
Submitted:
11 December 2025
Posted:
12 December 2025
You are already at the latest version
Abstract
Desmoplastic melanoma (DM) is a rare, aggressive melanoma subtype with high local recurrence rates (20-60%) following surgical excision. This systematic review evaluated the efficacy of adjuvant radiotherapy (RT) in improving local control and survival outcomes in DM patients. Following Preferred reporting items for systematic review and meta-analyses (PRISMA) guidelines, we searched PubMed/MEDLINE, ScienceDirect, Scopus, CINAHL, and EBSCO databases from inception through December 2025.. Thirteen studies (10 retrospective cohorts, 3 prospective trials) met the inclusion criteria. quality assessment using JBI tools revealed 69% high quality and 31% moderate quality studies. Adjuvant RT significantly reduced local recurrence rates from 17.2% (surgery alone) to 7.6% (surgery plus RT), representing a 56% relative risk reduction. All hypofractionated RT (e.g. 30 Gy/5 fractions) achieved comparable local control rates (90-95% at 5 years). High-risk features including positive margins, Breslow depth ˃4 mm, and neurotropism identified patients deriving greatest benefits from RT. Adjuvant radiotherapy significantly improves local control in DM following surgical excision and should be considered standardized of care for high-risk patients. Future randomized trials are needed to established definitive treatment.

Keywords:
desmoplastic melanoma
; adjuvant radiotherapy
; local control
; surgical excision
; resection margin
; neurotropism
; local recurrence
; survival
; spindle cell melanoma
1. Introduction
Desmoplastic melanoma (DM) is a rare and diagnostically challenging histological subtype of cutaneous melanoma, accounting for 1-4% of all melanoma cases [1,2,3]. First described by Conley in 1971, DM is characterized by malignant spindle cells within a prominent fibro-collagenous stroma and exhibits distinct clinicopathological features [4]. This subtype predominantly affects older males (male to female ratio 2.5;1) and arises in chronically sun exposed surfaces with the head and neck region accounting for 40-55% of cases [5,6,7].
DM presents significant diagnostic challenges due to its amelanotic, scar-like appearance, frequently mimicking benign lesions such as dermatofibroma or scar tissue [8]. This lead to delays in diagnosis and greater Breslow thickness at presentation [9]; Swedish registry data demonstrated a median thickness of 4.0 mm for DM compared with lower values for other melanoma subtypes [2]. Hallmark features for DM are neurotropism and propensity for perineural invasion, which complicate complete surgical clearance, particularly in the head and neck [10,11]. Molecularly, DM exhibits low BRAF (define full name) mutation frequency but high prevalence of NF1 (define full name) loss of function mutations and an extraordinarily high tumor mutational burden (median 62 mutation /megabase), with implications for immunotherapy responsiveness [12].
Wide local excision remains the treatment cornerstone [13]; however, DM exhibits substantially higher local recurrence rates (20-60%) compared with conventional melanomas (˂5%) [14,15]. A recent metal-analysis reported 21% overall local recurrence following excision escalating to 49% with positive margins, with neurotropism conferring 1.79-fold increased recurrence risk [16]. Pure DM (≥90% desmoplastic histology) demonstrated elevated local recurrence risk but paradoxically lower sentinel lymph node metastasis rates (3-7%) compared with mixed variants [17,18].
Given these high recurrence rates, adjuvant RT has emerged as a strategy to improve local control [19,20]. Retrospective series from major cancer centers report 5- years local control rates of 91-95% with adjuvant RT versus 74-76% with surgery alone[21,22]. The prospective NCCTG N0275 trial demonstrated a 2-years local recurrence rate of only 10% with hypofractionated RT (30 Gy/5 fractions) and acceptable toxicity [23]. However, current guidelines remain equivocal, recommending RT may be considered without definitive selections criteria [24].
The therapeutic landscape is continuously evolving with immune checkpoint inhibitors demonstrating remarkable efficacy in DM (70% response rate to anti-PD-1 therapy), attributed to its high mutational burden [25,26], however, optimal integration of RT and immunotherapy remains undefined [27].
Despite accumulating evidence, the existing literature is predominantly retrospective with heterogenous study designs, variable RT dose-fractionation schemes, and inconsistent outcome definitions [27,28]. Critically, the impact on survival endpoints remains controversial, with diverging conclusion across studies [29,30]. The sole randomized trial (RTN2) was terminated prematurely due to poor accrual. Local recurrence in DM carries an increased risk of distant metastatic progression [31,32].
The Research questions is: Among patients with desmoplastic melanoma treated with surgery, does adjuvant radiotherapy improve local control and survival compared with surgery alone? This systematic review aims to comprehensively evaluate the role of adjuvant RT following surgical excision of DM, focusing on local control and survival outcomes. By synthesizing available evidence, this review seeks to clarify the therapeutic role of postoperative RT, identify knowledge gaps, and provide recommendations for clinical practices and future research
2. Materials and Methods
This systematic review has been conducted following the preferred reporting items for systematic reviews and meta-analyses (PRISMA) and synthesis without meta-analysis (SWiM) guidelines [33].
2.1. Data Sources and Search Strategy
This review was registered in the PROSPERO database (number pending at the time of submission of manuscript) for systematic reviews. Researches conducted an intensive search using PubMed/MEDLINE, ScienceDirect, Scopus, CINAHL, EBSCO databases. The search strategy meticulously followed PRISMA standards for systematic reviews, ensuring the highest quality of research, to examine the effectiveness of adjuvant radiotherapy after surgery in melanoma patients. Articles were searched from database since inception up until December 2025, with no restrictions on the publication date. A combination of keywords was used, including (“adjuvant radiotherapy “OR” radiation therapy” (AND (“desmoplastic melanoma” OR” spindle cell melanoma “) AND (“surgical excision” OR” wide local excision”) AND (“local control” OR “survival”). Although specific histological subtypes such as pure and mixed desmoplastic melanoma were not widely used as primary search terms, studies distinguishing between these subtypes were explicitly included to allow for a comprehensive subgroup analysis of RT efficacy based on tumor histology. Only English language studies were included. All non-English articles, review articles, abstract, and non-peer reviewed sources were excluded. A total of 1,031 records were identified after removing duplicates. These were screened based on title and abstracts. A total of 207 records were excluded for the following reasons: the study objective was not relevant based on the title of the abstract (n-= 137), redundant reports of the same study (n= 52), and one study was excluded due to unavailability of full text and a critical appraisal score below 50% based on the abstract alone (n=18), making it insufficient for inclusion. The remaining (n=177) full-text articles were assessed for eligibility, and 50 met the inclusion criteria for the initial screening. Following a detailed quality assessment and focused analysis with comprehensive radiotherapy outcome data and methodological rigor, 13 high quality studies were selected for the final systematic review and evidence synthesis.
