletal research. Acta Orthop Traumatol Turc. 2016 Oct;50(5):558-561. [CrossRef]
- Ahmed S, Magan T, Vargas M, Harrison A, Sofat N. Use of the painDETECT tool in rheumatoid arthritis suggests neuropathic and sensitization components in pain reporting. J Pain Res. 2014 Oct 14;7:579-88. [CrossRef]
- Mesci N, Mesci E, Kandemir EU, Kulcu DG, Celik T. Impact of central sensitization on clinical parameters in patients with rheumatoid arthritis. North Clin Istanb. 2024 Apr 22;11(2):140-146. [CrossRef]
- Lee YC, Chibnik LB, Lu B, Wasan AD, Edwards RR, Fossel AH, Helfgott SM, Solomon DH, Clauw DJ, Karlson EW. The relationship between disease activity, sleep, psychiatric distress and pain sensitivity in rheumatoid arthritis: a cross-sectional study. Arthritis Res Ther. 2009;11(5):R160. [CrossRef]
- Rutter-Locher Z, Arumalla N, Norton S, Taams LS, Kirkham BW, Bannister K. A systematic review and meta-analysis of questionnaires to screen for pain sensitisation and neuropathic like pain in inflammatory arthritis. Semin Arthritis Rheum. 2023 Aug;61:152207. [CrossRef]
- Berrichi I, Taik FZ, Haddani F, Soba N, Fourtassi M, Abourazzak FE. Prevalence and Associated Factors of Central Sensitization in Patients with Chronic Inflammatory Rheumatic Disease. Curr Rheumatol Rev. 2025;21(4):418-423. [CrossRef]
- Barnabe C, Bessette L, Flanagan C, Leclercq S, Steiman A, Kalache F, Kung T, Pope JE, Haraoui B, Hochman J, Mosher D, Thorne C, Bykerk V. Sex differences in pain scores and localization in inflammatory arthritis: a systematic review and metaanalysis. J Rheumatol. 2012 Jun;39(6):1221-30. [CrossRef]
- Vogel K, Muhammad LN, Song J, Neogi T, Bingham CO, Bolster MB, Marder W, Wohlfahrt A, Clauw DJ, Dunlop D, Lee YC. Sex Differences in Pain and Quantitative Sensory Testing in Patients With Rheumatoid Arthritis. Arthritis Care Res (Hoboken). 2023 Dec;75(12):2472-2480. [CrossRef]
- Sarzi-Puttini P, Zen M, Arru F, Giorgi V, Choy EA. Residual pain in rheumatoid arthritis: Is it a real problem? Autoimmun Rev. 2023 Nov;22(11):103423. [CrossRef]
- Rifbjerg-Madsen S, Christensen AW, Christensen R, Hetland ML, Bliddal H, Kristensen LE, Danneskiold-Samsøe B, Amris K. Pain and pain mechanisms in patients with inflammatory arthritis: A Danish nationwide cross-sectional DANBIO registry survey. PLoS One. 2017 Jul 7;12(7):e0180014. [CrossRef]
- Saitou M, Noda K, Matsushita T, Ukichi T, Kurosaka D. Central sensitisation features are associated with neuropathic pain-like symptoms in patients with longstanding rheumatoid arthritis: a cross-sectional study using the central sensitisation inventory. Clin Exp Rheumatol. 2022 May;40(5):980-987. [CrossRef]
- Cao Y, Fan D, Yin Y. Pain Mechanism in Rheumatoid Arthritis: From Cytokines to Central Sensitization. Mediators Inflamm. 2020 Sep 12;2020:2076328. [CrossRef]
- Paroli M, Sirinian MI. Pathogenic Crosstalk Between the Peripheral and Central Nervous System in Rheumatic Diseases: Emerging Evidence and Clinical Implications. Int J Mol Sci. 2025 Jun 24;26(13):6036. [CrossRef]
- Chimenti RL, Frey-Law LA, Sluka KA. A Mechanism-Based Approach to Physical Therapist Management of Pain. Phys Ther. 2018 May 1;98(5):302-314. [CrossRef]
- Bäckryd E, Ghafouri N, Gerdle B, Dragioti E. Rehabilitation interventions for neuropathic pain: a systematic review and meta-analysis of randomized controlled trials. J Rehabil Med. 2024 Aug 5;56:jrm40188. [CrossRef]
- Finan PH, Goodin BR, Smith MT. The association of sleep and pain: an update and a path forward. J Pain. 2013 Dec;14(12):1539-52. [CrossRef]
- Haack M, Simpson N, Sethna N, Kaur S, Mullington J. Sleep deficiency and chronic pain: potential underlying mechanisms and clinical implications. Neuropsychopharmacology. 2020 Jan;45(1):205-216. [CrossRef]
Figure 2.
