
Submitted:
29 December 2025
Posted:
30 December 2025
You are already at the latest version
Abstract
Following World Health Organization (WHO) validation of lymphatic filariasis (LF) elimination as a public health problem, countries are required to implement post-validation surveillance (PVS) to detect potential resurgence and ensure sustained elimination. Despite WHO guidelines to implement at least two of four PVS strategies – targeted surveys, integration into standardised surveys, health facility-based screening, and molecular xenomonitoring (MX) – implementation varies widely. This review syn-thesised global evidence on PVS activities from 2007–2025 in the 23 countries and territo-ries validated as having eliminated LF. Studies were identified through PubMed, Scopus, Embase, Web of Science, and WHO Institutional Repository for Information Sharing (IRIS). Data on publication information, surveillance strategies, priority populations, and opera-tional challenges and enablers were extracted. Narrative synthesis using deductive con-tent analysis was applied. Thirty documents from 17 countries were included. Targeted surveillance and integration of PVS with other health programs were the most common approaches noted (reported in ten and nine countries respectively), followed by MX (seven countries) and health facility-based screening (four countries). Surveillance often focused on migrants and previous hotspots, with operational challenges linked to limited funding, workforce, and supply chains. Documents indicated that Sri Lanka, Thailand, China, and South Korea developed sustained PVS through national policies and domestic funding. Findings highlight the need for clear, contextualised guidance to operationalise sustaina-ble PVS in different settings.
Keywords:
disease surveillance
; neglected tropical diseases
; lymphatic filariasis
; elephantiasis
; elimination
1. Introduction
Lymphatic filariasis (LF) is a neglected tropical disease caused by three species of thread-like parasitic worms: Wuchereria bancrofti, Brugia malayi, and B. timori. W. bancrofti causes 90% of infections worldwide and is spread primarily by Aedes, Anopheles, and Culex genus mosquitoes. The typical vectors for Brugia spp. are mosquito species in the genera Mansonia and Aedes [1,2]. LF is endemic in 72 countries worldwide [3]. Chronic infection can lead to lymphoedema (tissue swelling caused by lymphatic dysfunction), elephantiasis (skin and tissue thickening) of limbs and scrotal hydrocoele [4]. The resulting disfigurement and disability can lead to physical impairment and social stigmatisation, and subsequent ostracism and loss of employment [5]. Prior to the establishment of the Global Programme for the Elimination of Lymphatic Filariasis (GPELF), chronic LF had an estimated burden of 5.25 million disability-adjusted life-years (DALYs) and an estimated economic burden of USD 2.5 billion annually, largely due to disability and loss of employment. In 2019, the burden was estimated to be 1.63 million DALYs [6,7].
The GPELF was launched in 2000 and is one of the largest global public health interventions ever mounted [8]. The programme aims to eliminate LF as a public health problem through multiple rounds of mass drug administration (MDA), as well as managing morbidity and preventing disability (MMDP) among those already infected ([8,9]. Regional and national programmes were also established, including the Pacific Programme for the Elimination of Lymphatic Filariasis (PacELF) in 1999 [1], the South-East Asia regional programme to eliminate lymphatic filariasis in 2000 [10], and various national programmes across the World Health Organization (WHO) Regional Office for Africa [11].
The WHO defines elimination of LF as a public health problem as reducing antigen or antibody prevalence to below 1% in W. bancrofti or Brugia spp. endemic regions, respectively; this represents a threshold at which further transmission is believed to be unlikely even if MDA does not continue [12,13]. The WHO Road Map for Neglected Tropical Diseases 2021–2030 (the Road Map) aims for all 72 LF-endemic countries to no longer require MDA and be implementing post-validation surveillance (PVS) or post-MDA surveillance by 2030 [14].
Following elimination as a public health problem, countries are validated by WHO; the validation process requires the preparation and submission of a dossier presenting evidence of sustained reduction of LF nationally [15]. This evidence is based on initial baseline prevalence surveys (known as A/B/C surveys), followed by a transmission assessment survey (TAS1) showing that the prevalence of infection is below the target threshold of 1% in a sample of children under seven years of age, which confirms MDA can be stopped. Subsequent TASs must then show that infection prevalence remains below 1% in children aged under seven years after two years (TAS2) and four years (TAS3) [15]. The Road Map aims for at least 80% of LF endemic countries (58/72) to have been validated for the elimination of LF as a public health problem by 2030 [16].
The dossier must also include a commitment to and description of proposed post-validation surveillance (PVS) activities [15]. PVS is defined as ongoing, sustained surveillance following elimination, with the primary aim of detecting and preventing resurgence of infection [13]. Due to LF’s long asymptomatic period and its low prevalence in a post-validation context, active case finding is required for PVS [13].
In 2007, China became the first country to be validated by WHO as having eliminated LF as a public health problem. Since then (up to November 2025), 22 additional countries have met the epidemiological threshold, prepared and submitted a dossier, and been validated by WHO as having eliminated LF. Twelve others have completed MDA but are still completing TAS; 39 countries still require MDA [3,9,17]. Figure 1 illustrates countries by LF elimination status, defined as: not endemic, not eliminated, having met the epidemiological threshold for elimination (in the process of preparing the validation dossier), and validated by the WHO as having eliminated LF.
WHO guidelines recommend that PVS be continued for at least ten years after validation to monitor for resurgence [13]. Where transmission is ongoing and has not been detected through PVS activities, this may result in re-establishment of transmission, threatening the successes of many years of MDA. Evidence emerging from several Pacific Island countries and territories and Sri Lanka indicates that, even after the criteria for elimination as a public health problem have been met, persistent LF transmission can continue [18,19,20], emphasising the need for sustained PVS. The second edition of the WHO’s guidelines for Monitoring and epidemiological assessment of mass drug administration in the global programme to eliminate lymphatic filariasis (released May 2025; thereafter referred to in this document as the WHO guidelines) includes the latest advice on what PVS activities should be conducted [13]. These guidelines recommend countries implement at least two of the following four PVS strategies: health-facility based screening, integration of PVS into existing population surveys, targeted LF surveillance of high-risk areas or groups, and molecular xenomonitoring (MX) [13].
The implementation of effective PVS requires a robust understanding of countries’ unique geographic and epidemiological profile, operational context, and challenges and enablers to PVS implementation [22]. Importantly, experiences in one country may inform approaches taken by another, though context, capacity, and need will inevitably differ. Given these challenges, the aims of this scoping review were to identify and synthesise publicly available evidence on PVS activities globally, establishing an evidence base on which future guidelines and strategies may draw. Specifically, the review aimed to:
- Profile publicly documented PVS activities, or lack thereof, in countries previously endemic for LF.
- Examine documented barriers and facilitators to the implementation of PVS strategies, and how these vary by context.
- Compare alignment of PVS activities with recently released recommendations in the WHO’s Monitoring and epidemiological assessment of mass drug administration in the global programme to eliminate lymphatic filariasis guidelines [13].
- Identify knowledge gaps in PVS implementation methods that may be addressed through further operational research.
2. Materials and Methods
The methods for this study have been registered on PROSPERO (registration ID: CRD42024618436).
2.1. Identifying Studies
This study was conducted in line with the Preferred Reporting Items for Systematic reviews and Meta-Analyses guidelines Extension for Scoping Reviews (PRISMA-ScR) [23]. The Population, Intervention/Exposure, Comparator, Outcome and Time (PICOT) framework was used to develop the search strategy, presented in Table 1. As this review aims to scope and critique the PVS strategies being employed across several countries, we determined that identifying a Comparator was not required.
PubMed, Scopus, Embase and Web of Science were used to search for peer-reviewed journal articles, and the WHO Institutional Repository for Information Sharing (IRIS) database was used to search for PVS-related grey literature reports published by WHO.
A search strategy using Medical Subject Headings (MeSH) search terms, free text keywords, and Boolean operators were developed. Appendix A presents the search terms used across each literature database.

Table 1.
PICOT components.
| PICOT | Component | Search Term | Add with |
|---|---|---|---|
| Population | Countries that have been validated as having eliminated LF by WHO | "Bangladesh"[Mesh] OR Bangladesh* OR "Cambodia"[Mesh] OR Cambodia* OR China [MeSH] OR Cook Island* OR "Egypt"[Mesh] OR Egypt* OR Kiribati* OR “i-Kiribati” OR "Laos"[Mesh] OR Laos OR "Malawi"[Mesh] OR Malawi* OR Maldiv* OR Marshall Island* OR Niue* OR Palau* OR “Republic of Korea”[Mesh] OR “South Korea” OR "Sri Lanka"[Mesh] OR Sri Lanka* OR "Thailand"[Mesh] OR Thai* OR "Togo"[Mesh] OR Togo* OR Tonga* OR Vanuatu* OR "Vietnam"[Mesh] OR Vietnam* OR "Yemen"[Mesh] OR Yemen* OR “Wallis and Futuna” OR Wallis* OR Futuna* OR "Brazil"[Mesh] OR Brazil* OR “Timor-Leste”[Mesh] OR Timor* | AND |
| Exposure or intervention | Lymphatic filariasis | "Elephantiasis, Filarial"[Mesh] OR "lymphatic filariasis" OR elephantias* OR filaria* OR “filarial elephantiasis” OR filarial lympho*dema OR "Wuchereria bancrofti" OR "Brugia malayi" OR "Brugia timori" OR Bancrofti* OR Brugia* | AND |
| Outcome | Post-validation surveillance | "post-elimination" OR "post-validation" OR elimination OR validation OR "Sentinel Surveillance"[Mesh] OR “sentinel surveillance” OR “Public Health Surveillance” [Mesh] OR “public health surveillance” OR "Population Surveillance"[Mesh] OR “population surveillance” OR "Monitoring, Physiologic"[Mesh] OR “physiologic monitoring” OR "Epidemiological Monitoring"[Mesh] OR "Mass Screening"[Mesh] OR “mass screening” | AND |
| Comparator | N/A | N/A | |
| Time | Jan 2007– Jun 2025 (inclusive) | Jan 2007– Jun 2025 (inclusive) | AND |
2.2. Data Management, Study Screening and Selection
Data management, study screening and selection were performed with the aid of Covidence software (https://www.covidence.org/). Search results from the selected databases were imported into Covidence, and duplicates removed.
