Submitted:
19 December 2025
Posted:
19 December 2025
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background: Early evidence from a nursing home in Yepes (Toledo, Spain) indicated that antihistamines combined with azithromycin prevented deaths and hospitalizations dur-ing the first COVID-19 wave. Subsequent data from the Consorci Sanitari de Terrassa (CST) showed that patients chronically taking antihistamines significantly reduced hos-pital admissions and mortality. However, a concerning rise in long COVID incidence (2–5%) after the third infection and a doubling of thrombosis rates in patients over 60 were observed. Objective: This study aimed to determine whether chronic antihistamine pre-scription is associated with a reduction in long COVID syndrome and thrombotic events. Methods: We analyzed anonymized data from the CST population (n=192,651 as of March 2025). Variables included age, gender, chronic antihistamine use, number of chronic treatments (nT), COVID-19 vaccination status, SARS-CoV-2 infection history, long COVID (LC) incidence, and aggregated thrombotic events. Odds ratios (OR) were calculated using chi-square tests. Results: The prevalence of LC increased progressively with successive in-fections in the non-antihistamine group. No significant differences were found with the antihistamine group, which presented no LC cases among the 52 patients with three documented infections. Thrombotic events were significantly less frequent in antihista-mine users with at least one chronic prescription (p< 0.0001). Conclusions: Results suggest a protective effect of antihistamines against thrombotic events. While confirmation via multicenter, randomized trials is needed, a pragmatic approach using antihistamines could be considered for symptomatic patients in the early stage of infection.
Keywords:
long COVID
; thrombosis
; vaccine
; COVID-19
1. Introduction
SARS-CoV-2 infection is associated with long COVID syndrome [1] and other long-lasting multi-organ effects [2,3], including cardiovascular sequelae [4].
The prevalence of long COVID has been shown to increase substantially after the third documented infection. Furthermore, overall thrombotic events—including ischemic cardiopathy, ischemic stroke, pulmonary thromboembolism, and thrombosis of retinal vessels—doubled from 2020 to 2024 in patients over 60 years old, even in those not on chronic treatments [5]
During the early stages of the pandemic, several targets were explored for drug repurposing. In one study, 29 FDA-approved drugs were identified as potential inhibitors of the interaction between host factors and the SARS-CoV-2 virus [6], including the antihistamine loratadine. Preliminary evidence of a protective effect from pragmatic use emerged from an experience at the Yepes nursing home for the elderly (Toledo, Spain). During the first wave, all residents became infected, but none died or required hospital admission after receiving treatment with antihistamines and azithromycin [7]; this contrasted with a mortality rate of 40% in the surrounding area [8]. The use of the same treatment in primary care patients in the same area was associated with a reduction in hospital admissions compared to national rates in Spain [9]. A similar, significant reduction in hospital admissions and death was observed among patients on chronic antihistamine therapy in a large integrated health care consortium in the metropolitan area of Barcelona. This study analyzed data from a population of over 150,000, encompassing more than 30,000 infections and over 1,400 hospital admissions [10].
The aim of the present study was to assess whether chronic antihistamine use was associated with a different risk of progression to long COVID syndrome and the development of thrombotic events following COVID-19.
2. Materials and Methods
The descriptive study of COVID-19 hospital admissions received approval from the Ethics Committee of the Consorci Sanitari de Terrassa (CST) on April 8, 2020 (ref. 02-20-161-021) and was registered as an observational trial at ClinicalTrials.gov on April 29, 2020 (NCT04367883). A subsequent amendment to analyze the variable of antihistamine treatment relative to the reference population was approved on June 13, 2022 (ref. 02-22-151-060) and posted on August 17, 2022 (NCT05504057; https://clinicaltrials.gov/study/NCT05504057, accessed November 30, 2025). Finally, the study was expanded to include long COVID syndrome and thrombotic events on February 24, 2025. The planning, conduct, and reporting of the study were in accordance with the principles of the Declaration of Helsinki.
2.1. Socioeconomic Environment
The socioeconomic profile of the Consorci Sanitari de Terrassa (CST) has been described in previous publications [10,11]. In brief, the CST is a public healthcare provider for a population of 192,651 residents (as of March 2025) in Barcelona’s North Metropolitan Health Region. Its network of primary care centers serves a demographically diverse area comprising rural, residential, and metropolitan communities. Prior to the pandemic, life expectancy in the region consistently exceeded 81 years. Furthermore, COVID-19 vaccination coverage exceeded 90% among elderly patients with multiple chronic conditions, while infection rates were similar across all centers, ranging from 22% to 27%. The proportion of residents aged over 60 varies across centers from 15.1% to 24%, with most CST centers serving populations where over one-fifth of residents fall within this age group. The ‘Hospital Universitari de Terrassa’ serves as the reference hospital for these centers.
2.2. Quantification of Long COVID Syndrome Prevalence and Thrombosis
The Data Analysis Control Department collected anonymized data from the entire CST population without exclusions. This included information on COVID-19 infections, hospital admissions, long COVID syndrome (LC), and thrombotic events (Thr)—including strokes, myocardial infarction, pulmonary thromboembolism, and retinal vessel thrombosis—from March 2020 to March 2025. Data on gender, age, number of chronic treatments (nt), and COVID-19 vaccination status relative to the first infection (V preinf, V postinf, or NoV) were also collected. Patients receiving acute antihistamine treatment and no other chronic therapies were categorized as the AntiHm group (subgroup 0nT). Case and hospitalization data have been analyzed previously [10,11]. The present study focuses specifically on the incidence of long COVID syndrome and thrombosis as long-term effects of COVID-19 infection.
The most likely SARS-CoV-2 variant responsible for each patient’s first infection was inferred by matching the infection date with the predominant variant circulating in Spain during that period, using data from the Covariants website [12].
2.4. Statistical Analysis
Patients were stratified by gender, age (≤60 or >60 years), number of SARS-CoV-2 infections, vaccination status, and number of chronic treatments (nT), as well as by the use of chronic antihistamine treatment (AntiHm or NoAntiHm). To calculate the odds ratio (OR) for the NoAntiHm/AntiHm comparison, only patients with at least one chronic prescription were included (≥1nT), thereby excluding those with no chronic treatments. Subgroups were compared using chi-square tests via OpenEpi [13], applied only to categories containing at least five cases.
3. Results
3.1. Long COVID Prevalence and Chronic Treatment with Antihistamines
The association between prevalent Long COVID (LC) and the number of infections, chronic treatments, vaccination status, and chronic antihistamine use is detailed in Table 1 and Supplementary Material S1. LC prevalence increased with the number of infections in the NoAntiHm group. Notably, no LC cases were identified among the 152 AntiHm patients with two infections who had been vaccinated prior to their first infection, nor among the 52 AntiHm patients with three or more infections. While no statistically significant differences were detected between the overall AntiHm and NoAntiHm groups, direct comparisons with specific polypharmacy subgroups were not possible, as most AntiHm subgroups either contained no cases or had fewer than five cases (see Supplementary Material S1).
