Submitted:
14 December 2025
Posted:
22 December 2025
You are already at the latest version
Abstract
A non-invasive therapeutic system and method for promoting redistribution of fat from visceral to subcutaneous compartments in a subject. An external applicator positioned over an abdominal region delivers combined mechanical stimulation, controlled thermal modulation, and neuro-adipose modulation under the control of a central controller. Mechanical oscillations and compressive forces mobilize visceral fat stores; dynamic heat-cool cycles modulate adipocyte metabolism and inflammatory signaling; and low-intensity neuro-adipose signals influence lipid storage pathways. The coordinated treatment protocol is designed to reduce high-risk visceral adiposity while enhancing storage of lipids in lower-risk subcutaneous adipose tissue. Sensors may provide feedback for safety and personalization, and an artificial intelligence algorithm may optimize treatment parameters based on subject-specific data and outcomes.
Keywords:
visceral adiposity
; fat redistribution
; mechanical stimulation
; thermal modulation
; neuromodulation
; artificial intelligence
; cardiometabolic risk
Introduction
Obesity represents a major global health burden, yet not all patterns of fat distribution carry equivalent metabolic risk [1]. Visceral adipose tissue (VAT), located deep within the abdominal cavity surrounding vital organs including the liver, pancreas, and intestines, is strongly associated with insulin resistance, non-alcoholic fatty liver disease, cardiovascular disease, type 2 diabetes, and increased overall mortality [1,2]. VAT directly correlates with hepatic steatosis, increased portal circulation of free fatty acids, and systemic inflammation [4].
In contrast, subcutaneous adipose tissue (SAT) beneath the skin, particularly in peripheral regions, is comparatively less harmful and may even serve as a protective metabolic buffer for lipid storage [2,5]. This distinction between high-risk visceral and relatively lower-risk subcutaneous depots highlights the importance of fat quality and distribution rather than total body weight alone [2].
Current Limitations and Unmet Need
Conventional weight-loss approaches focus on reducing total body weight or body mass index, without specifically targeting the distribution of fat between visceral and subcutaneous compartments [1]. Existing device-based therapies, such as cryolipolysis or radiofrequency, are typically designed to reduce local subcutaneous fat for cosmetic purposes and do not address the underlying metabolic risk associated with excessive visceral fat [3]. A critical gap exists: no dedicated systems currently aim to reduce visceral fat burden while intentionally preserving or augmenting subcutaneous fat as a safer storage compartment for lipids. This represents an unmet clinical need.
Emerging Mechanistic Insights
Emerging research suggests that mechanical stimuli, thermal modulation, and neuro-hormonal signaling can influence adipose tissue metabolism, including lipolysis, adipocyte differentiation, and lipid trafficking [6,7]. Electrical stimulation has been shown to promote lipolysis in human adipocytes through β-adrenergic signaling pathways [8]. Thermal cycling modulates heat shock protein expression and metabolic gene expression in adipocytes [9]. Sympathetic nervous system innervation of adipose tissue directly regulates lipid mobilization and storage capacity [10]. However, these insights have not been integrated into a coherent, non-invasive therapeutic device specifically designed to promote physiological redistribution of fat from visceral to subcutaneous depots as a strategy to lower cardiometabolic risk.
Proposed Solution
We propose a non-invasive therapeutic system that combines three synergistic modalities—directed mechanical stimulation, controlled thermal modulation, and neuro-adipose modulation—under intelligent control, with optional artificial intelligence-driven personalization, to achieve preferential mobilization of visceral fat while promoting safer storage in subcutaneous depots.
System Design and Architecture
Overview of the Therapeutic Approach
The system combines three principal modalities:
- Directed mechanical stimulation of abdominal tissues to mobilize visceral fat stores
- Controlled thermal modulation using alternating heat–cool cycles optimized to suppress visceral adipocyte activity and reduce inflammatory signaling
- Neuro-adipose modulation via low-intensity electrical or electromagnetic stimulation to shift lipid storage preference toward subcutaneous adipose tissue
External Applicator
The external applicator is configured as a belt, pad, or wrap that can be secured around the abdomen over regions of maximal visceral adiposity. The applicator provides a non-invasive interface between the therapeutic modules and the patient's abdominal tissues. It is designed for comfort, portability, and repeated daily use.
