
Submitted:
19 December 2025
Posted:
22 December 2025
You are already at the latest version
Abstract
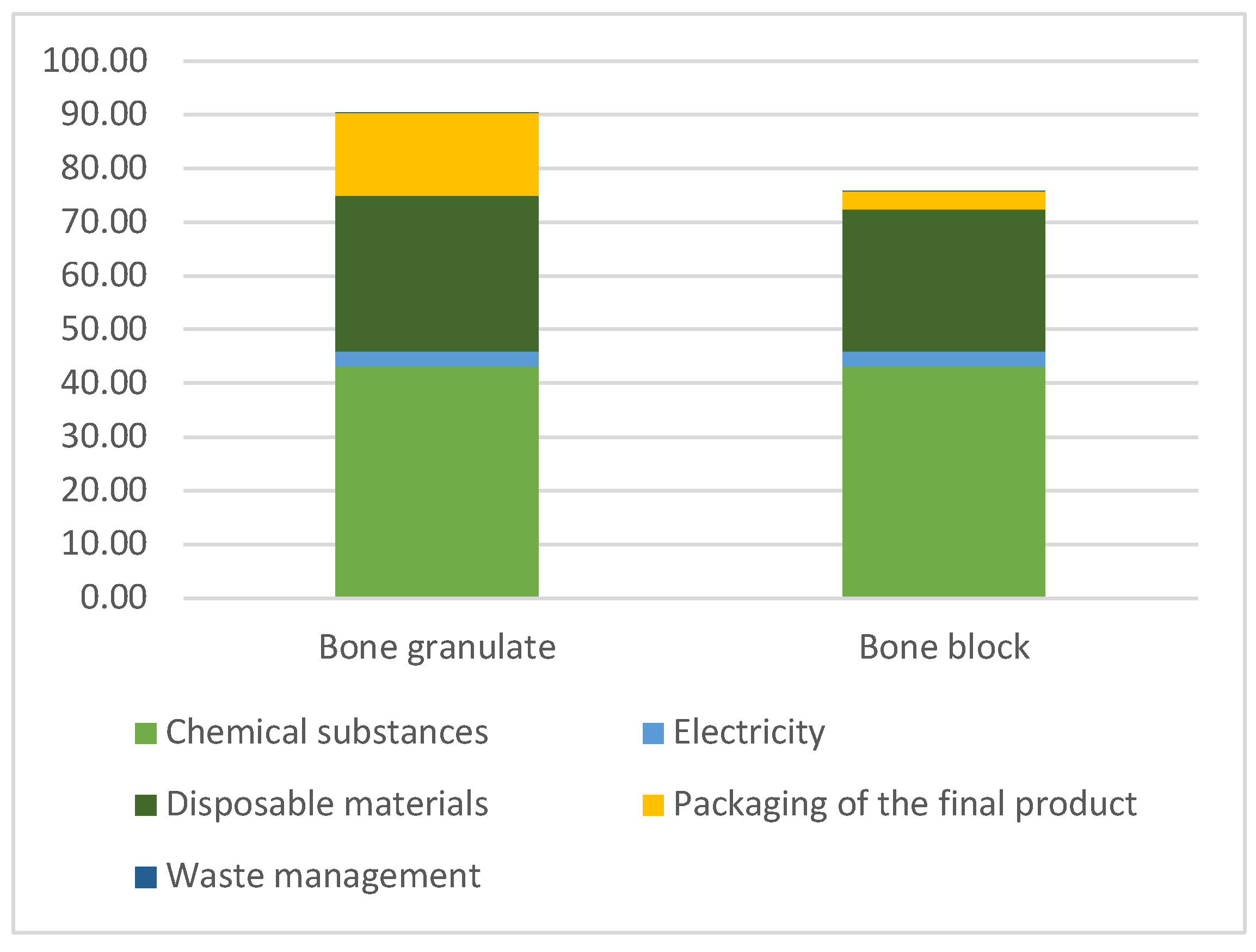
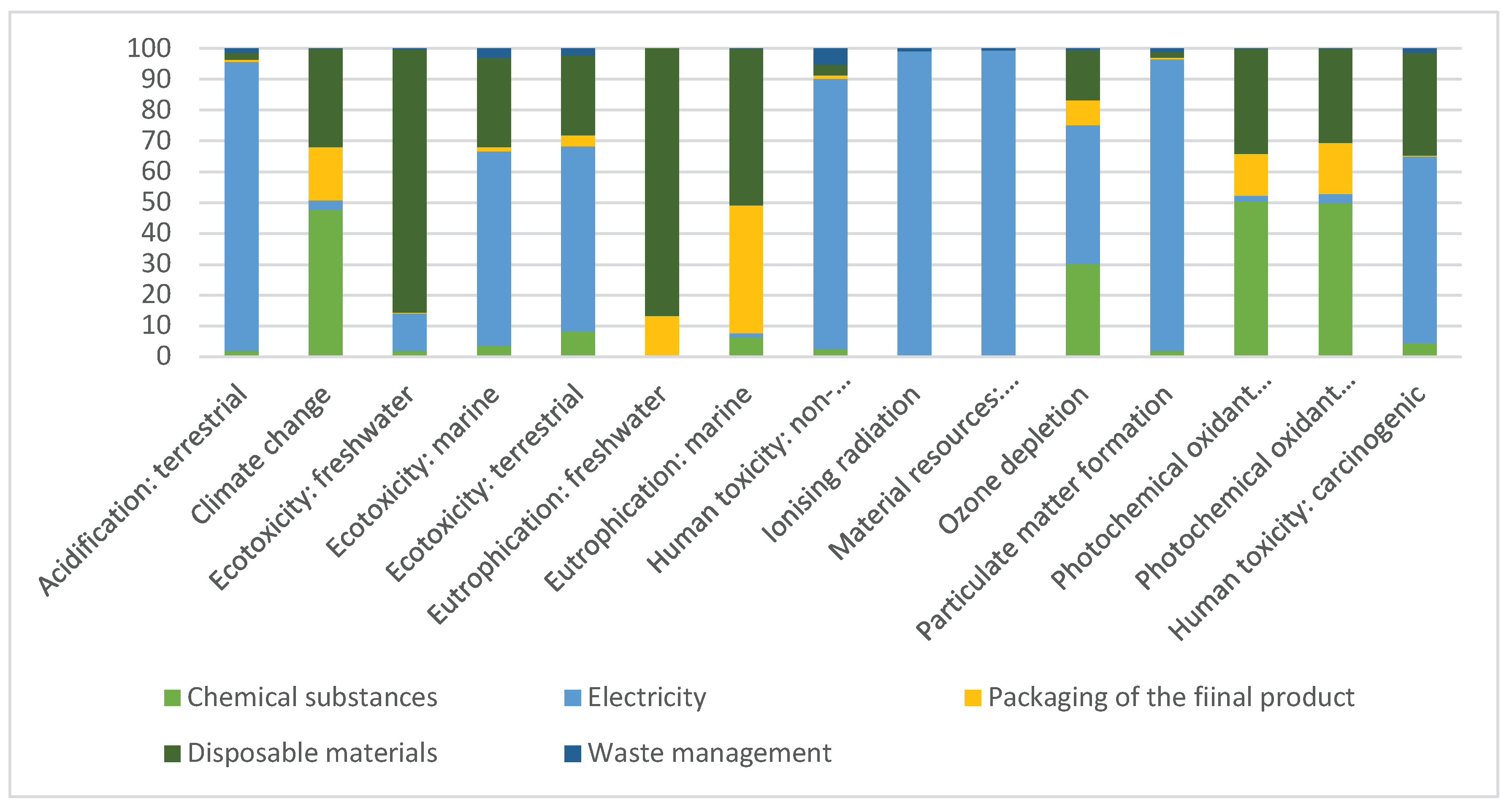
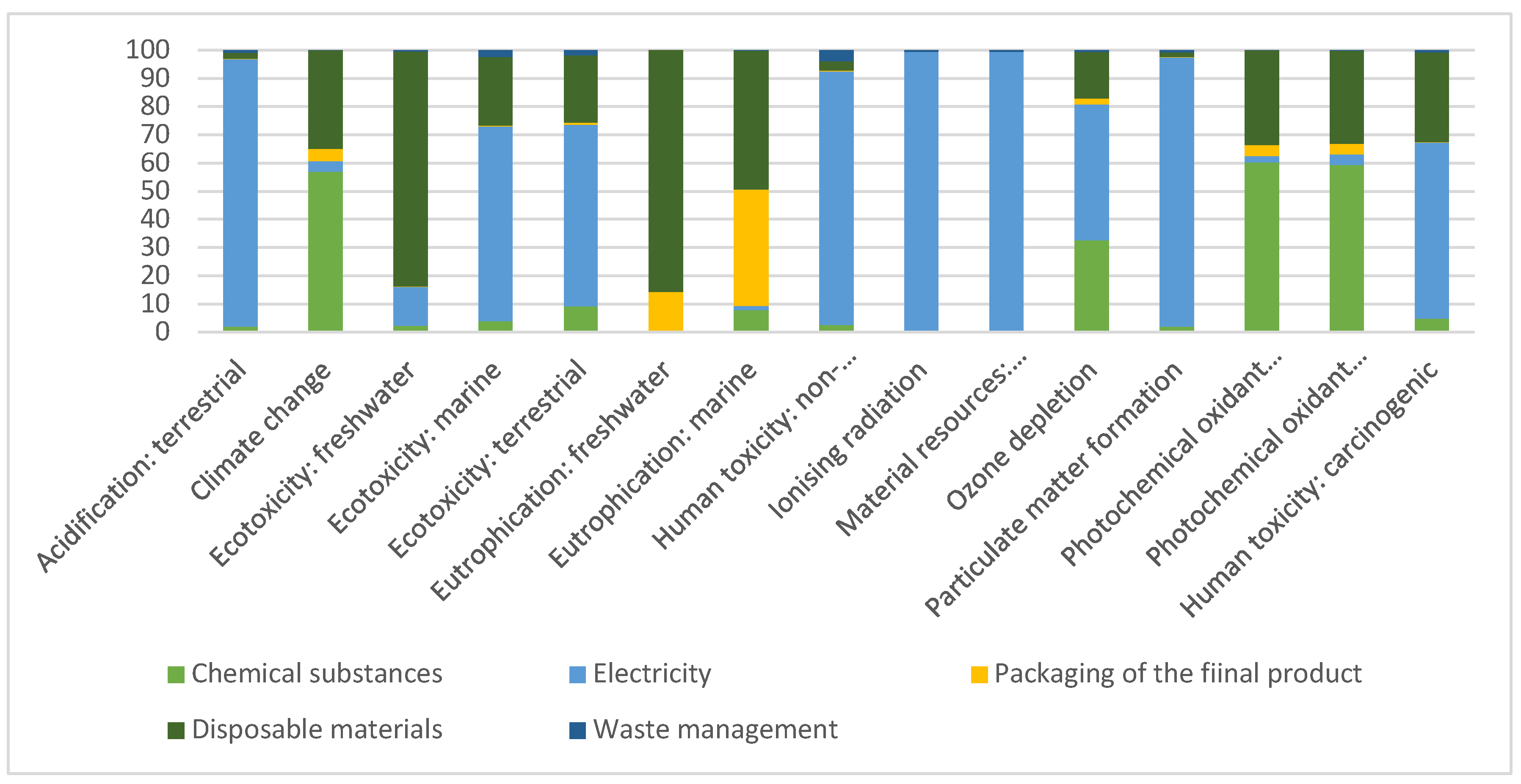
Background/Objectives: Bone grafting is fundamental in oral implantology in order to achieve appropriate aesthetic and functional results. One of the options for bone grafting is the use of allografts, which can be produced using femoral heads removed during orthopedic surgeries in accordance with the principles of the circular economy. The aim of this study was to examine the environmental impacts of the production of cancellous block and granulates bone graft materials produced in this way. Methods: The cradle-to-gate life cycle assessment was performed at the Petz Aladár University Teaching Hospital Tissue Bank Department, Győr, Hungary, with the system boundaries defined and the bone graft material produced during a production process defined as a functional unit. The environmental impacts were determined with the OpenLCA software, using the ReCiPe v1.03 2016 midpoint (H) and endpoint (H) assessment methods. Results: During the production process, 500g of bone graft material is produced in both forms, packaged as 1g. The carbon footprint of the production of the cancellous bone block was 75.754 kgCO2-Eq, while that of the bone granulates was 90.363 kgCO2-Eq, to which the chemicals used for degreasing and deantigenization of the bone tissue contributed the most. Within the impact categories, the material resource of metals-minerals, terrestrial ecotoxicity and climate change contributed the most to the environmental impacts. Within most impact categories, electricity was the most significant influencing factor. Conclusions: The environmental impact of the production of bone substitute granulates is greater than that of the bone block, to which the packaging of the products contributes primarily.