Documents were included if they:
- • described PVS activities conducted between January 1, 2007, to July 30, 2025 (inclusive) in a country or territory that has been validated by WHO as having eliminated LF as a public health problem;
- • were original research, activity reports, protocols, or WHO grey literature describing population-level surveillance; and
- • were published between January 1, 2007, and July 30, 2025 (inclusive).
Documents were excluded if they:
- • described surveillance activities that occurred before validation by WHO of elimination of LF; or
- • did not describe population-level surveillance activities (such as diagnostic validation and modelling studies, letters, editorials and commentary articles).
Two researchers (HJ and HL) independently screened the title and abstracts of included records using the above criteria. Where disagreement in screening assessments occurred, HJ and HL discussed and aimed to find consensus; if required, a third reviewer (AC) was consulted. If resolution was not found, a conservative approach was taken, and the article included for full text review. Following title and abstract screening, HJ conducted full text screening. Screening decisions were documented using a PRISMA flow diagram.
2.3. Data Extraction
Data was extracted into an Excel spreadsheet developed by the research team. Data were extracted for four categories:
- Publication information: year of publication, country of study setting, publication funding sources
- LF epidemiology: causative pathogen (W. bancrofti or Brugia spp.), year in which LF was validated as eliminated, targeted high-risk or priority populations (e.g. historic hot spots)
- PVS activities: years in which PVS activities were conducted, type of surveillance activities conducted, frequency of activities, sampling design (targeted or population-representative), surveillance type (active, passive, sentinel), type of testing (antigen, antibody, microfilaria, MX/PCR of mosquito samples), other activities (including risk reduction and vector management)
- Operational challenges or enablers: PVS activity funding sources; staffing and resources; technical capacity; and social, political, or economic drivers of PVS program implementation
2.4. Analysis
A deductive content analysis of the extracted data was conducted using the method developed by Elo and Kyngas (2008) [24]. A deductive approach was selected due to its applicability in testing existing models in different contexts [24]. In this case, this approach was used to examine the application of PVS strategies recommended by WHO in 2025 across countries endemic for LF [13]. Deductive coding was conducted using a constrained categorisation matrix using the data extraction fields described above, with a focus on identifying emerging themes relating to alignment with WHO guidelines, operational challenges, and enablers [24]. The analysis sought to capture information about PVS activities by country and challenges or enablers to their implementation. Additionally, the analysis also examined the alignment of documented efforts with WHO guidelines, specifically the number of activities implemented and whether they were sustained; that is, repeated PVS activities implemented over multiple years following validation, as opposed to single or short-term efforts. Further, the analysis sought to contrast approaches used by countries and extracted learnings that can be translated across settings.
Ethical Considerations and Funding
This review did not require ethical approval as it uses published publicly available data. This work was supported by the Operational Research and Decision Support for Infectious Diseases (ODeSI) program, which is funded by The University of Queensland's Health Research Accelerator (HERA) initiative (2021–2028).
3. Results
A total of 328 documents were identified, of which 58 were duplicates. Of the 270 unique documents that remained, 30 met the inclusion criteria. Figure 2 outlines the process of document identification and selection.
The majority of documents (22/30; 73%) were peer-reviewed journal articles and the remainder (n=8) were reports published by the WHO. The documents were published from 2009 to 2025.
Data were reported on PVS activities in 17 countries: Bangladesh [25], Cambodia [26], China [27,28,29,30,31,32,33], Egypt [34], Kiribati [35], Malawi [36], Maldives [34,37,38], Niue [39], Palau [40], South Korea [27,30,41,42], Sri Lanka [19,25,26,34,37,38,43,44,45,46], Thailand [25,34,37,38,47,48], Togo [49,50], Tonga [51], Vanuatu [26], Wallis and Futuna [52] and Yemen [53]. More than half of the countries (53%) for which PVS activities were reported were from the Western Pacific Region (WPR) of WHO.
Of the 23 countries that have eliminated LF as a public health problem, there was no literature found on PVS activities for six (26%) countries: the Cook Islands (which was validated as having eliminated LF in 2016), the Republic of the Marshall Islands (in 2017), Viet Nam (2018), Lao People’s Democratic Republic (2023), Brazil (2024), and Timor Leste (2024) [54].
3.1. Lymphatic Filariasis Elimination
The years in which LF was eliminated ranged from 2007 to 2023. Almost all documents (29/30, 97%) described activities relating to the surveillance of W. bancrofti in all 17 countries represented in the study. 18 of 39 documents (60%) described activities relating to Brugia spp. in Sri Lanka, China, South Korea and Thailand.
The average time between elimination and the first reporting of PVS activities was three years (range 0–9 years). This differed by publication type, with WHO reports published on average two years (range 0–5 years) after validation of elimination, while journal articles were available on average of six years’ delay (range 1–10 years).
3.2. Post-Validation Surveillance Activities
The PVS strategies described in the literature are summarised below in Table 1 by country. These include both WHO-recommended and other PVS activities. Other PVS activities included vector surveys (monitoring of mosquitos without further dissection or polymerase-chain reaction (PCR) testing for filarial DNA) and animal reservoir surveys of dogs and cats (reservoirs for Brugia spp.)[55].
WHO-Recommended PVS Strategies
Of the WHO-recommended strategies, targeted surveillance [19,25,26,27,29,30,32,33,37,38,40,43,44,45,47,48,50,51,52,56,57] and integration of PVS into existing population surveys [25,26,35,37,38,39,53,58] were the most common, described in ten and nine countries respectively. These were followed by MX (seven countries) [25,26,35,37,38,39,53,58] and health facility-based screening (four countries) [25,26,27,30,33,37,38,41,42,43,48,49,50,52]. However, a combination of the WHO-recommended strategies was described in more than half (nine) of the countries. The most common combination reported was targeted surveillance and MX, described in six countries [25,26,27,30,33,37,38,43,48,50].
Single PVS strategies were described in five countries: Malawi, Egypt, Kiribati, Niue, and Vanuatu. Kiribati, Niue, and Vanuatu reported integrating LF surveillance into other existing population-based surveillance programs, though the specific programs were not described in the literature [26,35,39]. Malawi and Egypt reported MMDP programs, but did not specify whether surveillance activities were conducted [36,56].
Documents described activities in nine countries that targeted ‘hotspots’; these were higher-risk areas that were generally formerly endemic regions with higher baseline LF prevalence [19,25,26,27,30,32,33,37,42,43,44,45,48,49,51,52]. Nine countries conducted targeted surveys of migrants from endemic countries [25,28,29,30,37,38,39,40,41,47,48,50,56]. LF surveillance was integrated into surveys for NCDs (such as the WHO STEPwise survey in Niue [39]), other NTDs such as trachoma and vaccine-preventable diseases such as tetanus [26]. Additionally, MX for LF was integrated into dengue surveillance programs in Sri Lanka [37].
Tonga, China, Bangladesh and Wallis and Futuna employed health-facility based testing. LF testing was integrated into routine checkups at a diabetes clinic in Tonga [51]; in Wallis and Futuna, the diagnosis of patients with lymphoedema and hypereosinophilia prompted a review of medical records and subsequent survey of children under 18 on the island of Futuna [52]. Other passive health-facility based surveillance was noted to have been conducted in China and Bangladesh, though the literature did not describe specific activities [50].
MX was described in six countries where it was primarily used to monitor high-risk areas, such as previously endemic provinces with historically high LF prevalence. As noted above, MX was not used as a standalone surveillance method and was generally used in conjunction with targeted surveys in high-risk areas [25,26,27,30,33,37,38,43,48,50].
Other Surveillance Strategies
Six countries used surveillance methods that were not one of the four WHO-recommended strategies. One document from China described the presentation of a symptomatic case triggering reactive case finding in their home district/village [32,57]. Additionally, animal reservoir (cat and dog) surveys were conducted in Brugia endemic regions in Sri Lanka and Thailand [25,38,44,45,48]. Yemen and the Maldives conducted vector surveillance, but did not conduct MX, noting constraints to PCR capabilities [38,53]. Wallis and Futuna identified that patients presenting with lymphoedema also had marked hypereosinophilia; following a review of medical records that identified the prevalence of hypereosinophilia was three times higher in Futuna than in Wallis, a survey of children under 18 on Futuna was triggered, which identified evidence of ongoing LF transmission [52].