Mechanical Stimulation Module
The mechanical module includes one or more actuators, such as:
- Vibration motors (electromagnetic or piezoelectric)
- Linear actuators (for pulsatile compression)
- Pneumatic bladders (for distributed pressure patterns)
- Other transducers capable of delivering controlled oscillatory forces
The mechanical stimulation is configured to generate low-frequency tissue oscillations or compressive pulses that propagate into deeper visceral tissues [12]. The parameters of the mechanical signal—including frequency (typically 5–80 Hz), amplitude, duty cycle, and waveform—are selected to promote mobilization of lipids from visceral adipocytes while minimizing discomfort [13].
Mechanism of action: Mechanical oscillations induce mechanical stress on adipocytes, activating mechanotransduction pathways that promote lipid mobilization and release from visceral depots.
Thermal Modulation Module
The thermal module includes heating and/or cooling elements, such as:
- Peltier thermoelectric devices
- Resistive heating elements
- Circulating fluid pads
- Capacitive coupling elements
These elements are capable of delivering localized, dynamic thermal patterns to the treatment region. Alternating heat–cool cycles are programmed to modulate adipocyte metabolism, attenuate inflammatory signaling, and preferentially suppress lipogenesis in visceral fat [9]. Thermal parameters are chosen within safe limits (typically 15–42 °C at skin surface) to avoid tissue damage while achieving desired metabolic effects [14].
Mechanism of action: Heat activates thermogenic pathways and upregulates uncoupling protein 1 (UCP1) and other thermogenic genes. Cooling suppresses lipogenic enzyme expression and reduces metabolic activity in visceral adipocytes. Alternating cycles prevent adaptation and maximize metabolic perturbation.
Neuro-Adipose Modulation Module
The neuromodulation component may include:
- Surface electrodes (for transcutaneous stimulation)
- Capacitive coupling plates (for non-contact modulation)
- Low-intensity electromagnetic emitters (for deeper tissue penetration)
These elements are configured to deliver targeted signals that influence sympathetic and parasympathetic innervation of abdominal adipose tissue [10]. By adjusting signal characteristics—such as frequency, intensity, and pulse pattern—the system can bias adrenergic signaling to reduce lipid storage in visceral depots and promote uptake into subcutaneous adipocytes with a more favorable receptor profile [8].
Mechanism of action: Low-intensity electrical stimulation activates β₃-adrenergic receptors in brown adipocytes and induces lipolysis via the cAMP-PKA pathway [7]. Electromagnetic fields modulate sympathetic tone and enhance catecholamine sensitivity in target adipose tissues.
Sensors and Monitoring
The device may further include sensors to monitor:
- Skin temperature (thermistors or IR sensors)
- Tissue impedance (bioimpedance measurement)
- Heart rate and heart rate variability (ECG or PPG)
- Respiration (optical or pressure sensors)
- Other physiological parameters
These sensors provide feedback to the controller to ensure that mechanical, thermal, and neuromodulation signals remain within safe and effective ranges. Imaging-based assessments of visceral fat, such as ultrasound or MRI performed separately, may be used to calibrate and evaluate treatment response over time [15].
Central Controller with Optional Artificial Intelligence
A microcontroller or embedded processor coordinates the three stimulation modalities according to predefined protocols. In some embodiments, an artificial intelligence (machine learning) algorithm is used to adapt stimulation patterns based on input data, including:
- Patient-specific visceral fat distribution (baseline imaging)
- Treatment history (previous sessions and responses)
- Real-time physiological responses during sessions
- Metabolic biomarkers
The artificial intelligence model may suggest optimized treatment profiles to maximize visceral fat mobilization while supporting increased subcutaneous lipid storage [11]. Machine learning algorithms (e.g., neural networks or ensemble methods) can be trained on historical patient cohorts to predict optimal parameter sets for new patients.
