Submitted:
26 December 2025
Posted:
29 December 2025
You are already at the latest version
Abstract
Diffusion-weighted imaging (DWI) has been increasingly utilized in the emergent evaluation of acute ischemic stroke (AIS). DWI enhances the sensitivity of diagnosis and enables the use of delayed reperfusion treatments in selected cases. However, DWI is not without limitations. DWI-negative AIS may be encountered in up to 1 out of 4 patients with minor stroke. We searched PubMed and Google Scholar for studies reporting on the prevalence of DWI-negative AIS from 2021 to 2025 and we extensively reviewed the relevant literature. Additionally, we included cases from our practice to highlight key points. DWI-negative AIS prevalence was 16% in one meta-analysis and ranged from 6,9% to 23,2% in identified studies that met our inclusion criteria. Biological, pathophysiological, technical, epidemiological and clinical factors that contribute to DWI-negative stroke are presented in detail. Overall, the application of diffusion imaging modalities in stroke is not bereft of blind spots despite enhanced sensitivity. Over-reliance on advanced neuroimaging and unfamiliarity with limitations predispose to errors in AIS assessment. Awareness about predisposing factors, treatment effect and prognosis guides appropriate decision-making, promoting good outcomes. Prospective appropriately-designed trials should address crucial issues such as the association between timing of imaging and DWI negativity.
Keywords:
DWI-negative stroke
; neuroimaging
; stroke
; DWI limitatitons
; DWI-Reversal
Abstract
Diffusion-weighted imaging (DWI) has been increasingly utilized in the emergent evaluation of acute ischemic stroke (AIS). DWI enhances the sensitivity of diagnosis and enables the use of delayed reperfusion treatments in selected cases. However, DWI is not without limitations. DWI-negative AIS may be encountered in up to 1 out of 4 patients with minor stroke. We searched PubMed and Google Scholar for studies reporting on the prevalence of DWI-negative AIS from 2021 to 2025 and we extensively reviewed the relevant literature. Additionally, we included cases from our practice to highlight key points. DWI-negative AIS prevalence was 16% in one meta-analysis and ranged from 6,9% to 23,2% in identified studies that met our inclusion criteria. Biological, pathophysiological, technical, epidemiological and clinical factors that contribute to DWI-negative stroke are presented in detail. Overall, the application of diffusion imaging modalities in stroke is not bereft of blind spots despite enhanced sensitivity. Over-reliance on advanced neuroimaging and unfamiliarity with limitations predispose to errors in AIS assessment. Awareness about predisposing factors, treatment effect and prognosis guides appropriate decision-making, promoting good outcomes. Prospective appropriately-designed trials should address crucial issues such as the association between timing of imaging and DWI negativity.
1. Introduction
Stroke inflicts great socio-economic burden, which is amplified in low and middle-income countries. In high-income countries, stroke incidence in younger adults has risen and overall stroke prevalence is expected to increase in concert with population growth and aging [1]. Acute reperfusion treatments constitute milestones in acute ischemic stroke management and their application is guided by standard and, in selected cases, advanced neuroimaging modalities. Non-contrast computed tomography (NCCT) has historically been used to exclude the presence of intracranial hemorrhage; a paradigm shift is currently underway, with healthcare systems switching to magnetic resonance (MR) modalities for the initial evaluation of acute ischemic stroke (AIS) in the emergency setting [2]. This shift is supported by the capacity of MR-based protocols to rule in AIS with a diagnostic accuracy reaching 97,5% [3]. DWI was initially applied in the study of central nervous system tumors and pioneering studies in the late 90s established its application in AIS [4,5]. However, MR-based AIS protocols have limitations and still miss a substantial portion of AIS patients, estimated at 6,8% of total cases in a large meta-analysis [6]. The term DWI-negative stroke has been applied to describe this subgroup of patients. Its prevalence is reported between 5 and 25,6% and it is particularly frequent in patients with milder deficits, consisting up to 24% of the minor stroke population [6,7,8]. Even so, there is significant heterogeneity among studies of DWI-negative stroke, particularly regarding the timing from symptom onset to first imaging and the follow-up imaging modality [8]. Additionally, data on the relationship between DWI status and endovascular treatment (EVT) remain sparse and the effect of reperfusion has not been completely outlined [9]. A reluctance to establish a stroke diagnosis has been postulated in the presence of a negative DWI scan [10]. Overreliance on imaging and lack of understanding of DWI limitations, especially by non-neurologists, could lead to withholding treatment in false-negative cases, incurring adverse outcomes and increasing disability. Herein, we reviewed the evidence on DWI-negative stroke extensively and delineated the biological, technical, and individual patient factors that predispose to it. The knowledge of when to expect a negative DWI sequence in a patient with AIS is expected to reinforce accurate diagnosis and treatment in clinical practice.
2.1. Biological Interpretation of Restricted Diffusion in Imaging Studies
Diffusion is the result of Brownian motion of particles in a fluid. In a completely homogeneous liquid, molecules diffuse freely, and their movement is random and isotropic. In the brain tissue, the motion of water molecules is limited by cell bodies and axon membranes and they diffuse in an anisotropic manner [11]. Pathological processes alter the distribution of water molecules between tissues [12]. In AIS, metabolic failure caused by ischemia and hypoxia leads to dysfunction of Na+/K+-ATPase pumps and an ion osmotic gradient that drives the intracellular shift of osmotically active molecules, mainly water particles [13]. This signals the initial step of cytotoxic edema and the first instance of ischemia that can be visualized by DWI within minutes of its onset [5]. During DWI acquisition, the apparent diffusion coefficient (ADC) is additionally calculated by an automated process. The ADC value for each brain region represents the degree of restricted diffusion of water molecules in that area. The ADC map sequence is derived by visual presentation of ADC values in every voxel. Inspection of the standard DWI sequence offers qualitative information about diffusion, while the intensity of signal depression in ADC maps is a quantitative assessment of restriction [12]. Thus, the ability of DWI to capture the initial stages of ischemia and quantitatively assess its severity renders them superior to other sequences.
MRI stroke protocols invariably consist of a combination of sequences; by comparing the features of identified abnormalities, valuable information about lesion age can be obtained. The absence of a visible abnormality in the Fluid Attenuated Inversion Recovery (FLAIR) sequence and the simultaneous identification of a lesion in DWI, termed a DWI-FLAIR mismatch, is thought to represent acute injury and tissue at risk that has not yet undergone irreversible ischemia [14]. At the tissue level, the institution of osmotic changes and cytotoxic edema caused by ischemia, creates ionic gradients that drive the influx of ions through the endothelial cells into the interstitial space to balance ionic concentrations. As ischemia and ionic edema progress, blood-brain barrier disruption and tight-junction damage support the development of vasogenic edema [13]. Signal intensity augments in FLAIR as tissue water content increases and vasogenic edema develops [15]. The DWI-FLAIR mismatch is used as a tissue-clock marker of ischemic penumbra to guide treatment in cases of unknown time of symptom onset or in patients presenting after awakening with symptoms [14,15]. As infarct age progresses from hours to days, dating can be achieved by examining the appearance of the ischemic lesion on the ADC map. Lesions frequently continue to appear hyperintense on DWI at 30 days; reduced ADC signal intensity in the acute phase progressively increases and transiently matches normal parenchyma, a phenomenon known as ADC pseudonormalization [16]. ADC pseudonormalization is expected at days 5-7 and, in some instances, up to 3 weeks after infarction, and subsequently ADC increases [15,16]. Bright appearance of the infarcted area on the ADC map, concurrent with low signal intensity on DWI due to gliosis, indicates chronic infarction [15]. When follow-up evaluation is performed in the subacute phase, the ADC pseudonormalization phenomenon can potentially lead to clinical misidentification of the event as DWI-negative or averted stroke.
DWI is considered to accurately represent the infarct core. However, the notion that DWI lesions completely match areas of irreversible ischemia has been repeatedly challenged [17,18,19,20]. The DWI lesion has been shown to include tissue with low pH that has not yet undergone adenosine triphosphate depletion, and thus may be salvageable if reperfusion is achieved [5,17]. The severity of ADC reduction additionaly informs about DWI reversibility, with mild ADC decreases associated with tissue salvageability and severe reductions predicting irreversible infarction. Even large volumes of DWI hyperintensities have been reported to reverse after successful revascularization with mechanical thrombectomy [21]. Ischemic core, by definition, indicates tissue destined to infarct; yet, there is selective neuronal loss and differences in cellular responses within the area of ischemia [18]. Grey matter (GM) is more vulnerable than white matter (WM), and GM lesions are less likely to exhibit reversibility of restricted diffusion after reperfusion treatment [18,20]. Furthermore, tissue fate depends greatly on inter-patient variability in susceptibility to ischemia, the degree and duration of hypoperfusion and collateral status [5,18,22]. Finally, the volume of DWI abnormality in relation to time from symptom onset has been shown to predict the rate of infarct growth, with greater volumes within the first hours associated with faster progression, lending support to interactions between collateral circulation and DWI lesion morphology [23]. The evidence suggests that DWI visualizes well the early changes taking place during acute infarction but the appearance and characteristics of the DWI lesion are insufficient to adequately inform about the processes that will lead to eventual tissue necrosis.