3.2. Thrombotic Events in the COVID Era by Gender, Polypharmacy, Vaccination and COVID-19 Waves
Up to 2,458 thrombotic events were recorded between March 1, 2020, and March 28, 2025, and are presented in Figure 1. Additionally, 90 hemorrhagic ictus occurred that are not represented in the figure about thrombosis. A progressive rise in thrombosis is observed, with 429, 493, 529, and 550 cases from 2021 to 2024, respectively. Thrombosis appeared in all polypharmacy groups and also in patients with no chronic prescriptions to treat any comorbidity in both genders (see W 0 or M 0 in Figure 1). Significant gender differences were found (p < 0.0001), with 59.3% of the registered thrombosis occurring in men.
Although thrombotic events appeared more frequent during colder months (October to March in each season), no clear relationship was observed between thrombotic events and COVID-19 waves when comparing them with COVID-19 admissions at the institution’s reference hospital (Figure 2). Therefore, COVID-19 waves that peaked in summer—such as waves 7–9 in 2021 (the Delta wave) and those in 2023 and 2024, which included several Omicron waves that rose during July of those years—were not directly correlated with thrombotic events in the same trimester.
The relationship of thrombotic events with vaccination status and age (below or over 60 years old) is illustrated in Figure 3. Thrombotic events are rising in both vaccinated individuals and those without vaccination records, in people over and under 60 years old.
The predominant SARS-CoV-2 variant at the time of the first infection in patients who had at least one documented infection before the thrombosis is represented in Figure 4
3.3. Thrombotic Events and Antihistamines
Overall, thrombotic events increased by 28% between 2021 and 2024, affecting 1.6% of AntiHm patients and 3.3% of No AntiHm patients with at least one chronic prescription (p < 0.0001) (Table 2).
Significant ORs (1.52–2.53) were found between the No AntiHm and AntiHm groups with at least 1 nt, when comparing thrombosis in vaccinated patients before or after the first infection and in non-infected patients (Table 3). Detailed data for age and nt subgroups, related to vaccination status and SARS-CoV-2 infection, are presented in Supplementary Data S2. No thrombosis appeared in patients treated incidentally with antihistamines who had no other chronic treatments (AntiHm 0nT, S2).
4. Discussion
To our knowledge, this is the first study to report an absence of long COVID in most subgroups of patients on chronic antihistamine therapy, alongside a substantial reduction in post-COVID-19 cardiovascular events in this population.
The present findings support the design of future prospective trials to confirm these observations, which should aim to include patients across all polypharmacy groups.
4.1. Antihistamines and Long COVID
The limited number of long COVID patients in each subgroup precludes definitive conclusions regarding the role of antihistamines in preventing long COVID. However, the higher frequency of subgroups with no long COVID cases within the antihistamine cohort suggests a potential protective effect.
These findings align with prior reports. Notably, no long COVID cases were documented following the pragmatic, empirical use of H1 antihistamines in primary care patients [9]. Furthermore, a randomized controlled trial of the H2 antihistamine famotidine reported improvement in cognitive and behavioral dysfunction following SARS-CoV-2 infection [14].
The results are consistent with a proposed histamine class-effect on neurological symptoms, mediated by several underlying mechanisms—including neuroactive ligand-receptor interactions. For instance, the antihistamine loratadine has been suggested to act as an antagonist of GRIN2B via this pathway [15]. GRIN genes encode N-methyl-D-aspartate receptors (NMDARs), and their dysregulation is linked to intellectual disability disorders [16].
4.2. Antihistamines, Respiratory Viruses and Thrombosis
While thrombotic events appeared in all polypharmacy groups in the No AntiHm group (including patients with no previous chronic conditions to ≥8 nT), the reduction in AntiHm-treated patients was highly significant in most polypharmacy subgroups, suggesting a protective role, as previously reported for H1 antihistamines in hospital admissions and death [7,9,10]. This antithrombotic effect is consistent with the previously reported effect of both H1 and H2 antihistamines on platelet-activating factor (PAF) [17]. The antihistamine H1 rupatadine is a well-known PAF antagonist [18]. Famotidine, an H2 antihistamine, was found to improve the rate of symptom resolution and reduce interferon-alpha plasma levels [19].”
Other respiratory viruses, such as influenza, have been linked to thrombotic events [20,21,22]. While several respiratory viruses typically circulate concurrently each winter in the studied area, surveillance data from public programs [23] indicate that the winter of 2020-2021 had a surprisingly low incidence of influenza. Influenza was detected in only 0.4% of 256 positive samples collected by sentinel healthcare workers from randomly selected patients, compared to 18.4% for SARS-CoV-2 and 80.9% for other viruses [24], Table 2. Therefore, the increase in thrombosis observed in the first half of 2021 cannot be attributed to seasonal influenza infection.
Exposure to respiratory viruses with thrombotic potential, which circulate more commonly in winter, may explain the higher number of thrombotic events during that season. Previous research has reported a higher incidence of thrombotic thrombocytopenic purpura [25], myocardial infarction [26], and strokes in winter, the latter also being linked to increased pollution on colder days [27]. Our results, which show a greater number of thrombotic events during the colder months from October to March, are consistent with these data.
The higher proportion of thrombotic events in men is consistent with previous studies, since it is known that estrogen signaling is anti-inflammatory with vascular protective effects [28].
While the relationship between thrombosis and vaccination has yielded controversial results, with some studies reporting more events [29,30] and others dismissing an association [31], it is important to note that the increase in thrombosis is also observed here in non-vaccinated and non-infected patients, as previously described [10]. Since COVID-19 has been reported to be thrombogenic through diverse mechanisms [32,33], the rise in thrombosis could be related to undiagnosed infections after 2022, which may be more frequent in the non-vaccinated group.
4.3. Limitations of the Study
The apparent rise in thrombotic events, assessed retrospectively in the population surviving as of 2025, could underestimate the true incidence by excluding patients who suffered early fatal thrombosis. However, the increase observed even among patients with low polypharmacy—who likely had higher survival rates—suggests that the rise is genuine.
The 15% increase in the population of the area during the last four years could also explain a global rise in thrombotic events, particularly in the subgroup without vaccination records, since they may represent patients who were not living in the CST area during the early stage of the pandemic. On the other hand, individuals below 60 years old had the possibility of being vaccinated outside the institution, and the rate of under-registration may be higher among those who, after four years, now belong to the group over 60. However, the rise observed in all polypharmacy subgroups, which implies the existence of vaccination records from early 2021, also suggests a long-lasting and real increase in thrombotic rates.