Treatment Method and Clinical Protocol
Patient Selection and Baseline Assessment
Suitable candidates are adults with documented visceral obesity (VAT area >100 cm2 on CT or equivalent ultrasound measurement) and associated metabolic risk factors (insulin resistance, dyslipidemia, or prediabetes) [4]. Baseline assessments include:
- Abdominal imaging (CT, MRI, or high-resolution ultrasound)
- Metabolic profiling (glucose, insulin, lipid panel, inflammatory markers)
- Cardiovascular risk assessment
- Body composition analysis
Treatment Session Protocol
- Positioning: Device is applied to the abdomen and secured in place.
- Parameter Selection: Clinician or artificial intelligence algorithm recommends treatment profile based on patient data.
- Mechanical Stimulation Phase: Low-frequency oscillations delivered for 10–15 minutes (e.g., 20–50 Hz, 1–5 mm amplitude).
- Thermal Modulation Phase: Alternating heat–cool cycles (e.g., 38 °C for 5 min, 20 °C for 5 min) repeated 3–4 times.
- Neuro-Adipose Modulation Phase: Concurrent or sequential low-intensity electrical stimulation (e.g., 10–100 μA, 10–50 Hz).
- Monitoring: Real-time sensor feedback ensures safety and efficacy.
- Session Duration: Typically 30–60 minutes per session.
Treatment Schedule
- Frequency: 3–5 sessions per week initially, adjustable based on response
- Duration: 8–12 weeks for initial assessment, with optional extension
- Frequency Modulation: Mechanical, thermal, and electrical parameters may be modulated weekly based on response and tolerance
Safety Considerations
All thermal, mechanical, and electrical parameters are maintained within established safe limits [14]:
- Skin temperature: <42 °C (to avoid thermal injury)
- Electrical current: <100 μA (to prevent sensation or tissue damage)
- Mechanical amplitude: <5 mm (to avoid muscle fatigue or discomfort)
- Duration: Monitored to prevent repetitive strain
Device Embodiments and Examples
Example 1: Abdominal Belt with Vibration and Peltier Elements
In one embodiment, the device is configured primarily as an abdominal belt containing arrays of vibration motors and Peltier elements. The neuromodulation is delivered via flexible electrodes embedded in the inner surface of the belt. The system operates at low mechanical frequencies (e.g., 20–50 Hz) and moderate thermal swings within a predefined safe range. Treatment parameters are manually configured by a clinician based on the patient's visceral fat index as determined by CT or ultrasound.
Key Features:
- Portable and easy to don/doff
- Manual parameter control by healthcare provider
- Suitable for clinical or home use
- Cost-effective manufacturing
Example 2: AI-Guided Compact Pad with Imaging Integration
In another embodiment, the device incorporates a more compact pad applied over the upper abdomen while the subject lies supine. Ultrasound imaging performed at baseline and at follow-up visits is used to quantify visceral fat thickness. An artificial intelligence model correlates the ultrasound measurements with session logs and metabolic biomarkers, progressively adjusting the mechanical and thermal protocols to enhance visceral fat reduction [11].
Key Features:
- Real-time imaging feedback
- Automated parameter optimization via artificial intelligence
- Personalized treatment protocols
- Integrated data logging and cloud connectivity
Example 3: Integrated Therapeutic Program
In yet another embodiment, the neuromodulation module is configured to deliver extremely low-intensity fields that primarily influence superficial nerve branches associated with adipose tissue, with the aim of modulating adipokine secretion and lipid trafficking pathways [10]. The device in this embodiment is integrated into a broader therapeutic program that includes dietary counseling, physical activity recommendations, and pharmacologic therapies, and the system tracks overall outcomes over several months [16].
Key Features:
- Multimodal treatment approach
- Integration with lifestyle and pharmacologic interventions
- Comprehensive health tracking
- Long-term outcome assessment
Advantages of the Invention
The system offers several advantages over conventional obesity treatments and body-contouring devices:
- Targets fat distribution, not just total weight: Focuses on the quality and location of adiposity rather than only the quantity of total body fat [2].
- Reduces high-risk visceral adiposity while preserving protective subcutaneous adipose tissue: Aims to reduce high-risk visceral adiposity while preserving or enhancing subcutaneous lipid buffering capacity [2].