Keywords:
1. Introduction
2. Materials and Methods
2.1. Objective and Scope
Goal, Scope
Functional Unit
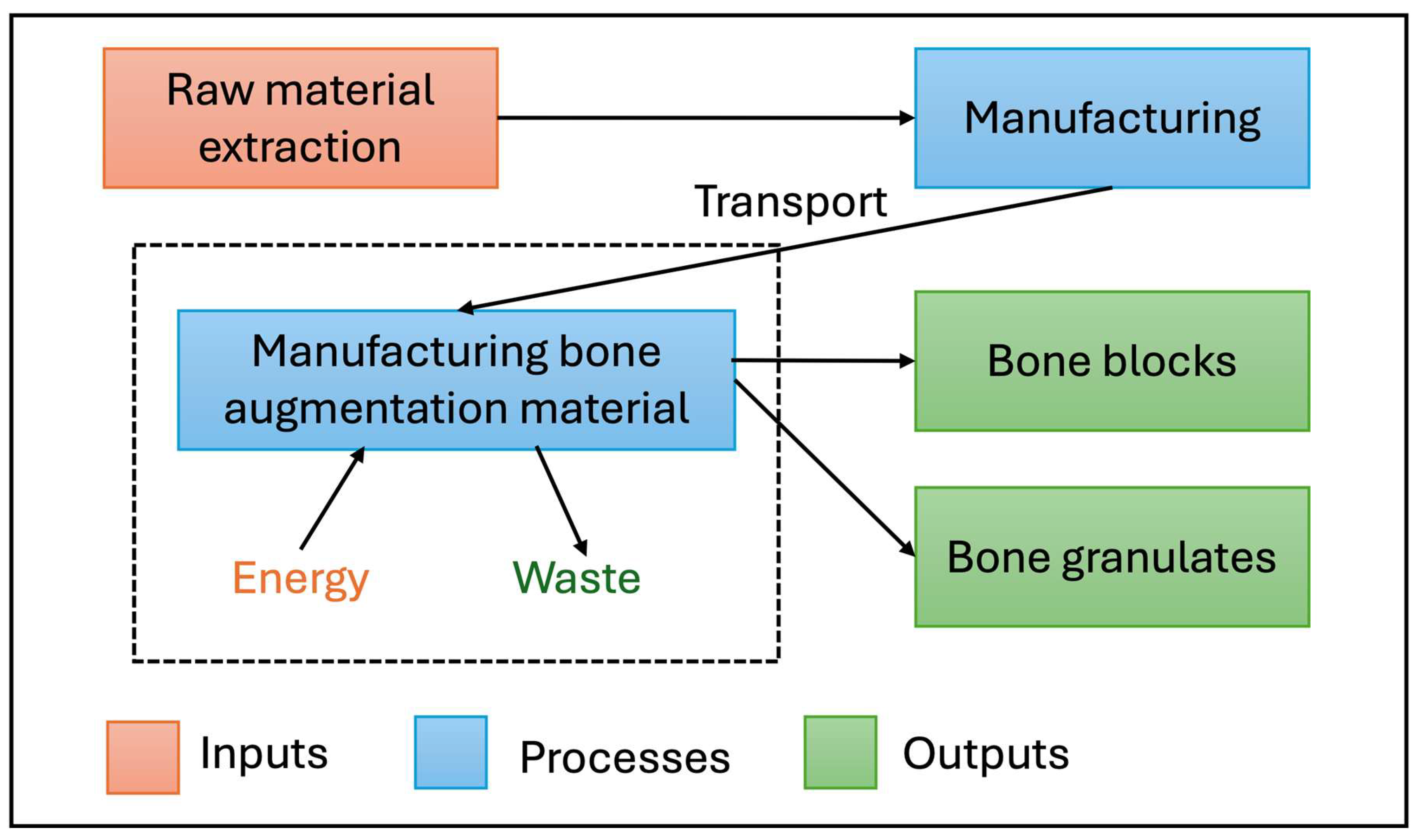
System Boundaries
2.2. Analysis of the Life Cycle Inventory
Data Collection
List of Assumptions
- During a processing cycle, an average of 24 femoral heads are processed, with a total weight of approximately 2720 g.
- Each work process is performed by one person wearing full protective equipment, including a sterile surgical gown, surgical mask, hair net and foot bag.
- Allografts are manipulated under sterile conditions in sterile fields.
- Bone waste generated during bone cutting and grinding cannot be reused due to metallic contamination and is therefore disposed of as infectious waste.
- The femoral heads received after surgeries are stored in a freezer for an average of 21 days until the 24 pieces are collected to start the processing process.
- The degreasing process takes an average of 28 days, during which the solution is changed initially every two days and then every three days; 2 liters of methanol-chloroform solution is used at one time.
- Deantigenization lasts two days, during which the container containing the allografts is placed in a thermostat, and the process is carried out with 2 liters of sodium azide-iodoacetic acid solution.
- Bleaching lasts one day, for which 2 liters of hydrogen peroxide solution is used.
- During the transitions between the different chemical solutions, the bones are rinsed with distilled water.
- In the case of bone granules, the different size fractions are separated by sieving and then packaged according to size categories.
- The instruments used during production was not part of the system boundaries because it was few and are re-sterilized several times for different production processes, so their environmental impact is not significant.
- To ensure the sterility of the allografts, the entire batch is first sterilized in an ethylene oxide sterilizer, then lyophilization and individual packaging are carried out in a separate, sterile room under sterile conditions.
- The lyophilization process takes one day.
- The packaging materials used for the final packaging of the allografts are sterilized in an autoclave, ensuring sterility for all the completed allografts at the same time.
- An average of 500 units of 1 g bone substitute preparation can be produced as a result of one processing cycle.
