Submitted:
29 December 2025
Posted:
30 December 2025
You are already at the latest version
Abstract
Backgraund/Objectives: Transient receptor potential melastatin 7 (TRPM7), a unıque ion channel protein, has important effects for the proliferation of many cancer cell lines and tumor progression in various cancers. This study aimed to investigate whether TRPM7 expression has an effect on the prognosis of patients with colorectal cancer (CRC). Methods: TRPM7 expression was evaluated in paraffin-embedded tu-mor tissues of 259 CRC patients, immunohistochemically. In addition, the ratio of CD4+/CD8+ lymphocytes in the tumor microenvironment was determined semi-quantitatively. Results: According to our data, tumor size was clearly higher in cases with high TRPM7 expression than those with low expression. TRPM7 overex-pression was closely related to high depth of tumor invasion, increased lymph node metastasis and high distant metastasis rate. These findings exposed that high TRPM7 expression is effective in the progression and aggressiveness of CRC. While there was a negative correlation between TRPM7 overexpression and the density of CD8+ TILs, a positive correlation was revealed between TRPM7 expression and the CD4+/CD8+ TILs ratio. This result aroused curiosity for further studies on what kind of connection is between the TRPM7 channel protein and TILs. Also, high TRPM7 expression was closely associated with low overall (OS) and disease-free survival (DFS) times. Fur-thermore, multivariate analyses revealed TRPM7 overexpression was independently related with short OS and DFS. Conclusions: In conclusion, the high TRPM7 expres-sion and CD4+/CD8+ TILs ratio are independent poor prognostic indicators in CRC. In the future, TRPM7 may be a promising biomolecule for new targeted treatment options for CRC.
Keywords:
colorectal cancer
; TRPM7
; TILs
; CD4+/CD8+ lymphocyte ratio
; survival
1. Introduction
Colorectal cancer (CRC) is the third most common malignant neoplasm across the world and is one of the major causes of cancer-related death [1,2,3]. The vast majority of colorectal cancers are adenocarcinomas that develop from benign adenomatous polyps in the colonic mucosa [1]. Despite the advances in modern surgical methods, radiotherapy and targeted therapies that have increased rapidly in recent years, the survival rate of patients with CRC has remained far from expectations due to the difficulty of early diagnosis and the presence of distant metastases at the time of diagnosis [3]. Tumor stage represented by the tumor-node-metastasis (TNM) system is still considered to be the most validating prognostic indicator [4]. However, patients in the same TNM stage may exhibit quite different clinical features, which makes it difficult to predict prognosis for some patients with CRC. Therefore, new molecular biomarkers are needed for reliable prognostic approaches and more effective targeted therapies [3].
The relationship between ion channels and cancer is one of the most interesting research topics in recent years. Various studies regarding this issue have exhibited significant findings that transient receptor potential (TRP) channels may be correlated with apoptosis, cell proliferation, cancer development, and tumor progression [5,6,7]. A variety of members of TRP superfamily, especially the TRPM, have been associated with some human cancers including gastrointestinal tract [8,9,10,11,12]. The TRPM7 protein is an important member of the TRPM subfamily and is a unique molecule joining an ion channel with a functional alpha-kinase domain [13,14]. TRPM7 is widely expressed in a variety of human tissues including liver, spleen, brain, heart, kidney, and lung [5,13]. In addition, TRPM7 expression has recently been displayed in breast cancer, retinoblastoma and gastric cancer [15,16,17]. TRPM7 channel protein is intensively expressed in various human tumor cells and lack of it inhibits tumor growth. TRPM7 overexpression is shown in breast cancer cells in relation to their proliferative potential [18]. In an another study, TRPM7 played a role in the carcinogenesis of nasopharyngeal carcinomas [19]. Also, it was determined that CRC LoVo cells sensitive to chemotherapy display higher TRPM7 expression compared to drug-resistant ones [20]. Recently, Su et al. reported that reduced TRPM7 expression inhibited CRC cell proliferation, migration, and in vitro invasion. They emphasized up-regulation of TRPM7 in CRC is associated with deeper tumor infiltration, positive lymph node metastasis, distant metastasis, and advanced clinical stage [8].
Since the tumor microenvironment (TME), which is affects all stages of tumor development and growth, is thought to play a key role in tumor behavior, the prognostic significance of tumor-infiltrating lymphocytes (TILs) has been an attracted subject of cancer researches [21,22,23]. Although there is still no consensus on whether TILs have a good or poor prognostic effect, various clinical and epidemiological investigations have shown that the presence, contents and amount of TILs are significantly associated with survival in CRC. Idos et al. stated that the density of CD8+ T lymphocytes in TME of CRC has a statistically significant prognostic effect on disease-free survival (DFS) and overall survival (OS) [21]. However, the prognostic significance of CD4+ TILs density and CD4+/CD8+ TILs ratio in CRC is still not fully investigated.
There are several in vitro and experimental studies investigating the relationship between TRPM7 and CRC. However, clinical studies involving a large patient population are needed. Therefore, in present study, it was aimed to investigate whether TRPM7 expression and CD4+/CD8+ TILs ratio have an effect on prognosis and survival in CRC. In addition, the relationship between TRPM7 expression and clinicopathological parameters including, histological tumor type, histological grade, depth of tumor invasion (pT), lymph node metastasis (pN), distant metastasis (DM) and TNM stage has also evaluated.
2. Materials and Methods
2.1. Patients and Pathological Evaluation
The present study was approved by the Fırat University Ethical Committee (Date: 14 January 2021, Approval No: 2021/01-06). The study included 259 patients with CRC treated by surgical resection between 2010-2017 at a single institution. The patients treated with adjuvant or neo-adjuvant chemotherapy were excluded. The clinical and pathological data were obtained from hospital medical archives. Pathological slides were evaluated retrospectively by two pathologists at different times. The survival information of the patients was obtained from the medical data processing records of the hospital. OS and DFS was determined as the interval between the dates of surgery and death or recurrence.
2.2. Immunohistochemistry
Immunohistochemical staining was carried out using the indirect immuno-peroxidase technique on formalin-fixed paraffin-embedded tissues. In the staining process, below antibodies were used: anti-TRPM7 (bs-9044R, BIOSS antibodies, Woburn, MA, USA), anti-CD4 (SP35, Ventana, Arizona, USA) and anti-CD8 (SP57, Ventana, Arizona, USA). Parafinized slides obtained from pathology blocks containing tumoral tissues were automatically stained with Ventana Bench Mark Ultra coater and ultra-View Universal DAB kit (Ventana, Tucson, AZ-85755, USA) in accordance with the manufacturer's specified procedures. The density and distribution of TPMR7 expression in tumor cells were evaluated immunohistochemically. Additionally, TILs density was evaluated by CD4 and CD8 staining.
2.3. The Evaluating of TRPM7 Expression Score
TRPM7 expression in CRC was assessed using the IHC-scoring method confirmed in previous studies [24,25]. While evaluating the preparations, cytoplasmic and membranous staining in tumor cells were taken into consideration. IHC-score was obtained multiplying the staining intensity [0: no staining, 1: weak staining (light yellow), 2: moderate staining (yellow brown), and 3: strong staining (brown)] by the percentage of positive stained cells (0: <5%; 1: 5% −20%; 2: 21% −50%; and 3: >50%). IHC-score ranged from 0 to 9. The mean value of the IHC-score 3.74±3.46 was accepted as the cut-off criterion. Patients with IHC-score below this value were considered as a low-TRPM7 expression group and those above were characterized as a high-TRPM7 expression or overexpression group.
2.4. Assessment of TILs Intensity and CD4+/CD8+ TILs Ratio
CD4+ and CD8+ TILs density was assessed holding to earlier studies [22,23]. Briefly, five fields with the intense infiltration of CRC were selected from each staining slide and the percentages of CD4+ and CD8+ TILs were evaluated. The mean of this five areas was put to use as the density of TILs. Firstly, a semi-quantitative staining score was specified according to the following features: 1 (<1% cells); 2 (1-10% cells); 3 (11-33% cells); 4 (34-66% cells); and 5 (67-100% cells). While evaluating CD4 and CD8 positivity, partial or complete positivity in the cytoplasm and/or plasma membrane of inflammatory cells was considered. Secondly, intensity of immunreactivity was scored as follows: 0 (absent), 1+ (slight), 2+ (moderate), and 3+ (intense). Finally, TILs IHC-scores were calculated by adding the mean staining scores and the intensity for each slide (ranging from 1 to 8). The patients were divided into two groups as a low and high CD4+ and CD8+ TILs density using median value of IHC-score (3.69±2.02, 3.56±2.07, respectively). In addition, CD4+/CD8+ TILs ratio was determined for each case. The mean value for this ratio was accepted as the cut-off criterion (1.67±1.67). Patients with below this value were considered as a low-CD4+/CD8+ TILs ratio group and those above were characterized as a high CD4+/CD8+ TILs ratio group.
2.5. Survival and Statistical Analysis
In the present study, SPSS version 26 software (IBM Corporation, Armonk, NY, USA) was used for statistical analysis of data. Obtained outcomes from this study were presented as means and standard deviations. Normality of groups was checked by the Shapiro-Wilk test. The expression of TRPM7 and clinicopathological features of the patients were compared according to the normality of the distribution. ANOVA and independent samples t test were used to determine the differences between groups with normal distribution. Chi-square and Mann-Whitney U tests were preferred to determine the differences between groups without normal distribution. Kaplan-Meier method (log-rank test) was used to achieve and compare the survival curves. Univariate and multivariate Cox proportional hazards regression analyses was applied to evaluate independent prognostic indicators associated with survival. For all statistical data, a P value less than 0.05 were considered statistically significant.
