Submitted:
05 December 2025
Posted:
08 December 2025
You are already at the latest version
Abstract
Nutritional management of children with short bowel syndrome (SBS) remains controversial and depends on multiple factors, including age, etiology, time from resection, extent of bowel loss, residual anatomy, bowel continuity, and associated complications. Consequently, recommendations across intestinal rehabilitation centers rely largely on clinical experience rather than evidence from controlled trials. The primary goals of nutritional management in SBS include progressive advancement of enteral nutrition (EN), discontinuation of parenteral nutrition (PN) with subsequent removal of feeding devices, optimization of intestinal adaptation, and ultimately, achievement of enteral autonomy while supporting normal growth and development. This review summarizes the physiological principles of enteral nutrition and provides practical recommendations for advancing the diet in children with SBS, with particular attention to anatomical variations of SBS and postoperative phases after bowel resection. Emerging areas of interest- including the use of blended diets and the role of EN in enhancing intestinal adaptation - are discussed. Finally, the influence of EN on enteral tolerance and intestinal motility is reported.
Keywords:
short bowel syndrome
; intestinal failure
; children
; nutritional management
; intestinal adaptation
; enteral nutrition
; parenteral nutrition
1. Introduction
Intestinal failure (IF) develops when intestinal length or function is insufficient to maintain adequate nutrient absorption and normal nutritional status [1,2]. The American Society for Parenteral and Enteral Nutrition (ASPEN) defines pediatric IF as a reduction in the actual functional intestinal mass below the level needed to sustain normal growth, adequate nutrient absorption, or electrolyte balance, leading to dependence on PN for a minimum of 60 days within a 74-day consecutive interval [1,2]. Short bowel syndrome (SBS) is the most common cause of IF worldwide, affecting 67% of adults and 85% of children [3,4] with IF. SBS remains a significant clinical challenge due to its associated high morbidity and mortality rates, as well as its profound socioeconomic impact. While the length of the remaining intestine after bowel loss is commonly used to define SBS, the functionality of the gut is of greater significance. Consequently, some medical centers classify SBS as a functional rather than an anatomical entity. The Canadian Association of Pediatric Surgeons defines SBS as the necessity of parenteral nutrition (PN) for more than 42 days following massive gut resection or having a residual intestinal length of less than 25% of the expected length for gestational age [5]. Although most nutrient absorption occurs in the proximal small intestine, the specific segment resected largely determines nutritional requirements, clinical presentation and potential nutrient deficiencies in SBS, as each segment has distinct absorptive and regulatory functions.
1.1. Anatomical Types of SBS
SBS can be anatomically classified into three types according to the presence or absence of a small-bowel ostomy, preservation of the ileocecal valve (ICV), and colonic continuity [6,7] (Figure 1).
Type 1- End jejunostomy (No Colon in Continuity). Type 1 SBS results from extensive resection of the small intestine and colon, including loss of the ileocecal valve, leaving children with an end-jejunostomy. Because the ileum normally absorbs most intestinal fluid (about 80%) and the colon absorbs the remaining 20% - with the ability to increase absorption when needed - loss of these segments leads to rapid transit, high-output losses, and a high risk of dehydration and electrolyte disturbances [8,9]. The jejunum’s high permeability further worsens sodium and fluid losses when children ingest low-sodium or markedly hypo- or hyperosmolar fluids. Resection of the distal ileum and proximal colon also eliminates L-cells that produce PYY, GLP-1, and GLP-2, hormones crucial for slowing transit and supporting mucosal adaptation [6,10], and reduces bile acid reabsorption, impairing fat absorption [7]. As a result, many children with Type 1 SBS require PN to maintain hydration and nutritional status.