2.2. Study Selection and Eligibility
The inclusion criteria were based on the PICO (Patient, Intervention, Comparison, Outcome) model. The population (P) consisted of adult patients (≥18 years) diagnosed with desmoplastic melanoma (DM) OR Neurotropic melanoma, validated by histopathological examination confirming the presence of desmoplasia or neurotropism. The intervention (I) involved surgical excision of the primary melanoma lesion followed by adjuvant RT as postoperative treatment. The outcomes (O) included the dose and timing of administrating RT, clinical improvements in local control, desmoplastic melanoma complications including local recurrence and regional node basin recurrence, distant metastasis rates, overall survival, disease-specific survival, and tests confirming improvement such as imaging studies and pathological assessments.
The timeframe spanned from database inception up to December 2025. Studies conducted among patients who received only chemotherapy alone, or only. Immunotherapy as single modality without radiotherapy, or only a standard single dose of radiotherapy without complete treatment course were excluded. Non-English publications, review articles without original data, and studies lacking specific outcomes data were excluded from this analysis.
2.3. Data Extraction and Synthesis
All relevant studies were selected based on inclusion and exclusion criteria (Figure 1). Two reviewers independently screened the title and abstracts of all identified articles. When title or abstracts did not provide sufficient detail, or disagreements among researcher arose, the full text was reviewed to determine the study eligibility. Any disagreements between reviewers were resolved through consensus or with input from a third reviewer.
Data were extracted using a standardized form that included study title, publication years, study design, sample size, patient demographics, tumor characteristics, treatment parameters, and main outcomes. According to PRISMA guidelines, we specifically sought outcomes data related to (1) the radiation dose regimen and fractionation schedule used in adjuvant RT treatment, (2) clinical improvements in local control particularly measured at standardized timepoints (2,3 and 5 years), (3) diagnostic assessments and prognostic indicators supporting treatment response evaluation, including pathological features, tumor characteristics (Clark level, Breslow depth, perineural invasion, resection margin status, and histological subtype), and (4) treatment outcomes such as local recurrence and distant metastasis, disease-specific survival and overall survival. Although not all studies reported on every outcome variable, we extracted all results that were compatible with the predefined domains and clinical relevance to adjuvant radiotherapy efficacy in desmoplastic melanoma.
When multiple results were presented (e.g., various radiations dose regimens, several follow up timepoints, or different outcome measures), we prioritized those that reflected clear evidence of therapeutic benefit form radiotherapy, particularly early and clinically significant improvements in local control compared to surgery alone. This method allowed us to compare findings consistently across heterogenous study designs and treatment protocols. Furthermore, due to the heterogeneity in study designs (retrospective cohorts, prospective studies clinical trials), sample size (ranging from small case series to large multi-institutional studies), radiation techniques (photons, electrons, protons, carbon ions), fractionation dosing), and outcomes measures reported, narrative synthesis rather than a meta-analysis was used to summarize and interpret the findings across studies. This qualitative approach enabled comprehensive evaluation of RT effectiveness, treatment related toxicity, and patient outcomes in the management of desmoplastic melanoma (Table 1).
3.4. Quality Assessment of Included Studies
Given the study designs (retrospective cohort, trial,), a formal Grading of Recommendations Assessment, Development and Evaluation (GRADE) assessment was not applicable; instead, methodological rigor was evaluated using the Joanna Briggs institute (JBI) critical appraisal tools. A summary of the quality assessment is presented in Table 2. Cohort studies were assessed using 11 questions, while experimental studies (randomized control trials and quasi-experimental) were evaluated using 13 and 9 questions respectively. Items were scored as “YES”,” NO”,” Unclear”, OR “Not applicable”. Studies with ≥80% positive scores were considered high quality, 50-79% moderate, and ˂50% low quality. Most included studies demonstrated moderate to high methodological quality.
3. Results
3.1. Characteristics of Included Study
The Systematic review included diverse range of study designs and clinical characteristics to comprehensively evaluate the efficacy of adjuvant RT in desmoplastic melanoma. Among the 13 included studies, 10 were retrospective cohort studies (77%) [19,20,21,22,28,35,36,37,38,40], and 3 were prospective clinical trials or prospective observational studies (23%) [23,31,41]. The studies were geographically diverse, with the majority from north America (8 studies, 62%)[19,21,22,23,28,35,37,38], Europe (1 study, 8%)[41], Asia (1 study, 8%) [40], and Australia/Oceania (3 studies,23%) [19,20,31], reflecting the global nature of melanoma research and treatment practices. The studies encompassed various health care settings, including academic medical centers (9 studies,69%) [19,20,21,22,31,35,38,40,41], specialized melanoma and cancer clinics (4 studies,31%) [23,28,36,37], highlighting the comprehensive nature of systematic review (Table 2).
3.2. Quality of Studies
Overall, most included primary research studies demonstrated moderate to high methodological quality according to JBI assessment criteria. Among the 10 retrospective cohort studies, 6 studies (60%) achieved high-quality scores (≥80%) [19,21,22,35,37,40], based on adequate documentation of patient’s selection, treatment parameters, radiotherapy dosing specifications, outcome measurement clarity, and appropriate follow -up durations ranging from 2 to 5 years. Four cohort studies (40%) [20,28,36,38], achieved moderate quality scores (50-79%) due to limited documentation of potential confounding factors or incomplete reporting of specific outcome data, though these studies still provided valuable clinical information on local recurrence rates and survival outcomes.
For the three prospective clinical trials, the rule phase II trial achieved high quality (95%) with comprehensive documentation of treatment protocols and outcomes. The Reijers (PRADO trial) achieved high quality (92%) as a well-designed prospective study with standardized response assessment and clearly defined primary and secondary endpoints [41]. The Pinkham Randomized trial achieved high quality (89%) based on JBI assessment criteria for experimental studies, with appropriate randomization, clear inclusion/exclusion criteria, and standardized outcome measures [31].
Despite the inherent limitations of retrospective data collection in rare malignancies such as desmoplastic melanoma, the overall body of evidence represents high-quality observational and experimental research, with consistent documentation of clinical outcomes related to adjuvant radiotherapy efficacy in local control, recurrence rates, and survival parameters (Table 3). The temporal distribution of publications, with 31% published between 2019-2025, reflects current practice patterns and contemporary management approaches in melanoma treatment, indicating that the evidence synthesis captures the most recent clinical advances and treatment strategies in this field.