3. Results
3.1. The Correlation Between Clinicopathological Parameters and Survival
Of the 259 patients, 114 (44.0%) were female and 145 (56.0%) were male. The mean age was 60.3±13.4 years (range 24-86). Most of the tumors were on the left side (n=157, 60.6%). Most of the cases consisted of patients with advanced TNM stage (stage III-IV) (n=146, 56.4%). Also, in 131 (50.6%) of the cases in this series, the CD8+ TILs density was low (Figure 1A) and high in 128 (49.4%) (Figure 1B). Again, CD4+ TIL density was determined as low in 129 (49.8%) cases (Figure 1C) and high in 130 (50.2%) cases (Figure 1D).
The clinicopathological features are detailed in Table 1. The follow-up period for survival analysis was determined as 5-years. The mean OS was 49.6±12.8 months and the 5-year survival rate was 50.6%. There was recurrence in 163 (62.9%) of the patients, and the mean DFS was determined to be 44.7±15.7 months. It was revealed clinicopathological parameters such as gender, age, tumor size and histopathological type had no effect on survival. Conversely, according to univariate Cox regression analysis, right tumor site, high histological grade, low CD8+ and high CD4+ TILs density, high pT and advanced TNM stage were found to be significantly associated with poor prognosis (Table 1).
In multivariate analyses, classical prognostic parameters such as histological grade, CD4+ TILs density, pT and pN were not found to be associated with both OS and DFS (Table 2). However, CD8+ TILs and TNM stage was determined to be the most valuable independent parameters among all other classical prognostic factors (Table 2). Both OS and DFS times were shown to be significantly reduced in patients with advanced TNM stage (34.0±8.93 months, 25.80±8.09 months, respectively) compared to those with early stage (59.89±0.66 months, 58.45±3.47 months, respectively).
3.2. Relationship Between TRPM7 Expression and Clinicopathological Parameters
Totally 259 tumor tissues and 60 adjacent non-neoplastic colorectal tissues were stained with anti-TRPM7 antibody, immunohistochemically. There was lower TRPM7 expression in the normal colonic mucosa compared to tumoral areas (Figure 2A). While low TRPM7 expression (Figure 2B) was observed in 122 (47.1%) of 259 cases, overexpression (Figure 2C and 2D) was observed in 137 (52.9%) of the cases.
The interrelation between TRPM7 expression and clinicopathological features is shown in Table 3. There was no significant correlation between TRPM7 expression and classical prognostic parameters such as gender, age, and tumor site (not shown). Our results proved high TRPM7 expression was closely related to high histological grade, high pT category, increased pN, high DM rate and advanced TNM stage (Table 3).
Also, it was found the tumor size was significantly higher in cases with TRPM7 overexpression than those with low expression (Figure 3A). There was a negative correlation between TRPM7 expression and CD8+ TILs density (Figure 3B). Contrarily, the patients with TRPM7 overexpression had high CD4+ TILs density (Figure 3C). Consistent with these findings, TRPM7 expression was higher in patients with a high CD4+/CD8+ TILs ratio (p<0.001) (Table 3). In this series, 73 (28.2%) of 259 cases had DM. There was a positive correlation between TRPM7 expression and DM. The TRPM7 expression score was higher in patients with DM than those without (Figure 3D). These data implicated that high TRPM7 expression is effective in the progression and aggressiveness of CRC.
3.3. The Effect of High CD4+/CD8+ TILs Ratio on Prognosis
The mean CD4+/CD8+ TILs ratio of all patients was 1.67±1.67 (range 0.14-8.0). There was no significant relationship between CD4+/CD8+ TILs ratio and histological type (p=0.103, ANOVA), histological grade (p=0.174, ANOVA) and pN (p=0.270). Contrarily, high CD4+/CD8+ TILs ratio was positively correlated with pT (Figure 4A), DM (Figure 4B), and TNM stage (Figure 4C). There was also a statistically significant relationship between CD4+/CD8+ TILs ratio and TRPM7 expression. The CD4+/CD8+ TILs ratio was higher in high TRPM7 expressive patients (Figure 4D).
The effect of CD4+/CD8+ TILs ratio on OS and DFS was also investigated in the study. The Kaplan-Meier survival curves displayed CD4+/CD8+ TILs ratio was importantly associated with poor OS (p<0.001, Log Rank) (Figure 5A) and short DFS time (p<0.001, Log Rank) (Figure 5B). In the univariate analyses the high CD4+/CD8+ TILs ratio was an importantly correlated with shorter OS (Figure 5C) and DFS time (Figure 5D). Moreover, in multivariate analyses, there was a significant association between high CD4+/CD8+ TILs ratio and worsening OS (Figure 5E) and DFS (Figure 5F). Taken together, the findings support that the high CD4+/CD8+ TILs ratio is a reliable independent marker of tumor progression and poor prognosis in CRC.
3.4. TRPM7 Overexpression Can Be Used as an Independent Poor Prognostic Biomarker in CRC
Whether TRPM7 expression could be used as a prognostic biomarker was evaluated using Kaplan-Meier analyses and Cox regression models. The survival curves displayed TRPM7 overexpression was importantly associated with poor OS (Figure 5G) and short DFS time (Figure 5H). The cases with high TRPM7 expression exhibited worsening biological behavior than those with low expression. According to univariate analysis, TRPM7 expression was substantially related with poor OS (HR 6.36, 95% CI 4.33-9.36, p<0.001) and DFS (HR 4.10, 95% CI 3.15-5.34, p<0.001) in CRC. The patients with high TRPM7 expression had significantly shorter mean OS (Figure 5I) and DFS time (Figure 5J) than those with low expression. Furthermore, multivariate analyses revealed TRPM7 overexpression was independently correlated with poor OS (Figure 5K) and DFS (Figure 5L) (Table 2). In short, univariate and multivariate analyses exposed that high TRPM7 expression was a biomarker indicating poor prognosis for CRC patients, independently.
4. Discussion
Recently, there are various studies claiming that TRPM7 plays a role in carcinogenesis and could be a potential target in cancer treatment [9,17,26]. TRPM7, a special member of the super family of TRP ion channels, has permeability for Ca2+ and Mg2+ ions. Because the Ca2+ ion is an efficient regulator of cell cycle and proliferation, the regulation of TRPM7 functions is thought to be vital for cancer cell growth and tumor biology [26,27]. TRPM7, which is basically a bivalent cation-permeable channel with an intrinsic kinase, accomplishes its physiological effects by doing as a cellular sensor and signal transducer thanks to its ion channel and kinase activity [9,28]. TRPM7 channel functionality depends on the activity of the endogenic kinase capable of phosphorylating serine and threonine residues of the protein. The TRPM7 channel is activated when the TRP domain of TRPM7 interacts with phosphatidylinositol-4,5-bisphosphate (PIP2). However, since stimulation of phospholipase C (PLC) leads to hydrolysis of PIP2, the channel is inactivated [9]. Additionally, the interaction between the kinase domain and the PLC arranges the activity of TRPM7 channel in an addicted way to cAMP and protein kinase A. TRPM7 kinase also has the capable of auto-phosphorylation, and this is regulated via the intracellular Mg2+ and ATP levels [29].
TRPM 7, widely expressed in normal tissues, has been shown to be overexpressed in various types of cancer, abnormally [24,28,30,31]. Studies investigating the effect of TRPM7 on pancreatic cancers revealed TRPM7 expression significantly increased in pancreatic adenocarcinoma cells and tissues [9,32,33]. TRPM7 expression in pancreatic cancer tissues was clearly demonstrated to positively associate with the tumor size and tumor stages [33]. These results shown high TRPM7 expression is related with tumor growth, progression and metastasis in pancreas cancer. Additionally, there are studies showing TRPM7 is overexpressed in cell lines and tissues of breast cancer and glioblastoma [34,35]. According to Guilbert et al., TRPM7 expression plays an important role in the proliferation of MCF7 breast cancer cells, and TRPM7 protein levels in breast cancer suggest its overexpression may be a feature of high-grade, highly proliferative breast cancer [34]. In the study of Wan et al., it was claimed TRPM7 regulate miR-28-5p expression, which represses proliferation and invasion of glioma cells by targeting Rap1b signaling. According to Wan et al., While TRPM7's channel activity is necessary for the growth of glioma cells, its kinase domain contributes to tumor progression through cell migration and invasion [33]. These results show that TRPM7 has an important contribution to the proliferation of cancer cells and tumor growth. Compatible with previous studies, we determined the tumor size was significantly larger in cases with TRPM7 overexpression compared to those with low expression. In recent study, Pugliese et al. reported TRPM7 expression to be higher in tumoral areas than adjacent non-neoplastic tissue in both IBD-related and sporadic cases [36]. A higher TRPM7 expression was determined in adenocarcinomas than in colonic adenomas. Also, TRPM7 expression was positively associated with histological grade [36]. Similarly, we found that tumors with high TRPM7 expression had significant loss of differentiation and high histological grade. Especially, this positive relationship between high histological grade and TRPM7 overexpression supports the view that TRPM7 may play a promotor role in the acquisition of a malignant phenotype.
