Submitted:
24 December 2025
Posted:
25 December 2025
You are already at the latest version
Abstract
Background/Objectives: This study assessed immediately after response of alternate rapid maxillary expan-sions-constrictions with 2-hinged expander on craniofacial structures, supporting teeth periodontium in Class III malocclusion with maxillary retrusion.
Materials and Methods: Treatment group consisted of 15 growing patients with Class III malocclusion, 6 girls 9 boys mean ages 12.60 and 13.10 years respectively, who were treated with 2-hinged expander/Alt-RAMEC; Control group consisted of untreated Class III malocclusion of 27 patients with, 7 girls 20 boys mean ages of 12.50 and 12.60 years respectively in Department of Orthodontics of the Ankara University.
The 2-hinged expander screw was daily four times opened the first week and closed second week. These recurrent series were completed with expansion in the 9th week. Craniofacial structures and periodontal status were evaluated at the end of Alt-RAMEC. The data were analyzed with the SPSS 20 package program. Groups were compared with the Mann Whitney U test. Intra group differences were analyzed by Wilcoxon test at T1-T2.
Results: Maxilla moved forward 2.56 mm. Wits appraisal and vertical dimension was increased. Positive changes occurred in the facial profile by forward movement of the maxilla in Alt-RAMEC group. Gingival index, bleeding index and periodontal pocket depth of supporting teeth showed significant increase while plaque index unchanged.
Conclusion: Satisfactory forward movement of the maxilla was achieved just after the combined use of the Alt-RAMEC protocol and the 2-hinge expander. An inflammatory reaction was detected in the periodontium of the supporting teeth where the 2-hinged expanders were placed.
Keywords:
Alt-RAMEC
; maxillary retrusion
; periodontal status
; skeletal class III
1. Introduction
Rapid maxillary expansion (RME), the oldest known method of separating the naso-maxillary complex from the cranium have been widely investigated [1,2,3]. Face mask (FM) after RME is an admitted concept for more effective stimulation of osteogenesis in circum-maxillary sutures [4,5,6,7]. Despite direct tension effect created by RME on the mid-palatal suture and its positive contribution to the transverse size of the maxilla is certain, it decreases towards the circum-maxillary sutures. Therefore, the sagittal effect of expansion on maxilla is less impressive than its transverse effect. Biederman and Chem suggested that the maxilla moves backward, if the rotation center of the RME is somewhere on the mid-palatal suture; and the maxilla moves forward, if rotation center occurs bilaterally at two points somewhere the postero-lateral of the maxilla [2]. It is necessary to keep the expansion period long to develop forward movement of the maxilla. However, over-expansion causes some problems such as buccal non-occlusion, palatal mucosal irritation, periodontal problems supporting teeth. Therefore, in the last decade, a new protocol called Alternate Rapid Maxillary Expansions and Constrictions (Alt-RAMEC) is introduced to ensure an effective forward movement of the maxilla without over-expansion [8]. Rationale of the Alt-RAMEC is based on consecutively pressure and tension force transmitting to the circum-maxillary sutures via mid-palatal suture to stimulate sutural osteogenesis. The foregoing is realized by developing rotation center in the posterior-lateral of the maxilla using 2-hinged expander [8]. Recently, the Alt-RAMEC combined use with tissue-born hyrax expander has been widely used for treatment of Class III malocclusion with maxillary retrusion with or without FM [9,10,11,12]. However, few studies have been presented concerning about the pure effect of Alt-RAMEC with alone 2-hinged expander on maxillary anterior movement [13,14].
Hard tissue periodontal structures after RME have been widely investigated [1,2,3]. Recently, the effect of RME and Alt-RAMEC on hard tissue periodontium has been quantitatively investigated by computed tomography (CT) [15,16]. The tooth-born expanders might cause more root resorption and buccal bone plate dehiscence than tooth-tissue-borne expanders ([15]. However, there is insufficient data in the literature regarding the effect of both RME and Alt-RAMEC on the soft tissue periodontium.
The aim of the present prospective comparative study, therefore, was to evaluate the pure effect of Alt-RAMEC combined use of 2-hinged expander on maxillary sagittal position for correction of growing skeletal Class III malocclusion with maxillary retrusion in comparison with in untreated Class III subjects. The aim of this study was to investigate the initial reaction in the maxilla and periodontium of the supporting teeth following the use of a 9-week Alt-RAMEC combined 2-hinged expander.
2. Materials and Methods
Subjects
This clinical prospective study was planned to be conducted using cone beam computed tomography (CBCT). However, because of the fact that the Ethics Committee did not approve using CBCT in growing individuals lateral cephalometric film were used.
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of Faculty of Dentistry, University of Ankara, Turkey, (Date. December 20, 2019/No. 36290600). Written and verbal informed consent were obtained from the parents or legal guardians prior to the interview.
According to the power analysis, it was determined that this clinical study should be conducted on a minimum of 20 patients. The study started with 20 patients (8 females and 12 males), but continued with 15 patients because the patients could not attend the clinical controls due to covid epidemic.
A sample of 15 patients 6 girls (mean ages 12.60±1.42 years); 9 boys (mean ages 13.10±1.92 years), respectively, with skeletal and dental Class III malocclusion with maxillary retrusion, no transvers discrepancy was treated consecutively with the Alt-RAMEC with 2-hinged expander at the Department of Orthodontics of the Ankara University.
Inclusion criteria on the pretreatment lateral cephalograms were maxillary retrusion with Nperp-A; -1±1.91, Nperp-Pg; 5.59±6.63, Wits appraisal; -3.13±2.88 mm, normodivergency with FH/MP; 22.46±3.38, anterior crossbite with overjet; -0.43±1.51 and overbite; 2.93±1.44, cervical vertebrae maturation (CVM) stage II and III, and late permanent dentition. Exclusion criteria were absence of maxillary posterior teeth, congenital tooth anomalies, impacted or ankylosed teeth, periodontal disease and previous orthodontic treatment (Table 1).
Alt-RAMEC group was compared to a sample of 27 subjects 7 girls (mean ages 12.50±1.54 years); 20 boys (mean ages: 12.60±1.45 years), respectively presenting untreated with skeletal and dental Class III malocclusion (Control Group). The lateral cephalograms belonging to the Control group were selected from among the cases enrolled between 1992 and 1993 from the files of the Department of Orthodontics, Ankara University, with the following criteria: Maxillary retrusion with Nperp-A; -2.14±4.10, Nperp-Pg; 4.43±3.82, Wits appraisal; 0.29±0.76 mm, normodivergency with FH/MP; 25.14±5.58, anterior crossbite with overjet, -0.14±0.38 and overbite, 0.14±0.38, CVM stage II and III (Table 1).
Appliances Design, Expansion Protocol
The tooth-born 2-hinged expander banded on the maxillary first premolars and molars was used for forward movement of the maxilla. The front and rear extensions of the 2-hinged expansion screw (Best Dent, Kaoshiung, Taiwan) placed at the midline of palate were placed from away 1-1.5 mm the palatal mucosa. While bands were cemented with glass ionomer, the anterior extension arms were bonded to the palatal surface of the incisors and canines (Figure 1 a,b). Expansion was commenced a day after cementation. Daily rhythm of the screw started with opening 4 times a day, two in the morning; two in the evening, in the first week; same rhythm was repeated with closing in second week. The procedure was continued for 9 consecutive weeks and was terminated in the 9th week with opening. The activation rate of the screw was 1 mm daily. The activation was performed at 5- or 10-minute intervals. Turning procedure was explained to the patient's parents and activation diary were kept by the patients (Table 2). Visits were arranged as one week, four weeks and nine weeks after the start of the Alt-RAMEC. Patients were prevised to apply to the clinic if the expander damaged. After positive overjet was achieved by Alt-RAMEC, quad helix was used for retention.
Cephalometric Analysis
Lateral cephalograms were taken before (T0) and immediately after the Alt-RAMEC (T1) according to a standardized technique [17]. Lateral cephalometric landmarks in the sagittal plane were measured by a Cartesian coordinate system in addition to conventional methods. A horizontal reference line (HRL) rotated 7 degrees downward the Sella-Nasion plane was used as the x-axis. A perpendicular line (VRL), passing through point T (the tuberculum Sella joins the top of the front wall of Sella Turcica) to the x-axis, served as the y-axis. 63 variables, 7 angular, 56 linear, were generated for each tracing to evaluate the skeletal, dental and the soft tissue profile changes (Figure 2, Figure 3, Figure 4, Figure 5, Figure 6 and Figure 7). The Alt-RAMEC group had a magnification of 1.08%, whereas the control group subjects had a 1.13% magnification. In order to standardize the data, all cephalometric measures were converted to a 1.08.0% enlargement because the majority of the cephalograms had this magnification factor. Dental casts were collected T0 and T1 for inter-canine, inter-first premolar inter-molar, and upper arch length measurements by means of a digital caliper (Shan, 0-150 mm digital caliper) (Figure 8).