Consequently, limitations of DWI arise from the biological properties of fluid movement within tissues, as well as from the methodological conventions used to investigate these phenomena. Despite progress since the initial conceptualization and application of DWI in clinical practice, basic mechanisms, such as marked diffusion decrease in acute ischemia and its relation to cell swelling, have not been completely elucidated [11].
2.2. Properties of Diffusion Imaging That Affect Visualization and Sensitivity
Many of the clinically relevant limitations of DWI stem from the technical aspects of the examination. Echo-planar imaging (EPI) is the standard for DWI sequences, allowing for relatively fast scans and reduction in the interference of motion-related artifacts [12]. A standard DWI protocol usually entails scanning in three orthogonal directions and a b-value = 1000 -1500 s/mm2, producing axial slices of a thickness of 5mm, with up to 2mm gap between each slice [5]. The b-value represents a principal parameter of DWI and determines the sensitivity of the sequence to the movement of water molecules. An increase in b-value can be employed to increase sensitivity to hyperacute and small lesions, but such increases also incur signal intensity reduction, an elevated signal-to-noise ratio and introduce artifacts [24,25]. Furthermore, axial slices with gaps in between them are vulnerable to missing small infarcts and an EPI sequence by itself is prone to susceptibility artifacts at the level of the brainstem. In theory, stronger magnetic fields could result in higher sensitivity by enhancing tissue resolution; however, the effect of the field’s strength remains a matter of debate. Initial reports suggested that the rate of false-negative DWI may be higher in 3T compared to 1,5 T magnetic resonance scanners, when evaluating hyperacute stroke patients [27]. A possible mediator of the latter might be the introduction of susceptibility artifacts in stronger fields. However, subsequent studies did not reproduce this finding and reported a similar or higher sensitivity from the use of 3T MRI [5,27]. Ract et al. found an increased identification rate of small and brainstem lesions by 3T MRI when using a 6-direction DWI with a b-value of 2000 s/mm2 , in comparison to 2 other 3T DWI protocols, suggesting that parameter optimization in higher field strength scanners could lead to better detection of smaller lesions [28].
During image acquisition, the DWI sequence is weighted for diffusion alterations by the use of strong gradient pulses but inadvertently information from T2 and spin density changes carries over to a variable extent and contributes to the final result, potentially interfering with DWI diagnostic accuracy [29,30]. Most notably, the T2 shine-through effect arises from the high tissue relaxation time necessary to produce diffusion-weighted images, causing processes that exhibit very long T2 decay times to appear as hyperintensities in DWI without a true underlying diffusion restriction. The T2-shine through phenomenon has also been noted in non-ischemic conditions, such as hypoglycemia, seizures, tumefactive demyelination and drug toxicity [31]. Its presence in stroke mimics may distort the results of studies reporting on DWI-negative AIS prevalence. Close inspection of the signal in the ADC map resolves diagnostic ambiguity in most cases [30,31]. An important impediment to DWI is the impact of eddy-current distortion, which is amplified in magnetic fields of greater strength. Eddy currents lead, among other effects, to geometric distortions and phase shift ghosts (ADC artifacts) and result in errors regarding ADC calculations [30]. Finally, the T2 blackout effect is of less frequent occurrence and pertains to lesions with very short T2 relaxation times that restrict diffusion. Despite true restriction of diffusion, the low T2 signal interferes with DWI signal intensity, leading to lower values and a less bright DWI appearance. This phenomenon is primarily present in cases of intracerebral hematomas [32], and is unlikely to be misinterpreted as DWI-negative AIS.
3.1. Factors Associated with Increased Probability of a Negative Initial DWI
Regarding lesion localization, posterior circulation infarction has been the most frequently identified association with DWI-negative AIS [3,7,33,34,35,36]. A recent meta-analysis estimated the prevalence of DWI-negative AIS at 11-16% overall and recapitulated this finding. Brainstem infarction is tied to the greatest incidence of negative DWI [7,8,37]. From a clinical standpoint, dizziness and internuclear ophthalmoplegia (INO) have been identified as more likely to be accompanied by a normal initial MRI examination [6]. Another study identified isolated vertigo, caudal brainstem syndromes, focal cortical and lacunar syndromes as presentations of DWI-negative stroke [37]. Cases with acute clinical syndromes indicating a brainstem lesion and a “normal” MRI assessment should raise suspicion for DWI-negative AIS and receive appropriate treatment in the emergency setting (Figure 1). Supratentorial lacunar infarcts and lacunar syndromes such as ataxic hemiparesis also represent predictors of negative acute MRI evaluation [7].
Mild deficits and a low National Institutes of Health Stroke Scale (NIHSS) at presentation are additional important predictors of DWI-negatives stroke [5,33]. In the meta-analysis by Alkhiri et al. one out of four patients with minor stroke had a neutral DWI study [8]. In a subgroup analysis of the PRISMS trial, approximately 1 out of 2 patients with mild, non-disabling stroke had negative DWI [38]. NIHSS score is a strong predictor of DWI status and has been associated with the risk of positive conversion in initially DWI-negative cases. The incidence of DWI-negative stroke declines as NIHSS score rises [35,39]. However, absence of diffusion abnormalities has also been reported in severe AIS with NIHSS scores as high as 19 at the time of imaging [40]. The cause may be marked hypoperfusion that produces severe clinical deficits but may be insufficient to establish restriction in diffusion at the time of scan [8,33,37]. These patients must not be missed, as they have been reported to respond to thrombolytic treatment, even in cases of large perfusion deficits [41].
Concerning individual patient characteristics, younger age and female sex have been associated with the probability of DWI-negative infarction, albeit inconsistently [3,8,10,27,38,40,42], as does a history of previous stroke or transient ischemic attack (TIA) [8,10,43]. In a large meta-analysis, ischemic heart disease was more commonly associated with DWI-negative stroke, as opposed to the presence of atrial fibrillation which increased the odds of DWI positivity [8]. In a study of DWI-negative patients with AIS and TIA, smoking and high initial systolic blood pressure were predictive of positive DWI conversion on follow-up imaging [39]. In an Asian cohort, current smoking reduced the likelihood of negative DWI, whereas hypertension and diabetes mellitus did not [40]. In another study in the Asian population, platelet count was correlated with DWI negativity, while hyperlipidemia was not [43]. In studies with greater ethnic/racial heterogeneity, the presence of traditional vascular risk factors, including smoking, did not significantly affect DWI status [8]. Concerning stroke etiology, small vessel disease and stroke of undetermined cause were associated with DWI negativity whereas cardioembolism was predictive of DWI-positive stroke [35,40]. In a small study of 27 patients with large vessel occlusion and negative DWI, M2 occlusion was more common than M1 [42]. Timing of imaging from symptom onset affects DWI outcome. Cut-offs reliably predicting DWI-negative AIS continue to be a matter of debate. Earlier works yielded inconsistent results [34,44,45]. Not all earlier studies applied strict time frames, and in some instances, patients who were imaged days after the index event were included. Saur et al. found that DWI status was time independent within 6 hours after stroke onset [44]. Bulut et al. found that increases in latency between symptom onset and MRI were associated with positive DWI. In this study, all DWI-negative patients were imaged within 7 hours, with a mean time of 4,3 hours [46]. In a more recent study, the majority of DWI-negative AIS patients were imaged within 6 hours, with a median time of 5 hours [37]. A meta-analysis suggested a potential increase in DWI-negative strokes when DWI was performed within 3 to 6 hours from symptom onset [6]. A low signal-to-noise ratio in the first hours of infratentorial infarction enhances this effect [34]. Posterior circulation infarction exhibits delayed visualization of DWI abnormalities when compared to anterior circulation [27]. Conversely, other studies suggested that DWI-negative patients were scanned at later time windows in comparison to those with DWI identifiable lesions [3,10]. Overall, MRI performed in the hyperacute phase of an ischemic event appears to be linked with increased odds of DWI negativity: for every hour elapsing from symptom onset to imaging, the probability for a positive DWI increases by 4% [35].