Type 2- Jejuno-colonic anastomosis. Type 2 SBS is characterized by extensive ileal resection with the remaining jejunum anastomosed to a portion of the colon. Under normal conditions, the jejunum absorbs most macronutrients and water-soluble vitamins, but the ileum can adapt substantially after jejunal resection. Studies show that protein, carbohydrate, and many vitamin and mineral absorptive capacities may be preserved when sufficient healthy ileum remains [11,12]. However, reduced jejunal hormone secretion may reduce pancreaticobiliary stimulation and contribute to gastric hypersecretion, altering the luminal environment [10]. Although the ileum plays a smaller role in macronutrient absorption, its slower transit and greater length allow significant adaptive potential. Ileal resection, as in Type 1 SBS, impairs bile acid reabsorption and limits mixed micelles formation [7,13].
Type 3- Jejuno–Ileo–Colonic Continuity (Colon and Ileocecal Valve Preserved). Type 3 SBS includes patients who retain a segment of terminal ileum, ICV and an intact colon. Beyond small-bowel length, preservation of the colon is increasingly recognized as a key determinant of outcomes. The colon can markedly increase its absorptive capacity, supporting fluid and electrolyte balance, slowing transit, and improving energy salvage. Retaining colonic continuity is associated with reduced fecal nutrient losses and a higher likelihood of decreasing PN dependence [14,15,16,17]; some experts equate preserving at least half the colon to maintain roughly 50 cm of small intestine, although this varies by patient [15,18]. Colonic fermentation of unabsorbed carbohydrates produces short-chain fatty acids (SCFAs), which provide additional calories and stimulate GLP-2 and PYY release, supporting mucosal adaptation [10,19,20]. When feasible, early restoration of intestinal continuity enhances these benefits and may improve overall energy salvage.
1.2. Intestinal Adaptation: Time Course and Features
Intestinal adaptation comprises structural and functional changes that increase absorptive capacity after resection [21]. Adaptation begins within 24–48 hours and may continue for 18–24 months; many reports suggest a practical plateau by 1–3 years in children, with ~90–95% of adaptive potential achieved in the earlier period and scope for additional incremental gains thereafter [21,22,23].