TRPM7 is thought to have a regulatory role in epithelial-mesenchymal transition (EMT), which is one of the important steps in tumor metastasis [28]. Epidermal growth factor (EGF) is associated with a temporary elevation of intracellular Ca2+ and activation of signal transducer and activator of transcription 3 (STAT3). TRPM7 gene silencing in a breast cancer cell line (MDA-MB468) given rise to suppress of EGF-induced Vimentin expression and phosphorylation of STAT3, which are markers of EMT [37]. According to Yee et al., in pancreatic adenocarcinoma, TRPM7 expression is necessary for Mg2+ dependent cell migration and cell invasion [33]. These results demonstrate that the Ca2+/Mg2+ homeostasis and associated signaling system provided by TRPM7 is essential for the migration and invasion of cancer cells and backs up the potential role of TRPM7 channels in tumor metastasis [28,33,37]. Su et al. evidently observed the up-regulation of TRPM7 expression in CRC tissues compared to non-tumoral areas [8]. They stated patients with TRPM7 overexpression had aggressive pathological features such as deeper tumor infiltration, positive lymph node metastasis, distant metastasis, and advanced clinical stage compared to those with low expression. Furthermore, they reported the down-regulation of TRPM7 expression in CRC cells reversed the EMT process with a decrease in N-cadherin and an increase in E-cadherin. And so, in vitro, they clearly demonstrated the reduced TRPM7 expression inhibits CRC cell proliferation, migration and invasion [8]. The results obtained in our study support the in vitro studies mentioned above. We showed both lymph node metastasis and distant metastasis rates in CRC patients with TRPM7 overexpression were significantly higher than those with low expression. One of the most important parameters affecting the prognosis in colorectal cancer is the occurrence of distant metastasis. Therefore, new studies are needed to determine whether the effect of TRPM7 on metastasis is only through Ca2+/Mg2+ homeostasis or through other pathways.
There are very few clinical studies investigating the effect of TRPM7 on the prognosis and survival of cancer patients [25,30]. Furthermore, the results of these studies are incompatible. Nakashima et al., demonstrated TRPM7 expression is negative correlated with pT, pN category and stage in esophagus cancer. They indicated the overall survival rate of the cases with high TRPM7 expression was importantly higher than that of those with low expression, also TRPM7 expression was an independent prognostic indicator for esophageal cancer [30]. However, Rybarczyk et al. revealed expression of TRPM7 was a potential biomarker of poor prognosis of pancreatic ductal adenocarcinoma [38]. In a recent study by Lee et al., which contained conflicting results with our study, it was determined that TRPM7 overexpression was negatively correlated with age and p53 in patients with rectal cancer [39]. They also found a positive correlation between TRPM7 expression and KRAS expression in rectal cancer. On the other hand, survival analysis in their study showed that TRPM7 overexpression had no prognostic significance in colon and rectal cancers. Contrarily, in our study, no significant difference was observed between TRPM7 expression and tumor site. In this study TRPM7 overexpression was closely related to aggressive histopathological features such as high histological grade, high pT, high pN category and distant metastasis rates in CRC. In addition, high TRPM7 expression in patients with CRC was associated with low OS and DFS rates according to univariate analysis. Moreover, in multivariate analysis, we established TRPM7 overexpression is a strong independent poor prognostic indicator.
TILs, particularly CD3+ and CD8+ T cells, are regarded as markers of the host immune response to the tumor, and many studies have indicated they are a strong independent positive predictor of relapse and OS in various cancers, including CRC [21,22,23,40,41]. However, CD4+ T cells are less defined as a prognostic marker in CRC [40,41]. It has been reported that the density of CD4+ TILs is a negative prognostic parameter in some malignant tumors such as breast, kidney, and lung cancer [42,43]. However, conflicting results were revealed about the effects of CD4+ TILs density on prognosis in CRC [40,41]. According to Kuwahara et al., while increased CD8+ TILs and CD4+ TILs density in CRC were closely associated with longer survival duration, low CD4+ TILs density had a markedly poor prognostic effect [40]. Contrarily, Lavotshkin et al. shown that longer DFS time was associated with higher CD8+ TILs density and lower CD4+/CD8+ ratios [44]. Diederichsen et al. stated patients with low CD4+/CD8+ ratios had a better clinical behavior with significantly higher 5-year survival, regardless of Dukes stage and age [41]. Consistent with previous studies, high CD8+ TILs rate was found as an independent good prognostic parameter in present study. High CD4+ TILs density and CD4+/CD8+ TILs ratio were closely associated with aggressive pathological features such as high pT, distant metastasis, and advanced TNM stage. Patients with high CD4+/CD8+ TILs ratio had shorter DFS and OS times compared to those with low. Except these, a negative relationship between TRPM7 expression and CD8+ TILs density was determined in present study. In contrast, patients with TRPM7 overexpression had high density of CD4+ TILs. Also, the high CD4+/CD8+ TILs ratio was found to be higher in patients with high TRPM7 expression compared to those with low expression. In light of these findings, hypothetically, it can be argued TRPM7 overexpression reduces the density of CD8+ T lymphocytes by reversing the function of T lymphocytes in host defense against the tumor thereby may adversely affect the prognosis. In our opinion, the role of TRPM7, which is known to have important effects on the regulation of lymphocyte functions, in the composing the TME and in the regulation of host defense against the tumor is worth investigating.
By the way, it would be useful to point out that our study has some limitations in order to positively influence future studies. First of all, this study is a retrospective study including cases from a single health center. Therefore, it should be taken into consideration that it may have the potential for selection bias. Secondly, patients who received chemotherapy are excluded from our study. However, in recent years, chemotherapy and targeted therapies have been widely used in the treatment of CRC. Therefore, it may be appropriate to include patients receiving chemotherapy in the study population in further studies to investigate whether potential biomarkers have therapeutic or prognostic value. Moreover, studies investigating the effects of agonist and antagonist agents for TRPM7 on CRC cell lines can be added to clinical studies.
Consequently, we have defined the pattern of TRPM7 expression in human CRC tissues, for the first time. According to our data, TRPM7 overexpression is closely associated with aggressive histopathological features and progression of CRC. The patients with high TRPM7 expression had shorter survival period. In multivariate analyses, TRPM7 overexpression, CD8+ TILs density and CD4+/CD8+ TILs ratio have been shown to be independent poor prognostic biomarkers. We also predicted TRPM7 may adversely affect the host immune response to the tumor by decreasing CD8+ TILs density. Therefore, the effects of TRPM7 on host defense in patients with CRC and its potential to be a target for new treatments are worth investigating.
Author Contributions
Conceptualization, C.M. and C.I.; methodology, C.M., software, C.M.; validation, C.I.; and C.M.; formal analysis, C.I.; and C.M.; investigation, C.I.; and C.M.; resources, C.I.; and C.M.; data curation, C.M.; writing—original draft preparation, C.I.; writing—review and editing, C.I.; and C.M.; visualization, C.M.; supervision, C.M.; project administration, C.I.; and C.M.; funding acquisition, C.I.; and C.M.” All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The present study was approved by the Fırat University Ethical Committee (Date: 14 January 2021, Approval No: 2021/01-06).
Informed Consent Statement
Not applicable.