The presence of another private hospital in the area may have led some patients to seek care and receive diagnoses at that facility. Consequently, the number of events detected in our study is likely an underestimate.
Finally, a chronic antihistamine prescription does not guarantee consistent medication intake. Future studies with a specific ‘intention-to-treat’ design are needed to confirm these findings.
5. Conclusions
The results suggest a protective effect of antihistamines against thrombotic events. While this finding requires confirmation through multicenter, randomized, prospective trials, a pragmatic approach using antihistamines could be considered for symptomatic patients in the early stages of respiratory viral infections.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, A.P.-S. methodology, A.P.-S. and R.R.-P.; validation, All authors; formal analysis, A.P.-S.; investigation, all authors.; resources, A.A.-G. and R.R.-P.; data curation, M.C.G.-A.; M.LL.; M, G-N; A.P.-S.; writing—original draft preparation, review and editing, A.P.-S.; supervision, R.R.-P; M.Ll.; C, L-P; R, V-F and A.A.-G.; project administration, R.R.-P. and A.A.-G.; All authors have read and agreed to the published version of the manuscript.
Funding
The research was funded by the GENERALITAT DE CATALUNYA, grant number PT-082023-EP subproject COVID-P.
Institutional Review Board Statement
The original descriptive study of patients with COVID-19 was approved by the Ethics Committee of CST on 8 April 2020, (ref 02-20-161-021), and the observational clinical trial was posted on 29 April 2020 (NCT 04367883). The study has been prolonged successively and complemented with several repurposing drugs on 13 June 2022 (https://clinicaltrials.gov/study/NCT05504057, accessed on 11 March 2025). The study was extended, including post-COVID-19 syndrome and thrombosis, on 24 February 2025. The planning, conduct, and reporting of the study were in line with the Declaration of Helsinki. The cross-sectional study of long COVID-19 prevalence in the Consorci Sanitari de Terrassa (CST) (Ref 02-24-156-028) was approved by the Ethics Committee of the CST on 29 January 2024.
Informed Consent Statement
Patient consent was waived due to the use of anonymized data
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author.
Acknowledgments
Authors wish to acknowledge the valuable contribution of Dr Mariana Castells, Professor of Medicine in the Harvard Medical School, for providing relevant bibliography on anti-histamines and platelet-activating factor. Authors also wish to thank the support given in the preparation of anonymized data provided by Marta González Salvador, from the Management, Control and Information, Analysis Unit, Hospital Universitari de Terrassa, Consorci Sanitari de Terrassa (CST). We also thank Juanes-González, M.; Calderón-Valdiviezo, A.I.; Losa-Puig, H.; León-Pérez, M.;Pueyo-Antón, L.; Franco-Romero, M.; for the initial research that led to stratify by number of chronic treatments.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| AntiHm | Antihistamines |
| LC | Long COVID |
| No V | Non-vaccinated |
| Preinf | Previous to the SARS-CoV-2 infection |
| Postinf | Posterior to the SARS-CoV-2 infection |
| Pre Thr | Previous to the thrombosis |
| Post Th | Posterior to the thrombosis |
| CoV | SARS-CoV-2 infection |
| CST | Consorci Sanitari de Terrassa |
References
- O’Mahoney, L.L.; Routen, A.; Gillies, C.; Jenkins, S.A.; Almaqhawi, A.; Ayoubkhani, D.; Banerjee, A.; Brightling, C.; Calvert, M.; Cassambai, S.; et al. The risk of Long Covid symptoms: A systematic review and meta-analysis of controlled studies. Nat. Commun. 2025, 16, 4249. [Google Scholar] [CrossRef]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef]
- Davis, H.E.; McCorkell, L.; Vogel, J.M.; Topol, E.J. Long COVID: Major findings, mechanisms and recommendations. Nat. Rev. Microbiol. Erratum in Nat. Rev. Microbiol. 2023, 21, 408.. 2023, 21, 133–146. [Google Scholar] [CrossRef]
- Koutsiaris, A.G.; Karakousis, K. Long COVID Mechanisms, Microvascular Effects, and Evaluation Based on Incidence. Life 2025, 15, 887. [Google Scholar] [CrossRef]
- Arévalo-Genicio, A.; García-Arqué, M.C.; Gragea-Nocete, M.; Llistosella, M.; Moro-Casasola, V.; Pérez-Díaz, C.; Puigdellívol-Sánchez, A.; Roca-Puig, R. Long COVID Syndrome Prevalence in 2025 in an Integral Healthcare Consortium in the Metropolitan Area of Barcelona: Persistent and Transient Symptoms. Vaccines 2025, 13, 905. [Google Scholar] [CrossRef] [PubMed]
- Gordon, D.E.; Jang, G.M.; Bouhaddou, M.; Xu, J.; Obernier, K.; White, K.M.; O’Meara, M.J.; Rezelj, V.V.; Guo, J.Z.; Swaney, D.L. A SARS-CoV-2 Protein Interaction Map Reveals Targets for Drug-Repurposing. Nature 2020, 583, 459–468. [Google Scholar] [CrossRef] [PubMed]
- Morán Blanco, J.I.; Alvarenga Bonilla, J.A.; Homma, S.; Suzuki, K.; Fremont-Smith, P.; Villar Gómez de Las Heras, K. Antihistamines and azithromycin as a treatment for COVID-19 on primary health care—A retrospective observational study in elderly patients. Pulm. Pharmacol. Ther. 2021, 67, 101989. [Google Scholar] [CrossRef]
- Bielza, R.; Sanz, J.; Zambrana, F.; Arias, E.; Malmierca, E.; Portillo, L.; Thuissard, I.J.; Lung, A.; Neira, M.; Moral, M.; et al. Clinical Characteristics, Frailty, and Mortality of Residents with COVID-19 in Nursing Homes of a Region of Madrid. J. Am. Med. Dir. Assoc. 2021, 22, 245–252. [Google Scholar] [CrossRef]
- Morán Blanco, J.I.; Alvarenga Bonilla, J.A.; Fremont-Smith, P.; Villar Gómez de Las Heras, K. Antihistamines as an early treatment for COVID-19. Heliyon 2023, 9, e15772. [Google Scholar] [CrossRef] [PubMed]
- Puigdellívol-Sánchez, A.; Juanes-González, M.; Calderón-Valdiviezo, A.; Losa-Puig, H.; Valls-Foix, R.; González-Salvador, M.; Lozano-Paz, C.; Vidal-Alaball, J. COVID-19 in Relation to Chronic Antihistamine Prescription. Microorganisms 2024, 12, 2589. [Google Scholar] [CrossRef]
- Puigdellívol-Sánchez, A.; Juanes-González, M.; Calderón-Valdiviezo, A.I.; Losa-Puig, H.; González-Salvador, M.; León-Pérez, M.; Pueyo-Antón, L.; Franco-Romero, M.; Lozano-Paz, C.; Cortés-Borra, A.; et al. COVID-19 Pandemic Waves and 2024–2025 Winter Season in Relation to Angiotensin-Converting Enzyme Inhibitors, Angiotensin Receptor Blockers and Amantadine. Healthcare (Basel) 2025, 13, 1270. [Google Scholar] [CrossRef] [PubMed]
- CoVariants; Hodcroft, E. Institute of Social and Preventive Medicine University of Bern, Switzerland & SIB Swiss Insitute of 375 Bioinformatics. Available online: https://covariants.org/ (accessed on 30 March 2025).