Correlations Between PainDETECT Scores and Clinical/Patient-Reported Outcome Measures in Rheumatoid Arthritis Patients. Scatterplots illustrating the relationships between PainDETECT scores and various clinical and patient-reported parameters in patients with rheumatoid arthritis. Each panel shows the Spearman correlation coefficient (r) between PainDETECT and the following variables: (A) Disease Activity Score in 28 joints (DAS28), (B) Visual Analogue Scale for pain intensity (VAS), (C) Functional Assessment of Chronic Illness Therapy–Fatigue (FACIT-F). All correlations were statistically significant (p < 0.01).
Figure 2.
Correlations Between PainDETECT Scores and Clinical/Patient-Reported Outcome Measures in Rheumatoid Arthritis Patients. Scatterplots illustrating the relationships between PainDETECT scores and various clinical and patient-reported parameters in patients with rheumatoid arthritis. Each panel shows the Spearman correlation coefficient (r) between PainDETECT and the following variables: (A) Disease Activity Score in 28 joints (DAS28), (B) Visual Analogue Scale for pain intensity (VAS), (C) Functional Assessment of Chronic Illness Therapy–Fatigue (FACIT-F). All correlations were statistically significant (p < 0.01).
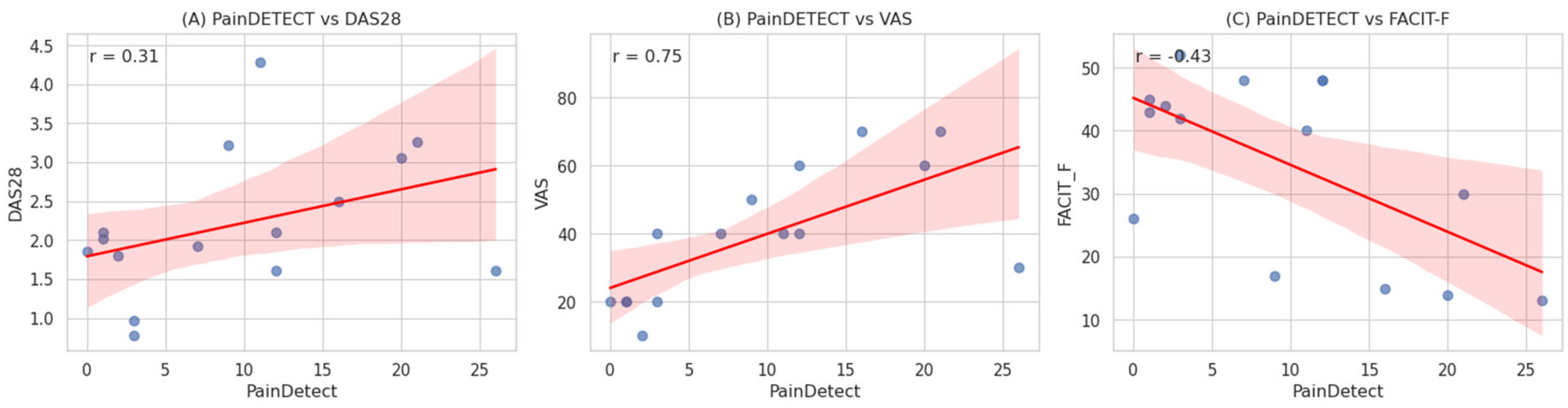

Table 1.
Demographic and Lifestyle Characteristics of RA Patients.
