Submitted:
01 January 2026
Posted:
04 January 2026
You are already at the latest version
Abstract
Environmental factors in the daily lives of people with dementia are not disease-modifying agents that directly influence neurodegenerative pathology. However, inadequate lighting, reduced nighttime visibility, complex pathways, excessive sensory stimulation, and unpredictable environmental changes frequently trigger delirium, nighttime agitation, falls, sleep fragmentation, and behavioral and psychological symptoms of dementia (BPSD). These in turn significantly accelerate disease progression, leading to increased rates of hospitalization, institutionalization, and caregiving breakdown.Many existing environmental improvement strategies are based on architectural ideals or comprehensive design theories, often lacking sufficient consideration for feasibility or sustainability in home or care settings. The aim of this paper is to redefine environmental interventions for people with dementia not as a form of treatment, but as a method to control progression-accelerating factors. By decomposing existing guidelines and environmental design research into "core active ingredients" and "excessive cognitive or operational burdens," we propose a minimal intervention model that can be sustainably implemented in real-world care settings.From an integrated review of the literature, we identify three core environmental intervention components for dementia care: (1) lighting that provides clear temporal cues for day and night; (2) simplified and visible nighttime pathways; and (3) optimization of sensory input, particularly through reduction of noise and unpredictable stimuli. These components do not halt disease progression, but they serve as a highly practical foundation for non-pharmacological interventions by mitigating acute deterioration events such as delirium, falls, BPSD, and hospitalization. This paper presents a model that organizes these relationships into a cascade of progression accelerators and proposes a feasible environmental intervention framework.
Keywords:
dementia
; environmental intervention
; non-pharmacological intervention
; progression-accelerating factors
; delirium
; falls
; BPSD
; implementation feasibility
1. Introduction
1.1. Redefining the "Environment" in Dementia Care
The environment is not a curative factor in dementia. However, it exerts a powerful influence as a condition that can sharply exacerbate the course of the disease.
Inappropriate lighting, complex pathways, sudden stimuli, and unfamiliar changes in layout have repeatedly been reported to disrupt temporal orientation, spatial cognition, and safety judgment in people with dementia, leading to delirium, nighttime agitation, and falls (Fleming & Purandare, 2010; Oh & Fong, 2017). Figure 1 conceptually illustrates the cascade of acute deterioration triggered by these environmental factors.
What is particularly important is that the effects of these environmental factors are not the result of chronic neurodegeneration, but can worsen or improve within relatively short periods and are often reversible. Therefore, the environment should not be regarded as “ancillary care,” but rather as the most upstream lever for controlling progression-accelerating factors (WHO, 2017).
1.2. Limitations of Conventional Environmental Design Approaches
Conventional environmental design theories often aspire to ideal architectural or facility layouts and tend to rely on the following implicit assumptions:
- Major renovations or dedicated equipment are feasible.
- Caregivers are consistently able to optimize environmental conditions.
- The person with dementia can understand and adapt to changes in the environment.
However, in home-based and general care settings, these assumptions are rarely met. As a result, interventions that are theoretically sound often fail to be implemented in practice, becoming “correct but unworkable.”
This paper aims to reconstruct the concept of the environment from a design-centered approach to one focused on implementation.
2. Constraints on Environmental Interventions in Dementia Care
2.1. Cognitive Constraints: Impaired Processing of Temporal and Spatial Cues
In dementia, impairments in temporal orientation, visuospatial perception, and attention allocation occur from early stages.
Inconsistent lighting or disorganized spatial layouts can easily lead to misperceptions of time or spatial confusion.
2.2. Emotional and Behavioral Constraints: Overstimulation and Reactive BPSD
Unpredictable stimuli and noise often trigger behavioral and psychological symptoms of dementia (BPSD) through anxiety and fear.These symptoms should not be interpreted as intentional behaviors, but rather as reactive responses to the surrounding environment (Cohen-Mansfield, 2001).
2.3. Implementation Constraints: Person-Dependent Environmental Management
When environmental adjustments rely on caregiver effort or vigilance, sustainability is compromised.
The environment must function as a stable structure—not as a system dependent on human effort.
3. Differentiating Core Active Ingredients from Excessive Implementation Burdens
3.1. Core Active Ingredients in Environmental Interventions
The main challenge in implementing environmental interventions for dementia has not been a lack of effectiveness, but rather the conflation of effective elements with components that impose excessive cognitive or operational burdens.