Periodontal Evaluation
Periodontal status in terms of bacterial plaque, periodontal pocket depth, bleeding and the amount of keratinized gingiva on probing by periodontal probe at the mesio-buccal and mesio-palatal sites of the maxillary central incisors, first premolars and molars were evaluated and scored [18] at T0 and T1 as follows:
1. Plaque Index (PI): Plaque existing on the four surfaces of the teeth is numbered between 0 and 3. The score value is obtained by total divided into four. 0 score means no plaque on the surface, 1 means a film-thick plaque invisible to the naked eye, but noticeable when the end tip is swept over the surface; 2 means a medium thickness plaque visible to the naked eye, 3 means intensive soft attachment or tartar.
2. Gingival Index (GI): Gingival margin is evaluated about color change, edema and bleeding and scored between 0-3. Healthy gingiva-0; slight inflammation and discoloration, edema, no bleeding-1; moderate inflammation, bright red gingiva, edema, bleeding-2; severe inflammation, marked redness and edema, tendency to spontaneous bleeding and ulceration-3.
3. Periodontal Pocket Depth (PPD): It is measured by the periodontal probe.
4. Bleeding Index (BI): Presence or absence of bleeding is monitored within 10-15 seconds after probing. A score is given as no bleeding-0, bleeding-1.
5. Keratinized Gingival Tissue Measurement (KGT): The distance between the gingival margin and the muco-gingival line, which is the borderline between the attached gingiva and oral mucosa, is measured.
Statistical Analysis
The data were analyzed with the SPSS 20 package program. Shapiro Wilk's test was conducted to investigate whether the distribution of variables is normal. The significance level (p) was evaluated at 0.05. The study groups were compared with the Mann Whitney U test. Standardized z values were used for the Mann Whitney U Test. Intra group changes were analyzed by Wilcoxon test.
Twenty-two lateral cephalograms selected randomly were retraced and measured by the same operator. A combined error of landmark location, tracing and measuring was determined. The error standard deviation for each dimension was calculated from the double determinations with the aid of Dahlberg’s formula. The repetition coefficient was found between 0.943 and 1.00.
3. Results
The ages, sexes and growth stages according to the CVM stages at baseline are shown in Table 1. Table 3 shows the comparisons of some important cephalometric values between the groups before treatment. Statistically significant difference was no observed between the groups except overjet and overbite before treatment.
Anterior movement of point A and ANS (A-VRL, Nperp–A, ANS-VRL) and posterior movement of the chin (Nperp-Pg) were significant in the Alt-RAMEC group after Alt-RAMEC (p< 0.05, p<0.01; Table 4). Point A and Nperp-A values presented significant differences between the groups. The anterior movement at points A and ANS were 2.56 mm and 2.40 mm for the Alt-RAMEC group; -1.57 mm and -1.43 mm for the Control group respectively. Posterior movement of the chin (Nperp-Pg) was significant for the Alt-RAMEC group (p<0.05; Table 4). Point PNS (PNS-HRL) showed significant differences between groups (p<0.05; Table 4); (PNS-HRL) increased significantly for the Alt-RAMEC group (p<0.05; Table 4). Co-A showed significant difference in both groups and it increased for the Alt-RAMEC group (p<0.05; Table 4). Point Co (Co-VRL) moved anteriorly in the control group (p<0.05; Table 4). Occlusal plane angle increased significantly in the control group (p<0.05; Table 4). (ANS-Me) increased significantly for the Alt-RAMEC group and also it showed a significant difference between the groups (p<0.05; Table 4). The Alt-RAMEC group presented significant increases for FH/MP and NBa-PtmGn angles and these values showed a significant difference between the groups.
(Ui-Nperp) and (Li-APg) were significant for the Alt-RAMEC group (p<0.05; Table 4). The decrease of overbite (-1.87) and increase of overjet (2.14) were significant for the Alt-RAMEC group and these values demonstrated a significant difference between the groups (p<0.05 and p<0.01; Table 4). Wits appraisal showed significant increase for the Alt-RAMEC group and it also showed a significant difference between the groups (p<0.05; Table 4).
4. Discussion
The common inference is that maxillary protraction using FM is facilitated after RME [4,5,6,7]. Combined use FM with RME qualified sutural expansion and protraction osteogenesis as a form of physeal distraction osteogenesis has been demonstrated both clinically and experimentally [1,19]. The mid-palatal suture is separated in 5 days with RME, while sutures surrounding the maxilla release in longer time. So, over-expansion is required to transmit the pressure and tension on the circum-maxillary sutures for easily protraction [6]. However, over-expansion increases the maxillary transverse dimension in cases where it is not necessary. Biederman and Chem suggested that the rotation center of expansion force is need to locate around the posterior-outer region of the maxilla for anterior movement of the maxilla [2]. Three decades later, the Alt-RAMEC protocol separating the maxilla from the surrounding sutures without over-expansion was introduced [8]. Actually, animal studies revealed that maxillary forward movement of 2.8 mm was achieved by the Alt-RAMEC combined use of 2-hinged expander [8,20].
Considering that the malocclusion type and growth period of the samples selected in this study are similar, it can be concluded that the significant forward movement in the maxilla is due to Alt-RAMEC combined use with 2-hinged expander. It was claimed that rotation center of expansion was carried to the posterior outer part of the maxilla by the 2-hinged expander [8]. 7-week Alt-RAMEC is sufficient to release sagittal sutures around the maxilla, while a 9-week Alt-RAMEC is required for coronal sutures [8,20]. Indeed, Huang et al. reported that the 2-hinged expander/Alt-RAMEC collaboration provides more maxillary anterior movement than the Hyrax expander/Alt-RAMEC, though the importance of the Alt-RAMEC rather than the expander type for skeletal maxillary advancement [21]. Actually, the amount of maxillary anterior displacement in the Alt-RAMEC group was almost twice that of the control group (2.56 mm versus -1.57 mm) in the present study. The conspicuous forward movement of the A and ANS points can be explained as moving the rotation center of expansion to the posterior region of the maxilla with Alt-RAMEC while there was no change in the PNS point in this study. Therefore, the immediate position of the maxilla confirmed the hypothesis that the rotation center develops in the posterior outer region of the maxilla by the Alt-RAMEC/2-hinged expander combination in this study. Counterclockwise rotation in the palatal plane, posterior rotation of the mandible and an increase of anterior face height were consistent with previous studies [8,9,10,11,12,13].
The posterior rotation of the mandible, an increase of the vertical facial dimension, lower anterior face height and facial axis angle occurred as a result of downward movement of PNS and the upper molars with Alt-RAMEC in this study. Contrarily, Kaya et al. reported that minimal rotational effect with application of FM to mini screw after Alt-RAMEC [11]. Maxillary and mandibular vertical positional changes contributed positively to the Wits value in this study as similar previous studies [11,12].
The forward movement of the upper incisors was as much as the maxillary movement, which is evidence that the 9-week-Alt-RAMEC creates maxillary skeletal movement in this study. The overjet increased by the forward movement of the maxilla and the backward movement of the mandible. Actually, effective expansion took place in the last week, as the Alt-RAMEC was completed in the 9th week with expansion, thus, buccal non-occlusion no occurred in this study.
Profile concavity was reduced by clockwise rotation of the mandible as a result of counterclockwise rotation of the maxilla in this study in addition to anterior movement of the nose and the upper lip as previous studies [9,10,11,12,13].
Individual variations for good periodontal condition is prominent [22]. CT studies showed that RME decreases the buccal bone thickness of the supporting teeth and increases the palatine bone thickness [15]. Gandedkar and Liou revealed that the Alt-RAMEC reduced the buccal alveolar bone thickness and thickened the palatal alveolar bone plate at the anterior anchor teeth. They related these results to the initial condition of the periodontal tissue of the supporting teeth [16]. However, there is still lack knowledge about the soft tissue periodontium response of supporting teeth to the Alt-RAMEC. Therefore, this prospective study could be the first to investigate the immediate effects of 9-weeks-Alt-RAMEC/2-hinged expander combination on the soft-tissue periodontium. Although plaque index controlled in this study, GI, BI, and PPD revealed significant increase for incisors and supporting teeth even though clinically not dramatic. These results could not be compared with any data, since no any previous study in regard the soft tissue periodontium response to the Alt-RAMEC.
5. Conclusions
- Evidence based on outcomes of this study revealed that Alt-RAMEC/2-hinged expander combinations provide more favorable immediate maxillary skeletal advancement (2.56 mm) in growing period.
- Class III malocclusion characterized by maxillary retrusion was improved by combination of both the maxillary counterclockwise rotation and the mandibular clockwise rotation.
- Although plaque formation was controlled, an inflammatory tendency was found in the soft tissue periodontal status during Alt-RAMEC.