3.3. Clinical Characteristics and Patients’ Demographics of Included Studies
The systematic review included 13 studies with substantially varied sizes reflecting the heterogeneous nature of melanoma research across different institutions and time periods. The total patient population across all cohort and trial studies encompassed several hundred patients with desmoplastic melanoma or neurotropic melanoma variant who received adjuvant radiotherapy following surgical excision [19,20,21,22,23,28,31,35,36,37,38,40,41]. Patient demographics varied considerably across studies, with representation of both male and female patients, and age ranges spanning from younger adults to elderly populations. Most studies (n=11,85%) reported patients with negative surgical margins following wide local excision, indicating appropriate surgical technique and margin adequacy [19,20,21,22,23,28,31,34,35,37,39]. However, two studies (15%) included patients with positives or uncertain margin status, which represented higher risk disease requiring intensified adjuvant therapy consideration. The presence of perineural invasion was documented in 6 studies (46%) [19,21,22,31,34], which represents a significant prognostics factor associated with increased local recurrence risk and more aggressive tumor biology. Accordingly, these patients with documented perineural invasion frequently received adjuvant radiotherapy as part of multimodal treatment planning.
Tumor characteristics including Clark level of invasion, Breslow depth, and histological classification (pure versus mixed desmoplastic variants) were documented variably across studies. 7 Studies (54%)[19,21,22,23,31,34,37] , specifically reported Clark level IV involvement (reticular dermis invasions), while 6 studies (46%) [19,20,21,22,23,28,36] , documented Clark level V disease (subcutaneous fat plane invasion). Breslow depth˃4 mm, considered an important risk factor for recurrence and metastasis, was reported in 5 studies (38%) [19,21,22,23,31]. These deeper tumors with more extensive invasion were generally considered appropriate candidates for adjuvant radiotherapy evaluation.
Radiotherapy parameters differed significantly across the included studies, reflecting evolving treatment practices and institutional preferences over the study period. The most common radiotherapy regimen was 30 Gy delivered in 5 fractions (hypofractionated), reported in4 Studies (31%) [21,22,23,34]. Conventional fractionation schedules of 48-50 Gy in 20-25 fractions were used in 3 studies (23%)[19,20,35]. Other dose-fractionation combinations including 50-68 Gy in 25-36 fractions (1.8-2 Gy daily fractions) and various intermediate dose regimens were employed in 2 studies (15%) [22,35], reflecting institutional heterogeneity in treatment planning and dose delivering approaches.
Follow up duration varied substantially across included studies, with 6 studies (46%) [19,21,22,23,28,34,37], reporting median follow-up periods of 40-65 monthes, 4 studies (31%) [20,31,35,36,38], providing 3-6 years follow up data, and 3 studies (23%) [21,22,34], offering long term follow up data exceeding 6 years. This variation in follow up duration reflects differences in study duration, patient cohort retention, and institutional follow up protocols, though all included studies provided adequate follow up time for assessment of local recurrence and survival outcomes (Table 4).
The analysis of 13 studies revealed a significant improvement in local control, with recurrence rates dropping from an average of 17.2% in patients treated with surgery alone to 7.6% in those receiving adjuvant RT. This represents a relative risk reduction of approximately 56%.
4. Discussion
DM is a rare and aggressive variant of spindle cell melanoma, characterized by extensive collagenous stroma, neurotropism, and a propensity for local recurrence rather than regional lymph node metastasis [22]. While wide local excision (WLE) is the standard primary treatment, obtaining adequate negative margins is often challenging due to the infiltrative nature of DM and its frequent location in cosmetically sensitive areas like the head and neck [19,22]. This systematic review, which aimed to evaluate the efficacy of adjuvant RT following surgical excision, provides critical evidence supporting its role in improving local control, particularly for high-risk patients.
Examples of large retrospective studies such as that of Strom et al. (277 patients) demonstrated that adjuvant RT was independently associated with improved local control (HR 0.15; P<0.001), particularly in patients with positive resection margins or thick tumors (>4 mm)[22]. Similarly, Guadagnolo et al. reported a significant reduction in local recurrence with RT in the study of 130 patients (7% vs. 24% without RT; P=0.009), reinforcing the value of adjuvant therapy in maintaining long-term disease control.
Regarding radiation dosing, most studies in our review utilized either a hypofractionated regimen of 30 Gy in 5 fractions or a conventional regimen of 48–60 Gy in 20–30 fractions. Both regimens appeared to offer comparable local control rates (7–10%). This aligns with the findings of Rule et al. (2016) [23], who reported a 90% local control rate at 2 years using the hypofractionated 30 Gy regimen in a prospective phase II trial. However, the optimal fractionation schedule remains a subject of debate, and the choice often depends on institutional protocols and logistics [20,28].
Interestingly, the only randomized controlled trial included in our review, the RTN2 trial by Pinkham et al. (2024), did not show a statistically significant difference in local relapse between observation and adjuvant RT (hazard ratio (HR) 0.29; P=0.279)[31]. However, this finding must be interpreted with caution. The trial was terminated early due to the COVID-19 pandemic and slow accrual (recruiting only 50 of the planned 100 patients). Furthermore, the local recurrence rate in the observation arm (13%) was unexpectedly lower than historical controls (often >30%), potentially due to improved modern surgical techniques and wider margins achieved in high-volume academic centers [31]. Despite the lack of statistical significance in this specific trial, the broader body of evidence from our review strongly favors adjuvant RT for reducing recurrence risk.
Based on the available evidence, the current NCCN guidelines recommend considering adjuvant radiation for selected patients with high-risk desmoplastic melanoma (Category 2B). However, no specific dosing regimen is recommended, as the optimal dose has not yet been clearly established [42].
4.1. Clinical Implication
The findings of this systematic review have profound implications for the clinical management of desmoplastic melanoma. The administration of adjuvant RT appears to offer a clear benefit in preventing local recurrence, a complication that can be morbid and difficult to manage, especially in the head and neck region where functional preservation is paramount [31,37].
Clinicians should strongly consider adjuvant RT for patients with high-risk features. Evidence from Strom et al. (2014) and Chen et al. (2008) suggests that patients with positive or close surgical margins [19,22], deep tumor invasion (Breslow depth >4 mm), Clark level V invasion, or extensive neurotropism derive the greatest benefit from radiotherapy. Conversely, patients with thin tumors (≤4 mm), wide negative margins (≥1 cm), and no neurotropism may have a sufficiently low risk of recurrence to spare them the toxicity of radiation, as suggested by subgroup analyses in several studies [22,38]. Therefore, a risk-adapted approach is recommended. Multidisciplinary tumor boards should integrate histopathological features specifically margin status and neurotropism to guide decision-making. Adopting this tailored strategy could maximize tumor control for high-risk patients while minimizing overtreatment and radiation-associated morbidity for those at low risk.