3.3. Diagnostic Testing Methods
A mix of diagnostic tests were used in PVS testing, with most countries using a combination of testing methods to validate their findings. The most commonly described was antigen testing using Alere Filariasis Test Strips (FTS), reported by ten countries in W. bancrofti endemic regions [19,27,30,37,38,39,40,43,48,50,51,52,57]. Rapid antibody tests were used in six countries in Brugia spp. endemic regions [19,26,27,30,33,39,43,44,45,48]. Microfilaria testing and MX were used to supplement these testing methods in eight [30,37,38,39,40,45,48,50,51,52,57] and five countries, respectively [26,27,30,33,37,38,42,43,45,49]. Most countries that used antigen testing (with the exception of the Maldives) reported conducting follow-up Mf testing [30,38,39,40,48,50,51,52,57].
3.4. Frequency of PVS
WHO guidelines recommend that PVS should continue for ten years after validation of LF’s elimination, and that data from PVS activities should be submitted annually to WHO; however, when PVS should commence, its frequency or methods are not stipulated [15]. Nine countries conducted one-off activities only (PVS activities that occurred over a single instance or over a short, defined period, rather than as part of an ongoing program): Malawi [36], Togo [49,50], Yemen [53,56], Kiribati [35], Niue [39], Palau [40], Tonga [51], Wallis and Futuna [52] and Vanuatu [26]. Sustained surveillance (repeated PVS activities implemented over multiple years) after validation of elimination was reported in six countries: the Maldives [25,37,38,56], Sri Lanka [25,37,38,46], Thailand [25,37,38,47,48,56], Cambodia [26], China [27,28,29,30,31,32,33], and South Korea [41]. The strategies used for sustained surveillance were reported as: targeted surveys in formerly endemic areas [25,27,29,30,32,33,34,37,38,47,48], migrant screening [25,28,29,30,34,37,38,41,47,48], and MX/vector surveillance or animal reservoir screening [25,27,33,37,38,41,48].
However, the identification of sustained or one-off surveillance should be interpreted cautiously: for example, Togo implemented multiple PVS approaches across three years, which does not constitute sustained surveillance for any single method but is reflective of continued, repeated PVS efforts [49,50]. Similarly, for countries like Tonga, where PVS was only conducted in 2024 and findings published in 2025, it is too early to determine future activities [51]. In addition, the frequency and continuity of PVS are difficult to assess from published literature alone, as academic and grey literature are incomplete and often lack detail on timing and repetition of activities, or the future plans of national programs.
3.5. Health System Constraints and Enablers
Eight countries cited financing constraints as a major barrier to PVS implementation, raising concerns about program sustainability [25,26,36,37,38,49,51]. For example, a 2017 WHO report noted that in Cambodia and Vanuatu, there was no national or international funding for PVS, raising concerns about long-term sustainability due to reliance on external donors [26]. Budget reductions were also described in Thailand, which has conducted sustained PVS since LF’s elimination in 2016; however, consistent funding from both the Thai national government and the WHO were also noted [25,37,38].
Issues relating to health workforce were reported in seven countries [25,26,36,37,38,46,49]. Countries reported significant limitations to technical capacity, such as limited access to laboratories capable of conducting enzyme-linked immunosorbent assay (ELISA) and PCR testing required for LF antibody detection and MX, respectively [26,38]. Shortages of specialist staff can particularly affect MX implementation, due to the requirement for trained entomologists [49]. High staff turnover also affected the quality of MMDP services [36].
Six countries faced challenges in the timely procurement of rapid diagnostic tests (RDTs), ELISA, and PCR testing supplies [25,26,37,38,49]. RDTs were generally not readily available in countries and had to be procured from the WHO; this particularly impacted small island nations, as WHO processes are challenging for the procurement of small quantities [25,38].
Documents from China, Sri Lanka, Thailand, and Tonga commented on the absence or ambiguity of PVS guidelines, including lack of recommendations on the frequency or duration of PVS and the thresholds for determining sustained elimination [25,26,27,43,44,51]. These documents were published between 2009 and 2025, noting that the latest guidelines on PVS were published in May 2025.
Six countries described enabling factors that strengthened program sustainability. Notably, Sri Lanka, South Korea, the Maldives, China, and Thailand included LF and other NTDs in national health policies and strategies [25,31,32,38,41]. Other activities included regular education of health professionals on LF surveillance and treatment [25,38,41], the development of databases to monitor LF [19,25,31,38,41], building specialist facilities for MMDP [33], and community health education [25,33].
Table 2.
Number of documents in which health system constraints and enablers of PVS were described, by country of activity.
Table 2.
Number of documents in which health system constraints and enablers of PVS were described, by country of activity.
| WHO region | Country | Constraints | Enablers | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Financing | Health workforce & technical capacity | Accessing PVS diagnostic tools and supplies | Policies and guidelines | Policies and guidelines | Health workforce & technical capacity | Infrastructure development | Data development | Health education | ||
| AFRO | Malawi | 1 | 1 | |||||||
| Togo | 1 | 1 | 1 | |||||||
| SEAR | Bangladesh | 1 | 1 | 1 | ||||||
| Maldives | 1 | 2 | 1 | 1 | ||||||
| Sri Lanka | 1 | 2 | 1 | 3 | 2 | 1 | 2 | |||
| Thailand | 3 | 1 | 2 | 1 | 1 | 1 | ||||
| WPRO | Cambodia | 1 | 1 | 1 | ||||||
| China | 1 | 2 | 1 | 1 | 1 | |||||
| South Korea | 1 | 1 | 1 | |||||||
| Tonga | 1 | 1 | ||||||||
| Vanuatu | 1 | 1 | 1 | |||||||
| No. documents describing theme | 10 | 9 | 8 | 6 | 7 | 3 | 1 | 6 | 2 | |
| No. countries in which theme occurred | 8 | 7 | 6 | 4 | 5 | 3 | 1 | 5 | 2 | |
Table 3.
Summary of documents reporting PVS activities.
| Country | Year LF eliminated | WHO region | Type of LF | Reference | Year published | Activities | Priority populations* | Years conducted |
|---|---|---|---|---|---|---|---|---|
| China | 2007 | WPR | W. bancrofti, B. malayi | Sun et al. [32] | 2020 | Targeted surveys | Historic hotspots | 2008 |
| W. bancrofti, B. malayi | Huang et al. [33] | 2020 | Targeted surveys, MX; MMDP | Historic hotspots | 1982–1992^ | |||
| W. bancrofti, B. malayi | Qian et al. [31] | 2019 | Health-facility based passive surveillance | Population-wide | 1980 onwards^ | |||
| W. bancrofti, B. malayi | WHO [30] | 2018 | Targeted surveys; passive surveillance | Migrants from endemic countries | 2007 onwards | |||
| W. bancrofti, B. malayi | Yang et al. [29] | 2014 | Targeted surveys, MMDP (incl. the establishment of new facilities) | Migrants from endemic countries | 2007 onwards | |||
| W. bancrofti, B. malayi | Sudomo et al. [28] | 2010 | MMDP | Migrants from endemic countries | 2007 onwards | |||
| W. bancrofti, B. malayi | WHO [27] | 2009 | Targeted surveys; MX; MMDP | Areas known to have weak surveillance systems and/or symptomatic cases, migrants from endemic countries | 2007 onwards | |||
| South Korea | 2008 | WPR | B. malayi | Riches et al. [42] | 2020 | MX | Historic hotspots | 2011 |
| W. bancrofti, B. malayi | Bahk et al. [30] | 2018 | Sentinel surveillance | Migrants from endemic countries | Unspecified | |||
| B. malayi | WHO [30] | 2018 | Targeted surveys; MX | Historic hotspots | School surveys 2009–2011; MX 2008 onwards | |||
| W. bancrofti, B. malayi | WHO [27] | 2009 | Targeted surveys; MX | Historic hotspots | 2009 | |||
| Cambodia | 2016 | WPR | W. bancrofti | WHO [26] | 2017 | Integrated surveillance | Historic hotspots | Unspecified |
| Maldives | 2016 | SEAR | W. bancrofti | WHO [25] | 2025 | School-based surveys, targeted surveys | Migrants from endemic countries | 2016 onwards |
| W. bancrofti | WHO [34] | 2024 | Targeted surveys | Historic hotspots; migrants from endemic countries | 2016 onwards | |||
| W. bancrofti | WHO [38] | 2023 | Targeted surveys, integrated surveillance, integrated MX, MMDP | Migrants from endemic countries | 2016 onwards | |||
| W. bancrofti | WHO [37] | 2020 | Targeted surveys; integrated MX | Migrants from endemic countries | 2016 onwards | |||
| Niue | 2016 | WPR | W. bancrofti | Craig et al. [39] | 2025 | Integration into STEPs | Migrants from endemic countries | 2024 |
| Sri Lanka | 2016 | SEAR | W. bancrofti, B. malayi | WHO [25] | 2025 | Targeted surveys, MX | Unspecified | 2017 onwards |
| W. bancrofti, B. malayi | WHO [34] | 2024 | Targeted surveys | Historic hotspots; migrants from endemic countries | Unspecified | |||
| W. bancrofti, B. malayi | Gunaratna et al. [46] | 2024 | MMDP | Unspecified | 2016 onwards | |||
| W. bancrofti, B. malayi | WHO [38] | 2023 | Targeted surveys, MX | Migrants from endemic countries | 2016 onwards | |||
| W. bancrofti, B. malayi | Mallawarachchi et al. [45] | 2021 | Targeted surveys, MX, cat and dog serosurveys | Historic hotspots | After 2018 (years unspecified) | |||
| B. malayi | WHO [37] | 2020 | Targeted surveys, integrated MX, MMDP | Migrants from endemic countries | Unspecified | |||
| W. bancrofti, B. malayi | Rahman et al. [19] | 2019 | Targeted surveys | Historic hotspots | 2018 | |||
| B. malayi | Mallawarachchi et al. [44] | 2018 | Targeted surveys; dog serosurveys | Historic hotspots | 2016–2017 | |||
| W. bancrofti, B. malayi | WHO [26] | 2017 | Targeted surveys | Historic hotspots | 2017 onwards | |||
| W. bancrofti | Rao et al. [43] | 2017 | Targeted surveys; MX | Historic hotspots | 2015–2017 | |||
| Vanuatu | 2016 | WPR | W. bancrofti | WHO [26] | 2017 | Integrated surveillance | Unspecified | Unspecified |
| Thailand | 2017 | WPR | W. bancrofti, B. malayi | WHO [25] | 2025 | Targeted surveys, cat serosurveys, integration with NCD screening | Migrants from endemic countries | 2017 onwards |
| W. bancrofti, B. malayi | WHO [34] | 2024 | Targeted surveys | Historic hotspots; migrants from endemic countries | 2017 onwards | |||