- Dean, A.G.; Sullivan, K.M.; Soe, M.M. OpenEpi: Open Source Epidemiologic Statistics for Public Health, Versión. Available online: https://www.openepi.com/Menu/OE_Menu.htm (accessed on 30 March 2025).
- Momtazmanesh, S.; Ansari, S.; Izadi, Z.; Shobeiri, P.; Vatankhah, V.; Seifi, A.; Ghiasvand, F.; Bahrami, M.; Salehi, M.; Noorbala, A.A.; Akhondzadeh, S. Effect of famotidine on cognitive and behavioral dysfunctions induced in post-COVID-19 infection: A randomized, double-blind, and placebo-controlled study. J Psychosom Res. 2023, 172, 111389. [Google Scholar] [CrossRef] [PubMed]
- Oh, K.K.; Adnan, M.; Cho, D.H. Network Pharmacology Study to Elucidate the Key Targets of Underlying Antihistamines against COVID-19. Curr. Issues Mol. Biol. 2022, 44, 1597–1609. [Google Scholar] [CrossRef]
- Korinek, M.; Candelas Serra, M.; Abdel Rahman, F.; Dobrovolski, M.; Kuchtiak, V.; Abramova, V.; Fili, K.; Tomovic, E.; Hrcka Krausova, B.; Krusek, J.; Cerny, J.; Vyklicky, L.; Balik, A.; Smejkalova, T. Disease-Associated Variants in GRIN1, GRIN2A and GRIN2B genes: Insights into NMDA Receptor Structure, Function, and Pathophysiology. Physiol Res. 2024, 73, S413–S434. [Google Scholar] [CrossRef]
- Sansom, J.E.; Brooks, J.; Burton, J.L.; Archer, C.B. Effects of H1- and H2-antihistamines on platelet-activating factor and bradykinin-induced inflammatory responses in human skin. Clin Exp Dermatol 1996, 21, 33–37. [Google Scholar] [CrossRef]
- Izquierdo, I.; Casas, L.; Cabrera, S.; Fernandez, A. How to handle off-label prescriptions of rupatadine, a second-generation antihistamine and PAF antagonist: a review. Drugs Context. 2024, 13, 2023–9-5. [Google Scholar] [CrossRef]
- Brennan, C.M.; Nadella, S.; Zhao, X.; Dima, R.J.; Jordan-Martin, N.; Demestichas, B.R.; Kleeman, S.O.; Ferrer, M.; von Gablenz, E.C.; Mourikis, N.; et al. Oral famotidine versus placebo in non-hospitalised patients with COVID-19: A randomised, double-blind,data-intense, phase 2 clinical trial. Gut 2022, 71, 879–888. [Google Scholar] [CrossRef]
- Bunce, P.E.; High, S.M.; Nadjafi, M.; Stanley, K.; Liles, W.C.; Christian, M.D. Pandemic H1N1 influenza infection and vascular thrombosis. Clin Infect Dis 2011, 52, e14–e17. [Google Scholar] [CrossRef]
- Chow, E.J.; Rolfes, M.A.; O’Halloran, A.; Anderson, E.J.; Bennett, N.M.; Billing, L.; et al. Acute Cardiovascular Events Associated With Influenza in Hospitalized Adults: A Cross-sectional Study. Ann Intern Med 2020, 173, 605–613. [Google Scholar] [CrossRef] [PubMed]
- Rubino, R.; Imburgia, C.; Bonura, S.; Trizzino, M.; Iaria, C.; Cascio, A. Thromboembolic Events in Patients with Influenza: A Scoping Review. Viruses 2022, 14, 2817. [Google Scholar] [CrossRef]
- Generalitat de Catalunya. Available online: https://sivic.salut.gencat.cat/ (accessed on 3 December 2025).
- Generalitat de Catalunya. Available online: https://scientiasalut.gencat.cat/bitstream/handle/11351/8851/pidirac_balanç_temporada_gripal_2020_2021.pdf (accessed on 3 December 2025).