3.2. Safety and Efficacy of Acute Reperfusion Therapies in DWI-Negative Stroke
Absence of a DWI lesion prior to reperfusion treatment has been associated with better outcomes and a lower risk of intracerebral hemorrhage [8,36,40,42]. In their meta-analysis Alkihi et al. found markedly lower rates of symptomatic intracerebral hemorrhage (sICH). All types of stroke were included, but the study was biased towards patients with minor deficits [8]. In a study directly examining the association between DWI negativity and treatment effect in posterior circulation stroke, a greater proportion of the 100 DWI-negative AIS patients treated with tenecteplase had excellent functional outcome and lower overall mortality compared to the control group [47]. Furthermore, Zhu et al. performed MRI within 72 hours after intravenous thrombolysis (IVT) and reported a statistically significant reduction in hospitalization days and better functional outcome in patients with negative DWI [36]. Accordingly, in a recent study, DWI-negative stroke patients treated with IVT experienced less early neurological deterioration compared to those with a positive DWI [43]. Finally, in a small study of wake-up strokes, the DWI-negative group experienced no hemorrhages after IVT, had lower mRS score and showed a trend towards favorable functional outcome at discharge [48].
Interestingly, the degree of signal reduction in ADC maps is a reliable predictor of hemorrhagic transformation following acute reperfusion treatment [5]. Absence of findings in the DWI of a patient with acute neurological deficits may cause reluctance to treat [10]. Suspicion of a stroke mimic may lead to inappropriate delays or omissions in treatment, leading to potentially harmful effects. Yet, these patients exhibit low hemorrhagic risk and better odds for good prognosis when treated with IVT, including individuals who present in the extended time-window (Figure 2). Limited data suggest that DWI-negative AIS patients are not treated less than their DWI-positive counterparts. A systematic review of 12,018 AIS patients demonstrated higher percentages of IVT in the DWI-negative group (16,31% vs 8,82%) [40]. These patients tended to be younger and presented with lower NIHSS scores possibly leading treating physicians to perceive them as ideal candidates for IVT.
We did not identify any study focusing on the characteristics of DWI-negative patients who were treated with MT. Two of the studies that demonstrated a positive association between negative initial DWI and good outcomes after treatment included MT patients [42,48]. The total number of 20 patients is too small to allow generalization of the findings. Overall, DWI volume before MT, as well as 24 hours after intervention, has been associated with prognosis, with greater volumes inversely correlating to favorable outcomes [47]. Regarding treatment effect, Launhardt et al. performed thrombectomy in 28 patients with basilar artery occlusion, and 5 exhibited DWI lesion reversal following successful reperfusion, which was associated with increased rate of good clinical outcome. They found that DWI reversibility was present only in brainstem infarcts and suggested that this phenomenon might not be uncommon in this brain region [49].
Spontaneous reperfusion, reperfusion following treatment and the reversal of DWI phenomenon (DWIR) may affect the prevalence of DWI-negative AIS. DWIR refers to decreases in the number of hyperintense DWI voxels or in lesion volume in follow-up MRI of treated AIS patients. It is usually partial and only 0,8% of lesions were reported to exhibit complete and sustained reversal prior to widespread use of MT [50,51]. DWIR is estimated to take place in approximately 20-25% of AIS, is associated with spontaneous recanalization, reperfusion treatments, earlier initiation of IVT and MT, is more frequent in small lesion volumes but can be also present in volumes > 70ml and represents a reiteration of the observation that in hyperacute infarction, DWI volume does not entirely equate to the ischemic core [17,51,52,53,54]. Skattor et al. investigated 303 patients who underwent MT and found a greater extent of DWIR in the WM, no difference in likelihood of reversal between cortical and WM regions and a persistence of DWIR after one month in 47% of patients with initial reversal [20]. The magnitude of MT effect may be greater than that of IVT and has been demonstrated even in AIS with large infarct core [20,53]. In an evaluation of 211 MT-treated patients with DWI-ASPECTS 0-5, successful reperfusion predicted DWIR and DWIR exhibited statistically significant association with early neurological improvement and clinical outcomes at 3 months [9].
Spontaneous recanalization has been reported to occur in 20-25% of cases of acute stroke [37,55,56]. Early spontaneous recanalization has been postulated as a mechanism of DWI negativity [7]. Recanalization rates increase with the use of reperfusion treatments during the acute phase [57]. Patients who are scanned very early after symptom onset have elevated odds of a normal DWI. Li et al. enrolled 437 stroke patients who received IVT within 4,5 hours; 54 patients (12,36%) had negative post-IVT DWI [58]. A recent study included 151 AIS patients; 23,2% had negative DWI post-IVT and an association with posterior circulation infarction and lower NIHSS scores was demonstrated. Notably, deficits in the initial CT perfusion (CTP) were found in 37% of the post-IVT DWI-negative group [36]. Additionally, shorter time between symptom onset and treatment administration, as well as longer duration to MRI scan after IVT, have been associated with increased odds of DWI negativity [43,47].
Cases of neurological deficit resolution and negative MRI evaluation following reperfusion treatment (IVT or MT) are referred to as averted or aborted strokes (Figure 3). Predisposing factors for averted stroke and DWI-negative AIS significantly overlap; low NIHSS, younger age, female sex and no evident LVO are associated with both [8,10,22]. Importantly, earlier IVT was linked with better odds of early symptom resolution but not with tissue-defined aversion of stroke [22]. Averted stroke may form a non-trivial proportion of DWI-negative AIS cases. A review of 8101 DWI-negative AIS stroke syndromes reported that aborted stroke comprised 5,2% of all cases [37]. Symptom resolution within 24 hours is frequent after reperfusion treatment in this patient population. An earlier study comprising 254 IVT-treated patients classified 3,5% of the cases as stroke mimics and 9,1% of them as TIAs based on normal DWI on subsequent assessment. The authors suggested that the term averted stroke might have better fit the description of the TIA group, owing to the likelihood that the natural course of the event was altered by treatment [59].
4. Discussion
Our comprehensive review identified rates of DWI-negative stroke ranging widely from 6,6%, to 23,2% in studies including various lesion localizations; however, posterior circulation ischemia is associated with higher rates of DWI negativity (Table 1). The relationship between timing of the scan and symptom onset remains a matter of debate. Nonetheless, large studies support a link between DWI-negative AIS and imaging within the first 6 hours; an increase in the rate of DWI positivity for every hour elapsing from symptom onset suggests that hyperacute scans, combined with other predisposing factors, elevate the probability of negative DWI [5,8,35,37,39,46]. Conversely, an increase in time from IVT administration to MRI completion has been associated with DWI negativity [47], likely owing to the longer duration available to the thrombolytic agent to exert its effect.
Many institutions have added coronal and sagittal diffusion imaging to their MRI protocols to enhance sensitivity, especially in cases of brainstem stroke. Coronal DWI performσ excellently in identifying midbrain lesions and the combination of axial and coronal DWI had perfect accuracy in a study of 134 brainstem AIS [60]. In another study, the application of thin 3mm axial slices increased sensitivity to 100% in the detection of infratentorial lesions; however, the addition of 3mm coronal slices did not improve diagnostic performance [61]. One out of three DWI-negative AIS patients may harbor underlying perfusion deficits and the inclusion of perfusion-weighted imaging (PWI) increases sensitivity of stroke detection [3,36]. The ensuing increase in scanning time is acceptable to avoid missing potentially treatable strokes; yet, 2 to3 out of 100 patients escape detection by the combined use of DWI and PWI. Moreover, perfusion imaging also has limitations, including posterior circulation and lacunar stroke and is more susceptible to motion artifacts [62]. Arterial spin labeling imaging is a promising approach for perfusion evaluation, which may efficiently identify penumbra and diffusion-perfusion mismatch in stroke patients [63]. Meticulous inspection of the FLAIR sequence may obviate the need for additional perfusion imaging. In a setting of large-vessel occlusion, thrombus visualization on FLAIR was present in 68,1% of DWI-negative AIS patients and the “spaghetti sign”, caused by slow flow, was present in 83% of DWI-negative cases [42].