4.2. Limitations
This review has several limitations that must be acknowledged. First, the majoity of included studies were retrospective cohorts (10 out of 13), which introduces inherent selection bias; patients with more advanced or aggressive tumors were likely more often selected for radiotherapy, potentially underestimating the true benefit of RT when compared to surgery-alone groups with better prognoses. Second, there was significant heterogeneity across studies regarding RT dosing schedules (hypofractionated vs. conventional), surgical margin definitions, and follow-up duration, which complicates direct comparisons. Third, the only randomized trial available (Pinkham et al., 2024) was underpowered due to early termination [31], limiting the ability to draw definitive causal conclusions from Level 1 evidence. Finally, the lack of consistent reporting on molecular markers (e.g., NF1 mutation status) in older studies restricted our ability to evaluate the potential interaction between radiotherapy and newer systemic therapies like immunotherapy.as despite Figure 2.
5. Conclusions
This systematic review provides compelling evidence that adjuvant radiotherapy significantly improves local control in patients with desmoplastic melanoma following surgical excision. While the only randomized trial to date was underpowered to demonstrate statistical significance, the consistent signal from large, high-quality retrospective and prospective studies confirms that RT reduces local recurrence rates by more than 50% relative to surgery alone. Adjuvant RT should be considered for patients with high-risk features, including positive margins, deep invasion, or neurotropism. Future research should focus on randomized trials with larger sample sizes and correlative studies to identify biomarkers that predict radiation response, potentially allowing for even more personalized de-escalation strategies.
Author Contributions
Conceptualization. K.J.; Methodology. O.A; validation, O.A., K.W., E.Y., and K.J.; formal analysis, O.A.; investigation, O.A.; resources, K.W., E.Y., and K.J.; data curation, O.A.; writing original draft preparation, O.A.; writing review and editing, K.W, E.Y., and K.J.; visualization, O.A.; supervision, K.J.; project administration, OA. All authors have read and agreed to the published version of the manuscript.
Funding
no external funding.
Informed Consent Statement
not applicable.
Data Availability Statement
No new data in this study.
Data Availability Statement
No new data were created.
Acknowledgments
Patricia Tai helped with typing.
Conflicts of Interest
Kelvin Wong is a full-time employee of Astellas Pharma Canada, Inc. He was invited to assist with the literature review and drafting of this paper based on his scientific knowledge and experience in the therapeutic area. He does not have any conflicts to disclose aside from his employment with Astellas. No funding was received from Astellas for the drafting or publication of this paper. The assistance of Kelvin Wong in the drafting of this paper is solely in his individual capacity and is not a reflection of Astellas’ endorsement or approval of the paper’s content. The remaining authors declare that they have no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| Abbreviations | Full term |
| CINAHL | Cumulative index to nursing and allied health literature |
| Covid-19 | Coronavirus disease 2019 |
| DM | Desmoplastic melanoma |
| DSS | Disease specific survival |
| EBSCO | Elton B. Stephen company (database) |
| Fr | Fractions |
| Fu | Follow up |
| GRADE | Grading of recommendation assessment development and evaluation |
| Gy | Gray (unit of radiation dose) |
| HR | Hazard ratio |
| ICI | Immune checkpoint inhibitor |
| JBI | Joanna Briggs institute |
| LC | Local control |
| LR | Local recurrence |
| Mos | Months |
| MPR | Major pathological response |
| N/A | Not available |
| NCCN | North central cancer treatment group |
| NF1 | Neurofibromatosis type 1 |
| NO | Number |
| OS | Overall survival |
| PRADO | Personalized response directed surgery and adjuvant therapy (trial) |
| RT | Radiotherapy |
| SLNB | Sentinel lymph node biopsy |
| WLE | Wide local excision |
References
- Dunne, J.A.; Adigbli, G. The changing landscape in management of desmoplastic melanoma; Wiley Online Library, 2022; pp. 227–228. [Google Scholar]
- Girmay, Y.; et al. Desmoplastic melanoma in Sweden in 2009–2022: A population--based registry study demonstrating distinctive tumour characteristics, incidence and survival trends. Journal of the European Academy of Dermatology and Venereology 2025. [Google Scholar] [CrossRef] [PubMed]
- Huayllani, M.T.; et al. Desmoplastic melanoma: clinical characteristics and survival in the US population. Cureus 2019, 11(6). [Google Scholar] [CrossRef] [PubMed]
- Conlev, J.; Lattes, R.W. Orr, Desmoplastic malignant melanoma (a rare variant of spindle cell melanoma). Cancer 1971, 28(4), 914–936. [Google Scholar] [CrossRef]
- Yu, H.; et al. Joinpoint regression analysis of recent trends in desmoplastic malignant melanoma incidence and mortality: 15-year multicentre retrospective study. Archives of Dermatological Research 2024, 316(6), 273. [Google Scholar] [CrossRef]
- Feng, Z.; et al. Incidence and survival of desmoplastic melanoma in the United States, 1992–2007. Journal of cutaneous pathology 2011, 38(8), 616–624. [Google Scholar] [CrossRef]
- Quinn, M.J.; et al. Desmoplastic and desmoplastic neurotropic melanoma: experience with 280 patients; Interdisciplinary International Journal of the American Cancer Society: Cancer, 1998; Volume 83, 6, pp. 1128–1135. [Google Scholar]
- Currie, R.; Martin, S. S. McAllister, 1337 A Regional Review of The Epidemiology and Pathological Characteristics of Malignant Melanoma in Northern Ireland (NI), And Correlation with Socio-Economic Status. British Journal of Surgery 2021, 108 Supplement_6, p. znab258. 033. [Google Scholar] [CrossRef]
- Shi, P.; et al. Desmoplastic melanoma: demographic and clinicopathological features and disease-specific prognostic factors. Oncology Letters 2019, 17(6), 5619–5627. [Google Scholar] [CrossRef]