- Jacobs, J.W.; Stanek, C.G.; Booth, G.S.; Symeonidis, A.; Shih, A.W.; Allen, E.S.; Gavriilaki, E.; Grossman, B.J.; Pavenski, K.; Moorehead, A.; et al. The seasonal distribution of immune thrombotic thrombocytopenic purpura is influenced by geography: Epidemiologic findings from a multi-center analysis of 719 disease episodes. Am J Hematol. 2024, 99, 2063–2074. [Google Scholar] [CrossRef]
- Javaid, S.S.; Zahid, K.; Ashfaq, H.; Rahman, S.; Shahid, S.; Abbasi, M.B.; Imran, S.; Thada, P.K.; Mengal, A.; Habib, H.; Ullah, M.S.; Kumar, S.; Farooqui, S.K. Seasonal variations in hospitalizations of heart failure patients: a United States nationwide analysis. Minerva Cardiol Angiol Epub ahead of print. 2025. [Google Scholar] [CrossRef]
- Li, L.; Ge, Q.; Sun, S.; Yang, S.; Wei, J.; Sun, Y.; Fan, X.; Liu, J.; Deng, S.; Lisen, L.; Song, Q.; Ding, J.; Wang, S. Association between air pollution-cold wave sequential events and ischaemic stroke incidence among elderly adults in Tianjin, China: a retrospective cohort study. BMJ Open. 2025, 15, e096297. [Google Scholar] [CrossRef]
- Cassavaugh, J.; Longhi, M.S.; Robson, S.C. Impact of Estrogen on Purinergic Signaling in Microvascular Disease. Int J Mol Sci. 2025, 26, 2105. [Google Scholar] [CrossRef]
- Luo, C.; Du, J.; Cuker, A.; Lautenbach, E.; Asch, D.A.; Poland, G.A.; Tao, C.; Chen, Y. Comparability of clinical trials and spontaneous reporting data regarding COVID-19 vaccine safety. Sci Rep. 2022, 12, 10946. [Google Scholar] [CrossRef]
- Anastasiou, T.; Sanidas, E.; Lytra, T.; Mimikos, G.; Gogas, H.; Mantzourani, M. Update on Thromboembolic Events After Vaccination Against COVID-19. Vaccines (Basel). 2025, 13, 833. [Google Scholar] [CrossRef] [PubMed]
- Joy, M.; Agrawal, U.; Fan, X.; Robertson, C.; Anand, S.N.; Ordonez-Mena, J.; Byford, R.; Goudie, R.; Jamie, G.; Kar, D.; Williams, J.; Marsden, G.L.; Tzortziou-Brown, V.; Sheikh, S.A.; Hobbs, F.D.R.; de Lusignan, S. Thrombocytopenic, thromboembolic and haemorrhagic events following second dose with BNT162b2 and ChAdOx1: self-controlled case series analysis of the English national sentinel cohort. Lancet Reg Health Eur. 2023, 32, 100681. [Google Scholar] [CrossRef] [PubMed]
- Khan, G.A.; Huwaikem, M.; Chowdhury, K.; Albugami, H.F.; Ghosh, A. The Role of Sterile Inflammation in Thrombosis: Consequences for Cardiovascular Disease and COVID-19. Mediators Inflamm. 2025, 2025, 8054886. [Google Scholar] [CrossRef]
- Prakash, S.; Choudhury, P.; Bisht, S. Diabetic cardiomyopathy and COVID-19: intersecting pathways and amplified cardiovascular risk. Front Pharmacol. 2025, 16, 1683159. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Total number of thrombotic events, stratified by gender (W, women; M, men), trimester, and polypharmacy group (0, 1, 2–4, 5–7, or ≥8 chronic treatments [nT]), from the beginning of the pandemic in March 2020 (the first column represents only one month) to March 2025.
Figure 1.
Total number of thrombotic events, stratified by gender (W, women; M, men), trimester, and polypharmacy group (0, 1, 2–4, 5–7, or ≥8 chronic treatments [nT]), from the beginning of the pandemic in March 2020 (the first column represents only one month) to March 2025.
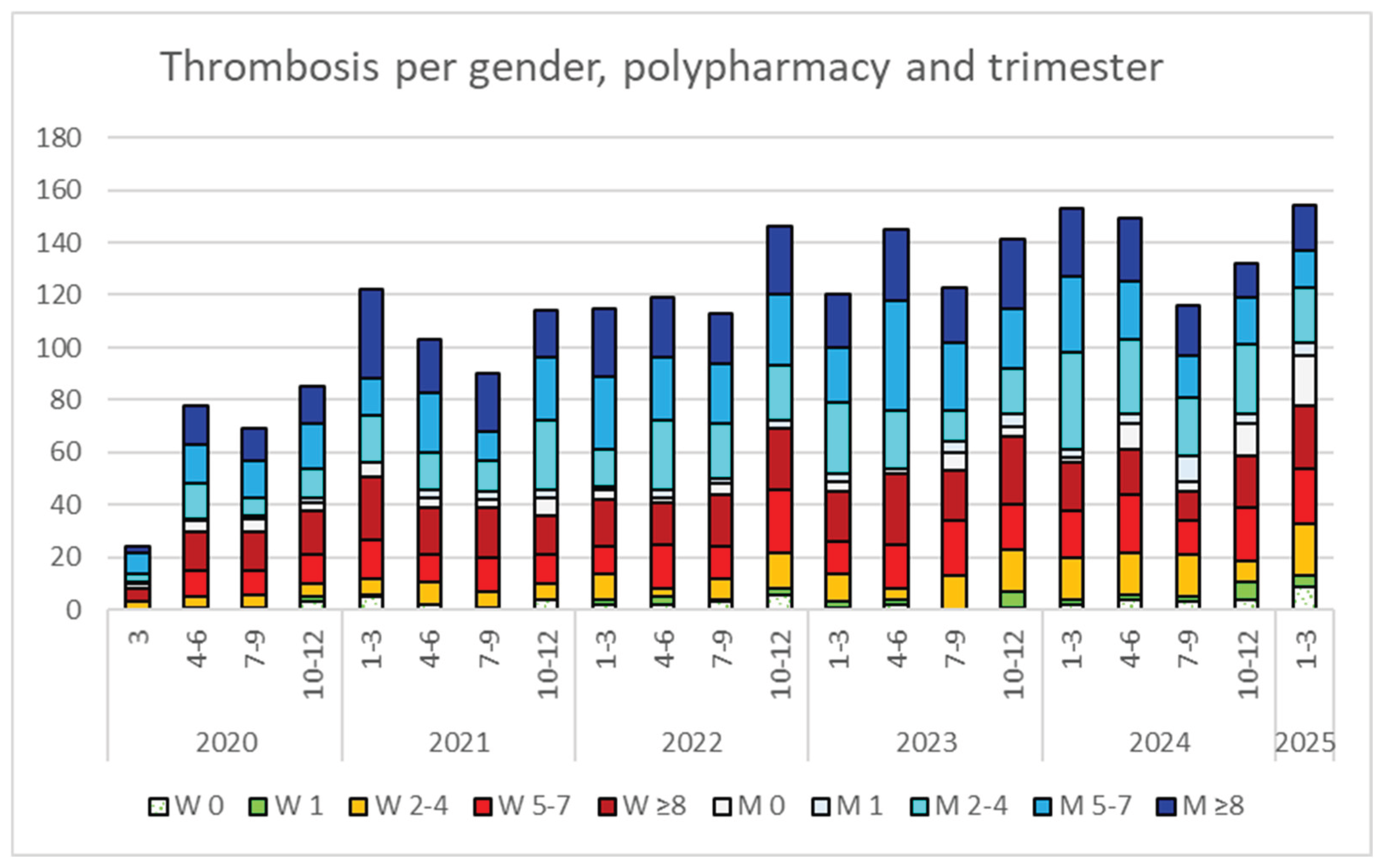
Figure 2.
Total number of hospital admissions stratified by gender (W, women; M, men), trimester, and polypharmacy group (0, 1, 2–4, 5–7, or ≥8 chronic treatments [nT]) from March 2020 to March 2025.
Figure 2.
Total number of hospital admissions stratified by gender (W, women; M, men), trimester, and polypharmacy group (0, 1, 2–4, 5–7, or ≥8 chronic treatments [nT]) from March 2020 to March 2025.