Processing algorithms capable of extracting information about perfusion status from DWI sequences based on intravoxel incoherent motion are presently in development and are limited to research purposes [64]. Furthermore, the application of Artificial Intelligence (AI) software promises faster and more accurate evaluation and processing of DWI. Deep-learning-based AI applications have performed adequately in testing scenarios, with an accuracy of 95% at identifying stroke patients and with a sensitivity of 83,5% to DWI lesions [65]. A two-stage deep-learning, externally validated, module correctly identified patients with unknown time of onset within the 4,5 hours therapeutic window based on DWI-FLAIR mismatch [66]. Nevertheless, AI missed smaller lesions and infarcts with lower ADC signal or minimal slice coverage, similarly to human-read DWI scans [65]. Likewise, automated ADC thresholding software did not consistently match manual delineation performed by an expert and was unreliable for abnormalities of very small size [19]. The inherent variability in ADC lesion values between patients and the influence of parenchymal ADC were important factors contributing to subpar performance by the automated tool [19]. Overall, software with clinical implications needs further testing in prospective trials focused on outcomes before routine implementation [65]. Correctly identifying an acute cerebrovascular event despite a negative DWI study has important prognostic and decision-making value. In comparison to DWI-positive AIS, DWI-negative patients had better odds of good outcomes at discharge and at 3-month follow-up and lower rates of stroke recurrence, combined vascular events, severe disability and mortality [8,40]. Additionally, DWI-negative AIS patients are good candidates for acute reperfusion treatments with lower rates of hemorrhagic complications and favorable functional outcomes compared to their DWI-positive counterparts [8,36,41,43,47,48,58]. Furthermore, conversion to positive DWI on follow-up after an initial negative scan has been associated with early neurological deterioration and a greater risk of stroke recurrence [39]. Kim et al. have devised the predictive DWI-CONVERSION score which uses factors such as the presence of atrial fibrillation, objective hemiparesis, high blood pressure and cholesterol at presentation, NIHSS and symptom duration to identify patients at risk for delayed conversion [39]. Interestingly, studies following DWI-negative patients for longer periods found that lower stroke recurrence risk and better functional outcome were not sustained 1 year after the index event [8]. It is likely that DWI negativity contributes differently depending on disease duration and that other factors may exert a greater impact than DWI status in later stages.
The phenomenon of DWIR has been reported in 26,5% of ischemic strokes and acute reperfusion treatments are a major contributor to it [20,51,52]. A proportion of patients with small infarct volumes are expected to transiently reverse to a volume close to zero. Minute hyperintensities may be missed, and cases erroneously marked as DWI-negative AIS might be included in studies, leading to an inflated prevalence. Instances of persistent and complete lesion reversal are rare and may be better classified as averted stroke [22,50]. A minority of studies on DWI-negative AIS elected to enroll patients after treatment administration without prior MRI [27,36,43,47]. This approach is problematic because it confounds factors predisposing to DWI negativity with treatment effect. We decided not to focus on factors predisposing to DWI-negativity derived from post-IVT AIS studies. Future systematic reviews investigating predictors of DWI-negative stroke had better follow a similar approach to reduce biases. Treatment alters the natural progression of infarction, and in case of early symptom resolution, differentiation between stroke and TIA may be difficult. Furthermore, tenecteplase has been introduced in recent years as an alternative to alteplase and has been shown to act more rapidly and achieve higher rates of complete recanalization [67,68]. Thus, studies using different thrombolytic agents should not be combined in meta-analyses of DWI-negative AIS due to potentially substantial heterogeneity in treatment effects.
Studies that do not incorporate follow-up MRI after a DWI negative scan are at increased risk of including stroke mimics [69]. For instance, transient cytotoxic oedema with restricted diffusion may occur in the post-ictal state due to seizure-related metabolic exhaustion and is typically reversible, thus being distinguishable from irreversible ischemic injury [70]. On the other hand, stroke chameleons are events with uncommon AIS symptoms, which are easy to misidentify under the circumstances of a negative initial DWI. Stroke chameleons share predisposing factors with DWI-negative AIS, notably infratentorial location, younger age, lower blood pressure values at presentation, undetermined etiology and lower NIHSS scores [71]. DWI-negative stroke chameleons are expected to be underrepresented in relevant studies and may lead to potential prevalence underestimation. Finally, the rate of identification of subtle DWI lesions may vary significantly between rater-dependent methods and automated algorithms. A subgroup analysis of WAKE-UP using a convolutional neural network for DWI lesion segmentation, found that 4 patients who were randomized in the trial had no identifiable DWI lesion volume [51,72]. Consequently, future studies on DWI-negative AIS should use validated methods and multiple follow-up imaging evaluations to reduce erroneous inclusions.
The case descriptions herein highlight how confidence in diagnosing acute stroke in the absence of DWI findings guides appropriate management and underscore that, despite constant advances in imaging, stroke remains first and foremost a clinical diagnosis. In our first case a young adult presented hyperacutely with dizziness and signs of INO, a phenotype associated with increased likelihood of negative initial DWI. The second patient sought medical help after symptom fluctuation suggesting spontaneous recanalization followed by subsequent reocclusion. The important clinical deficits, moderately high NIHSS, increased time to imaging and cardioembolic cause would favor DWI positivity in the absence of a counteracting mechanism. Indeed, there was DWI conversion in the post-IVT MRI 24 hours later, with a substantial DWI lesion. Finally, we included a case of averted stroke following treatment with IVT in a presumed etiological background of small vessel disease. Patients with averted stroke should not be misidentified as stroke mimics; however, diagnosing stroke in the context of symptom resolution and negative imaging studies is demanding. Understanding biological and epidemiological factors that predispose to DWI negativity offers additional guidance. These cases highlight the integral role of stroke neurologists in the treatment of DWI-negative AIS.
5. Conclusions