- Combines synergistic modalities: Mechanical, thermal, and neuromodulation modalities work in a coordinated manner for additive and synergistic effects [17].
- Personalized and adaptive: Utilizes feedback and optional artificial intelligence-based personalization to tailor treatment to individual patients and their response trajectories [11].
- Non-invasive and integrable: Non-invasive and potentially suitable as an adjunct to lifestyle interventions, pharmacologic therapies, or bariatric procedures [16].
- Novel paradigm: Represents a paradigm shift from weight-centric to adiposity-quality-centric obesity management.
Mechanism of Action and Physiologic Rationale
The combined effect of the three modalities is to:
- Promote lipolysis and efflux of lipids from visceral depots
- Encourage uptake and safe storage of lipids within subcutaneous adipocytes
- Reduce visceral fat burden and associated metabolic risk
- Achieve results without relying solely on overall weight loss
By focusing on redistributing fat from high-risk visceral compartments to lower-risk subcutaneous compartments, this approach provides a novel therapeutic paradigm that addresses the quality and distribution of adiposity rather than quantity alone [2].
Discussion
The pathophysiology of visceral obesity is multifactorial, involving not only the quantity of fat but also its anatomical distribution and metabolic characteristics [1,2]. VAT is metabolically active, produces pro-inflammatory adipokines, and is strongly linked to insulin resistance and multiple cardiometabolic disorders. In contrast, SAT, particularly in lower-body regions, has been suggested to have a more favorable metabolic profile and may even exert protective effects [2,5].
Current therapeutic approaches have largely ignored the opportunity to selectively target VAT mobilization while promoting safer lipid storage in subcutaneous depots. The integrated system described herein addresses this gap by leveraging multiple, mechanistically complementary stimulation modalities—mechanical, thermal, and neuro-adipose—in a coordinated, feedback-controlled manner.
The mechanical component activates mechanotransduction pathways known to influence adipocyte function [12,13]. The thermal component exploits the temperature sensitivity of adipocyte metabolism and inflammatory gene expression [9,14]. The neuromodulation component targets sympathetic innervation and β-adrenergic signaling, which are central regulators of lipid mobilization and storage [7,8,10]. Together, these modalities are hypothesized to create an environment conducive to preferential mobilization of VAT and preferential storage of mobilized lipids in SAT.
The incorporation of artificial intelligence and real-time sensor feedback allows for personalization and dynamic adaptation of the treatment protocol based on individual patient characteristics and treatment response. This represents an advance over static, one-size-fits-all approaches and aligns with contemporary trends in precision medicine.
Limitations of the current work include the need for prospective, randomized controlled trials to establish efficacy and safety in human subjects, detailed characterization of the signaling pathways activated by each modality in vivo, and optimization of device design and treatment parameters. Future work should also address long-term durability of effects, integration with lifestyle and pharmacologic interventions, and cost-effectiveness analysis.
Conclusion
We present a novel, non-invasive therapeutic system that integrates mechanical stimulation, thermal modulation, and neuro-adipose modulation to selectively reduce visceral adiposity and promote redistribution of lipids toward subcutaneous depots. This approach addresses a significant unmet clinical need in obesity management by focusing on fat quality and distribution rather than weight alone, with potential applications in cardiometabolic risk reduction. Further clinical investigation is warranted to establish safety, efficacy, and optimal use in the management of visceral obesity.
Patent Claims (Supplementary)
Claim 1 (Independent Claim – Device): A non-invasive therapeutic system for redistributing fat from visceral to subcutaneous compartments in a subject, the system comprising:
- An external applicator configured to be positioned over an abdominal region of the subject
- A mechanical stimulation module disposed in the applicator and configured to deliver controlled mechanical oscillations or compressive forces to abdominal tissues (frequency range: 5–80 Hz)
- A thermal modulation module disposed in the applicator and configured to deliver controlled heating and cooling cycles to the abdominal region (temperature range: 15–42 °C)
- A neuro-adipose modulation module configured to deliver low-intensity electrical or electromagnetic signals to influence adipose-related neural pathways (current: <100 μA)
- A controller configured to coordinate operation of the mechanical stimulation module, the thermal modulation module, and the neuro-adipose modulation module according to a treatment protocol designed to reduce visceral fat burden and promote storage of lipids in subcutaneous adipose tissue
Claim 2: The system of claim 1, wherein the mechanical stimulation module comprises one or more vibration actuators or pneumatic bladders configured to generate low-frequency oscillations in the range of about 5 Hz to about 80 Hz.