Life Cycle Inventory
2.3. Assessing the Life Cycle Impact
3. Results
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| LCA | Life Cycle Assessment |
| ISO | International Organization for Standardization |
| CO2 | carbon dioxide |
| LCI | Life Cycle Inventory |
| LCIA | Life Cycle Impact Assessment |
| HIV | Human Immunodeficiency Virus |
| AIDS | Acquired immunodeficiency syndrome |
| HBsAg | Hepatitis B surface Antigen |
| HBcoreAg | Hepatitis B core Antigen |
| HCV | Hepatitis C Virus |
| GHG | greenhouse gases |
References
- Dziuba R, Kucharska M, Madej-Kiełbik L, Sulak K, Wiśniewska-Wrona M. Biopolymers and Biomaterials for Special Applications within the Context of the Circular Economy. Materials (Basel). 2021 Dec 13;14(24):7704. [CrossRef] [PubMed] [PubMed Central]
- Abed R, Ashley P, Duane B, Crotty J, Lyne A. An environmental impact study of inter-dental cleaning aids. J Clin Periodontol. 2023 Jan;50(1):2-10. Epub 2022 Oct 6. [CrossRef] [PubMed] [PubMed Central]
- Almutairi W, Saget S, Mc Donnell J, Tarnowski A, Johnstone M, Duane B. The planetary health effects of COVID-19 in dental care: a life cycle assessment approach. Br Dent J. 2022 Aug;233(4):309-316. Epub 2022 Aug 26. [CrossRef] [PubMed] [PubMed Central]
- Suresh P, Crotty J, Tesanovic S, Alaweed O, Doyle S, Kiandee M, Hayes E, Umeh V, Khalilinejad B, Duane B. A life cycle analysis of the environmental impact of procurement, waste and water in the dental practice. Br Dent J. 2024 Apr;236(7):545-551. Epub 2024 Apr 12. 7. [CrossRef] [PubMed] [PubMed Central]
- Borglin L, Pekarski S, Saget S, Duane B. The life cycle analysis of a dental examination: Quantifying the environmental burden of an examination in a hypothetical dental practice. Community Dent Oral Epidemiol. 2021 Dec;49(6):581-593. Epub 2021 Mar 8. Erratum in: Community Dent Oral Epidemiol. 2024 Aug;52(4):613-617. doi: 10.1111/cdoe.12952. 10.1111/cdoe.12630.
- Ferawati U, Nuraini N,Fitria A Analysis of Medical Waste Management at UPTD Datu Beru Takengon Hospital. PROMOTOR. 2025 8. 586-591. [CrossRef]
- Attrah, M.; Elmanadely, A.; Akter, D.; Rene, E.R. A Review on Medical Waste Management: Treatment, Recycling, and Disposal Options. Environments 2022, 9, 146. [CrossRef]
- Pollice B, Thiel CL, Baratz ME. Life Cycle Assessment in Orthopedics. Oper Tech Orthop. 2022 Dec;32(4):100998. Epub 2022 Sep 22. [CrossRef] [PubMed] [PubMed Central]
- Kheirabadi S, Sheikhi A. Recent advances and challenges in recycling and reusing biomedical materials. Curr Opin Green Sustain Chem. 2022 Dec;38:100695. Epub 2022 Sep 6. [CrossRef] [PubMed] [PubMed Central]
- Gallego L, Harvey K, Pevida M, García-Consuegra L, García-Suárez O, Meana Á, Alvarez-Viejo M, Junquera L. From Waste to Innovation: A Circular Economy Approach for Tissue Engineering by Transforming Human Bone Waste into Novel Collagen Membranes. Biomolecules. 2025 Jan 15;15(1):132. 1, 132. [CrossRef] [PubMed] [PubMed Central]
- Kumar V, KhanV, Gaurav G. Environmental And Healthcare Issues Of Medical Waste. International Journal of Environmental Sciences. 2025 11. 1093-1101. [CrossRef]
- Smith L, Ali M, Agrissais M, Mulligan S, Koh L, Martin N. A comparative life cycle assessment of dental restorative materials. Dent Mater. 2023 Jan;39(1):13-24. Epub 2022 Nov 23. Jan. [CrossRef] [PubMed]
- Prinz RAD, da Rocha LR, Eirado TP, da Silva Pinto J, Guimarães JAM, Fogagnolo F, Dias RB. Biological parameters for quality evaluation of allografts from the Brazilian National Institute of Traumatology and Orthopedics tissue bank. Cell Tissue Bank. 2024 Jun;25(2):625-632. Epub 2024 Feb 17. Jun; 2. [CrossRef] [PubMed]
- Ostojić M, Bulj Z, Kordić D, Šunjić D, Buntić A, Juka K, Bliznac I, Topić A, Ostojić Z, Rotim K, Bekić M. ESTABLISHMENT OF THE BONE TISSUE BANK AT MOSTAR UNIVERSITY CLINICAL HOSPITAL. Acta Clin Croat. 2019 Dec;58(4):571-575. 4. [CrossRef] [PubMed] [PubMed Central]
- Jack GZ. Use of Autogenous Bone Graft from the Iliac Crest to Restore an Atrophic Maxilla with Implant-Retained Prosthesis. Clinical showcase. JCDA 2006 July-August 2006, Vol. 72, No. 6.