Data Availability Statement
Data sharing is not applicable due to restrictions related to the local hospital's management.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Kokoropoulos, P.; Christodoulou, S.; Tsiakanikas, P.; Poulios, E.; Vassiliu, P.; Kontos, C.K.; Arkadopoulos, N. A Retrospective Study in Colorectal Adenocarcinoma Uncovers the Potential of Circ-CCT3 as a Predictor of Tumor Recurrence. Biomedicines 2025, 13, 2432. [Google Scholar] [CrossRef]
- Xue, Y.; Jiang, Z.; Gu, J.; Deng, S.; Cai, K.; Wu, K. Analysis of Immune Cell Infiltration Distribution and Prognostic Value in Obstructive Colorectal Cancer. Biomedicines 2025, 13, 2596. [Google Scholar] [CrossRef] [PubMed]
- Fagarasan, G.; Gheban, B.A.; Fagarasan, V.; Crisan, D.; Telecan, T.; Bintintan, V.V.; Seicean, R.L.; Caziuc, A.; Dindelegan, G.C. B and T Tumor-Infiltrating Lymphocyte Subtypes According to Subsite: A Colon Cancer Immunophenotyping Map. Biomedicines 2025, 13, 2856. [Google Scholar] [CrossRef] [PubMed]
- Betge, J.; Langner, C. Vascular Invasion, Perineural Invasion, and Tumour Budding: Predictors of Outcome in Colorectal Cancer. Acta. Gastroenterol. Belg 2011, 74, 516–529. [Google Scholar] [PubMed]
- Park, HS.; Hong, C.; Kim, B.J.; So, I. The Pathophysiologic Roles of TRPM7 Channel. Korean. J Physiol. Pharmacol. 2014, 18, 15–23. [Google Scholar] [CrossRef]
- Liu, H.; Dilger, J.P.; Lin, J. Lidocaine Suppresses Viability and Migration of Human Breast Cancer Cells: TRPM7 as a Target for Some Breast Cancer Cell Lines. Cancers 2021, 13, 234. [Google Scholar] [CrossRef]
- Sanchez, M.G.; Sanchez, A.M.; Collado, B.; Malagarie-Cazenave, S.; Olea, N.; Carmena, M.J.; Prieto, J.C.; Diaz-Laviada, I. Expression of the transient receptor potential vanilloid 1 (TRPV1) in LNCaP and PC-3 prostate cancer cells and in human prostate tissue. Eur. J. Pharmacol. 2005, 515, 20–27. [Google Scholar] [CrossRef]
- Su, F.; Wang, B.F.; Zhang, T.; Hou, X.M.; Feng, MH. TRPM7 deficiency suppresses cell proliferation, migration, and invasion in human colorectal cancer via regulation of epithelial-mesenchymal transition. Cancer Biomark. 2019, 26, 451–460. [Google Scholar] [CrossRef]
- Yee, N.S.; Chan, A.S.; Yee, J.D.; Yee, R.K. TRPM7 and TRPM8 ion channels in pancreatic adenocarcinoma: potential roles as cancer biomarkers and targets. Scientifica. (Cairo). 2012; p. 415158. [Google Scholar]
- Anderson, K.J.; Cormier, R.T.; Scott, P.M. Role of ion channels in gastrointestinal cancer. World J. Gastroenterol. 2019, 25, 5732–5772. [Google Scholar] [CrossRef]
- Dai, Q.; Shrubsole, M.J.; Ness, R.M.; Schlundt, D.; Cai, Q.; Smalley, W.E.; Li, M.; Shyr, Y.; Zheng, W. The relation of magnesium and calcium intakes and a genetic polymorphism in the magnesium transporter to colorectal neoplasia risk. Am. J. Clin. Nutr. 2007, 86, 743–751. [Google Scholar] [CrossRef]
- Kim, B.J.; Hong, C. Role of transient receptor potential melastatin type 7 channel in gastric cancer. Integr. Med. Res. 2016, 5, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Furuya, H.; Faouzi, M.; Zhang, Z.; Monteilh-Zoller, M.; Kawabata, K.G.; Horgen, F.D.; Kawamori, T.; Penner, R.; Fleig, A. Inhibition of TRPM7 suppresses cell proliferation of colon adenocarcinoma in vitro and induces hypomagnesemia in vivo without affecting azoxymethane-induced early colon cancer in mice. Cell. Commun. Signal. 2017, 15, 30. [Google Scholar] [CrossRef] [PubMed]
- Fleig, A.; Chubanov, V. TRPM7. Handb. Exp. Pharmacol. 2014, 222, 521–546. [Google Scholar] [PubMed]
- Dhennin-Duthille, I.; Gautier, M.; Faouzi, M.; Guilbert, A.; Brevet, M.; Vaudry, D.; Ahidouch, A.; Sevestre, H.; Ouadid-Ahidouch, H. High expression of transient receptor potential channels in human breast cancer epithelial cells and tissues: correlation with pathological parameters. Cell. Physiol. Biochem. 2011, 28, 813–822. [Google Scholar] [CrossRef]
- Hanano, T.; Hara, Y.; Shi, J.; Morita, H.; Umebayashi, C.; Mori, E.; Sumimoto, H.; Ito, Y.; Mori, Y.; Inoue, R. Involvement of TRPM7 in cell growth as a spontaneously activated Ca2+ entry pathway in human retinoblastoma cells. J. Pharmacol. Sci. 2004, 95, 403–419. [Google Scholar] [CrossRef]
- Sterea, A.M.; Egom, E.E.; El Hiani, Y. TRP channels in gastric cancer: New hopes and clinical perspectives. Cell. Calcium 2019, 82, 102053. [Google Scholar] [CrossRef]
- Middelbeek, J.; Kuipers, A.J.; Henneman, L.; Visser, D.; Eidhof, I.; van-Horssen, R.; Wieringa, B.; Canisius, S.V.; Zwart, W.; Wessels, L.F.; et al. TRPM7 is required for breast tumor cell metastasis. Cancer. Res. 2012, 72, 4250–4261. [Google Scholar] [CrossRef]
- Qin, Y.; Liao, Z.W.; Luo, J.Y.; Wu, W.Z.; Lu, A.S.; Su, P.X.; Lai, B.Q.; Wang, X.X. Functional characterization of TRPM7 in nasopharyngeal carcinoma and its knockdown effects on tumorigenesis. Tumour. Biol. 2016, 37, 9273–9283. [Google Scholar] [CrossRef]
- Castiglioni, S.; Cazzaniga, A.; Trapani, V.; Cappadone, C.; Farruggia, G.; Merolle, L.; Wolf, F.I.; Iotti, S.; Maier, J.A.M. Magnesium homeostasis in colon carcinoma LoVo cells sensitive or resistant to doxorubicin. Sci. Rep. 2015, 5, 16538. [Google Scholar] [CrossRef]
- Idos, G.E.; Kwok, J.; Bonthala, N.; Kysh, L.; Gruber, S.B.; Qu, C. The Prognostic Implications of Tumor Infiltrating Lymphocytes in Colorectal Cancer: A Systematic Review and Meta-Analysis. Sci. Rep. 2020, 10, 3360. [Google Scholar] [CrossRef]
- Lu, J.; Xu, Y.; Wu, Y.; Huang, X.Y.; Xie, J.W.; Wang, J.B.; Lin, J.X.; Li, P.; Zheng, C.H.; Huang, A.M.; et al. Tumor infiltrating CD8+ T cells combined with tumor-associated CD68+ macrophages predict postoperative prognosis and adjuvant chemotherapy benefit in resected gastric cancer. BMC. Cancer 2019, 19, 920. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; He, Q.; Liu, J.; Xiao, Y.; Xiao, C.; Chen, K.; Xie, D.; Zhang, X. CD8+ tumor-infiltrating lymphocytes as a novel prognostic biomarker in lung sarcomatoid carcinoma, a rare subtype of lung cancer. Cancer. Manag. Res. 2018, 10, 3505–3511. [Google Scholar] [CrossRef] [PubMed]
- Gao, S.L.; Kong, C.Z.; Zhang, Z.; Li, Z.L.; Bi, J.B.; Liu, X.K. TRPM7 is overexpressed in bladder cancer and promotes proliferation, migration, invasion and tumor growth. Oncol. Rep. 2017, 38, 1967–1976. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Zhang, M.; Duan, X.; Chen, Y.; Li, E.; Luo, L.; Wu, W.; Peng, Z.; Qiu, H.; Zeng, G. TRPM7 Regulates AKT/FOXO1-Dependent Tumor Growth and Is an Independent Prognostic Indicator in Renal Cell Carcinoma. Mol. Cancer. Res. 2018, 16, 1013–1023. [Google Scholar] [CrossRef]