Claim 3: The system of claim 1, wherein the thermal modulation module comprises one or more Peltier elements configured to produce alternating heat–cool cycles within a predetermined safe temperature range (15–42 °C at skin surface).
Claim 4: The system of claim 1, wherein the neuro-adipose modulation module comprises surface electrodes or capacitive coupling elements configured to deliver low-intensity signals adapted to modulate adrenergic signaling in visceral and subcutaneous adipose tissues.
Claim 5: The system of claim 1, further comprising one or more sensors selected from the group consisting of temperature sensors, tissue impedance sensors, heart rate sensors, and respiration sensors, the sensors being configured to provide real-time feedback to the controller for adjusting the treatment protocol.
Claim 6: The system of claim 1, wherein the controller comprises an artificial intelligence module configured to adapt one or more parameters of the mechanical, thermal, or neuro-adipose modulation based on subject-specific data including visceral fat measurements, treatment history, and prior treatment responses.
Claim 7 (Independent Claim – Method): A method of treating visceral obesity in a subject, the method comprising:
- Positioning an external applicator over an abdominal region of the subject
- Applying, via the applicator, mechanical stimulation to the abdominal region to mobilize visceral fat stores (5–80 Hz oscillations)
- Applying, via the applicator, controlled thermal modulation comprising heating and cooling cycles (alternating 38 °C and 20 °C)
- Applying, via the applicator, neuro-adipose modulation to influence adipose-related neural signaling (<100 μA electrical current)
- Repeating the applying steps over a plurality of treatment sessions (3–5 per week for 8–12 weeks) to reduce visceral fat burden while promoting redistribution of lipids to subcutaneous adipose tissue
Claim 8: The method of claim 7, further comprising monitoring one or more physiological parameters (temperature, impedance, heart rate, respiration) during the applying steps and adjusting the mechanical, thermal, or neuro-adipose modulation based on the monitored parameters in real-time.
Claim 9: The method of claim 7, wherein the treatment protocol is personalized using an artificial intelligence algorithm trained on data linking modulation parameters, visceral fat changes, and metabolic outcomes, thereby optimizing therapeutic efficacy for each individual subject.
Figure Legends and Captions
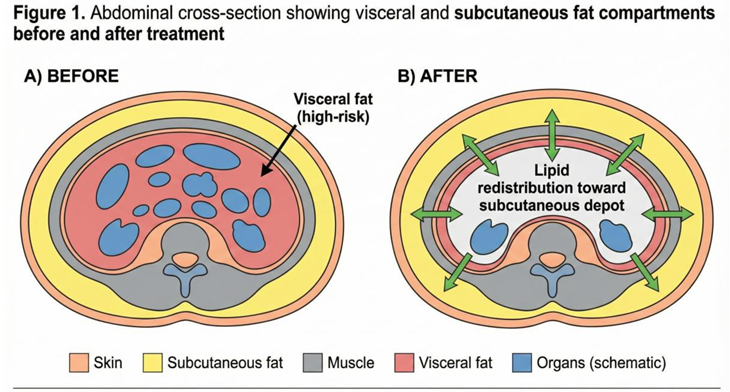
Figure 1: Schematic cross-sectional view of the abdomen showing visceral and subcutaneous fat compartments before (A) and after treatment (B) using the system of the invention. Panel A illustrates the enlarged visceral adipose depot surrounding intra-abdominal organs and the subcutaneous adipose layer. Panel B shows the reduced visceral adiposity and enhanced subcutaneous lipid storage following treatment, with arrows indicating lipid redistribution pathways.