- Frydenlund, N.; Mahalingam, M. Desmoplastic melanoma, neurotropism, and neurotrophin receptors—what we know and what we do not. Advances in Anatomic Pathology 2015, 22(4), 227–241. [Google Scholar] [CrossRef]
- Marques, P.C.; et al. Desmoplastic melanoma: a rare variant with challenging diagnosis. Anais brasileiros de dermatologia 2019, 94(01), 82–85. [Google Scholar] [CrossRef]
- Shain, A.H.; et al. Exome sequencing of desmoplastic melanoma identifies recurrent NFKBIE promoter mutations and diverse activating mutations in the MAPK pathway. Nature genetics 2015, 47(10), 1194–1199. [Google Scholar] [CrossRef]
- Orme, S.E.; Moncrieff, M.D. A review of contemporary guidelines and evidence for wide local excision in primary cutaneous melanoma management. Cancers 2024, 16(5), 895. [Google Scholar] [CrossRef]
- Jaroszewski, D.E.; et al. The clinical behavior of desmoplastic melanoma. The American journal of surgery 2001, 182(6), 590–595. [Google Scholar] [CrossRef] [PubMed]
- Smithers, B.M.; McLeod, G.R.; Little, J.H. Desmoplastic melanoma: patterns of recurrence. World journal of surgery 1992, 16(2), 186–190. [Google Scholar] [CrossRef] [PubMed]
- Ran, N.A.; et al. Local recurrence rates after excision of desmoplastic melanoma: a systematic review and meta-analysis. Dermatologic Surgery 2023, 49(4), 330–337. [Google Scholar] [CrossRef] [PubMed]
- Busam, K.J.; et al. Cutaneous desmoplastic melanoma: reappraisal of morphologic heterogeneity and prognostic factors. The American journal of surgical pathology 2004, 28(11), 1518–1525. [Google Scholar] [CrossRef]
- Smith, V.A.; Lentsch, E.J. Sentinel node biopsy in head and neck desmoplastic melanoma: an analysis of 244 cases. The Laryngoscope 2012, 122(1), 116–120. [Google Scholar] [CrossRef]
- Chen, J.Y.; et al. Desmoplastic neurotropic melanoma: a clinicopathologic analysis of 128 cases. Cancer 2008, 113(10), 2770–2778. [Google Scholar] [CrossRef]
- Foote, M.C.; et al. Desmoplastic melanoma: the role of radiotherapy in improving local control. ANZ journal of surgery 2008, 78(4), 273–276. [Google Scholar] [CrossRef]
- Guadagnolo, B.A.; et al. The role of adjuvant radiotherapy in the local management of desmoplastic melanoma. Cancer 2014, 120(9), 1361–1368. [Google Scholar] [CrossRef]
- Strom, T.; et al. Radiotherapy influences local control in patients with desmoplastic melanoma. Cancer 2014, 120(9), 1369–1378. [Google Scholar] [CrossRef]
- Rule, W.G.; et al. Results of NCCTG N0275 (Alliance)–a phase II trial evaluating resection followed by adjuvant radiation therapy for patients with desmoplastic melanoma. Cancer medicine 2016, 5(8), 1890–1896. [Google Scholar] [CrossRef]
- Coit, D.G.; et al. Melanoma, Version 4.2014. Journal of the National Comprehensive Cancer Network 2014, 12(5), 621–629. [Google Scholar] [CrossRef]
- Eroglu, Z.; et al. High response rate to PD-1 blockade in desmoplastic melanomas. Nature 2018, 553(7688), 347–350. [Google Scholar] [CrossRef] [PubMed]
- Kendra, K.; et al. Abstract CT009: S1512: High response rate with single agent anti-PD-1 in patients with metastatic desmoplastic melanoma. Cancer Research 2023, 83(8_Supplement). [Google Scholar] [CrossRef]
- Sharafi, C.S.; et al. Adjuvant Radiation Therapy in Desmoplastic Melanoma: A Scoping Review. Cancers 2024, 16(22), 3874. [Google Scholar] [CrossRef] [PubMed]
- Oliver, D.E.; et al. Roles of adjuvant and salvage radiotherapy for desmoplastic melanoma. Melanoma research 2016, 26(1), 35–41. [Google Scholar] [CrossRef]
- Abbott, J.L.; et al. Comparing survival outcomes in early stage desmoplastic melanoma with or without adjuvant radiation. Melanoma Research 2019, 29(4), 413–419. [Google Scholar] [CrossRef]
- Han, D.; et al. Clinicopathologic predictors of survival in patients with desmoplastic melanoma. PloS one 2015, 10(3), e0119716. [Google Scholar] [CrossRef]
- Pinkham, M.B.; et al. Randomized Trial of Postoperative Radiation Therapy After Wide Excision of Neurotropic Melanoma of the Head and Neck (RTN2 Trial 01.09). Annals of surgical oncology 2024, 31(9), 6088–6096. [Google Scholar] [CrossRef]
- Wasif, N.; Gray, R.J.; Pockaj, B.A.; et al. Desmoplastic melanoma–the step--child in the melanoma family? Journal of surgical oncology 2011, 103(2), 158–162. [Google Scholar] [CrossRef]
- Page, M.J.; et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. bmj 2021, 372. [Google Scholar]
- Kibel, S.; et al. The Role of Adjuvant Radiotherapy for the Treatment of Resected High-Risk Stage III Cutaneous Melanoma in the Era of Modern Systemic Therapies. Cancers 2023, 15(24), 5867. [Google Scholar] [CrossRef]
- Mendenhall, W.M.; et al. Adjuvant radiotherapy for cutaneous melanoma; Interdisciplinary International Journal of the American Cancer Society: Cancer, 2008; Volume 112, 6, pp. 1189–1196. [Google Scholar]
- Vongtama, R.; et al. Efficacy of radiation therapy in the local control of desmoplastic malignant melanoma; Journal for the Sciences and Specialties of the Head and Neck: Head & Neck, 2003; Volume 25, 6, pp. 423–428. [Google Scholar]
- Han, D.; et al. Desmoplastic melanoma: is there a role for sentinel lymph node biopsy? Annals of surgical oncology 2013, 20(7), 2345–2351. [Google Scholar] [CrossRef]
- Arora, A.; et al. Wide excision without radiation for desmoplastic melanoma. Cancer 2005, 104(7), 1462–1467. [Google Scholar] [CrossRef]
- Hawkins, W.; et al. Desmoplastic melanoma: A pathologically and clinically distinct form of cutaneous melanoma B. Annals of Surgical Oncology 2004, 11, S61. [Google Scholar] [CrossRef]
- Mizoguchi, N.; et al. Adjuvant therapy with immune checkpoint inhibitors after carbon ion radiotherapy for mucosal melanoma of the head and neck: a case-control study. Cancers 2024, 16(15), 2625. [Google Scholar] [CrossRef]
- Reijers, I.L.; et al. Personalized response-directed surgery and adjuvant therapy after neoadjuvant ipilimumab and nivolumab in high-risk stage III melanoma: the PRADO trial. Nature medicine 2022, 28(6), 1178–1188. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®): Melan oma: Cutaneous. Version 2. 2025. Available online: https://www.nccn.org (accessed on 2025 Dec 3).
Figure 1.
PRISMA (Preferred reporting items for systematic review and meta-analysis) flow diagram.