- Lee, E.H.; Chun, S.Y.; Kim, B.; Yoon, B.H.; Lee, J.N.; Kim, B.S.; Yoo, E.S.; Lee, S.; Song, P.H.; Kwon, T.G.; et al. Knockdown of TRPM7 prevents tumor growth, migration, and invasion through the Src, Akt, and JNK pathway in bladder cancer. BMC. Urol. 2020, 20, 145. [Google Scholar] [CrossRef]
- Liu, H.; Dilger, J.P.; Lin, J. The Role of Transient Receptor Potential Melastatin 7 (TRPM7) in Cell Viability: A Potential Target to Suppress Breast Cancer Cell Cycle. Cancers. (Basel) 2020, 12, 131. [Google Scholar] [CrossRef]
- Yee, N.S. Role of TRPM7 in Cancer: Potential as Molecular Biomarker and Therapeutic Target. Pharmaceuticals. (Basel) 2017, 10, 39. [Google Scholar] [CrossRef]
- Demeuse, P.; Penner, R.; Fleig, A. TRPM7 channel is regulated by magnesium nucleotides via its kinase domain. J Gen. Physiol. 2006, 127, 421–434. [Google Scholar] [CrossRef]
- Nakashima, S.; Shiozaki, A.; Ichikawa, D.; Hikami, S.; Kosuga, T.; Konishi, H.; Komatsu, S.; Fujiwara, H.; Okamoto, K.; Kishimoto, M.; et al. Transient Receptor Potential Melastatin 7 as an Independent Prognostic Factor in Human Esophageal Squamous Cell Carcinoma. Anticancer. Res. 2017, 37, 1161–1167. [Google Scholar] [CrossRef]
- Liu, K.; Xu, S.H.; Chen, Z.; Zeng, Q.X.; Li, Z.J.; Chen, Z.M. TRPM7 overexpression enhances the cancer stem cell-like and metastatic phenotypes of lung cancer through modulation of the Hsp90α/uPA/MMP2 signaling pathway. BMC. Cancer 2018, 26, 1167. [Google Scholar] [CrossRef]
- Yee, N.S.; Zhou, W.; Liang, I.C. Transient receptor potential ion channel TRPM7 regulates exocrine pancreatic epithelial proliferation by Mg2+-sensitive Socs3a signaling in development and cancer. Dis. Mod. Mech. 2011, 4, 240–254. [Google Scholar] [CrossRef]
- Yee, N.S.; Kazi, A.A.; Li, Q.; Yang, Z.; Berg, A.; Yee, R.K. Aberrant over-expression of TRPM7 ion channels in pancreatic cancer: Required for cancer cell invasion and implicated in tumor growth and metastasis. Biol. Open. 2015, 4, 507–514. [Google Scholar] [CrossRef] [PubMed]
- Guilbert, A.; Gautier, M.; Dhennin-Duthille, I.; Haren, N.; Sevestre, H.; Ouadid-Ahidouch, H. Evidence that TRPM7 is required for breast cancer cell proliferation. Am. J. Physiol. Cell. Physiol. 2009, 297, C493–C502. [Google Scholar] [CrossRef] [PubMed]
- Wan, J.; Guo, A.A.; Chowdhury, I.; Guo, S.; Hibbert, J.; Wang, G.; Liu, M. TRPM7 Induces Mechanistic Target of Rap1b Through the Downregulation of miR-28-5p in Glioma Proliferation and Invasion. Front. Oncol. 2019, 9, 1413. [Google Scholar] [CrossRef] [PubMed]
- Pugliese, D.; Armuzzi, A.; Castri, F.; Benvenuto, R.; Mangoni, A.; Guidi, L.; Gasbarrini, A.; Rapaccini, G.L.; Wolf, F.I.; Trapani, V. TRPM7 is overexpressed in human IBD-related and sporadic colorectal cancer and correlates with tumor grade. Dig. Liver. Dis. 2020, 52, 1188–1194. [Google Scholar] [CrossRef]
- Davis, F.M.; Azimi, I.; Faville, R.A.; Peters, A.A.; Jalink, K.; Putney, J.W.; Goodhill, G.J., Jr.; Thompson, E.W.; Roberts-Thomson, S.J.; Monteith, G.R. Induction of epitheial-mesenchymal transition (EMT) in breast cancer cells is calcium signal dependent. Oncogene 2014, 33, 2307–2316. [Google Scholar] [CrossRef]
- Rybarczyk, P.; Gautier, M.; Hague, F.; Dhennin-Duthille, I.; Chatelain, D.; Kerr-Conte, J.; Pattou, F.; Regimbeau, J.M.; Sevestre, H.; Ouadid-Ahidouch, H. Transient receptor potential melastatinrelated 7 channel is overexpressed in human pancreatic ductal adenocarcinomas and regulates human pancreatic cancer cell migration. Int. J Cancer 2012, 131, E851-861. [Google Scholar] [CrossRef]
- Lee, J.C.; Bae, A.N.; Lee, H.J.; Lee, J.H. Clinical and Prognostic Values of TRPM7 in Colon and Rectal Cancers. Medicina [Kaunas] 2022, 58, 1582. [Google Scholar] [CrossRef]
- Kuwahara, T.; Hazama, S.; Suzuki, N.; Yoshida, S.; Tomochika, S.; Nakagami, Y.; Matsui, H.; Shindo, Y.; Kanekiyo, S.; Tokumitsu, Y.; et al. Intratumoural-infiltrating CD4 + and FOXP3 + T cells as strong positive predictive markers for the prognosis of resectable colorectal cancer. Br. J Cancer 2019, 121, 659–665. [Google Scholar] [CrossRef]
- Diederichsen, A.C.; Hjelmborg, J.V.; Christensen, P.B.; Zeuthen, J.; Fenger, C. Prognostic value of the CD4+/CD8+ ratio of tumour infiltrating lymphocytes in colorectal cancer and HLA-DR expression on tumour cells. Cancer. Immunol. Immunother. 2003, 52, 423–428. [Google Scholar] [CrossRef]
- Droeser, R.; Zlobec, I.; Kilic, E.; Güth, U.; Heberer, M.; Spagnoli, G.; Oertli, D.; Tapia, C. Differential pattern and prognostic significance of CD4 +, FOXP3 + and IL-17 + tumor infiltrating lymphocytes in ductal and lobular breast cancers. BMC. Cancer 2012, 12, 134. [Google Scholar] [CrossRef]
- Kinoshita, T.; Muramatsu, R.; Fujita, T.; Nagumo, H.; Sakurai, T.; Noji, S.; Takahata, E.; Yaguchi, T.; Tsukamoto, N.; Kudo-Saito, C.; et al. Prognostic value of tumor-infiltrating lymphocytes differs depending on histological type and smoking habit in completely resected non-small-cell lung cancer. Ann. Oncol. 2016, 27, 2117–2123. [Google Scholar] [CrossRef]
- Lavotshkin, S.; Jalas, J.R.; Torisu-Itakura, H.; Ozao-Choy, J.; Lee, J.H.; Sim, M.S.; Stojadinovic, A.; Wainberg, Z.; Bifulco, C.B.; Fox, B.A.; et al. Immunoprofiling for prognostic assessment of colon cancer: a novel complement to ultrastaging. J Gastrointest Surg. 2015, 19, 999–1006. [Google Scholar] [CrossRef]
Figure 1.
Representative TILs density in colorectal cancer tissues. Arrows show CD8 and CD4 positive T lymphocytes in the tumor microenvironment. (A) low CD8+ TILs density (CD8x200). (B) high CD8+ TILs density (CD8x200) (C) low staining intensity for CD4+ T lymphocytes (CD4x200) (D) high density of CD4+ TILs (CD4x200).
Figure 1.
Representative TILs density in colorectal cancer tissues. Arrows show CD8 and CD4 positive T lymphocytes in the tumor microenvironment. (A) low CD8+ TILs density (CD8x200). (B) high CD8+ TILs density (CD8x200) (C) low staining intensity for CD4+ T lymphocytes (CD4x200) (D) high density of CD4+ TILs (CD4x200).
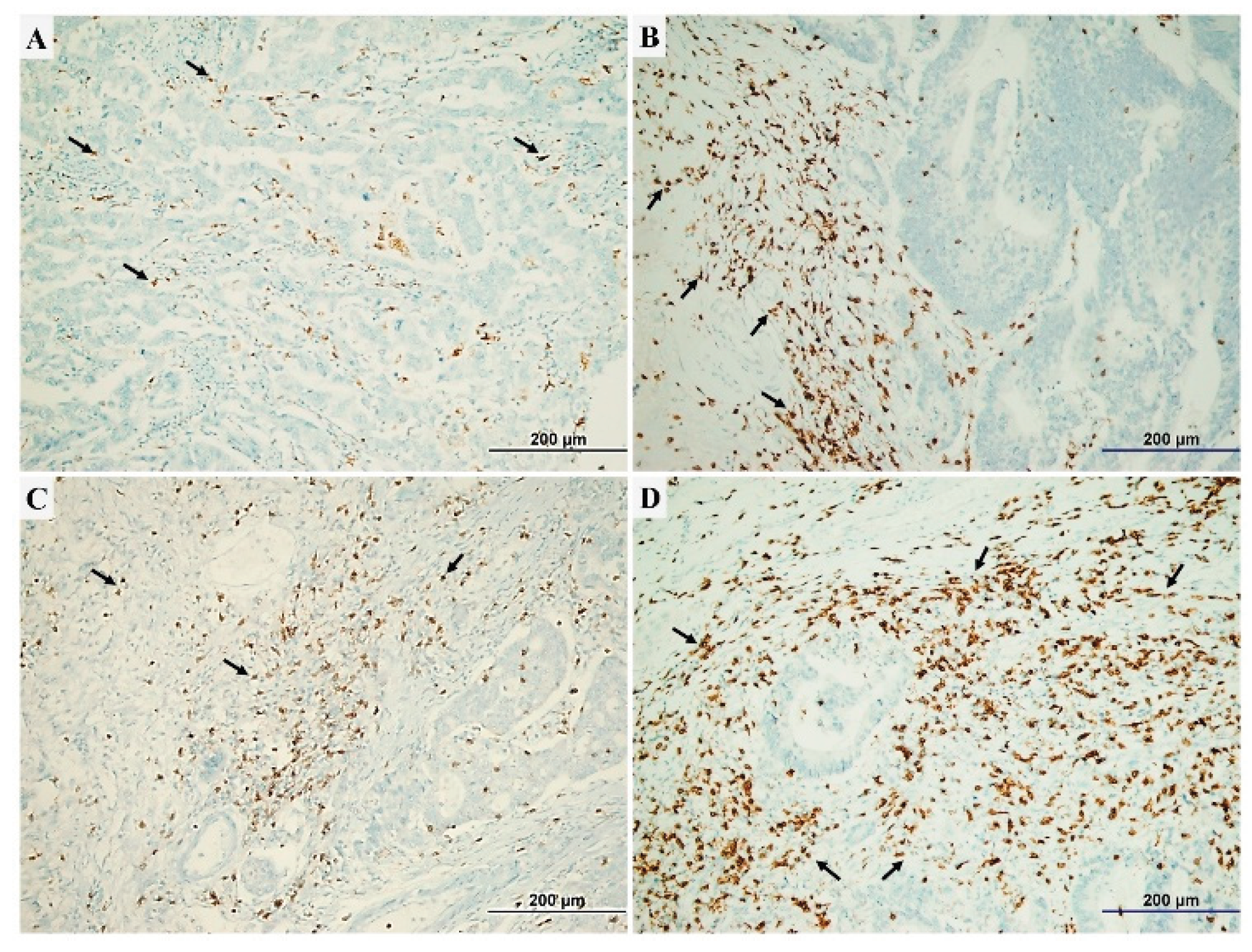
Figure 2.