- Freilich MM, Sándor GK. In-office iliac crest bone harvesting for peri-implant jaw reconstruction. J Can Dent Assoc. 2006 Jul-Aug;72(6):543-7. [PubMed]
- Pereira E, Messias A, Dias R, Judas F, Salvoni A, Guerra F. Horizontal Resorption of Fresh-Frozen Corticocancellous Bone Blocks in the Reconstruction of the Atrophic Maxilla at 5 Months. Clin Implant Dent Relat Res. 2015 Oct;17 Suppl 2(Suppl 2):e444-58. Epub 2014 Oct 27. [CrossRef] [PubMed] [PubMed Central]
- Sethi A, Kaus T, Cawood JI, Plaha H, Boscoe M, Sochor P. Onlay bone grafts from iliac crest: a retrospective analysis. Int J Oral Maxillofac Surg. 2020 Feb;49(2):264-271. Epub 2019 Jul 24. [CrossRef] [PubMed]
- Csönge L, Bozsik Á, Tóth-Bagi Z, Gyuris R, Kónya J. Regenerative medicine: characterization of human bone matrix gelatin (BMG) and folded platelet-rich fibrin (F-PRF) membranes alone and in combination (sticky bone). Cell Tissue Bank. 2021 Dec;22(4):711-717. Epub 2021 Jun 1. 4. [CrossRef] [PubMed] [PubMed Central]
- Sheikh Z, Sima C, Glogauer M. Bone Replacement Materials and Techniques Used for Achieving Vertical Alveolar Bone Augmentation. Materials (Basel). 2015 May 27;8(6):2953–93. 6. [CrossRef] [PubMed Central]
- Kim NH, Yang BE, On SW, Kwon IJ, Ahn KM, Lee JH, Byun SH. Customized three-dimensional printed ceramic bone grafts for osseous defects: a prospective randomized study. Sci Rep. 2024 Feb 10;14(1):3397. 1. [CrossRef] [PubMed] [PubMed Central]
- Ferraz MP. Bone Grafts in Dental Medicine: An Overview of Autografts, Allografts and Synthetic Materials. Materials (Basel). 2023 May 31;16(11):4117. [CrossRef] [PubMed] [PubMed Central]
- Ma G, Wu C, Shao M. Simultaneous implant placement with autogenous onlay bone grafts: a systematic review and meta-analysis. Int J Implant Dent. 2021 Apr 30;7(1):61. [CrossRef] [PubMed] [PubMed Central]
- Lehmijoki M, Holming H, Thorén H, Stoor P. Rehabilitation of the severely atrophied dentoalveolar ridge in the aesthetic region with corticocancellous grafts from the iliac crest and dental implants. Med Oral Patol Oral Cir Bucal. 2016 Sep 1;21(5):e614-20. 5. [CrossRef] [PubMed] [PubMed Central]
- Matichescu A, Ardelean LC, Rusu LC, Craciun D, Bratu EA, Babucea M, Leretter M. Advanced Biomaterials and Techniques for Oral Tissue Engineering and Regeneration-A Review. Materials (Basel). 2020 Nov 23;13(22):5303. 22. [CrossRef] [PubMed] [PubMed Central]
- Dutra Roos B, Valdomiro Roos M, Camisa Júnior A, Moreno Ungaretti Lima E, Noshang Pereira R, Luciano Zangirolami M, Machado de Albuquerque G. Prevalence of microbiological markers in bone tissue from live and cadaver donors in the musculoskeletal tissue bank of Passo Fundo. Rev Bras Ortop. 2014 Mar 20;49(4):386-90. 4. [CrossRef] [PubMed] [PubMed Central]
- Braun C, Löwel M, Heuer M, Pruß A, Schulz T. Bioburden of postmortem bone tissues with a procurement time exceeding 36 h. Cell Tissue Bank. 2025 May 26;26(3):27. 3. [CrossRef] [PubMed] [PubMed Central]
- Van Rompaey V, Vandamme W, Muylle L, Van de Heyning PH. Temporal bone bank: complying with European Union directives on human tissue and cells. Cell Tissue Bank. 2012 Jun;13(2):231-40. 2. [CrossRef] [PubMed]
- Ip VHY, Sherman J, Eckelman MJ. Building a sustainable future in health care: collaboration and framework for meaningful life cycle assessment. Can J Anaesth. 2024 Nov;71(11):1441-1446. English. Nov; 11. [CrossRef] [PubMed]
- Wood N. Environmental sustainability in dentistry: A call for ethical and eco-conscious practices. South African Dental Journal. 2023 78. 287-289. [CrossRef]
- Winter S, McDonagh G, Lappin D, Smith AJ. Assessing the efficacy and cost of detergents used in a primary care automated washer disinfector. Br Dent J. 2018 Aug 24;225(4):315-319. 4. [CrossRef] [PubMed]