Author Contributions
Conceptualization, N.C.T and H.G.; methodology, N.C.T.; software, N.C.T.; validation, N.C.T, and H.G.; formal analysis, N.C.T.; investigation, N.C.T; resources, N.C.T.; data curation, N.C.T.; writing—original draft preparation, N.C.T.; writing—review and editing, H.G.; visualization, N.C.T.; supervision, H.G.; project administration, H.G. All authors have read and agreed to the published version of the manuscript.
Funding
“This research received no external funding”.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ankara University, Faculty of Dentistry, Non-Clinical Scientific Studies Ethics Committee (December 20, 2019/No. 36290600).
Informed Consent Statement
“Informed consent was obtained from all subjects involved in the study.” “Written informed consent has been obtained from the patient(s) to publish this paper”
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| RME | Rapid Maxillary Expansion (RME) |
| Alt-RAMEC | Alternate Rapid Maxillary Expansion and Construction |
| FM | Face Mask |
| CT | Computerized Tomography |
| CBCT | Cone Beam Computerized Tomography |
| HRL | Horizontal Reference Line |
| VRL | Perpendicular Line |
| CVM | Cervical Vertebrae Maturation |
| PI | Plaque Index |
| GI | Gingival Index |
| PPD | Periodontal Pocket Depth |
| BI | Bleeding Index |
| KGT | Keratinized Gingival Tissue |
References
- Haas, AJ. Rapid expansion of the maxillary dental arch and nasal cavity by opening the midpalatal suture. Angle Orthod. 1961, 31, 73–90. [Google Scholar]
- Biederman, W; Chem, B. Rapid correction of Class III malocclusion by midpalatal expansion. Am J Orthod. 1973, 63, 47–55. [Google Scholar] [CrossRef]
- Krag, G; Duterloo, HS; Ten Bosch, JJ. The initial effect of the orthopedic forces: a study of alterations in the craniofacial complex of a macerated human skull. Am J Orthod. 1982, 81, 57–64. [Google Scholar] [CrossRef]
- Nanda, R. Protraction of maxilla in Rhesus monkeys by controlled extraoral forces. Am J Orthod. 1978, 74, 121–141. [Google Scholar] [CrossRef]
- Williams, MD; Sarver, DM; Sadowsky, PL; Bradley, E. Combined rapid maxillary expansion and protraction facemask in the treatment of Class III malocclusions in growing children: A prospective long-term study. Semin Orthod. 1997, 3, 265–274. [Google Scholar] [CrossRef]
- Alcan, T; Keles, A; Erverdi, N. The effects of a modified protraction headgear on maxilla. Am J Orthod Dentofacial Orthop. 2000, 117, 27–38. [Google Scholar] [CrossRef] [PubMed]
- Vaughn, GA; Mason, B; Moon, HB; Turley, PK. The effects of maxillary protraction therapy with or without rapid palatal expansion: A prospective, randomized clinical trial. Am J Orthod Dentofacial Orthop. 2005, 128, 299–309. [Google Scholar] [CrossRef] [PubMed]
- Liou, EJW; Tsai, WC. A new protocol for maxillary protraction in cleft patients: repetitive weekly protocol of Alternate Rapid Maxillary Expansions and Constrictions. Cleft Palate Craniofac J. 2005, 42, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Masucci, C; Franchi, L; Giuntini, V; Defraia, E. Short-term effects of a modified Alt-RAMEC protocol for early treatment of Class III malocclusion: a controlled study. Orthod Craniofac Res. 2014, 17, 259–269. [Google Scholar] [CrossRef]
- Canturk, BH; Celikoglu, M. Comparison of the effects of face mask treatment started simultaneously and after the completion of the alternate rapid maxillary expansion and constriction procedure. Angle Orthod. 2015, 85, 284–291. [Google Scholar] [CrossRef]
- Kaya, D; Kocadereli, İ; Kan, B; Tasar, F. Effects of facemask treatment anchored with miniplates after alternate rapid maxillary expansions and constrictions: A pilot study. Angle Orthod. 2011, 81, 639–646. [Google Scholar] [CrossRef]
- Isci, D; Turk, T; Elekdag-Turk, S. Activation–deactivation rapid palatal expansion and reverse headgear in Class III cases. Eur J Orthod. 2010, 32, 706–715. [Google Scholar] [CrossRef]
- Sitaropoulou, V; Yılmaz, HN; Yılmaz, B; Küçükkeles, N. Three-dimensional evaluation of treatment results of the Alt-RAMEC and facemask protocol in growing patients. J Orofac Orthop. 2020, 81, 407–418. [Google Scholar] [CrossRef] [PubMed]
- Gökalp, H. Quantitative Evaluation of Consecutively Rapid Maxillary Expansions and Constrictions Effects on Circum-Maxillary Sutures in Boys by SPECT Bone Scintigraphy. EC Dental Science. 2020, 19, 48–59. [Google Scholar]
- Garib, DG; Henriques, JFC; Janson, G; de Freitas, MR; Fernandes, AY. Periodontal effects of rapid maxillary expansion with tooth-tissue-borne and tooth-borne expanders: a computed tomography evaluation. Am J Orthod Dentofacial Orthop. 2006, 129, 749–758. [Google Scholar] [CrossRef]
- Gandedkar, NH; Liou, EJW. The immediate effect of alternate rapid maxillary expansions and constrictions on the alveolus: a retrospective cone beam computed tomography study. Prog Orthod. 2018, 19, 40. [Google Scholar] [CrossRef]
- Broadbent, BH. A new x-ray technique and its application to orthodontia. Angle Orthod. 1931, 1, 45–66. [Google Scholar]
- Silness, J; Löe, H. Periodontal disease in pregnancy. 3. Response to local treatment. Acta Odontol Scand. 1966, 24, 747–759. [Google Scholar] [CrossRef] [PubMed]
- Liu, C; Song, R; Song, Y. Sutural expansion osteogenesis for management of the bony-tissue defect in cleft palate repair: experimental studies in dogs. Plast Reconstr Surg. 2000, 105, 2012–2025. [Google Scholar] [CrossRef]
- Wang, YC; Chang, PMS; Liou, EJW. Opening of circumaxillary sutures by alternate rapid maxillary expansions and constrictions. Angle Orthod. 2009, 79, 230–234. [Google Scholar] [CrossRef]
- Huang, CT; Wang, YC; Huang, CS; Liou, EJW. Maxillary displacement after rapid maxillary expansions: An animal study. J Taiwan Assoc Orthod. 2008, 20, 19–23. [Google Scholar]
- Greenbaum, KR; Zachrisson, BU. The effect of palatal expansion therapy on the periodontal supporting tissues. Am J Orthod. 1982, 81, 12–21. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
a. The 2-hinged expander before cementation, b. after cementation.

Figure 2.
Points, horizontal and vertical reference lines.
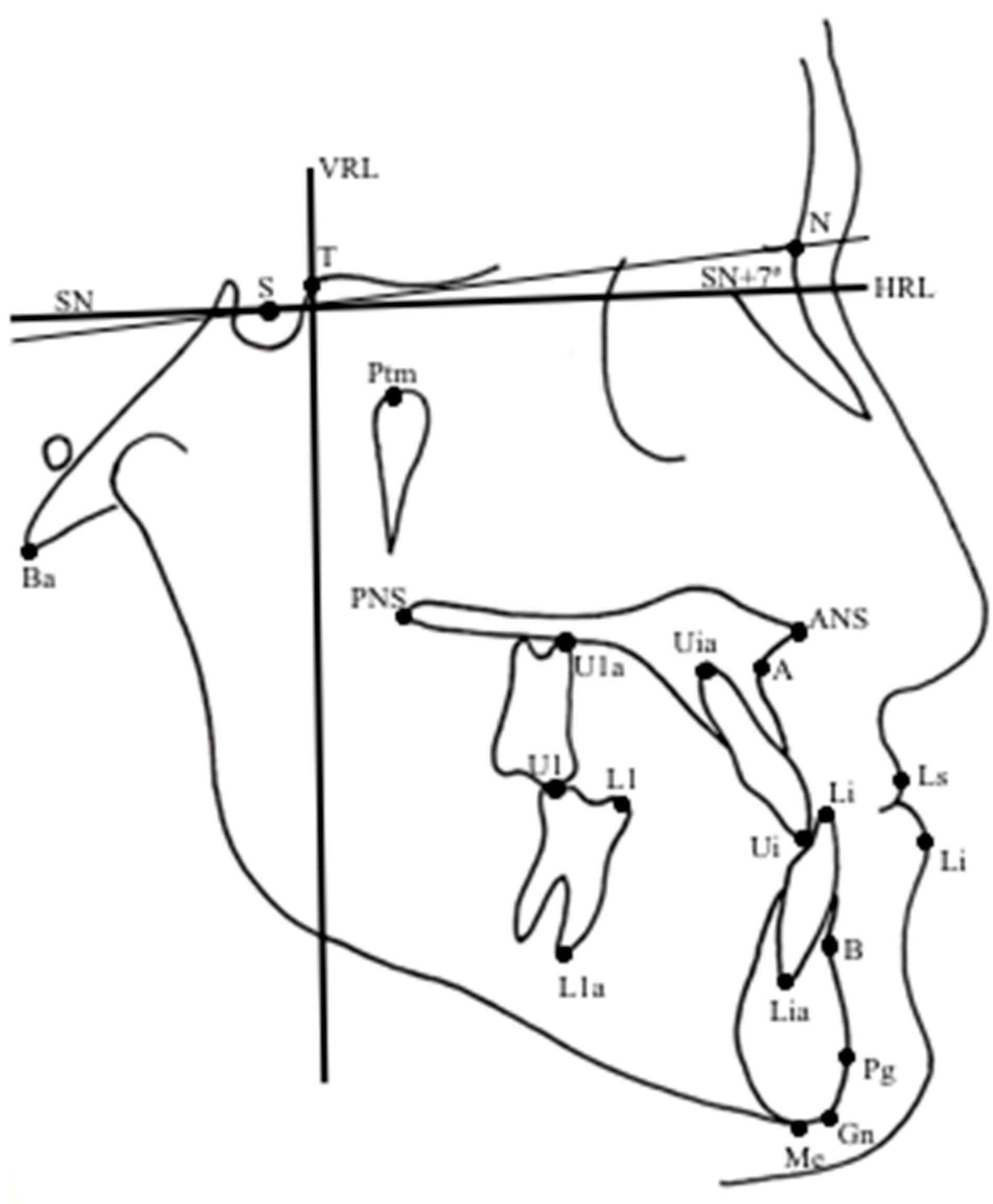
Figure 3.