Representative figures of TRPM7 expression in CRC specimens. Arrows show cytoplasmic TRPM7 expression in normal colonic mucosa and tumor cells. (A) Low staining (normal mucosa adjacent to tumor) (TRPM7x400). (B) low cytoplasmic TRPM7 expression in moderate differentiated tumor (TRPM7x400). (C) high expression of TRPM7 in mucinous adenocarcinoma cells (TRPM7x400). (D) TRPM7 overexpression in tumor cells (TRPM7x400).
Figure 2.
Representative figures of TRPM7 expression in CRC specimens. Arrows show cytoplasmic TRPM7 expression in normal colonic mucosa and tumor cells. (A) Low staining (normal mucosa adjacent to tumor) (TRPM7x400). (B) low cytoplasmic TRPM7 expression in moderate differentiated tumor (TRPM7x400). (C) high expression of TRPM7 in mucinous adenocarcinoma cells (TRPM7x400). (D) TRPM7 overexpression in tumor cells (TRPM7x400).
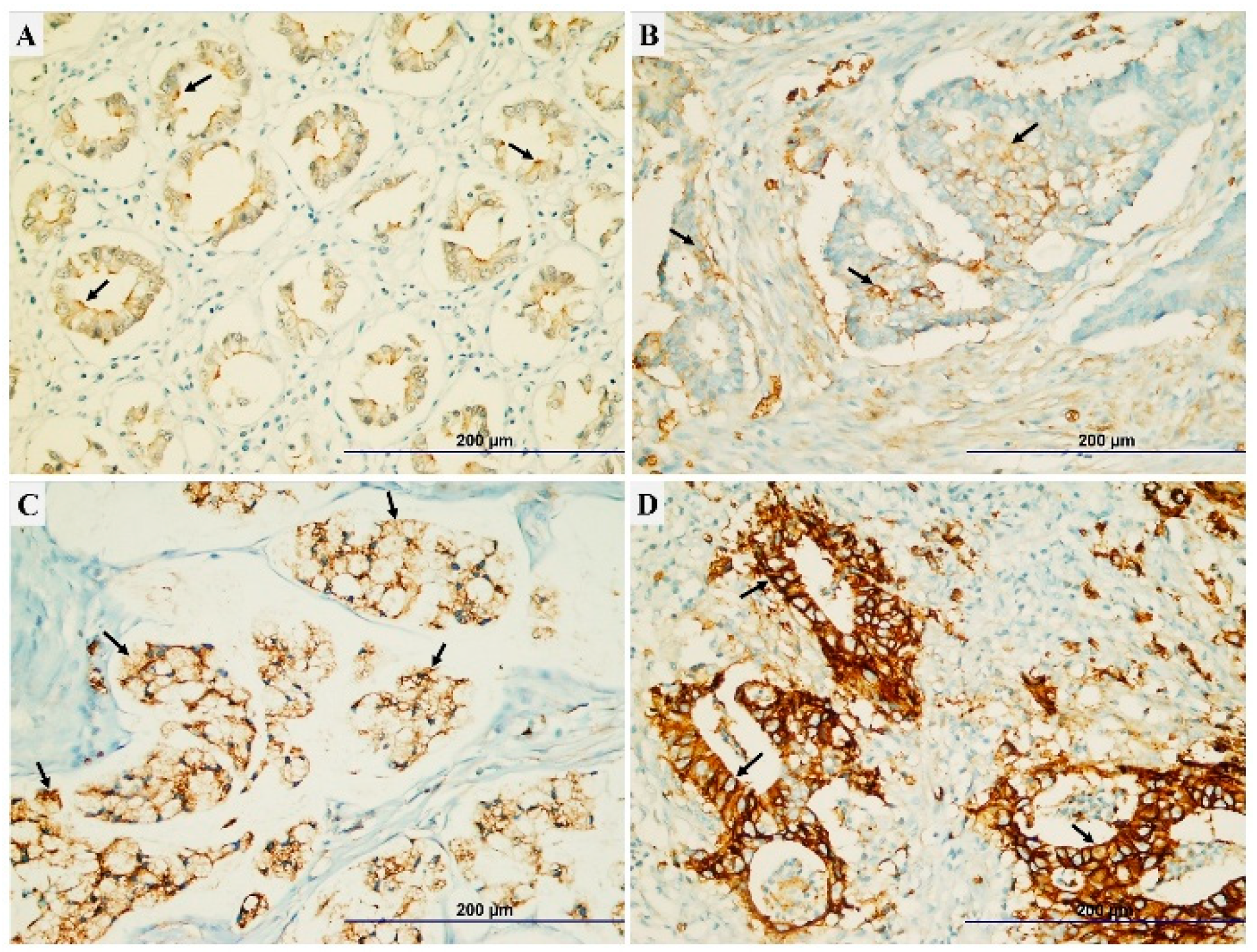
Figure 3.
Representative images showing the interrelationship between TRPM7 expression and prognostic parameters including tumor size, CD8+ TILs density, CD4+ TILs density and distant metastasis. (A) The TRPM7 expression was higher in tumors with great size (3.99±2.34) compared to those with small size (3.37±2.14) (p=0.005, t-test). (B) in tumoral tissues with high TRPM7 expression, the density of CD8+ TILs was significantly low (p=0.003, Mann-Whitney U test). (C) in tumors with high TRPM7 expression, the density of CD4+ TILs was significantly high (p=0.009, Mann-Whitney U test). (D) Patients with TRPM7 overexpression had a higher rate of distant metastases (p<0.001, t-test).
Figure 3.
Representative images showing the interrelationship between TRPM7 expression and prognostic parameters including tumor size, CD8+ TILs density, CD4+ TILs density and distant metastasis. (A) The TRPM7 expression was higher in tumors with great size (3.99±2.34) compared to those with small size (3.37±2.14) (p=0.005, t-test). (B) in tumoral tissues with high TRPM7 expression, the density of CD8+ TILs was significantly low (p=0.003, Mann-Whitney U test). (C) in tumors with high TRPM7 expression, the density of CD4+ TILs was significantly high (p=0.009, Mann-Whitney U test). (D) Patients with TRPM7 overexpression had a higher rate of distant metastases (p<0.001, t-test).
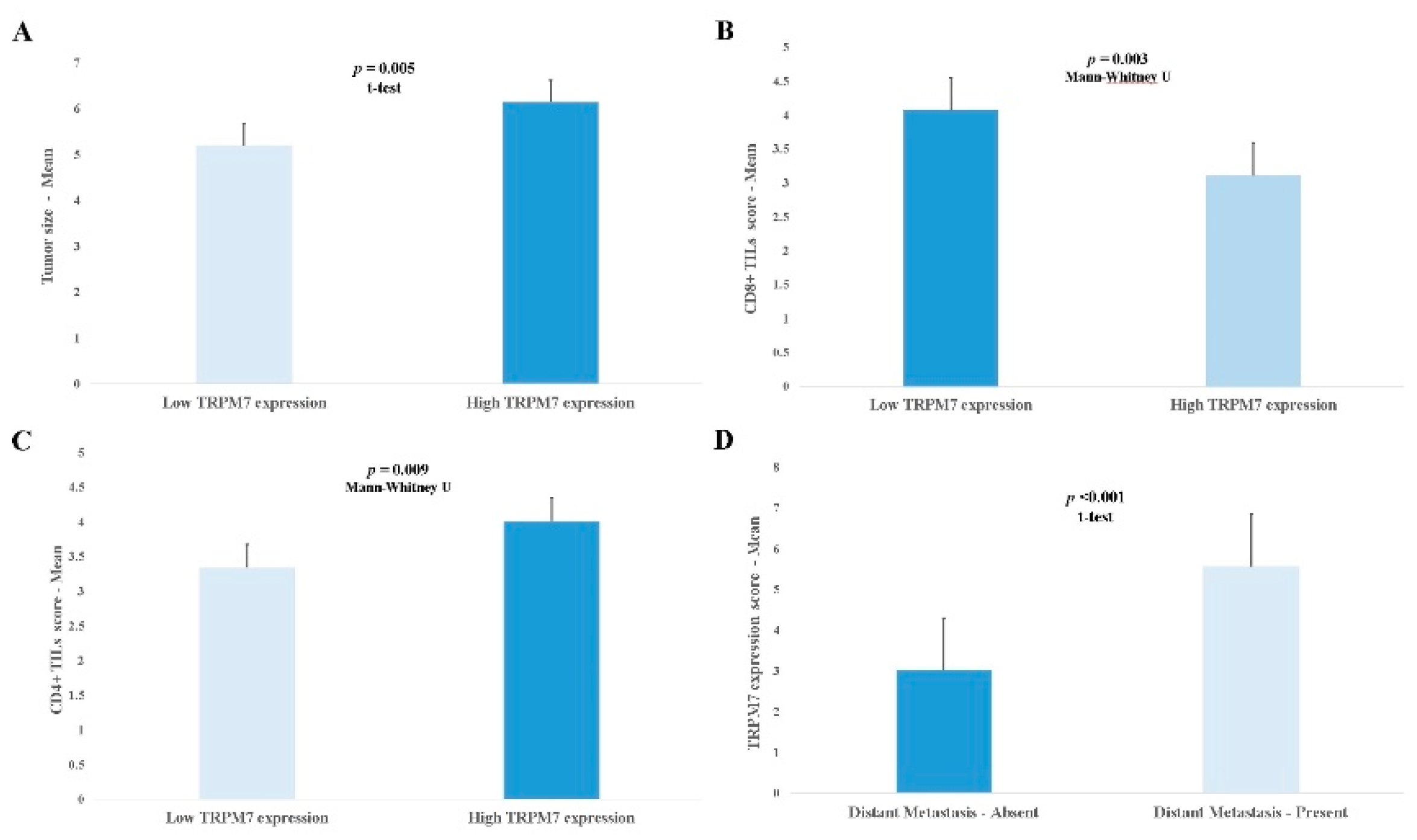
Figure 4.