In this section, we integrate existing studies and guidelines to decompose environmental interventions into "core active ingredients" and "components that should be eliminated due to their implementation burden" (see Figure 2).
The literature review identifies the following three elements as core active ingredients:
- Lighting that clarifies temporal cues for day and night
Providing sufficient brightness during the day and avoiding excessive lighting at night supports circadian rhythm stabilization and helps reduce nighttime agitation and delirium
(Rea & Figueiro, 2018; Van Hoof et al., 2009).
- Simplification of nighttime pathways and assurance of visibility
Fixing the walking route, using floor-level lighting, and removing obstacles can reduce the risk of falls
(Allan et al., 2009; NICE, 2013).
- Optimization of sensory stimulation
Reducing noise and sudden stimuli decreases the frequency of BPSD and delirium
(Livingston et al., 2014).
These three elements are all applicable without increasing environmental complexity, and as shown in Figure 2, they can be clearly distinguished from design features that impose excessive implementation burdens.
3.2. Implementation Burdens to Be Eliminated
- Frequent rearrangement of furniture or layout
- Excessive signage and information displays
- Requiring the person with dementia to understand and adapt to environmental changes
- Management dependent on caregiver attention and vigilance
4. Dementia-Adapted Minimal Environmental Intervention Model
4.1. Minimal Component ①: Bright Days, Dark Nights
To implement the core active ingredients sustainably in home and care settings, we propose a dementia-adapted minimal environmental intervention model (see Figure 3).
Key lighting principles include:
- Daytime: Maximize natural light and maintain sufficient indoor brightness.
- Nighttime: Use minimal lighting only to ensure footpath visibility.
4.2. Minimal Component ②: Fixed Nighttime Pathways
- Establish a consistent route from bed to toilet.
- Avoid rearranging furniture.
4.3. Minimal Component ③: Reduced Sensory Load
- Avoid keeping the television on continuously or at high volume.
- Minimize nighttime verbal interactions and sudden physical contact.
As shown in Figure 3, this model is characterized by transferring the responsibility for safety and predictability from the person to the environment itself, thereby maximizing emotional security and environmental predictability without relying on the individual's cognitive effort or adaptive capacity.
5. Implementation Protocol (Summary)
- Frequency: Continuous (applied at all times)
- Responsible party: The environment itself (do not place responsibility on the person with dementia)
- Inspection: Simple weekly checks
6. Implications for Research, Practice, and Policy
Figure 1 through 3 presented in this paper systematize environmental interventions for dementia in three dimensions:
The value of environmental interventions should be assessed not by cognitive function scores, but by cost-related outcomes such as delirium, falls, hospitalizations, and institutionalization.
The novelty of this paper lies in redefining the environment not as a treatment, but as a means of controlling progression-accelerating conditions.
7. Conclusion
Environmental interventions for people with dementia represent one of the most cost-effective, immediate, and reproducible foundational strategies available.
By preserving the core active ingredients while eliminating excessive burdens, the environment can function as an implementation-science–based intervention that builds a “brain-friendly world.”
This concept is embodied in the minimal environmental intervention model presented in Figure 3.
Appendix
Environmental Adjustment Support Manual for People with Dementia
(Implementation Guide for Care and Home Settings)
Appendix
1. Purpose and Positioning
This manual provides implementation guidelines for making environmental adjustments for people with dementia that are safe and sustainable in both home and care settings.
This program is not a therapeutic intervention aimed at suppressing or improving the progression of dementia itself.
Rather, it is a non-pharmacological intervention focused on preventing acute deterioration—such as delirium, nighttime agitation, falls, and BPSD—that may be triggered by inappropriate environmental conditions.
This manual is intended for use by:
- Care workers engaged in facility-based or home-based dementia care
- Family caregivers supporting individuals with dementia
- Medical and welfare professionals seeking to integrate environmental adjustments into daily care without excessive burden
※ This manual is not a clinical trial protocol, but a practical implementation guide for daily care.
※ It does not claim to improve cognitive function or exert disease-modifying effects through environmental changes.
2. Target Users
Primary Target Population
- Individuals with mild to moderate dementia
- Individuals prone to instability in orientation to time, place, or situation
- Individuals exhibiting nighttime agitation, falls, delirium, or hypersensitivity to sensory stimuli
Exclusion Criteria / Cases Requiring Caution
- Persistent severe agitation or aggression, where environmental adjustments alone are insufficient to ensure safety
- Medically unstable conditions such as acute delirium, infection, or severe pain
- Situations where acute-phase medical symptoms requiring clinical judgment take priority
※ Final decisions should always be based on clinical judgment.