Linear, angular skeletal measurements.
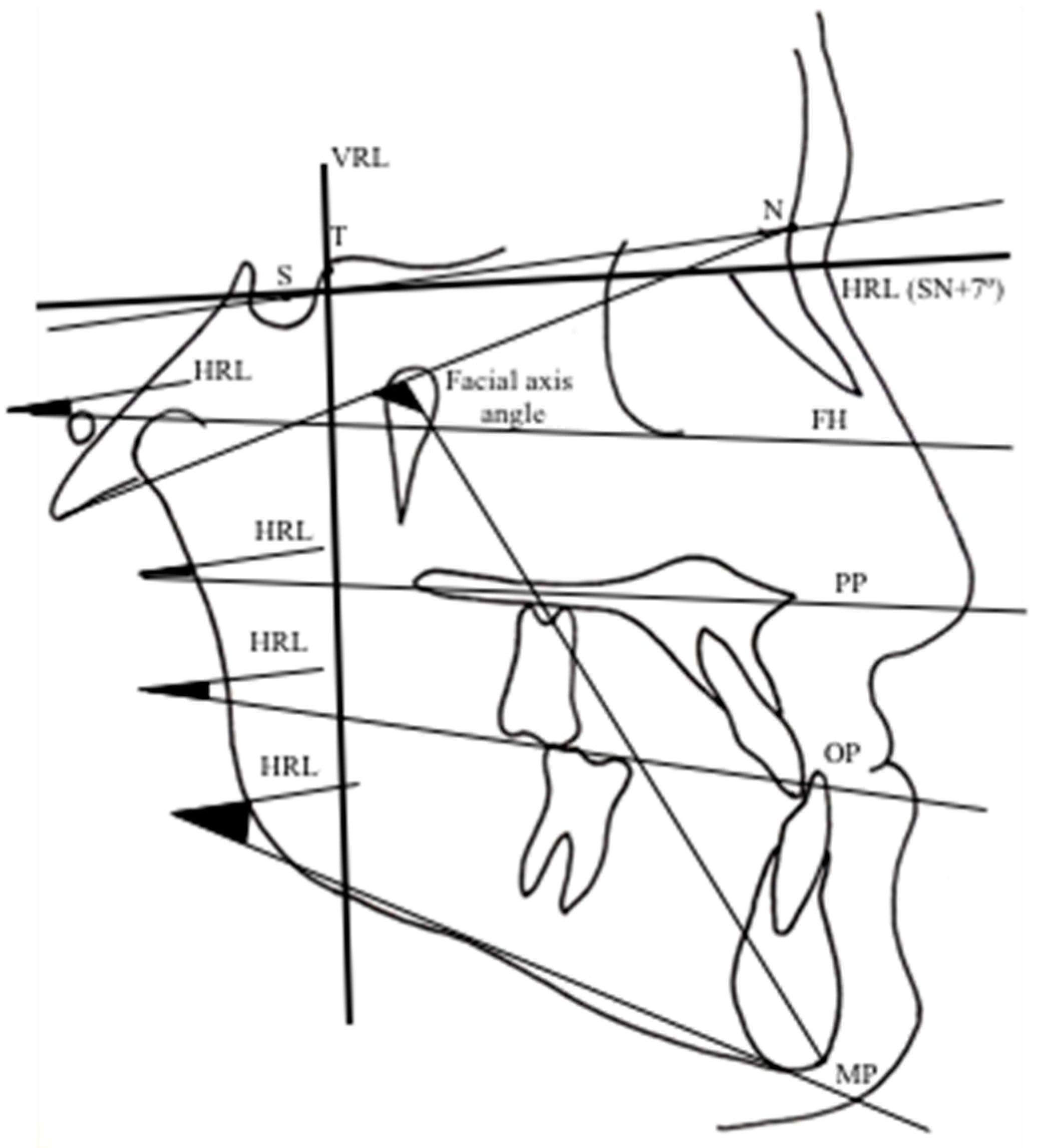
Figure 4.
Overjet, overbite and linear skeletal measurements.
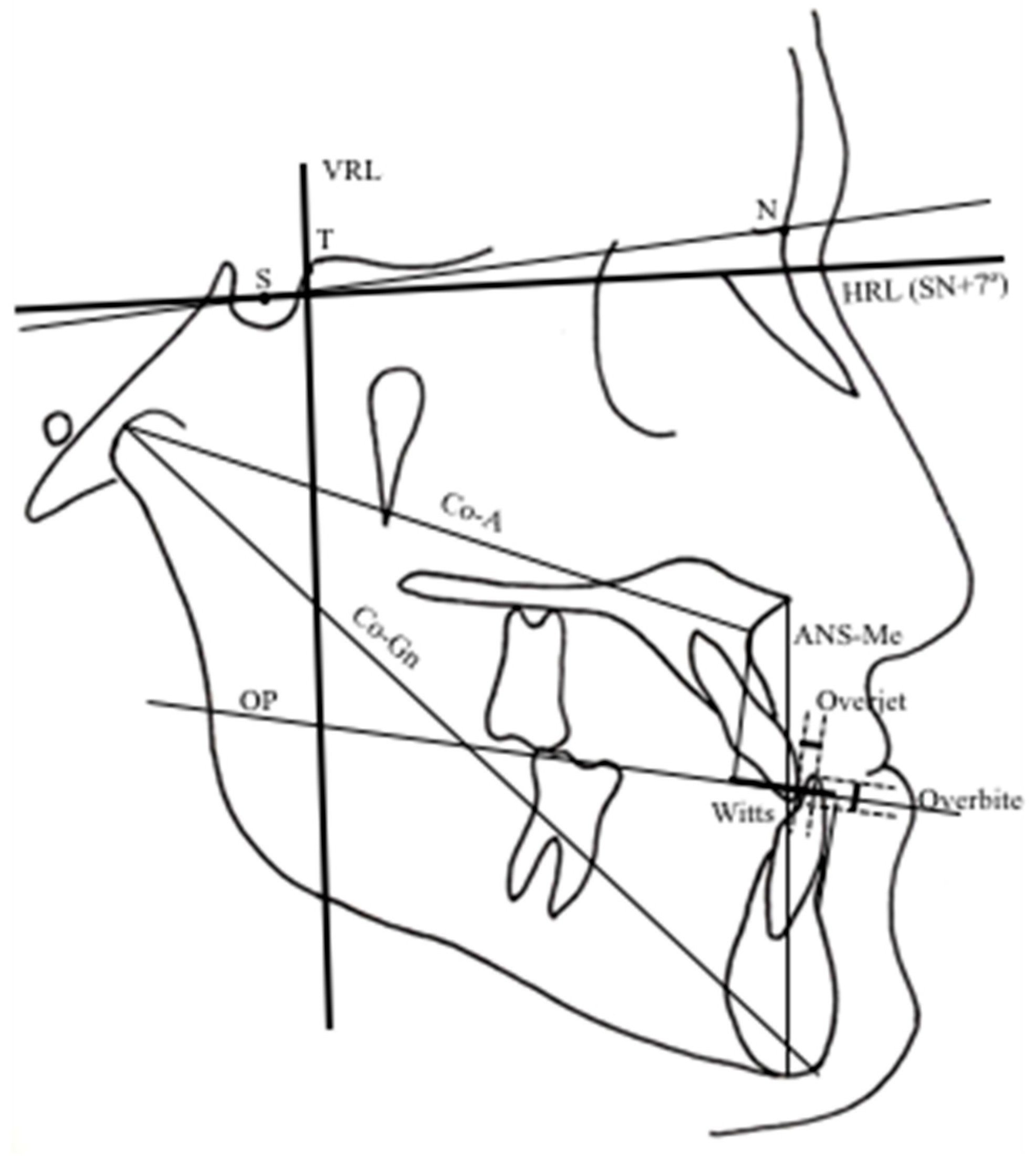
Figure 5.