The correlation between CD4+/CD8+ TILs ratio and basic prognostic indicators of CRC, and TRPM7 expression. (A) the ratio of CD4+/CD8+ TILs was significantly higher in patients with deeper tumor invasion (1.92±1.79) compared to those with more superficial (1.48±1.92) (p=0.008, ANOVA). (B) Distant metastasis was significantly more common in cases with high CD4+/CD8+ TILs (p<0.001, t-test). (C) The CD4+/CD8+ TILs ratio was significantly higher in patients with advanced TNM stage (2.34±2.00) than those with early TNM stage (1.49±1.71) (p=0.001, ANOVA). (D) The CD4+/CD8+ TILs ratio was importantly high in tumors with TRPM7 overexpression (p<0.001, t-test).
Figure 4.
The correlation between CD4+/CD8+ TILs ratio and basic prognostic indicators of CRC, and TRPM7 expression. (A) the ratio of CD4+/CD8+ TILs was significantly higher in patients with deeper tumor invasion (1.92±1.79) compared to those with more superficial (1.48±1.92) (p=0.008, ANOVA). (B) Distant metastasis was significantly more common in cases with high CD4+/CD8+ TILs (p<0.001, t-test). (C) The CD4+/CD8+ TILs ratio was significantly higher in patients with advanced TNM stage (2.34±2.00) than those with early TNM stage (1.49±1.71) (p=0.001, ANOVA). (D) The CD4+/CD8+ TILs ratio was importantly high in tumors with TRPM7 overexpression (p<0.001, t-test).
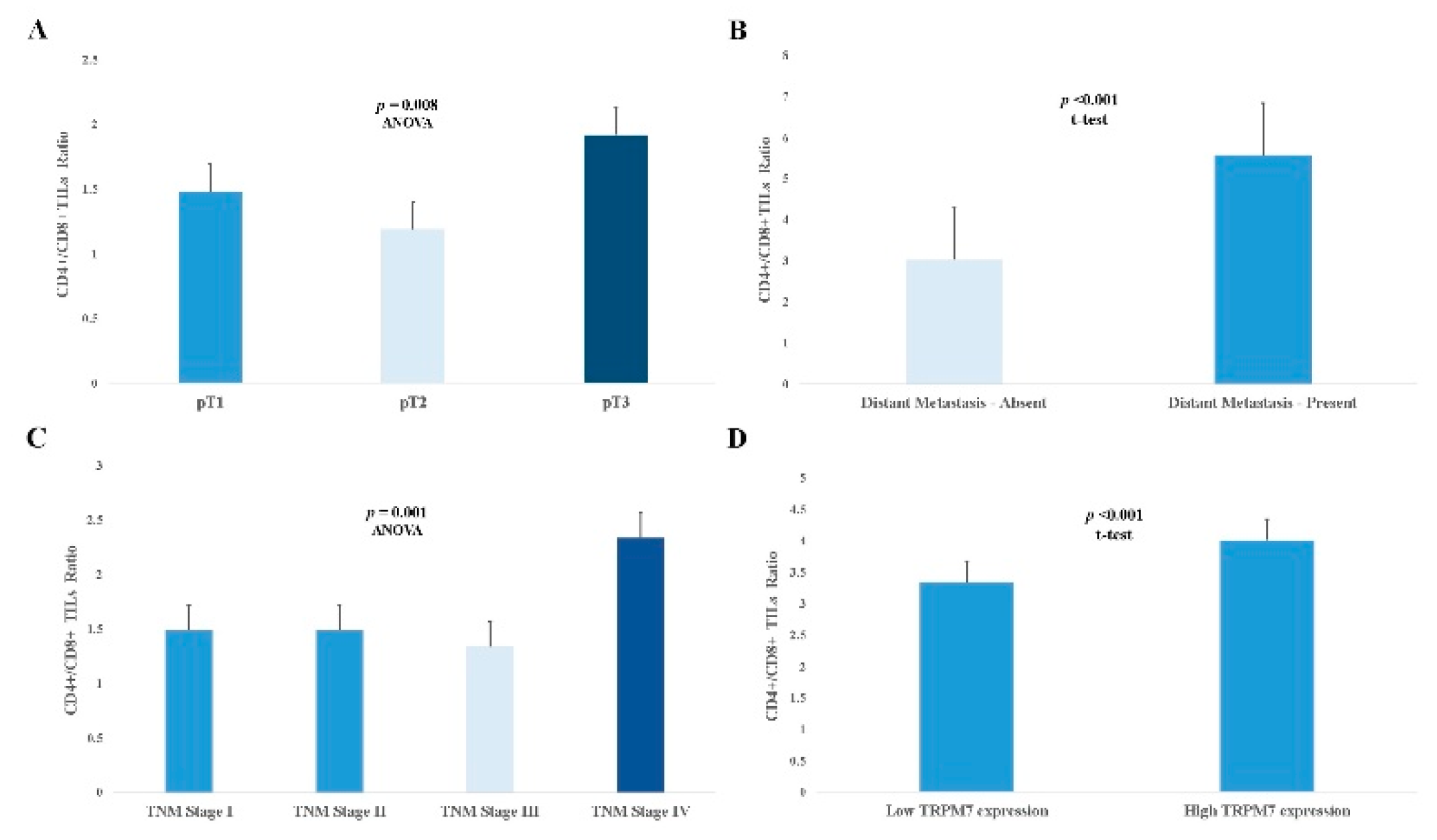
Figure 5.
Representative Kaplan-Meier survival curves and Cox proportional regression analyses according to CD4+/CD8+ TILs ratio and TRPM7 expression. Patients with high CD4+/CD8+ TILs ratio had a poor (A) overall (p<0.001, Log Rank) and (B) disease-free survival rates (p<0.001, Log Rank) than those with low CD4+/CD8+ TILs ratio. In univariate Cox regression analyzes, high CD4+/CD8+ TILs ratio was significantly associated with both poor (C) overall (p <0.001) and (D) disease-free survival (p <0.001). According to multivariate analyses, patients with high CD4+/CD8+ TILs ratio had shorter (E) overall (HR 1.77, 95% CI 1.22-2.56, p=0.002) and (F) disease-free survival times (HR 1.89, 95% CI 1.35-2.64, p<0.001). (G) The patients with high TRPM7 expression had a poor overall (p<0.001, Log Rank) and (H) disease-free survival rates (p<0.001, Log Rank) than those with low expression. In univariate Cox regression analyzes, high TRPM7 expression was significantly associated with both (I) overall (p<0.001) and (J) disease-free survival (p<0.001). According to multivariate Cox regression analyzes, TRPM7 overexpression was significantly correlated with both worsened (K) overall (p<0.001) and (L) disease-free survival time (p<0.001), independently.
Figure 5.
Representative Kaplan-Meier survival curves and Cox proportional regression analyses according to CD4+/CD8+ TILs ratio and TRPM7 expression. Patients with high CD4+/CD8+ TILs ratio had a poor (A) overall (p<0.001, Log Rank) and (B) disease-free survival rates (p<0.001, Log Rank) than those with low CD4+/CD8+ TILs ratio. In univariate Cox regression analyzes, high CD4+/CD8+ TILs ratio was significantly associated with both poor (C) overall (p <0.001) and (D) disease-free survival (p <0.001). According to multivariate analyses, patients with high CD4+/CD8+ TILs ratio had shorter (E) overall (HR 1.77, 95% CI 1.22-2.56, p=0.002) and (F) disease-free survival times (HR 1.89, 95% CI 1.35-2.64, p<0.001). (G) The patients with high TRPM7 expression had a poor overall (p<0.001, Log Rank) and (H) disease-free survival rates (p<0.001, Log Rank) than those with low expression. In univariate Cox regression analyzes, high TRPM7 expression was significantly associated with both (I) overall (p<0.001) and (J) disease-free survival (p<0.001). According to multivariate Cox regression analyzes, TRPM7 overexpression was significantly correlated with both worsened (K) overall (p<0.001) and (L) disease-free survival time (p<0.001), independently.