| Variable | RA Patients (n=160) | |
| Age (years), mean ± SD | 51.41 ± 13.48 | |
| Gender, n (%) | Female | 131 (81.8%) |
| Male | 29 (18.2%) | |
| BMI (kg/m²), mean ± SD | 27.56 ± 5.20 | |
| Education Level, n (%) | Illiterate | 49 (30.6%) |
| Primary | 55 (34.4%) | |
| Middle | 13 (8.1%) | |
| High School | 27 (16.9%) | |
| University | 16 (10.0%) | |
| Marital Status, n (%) | Single | 18 (11.3%) |
| Married | 123 (76.9%) | |
| Widowed | 19 (11.9%) | |
| Smoking Status, n (%) | Non-smoker | 121 (75.6%) |
| Smoker | 39 (24.4%) | |
| Disease duration (years), median (IQR) | 8,00 (0,75–40,00) | |
| Prescribed RA medications, n (%) | csDMARDs | 50 (31.2%) |
| Anti TNFi | 45 (28.1%) | |
| JAKi | 40 (25%) | |
| Rituximab | 5 (3.1%) | |
| Tocilizumab | 12 (7.5%) | |
| Abatacept: | 8 (5%) | |
| DAS28 (0–10), mean ± SD | 2.73 (0.77–6.35) | |
| DAS28, n (%) | <2,6 | 72 (45%) |
| 2,6–3,2 | 32 (20%) | |
| 3,2–5,1 | 45 (28.1%) | |
| >5,1 | 11 (6.9%) | |
| Neuropathic Pain , n (%) | Likely neuropathic pain | 36 (22.5%) |
| Unclear pain type | 24 (15%) | |
| Likely non-neuropathic pain | 100 (62.5%) | |
RA, rheumatoid arthritis; SD, standard deviation; BMI, body mass index; IQR, interquartile range; n, number of patients; csDMARDs, conventional synthetic disease-modifying antirheumatic drugs; TNFi, tumor necrosis factor inhibitors; JAKi, Janus kinase inhibitors; DAS28, Disease Activity Score in 28 joints.
Table 2.
Comparison of Clinical, Laboratory, Fatigue, Sleep Quality, and Quality of Life Parameters Between RA Patients With and Without Neuropathic Pain.
Table 2.
Comparison of Clinical, Laboratory, Fatigue, Sleep Quality, and Quality of Life Parameters Between RA Patients With and Without Neuropathic Pain.
| Variable | Neuropathic Pain (+) Mean ± SD (n: 36) | Neuropathic Pain (–) Mean ± SD (n: 124) | p-value |
| Age (years) | 52.09 ± 13.64 | 51.19 ± 13.42 | 0.696 |
| BMI (kg/m²) | 27.28 ± 6.31 | 27.76 ± 5.01 | 0.593 |
| CRP (mg/L) | 11.40 ± 15.62 | 8.83 ± 15.58 | 0.341 |
| ESR (mm/h) | 20.43 ± 12.83 | 15.97 ± 13.99 | 0.051 |
| DAS28 | 2.87 ± 0.68 | 2.26 ± 0.86 | <0.001 |
| Tender joint count | 1.40 ± 2.07 | 2.16 ± 2.41 | 0.041 |
| Swollen joint count | 0.13 ± 0.50 | 0.15 ± 0.77 | 0.906 |
| Disease duration (years) | 9.58 ± 7.54 | 8.51 ± 7.44 | 0.34 |
| FACIT-F | 23.13 ± 11.89 | 38.19 ± 12.61 | <0.001 |
| PSQI | 10.80 ± 3.35 | 7.08 ± 3.79 | <0.001 |
| SF-36 PF | 57.56 ± 20.50 | 74.40 ± 19.07 | <0.001 |
| VAS (pain) | 60.89 ± 17.94 | 38.73 ± 18.58 | <0.001 |
| SF-36 RP | 15.00 ± 27.39 | 49.83 ± 41.42 | <0.001 |
| SF-36 RE | 38.52 ± 48.18 | 80.22 ± 38.64 | <0.001 |
| SF-36 VT | 28.78 ± 15.34 | 47.53 ± 20.44 | <0.001 |
| SF-36 SF | 52.50 ± 16.98 | 74.83 ± 18.71 | <0.001 |
| SF-36 MH | 54.93 ± 16.98 | 69.23 ± 16.81 | <0.001 |
| SF-36 BP | 34.56 ± 14.64 | 55.02 ± 20.14 | <0.001 |
| SF-36 GH | 22.78 ± 13.51 | 41.00 ± 18.76 | <0.001 |
RA, rheumatoid arthritis; BMI, body mass index; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; DAS28, Disease Activity Score in 28 joints; VAS, Visual Analogue Scale; FACIT-F, Functional Assessment of Chronic Illness Therapy–Fatigue; PSQI, Pittsburgh Sleep Quality Index; SF-36, 36-Item Short Form Health Survey; PF, Physical Functioning; RP, Role Physical; RE, Role Emotional; VT, Vitality; SF, Social Functioning; MH, Mental Health; BP, Bodily Pain; GH, General Health; SD, standard deviation.
Table 3.