Earlier studies considered the phenomenon of DWI-negative AIS as false-negative. However, a negative DWI may be an expected finding in specific instances of hyperacute stroke. The application of advanced diffusion imaging modalities for acute stroke evaluation has enhanced sensitivity but is not bereft of limitations and blind spots, stemming from the biological correlates of diffusion imaging and the technical aspects of the examination. In a statement paper, the American Academy of Neurology recommended using DWI for acute stroke diagnosis owing to its superiority but noted that it is expected to be insufficient in specific patient populations [73]. Awareness about predisposing factors, interactions with treatment and association with prognosis guides appropriate decision-making. Future research should clarify DWI-negative AIS definition, prevalence and predisposing factors by inclusion of different ethnical populations and onset-to-imaging time intervals.
Author Contributions
Conceptualization, I.N., I.K. and T.K.; methodology, I.N. and I.K.; formal analysis, I.N.,M.M. and S.F.; resources, M.M.,S.F. and T.K.; writing—original draft preparation, I.N., I.K., and T.K.; writing—review and editing, S.F., N.G. and T.K..; supervision, N.G. and T.K.; project administration, T.K.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| MDPI | Multidisciplinary Digital Publishing Institute |
| DOAJ | Directory of open access journals |
| DWI | Diffusion-weighted imaging |
| AIS | Acute ischemic stroke |
| DWI-negative | DWI-negative stroke |
| IVT | Intravenous thrombolysis |
| MT | Mechanical thrombectomy |
| NCCT | Non-contrast computed tomography |
| MR | Magnetic resonance |
| ADC | Apparent diffusion coefficient |
| FLAIR | Fluid attenuated inversion recovery |
| BBB | Blood-brain barrier |
| GM | Gray matter |
| WM | White matter |
| EPI | Echo-planar imaging |
| SNR | Signal-to-noise |
| T | Tesla |
| INO | Intranuclear ophthalmoplegia |
| NIHSS | National Institutes of Health Stroke Scale |
| TIA | Transient ischemic attack |
| LVO | Large vessel occlusion |
| DWIR | DWI-Reversal |
| ICH | Intracerebral hemorrhage |
| ASPECTS | Alberta Stroke Program Early CT Score |
| CTP | Computed tomography perfusion |
| CTA | Computed tomography angiography |
| SWI | Susceptibility-weighted imaging |
| PWI | Perfusion-weighted imaging |
| ASL | Arterial spin labeling |
| AI | Artificial intelligence |
| Afib | Atrial fibrillation |
References
- Feigin, VL; Abate, MD; Abate, YH; et al. Global, regional, and national burden of stroke and its risk factors, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. The Lancet Neurology 2024, 23(10), 973–1003. [Google Scholar] [CrossRef]
- Rapillo, CM; Dunet, V; Pistocchi, S; et al. Moving From CT to MRI Paradigm in Acute Ischemic Stroke: Feasibility, Effects on Stroke Diagnosis and Long-Term Outcomes. Stroke 2024, 55(5), 1329–1338. [Google Scholar] [CrossRef]
- Simonsen, CZ; Madsen, MH; Schmitz, ML; Mikkelsen, IK; Fisher, M; Andersen, G. Sensitivity of diffusion- and perfusion-weighted imaging for diagnosing acute ischemic stroke is 97.5%. Stroke 2015, 46(1), 98–101. [Google Scholar] [CrossRef]
- Welch, KM; Windham, J; Knight, RA; et al. A model to predict the histopathology of human stroke using diffusion and T2-weighted magnetic resonance imaging. Stroke 1995, 26(11), 1983–1989. [Google Scholar] [CrossRef]
- Nagaraja, N. Diffusion weighted imaging in acute ischemic stroke: A review of its interpretation pitfalls and advanced diffusion imaging application. Journal of the Neurological Sciences 2021, 425, 117435. [Google Scholar] [CrossRef] [PubMed]
- Edlow, BL; Hurwitz, S; Edlow, JA. Diagnosis of DWI-negative acute ischemic stroke. Neurology 2017, 89(3), 256–262. [Google Scholar] [CrossRef]
- Sylaja, PN; Coutts, SB; Krol, A; Hill, MD; Demchuk, AM. When to Expect Negative Diffusion-Weighted Images in Stroke and Transient Ischemic Attack. Stroke 2008, 39(6), 1898–1900. [Google Scholar] [CrossRef]
- Alkhiri, A; Alturki, F; Alansari, NM; et al. Prognosis and distribution of ischemic stroke with negative diffusion-weighted imaging: a systematic review and meta-analysis. Front Neurol 2024, 15. [Google Scholar] [CrossRef]
- Panni, P; Lapergue, B; Maïer, B; et al. Clinical Impact and Predictors of Diffusion Weighted Imaging (DWI) Reversal in Stroke Patients with Diffusion Weighted Imaging Alberta Stroke Program Early CT Score 0–5 Treated by Thrombectomy. Clin Neuroradiol. 2022, 32(4), 939–950. [Google Scholar] [CrossRef] [PubMed]
- Makin, SDJ; Doubal, FN; Dennis, MS; Wardlaw, JM. Clinically Confirmed Stroke With Negative Diffusion-Weighted Imaging Magnetic Resonance Imaging. Stroke 2015, 46(11), 3142–3148. [Google Scholar] [CrossRef] [PubMed]
- Le Bihan, D. Diffusion MRI: what water tells us about the brain. EMBO Mol Med. 2014, 6(5), 569–573. [Google Scholar] [CrossRef]
- Baliyan, V; Das, CJ; Sharma, R; Gupta, AK. Diffusion weighted imaging: Technique and applications. World J Radiol. 2016, 8(9), 785–798. [Google Scholar] [CrossRef]
- Gu, Y; Zhou, C; Piao, Z; et al. Cerebral edema after ischemic stroke: Pathophysiology and underlying mechanisms. Front Neurosci. 2022, 16, 988283. [Google Scholar] [CrossRef]
- Thomalla, G; Rossbach, P; Rosenkranz, M; et al. Negative fluid-attenuated inversion recovery imaging identifies acute ischemic stroke at 3 hours or less. Annals of Neurology 2009, 65(6), 724–732. [Google Scholar] [CrossRef]
- Bachtiar, NA; Murtala, B; Muis, M; et al. Non-Contrast MRI Sequences for Ischemic Stroke: A Concise Overview for Clinical Radiologists. Vasc Health Risk Manag 2024, 20, 521–531. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, AK; Mehrotra, G; Bhargava, SK; Agarwal, S; Tripathi, RP. Studies on the time course of apparent diffusion coefficient and signal intensities on T2- and diffusion-weighted MR Imaging in acute cerebral ischemic stroke. J Med Phys. 2008, 33(4), 162–170. [Google Scholar] [CrossRef] [PubMed]
- Asdaghi, N; Campbell, BCV; Butcher, KS; et al. DWI Reversal Is Associated with Small Infarct Volume in Patients with TIA and Minor Stroke. American Journal of Neuroradiology 2014, 35(4), 660–666. [Google Scholar] [CrossRef] [PubMed]
- Goyal, M; Ospel, JM; Menon, B; et al. Challenging the Ischemic Core Concept in Acute Ischemic Stroke Imaging. Stroke 2020, 51(10), 3147–3155. [Google Scholar] [CrossRef]
- Gosch, V; Villringer, K; Galinovic, I; et al. Automated acute ischemic stroke lesion delineation based on apparent diffusion coefficient thresholds. Front Neurol 2023, 14. [Google Scholar] [CrossRef]
- Skattør, TH; Offersen, CM; Nome, T; et al. Mapping DWI signal reversal and long-term tissue outcomes following endovascular therapy in acute ischemic stroke. Eur Radiol. Published online. 1 September 2025. [CrossRef]
- Dang, HQ; Nguyen, TQ; Chiem, DN; et al. Near-Complete Reversal of Large Diffusion-Weighted Imaging Lesion after Thrombectomy: A Case Report and Literature Review. Cerebrovasc Dis Extra 2024, 14(1), 185–192. [Google Scholar] [CrossRef]
- Navi, BB; Bach, I; Czap, AL; et al. Strokes Averted by Intravenous Thrombolysis: A Secondary Analysis of a Prospective, Multicenter, Controlled Trial of Mobile Stroke Units. Ann Neurol. 2024, 95(2), 347–361. [Google Scholar] [CrossRef]