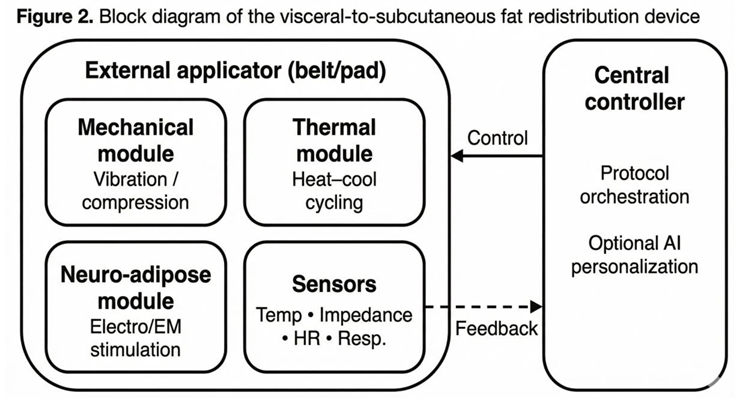
Figure 2: Block diagram of the visceral-to-subcutaneous fat redistribution device. The external applicator (belt/pad) incorporates three principal stimulation modules (mechanical, thermal, and neuro-adipose) plus integrated sensors. All components are coordinated by a central controller with optional artificial intelligence capabilities. Feedback from sensors enables real-time protocol adjustment. The system operates autonomously or under clinician oversight.
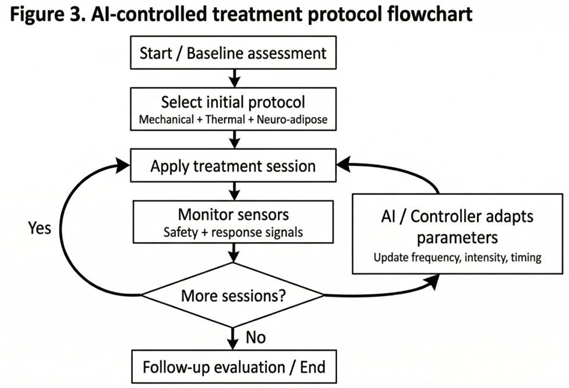
Figure 3: Flowchart of the AI-controlled treatment protocol for visceral fat redistribution. The workflow begins with baseline assessment (imaging and metabolic profiling), proceeds through protocol selection and iterative treatment sessions, and incorporates real-time sensor monitoring and AI-driven parameter adaptation. The cycle continues for 8–12 weeks with periodic imaging evaluation to assess visceral fat reduction and metabolic improvement.
Glossary of Terms
| Term | Definition |
| Adipocyte | Specialized cell that stores energy in the form of triglycerides; primary cell type of adipose tissue |
| Adipokines | Bioactive peptides secreted by adipose tissue that regulate metabolism, inflammation, and immune function |
| Adiposity | The state of being obese; the degree of body fat |
| Alternating heat–cool cycles | Repetitive heating and cooling patterns applied to tissue to modulate metabolic activity |
| Applicator | External device (belt, pad, or wrap) designed to deliver therapeutic stimuli to the abdomen |
| Cardiometabolic risk | Integrated risk for cardiovascular disease and metabolic disorders (diabetes, dyslipidemia) |
| Cryolipolysis | Non-invasive fat reduction technique using controlled cooling |
| Hepatic steatosis | Accumulation of triglycerides within hepatocytes; fatty liver disease |
| Lipolysis | Breakdown of triglycerides into free fatty acids and glycerol |
| Lipogenesis | Synthesis and storage of lipids within adipocytes |
| Mechanotransduction | Process by which mechanical stimuli are converted into biochemical signals |
| Metabolic risk | Risk of developing metabolic disorders based on body composition and biomarkers |
| Neuromodulation | Therapeutic alteration of nerve activity through targeted electrical or electromagnetic stimulation |
| Non-invasive | Medical treatment that does not involve penetrating the skin or body cavity |
| Peltier element | Thermoelectric device that can heat or cool based on applied electrical current |
| Subcutaneous adipose tissue (SAT) | Fat depot located beneath the skin; generally considered lower metabolic risk |
| Visceral adipose tissue (VAT) | Fat depot located within the abdominal cavity surrounding organs; associated with higher metabolic risk |
| β-adrenergic signaling | Cellular signaling pathway activated by norepinephrine and epinephrine that promotes lipolysis |
References
- Shetty, S; Chopra, A. Visceral adiposity and cardiometabolic risk. Am J Clin Nutr. 2025, 121(4), 743–756. [Google Scholar] [CrossRef]