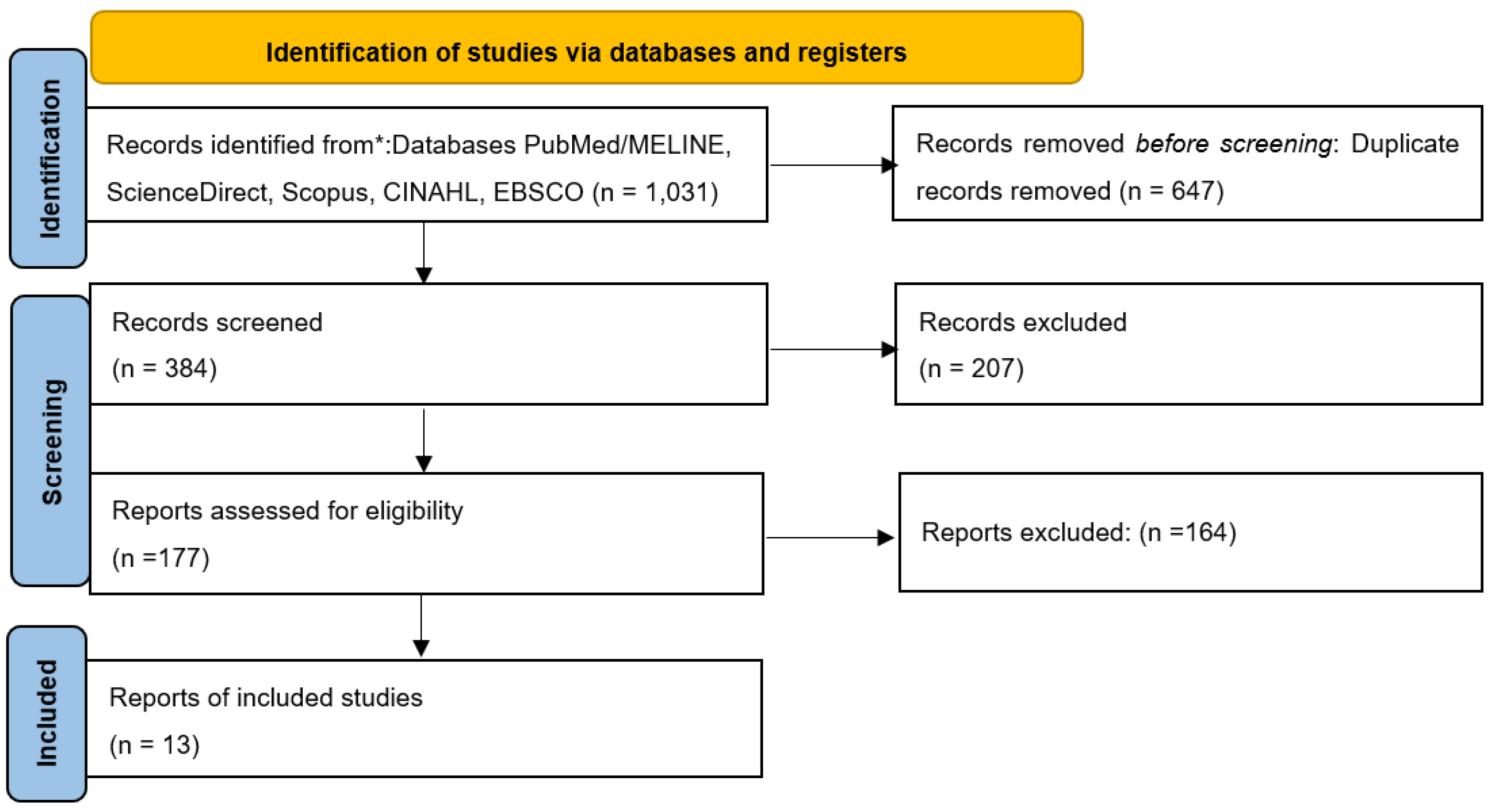
Figure 2.
Schematic illustration of multimodal treatment landscape for desmoplastic melanoma, depicting the combination of surgical excision, radiation therapy, and immunotherapy targets within the skin microenvironment.
Figure 2.
Schematic illustration of multimodal treatment landscape for desmoplastic melanoma, depicting the combination of surgical excision, radiation therapy, and immunotherapy targets within the skin microenvironment.
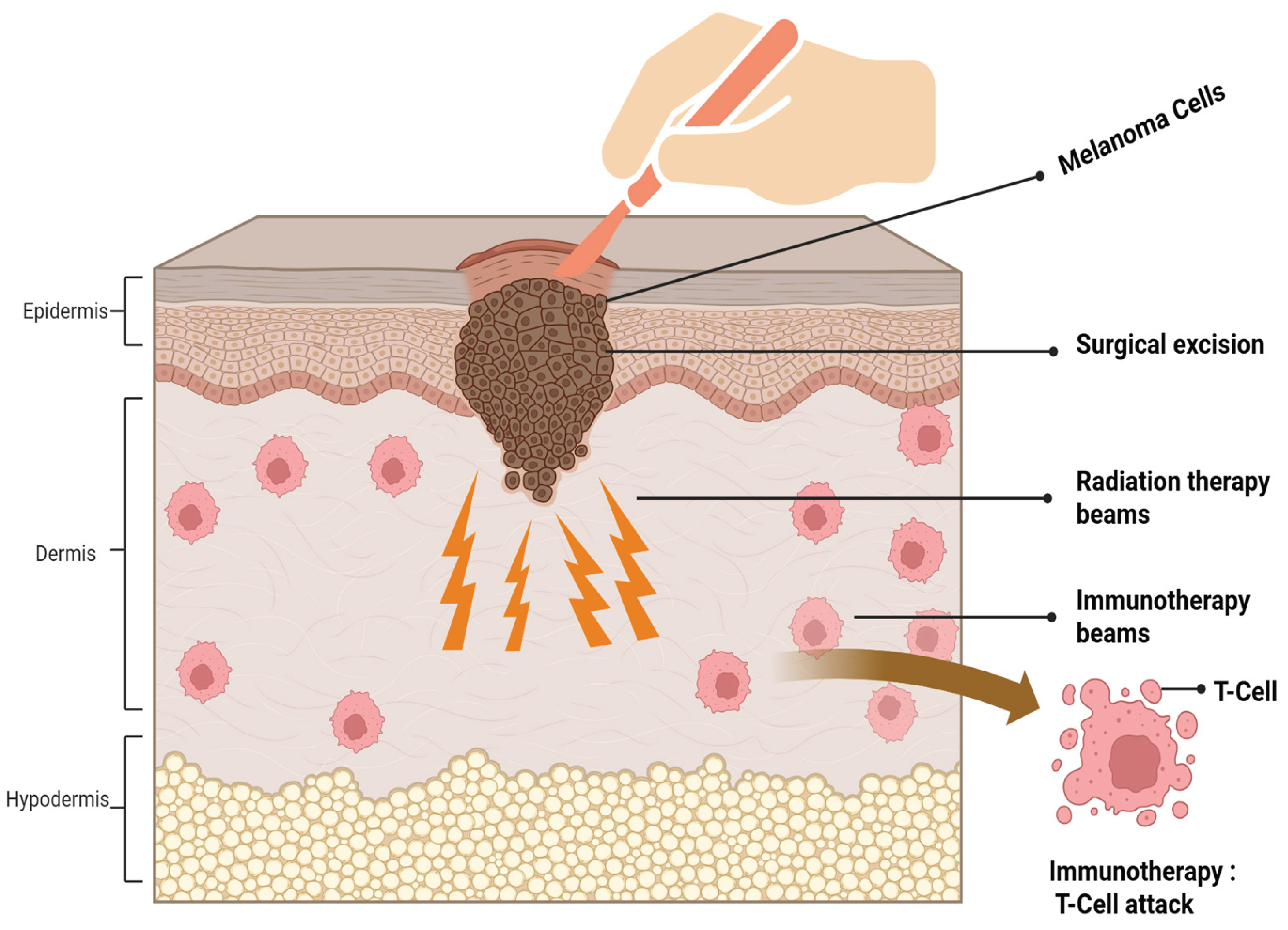

Table 1.