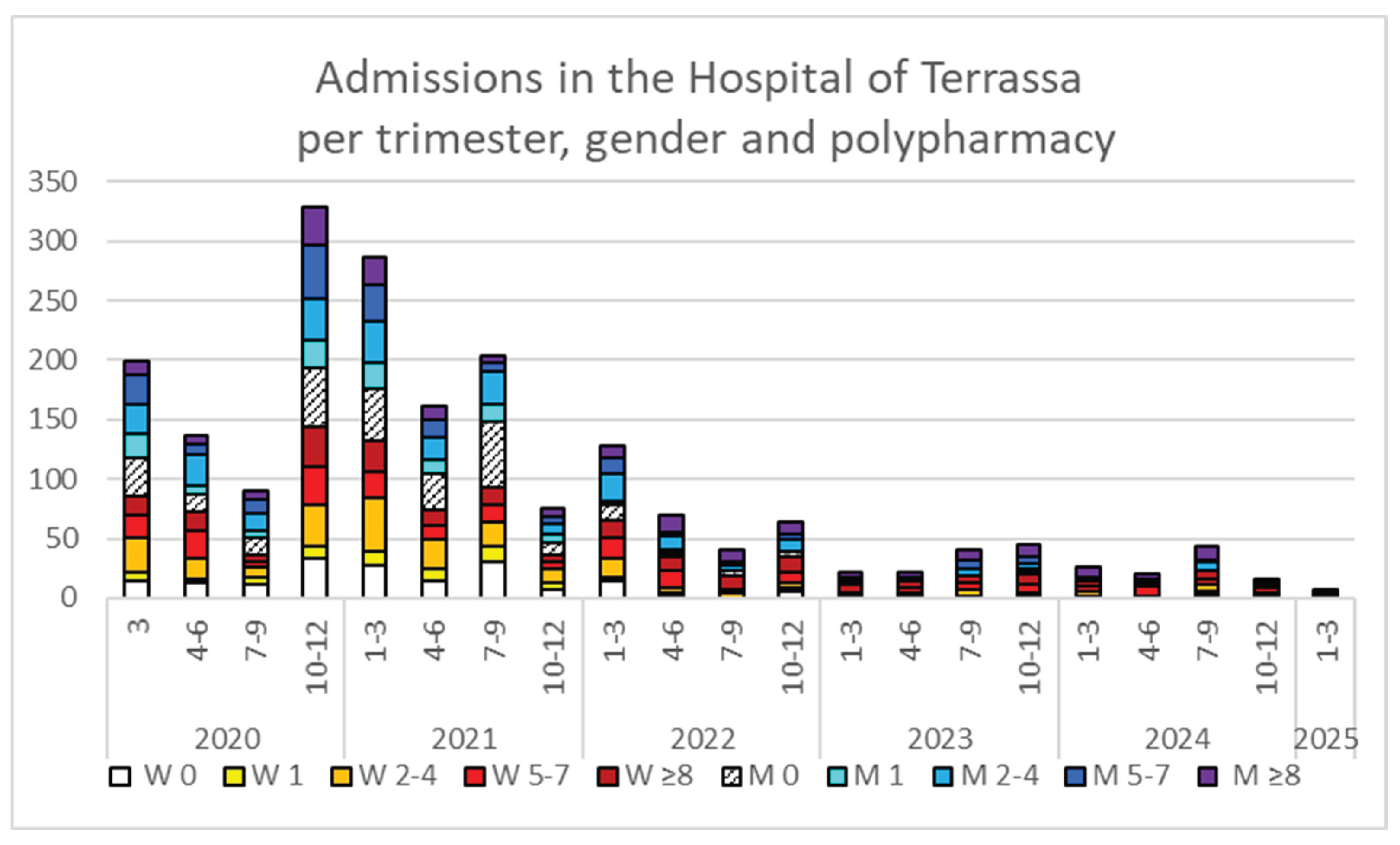
Figure 3.
Total number of thrombotic events in relation to vaccination status and age over or below 60 years old.
Figure 3.
Total number of thrombotic events in relation to vaccination status and age over or below 60 years old.
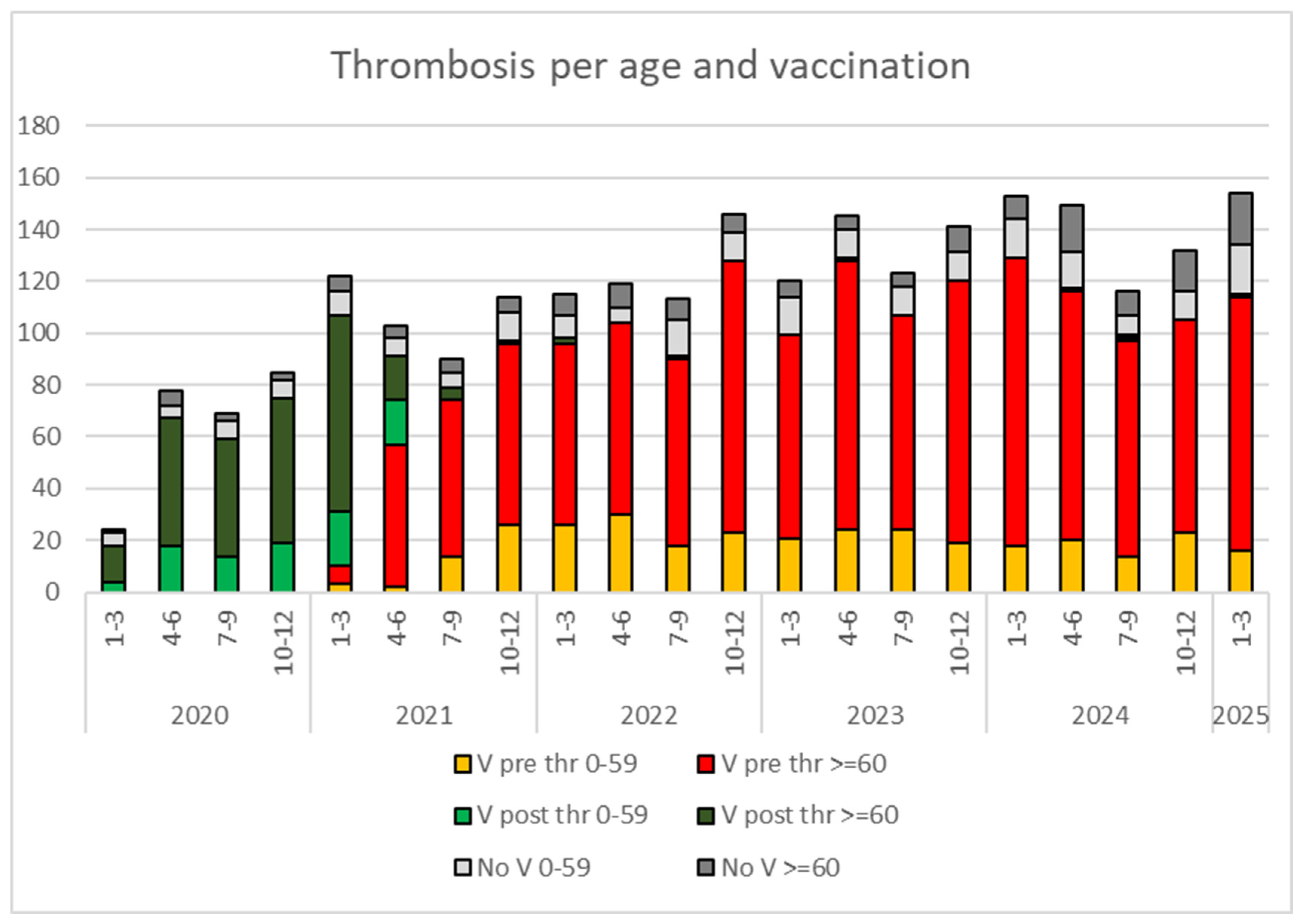
Figure 4.