- Brett D. Sustainable Dentistry Making a Difference. Book. Springer 2022. [CrossRef]
- Künzle P, Frank AC, Paris S. Environmental Impact of a Tooth Extraction: Life Cycle Analysis in a University Hospital Setting. Community Dent Oral Epidemiol. 2025 Jun 27. Epub ahead of print. [CrossRef] [PubMed]
- Akintoye SO, Giavis P, Stefanik D, Levin L, Mante FK. Comparative osteogenesis of maxilla and iliac crest human bone marrow stromal cells attached to oxidized titanium: a pilot study. Clin Oral Implants Res. 2008 Nov;19(11):1197-201. 11. [CrossRef] [PubMed] [PubMed Central]
- Mishchenko O, Yanovska A, Kosinov O, Maksymov D, Moskalenko R, Ramanavicius A, Pogorielov M. Synthetic Calcium-Phosphate Materials for Bone Grafting. Polymers (Basel). 2023 Sep 19;15(18):3822. [CrossRef] [PubMed] [PubMed Central]
- Naujokat H, Loger K, Gülses A, Flörke C, Acil Y, Wiltfang J. Effect of enriched bone-marrow aspirates on the dimensional stability of cortico-cancellous iliac bone grafts in alveolar ridge augmentation. Int J Implant Dent. 2022 Sep 5;8(1):34. 1. [CrossRef] [PubMed] [PubMed Central]
- Wortmann DE, van Minnen B, Delli K, Schortinghuis J, Raghoebar GM, Vissink A. Harvesting anterior iliac crest or calvarial bone grafts to augment severely resorbed edentulous jaws: a systematic review and meta-analysis of patient-reported outcomes. Int J Oral Maxillofac Surg. 2023 Apr;52(4):481-494. Epub 2022 Oct 13. 4. [CrossRef] [PubMed]
- Bhumiratana S, Bernhard JC, Alfi DM, Yeager K, Eton RE, Bova J, Shah F, Gimble JM, Lopez MJ, Eisig SB, Vunjak-Novakovic G. Tissue-engineered autologous grafts for facial bone reconstruction. Sci Transl Med. 2016 Jun 15;8(343):343ra83. 343. [CrossRef] [PubMed] [PubMed Central]
- Wortmann DE, Klein-Nulend J, van Ruijven LJ, Schortinghuis J, Vissink A, Raghoebar GM. Incorporation of anterior iliac crest or calvarial bone grafts in reconstructed atrophied maxillae: A randomized clinical trial with histomorphometric and micro-CT analyses. Clin Implant Dent Relat Res. 2021 Jun;23(3):492-502. Epub 2021 May 30. 3. [CrossRef] [PubMed] [PubMed Central]
- Peeva-Petreska M, Veleska-Stevkovska D, Cucchi A, Perale G, Viktor S. Jaw’s Bone Augmentation with New Generation of Bone Composite Substitute Materials. Ecronicon, 2019.
- Monje A, Monje F, Galindo-Moreno P, Montanero-Fernandez J, Suarez F, Wang HL. Microstructural and densiometric analysis of extra oral bone block grafts for maxillary horizontal bone augmentation: a comparison between calvarial bone and iliac crest. Clin Oral Implants Res. 2014 Jun;25(6):659-64. Epub 2013 Apr 28. 6. [CrossRef] [PubMed]
- C, *!!! REPLACE !!!*; Kim, SY. Kim YK, Kim SG, Byeon JH, Lee HJ, Um IU, Lim SC, Kim SY. Development of a novel bone grafting material using autogenous teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010 Apr;109(4):496-503. Epub 2010 Jan 8. 4. [CrossRef] [PubMed]
- Chaair H, Labjar H, Britel O. Synthesis of β-tricalcium phosphate. Morphologie. 2017 Sep;101(334):120-124. Epub 2017 Sep 21. [CrossRef] [PubMed]
- Patiño-Marín N, Villa García LD, Aguirre López EC, Medina-Solís CE, Martínez Zumarán A, Martínez Rider R, Márquez Preciado R, Rosales García P, Salas Orozco MF. Sterilization and Disinfection: Ensuring Infection Control in Dental Practices. Cureus. 2025 Feb 15;17(2):e79041. 2. [CrossRef] [PubMed] [PubMed Central]
- Ionut-Daniel GG, Maria-Alexandra M, Oana B, Iris.Malina M, Ana-Emanuela B, Doinita TO, Ionut-Catalin B, Carmen Elena C, Efficiency of disinfection and sterilization in dental medicine practice. Review. Romanian J of Medical and Dental Education. 2023;12(3), 45-50.