Maxillary and mandibular skeletal linear measurements.
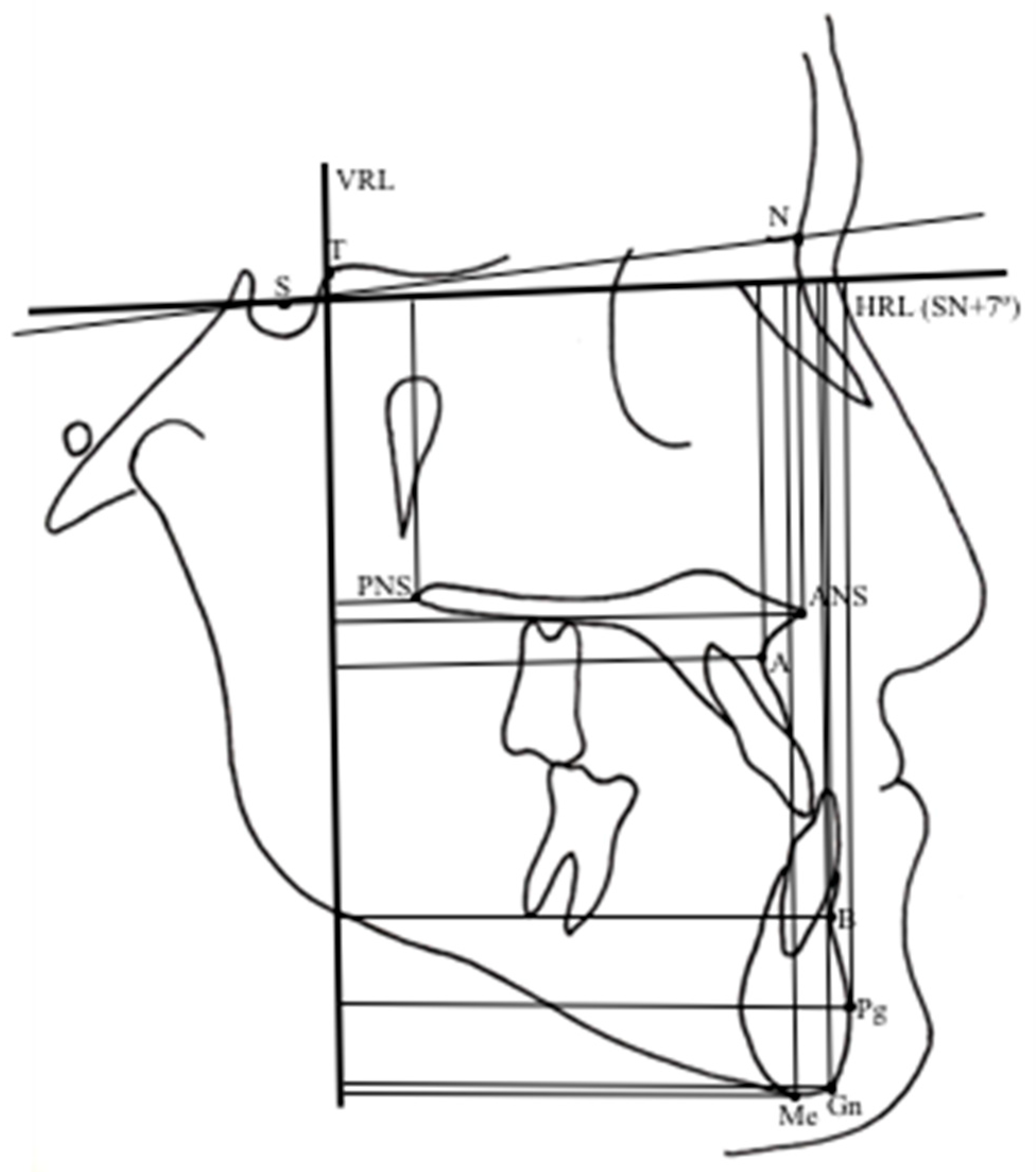
Figure 6.
Dental linear measurements.
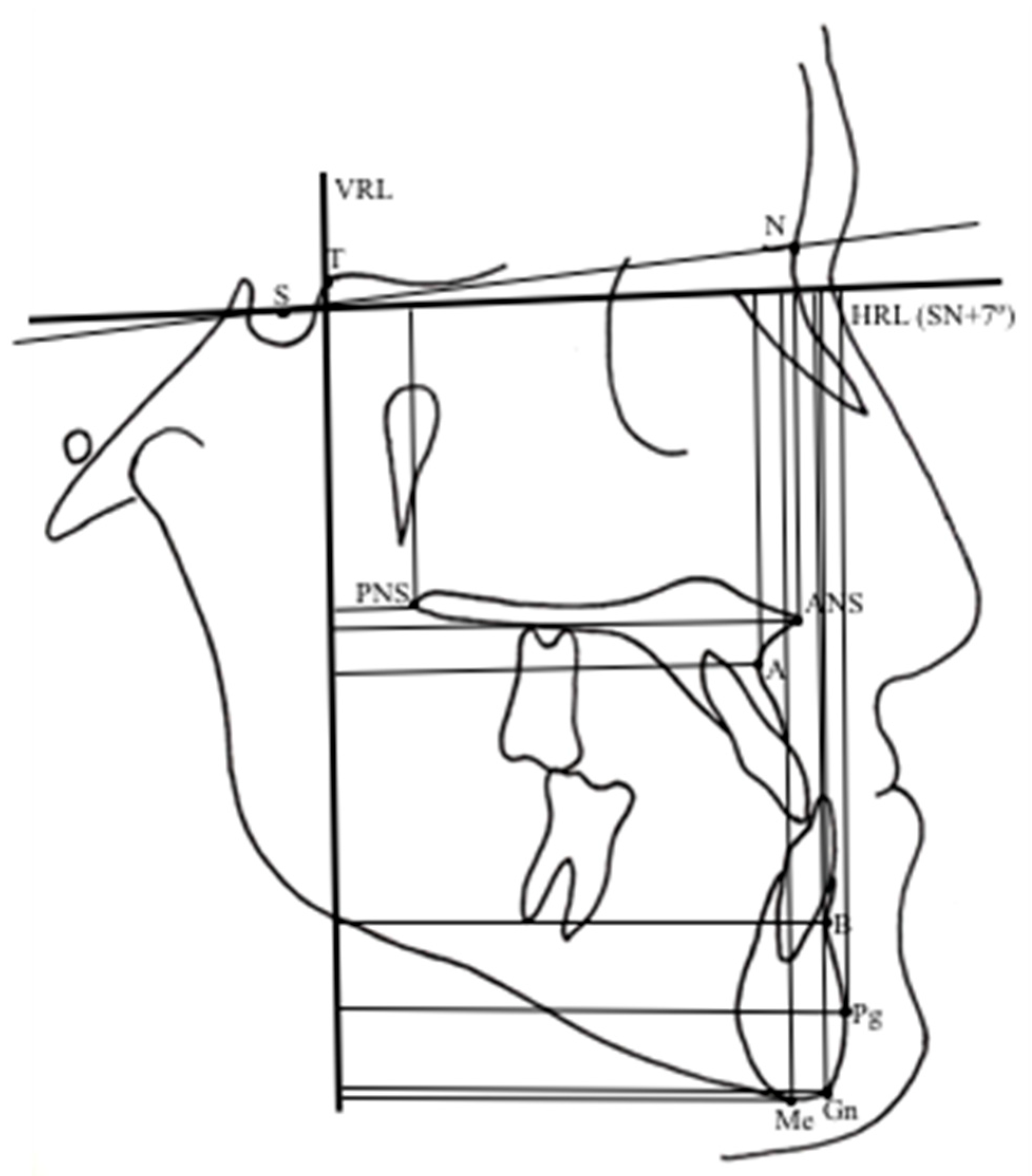
Figure 7.
Soft tissue profile linear measurements.