SARS-CoV-2 variant detected prior to the thrombosis. The first number in each label indicates the year in which the variant appeared. The first two waves (in reddish tones) correspond to specific Spanish variants, while Alpha (orange) emerged at the end of 2020. Transitional periods between variants, before the next one becomes predominant, are shown as dotted, borderless columns. The Delta variant is shown in yellow, while the various Omicron variants appear in a green scale (2022), brown (2023), or blue-gray (2024). Note the reduced number of detected infections for variants that appeared after the end of full suspicion-based diagnoses in March 2022 (after Omicron 21K, which was predominant in the first trimester of 2022).
Figure 4.
SARS-CoV-2 variant detected prior to the thrombosis. The first number in each label indicates the year in which the variant appeared. The first two waves (in reddish tones) correspond to specific Spanish variants, while Alpha (orange) emerged at the end of 2020. Transitional periods between variants, before the next one becomes predominant, are shown as dotted, borderless columns. The Delta variant is shown in yellow, while the various Omicron variants appear in a green scale (2022), brown (2023), or blue-gray (2024). Note the reduced number of detected infections for variants that appeared after the end of full suspicion-based diagnoses in March 2022 (after Omicron 21K, which was predominant in the first trimester of 2022).
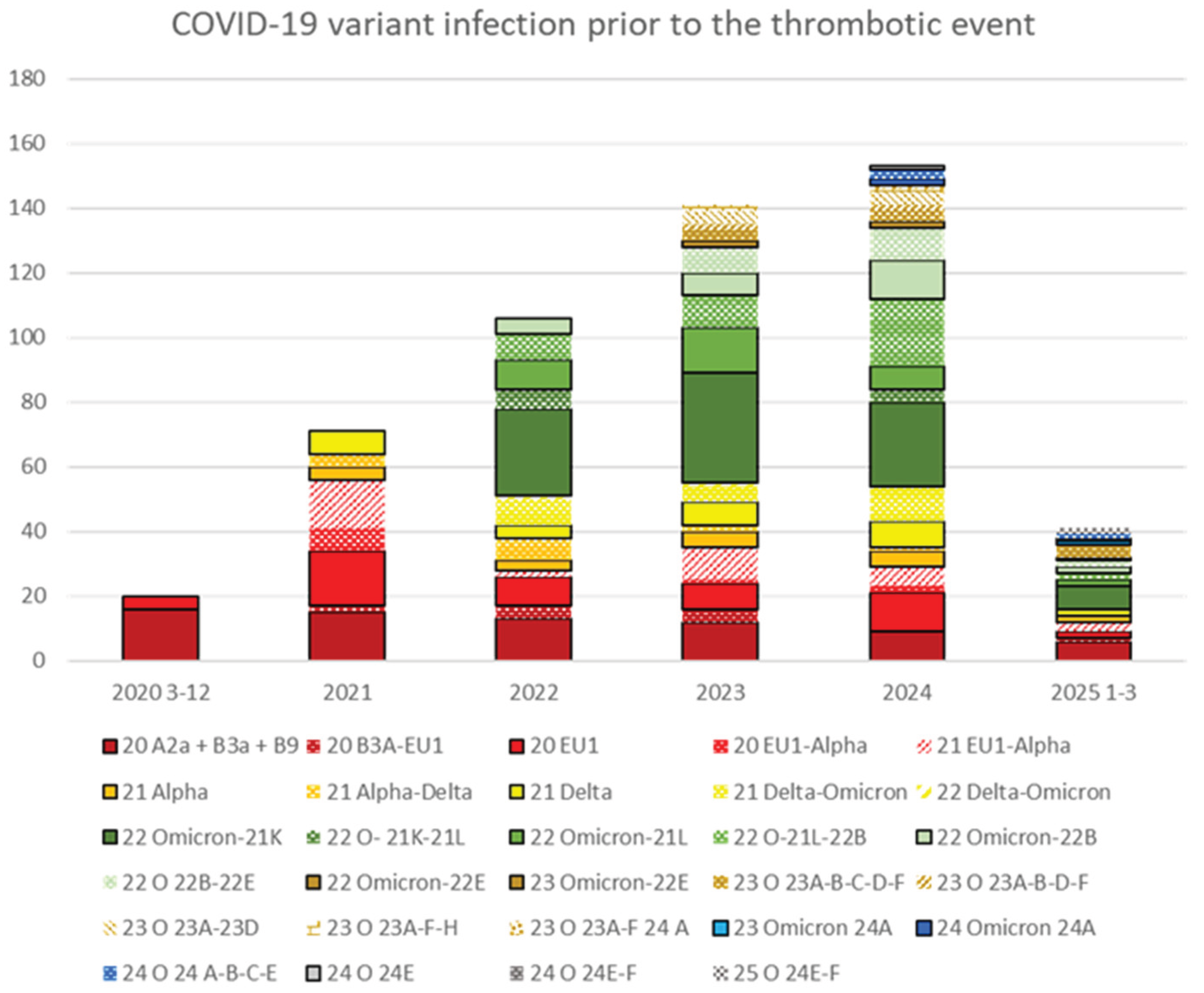

Table 1.
Analysis of Long COVID (LC) in relation to vaccination status and number of SARS-CoV-2 infections among patients on chronic medication. Statistical comparisons are shown between groups receiving antihistamine treatment (AntiHm) or not (No AntiHm), stratified by whether vaccination occurred before (V pre-inf) or after (V post-inf) the first infection. A more detailed analysis, stratified by increasing number of chronic medications, is provided in Supplementary Material S1.
Table 1.