| W. bancrofti, B. malayi | Meetham et al. [48] | 2023 | Targeted surveys, cat serosurveys | Historic hotspots; migrants from endemic countries | 2017 onwards | |||
| W. bancrofti, B. malayi | WHO [38] | 2023 | Targeted surveys, MX, cat serosurveys | Migrants from endemic countries | 2017 onwards | |||
| W. bancrofti, B. malayi | Bizhani et al. [47] | 2021 | Targeted surveys | Migrants from endemic countries | 2017 onwards | |||
| B. malayi | WHO [37] | 2020 | Targeted surveys, MX | Historic hotspots, migrants from endemic countries | 2017 onwards | |||
| Togo | 2017 | AFR | W. bancrofti | Dorkenoo et al. [50] | 2021 | Targeted surveys, MX, MMDP, cat serosurveys | Migrants from endemic countries | 2018 |
| W. bancrofti | Dorkenoo et al. [49] | 2018 | MX | Historic hotspots | 2016–2017 | |||
| Tonga | 2017 | WPR | W. bancrofti | Lawford et al. [51] | 2025 | Targeted surveys, health-facility based screening | Historic hotspots | 2024 |
| Egypt | 2018 | EMR | W. bancrofti | WHO [34] | 2024 | Unspecified PVS, MMDP | Unspecified | After 2018 (years unknown) |
| Palau | 2018 | WPR | W. bancrofti | WHO [40] | 2020 | Targeted surveys | Migrants from endemic countries | 2017 onwards |
| Wallis and Futuna | 2015 | WPR | W. bancrofti | Couteaux et al. [52] | 2025 | Targeted surveys; health-facility based screening | Areas with greater prevalence of hypereosinophilia | 2024 |
| Kiribati | 2019 | WPR | W. bancrofti | WHO [35] | 2023 | Integrated surveillance | Unspecified | Unspecified |
| Yemen | 2019 | EMR | W. bancrofti | WHO [34] | 2024 | Unspecified PVS, MMDP | Unspecified | After 2019 (years unknown) |
| W. bancrofti | WHO [53] | 2022 | Integrated surveillance and MX, MMDP | Unspecified | Unknown | |||
| Malawi | 2020 | AFR | W. bancrofti | Barrett et al. [36] | 2024 | MMDP | Unspecified | 2020 onwards |
| Bangladesh | 2023 | SEAR | W. bancrofti | WHO [25] | 2025 | Targeted surveys, health-facility based screening | Historic hotspots; areas of low socioeconomic status | 2023 onwards |
*This column identifies whether priority populations were included in surveillance activities – however sampling may not be limited to these groups. ^Describes surveillance activities that took place at a provincial level after elimination within that province, but prior to validation of elimination at a national level.
4. Discussion
This review synthesised 30 documents reporting PVS activities in 17 of the 23 countries and territories validated by WHO as having eliminated LF. An overarching theme in our extracted documents was the tension between constraints to establishing PVS programs, and the need for active case finding due to LF’s long asymptomatic incubation period, and low prevalence in a post-validation context.
Of the new WHO-recommended strategies released in 2025 (at the end of this review’s study period) in the guidelines for Monitoring and epidemiological assessment of mass drug administration in the global programme to eliminate lymphatic filariasis [13], the literature most commonly reports implementation of targeted surveys focusing on migrants or previous hotspots, in combination with MX or vector surveillance. These approaches were already being implemented before the release of the guidelines, suggesting that countries were pragmatically balancing epidemiological need with resource availability and opportunity. Targeted surveillance was also considered cost-effective, as it concentrates efforts on higher-risk areas and populations most likely to require more intensive follow-up [59,60,61].
While integration of PVS into existing health programs and health-facility based screening were also described, single-disease, siloed approaches to PVS were reported in several countries included in our study. In the context of constrained resources, this suggests that integration of LF surveillance may be an underutilised opportunity to address the WHO requirement to sustain PVS for ten years. A qualitative study conducted by Craig et. al. found that, among Pacific Island country and territory representatives, integration was seen to be well-suited to small island contexts due to their effective use of limited resources and reducing burden on surveyed communities; opportunities identified for integration included other seroprevalence surveys (e.g. to monitor vaccine-preventable diseases), screening programs for NCDs, as well as implementing enhanced surveillance through investigating eosinophilia cases identified through routine blood testing [52,62].
However, some documents reinforced the importance of considering each country’s epidemiological context when selecting programs for integration. In Togo, for example, where the primary risk of LF resurgence stems from cross-border reintroduction, passive laboratory-based surveillance was found to be less effective than targeted surveys conducted in border regions with large migrant populations [50]. Similarly, in Tonga, targeted surveys in remote outer islands identified high-prevalence clusters, whereas no positive cases were detected through screening at a diabetes clinic in the capital, an urban setting less likely to capture individuals from remote communities [51]. These findings underscore the importance of context when designing PVS strategies, particularly where transmission risk is localised or linked to specific populations.
The most commonly reported challenges to PVS implementation were financing constraints [25,26,36,37,38,49], limited technical capacity [26,36,38,46,49], and supply chain issues [25,26,37,38,49]. These were particularly notable among reports related to small island nations and low-income settings [25,26,36,37,38,49], where reliance on external donors’ support and limited laboratory infrastructure hindered sustained surveillance. Addressing these challenges requires strengthening health system capacity, through assessing financing models, improving access to technical support, and the availability of essential equipment. Development partners, including donors, are well-positioned to assist countries to overcome these barriers in the short-to-medium term. We also note that ad-hoc approaches do little to strengthen health systems; examining the approach of countries where PVS has been embedded in national health strategies and supported by domestic financing (namely Sri Lanka, the Republic of Korea, China, and Thailand) will provide valuable insights into how surveillance can be designed for long-term sustainability.
Financing constraints likely underpinned other findings we observed across countries, many of which were low- and middle-income, and/or had small populations and workforces. For example, in more than half of the countries represented in our review, we only identified evidence for one-off PVS activities; the WHO recommends that PVS should continue for at least ten years, though it does not specify the frequency of interventions [13]. Financing constraints may also account for only a single PVS strategy being described in some countries; while the latest PVS guidelines recommend that at least two PVS activities are used, we note that this review describes activities that largely take place prior to the guidelines’ release [13]. In settings where resources are stretched, program managers may prioritise approaches that are feasible within existing budgets, even if these do not fully align with international guidance. These findings highlight the need for sustainable financing mechanisms that are cognisant of contextual challenges to support robust PVS.
Conversely, Sri Lanka, South Korea, China, and Thailand stood out as countries reporting robust and sustained PVS systems, utilising a combination of surveillance strategies. In these four countries, efforts to build governance and program sustainability were evident, notably through the inclusion of LF and other NTDs in national budgets, national health strategies, and a commitment to ongoing implementation [25,32,38,41,48]. These examples suggest that institutional commitment and governance structures are critical enablers of long-term surveillance.
It is important to note that the integration of LF into national health agendas often depends on the availability of clear international guidance. Multiple publications reported difficulties stemming from the absence or ambiguity of PVS guidelines [25,26,27,43,44,51]. Most countries were validated as having eliminated LF as a public health problem between 2016 and 2018; WHO guidelines on specific PVS strategies to use were published in 2025, nearly a decade into many countries’ post-validation phases [13]. Timely guidance is essential to provide a framework for countries to refer to when developing national surveillance strategies.
Now that the 2025 PVS guidelines are available, the next critical steps will involve translating these recommendations into actionable strategies fit for each countries’ unique context. This may involve supporting countries to assess epidemiological information, consider context and resource availability, and design appropriate PVS strategies. To ensure community and political support to drive PVS, continued advocacy will be required to stakeholders including policymakers, development agencies and other international partners. Additionally, the forthcoming WHO Integrated Surveillance Planning Toolkit for Neglected Tropical Diseases in Post-Validation or Verification Settings will provide practical guidance to help countries design integrated, risk-based surveillance strategies [63]. Leveraging such tools can support evidence-based planning, facilitate resource mobilisation, and promote integration with existing health systems, reducing costs and operational burden while strengthening sustainability.
A key limitation of our study is that it relied on publicly accessible documented evidence of PVS, and that grey literature searches were limited to the WHO IRIS database. In all likelihood, some activities have been conducted but are yet to be reported; this limits the insights that were able to be drawn, particularly about the longevity of PVS activities. Conversely, the absence of literature about PVS from six countries that have eliminated LF as a public health problem raises the question as to whether PVS has been conducted. This limits opportunities for cross-country learning and highlights the need for operational research and reflective practice to inform future surveillance strategies, particularly as countries interpret and implement the 2025 WHO PVS guidelines.