※ Even for individuals with severe dementia, this program may still be applied in an adaptive manner to maintain an environment that does not induce confusion or anxiety.
3. Basic Design Principles
This program is based on the following four principles:
1. Minimization of Cognitive Load
- Do not require the individual to understand, learn, or adapt to the environment
- Avoid interventions that rely on explanations, memory, or judgment
2. Emotional Safety
- Avoid sudden stimuli or environmental changes
- If anxiety, confusion, or fear reactions are observed, reduce or stop the intervention immediately
3. Predictability and Stability
- Keep lighting, pathways, and layout as fixed and consistent as possible
- Do not create environments that change from day to day
4. Environment-Led Support
- Do not rely on the individual’s attention, judgment, or effort
- Aim to create a state in which “safety is ensured even if the person does nothing”
4. Overall Implementation Framework
Frequency and Duration
- Environmental adjustments: Applied continuously
- Inspection and confirmation: Simple checks conducted approximately once per week
Implementation Setting
- The individual's familiar living environment
- Does not assume major renovations or the use of special equipment
- Makes use of existing resources such as furniture, lighting, and acoustic conditions
5. Core Support Elements (Three Essential Components)
5.1 Lighting Environment That Clarifies Temporal Cues
Objective
- Prevent day-night reversal, nighttime agitation, and delirium
- Support the stabilization of circadian rhythms
Methods
- During the daytime, ensure the environment is as bright as possible, using natural and indoor light
- During the nighttime, avoid excessive lighting and use only minimal foot-level lighting as needed
Precautions
- Do not suddenly switch on ceiling lights at night
- Avoid frequent changes to the color or position of lighting
5.2 Simplifying Nighttime Pathways and Ensuring Visibility
Objective
- Prevent falls, disorientation, and anxiety reactions during the night:
Methods
- Fix the route from bed to toilet
- Remove obstacles from walkways
- Install minimal lighting that allows clear visibility of the floor
Avoid the Following
- Frequent rearrangement of furniture layout
- Temporarily placing objects along the walking path
5.3 Optimization of Sensory Stimulation (Reducing Noise and Sudden Stimuli)
Objective
- Prevent the onset of BPSD, delirium, and anxiety reactions
Methods
- Avoid leaving the TV or radio on continuously or at high volume
- Reduce sudden verbal interactions or physical contact during the night
- Minimize unpredictable sounds and light stimuli
Precautions
- It is not necessary to enforce total silence
- The problems arise from stimuli that are:
"sudden," "intense," or "unpredictable"
6. Interventions That Should Not Be Implemented (Explicit Exclusions)
The following interventions are not included in this program:
- Explaining the reasons for environmental changes and expecting the individual to understand
- Using signs, labels, or notices as cognitive compensation
- Safety measures that depend on the individual's attention or judgment
- Frequent redecorating or rearranging of furniture
※ The goal is not the elimination of all environmental stimuli, but rather the restructuring of the type and amount of stimulation.
7. Criteria for Adjustment and Discontinuation
Adjustable Elements
- Light intensity (may be reduced if needed)
- Level of sensory stimulation (sound, light, human traffic)
- Degree of pathway simplification
Criteria for Discontinuation or Re-evaluation
- Clear increase in anxiety, fear, or confusion
- Worsening of nighttime agitation or delirium
- Cases where fall risk increases as a result of the intervention
8. Safety and Burden Management
- The intervention carries extremely low physical invasiveness
- The greatest risk is overzealous environmental modifications driven by good intentions
- Do not aim for a perfect environment
- The mere fact that the environment remains stable is, in itself, the most effective intervention
9. Consistency with Existing Evidence
This manual has been reconstructed as a minimal intervention model adapted to the real-world implementation context of dementia care, while incorporating findings from existing review studies and guidelines, including:
- The relationship between lighting environment, circadian rhythm, sleep, and delirium
- The relationship between environmental factors, falls, and BPSD
- The positioning of environmental adjustments as a form of non-pharmacological intervention
10. Applications in Research and Practice
For Research Use
- Supplementary material to describe the content of interventions
- Documentation of implementation methods and fidelity
- Clarification of the definition of non-pharmacological interventions
For Practical Use
- A simple manual for care workers
- Handout materials for family caregivers
- Shared reference for aligning care policies and environmental strategies
Figure 1.