- Rocha, M; Desai, SM; Jadhav, AP; Jovin, TG. Prevalence and Temporal Distribution of Fast and Slow Progressors of Infarct Growth in Large Vessel Occlusion Stroke. Stroke 2019, 50(8), 2238–2240. [Google Scholar] [CrossRef]
- Kim, HJ; Choi, CG; Lee, DH; Lee, JH; Kim, SJ; Suh, DC. High-b-Value Diffusion-Weighted MR Imaging of Hyperacute Ischemic Stroke at 1.5T. AJNR Am J Neuroradiol. 2005, 26(2), 208–215. [Google Scholar]
- Cihangiroglu, M; Citci, B; Kilickesmez, O; et al. The utility of high b-value DWI in evaluation of ischemic stroke at 3 T. European Journal of Radiology 2011, 78(1), 75–81. [Google Scholar] [CrossRef] [PubMed]
- Rosso, C; Drier, A; Lacroix, D; et al. Diffusion-weighted MRI in acute stroke within the first 6 hours. Neurology 2010, 74(24), 1946–1953. [Google Scholar] [CrossRef]
- Zuo, L; Zhang, Y; Xu, X; et al. A retrospective analysis of negative diffusion-weighted image results in patients with acute cerebral infarction. Sci Rep. 2015, 5(1), 8910. [Google Scholar] [CrossRef]
- Ract, I; Ferré, JC; Ronzière, T; Leray, E; Carsin-Nicol, B; Gauvrit, JY. Improving detection of ischemic lesions at 3 Tesla with optimized diffusion-weighted magnetic resonance imaging. Journal of Neuroradiology 2014, 41(1), 45–51. [Google Scholar] [CrossRef] [PubMed]
- Burdette, JH; Elster, AD; Ricci, PE. Acute cerebral infarction: quantification of spin-density and T2 shine-through phenomena on diffusion-weighted MR images. Radiology 1999, 212(2), 333–339. [Google Scholar] [CrossRef]
- Le Bihan, D; Poupon, C; Amadon, A; Lethimonnier, F. Artifacts and pitfalls in diffusion MRI. Journal of Magnetic Resonance Imaging 2006, 24(3), 478–488. [Google Scholar] [CrossRef] [PubMed]
- Gaddamanugu, S; Shafaat, O; Sotoudeh, H; et al. Clinical applications of diffusion-weighted sequence in brain imaging: beyond stroke. Neuroradiology 2022, 64(1), 15–30. [Google Scholar] [CrossRef]
- Silvera, S; Oppenheim, C; Touzé, E; et al. Spontaneous Intracerebral Hematoma on Diffusion-weighted Images: Influence of T2-shine-through and T2-blackout Effects. American Journal of Neuroradiology 2005, 26(2), 236–241. [Google Scholar]
- Brunser, AM; Hoppe, A; Illanes, S; et al. Accuracy of Diffusion-Weighted Imaging in the Diagnosis of Stroke in Patients With Suspected Cerebral Infarct. Stroke 2013, 44(4), 1169–1171. [Google Scholar] [CrossRef]
- Oppenheim, C; Stanescu, R; Dormont, D; et al. False-negative Diffusion-weighted MR Findings in Acute Ischemic Stroke. AJNR Am J Neuroradiol. 2000, 21(8), 1434–1440. [Google Scholar] [PubMed]
- Brunser, AM; Cavada, G; Venturelli, PM; et al. Diffusion-weighted imaging determinants for acute ischemic stroke diagnosis in the emergency room. Neuroradiology 2018, 60(7), 687–692. [Google Scholar] [CrossRef] [PubMed]
- Zhu, C; Qin, W; Xu, J; Hu, W. Perfusion deficits in thrombolysis-treated acute ischemic stroke patients with negative or positive diffusion-weighted imaging. BMC Neurology 2023, 23(1), 380. [Google Scholar] [CrossRef]
- Pektezel, MY; Arsava, EM; Göçmen, R; Oğuz, KK; Topçuoğlu, MA. Diffusion-Weighted-Imaging Negative Stroke Syndromes. Turk J Neurol. 2021, 27(2), 151–157. [Google Scholar] [CrossRef]
- Wang, LL; Khatri, P; Prabhakaran, S; et al. DWI Positivity in Mild, Nondisabling Acute Cerebral Ischemia: Data From the PRISMS Trial. Stroke: Vascular and Interventional Neurology 2025, 5(2), e001613. [Google Scholar] [CrossRef]
- Kim, K; Kim, BJ; Huh, J; et al. Delayed Lesions on Diffusion-Weighted Imaging in Initially Lesion-Negative Stroke Patients. J Stroke 2021, 23(1), 69–81. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y; Jing, J; Pan, Y; Wang, M; Meng, X; Wang, Y. Distribution and prognosis of acute ischaemic stroke with negative diffusion-weighted imaging. Stroke Vasc Neurol. 2022, 7(6). [Google Scholar] [CrossRef]
- Fustier, A; Naggara, O; Tisserand, M; et al. Total mismatch in anterior circulation stroke patients before thrombolysis. J Neuroradiol. 2013, 40(3), 158–163. [Google Scholar] [CrossRef]
- Mekue Fotso, V; Leibinger, F; Rivas Lamelo, S; et al. Management of patients with diffusion-weighted imaging-negative acute ischemic stroke: Retrospective analysis of 47 consecutive patients. Journal of Stroke and Cerebrovascular Diseases 2024, 33(11), 107924. [Google Scholar] [CrossRef] [PubMed]
- Li, J; Huang, C; Liu, Y; et al. DWI and Clinical Characteristics Correlations in Acute Ischemic Stroke After Thrombolysis. medRxiv. Preprint posted online 2025, 2025.06.03.25328925. [Google Scholar] [CrossRef]
- Saur, D; Kucinski, T; Grzyska, U; et al. Sensitivity and interrater agreement of CT and diffusion-weighted MR imaging in hyperacute stroke. AJNR Am J Neuroradiol. 2003, 24(5), 878–885. [Google Scholar]
- Chalela, JA; Kidwell, CS; Nentwich, LM; et al. Magnetic resonance imaging and computed tomography in emergency assessment of patients with suspected acute stroke: a prospective comparison. The Lancet 2007, 369(9558), 293–298. [Google Scholar] [CrossRef] [PubMed]
- Bulut, HT; Yildirim, A; Ekmekci, B; Eskut, N; Gunbey, HP. False-Negative Diffusion-Weighted Imaging in Acute Stroke and its Frequency in Anterior and Posterior Circulation Ischemia. Journal of Computer Assisted Tomography 2014, 38(5), 627. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y; Fu, S; Hu, S; et al. Efficacy and safety of intravenous tenecteplase thrombolysis in diffusion-weighted imaging-negative posterior circulation ischemic stroke. Front Neurol 2025, 16. [Google Scholar] [CrossRef]
- Seyhan, M; Mackenrodt, D; Gunreben, I; et al. Should IV Thrombolysis be given in Patients with Suspected Ischemic Stroke but Unknown Symptom Onset and Without Diffusion-Weighted Imaging Lesion? – Results of a Case-Control Study. Journal of Stroke and Cerebrovascular Diseases 2020, 29(2). [Google Scholar] [CrossRef]
- Launhardt, N; Jesser, J; Hasan, D; et al. DWI Reversibility in Acute Ischemic Stroke Due to Basilar Artery Occlusion Following Successful Recanalization. Clin Neuroradiol. 2025, 35(3), 551–558. [Google Scholar] [CrossRef]
- Freeman, JW; Luby, M; Merino, JG; et al. Negative Diffusion Weighted Imaging After IV tPA is Rare and Unlikely To Indicate Averted Infarction. Stroke 2013, 44(6), 1629–1634. [Google Scholar] [CrossRef]
- Scheldeman, L; Wouters, A; Bertels, J; et al. Reversibility of Diffusion-Weighted Imaging Lesions in Patients With Ischemic Stroke in the WAKE-UP Trial. Stroke 2023, 54(6), 1560–1568. [Google Scholar] [CrossRef]
- Nagaraja, N; Forder, JR; Warach, S; Merino, JG. Reversible diffusion-weighted imaging lesions in acute ischemic stroke. Neurology 2020, 94(13), 571–587. [Google Scholar] [CrossRef] [PubMed]
- Skattør, TH; Bakke, KM; Nome, T; et al. Significance of Subtle Diffusion Weighted Imaging Lesion Dynamics: A Comparative Analysis of Methods for Detecting Diffusion Weighted Imaging Lesion Reversal in Endovascular Stroke Treatment. Stroke: Vascular and Interventional Neurology 2025, 0(0), e001835. [Google Scholar] [CrossRef]
- Skattør, TH; Bjørnerud, A; Nome, T; et al. Predicting lesion reversal in acute cerebral ischaemia via apparent diffusion coefficient threshold on diffusion-weighted MRI. Eur Radiol. Published online. 29 September 2025. [CrossRef]