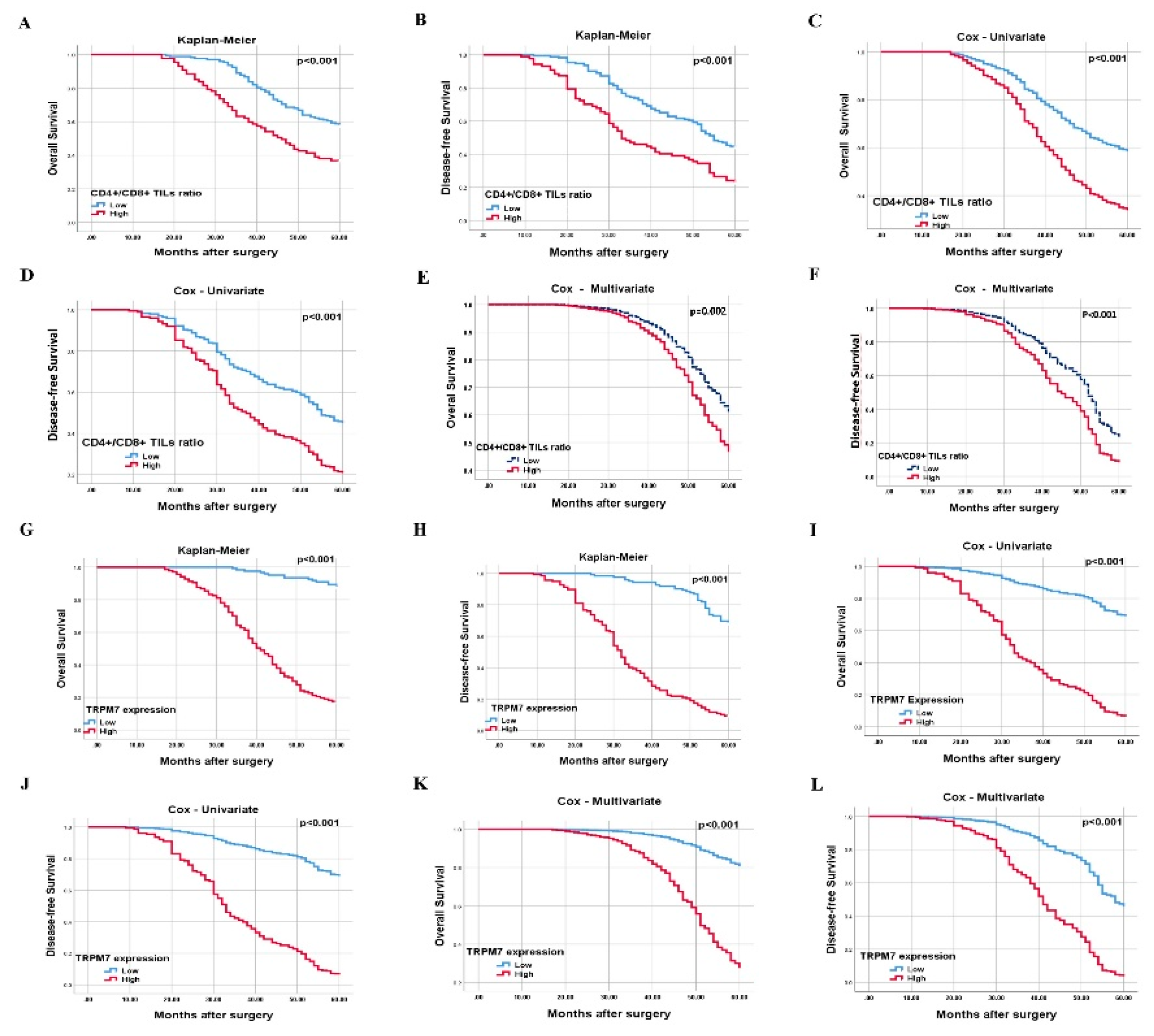

Table 1.
Clinical and pathological features of study cases and their relationship with overall survival [N=259] [univariate Cox regression analysis].
Table 1.
Clinical and pathological features of study cases and their relationship with overall survival [N=259] [univariate Cox regression analysis].
| Parameters | Overall survival [Univariate] | ||
|---|---|---|---|
|
N [%] |
HR [95% CI] | P value | |
| Gender Female Male |
114 [44.0] 145 [56.0] |
1.13 [0.79-1,6] |
0.491 |
| Age 19-44 45-54 55 ≥ |
34 [13.1] 86 [33.2] 139 [53.7] |
1.23 [0.95-1.59] |
0.109 |
| Tumor size [cm] < 5 ≥ 5 |
105 [40.5] 154 [59,5] |
1.39 [0.97-2.31] | 0.070 |
| Tumor site Left Right |
157 [60.6] 105 [39.4] |
0.64 [0.45-0.92] |
0.015 |
| Histopathologic type Adenocarcinoma Mucinous Signet-ring |
154 [59.5] 82 [31.7] 23 [8.9] |
1.27 [0.98-1.66] |
0.075 |
| Histologic grade Well Moderate Poor |
44 [17.0] 173 [66.8] 42 [16.2] |
2.16 [1.56-2.99] |
< 0.001 |
| CD8+ TILs density Low High |
131 [50.6] 128 [49.4] |
0.58 [0.41-0.83] |
0.003 |
| CD4+ TILs density Low High |
129 [49.8] 130 [50.2] |
0.61 [0.43-0.87] |
0.007 |
| CD4+/CD8+ TILs ratio Low High |
172 [66.4] 87 [33.6] |
2.02 [1.42-2.86] |
<0.001 |
| Depth of invasion Submucosa Muscularis propria Pericolorectal tissues |
34 [3.1] 68 [26.3] 157 [60.6] |
2.80 [1.98-3.97] |
< 0.001 |
| Lymph node status Absent 1-3 ≥ 4 |
113 [43.6] 97 [37.5] 49 [18.9] |
3.65 [2.90-4.60] |
< 0.001 |
| Distant Metastasis Absent Present |
186 [71.8] 73 [28.2] |
12.93 [8.67-19.28] |
< 0.001 |
| TNM staging Stage I Stage II Stage III Stage IV |
59 [22.8] 54 [20.8] 78 [30.1] 68 [26.3] |
5.92 [4.45-7.88] |
< 0.001 |
HR: hazard ratio, CI: confidence interval.
Table 2.
Classical prognostic parameters and the effect of TRPM7 overexpression on overall and disease-free survival [multivariate Cox regression analysis].
Table 2.
Classical prognostic parameters and the effect of TRPM7 overexpression on overall and disease-free survival [multivariate Cox regression analysis].
| Cox regression analyses [Multivariate] | ||||
|---|---|---|---|---|
| Parameters | Disease-free survival | Overall survival | ||
| HR [95% CI] | P value | HR [95% CI] | P value | |
| Gender [male/female] | 0.90 [0.63-1.27] | 0.553 | 1.00 [0.67-1.49] | 0.964 |
| Age [19-44/45-54/≥ 55] | 1.08 [0.86-1.36] | 0.500 | 1.18 [0.91-1.53] | 0.205 |
| Site [left/right] | 0.63 [0.45-0.88] | 0.007 | 0.72 [0.49-1.07] | 0.107 |
| Type [adeno/mucinous/signet ring] | 1.06 [0.83-1.35] | 0.626 | 1.05 [0.81-1.37] | 0.677 |
| Grade [well/moderate/poor] | 1.24 [0.92-1.69] | 0.154 | 1.12 [0.81-1.55] | 0.478 |
| CD8+ TILs density [low/high] | 0.47 [0.34-0.66] | <0.001 | 0.59 [0.40-0.85] | 0.006 |
| CD4+ TILs density [low/high] | 0.90 [0.62-1.32] | 0.619 | 1.22 [0.79-1.88] | 0.351 |
| CD4+/CD8+ TILs ratio [low/high] | 1.89 [1.35-2.64] | <0.001 | 1.77 [1.22-2.56] | 0.002 |
| pT [pT1/pT2/pT3] | 0.89 [0.62-1.26] | 0.517 | 1.00 [0.63-1.59] | 0.978 |
| pN [absent/1-3/≥ 4] | 1.37 [0.96-1.95] | 0.077 | 1.42 [0.98-2.07] | 0.063 |
| TNM stage [I/II/III/IV] | 2.32 [1.49-3.62] | <0.001 | 3.30 [1.78-6.10] | <0.001 |
| TRPM7 expression [low/high] | 4.08 [2.65-6.28] | <0.001 | 5,81 [3.16-10.65] | <0.001 |
HR: hazard ratio, CI: confidence interval.
Table 3.
The correlation between TRPM7 expression and classical prognostic parameters.
| Parameters | TRPM7 expression | P value |
|---|---|---|
| Mean ± SD | ||
| Histopathologic type Adenocarcinoma Mucinous Signet-ring |
3.79±2.26 3.30±2.15 4.91±2.42 |
0.010 * |
| Histologic grade Well Moderate Poor |
2.86±1.98 3.74±2.30 4.64±2.15 |
0.001 * |
| CD4+ TILs density Low High |
3.39±2.27 4.08±2.23 |
0.009 ** |
| CD8+ TILs density Low High |
4.14±2.30 3.32±2.18 |
0.003 ** |
| CD4+/CD8+ TILs ratio Low High |
3.33±2.23 4.54±2.17 |
<0.001** |
| Depth of invasion Submucosa Muscularis propria Pericolorectal tissues |
2.05±1.04 3.39±2.09 4.25±2.35 |
<0.001 * |
| Lymph node status Absent 1-3 ≥ 4 |
2.31±1.40 4.65±2.21 5.20±2.19 |
<0.001 * |
| Distant Metastasis Absent Present |
3.02±2.01 5.57±1.85 |
<0.001 *** |
| TNM staging Stage I Stage II Stage III Stage IV |
2.35±1.42 2.22±1.38 4.24±2.30 5.57±1.83 |
<0.001 * |
SD: Standart deviation, * ANOVA, ** Mann-Whitney U, *** independent-samples t-test.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