- Cesaro, A; Bianconi, V; Grandi, AM; et al. Visceral adipose tissue and residual cardiovascular risk. Front Cardiovasc Med. 2023, 10, 1187735. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Castell, M; Boswell-Ruys, E; Sanchez-Niño, MD; Ortiz, A. Estimated visceral adiposity is associated with risk of cardiometabolic conditions: Insights from the Barcelona cohort. Sci Rep. 2021, 11(1), 8847. [Google Scholar] [CrossRef]
- Neeland, IJ; Poirier, P; Després, JP. Cardiovascular and metabolic heterogeneity of obesity: Pathophysiologic insights. J Am Coll Cardiol. 2018, 72(17), 2093–2109. [Google Scholar] [CrossRef]
- Porter, SA; Massaro, JM; Hoffmann, U; et al. Abdominal subcutaneous adipose tissue: A protective fat depot? Diabetes Care 2009, 32(6), 1068–1075. [Google Scholar] [CrossRef] [PubMed]
- Zeng, W; Pirzgalska, RM; Pereira, MM; et al. Sympathetic neuro-adipose connections mediate leptin-driven lipolysis. Cell. 2015, 163(1), 84–94. [Google Scholar] [CrossRef] [PubMed]
- Gupta, RK; Arany, Z; Seale, P; Mepani, RJ. Transcriptional control of thermogenic program in adipocytes. Nat Rev Mol Cell Biol. 2010, 11(12), 855–867. [Google Scholar] [CrossRef]
- Kipnis, J; Cohen, H; Bergman, O; Szabó, G; Eisenbach, M. Effect of electrical stimulation on lipolysis of human white adipocytes. Int J Obes (Lond) 2011, 35(4), 525–532. [Google Scholar] [CrossRef]
- Scheele, C; Nielsen, S; Pedersen, BK. RIP140 as a regulator of metabolic flexibility. Int J Obes (Lond) 2012, 36(2), 200–206. [Google Scholar] [CrossRef]
- Bartness, TJ; Liu, X; Shanley, SA; Dohm, GL. Cold-induced mobilization of lipid metabolism in adipose tissue of the Syrian hamster. Am J Physiol Regul Integr Comp Physiol. 2010, 296(2), R383–R393. [Google Scholar] [CrossRef]
- LeCun, Y; Bengio, Y; Hinton, GE. Deep learning. Nature 2015, 521(7553), 436–444. [Google Scholar] [CrossRef] [PubMed]
- Sigrist, RM; Liau, J; Kaffas, AE; Chammas, MC; Willmann, JK. Ultrasound elastography: Review of techniques and clinical applications. Theranostics 2017, 7(5), 1303–1329. [Google Scholar] [CrossRef] [PubMed]
- Zuo, H; Lin, T; Wang, X; Wan, G; Tan, Y. Mechanisms of mechanical stimulation-induced adipogenesis and anti-adipogenesis. J Cell Physiol. 2019, 234(11), 19631–19644. [Google Scholar] [CrossRef]
- Pennes, HH. Analysis of tissue and arterial blood temperatures in the resting human forearm. J Appl Physiol. 1948, 1(2), 93–122. [Google Scholar] [CrossRef] [PubMed]
- Karastergiou, K; Semple, RK; Kaur, P; Gopaul, NK. Comprehensive assessment of the role of visceral adiposity in the development of non-alcoholic fatty liver disease. Hepatology 2011, 53(4), 1164–1174. [Google Scholar] [CrossRef]
- Apovian, CM; Aronne, LJ; Bessesen, DH; et al. Pharmacological management of obesity: An Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2015, 100(2), 342–362. [Google Scholar] [CrossRef]
- Steinemann, E; Schmid, A; Kanaoka, Y. Combined multi-modal stimulation for metabolic tissue remodeling. Adv Mater Technol. 2018, 3(8), 1700258. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