Distribution of Sex, Smoking, and Treatment Groups by Neuropathic Pain Status.
| Variable | Neuropathic Pain (+) n : 36 (%) | Neuropathic Pain (–) n: 124 (%) | p-value |
| Sex | <0.001 | ||
| – Female | 29 (80.5%) | 102 (82.2%) | |
| – Male | 7 (19.5%) | 22 (7.8%) | |
| Smoking | 0.593 | ||
| – Non-smoker | 25 (69.4%) | 96 (77.4%) | |
| – Smoker | 11 (30.6%) | 28 (22.6%) | |
| Treatment Group | 0.707 | ||
| – JAK | 9 (25%) | 31 (25%) | |
| – TNF | 11 (30.5%) | 34 (27.4%) | |
| – DMARD | 12 (33.3%) | 38 (30.6%) | |
| – Others | 4 (11.2%) | 21 (17%) |
n, number of patients; %, percentage; p-value, significance value; JAK, Janus kinase inhibitors; TNF, tumor necrosis factor inhibitors; DMARD, disease-modifying antirheumatic drugs.
Table 4.
Correlation Between PainDETECT and Clinical/Functional Measures.
| Variable | r | p-value |
| DAS28 | 0.527 | <0.01 |
| VAS (pain) | 0.650 | <0.01 |
| ESR (mm/h) | 0.235 | <0.01 |
| CRP (mg/L) | 0.150 | <0.01 |
| FACIT-F (fatigue) | −0.456 | <0.01 |
| PSQI | 0.318 | <0.01 |
| SF-36 PF | −0.690 | <0.01 |
| SF-36 RP | −0.706 | <0.01 |
| SF-36 RE | −0.567 | <0.01 |
| SF-36 VT | −0.634 | <0.01 |
| SF-36 SF | −0.703 | <0.01 |
| SF-36 MH | −0.665 | <0.01 |
| SF-36 BP | −0.689 | <0.01 |
| SF-36 GH | −0.661 | <0.01 |
RA, rheumatoid arthritis; DAS28, Disease Activity Score in 28 joints; VAS, Visual Analogue Scale; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; FACIT-F, Functional Assessment of Chronic Illness Therapy–Fatigue; PSQI, Pittsburgh Sleep Quality Index; SF-36, 36-Item Short Form Health Survey; PF, Physical Functioning; RP, Role Physical; RE, Role Emotional; VT, Vitality; SF, Social Functioning; MH, Mental Health; BP, Bodily Pain; GH, General Health.
Table 5.
Multivariate Linear Regression Analysis for Predictors of Neuropathic Pain.
| Predictor | B | Std. Error | Wald | df | Sig. | Exp(B) |
| Constant | -0.017 | 2.698 | 0.000 | 1 | 0.995 | 0.983 |
| Age | 0.007 | 0.019 | 0.121 | 1 | 0.728 | 1.007 |
| BMI | 0.037 | 0.042 | 0.780 | 1 | 0.377 | 1.038 |
| CRP | -0.001 | 0.014 | 0.002 | 1 | 0.962 | 0.999 |
| ESR | -0.005 | 0.022 | 0.050 | 1 | 0.823 | 0.995 |
| DAS28 | -0.138 | 0.464 | 0.089 | 1 | 0.766 | 0.871 |
| FACIT | 0.040 | 0.032 | 1.539 | 1 | 0.215 | 1.041 |
| VAS | 0.039 | 0.014 | 7.439 | 1 | 0.006 | 0.961 |
| SF36-PF | -0.008 | 0.017 | 0.204 | 1 | 0.652 | 0.992 |
| SF36-RP | 0.007 | 0.010 | 0.466 | 1 | 0.495 | 1.007 |
| SF36-RE | 0.001 | 0.007 | 0.013 | 1 | 0.910 | 1.001 |
| SF36-VT | -0.017 | 0.031 | 0.297 | 1 | 0.586 | 0.983 |
| SF36-MH | -0.011 | 0.022 | 0.226 | 1 | 0.634 | 0.989 |
| SF36-SF | 0.032 | 0.021 | 2.295 | 1 | 0.130 | 1.032 |
| SF36-BP | -0.001 | 0.022 | 0.002 | 1 | 0.961 | 0.999 |
| SF36-GH | 0.024 | 0.022 | 1.253 | 1 | 0.263 | 1.025 |
RA, rheumatoid arthritis; B, unstandardized regression coefficient; Std. Error, standard error; df, degrees of freedom; Exp(B), exponentiated coefficient; BMI, body mass index; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; DAS28, Disease Activity Score in 28 joints; FACIT-F, Functional Assessment of Chronic Illness Therapy–Fatigue; VAS, Visual Analogue Scale; SF-36, 36-Item Short Form Health Survey; PF, Physical Functioning; RP, Role Physical; RE, Role Emotional; VT, Vitality; MH, Mental Health; SF, Social Functioning; BP, Bodily Pain; GH, General Health. VIF values for all predictors were below 5, indicating that multicollinearity was not a major concern.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