Environmental deterioration as an upstream accelerator of adverse outcomes in dementia. In people with dementia, environmental factors do not directly modify neurodegenerative pathology but function as upstream triggers that precipitate disorientation, anxiety, sleep fragmentation, delirium, falls, and subsequent hospitalization and institutionalization. Environmental interventions are therefore best conceptualized as strategies to control progression-accelerating conditions rather than disease-modifying treatments.
Figure 1.
Environmental deterioration as an upstream accelerator of adverse outcomes in dementia. In people with dementia, environmental factors do not directly modify neurodegenerative pathology but function as upstream triggers that precipitate disorientation, anxiety, sleep fragmentation, delirium, falls, and subsequent hospitalization and institutionalization. Environmental interventions are therefore best conceptualized as strategies to control progression-accelerating conditions rather than disease-modifying treatments.
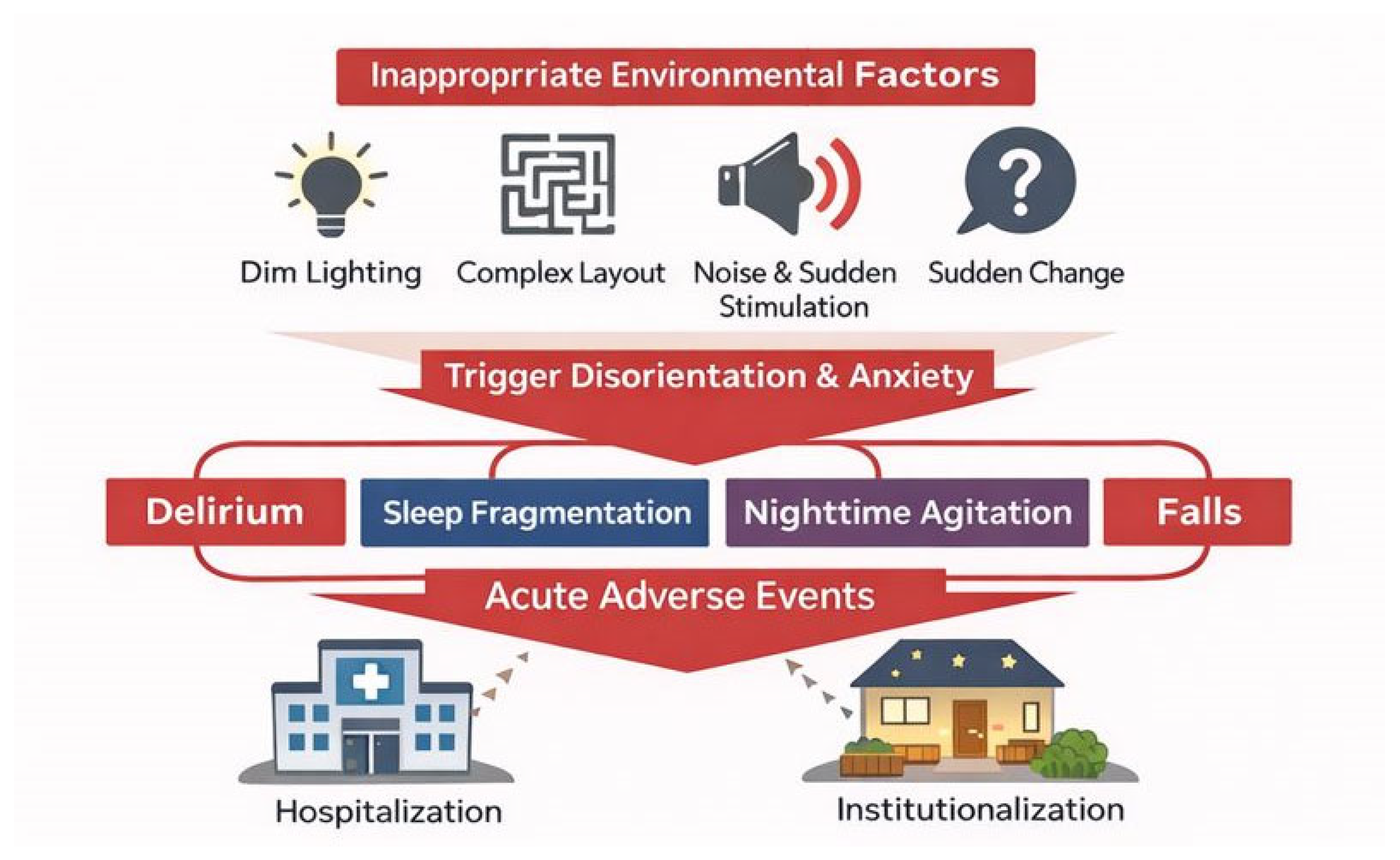
Figure 2.