- Berrada, K; Ouali, IE; Aouadi, SE; Fikri, M; Jiddane, M; Touarsa, F. When stroke hides: A case of negative diffusion MRI. Radiol Case Rep. 2025, 20(10), 5375–5381. [Google Scholar] [CrossRef]
- Li, M; Fu, W; Zhang, K; Hou, Z; Yu, Y; Ma, N. Risk factors and outcomes of patients with early spontaneous recanalization after acute middle cerebral artery occlusion. Quant Imaging Med Surg. 2025, 15(11), 10459–10469. [Google Scholar] [CrossRef]
- Gomis, M; Dávalos, A. Recanalization and Reperfusion Therapies of Acute Ischemic Stroke: What have We Learned, What are the Major Research Questions, and Where are We Headed? Front Neurol 2014, 5. [Google Scholar] [CrossRef]
- Li, G; Feng, X; Wang, C; et al. In-hospital clinical outcomes in diffusion weighted imaging-negative stroke treated with intravenous thrombolysis. BMC Neurol. 2022, 22, 349. [Google Scholar] [CrossRef]
- Uchino, K; Massaro, L; Hammer, MD. Transient Ischemic Attack after Tissue Plasminogen Activator: Aborted Stroke or Unnecessary Stroke Therapy? Cerebrovasc Dis 2009, 29(1), 57–61. [Google Scholar] [CrossRef]
- Alhaj Omar, O; Yenigün, M; Alchayah, F; et al. Combining Coronal and Axial DWI for Accurate Diagnosis of Brainstem Ischemic Strokes: Volume-Based Correlation with Stroke Severity. Brain Sciences 2025, 15(8), 823. [Google Scholar] [CrossRef] [PubMed]
- Lozano, RJ; Shareef, F; Neupane, A; et al. Detectability of acute ischemic stroke with thin (3 mm) axial versus thin (3 mm) coronal diffusion-weighted imaging in patients presenting to the emergency department with acute dizziness. Emerg Radiol. 2025, 32(2), 225–231. [Google Scholar] [CrossRef] [PubMed]
- Nicolas-Jilwan, M; Wintermark, M. Automated Brain Perfusion Imaging in Acute Ischemic Stroke: Interpretation Pearls and Pitfalls. Stroke 2021, 52(11), 3728–3738. [Google Scholar] [CrossRef]
- ElBeheiry, AA; Hanora, MA; Youssef, AF; Al Neikedy, AAM; Elhabashy, A; Khater, HM. Role of arterial spin labeling magnetic resonance perfusion in acute ischemic stroke. Egyptian Journal of Radiology and Nuclear Medicine 2023, 54(1), 43. [Google Scholar] [CrossRef]
- Zimmermann, J; Reolon, B; Michels, L; et al. Intravoxel incoherent motion imaging in stroke infarct core and penumbra is related to long-term clinical outcome. Sci Rep. 2024, 14(1), 29631. [Google Scholar] [CrossRef]
- Alis, C; Ay, E; Genc, G; Bulut, S. Evaluating Deep Learning-Based Commercial Software for Detecting Ischemic Lesions on DWI in Stroke Patients. Diagnostics 2025, 15(18), 2357. [Google Scholar] [CrossRef]
- Namgung, E; Kim, YS; Lee, EJ; et al. Deep learning to identify stroke within 4.5 h using DWI and FLAIR in a prospective multicenter study. Sci Rep. 2025, 15(1), 26262. [Google Scholar] [CrossRef] [PubMed]
- Katsanos, AH; Psychogios, K; Turc, G; et al. Off-Label Use of Tenecteplase for the Treatment of Acute Ischemic Stroke: A Systematic Review and Meta-analysis. JAMA Netw Open. 2022, 5(3), e224506. [Google Scholar] [CrossRef]
- Miller, SE; Warach, SJ. Evolving Thrombolytics: from Alteplase to Tenecteplase. Neurotherapeutics 2023, 20(3), 664–678. [Google Scholar] [CrossRef] [PubMed]
- Pensato, U; Singh, N; Joundi, RA; et al. Left-Sided Neurological Symptoms and Negative Diffusion-Weighted MRI in Suspected Minor Stroke Patients. Canadian Journal of Neurological Sciences Published online. 2025, 1–6. [Google Scholar] [CrossRef]
- Lansberg, MG; O’Brien, MW; Norbash, AM; Moseley, ME; Morrell, M; Albers, GW. MRI abnormalities associated with partial status epilepticus. Neurology 1999, 52(5), 1021–1021. [Google Scholar] [CrossRef] [PubMed]
- Brunser, AM; Lavados, PM; Muñoz-Venturelli, P; et al. Clinical and Radiological Differences between Patients Diagnosed with Acute Ischemic Stroke and Chameleons at the Emergency Room: Insights from a Single-Center Observational Study. Cerebrovasc Dis. 2025, 54(3), 315–322. [Google Scholar] [CrossRef]
- Thomalla, G; Simonsen, CZ; Boutitie, F; et al. MRI-Guided Thrombolysis for Stroke with Unknown Time of Onset. New England Journal of Medicine 2018, 379(7), 611–622. [Google Scholar] [CrossRef] [PubMed]
- Schellinger, PD; Bryan, RN; Caplan, LR; et al. Evidence-based guideline: The role of diffusion and perfusion MRI for the diagnosis of acute ischemic stroke. Neurology 2010, 75(2), 177–185. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
A 49-year-old man presented with dizziness. Clinical examination revealed isolated internuclear opthalmoplegia, indicative of a dorsal pontine lesion. In the initial scan, 2 hours after symptom initiation DWI (a) and ADC map (b) were normal. No signs of bleeding were noted in NCCT (c) and the patient received intravenous thrombolysis with tenecteplase. Repeat imaging within 24 hours revealed a small DWI hyperintensity at the level of the pons (d) along with a corresponding decrease in ADC map (e), consistent with infarction in the area of the medial longitudinal fasciculus. The patient’s symptoms had improved at discharge (NIHSS score: 1, modified Rankin score: 1) and an excellent outcome with no disability (NIHSS score: 0, mRS: 0) was documented at follow-up 3 months later.
Figure 1.
A 49-year-old man presented with dizziness. Clinical examination revealed isolated internuclear opthalmoplegia, indicative of a dorsal pontine lesion. In the initial scan, 2 hours after symptom initiation DWI (a) and ADC map (b) were normal. No signs of bleeding were noted in NCCT (c) and the patient received intravenous thrombolysis with tenecteplase. Repeat imaging within 24 hours revealed a small DWI hyperintensity at the level of the pons (d) along with a corresponding decrease in ADC map (e), consistent with infarction in the area of the medial longitudinal fasciculus. The patient’s symptoms had improved at discharge (NIHSS score: 1, modified Rankin score: 1) and an excellent outcome with no disability (NIHSS score: 0, mRS: 0) was documented at follow-up 3 months later.
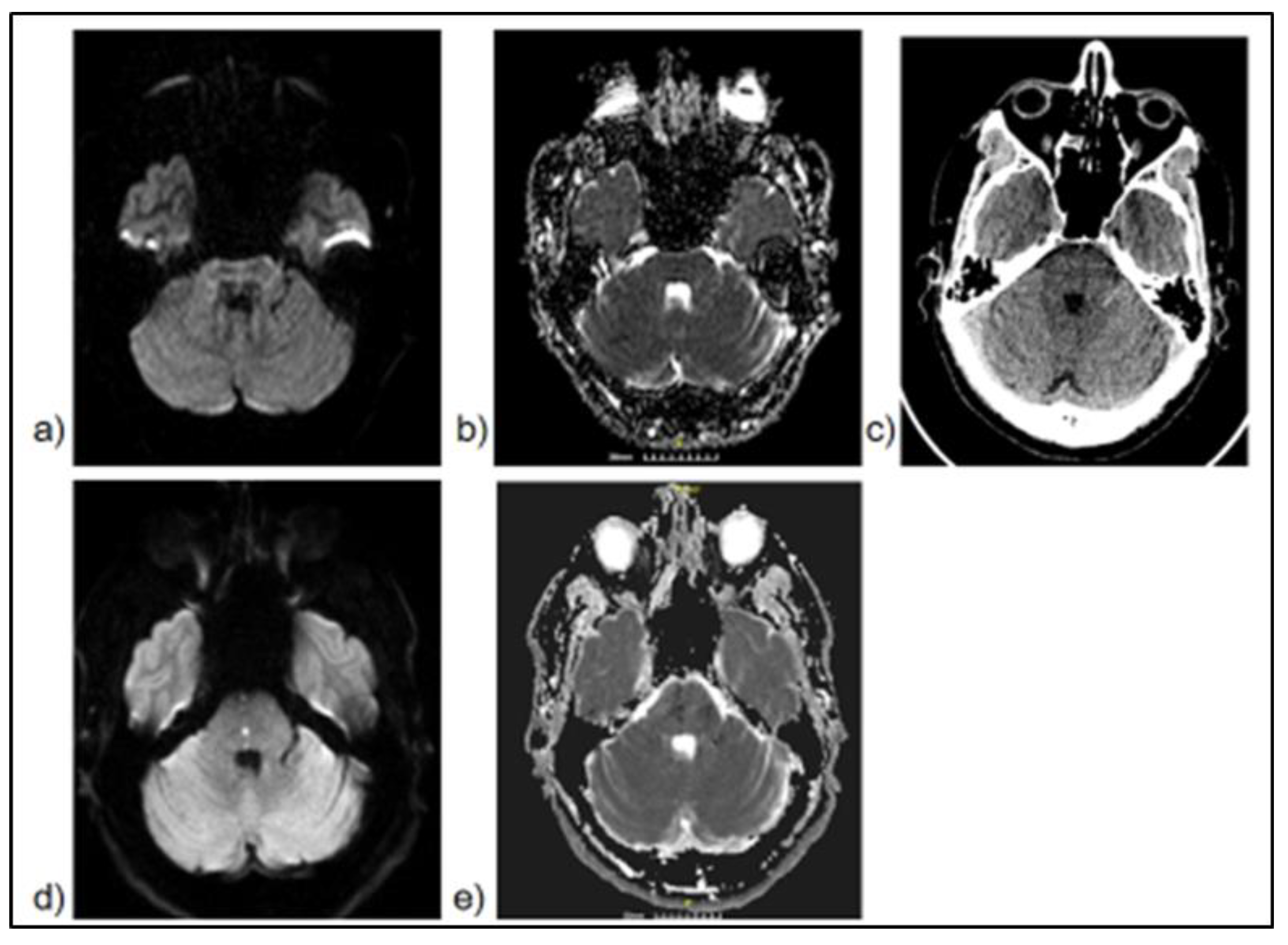
Figure 2.
A 68-year-old woman with a history of hypertension and hypothyroidism awoke from her afternoon sleep with right-sided weakness and difficulty in speaking. She then experienced a transient improvement, without full resolution of symptoms and then deteriorated. She arrived in our hospital 6 hours after symptom onset. Neurological examination revealed aphasia, right-sided facial droop and right arm weakness (NIHSS score: 9). Emergent MRI revealed no signs of lesion in DWI (a) and ADC map (b). CT angiography ruled out the presence of LVO and the peripheral MCA branches showed adequate filling (c). Based on the absence of bleeding and a neutral MRI scan, she was treated as a DWI-negative AIS and received IVT with tenecteplase. Early improvement was noted and subsequent MRI evaluation 20 hours after the first scan revealed an infarct in the distribution of the left MCA (d-f). She was discharged after a short hospitalization, with minimal disability (NIHSS score: 1, mRS: 1). Work-up led to the diagnosis of atrial fibrillation. Initial symptom fluctuation suggests a potential degree of spontaneous reperfusion and improvement after IVT indicates successful recanalization.
Figure 2.