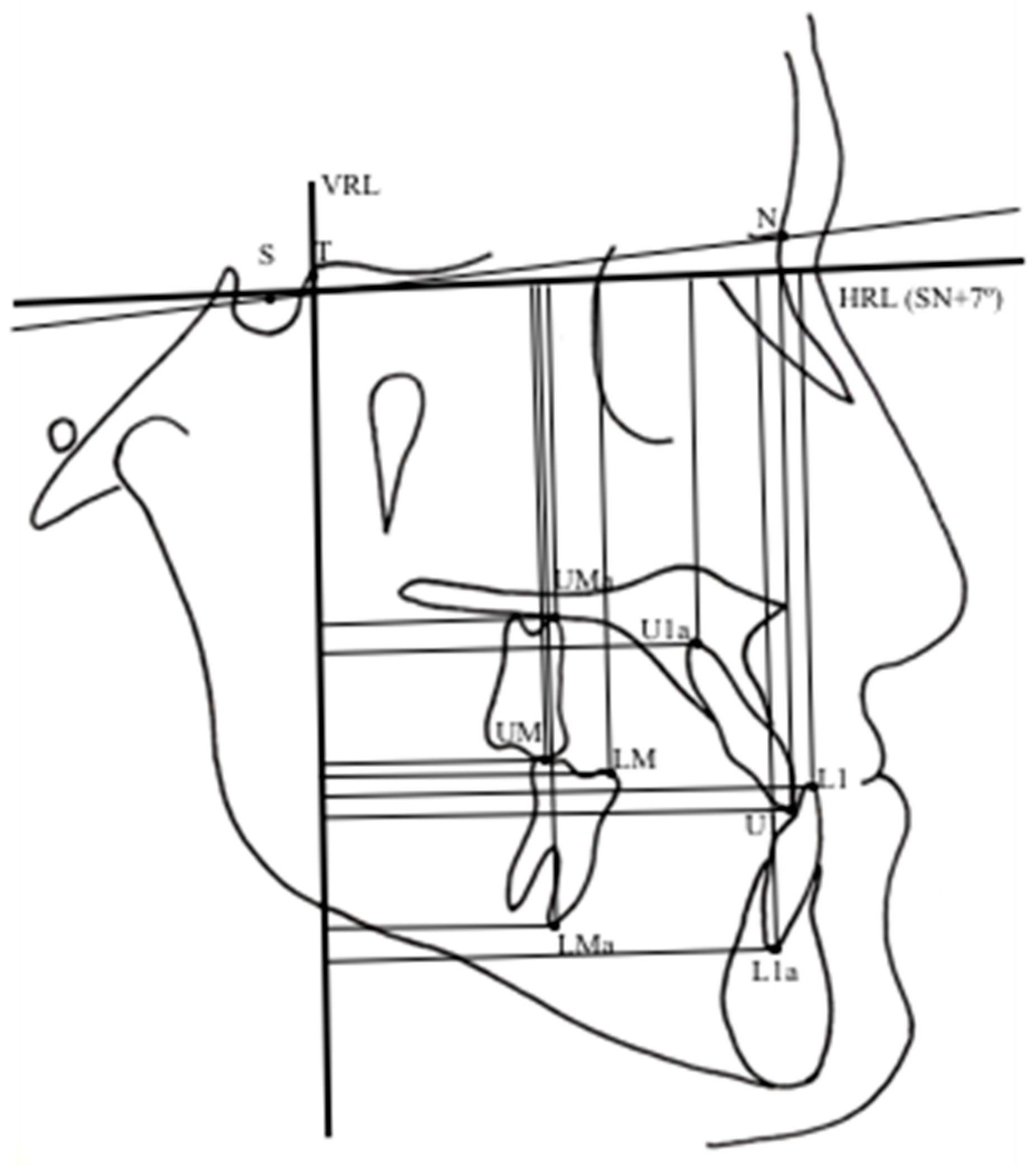
Figure 8.
Transvers upper dental cast measurements.
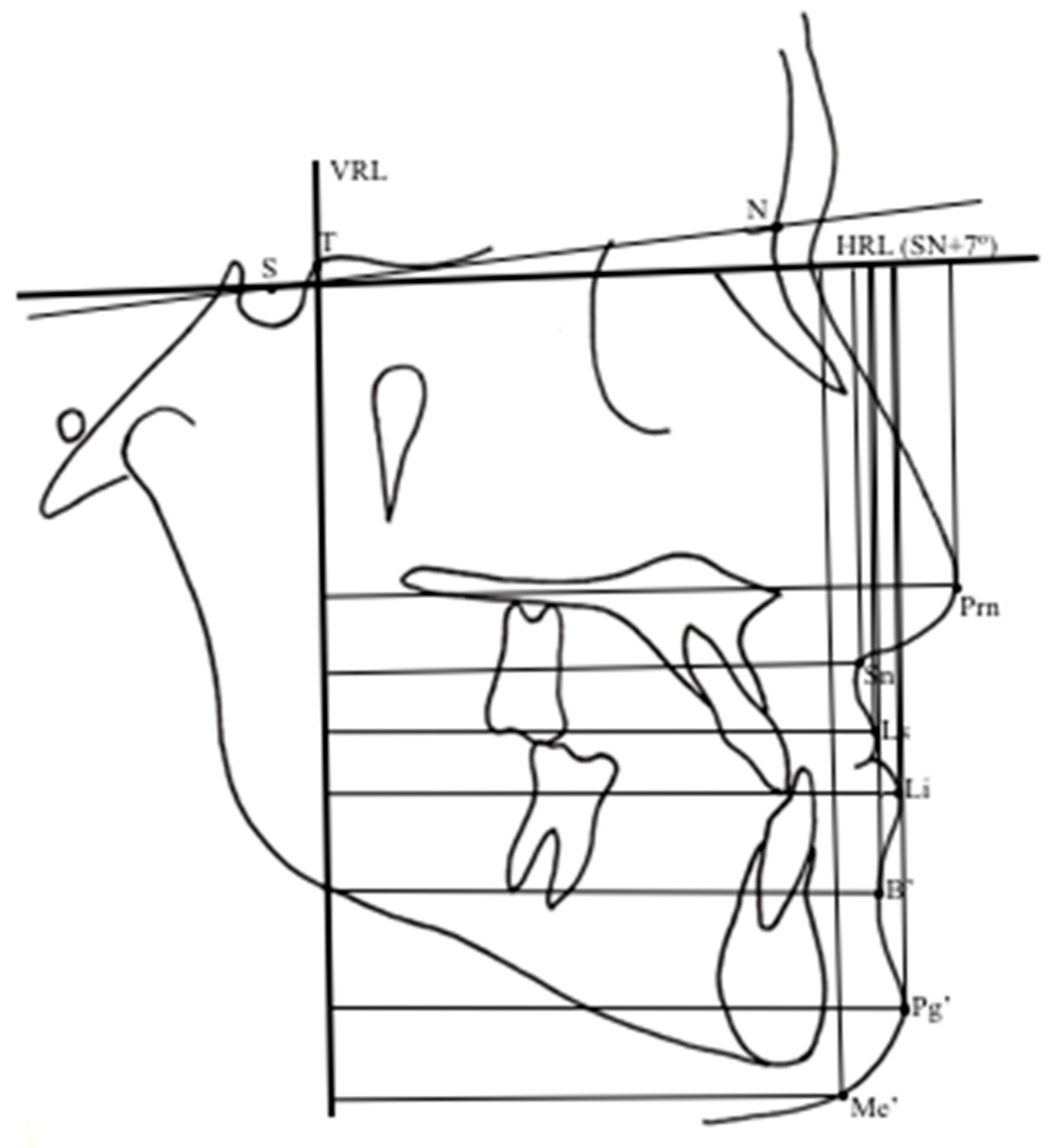

Table 1.
Growth periods according to cervical vertebra maturation method, mean age and sex distribution in the study groups at baseline.
Table 1.
Growth periods according to cervical vertebra maturation method, mean age and sex distribution in the study groups at baseline.
| n= 15 | Alt-RAMEC Group | Control Group | |||||
|---|---|---|---|---|---|---|---|
| Age (Year) | CVM* Stages | n= 7 | Age (Year) | CVM* Stages | |||
| Mean±SD | CVM II | CVM III | Mean±SD | CVM II | CVM III | ||
| Females 6 | 12.6±1.42 | 3 | 3 | Females 1 | 12.5±1.54 | 0 | 7 |
| Males 9 | 13.1±1,92 | 5 | 4 | Males 6 | 12.6±1.45 | 13 | 7 |
Abbreviation: *CVM; Cervical Vertebra Maturation.
Table 2.