- Ma Y, Han S. Carbon Neutral Hand Surgery: Simple Changes to Reduce Carbon Footprint. Plast Surg (Oakv). 2024 Feb;32(1):108-112. Epub 2022 Mar 24. [CrossRef] [PubMed] [PubMed Central]
- Snigdha, Hiloidhari M, Bandyopadhyay S. Environmental footprints of disposable and reusable personal protective equipment ‒ a product life cycle approach for body coveralls. J Clean Prod. 2023 Mar 25;394:136166. Epub 2023 Jan 27. [CrossRef] [PubMed] [PubMed Central]
- https://healthcarelca.com (accessed on 09.11.2025). (accessed on 09.11.2025).

| Nr | Device | Model | Performance |
| 1 | Fridge/Freezer | Midea Chest Freezer HS-543CN | 333 W |
| 2 | Bone cutting machine | N/A | 1500 W |
| 3 | Thermostat | L MIM | 5500 W |
| 4 | Bone grinding machine | Ikawerke | 1000 W |
| 5 | Sieve machine | Retsch AS 200 | 315 W |
| 6 | Ethylen oxide steriliser | Steri-Vac 5XL Gas Sterilizer | 2300 W |
| 7 | Sealer machine | Steriking RS 3200 | 240 W |
| 8 | Lyophilizer | Scanvac Coolsafe 90-80 Superior | 2100 W |
| 9 | Air conditioner | AUX | 5400 W |
| 10 | Laptop | Lenovo E1 Vision | 15 W |
| 11 | Laminar box | Laminar Box Airflow BPV-1200 FRM | 750 W |
| 12 | Autoclave | N/A | 1000 W |
| Impact category | Reference unit | Results | |
| Cortico-cancellous or cancellous bone blocks | Bone granulates | ||
| Acidification: terrestrial | kg SO2-Eq | 3.55182E+00 | 3.60037E+00 |
| Climate change | kg CO2-Eq | 7.57547E+01 | 9.03633E+01 |
| Ecotoxicity: freshwater | kg 1,4-DCB-Eq | 1.23332E-02 | 1.41085E-02 |
| Ecotoxicity: marine | kg 1,4-DCB-Eq | 1.18627E-01 | 1.28481E-01 |
| Ecotoxicity: terrestrial | kg 1,4-DCB-Eq | 2.30777E+02 | 2.49541E+02 |
| Energy resources: non-renewable, fossil | kg oil-Eq | 0.00000E+00 | 0.00000E+00 |
| Eutrophication: freshwater | kg P-Eq | 4.61170E-05 | 5.24151E-05 |
| Eutrophication: marine | kg N-Eq | 1.32341E-04 | 1.60673E-04 |
| Human toxicity: carcinogenic | kg 1,4-DCB-Eq | 2.68543E-01 | 2.58623E-01 |
| Human toxicity: non-carcinogenic | kg 1,4-DCB-Eq | 1.49157E+01 | 1.53398E+01 |
| Ionising radiation | kBq Co-60-Eq | 1.60606E+01 | 1.61292E+01 |
| Land use | m2*a crop-Eq | 1.34146E-05 | 1.34146E-05 |
| Material resources: metals/minerals | kg Cu-Eq | 4.60250E+02 | 4.61993E+02 |
| Ozone depletion | kg CFC-11-Eq | 2.70411E-04 | 2.91374E-04 |
| Particulate matter formation | kg PM2.5-Eq | 1.07648E+00 | 1.08982E+00 |
| Photochemical oxidant formation: human health | kg NOx-Eq | 3.28775E-01 | 3.92283E-01 |
| Photochemical oxidant formation: terrestrial ecosystems | kg NOx-Eq | 3.33479E-01 | 3.97041E-01 |
| Water use | m3 | 4.00000E-03 | 4.00000E-03 |
| Impact category | Cortico-cancellous or cancellous bone blocks | Bone granulates |
| Climate change: human health | 7,03042E-05 | 8,38616E-05 |
| Human toxicity: carcinogenic | 5,34478E-06 | 5,28305E-06 |
| Human toxicity: non-carcinogenic | 3,398E-06 | 3,49463E-06 |
| Ionising radiation | 1,36462E-07 | 1,37044E-07 |
| Ozone depletion | 1,43562E-07 | 1,54691E-07 |
| Particulate matter formation | 0,000675749 | 0,000684133 |
| Photochemical oxidant formation: human health | 2,99189E-07 | 3,56981E-07 |
| Total | 0,000744685 | 0,000766855 |
| Total in days: | 0,271990604 | 0,280087806 |
| Total in hours | 6,5277745 | 6,72210735 |
| Total in minutes /1g of product | 0,78333 | 0,806652 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