5. Conclusions
Our review demonstrates that LF PVS is implemented with considerable variation across countries and territories, shaped by differences in epidemiological risk, health system capacity, and resource availability. Targeted surveys and MX were the most frequently reported PVS strategies used, while integration with existing standardised population surveys and health facility-based screening were less commonly reported. Financing and resource constraints underpinned many challenges to PVS implementation, affecting the scope and longevity of surveillance programs.
Countries with more sustained and integrated approaches to PVS demonstrate how institutional commitment and governance structures are critical enablers of sustained surveillance. The findings also highlight the importance of timely international guidance, particularly given the lag between LF validation and the release of WHO’s 2025 PVS recommendations. Strengthening national ownership, improving integration with existing health systems, and ensuring access to technical and financial resources will be essential to maintaining LF elimination and preventing resurgence.
Author Contributions
Conceptualisation AC, HL, HJ; Methodology HJ, HL; Study screening and selection HJ, HL; Data extraction and analysis HJ, HL; Writing (original draft preparation) HJ; Writing (review and editing) HL, AC, AM, CL; Supervision AC, CL, AM.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AFR | WHO African Region |
| AMR | WHO Region of the Americas |
| DALY | disability-adjusted life-years |
| ELISA | enzyme-linked immunosorbent assay |
| EMR | WHO Eastern Mediterranean Region |
| FTS | Filarial test strip |
| GBD | Global Burden of Disease |
| GPELF | Global Program for the Elimination of Lymphatic Filariasis |
| HERA | The University of Queensland's Health Research Accelerator initiative |
| IRIS | WHO Institutional Repository for Information Sharing |
| Lao PDR | Lao People’s Democratic Republic |
| LF | Lymphatic filariasis |
| MDA | Mass drug administration |
| MMDP | Morbidity management and disability prevention |
| MX | Molecular xenomonitoring |
| NCD | Non-communicable disease |
| NTD | Neglected tropical disease |
| PCR | Polymerase chain reaction |
| PICOT | The Population, Intervention/Exposure, Comparator, Outcome and Time framework |
| PRISMA | Preferred Reporting Items for Systematic reviews and Meta-Analyses guidelines |
| PVS | Post-validation surveillance |
| RDT | Rapid diagnostic test |
| RMI | Republic of the Marshall Islands |
| SEAR | WHO South-East Asian Region |
| STEPs | WHO STEPwise approach to non-communicable disease risk factor survey |
| TAS | Transmission assessment survey |
| USD | United States dollars |
| WHO | World Health Organization |
| WPR | WHO Western Pacific Region |
Appendix A: Search Terms by Database
| Database | Search terms |
| PubMed | ("Bangladesh"[Mesh] OR Bangladesh* OR "Cambodia"[Mesh] OR Cambodia* OR Cook Island* OR "Egypt"[Mesh] OR Egypt* OR Kiribati* OR "I-Kiribati" OR "Laos"[Mesh] OR Laos OR "Malawi"[Mesh] OR Malawi* OR Maldiv* OR Marshall Island* OR Niue* OR Palau* OR "Sri Lanka"[Mesh] OR Sri Lanka* OR "Thailand"[Mesh] OR Thai* OR "Togo"[Mesh] OR Togo* OR Tonga* OR Vanuatu* OR "Vietnam"[Mesh] OR Vietnam* OR "Yemen"[Mesh] OR Yemen* OR "Wallis and Futuna" OR Wallis* OR Futuna* OR "Brazil"[Mesh] OR Brazil* OR "Timor-Leste"[Mesh] OR Timor*) AND ("Elephantiasis, Filarial"[Mesh] OR "lymphatic filariasis" OR elephantias* OR filaria* OR "filarial elephantiasis" OR filarial lympho*dema OR "Wuchereria bancrofti" OR "Brugia malayi" OR "Brugia timori" OR Bancrofti* OR Brugia*) AND ("Sentinel Surveillance"[Mesh] OR "sentinel surveillance" OR "Public Health Surveillance"[Mesh] OR "public health surveillance" OR "Population Surveillance"[Mesh] OR "population surveillance" OR "Monitoring, Physiologic"[Mesh] OR "physiologic monitoring" OR "Epidemiological Monitoring"[Mesh] OR "epidemiological monitoring" OR "Mass Screening"[Mesh] OR "mass screening") AND ("post-elimination" OR "post-validation" OR elimination OR validation) AND (PUBYEAR > 2006 AND PUBYEAR < 2026) |
| Scopus | (Bangladesh* OR Cambodia* OR Cook Island* OR Egypt* OR Kiribati* OR “I-Kiribati” OR Lao* OR Malawi* OR Maldiv* OR Marshall Island* OR Niue* OR Palau* OR Sri Lanka* OR Thai* OR Togo* OR Tonga* OR Vanuatu* OR Vietnam* OR Yemen* OR Wallis* OR Futuna* OR Brazil* OR Timor*) AND ("lymphatic filariasis" OR "elephantiasis" OR "filarial elephantiasis" OR "Wuchereria bancrofti" OR "Brugia malayi" OR "Brugia timori" OR "filarial infection”) AND ("sentinel surveillance" OR "public health surveillance" OR "population surveillance" OR "physiologic monitoring" OR "epidemiological monitoring" OR "mass screening") AND ("post-elimination" OR "post-validation" OR elimination OR validation) AND (PUBYEAR > 2006 AND PUBYEAR < 2026) |
| Embase | (Bangladesh* OR Cambodia* OR Cook Island* OR Egypt* OR Kiribati* OR “I-Kiribati” OR Lao* OR Malawi* OR Maldiv* OR Marshall Island* OR Niue* OR Palau* OR Sri Lanka* OR Thai* OR Togo* OR Tonga* OR Vanuatu* OR Vietnam* OR Yemen* OR Wallis* OR Futuna* OR Brazil* OR Timor*) AND ("lymphatic filariasis" OR "elephantiasis" OR "filarial elephantiasis" OR "Wuchereria bancrofti" OR "Brugia malayi" OR "Brugia timori" OR "filarial infection”) AND ("sentinel surveillance" OR "public health surveillance" OR "population surveillance" OR "physiologic monitoring" OR "epidemiological monitoring" OR "mass screening") AND ("post-elimination" OR "post-validation" OR elimination OR validation) AND [2007-2025]/py |
| Web of Science | (Bangladesh* OR Cambodia* OR Cook Island* OR Egypt* OR Kiribati* OR “I-Kiribati” OR Lao* OR Malawi* OR Maldiv* OR Marshall Island* OR Niue* OR Palau* OR Sri Lanka* OR Thai* OR Togo* OR Tonga* OR Vanuatu* OR Vietnam* OR Yemen* OR Wallis* OR Futuna* OR Brazil* OR Timor*) AND ("lymphatic filariasis" OR "elephantiasis" OR "filarial elephantiasis" OR "Wuchereria bancrofti" OR "Brugia malayi" OR "Brugia timori" OR "filarial infection”) AND ("sentinel surveillance" OR "public health surveillance" OR "population surveillance" OR "physiologic monitoring" OR "epidemiological monitoring" OR "mass screening") AND ("post-elimination" OR "post-validation" OR elimination OR validation) AND [2007-2025]/py |
| WHO IRIS | (Bangladesh* OR Cambodia* OR Cook Island* OR Egypt* OR Kiribati* OR “I-Kiribati” OR Lao* OR Malawi* OR Maldiv* OR Marshall Island* OR Niue* OR Palau* OR Sri Lanka* OR Thai* OR Togo* OR Tonga* OR Vanuatu* OR Vietnam* OR Yemen* OR Wallis* OR Futuna* OR Brazil* OR Timor*) AND ("lymphatic filariasis" OR "elephantiasis" OR "filarial elephantiasis" OR "Wuchereria bancrofti" OR "Brugia malayi" OR "Brugia timori" OR "filarial infection”) AND ("sentinel surveillance" OR "public health surveillance" OR "population surveillance" OR "physiologic monitoring" OR "epidemiological monitoring" OR "mass screening") AND ("post-elimination" OR "post-validation") [1] AND Date issued: [2007 TO 2025] |
| 1 The terms ‘validation’ and ‘post-validation’ refer to distinct stages of the elimination process in WHO publications; the terms ‘elimination’ and ‘validation’ were removed when searching this database to maintain specificity. | |
References
- Ichimori, K.; Graves, P.M. Overview of PacELF-the Pacific Programme for the Elimination of Lymphatic Filariasis. Trop Med Health 2017, 45, 34. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Lymphatic Filariasis. Available online: https://www.cdc.gov/dpdx/lymphaticfilariasis/modules/W_bancrofti_LifeCycle_lg.jpg (accessed on 17 October 2025).
- World Health Organization. Lymphatic filariasis (Elephantiasis). Available online: https://www.who.int/data/gho/data/themes/topics/lymphatic-filariasis (accessed on 3/12/2024).