Decomposition of environmental interventions into active ingredients and excessive implementation burdens. Evidence-based environmental interventions for dementia can be decomposed into a small set of core active ingredients that stabilize orientation, safety, and emotional regulation, and ancillary elements that impose excessive cognitive or operational burden. Removing these burdens enhances feasibility and sustainability without sacrificing effectiveness.
Figure 2.
Decomposition of environmental interventions into active ingredients and excessive implementation burdens. Evidence-based environmental interventions for dementia can be decomposed into a small set of core active ingredients that stabilize orientation, safety, and emotional regulation, and ancillary elements that impose excessive cognitive or operational burden. Removing these burdens enhances feasibility and sustainability without sacrificing effectiveness.
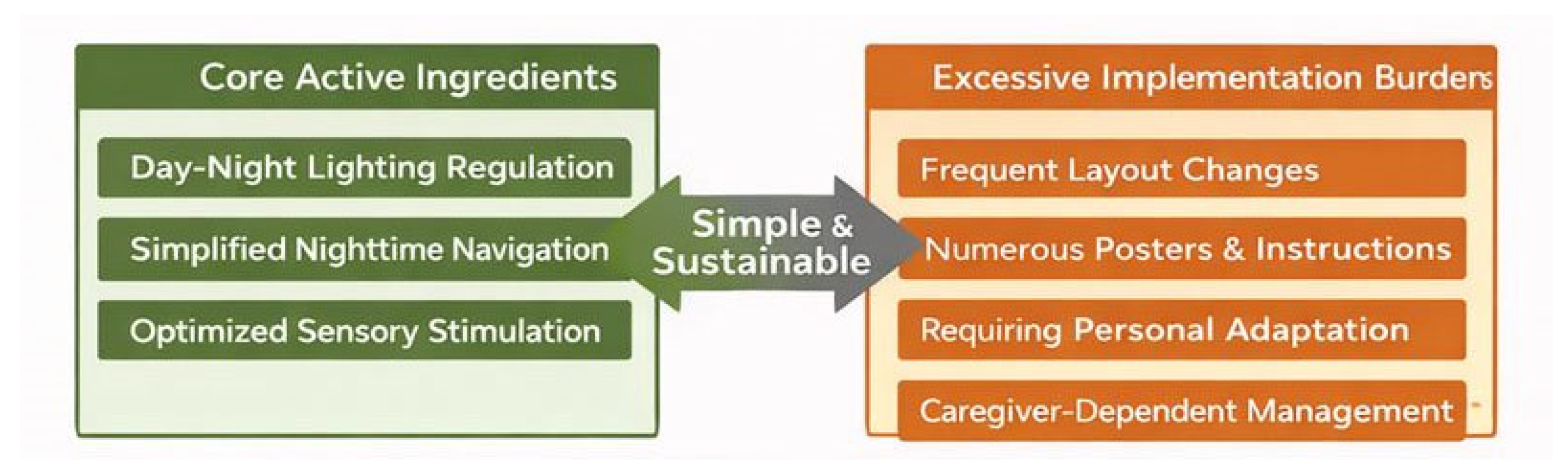
Figure 3.
Dementia-adapted minimal environmental intervention model. The proposed model shifts responsibility from the person with dementia to the environment itself by prioritizing predictability, simplicity, and sensory stability. By focusing on a minimal set of environmental components, the model maximizes feasibility and cumulative exposure to effective conditions while minimizing cognitive and operational burden.
Figure 3.
Dementia-adapted minimal environmental intervention model. The proposed model shifts responsibility from the person with dementia to the environment itself by prioritizing predictability, simplicity, and sensory stability. By focusing on a minimal set of environmental components, the model maximizes feasibility and cumulative exposure to effective conditions while minimizing cognitive and operational burden.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