Custom diary asked to report 2-hinged expander activations for each subject. .
| Screw opening- First week | Screw closing- Second week | |||||
| Morning | Evening | Morning | Evening | |||
| 1st | 2 turns | 2 turns | 8th day | 2 turns | 2 turns | |
| 2nd day | 9th day | |||||
| 3rd day | 10th day | |||||
| 4th day | 11th day | |||||
| 5th day | 12th day | |||||
| 6th day | 13th day | |||||
| 7th day | 14th day | |||||
| Screw opening- Third week | Screw closing- Fourth week | |||||
| Morning | Evening | Morning | Evening | |||
| 15 th day | 2 turns | 2 turns | 22 th day | 2 turns | 2 turns | |
| 16 th day | 23 th day | |||||
| 17th day | 24 th day | |||||
| 18 th day | 25 th day | |||||
| 19 th day | 26th day | |||||
| 20 th day | 27 th day | |||||
| 21 th day | 28 th day | |||||
| Screw opening- Fifth week | Screw closing- Sixth week | |||||
| Morning | Evening | Morning | Evening | |||
| 29th day | 2 turns | 2 turns | 36 th day | 2 turns | 2 turns | |
| 30 th day | 37 th day | |||||
| 31 th day | 38 th day | |||||
| 32 th day | 39 th day | |||||
| 33 th day | 40 th day | |||||
| 34 th day | 41 th day | |||||
| 35 th day | 42 th day | |||||
| Screw opening- Seventh week | Screw closing- Eigth week | |||||
| Morning | Evening | Morning | Evening | |||
| 43 th day | 2 turns | 2 turns | 50 th day | 2 turns | 2 turns | |
| 44 th day | 51 th day | |||||
| 45 th day | 52 th day | |||||
| 46 th day | 53 th day | |||||
| 47 th day | 54 th day | |||||
| 48 th day | 55 th day | |||||
| 49 th day | 56 th day | |||||
| Screw opening- Nineth week | ||||||
| Morning | Evening | |||||
| 2 turns | 2 turns | |||||
| 57th | ||||||
| 58 th | ||||||
| 59 th | ||||||
| 60 th | ||||||
| 61 th | ||||||
| 62 th | ||||||
| 63 th | ||||||
Table 3.
Comparison of study groups with the Mann Whitney U test at the beginning of the Alt-RAMEC.
| Measurements | Alt-RAMEC (T0) | Control (T0) | |||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | P | |
| Nperp-A, mm | -1.00 | 1.91 | -2.14 | 4.10 | Ns |
| Co-A, mm | 85.67 | 7.29 | 88.71 | 6.60 | Ns |
| B-VR, mm | 63.33 | 7.76 | 61.14 | 11.81 | Ns |
| Pog-Nperp, mm | 5.59 | 6.63 | 4.43 | 3.82 | Ns |
| Wits appraisal, mm | -0.67 | 3.09 | 0.57 | 1.40 | Ns |
| FH/MP, ° | 22.46 | 3.38 | 25.14 | 5.58 | Ns |
| NBa/Ptm-Gn, ° | 90.9 | 3.20 | 91.57 | 4.08 | Ns |
| Overjet, mm | -0.43 | 1.51 | 0.14 | 0.38 | ** |
| Overbite, mm | 2.93 | 1.44 | 0.14 | 0.38 | ** |
Significance level: *P <.05; **P<0.01; NS, not significant.
Table 4.
Comparisons of the changes on lateral cephalometric films by treatment/control periods between the 2 groups.
Table 4.
Comparisons of the changes on lateral cephalometric films by treatment/control periods between the 2 groups.
| Measurements | Alt-RAMEC (T0) | Alt-RAMEC (T1) |
Control (T0) |
Control (T1) |
Mann Whitney U Test P |
||||||
| Maxillary Skeletal | Mean | SD | Mean | SD | P | Mean | SD | Mean | SD | P | |
| Nperp-A, mm | -1.00 | 1.91 | -0.17 | 2.18 | * | -2.14 | 4.10 | -2.57 | 4.39 | Ns | ** |
| A-VRL , mm | 59.37 | 4.01 | 61.93 | 3.98 | ** | 62.71 | 6.32 | 61.14 | 8.12 | Ns | ** |
| A-HRL, mm | 45.57 | 5.60 | 46.70 | 5.93 | Ns | 49.86 | 3.18 | 50.79 | 4.18 | Ns | Ns |
| ANS-VRL, mm | 63.80 | 3.70 | 66.20 | 8.29 | ** | 69.00 | 5.86 | 67.57 | 8.54 | Ns | ** |
| ANS-HRL, mm | 40.97 | 5.45 | 42.97 | 5.38 | Ns | 43.71 | 4.19 | 47.71 | 3.82 | Ns | Ns |
| PNS-VRL, mm | 17.13 | 4.10 | 17.40 | 3.40 | Ns | 16.36 | 4.84 | 17.00 | 5.16 | Ns | Ns |
| PNS-HRL, mm | 40.23 | 4.07 | 41.80 | 4.32 | * | 40.93 | 7.66 | 41.93 | 7.37 | Ns | * |
| Co-A, mm | 85.67 | 7.29 | 88.70 | 5.37 | * | 88.71 | 6.60 | 90.21 | 4.98 | Ns | * |
| Maxillary Dental | |||||||||||
| Ui-Nperp, mm | 20.90 | 2.93 | 22.90 | 3.32 | * | 14.14 | 4.74 | 15.29 | 5.02 | Ns | Ns |
| Ui-APg, mm | 5.97 | 1.93 | 6.17 | 2.24 | Ns | 4.71 | 2.06 | 3.71 | 3.15 | Ns | Ns |
| Ui-VRL, mm | 63.00 | 5.89 | 64.30 | 4.69 | Ns | 65.79 | 6.87 | 66.71 | 10.81 | Ns | Ns |
| Ui-HRL, mm | 67.60 | 7.61 | 68.70 | 6.82 | Ns | 71.43 | 6.65 | 73.79 | 6.04 | Ns | Ns |
| Uia- VRL, mm | 54.70 | 4.12 | 54.90 | 3.27 | Ns | 59.00 | 10.83 | 58.93 | 9.10 | Ns | Ns |
| Uia- HRL, mm | 51.20 | 13.62 | 52.70 | 12.84 | Ns | 50.57 | 8.54 | 52.36 | 7.87 | Ns | Ns |
| U1- VRL, mm | 37.03 | 4.96 | 37.60 | 3.22 | Ns | 35.57 | 5.38 | 36.64 | 7.45 | Ns | Ns |
| U1- HRL, mm | 58.33 | 10.93 | 59.60 | 8.49 | Ns | 60.57 | 11.84 | 63.43 | 9.95 | Ns | * |
| U1a-VRL, mm | 36.10 | 3.31 | 37.20 | 3.25 | Ns | 35.86 | 5.34 | 37.79 | 6.15 | Ns | Ns |
| U1a-HRL, mm | 50.00 | 13.46 | 51.83 | 13.76 | Ns | 43.43 | 7.23 | 46.57 | 5.50 | * | Ns |
| Mandibular Skeletal | |||||||||||
| Nperp-Pg, mm | 5.59 | 6.63 | 2.57 | 5.95 | * | 4.43 | 3.82 | 8.00 | 4.86 | Ns | Ns |
| B-VRL, mm | 63.33 | 7.76 | 61.37 | 5.77 | Ns | 61.14 | 11.81 | 59.36 | 11.1 | Ns | Ns |
| B-HRL, mm | 83.63 | 9.32 | 86.27 | 7.60 | Ns | 86.07 | 11.03 | 87.86 | 6.39 | Ns | Ns |
| Pg-VRL, mm | 63.03 | 7.32 | 61.43 | 7.48 | Ns | 61.07 | 12.1 | 61.43 | 11.98 | Ns | Ns |
| Pg-HRL, mm | 98.33 | 10.85 | 100.60 | 9.27 | Ns | 99.00 | 17.11 | 102.300 | 7.81 | Ns | Ns |
| Go-VRL, mm | 7.30 | 4.31 | 7.37 | 6.21 | Ns | 4.71 | 4.39 | 5.57 | 4.86 | Ns | Ns |
| Go-HRL, mm | 73.33 | 5.79 | 74.07 | 5.91 | Ns | 99.00 | 17.11 | 102.00 | 7.81 | Ns | Ns |
| Co-VRL, mm | 9.53 | 3.38 | 9.40 | 3.38 | Ns | 11.86 | 4.38 | 15.43 | 6.95 | * | Ns |
| Co-HRL, mm | 21.80 | 2.98 | 22.33 | 2.89 | Ns | 81.86 | 11.55 | 78.57 | 4.43 | Ns | Ns |
| Co-Gn, mm | 125.22 | 9.94 | 126.03 | 10.01 | Ns | 116.57 | 8.79 | 114.64 | 6.71 | Ns | Ns |