- World Health Organization; Regional Office for South-East. FAQs: Frequently asked questions on Lymphatic Filariasis (elephantiasis); WHO Regional Office for South-East Asia: New Delhi, 2014. [Google Scholar]
- Hofstraat, K.; van Brakel, W.H. Social stigma towards neglected tropical diseases: a systematic review. Int Health 2016, 8, i53–i70. [Google Scholar] [CrossRef]
- Mathew, C.G.; Bettis, A.A.; Chu, B.K.; English, M.; Ottesen, E.A.; Bradley, M.H.; Turner, H.C. The Health and Economic Burdens of Lymphatic Filariasis Prior to Mass Drug Administration Programs. Clin Infect Dis 2020, 70, 2561–2567. [Google Scholar] [CrossRef]
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Ottesen, E.A.; Hooper, P.J.; Bradley, M.; Biswas, G. The Global Programme to Eliminate Lymphatic Filariasis: Health Impact after 8 Years. PLOS Neglected Tropical Diseases 2008, 2, e317. [Google Scholar] [CrossRef]
- World Health Organization. Global Programme to Eliminate Lymphatic Filariasis. Available online: https://www.who.int/teams/control-of-neglected-tropical-diseases/lymphatic-filariasis/global-programme-to-eliminate-lymphatic-filariasis (accessed on 18 September 2025).
- Kapa, D.R.; Mohamed, A.J. Progress and impact of 20 years of a lymphatic filariasis elimination programme in South-East Asia. International Health 2021, 13, S17–S21. [Google Scholar] [CrossRef]
- Deribe, K.; Bakajika, D.K.; Zoure, H.M.G.; Gyapong, J.O.; Molyneux, D.H.; Rebollo, M.P. African regional progress and status of the programme to eliminate lymphatic filariasis: 2000-2020. International Health 2021, 13, S22–S27. [Google Scholar] [CrossRef]
- Collyer, B.S.; Irvine, M.A.; Hollingsworth, T.D.; Bradley, M.; Anderson, R.M. Defining a prevalence level to describe the elimination of Lymphatic Filariasis (LF) transmission and designing monitoring & evaluating (M&E) programmes post the cessation of mass drug administration (MDA). PLoS Negl Trop Dis 2020, 14, e0008644. [Google Scholar] [CrossRef]
- World Health Organisation. Monitoring and epidemiological assessment of mass drug administration in the global programme to eliminate lymphatic filariasis: a manual for national elimination programmes, 2nd ed; World Health Organization: Geneva, Switzerland, 2025. [Google Scholar]
- World Health; O. Ending the neglect to attain the sustainable development goals: a framework for monitoring and evaluating progress of the road map for neglected tropical diseases 2021−2030; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- World Health Organization. Validation of elimination of lymphatic filariasis as a public health problem; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- World Health Organisation. Ending the neglect to attain the Sustainable Development Goals: A road map for neglected tropical diseases 2021–2030; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- World Health Organisation. Global programme to eliminate lymphatic filariasis: Progress report on mass drug administration in 2007; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Craig, A.; Sanikullah, K. Post-validation surveillance for lymphatic filariasis. COR-NTD Meeting for the Pacific Islands 2024 Breakout Reports 2024. [Google Scholar]
- Rahman, M.A.; Yahathugoda, T.C.; Tojo, B.; Premaratne, P.; Nagaoka, F.; Takagi, H.; Kannathasan, S.; Murugananthan, A.; Weerasooriya, M.V.; Itoh, M. A surveillance system for lymphatic filariasis after its elimination in Sri Lanka. PARASITOLOGY INTERNATIONAL 2019, 68, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Lawford, H.; Tukia, O.; Takai, J.; Sheridan, S.L.; Ward, S.; Jian, H.; Martin Mario, B.; 'Ofanoa, R.; Lau, C. Localised Transmission of Lymphatic Filariasis in Tonga Seven Years after Validation of Elimination as a Public Health Problem. Preprints with The Lancet 2024. [Google Scholar] [CrossRef]
- World Health Organization. Lymphatic Filariasis Status of Mass Drug Administration: 2025. Available online: https://apps.who.int/neglected_diseases/ntddata/lf/lf.html (accessed on 20/11/2025).
- Lawford, H.; Jian, H.; Tukia, O.; Takai, J.; Couteaux, C.; Thein, C.; Jetton, K.; Tabunga, T.; Bauro, T.; Nehemia, R.; et al. Barriers and Facilitators to Implementing Post-Validation Surveillance of Lymphatic Filariasis in Pacific Island Countries and Territories: A Conceptual Framework Developed from Qualitative Data. SSRN 2025. [Google Scholar]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Elo, S.; Kyngas, H. The qualitative content analysis process. J Adv Nurs 2008, 62, 107–115. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Meeting of the National Programme Managers and Regional Technical Advisory Group for Lymphatic Filariasis Elimination Kathmandu, Nepal. 25-27 June 2024. Available online: https://www.who.int/publications/i/item/SEA-NCD-111 (accessed on 21/07/2025).
- World Health Organization; Regional Office for the Western Pacific. Informal Consultation on Post-elimination Surveillance of Neglected Tropical Diseases, Siem Reap, Cambodia, 13-14 June 2017: meeting report; WHO Regional Office for the Western Pacific: Manila, 2017. [Google Scholar]
- World Health Organization. Regional Office for the Western Pacific. First Mekong-Plus Programme Managers Workshop on Lymphatic Filariasis and Other Helminthiasis; WHO Regional Office for the Western Pacific: Phnom Penh, Cambodia; Manila, 23-26 March 2009. [Google Scholar]
- Sudomo, M.; Chayabejara, S.; Duong, S.; Hernandez, L.; Wu, W.-P.; Bergquist, R. Chapter 8 - Elimination of Lymphatic Filariasis in Southeast Asia. In Advances in Parasitology; Zhou, X.-N., Bergquist, R., Olveda, R., Utzinger, J., Eds.; Academic Press, 2010; Volume 72, pp. 205–233. [Google Scholar]
- Yang, G.J.; Liu, L.; Zhu, H.R.; Griffiths, S.M.; Tanner, M.; Bergquist, R.; Utzinger, J.; Zhou, X.N. China's sustained drive to eliminate neglected tropical diseases. The Lancet Infectious Diseases 2014, 14, 881–892. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Regional Office for the Western Pacific. Programme Managers Meeting on Neglected Tropical Diseases in the Asia Subregion, Manila, Philippines, 13-14 March 2019 : meeting report. Manila, 2018.
- Qian, M.B.; Chen, J.; Bergquist, R.; Li, Z.J.; Li, S.Z.; Xiao, N.; Utzinger, J.; Zhou, X.N. Neglected tropical diseases in the People's Republic of China: Progress towards elimination. Infectious Diseases of Poverty 2019, 8. [Google Scholar] [CrossRef] [PubMed]
- Sun, D.J.; Fang, Y.; Huang, Y.; Zhang, Y. Contributions to the lymphatic filariasis elimination programme and post-elimination surveillance in China by NIPD-CTDR. Adv Parasitol 2020, 110, 145–183. [Google Scholar] [CrossRef]
- Huang, X.; Deng, X.; Kou, J.; Liu, X.; Wang, H.; Cheng, P.; Gong, M. Elimination of Lymphatic Filariasis in Shandong Province, China, 1957-2015. Vector-Borne and Zoonotic Diseases 2020, 20, 875–881. [Google Scholar] [CrossRef]
- World Health Organization = Organisation mondiale de la; S. Global programme to eliminate lymphatic filariasis: progress report, 2023 = Programme mondial pour l’élimination de la filariose lymphatique: rapport de situation, 2023. Weekly Epidemiological Record = Relevé épidémiologique hebdomadaire 2024, 99, 565–576. [Google Scholar]
- World Health Organization. Global report on neglected tropical diseases 2023; World Health Organization: Geneva, 2023. [Google Scholar]
- Barrett, C.; Chiphwanya, J.; Matipula, D.E.; Douglass, J.; Kelly-Hope, L.A.; Dean, L. Addressing the Syndemic Relationship between Lymphatic Filariasis and Mental Distress in Malawi: The Potential of Enhanced Self-Care. Trop Med Infect Dis 2024, 9. [Google Scholar] [CrossRef]
- World Health Organization; Regional Office for South-East. Report on the virtual meeting of the regional programme review group (RPRG) for lymphatic filariasis, soil-transmitted helminthiasis and schistosomiasis in the WHO South-East Asia Region; World Health Organization. Regional Office for South-East Asia: New Delhi, 2020. [Google Scholar]
- World Health, Organization. Regional Office for South-East, A. Meeting of National Programme Managers for lymphatic filariasis, soil-transmitted helminthiasis and schistosomiasis and the Regional Programme Review Group of the WHO South-East Asia Region. New Delhi, 2023.
- Craig, A.T.; Lawford, H.; Mokoia, G.; Ikimau, M.; Fetaui, P.; Marqardt, T.; Lau, C.L. Integrating post-validation surveillance of lymphatic filariasis with the WHO STEPwise approach to non-communicable disease risk factor surveillance in Niue, a study protocol. PLoS One 2025, 20, e0315625. [Google Scholar] [CrossRef]
- World Health Organization. Programme Managers Meeting on Neglected Tropical Diseases (NTD) in the Pacific, Nadi, Fiji, 20-22 February 2018 : meeting report. 2020.