A 68-year-old woman with a history of hypertension and hypothyroidism awoke from her afternoon sleep with right-sided weakness and difficulty in speaking. She then experienced a transient improvement, without full resolution of symptoms and then deteriorated. She arrived in our hospital 6 hours after symptom onset. Neurological examination revealed aphasia, right-sided facial droop and right arm weakness (NIHSS score: 9). Emergent MRI revealed no signs of lesion in DWI (a) and ADC map (b). CT angiography ruled out the presence of LVO and the peripheral MCA branches showed adequate filling (c). Based on the absence of bleeding and a neutral MRI scan, she was treated as a DWI-negative AIS and received IVT with tenecteplase. Early improvement was noted and subsequent MRI evaluation 20 hours after the first scan revealed an infarct in the distribution of the left MCA (d-f). She was discharged after a short hospitalization, with minimal disability (NIHSS score: 1, mRS: 1). Work-up led to the diagnosis of atrial fibrillation. Initial symptom fluctuation suggests a potential degree of spontaneous reperfusion and improvement after IVT indicates successful recanalization.
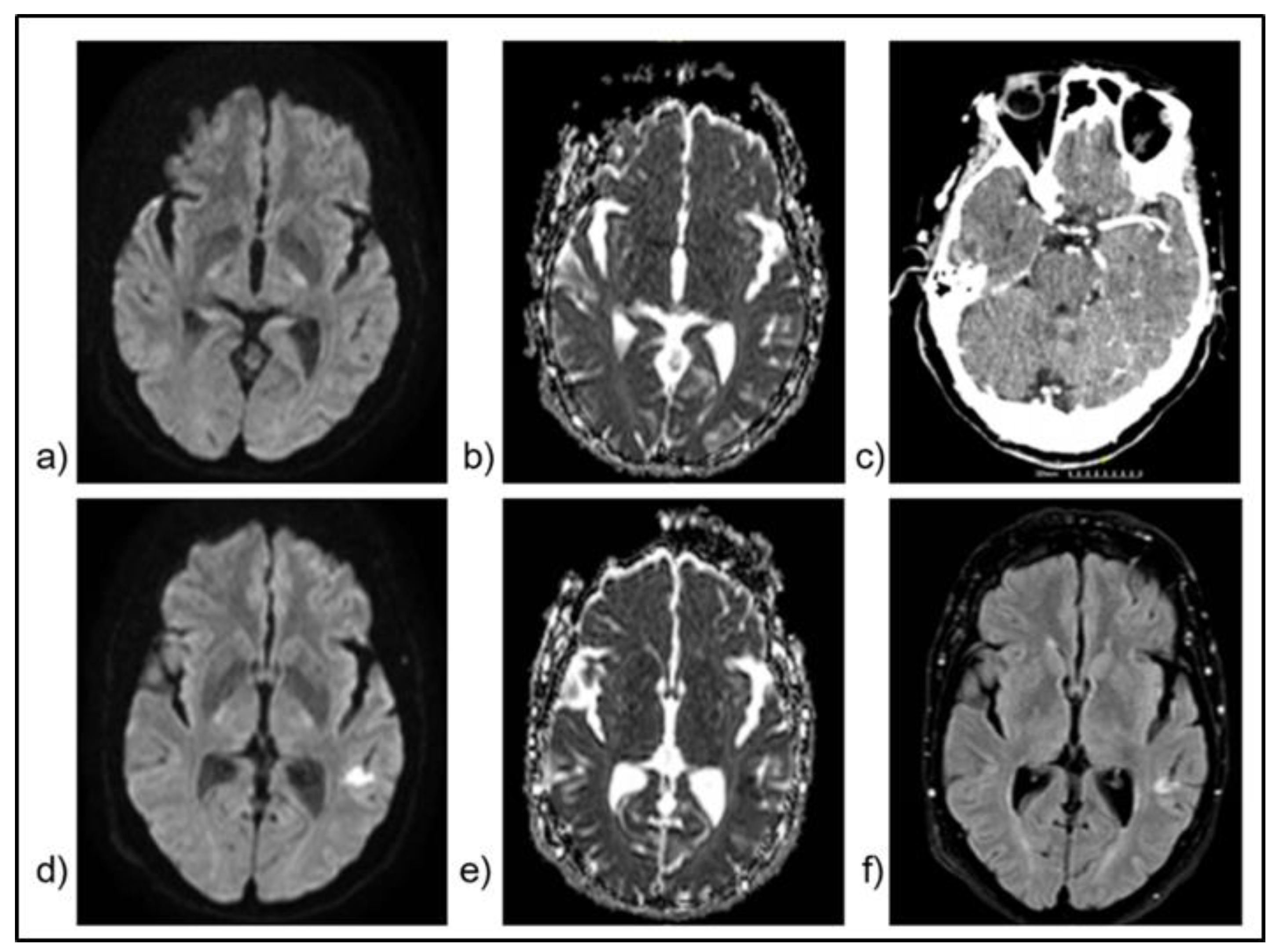
Figure 3.
A 83-year old woman with a medical history of hypertension, end-stage renal disease and breast cancer in remission, presented with right hemiparesis 3 hours after symptom onset (NIHSS score: 6, mRS: 4). Initial NCCT (a-b) and CT angiography (CTA) (c) were unrevealing of parenchymal damage or large vessel occlusion. She received IVT with alteplase within 30 minutes of arrival and experienced complete symptom resolution within the first 20 hours. In MRI 9 days later, no signal hyperintensities were noted in DWI (d) and FLAIR (e) sequences. In T2* imaging (f) signal depression indicating bleeding or the presence of thrombus within a vessel was not identified. Thorough investigation during hospitalization did not reveal any likely cause of stroke mimic. This case represents an averted stroke: complete symptom resolution following reperfusion treatment, with negative subsequent imaging. .
Figure 3.
A 83-year old woman with a medical history of hypertension, end-stage renal disease and breast cancer in remission, presented with right hemiparesis 3 hours after symptom onset (NIHSS score: 6, mRS: 4). Initial NCCT (a-b) and CT angiography (CTA) (c) were unrevealing of parenchymal damage or large vessel occlusion. She received IVT with alteplase within 30 minutes of arrival and experienced complete symptom resolution within the first 20 hours. In MRI 9 days later, no signal hyperintensities were noted in DWI (d) and FLAIR (e) sequences. In T2* imaging (f) signal depression indicating bleeding or the presence of thrombus within a vessel was not identified. Thorough investigation during hospitalization did not reveal any likely cause of stroke mimic. This case represents an averted stroke: complete symptom resolution following reperfusion treatment, with negative subsequent imaging. .


Table 1.
Studies reporting on DWI-negative AIS prevalence since 2021.
| Study | DWI-negative AIS prevalence | Description/Limitations |
| Pektezel et al., 2021 [37] |
6,6% 8101 cases, 535 DWI-negative |
Combination of a single center cohort of 1506 patients [DWI-negative n=20, (1,3%)] with cases from the literature: increased heterogeneity and potential underestimation. |
| Kim et al., 2021 [39] |
13,2% 5,271 cases, 694 DWI-negative |
Retrospective single-center study that included TIA patients: potential overestimation. |
| Wang, Yu et al., 2022 [40] |
7,7% 12,026 cases, 932 DWI-negative |
Prospective multicenter cohort study, included a relatively low number of non-minor (NIHSS > 5) AIS patients. |
| Zhu et al., 2023 [36] |
23,2% 151 cases, 35 DWI-negative |
Retrospective single-center study, smaller sample size compared to the other studies. DWI status was evaluated post-IVT. |
| Fotso et al., 2024 [42] |
3,9% 1210 cases, 47 DWI-negative |
Retrospective single-center study. Only patients with anterior circulation AIS were enrolled. |
| Li et al., 2025 [43] |
22,74% 277 cases, 63 DWI- negative |
Single-center study. Included only posterior circulation strokes. DWI status was evaluated post-IVT. Small sample size and missing clinical data in a small number of patients, variability in follow-up: may have introduced biases and the risk of stroke mimics inclusion. |
| Alkhiri et al., 2024 [8] |
16%, 11% after sensitivity analysis. 16.268 cases, 2603 DWI-negative |
Meta-analysis. Significant heterogeneity between studies, I2 = 91% estimated by the authors after sensitivity analysis. Temporal heterogeneity: the earliest study was conducted in 2000 and the most recent in 2023. Due to potential overrepresentation of minor stroke patients, sensitivity analysis was performed. |
|
DWI: Diffusion-weighted imaging, AIS: Acute ischemic stroke, TIA: Transient ischemic attack, NIHSS: National Institutes of Health Stroke Scale, IVT: Intravenous thrombolysis, I2 : I2 heterogeneity index | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