| Mandibular Dental | |||||||||||
| Li-APg, mm | 5.47 | 2.30 | 4.87 | 2.20 | * | 3.00 | 1.41 | 3.57 | 1.90 | Ns | Ns |
| Li-VRL, mm | 64.93 | 4.76 | 65.400 | 5.11 | Ns | 63.93 | 10.58 | 65.36 | 11.21 | Ns | Ns |
| Li-HRL, mm | 66.33 | 6.97 | 68.20 | 6.30 | Ns | 71.57 | 7.11 | 73.00 | 6.24 | Ns | Ns |
| Lia-VRL, mm | 55.73 | 7.59 | 56.73 | 7.03 | Ns | 46.00 | 17.35 | 53.00 | 13.89 | Ns | Ns |
| Lia-HRL, mm | 86.73 | 7.38 | 88.67 | 6.76 | Ns | 92.00 | 8.08 | 93.57 | 8.16 | Ns | Ns |
| L1-VRL, mm | 39.80 | 7.36 | 40.93 | 4.03 | Ns | 43.36 | 13.48 | 37.29 | 7.50 | Ns | Ns |
| L1-HRL, mm | 68.73 | 10.83 | 68.20 | 8.95 | Ns | 68.57 | 7.30 | 69.86 | 4.88 | Ns | Ns |
| L1a-VRL, mm | 35.47 | 12.92 | 33.40 | 4.88 | Ns | 31.71 | 8.40 | 32.43 | 11.31 | Ns | Ns |
| L1a-HRL, mm | 83.20 | 8.80 | 85.20 | 7.66 | Ns | 86.00 | 7.75 | 87.43 | 5.13 | Ns | Ns |
| Interdental | |||||||||||
| Overjet, mm | -2.57 | 0.86 | -0.43 | 1.51 | ** | 0.14 | 0.38 | 0.29 | 0.76 | Ns | ** |
| Overbite, mm | 2.93 | 1.44 | 1.63 | 1.06 | * | 0.14 | 0.38 | 1.36 | 1.18 | Ns | * |
| Maxillo-Mandibular | |||||||||||
| Wits, mm | -3.13 | 2.88 | -0.67 | 3.09 | * | 0.29 | 0.76 | 0.57 | 1.40 | Ns | * |
| Vertical | |||||||||||
| PP/HRL, ° | 3.80 | 2.46 | 3.87 | 1.96 | Ns | 8.14 | 6.20 | 7.71 | 3.59 | Ns | Ns |
| OP/HRL, ° | 9.53 | 3.38 | 10.60 | 4.7 | Ns | 22.71 | 9.45 | 24.14 | 7.36 | * | Ns |
| MP/HRL, ° | 23.87 | 6.2 | 25.20 | 5.53 | Ns | 22.71 | 9.45 | 24.14 | 7.36 | Ns | Ns |
| FH/MP, ° | 21.80 | 2.98 | 24.70 | 3.26 | ** | 25.14 | 5.58 | 25.57 | 5.38 | Ns | Ns |
| NBa/Ptm-Gn, ° | 88.33 | 3.56 | 87.00 | 3.51 | * | 91.57 | 4.08 | 90.57 | 4.79 | Ns | * |
| ANS-Me, mm | 65.28 | 6.07 | 68.12 | 5.28 | ** | 68.14 | 4.30 | 68.43 | 2.82 | Ns | ** |
| Soft tissue Profile | |||||||||||
| Prn-VRL, mm | 89.07 | 5.51 | 90.80 | 5.97 | * | 95.00 | 3.32 | 96.57 | 6.24 | Ns | * |
| Prn-HRL, mm | 35.73 | 7.46 | 35.47 | 5.79 | Ns | 45.86 | 4.46 | 46.57 | 4.46 | Ns | Ns |
| Sn-VRL, mm | 74.73 | 4.46 | 76.33 | 4.48 | Ns | 81.43 | 5.06 | 80.43 | 6.58 | Ns | * |
| Sn-HRL, mm | 46.93 | 7.04 | 46.80 | 6.18 | Ns | 54.00 | 1 2.85 | 56.43 | 13.67 | * | Ns |
| Ls-E line, mm | -6.93 | 2.89 | -5.60 | 2.75 | * | -3.50 | 3.14 | -3.93 | 5.47 | Ns | * |
| Ls-VRL, mm | 76.87 | 5.13 | 78.50 | 5.10 | Ns | 78.79 | 6.95 | 76.64 | 10.17 | Ns | * |
| Ls-HRL, mm | 57.73 | 6.70 | 59.07 | 6.27 | Ns | 64.14 | 9.53 | 63.29 | 5.91 | Ns | Ns |
| Li-E, mm | -0.33 | 3.81 | -1.13 | 3.18 | Ns | -0.57 | 4.65 | 0.71 | 3.9 | Ns | Ns |
| Li-VRL, mm | 77.40 | 5.90 | 77.00 | 8.49 | Ns | 75.71 | 12.808 | 80.00 | 9.95 | * | Ns |
| Li-HRL, mm | 73.73 | 7.46 | 75.47 | 7.04 | Ns | 78.29 | 9.89 | 84.00 | 7.57 | * | Ns |
| B’-VRL, mm | 73.47 | 11.78 | 73.67 | 7.02 | Ns | 73.86 | 10.96 | 77.43 | 8.87 | * | Ns |
| B’-HRL, mm | 83.13 | 8.16 | 85.93 | 7.69 | Ns | 84.71 | 12.85 | 86.57 | 13.15 | Ns | Ns |
| Pg’-VRL, mm | 75.07 | 11.07 | 72.53 | 8.58 | Ns | 66.43 | 16.62 | 67.29 | 11.61 | Ns | Ns |
| Pg’-HRL, mm | 96.53 | 8.27 | 98.07 | 8.19 | Ns | 102.43 | 5.68 | 101.71 | 9.39 | Ns | Ns |
| Me’-VRL, mm | 55.60 | 6.87 | 54.93 | 8.49 | Ns | 49.79 | 9.49 | 52.07 | 10.21 | Ns | Ns |
| Me’-HRL, mm | 109.33 | 13.56 | 113.07 | 11.26 | Ns | 109.71 | 6.87 | 111.86 | 7.47 | Ns | Ns |
| Naso-labial angle | 102.87 | 14.34 | 103.27 | 13.04 | Ns | 113.57 | 16.37 | 114.57 | 15.16 | Ns | Ns |
| Mento-labial angle | 136.73 | 11.91 | 142.33 | 9.95 | Ns | 125.86 | 24.51 | 127.71 | 16.35 | Ns | Ns |
Significance level: *P <0.05; **P <0.01; NS, not significant.
Table 5.
Inter-canine, inter-first premolar and inter-first molar distance measurements on upper orthodontic cast before (T0) and immediately after Alt-RAMEC (T1).
Table 5.
Inter-canine, inter-first premolar and inter-first molar distance measurements on upper orthodontic cast before (T0) and immediately after Alt-RAMEC (T1).
| Measurements | Alt-RAMEC (T0) | Alt-RAMEC (T1) |
P | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| Intercanine distance, mm | 34.77 | 3.16 | 37.83 | 2.60 | ** |
| First inter first premolar distance, mm | 31.19 | 2.69 | 36.52 | 2.43 | ** |
| Intermolar distance, mm | 39.98 | 3.71 | 40.85 | 3.66 | * |
| Upper arch lenght, mm | 37.54 | 4.28 | 38.86 | 4.14 | * |
Significance level: *P <0.05; **P <0.01; NS, not significant.
Table 6.
Changes of soft-tissue periodontium of the upper incisors, first premolars and first molars before (T0) and immediately after (T1) Alt-RAMEC.
Table 6.
Changes of soft-tissue periodontium of the upper incisors, first premolars and first molars before (T0) and immediately after (T1) Alt-RAMEC.
| Incisors (T0) |
Incisors (T1) |
P | Premolars (T0) |
Premolars (T1) |
P | Molars (T0) |
Molars (T1) |
P | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | ||||
| PI | 0.61 | 0.47 | 0.73 | 0.32 | NS | 0.71 | 0.47 | 0.83 | 0.32 | NS | 0.81 | 0.47 | 0.83 | 0.32 | NS |
| GI | 0.54 | 0.12 | 0.78 | 0.31 | * | 0.63 | 0.12 | 0.77 | 0.31 | * | 0.78 | 0.12 | 0.87 | 0.31 | * |
| PPD | 1.18 | 0.22 | 1.33 | 0.28 | * | 1.17 | 0.22 | 1.55 | 0.28 | * | 1.23 | 0.22 | 1.37 | 0.28 | * |
| BI | 1.00 | 1.01 | 1.00 | 1.00 | ** | 1.00 | 1.00 | 1.00 | 1.00 | ** | 1.00 | 1.00 | 1.00 | 1.00 | ** |
| KGT | 7.80 | 1.52 | 8.13 | 1.19 | NS | 6.07 | 1.67 | 7.13 | 1.46 | NS | 6.13 | 1.42 | 7.13 | 1.25 | NS |
Significance level: *P<0.05; **P <0.01; NS, not significant. Abbreviations: PI-Plaque Index, GI-Gingival Index, BI-Bleeding Index, PPD-Periodontal Pocket Dept, KGT- Keratinized Gingival Tissue measurement.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