- Bahk, Y.Y.; Shin, E.H.; Cho, S.H.; Ju, J.W.; Chai, J.Y.; Kim, T.S. Prevention and control strategies for parasitic infections in the Korea centers for disease control and prevention. Korean Journal of Parasitology 2018, 56, 401–408. [Google Scholar] [CrossRef]
- Riches, N.; Badia-Rius, X.; Mzilahowa, T.; Kelly-Hope, L.A. A systematic review of alternative surveillance approaches for lymphatic filariasis in low prevalence settings: Implications for post-validation settings. PLoS Negl Trop Dis 2020, 14, e0008289. [Google Scholar] [CrossRef]
- Rao, R.U.; Samarasekera, S.D.; Nagodavithana, K.C.; Dassanayaka, T.D.M.; Punchihewa, M.W.; Ranasinghe, U.S.B.; Weil, G.J. Reassessment of areas with persistent Lymphatic Filariasis nine years after cessation of mass drug administration in Sri Lanka. PLoS Neglected Tropical Diseases 2017, 11. [Google Scholar] [CrossRef]
- Mallawarachchi, C.H.; Nilmini Chandrasena, T.G.A.; Premaratna, R.; Mallawarachchi, S.; de Silva, N.R. Human infection with sub-periodic Brugia spp. in Gampaha District, Sri Lanka: a threat to filariasis elimination status? Parasit Vectors 2018, 11, 68. [Google Scholar] [CrossRef]
- Mallawarachchi, C.H.; Chandrasena, T.; Withanage, G.P.; Premarathna, R.; Mallawarachchi, S.; Gunawardane, N.Y.; Dasanayake, R.S.; Gunarathna, D.; de Silva, N.R. Molecular Characterization of a Reemergent Brugia malayi Parasite in Sri Lanka, Suggestive of a Novel Strain. Biomed Res Int 2021, 2021, 9926101. [Google Scholar] [CrossRef]
- Gunaratna, I.E.; Chandrasena, N.; Vallipuranathan, M.; Premaratna, R.; Ediriweera, D.; de Silva, N.R. The impact of the National Programme to Eliminate Lymphatic Filariasis on filariasis morbidity in Sri Lanka: Comparison of current status with retrospective data following the elimination of lymphatic filariasis as a public health problem. PLoS Negl Trop Dis 2024, 18, e0012343. [Google Scholar] [CrossRef]
- Bizhani, N.; Hashemi Hafshejani, S.; Mohammadi, N.; Rezaei, M.; Rokni, M.B. Lymphatic filariasis in Asia: a systematic review and meta-analysis. Parasitol Res 2021, 120, 411–422. [Google Scholar] [CrossRef]
- Meetham, P.; Kumlert, R.; Gopinath, D.; Yongchaitrakul, S.; Tootong, T.; Rojanapanus, S.; Padungtod, C. Five years of post-validation surveillance of lymphatic filariasis in Thailand. INFECTIOUS DISEASES OF POVERTY 2023, 12. [Google Scholar] [CrossRef]
- Dorkenoo, M.A.; de Souza, D.K.; Apetogbo, Y.; Oboussoumi, K.; Yehadji, D.; Tchalim, M.; Etassoli, S.; Koudou, B.; Ketoh, G.K.; Sodahlon, Y.; et al. Molecular xenomonitoring for post-validation surveillance of lymphatic filariasis in Togo: no evidence for active transmission. Parasit Vectors 2018, 11, 52. [Google Scholar] [CrossRef]
- Dorkenoo, M.A.; Tchankoni, M.K.; Yehadji, D.; Yakpa, K.; Tchalim, M.; Sossou, E.; Bronzan, R.; Ekouevi, D.K. Monitoring migrant groups as a post-validation surveillance approach to contain the potential reemergence of lymphatic filariasis in Togo. Parasit Vectors 2021, 14, 134. [Google Scholar] [CrossRef]
- Lawford, H.L.S.; Tukia, O.; Takai, J.; Sheridan, S.; Ward, S.; Jian, H.; Martin, B.M.; Ofanoa, R.; Lau, C.L. Persistent lymphatic filariasis transmission seven years after validation of elimination as a public health problem: a cross-sectional study in Tonga. The Lancet Regional Health - Western Pacific 2025, 57. [Google Scholar] [CrossRef]
- Couteaux, C.; Demaneuf, T.; Bien, L.; Munoz, M.; Worms, B.; Chesimar, S.; Takala, G.; Lie, A.; Jessop, V.; Selemago, M.K.; et al. Postelimination Cluster of Lymphatic Filariasis, Futuna, 2024. Emerg Infect Dis 2025, 31, 488–496. [Google Scholar] [CrossRef]
- World Health Organization. Regional Office for the Eastern, M. Summary report on the twentieth meeting of the Regional Programme Review Group and national neglected tropical diseases programme managers, virtual meeting; WHO Regional Office for the Eastern Mediterranean: Cairo, Egypt, 2022. [Google Scholar]
- World Health Organization. PCT Databank - Lymphatic filariasis. Available online: https://www.who.int/teams/control-of-neglected-tropical-diseases/data-platforms/pct-databank/lymphatic-filariasis (accessed on 2 September 2025).
- Naing, C.; Whittaker, M.A.; Tung, W.S.; Aung, H.; Mak, J.W. Prevalence of zoonotic (brugian) filariasis in Asia: A proportional meta-analysis. Acta Trop 2024, 249, 107049. [Google Scholar] [CrossRef]
- World Health Organization = Organisation mondiale de la; S. Global programme to eliminate lymphatic filariasis: progress report, 2022 – Programme mondial pour l’élimination de la filariose lymphatique: rapport de situation, 2022. Weekly Epidemiological Record = Relevé épidémiologique hebdomadaire 2023, 98, 489–501. [Google Scholar]
- Harrington, H.; Asugeni, J.; Jimuru, C.; Gwalaa, J.; Ribeyro, E.; Bradbury, R.; Joseph, H.; Melrose, W.; MacLaren, D.; Speare, R. A practical strategy for responding to a case of lymphatic filariasis post-elimination in Pacific Islands. Parasit Vectors 2013, 6, 218. [Google Scholar] [CrossRef] [PubMed]
- Badia-Rius, X.; Adamou, S.; Taylor, M.J.; Kelly-Hope, L.A. Morbidity hotspot surveillance: A novel approach to detect lymphatic filariasis transmission in non-endemic areas of the Tillabéry region of Niger. Parasite Epidemiology and Control 2023, 21. [Google Scholar] [CrossRef] [PubMed]
- Joseph, H.; Moloney, J.; Maiava, F.; McClintock, S.; Lammie, P.; Melrose, W. First evidence of spatial clustering of lymphatic filariasis in an Aedes polynesiensis endemic area. Acta Trop 2011, 120 Suppl 1, S39–S47. [Google Scholar] [CrossRef]
- Washington, C.H.; Radday, J.; Streit, T.G.; Boyd, H.A.; Beach, M.J.; Addiss, D.G.; Lovince, R.; Lovegrove, M.C.; Lafontant, J.G.; Lammie, P.J.; et al. Spatial clustering of filarial transmission before and after a Mass Drug Administration in a setting of low infection prevalence. Filaria Journal 2004, 3, 3. [Google Scholar] [CrossRef]
- Lau, C.L.; Won, K.Y.; Becker, L.; Soares Magalhaes, R.J.; Fuimaono, S.; Melrose, W.; Lammie, P.J.; Graves, P.M. Seroprevalence and Spatial Epidemiology of Lymphatic Filariasis in American Samoa after Successful Mass Drug Administration. PLoS Neglected Tropical Diseases 2014, 8. [Google Scholar] [CrossRef]
- 6Craig, A.C., Clément; Jetton, Ken; Nehemia, Roger; Sokana, Oliver; Tong, Tanebu; Bauro, Temea; Baratio, Taulanga; Tukia, Ofa; Takai, Joseph; Viali, Satupaitea; Gama Soares, Noel; Ome-Kaius, Maria; Yohogu, Mary; Volavola, Litiana; Tatui, Patricia; Taleo, Fasihah; Saketa, Sala; Tucker, Andie; Mackenzie, Charles; Gass, Katherine; Jian, Holly; Lau, Colleen; Lawford, Harriet. Enablers of Post-Validation Surveillance for Lymphatic Filariasis in the Pacific Islands: A Nominal Group Technique and Expert Elicitation. Preprints with The Lancet, 2025.
- PATH. Landscaping report: Integrated surveillance planning toolkit for neglected tropical diseases in post–validation or verification settings; PATH: Seattle, USA, 2023. [Google Scholar]
Figure 1.
Status of LF elimination as a public health problem in endemic countries, 2025. Data source: World Health Organization [21].
Figure 1.
Status of LF elimination as a public health problem in endemic countries, 2025. Data source: World Health Organization [21].