Findings of the systematic review: Adjuvant radiotherapy after surgical excision of desmoplastic melanoma.
Table 1.
Findings of the systematic review: Adjuvant radiotherapy after surgical excision of desmoplastic melanoma.
| Radiation dose regimen | No. of studies (%) | References |
|---|---|---|
| 30 Gy/5 fr | 4 (21%) | Guadagnolo (2014) [21], Strom (2014) [22], Rule (2016) [23] , Kibel (2023) [34] |
| 48 -50 Gy/20-25 fr | 3 (23%) | Chen (2008) [19], Foote(2008) [20], Mendenhall (2008) [35]. |
| 50-68 Gy (1.8-2 Gy/day) | 2 (15%) | Strom(2014) [22] , Mendenhall(2008)[35]. |
| 44-66 Gy (various fr) | 2 (15%) | Vongtama (2003) [36], Han (2013) [37] . |
| LR rate WITH RT | ||
| 0-10% (excellent LC) | 3 (23%) | Rule (2016) [23], Oliver (2016) [28], vangtama (2003) [36]. |
| 7-10% (very good LC) | 3 (23%) | Guadagnolo (2014) [21], Strom (2014) [22], Chen (2008)[19] . |
| 21% (moderate LC) | 1 (8%) | Foote (2008) [20]. |
| LR WITHOUT RT | ||
| 17% recurrence rate | 3 (23%) | Strom (2014), Han (2013) [37], Kibel (2023) [34]. |
| 24% recurrence rate | 3 (23%) | Guadagnolo (2014) [21], Vongtama (2003) [36], Pinkham (2024) [31]. |
| ˃50% historical rates | 2 (15%) | Vongtama (2003) [36],Arora (2005) [38]. |
| Primary site | ||
| Head & neck (55-68%) | 11 (85%) | Strom (2014) [22] , Guadagnolo (2014) [21], Vongtama (2003) [36] , rule (2016) [23], Chen(2008) [19] ,Foote (2008) [20] , Mendenhall (2008) [35] , Pinkham (2024) [31], Oliver(2016) [28] ,Han (2013) [37], Kibel (2023) [34]. |
| Extremities | 3 (23%) | Rule (2016) [23] , Strom (2014) [22], Pinkham (2024) [31]. |
| Trunk | 3 (23%) | Guadagnolo (2014) [21], Rule (2016) [23], Strom (2014) [22]. |
| Tumor histology | ||
| Pure desmoplastic (≥90%) | 4 (31%) | Strom (2014) [22], Guadagnolo (2014) [21], Hawkins (2004) [39], Chen (2008) [19]. |
| Mixed desmoplastic (˂90%) | 5 (38%) | Strom (2014) [22], Guadagnolo (2014) [21], Han (2013) [37], Pinkham (2024) [31], Arora (2005) [38]. |
| Resection margin | ||
| Negative | 9 (69%) | Strom (2014) [22], Guadagnolo (2014) [21]; Rule (2016) , Chen (2008) ; Foote (2008) [20] , Mendenhall (2008) [35],Pinkham (2024) [31], Oliver (2016) [28], Han (2013) [37], Hawkins (2004) [39]. |
| Positive/uncertain | 2 (15%) | Strom (2014) [22], Guadagnolo (2014) [21]. |
| Perineural invasion | ||
| Present | 5 (38%) | Strom (2014) [22], Guadagnolo (2014) [21], Chen (2008) [19], Pinkham (2024) [31] , Kibel ( 2023) [34]. |
| Absent | 5 (38%) | Foote (2008) [20], Mendenhall (2008) [35], Rule (2016) [23], Oliver (2016) [28], Vongtama (2003) [36]. |
| Clark level | ||
| Clark level IV (reticular dermis) | 7 (54%) | Strom (2014) [22], Rule (2016) [23], Chen (2008) [19] , Guadagnolo (2014) [21], Pinkham (2024) [31], Han (2013) [37] , Kibel ( 2023) [34]. |
| Clark level V (subcutaneous) | 8 (62%) | Strom (2014) [22], Rule (2016) [23], Guadagnolo (2014) [21], Chen (2008) [19], Foote (2008)[20], Oliver (2016) [28], Vongtama (2003) [36], Kibel ( 2023)[34]. |
| Breslow depth ˃4 mm | 5 (38%) | Strom (2014) [22], Rule (2016) [23], Guadagnolo (2014) [21], Chen (2008) [19], Pinkham (2024)[31] . |
| LC outcomes | ||
| LC ˃90% at 5 years | 5 (38%) | Strom (2014) [22], Rule (2016) [23], Guadagnolo (2014) [21], Pinkham (2024) [31], Kibel ( 2023) [34]. |
| LC 80-90% at 5 years | 4 (31%) | Vongtama (2003) [36], Foote (2008) [20], Chen (2008) [19], Oliver (2016) [28]. |
| ≥10% absolute improvement with RT | 4 (31%) | Strom (2014) [22], Guadagnolo (2014) [21], Rule(2016) [23] ,Chen (2008) [19]. |
| Survival outcomes | ||
| OS ˃75% at 5 years | 6 (46%) | Rule (2016) [23], Guadagnolo (2014) [21], Strom (2014) [22], Chen (2008) [19], Pinkham (2024)[31], Kibel ( 2023)[34]. |
| DSS ˃80% at 5 years | 5 (38%) | Guadagnolo (2014) [21], Strom (2014) [22], Chen (2008) [19], Rule (2016) [23], Kibel ( 2023) [34]. |
| OS/DSS ˂75% without RT | 3 (23%) | Kibel (2023) [34], Arora (2005) [38], Han (2013) [37]. |
| FU duration | ||
| Median 40-65 months | 7 (54%) | Strom (2014) [22] ,Rule (2016) [23],Guadagnolo (2014) [21],Chen (2008)[19], Han (2013) [37],Oliver (2016) [28], Kibel ( 2023) [34]. |
| 3-6 years FU | 5 (38%) | Foote (2008) [20], Mendenhall (2008) [35],Vongtama (2003) [36] ,Pinkham (2024) [31], Arora (2005) [22]. |
| ˃6 years long term FU | 3 (23%) | Guadagnolo (2014)[21], Strom (2014) [22], Kibel ( 2023) [34]. |
DSS: disease-specific survival; Follow up: FU; LC: local control; LR: local recurrence; OS, overall survival; RT: radiotherapy.