Analysis of Long COVID (LC) in relation to vaccination status and number of SARS-CoV-2 infections among patients on chronic medication. Statistical comparisons are shown between groups receiving antihistamine treatment (AntiHm) or not (No AntiHm), stratified by whether vaccination occurred before (V pre-inf) or after (V post-inf) the first infection. A more detailed analysis, stratified by increasing number of chronic medications, is provided in Supplementary Material S1.
| No AntiHm | AntiHm | OR No AntiHm/ | p | |||||
| V n inf | inf no LC | LC | % | inf no LC | LC | % | /antiHm | (1-2 tailed) |
| V, inf? ? | 30253 | 26 | 0.1% | 3590 | 11 | 0.3% | ||
| No V, inf? | 13079 | 12 | 0.1% | 1782 | 0.0% | |||
| 1 | ||||||||
| V preinf | 9806 | 51 | 0.5% | 1526 | 12 | 0.8% | 0.66 | 0.09-0.19 |
| V post inf | 3478 | 94 | 2.7% | 556 | 13 | 2.3% | 1.16 | 0.31-0.63 |
| No V | 4786 | 42 | 0.9% | 794 | 6 | 0.8% | 1.16 | 0.36-0.73 |
| 2 | ||||||||
| V preinf | 839 | 7 | 0.8% | 152 | 0.0% | |||
| V post inf | 808 | 34 | 4.2% | 158 | 9 | 5.7% | 0.74 | 0.21-0.42 |
| No V | 485 | 8 | 1.6% | 115 | 2 | 1.7% | 0.95 | 0.48-0.96 |
| ≥3 | ||||||||
| V preinf | 77 | 2 | 2.6% | 18 | 0.0% | |||
| V post inf | 144 | 9 | 6.3% | 22 | 0.0% | |||
| No V | 49 | 5 | 10.2% | 10 | 0.0% |
Table 2.
Absolute number of thrombotic events from March 1, 2020, to March 28, 2025, stratified by the number of chronic treatments (nT) in patients receiving acute antihistamine treatment without chronic therapies (AntiHm, nT=0) or those on chronic antihistamine regimens (AntiHm) versus those not on chronic antihistamines (NoAntiHm). Odds ratios (ORs) are detailed for calendar years with complete data and for subgroups with more than five events. Asterisks (*) indicate ratios that were statistically significant in both one- and two-tailed comparisons.
Table 2.
Absolute number of thrombotic events from March 1, 2020, to March 28, 2025, stratified by the number of chronic treatments (nT) in patients receiving acute antihistamine treatment without chronic therapies (AntiHm, nT=0) or those on chronic antihistamine regimens (AntiHm) versus those not on chronic antihistamines (NoAntiHm). Odds ratios (ORs) are detailed for calendar years with complete data and for subgroups with more than five events. Asterisks (*) indicate ratios that were statistically significant in both one- and two-tailed comparisons.
| Thrombosis | 2020 3-12 | 2021 | 2022 | 2023 | 2024 | 2025 1-3 | No Thrombosis Total general | |
| AntiHm/nT | 13 | 26 | 38 | 34 | 38 | 13 | 10253 | 10415 |
| 0 | 1639 | 1639 | ||||||
| 1 | 1 | 1 | 2005 | 2007 | ||||
| 2-4 | 3 | 9 | 6 | 2 | 10 | 1 | 3878 | 3909 |
| 5-7 | 1 | 4 | 14 | 14 | 13 | 5 | 1629 | 1680 |
| ≥8 | 9 | 12 | 18 | 18 | 14 | 7 | 1102 | 1180 |
| No AntiHm/nT | 243 | 403 | 455 | 495 | 512 | 141 | 179987 | 182236 |
| 0 | 18 | 31 | 23 | 21 | 41 | 28 | 117980 | 118142 |
| 1 | 8 | 9 | 17 | 22 | 33 | 9 | 19556 | 19654 |
| 2-4 | 48 | 88 | 111 | 120 | 159 | 40 | 25608 | 26174 |
| 5-7 | 83 | 117 | 151 | 165 | 145 | 30 | 10639 | 11330 |
| ≥8 | 86 | 158 | 153 | 167 | 134 | 34 | 6204 | 6936 |
| No AntiHm≥1nT | 225 | 372 | 432 | 474 | 471 | 113 | 62007 | 64094 |
| Total general | 256 | 429 | 493 | 529 | 550 | 154 | 190240 | 192651 |
| OR No AntiHm/AntiHm | ||||||||
| 2-4 | 1.5 | 2.8* | 9.0* | 2.4* | ||||
| 5-7 | 4.3* | 1.6 | 1.7* | 1.7 | ||||
| ≥8 | 2.2* | 1.4 | 1.6* | 1.6 | ||||
Table 3.
Number of thrombotic events in patients receiving at least one chronic treatment (≥1nT), categorized by antihistamine use (AntiHm or NoAntiHm groups). For clarity, statistically significant results (*) are shown only for the comparison of patients who were both infected and vaccinated prior to the thrombotic event.
Table 3.
Number of thrombotic events in patients receiving at least one chronic treatment (≥1nT), categorized by antihistamine use (AntiHm or NoAntiHm groups). For clarity, statistically significant results (*) are shown only for the comparison of patients who were both infected and vaccinated prior to the thrombotic event.
| No AntiHm ≥1nT |
AntiHm ≥1nT |
||||||
| OR (p) No AntiHm/Antihm |
|||||||
| V pre thr | V post thr | No thr | V pre thr | V post thr | No Thr | ||
| V | 1470 | 324 | 43834 | 123 | 21 | 5923 | |
| V preinf | 343 | 63 | 10376 | 39 | 7 | 1662 | |
| CoV | |||||||
| CoV pre Thr | 260 | 1 | 27 | 1.52 (0.01)* | |||
| CoV post thr | 83 | 62 | 12 | 7 | |||
| CoV No Thr | 10376 | 1662 | |||||
| V postinf | 100 | 60 | 4407 | 9 | 6 | 743 | |
| CoV | |||||||
| CoV pre Thr | 100 | 41 | 9 | 5 | 1.84 (0.03*) | ||
| CoV post thr | 19 | 1 | |||||
| CoV No Thr | 4407 | 743 | |||||
| No CoV | 1027 | 201 | 29051 | 75 | 8 | 3518 | 1.62 (0.00001)* |
| No V | Trh-18466 | Thr-2709 | |||||
| CoV | |||||||
| CoV pre Thr | 52 | 5 | 3.47 (p=0.10) | ||||
| CoV post thr | 20 | 1 | |||||
| CoV No Thr | 5303 | 921 | |||||
| No CoV | |||||||
| No Cov Thr | 221 | 12 | 2.53 (p=0.0006*) | ||||
| No CoV no Thr | 12870 | 1770 | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