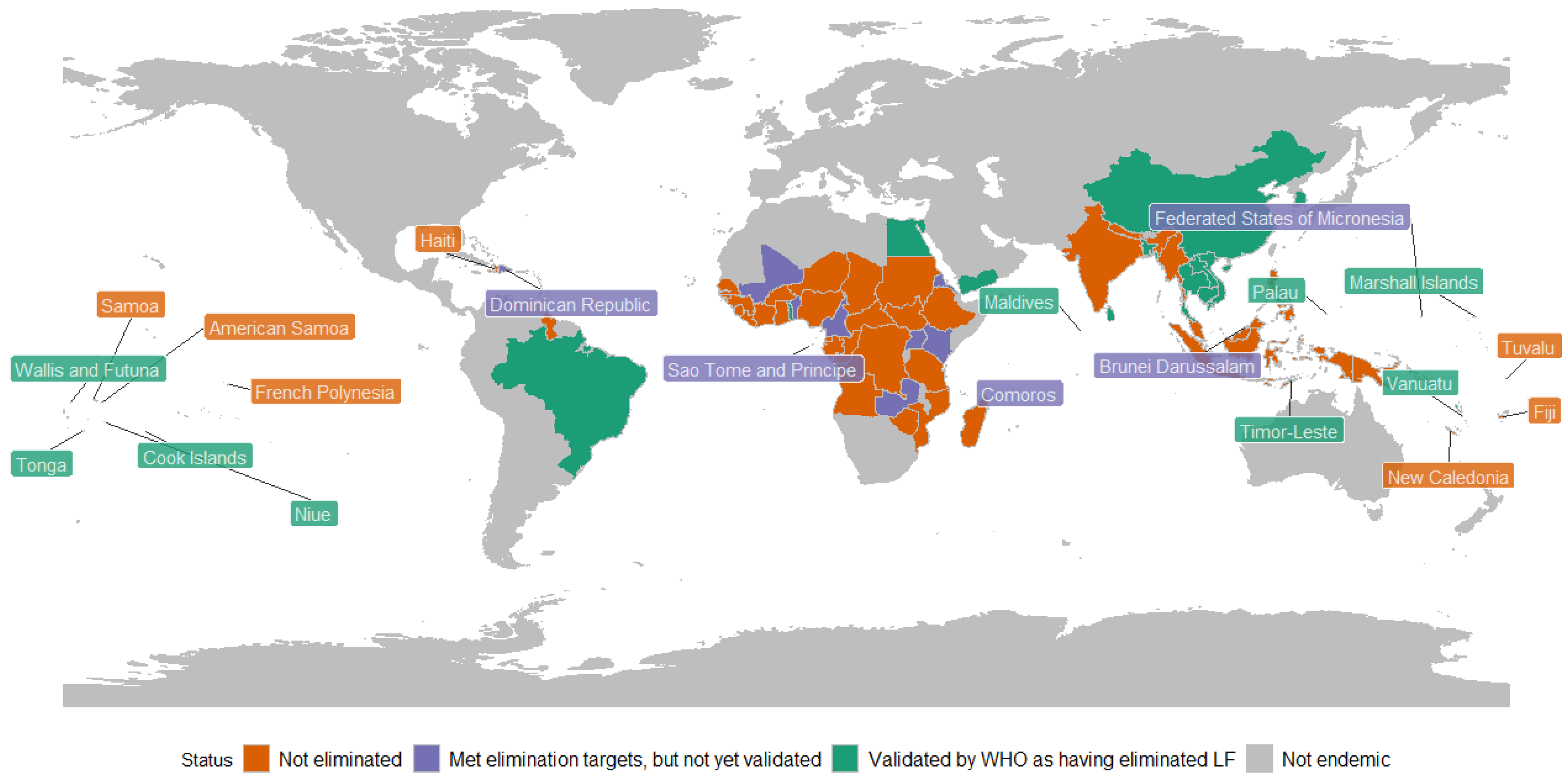
Figure 2.
PRISMA diagram showing study selection process.
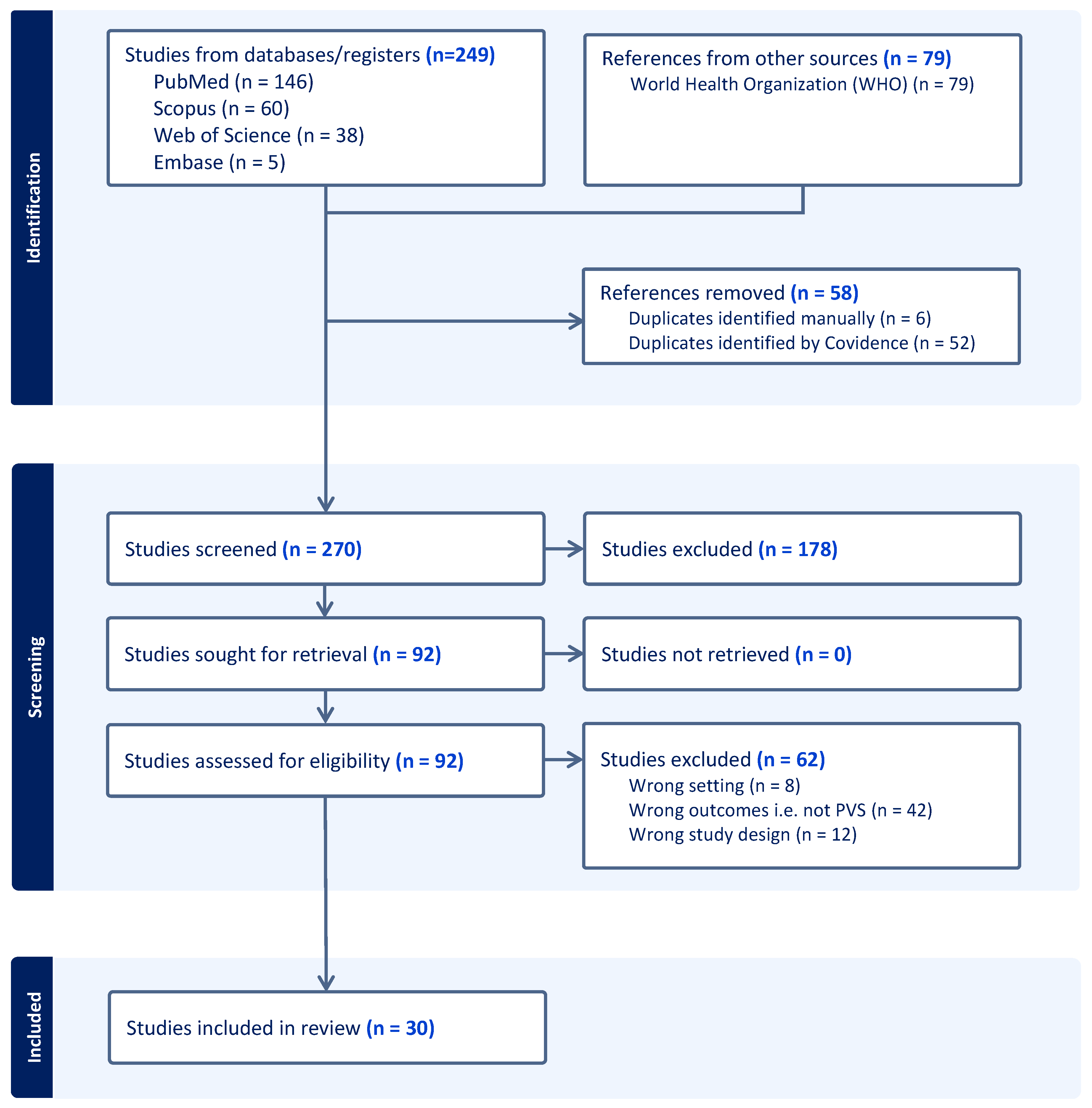
Table 1.
Number of documents in which PVS activities were described, by country of activity.
| WHO region | Country | Year LF eliminated | WHO-recommended PVS activities | Other surveillance activities | Sustained surveillance^ | Alignment with 2025 WHO guidelines (≥2 strategies + sustained surveillance) | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Targeted surveys |
Integration into existing standardised surveys |
Health facility-based screening | Molecular xenomonitoring | Morbidity management and disability prevention | Vector surveys | Animal reservoir surveys | |||||
| AFR | Malawi | 2020 | 1 | ||||||||
| Togo | 2017 | 1 | 2 | 1 | |||||||
| AMR | Brazil* | 2024 | |||||||||
| EMR | Egypt | 2018 | 1 | ||||||||
| Yemen | 2019 | 1 | 1 | 1 | |||||||
| SEAR | Bangladesh | 2023 | 1 | 1 | 1 | 1 | |||||
| Maldives | 2016 | 3 | 2 | 1 | 1 | ✓ | ✓ | ||||
| Sri Lanka | 2016 | 8 | 1 | 5 | 2 | 2 | ✓ | ✓ | |||
| Thailand | 2017 | 5 | 1 | 4 | 1 | 3 | ✓ | ✓ | |||
| Timor Leste* | 2024 | ||||||||||
| WPR | Cambodia | 2016 | 1 | ✓ | |||||||
| China | 2007 | 5 | 1 | 2 | 3 | ✓ | ✓ | ||||
| Cook Islands* | 2016 | ||||||||||
| Kiribati | 2019 | 1 | |||||||||
| Lao PDR* | 2023 | ||||||||||
| RMI* | 2017 | ||||||||||
| Niue | 2016 | 1 | |||||||||
| Palau | 2018 | 1 | |||||||||
| South Korea | 2008 | 2 | 4 | ✓ | ✓ | ||||||
| Tonga | 2017 | 1 | 1 | ||||||||
| Vanuatu | 2016 | 1 | |||||||||
| Viet Nam* | 2018 | ||||||||||
| Wallis & Futuna | 2018 | 1 | |||||||||
| No. documents describing activities | 28 | 10 | 4 | 18 | 11 | 2 | 5 | - | - | ||
| No. countries in which activities occurred | 9 | 9 | 4 | 6 | 8 | 2 | 2 | - | - | ||
*Countries without PVS activities recorded in extracted literature; ^ Repeated PVS activities implemented over multiple years following validation; AFR = African Region; AMR = Region of the Americas; EMR = Eastern Mediterranean Region; SEAR = South-East Asian Region; WPR=Western Pacific Region; Lao PDR = Lao People’s Democratic Republic ; RMI = Republic of the Marshall Islands.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