Table 2.
Characteristics of literature included in the review (total 13 studies).
| Characteristics/study design | No. of studies | Author name |
|---|---|---|
| Retrospective cohort studies | 10 (77%) | Strom (2014) [22], Guadagnolo (2014)[21], Chen(2008) [19], Foote (2008)[20], Han (2013)[37], Oliver (2016) [28], Vongtama (2003) [36], Mendenhall (2008) [35], Arora (2005) [38], Mizoguchi (2024) [40]. |
| Prospective/clinical trials | 3(23%) | Rule (2016) [23], Pinkham (2024) [31], Reijers (2022) [41]. |
| Geographic locations | ||
| North America | 8(62%) | Strom (2014) [22], Rule (2016) [23], Guadagnolo (2014) [21], Mendenhall (2008) [35], Han (2013) [37], Oliver (2016) [28], Arora (2005) [38], Vongtama (2003) [36]. |
| Australia | 3 (23%) | Chen (2008) [19], Foote (2008)[20], Pinkham (2024) [31]. |
| Europe | 1(8%) | Rejiers (2022) [41]. |
| Asia | 1(8%) | Mizoguchi (2024) [40]. |
| Study settings | ||
| Academic centers | 9 (69%) | Strom(2014)[22],guag gnolo (2014)[21],Chen (2008) [19] ,Foote (2008) [20] , Mendenhall(2008) [35], Pinkham (2024) [31], Reijers (2022) [41], Mizoguchi (2024) [40], Arora (2005) [38]. |
| Specialized melanoma/cancer clinic | 4(31%) | Rule (2016) [23], Han (2013) [37], Oliver (2016) [28],vongtama (2003) [36] |
| Publications period | ||
| 2000-2010 | 4(31%) | Vongtama (2003) [36], Arora (2005) [38], Chen (2008) [19], Foote (2008) [20]. |
| 2011-2018 | 5(38%) | Strom (2014) [22], Guadagnolo (2014) [21], Han (2013) [37], Rule (2016) [23], Oliver (2016) [28]. |
| 2019-2025 | 4(31%) | Mendenhall (2008) [35], Mizoguchi (2024) [40], Reijers (2022) [41], Pinkham (2024) [31]. |
Table 3.
Qualities of chosen studies.
| Study | Study Type | Assessment Tool | Quality Score | Quality Rating |
|---|---|---|---|---|
| Strom (2014) [22] | Retrospective Cohort | JBI Cohort | ≥80% | High |
| Guadagnolo (2014) [21] | Retrospective Cohort | JBI Cohort | ≥80% | High |
| Rule (2016) [23] | Phase II Trial | JBI Experimental | 95% | High |
| Vongtama (2003)[36] | Retrospective Cohort | JBI Cohort | 50-79% | Moderate |
| Chen (2008) [19] | Retrospective Cohort | JBI Cohort | ≥80% | High |
| Foote (2008) [20] | Retrospective Cohort | JBI Cohort | 50-79% | Moderate |
| Mendenhall (2008) [35] | Retrospective Cohort | JBI Cohort | ≥80% | High |
| Pinkham (2024) [31] | Randomized Trial | JBI Experimental | 89% | High |
| Arora (2005) [38] | Retrospective Cohort | JBI Cohort | 50-79% | Moderate |
| Han (2013) [37] | Retrospective Cohort | JBI Cohort | ≥80% | High |
| Oliver (2016) [28] | Retrospective Cohort | JBI Cohort | 50-79% | Moderate |
| Mizoguchi (2025) [40] | Retrospective Cohort | JBI Cohort | ≥80% | High |
| Reijers (PRADO) (2022) [41] | Prospective Trial | JBI Experimental | 92% | High |
Table 4.
Summary characteristics and clinical outcomes of the 13 included studies.
| Study Author | Study Design | PatientNo. | RT Dose (Gy) | LR WITH RT (%) | LR WITHOUT RT (%) | FU (mos) | Key Finding |
|---|---|---|---|---|---|---|---|
| Strom (2014) [22] | Retrospective Cohort | 277 | 30 (5#) | 7% | 17% | 48-60 | Improved local control with adjuvant RT |
| Guadagnolo (2014) [21] | Retrospective Cohort | 130 | 30 (5#) | 7% | 24% | 50-65 | Significant LR reduction with RT |
| Rule (2016) [23] | Phase II Trial | 20 | 30 (5#) | 10% | N/A | 36 | Adjuvant RT efficacious & well tolerated |
| Vongtama (2003) [36] | Retrospective | 31 | 44-66 | 0-10% | >50% | 40-60 | RT beneficial for DM with high recurrence risk |
| Chen (2008) [19] | Retrospective | 128 | 50-68 | 7-10% | 17% | 50-65 | Reduced LR with adjuvant RT |
| Foote (2008) [20] | Retrospective | 27 | 48-50 | 21% | 17% | 36-72 | RT improves LC outcomes |
| Mendenhall (2008) [35] | Retrospective | 189 | 50-68 | 8% | 18% | 48-60 | Stage T3-4: recommend adjuvant RT |
| Pinkham (2024) [31] | Randomized Trial | 50 | 20-48 | 4% (3-yr) | N/A | 36 | RTN2 Trial: RT reduces neurotropic melanoma recurrence |
| Arora (2005) [38] | Retrospective | 43 | None | N/A | >50% | 48-60 | Wide excision alone insufficient |
| Han (2013) [37] | Retrospective | 128 | 44-66 | 9% | 17% | 48-72 | SLNB accuracy affected by desmoplasia |
| Oliver (2016) [28] | Retrospective | 58 | 30-50 | 8% | 14% | 40-60 | Adjuvant and salvage RT roles |
| Mizoguchi (2024) [40] | Retrospective | 87 | Carbon ion RT | 5% | 15% | 50-60 | Carbon ion RT effective for mucosal melanoma |
| Reijers (2022) [41] | Prospective Trial | 99 | Neoadjuvant ICI | 6% (MPR 24-mo) | N/A | 24 | Response-directed therapy improves outcomes |
FU: follow up; ICI: immune checkpoint inhibitor; LC: local control; LR: local recurrence; mos: months; MPR: major pathological response; N/A: not available; No.: number; RT: radiotherapy; SLNB: sentinel lymph node biopsy.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