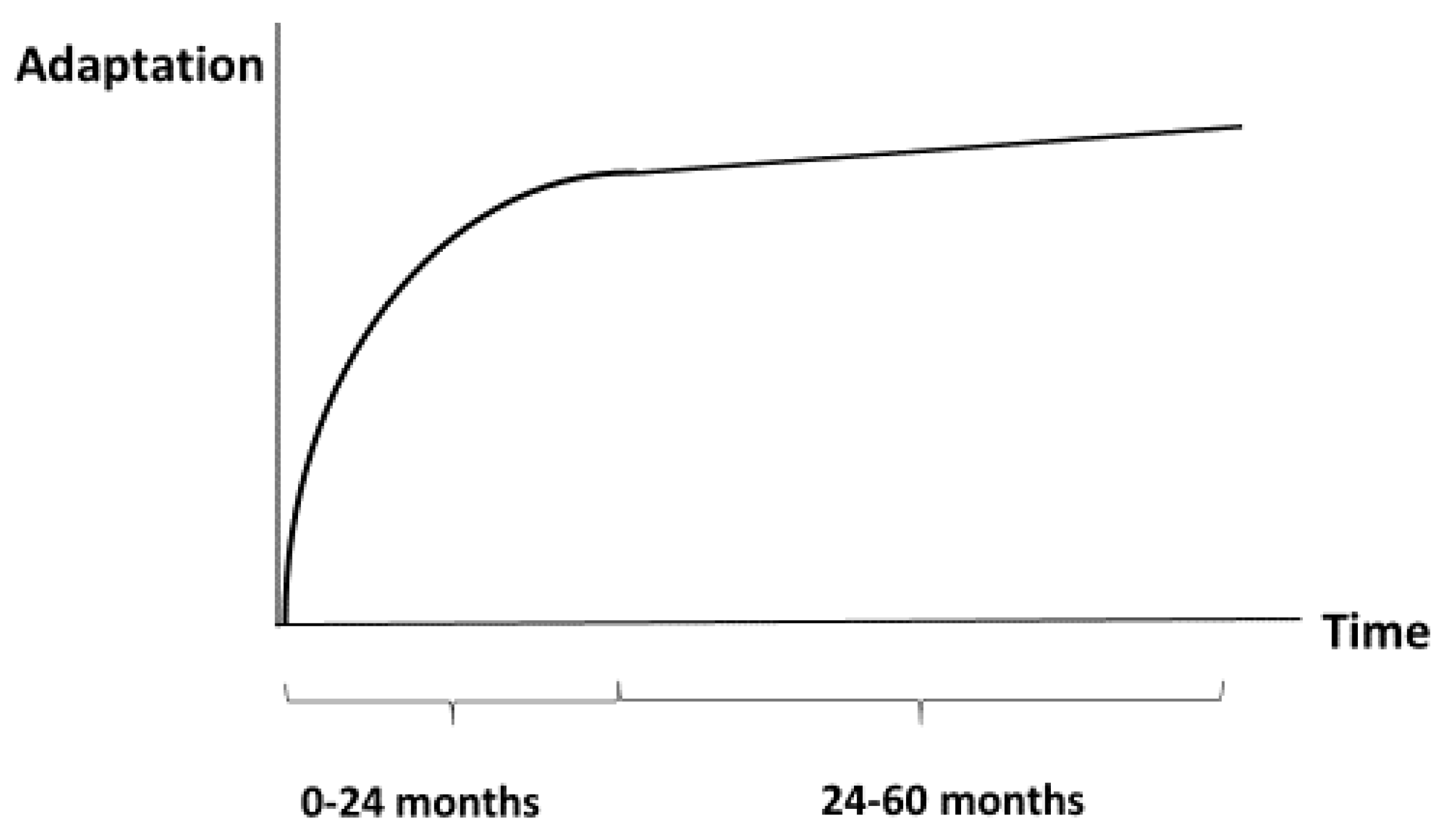
Figure 2.
Schematic diagram of development of intestinal adaptation during first 5 years. Accelerated development during first 24 months following by slow development during next 36 months.
Figure 2.
Schematic diagram of development of intestinal adaptation during first 5 years. Accelerated development during first 24 months following by slow development during next 36 months.
Hallmarks of intestinal adaptation include bowel elongation and dilation, increased crypt proliferation with deeper crypts, increased number of enterocytes, and taller villi, collectively expanding surface area and absorption. Clinically, adaptation manifests as stabilization of fluid/electrolyte balance, improved nutrient absorption with weight gain, and reduced stool losses [20,21,22,23].
1.3. Postoperative Phases of SBS
Nutritional management of patients (adults and children) with SBS has traditionally been divided into three phases (Figure 3) [6,24,25]:
- Acute Phase: This phase begins immediately after surgery and typically lasts 3 to 4 weeks. It is characterized by poor absorption of fluids, electrolytes, and nutrients, leading to significant intestinal losses and metabolic disturbances, as well as gastric hypersecretion due to the absence of inhibitory hormones normally released from the terminal ileum.
- Adaptation Phase: Lasting 1 to 2 years, this phase involves adaptive changes in the remaining small bowel to increase both the absorptive surface (structural adaptation) and the absorptive capacity of isolated enterocytes (functional adaptation), ultimately resulting in improved nutrient and micronutrient absorption. These processes are stimulated by the presence of nutrients in the bowel, gastrointestinal secretions, hormones released by the remaining bowel, and the production of peptide growth factors.
- Maintenance Phase: This final phase lasts several years. The goals for managing children with SBS during this phase include achieving enteral autonomy, discontinuing parenteral nutrition, and removing feeding devices while ensuring continued weight gain and growth velocity.
Parenteral nutrition (PN) remains a life-saving therapy for children with SBS. It is indispensable for maintaining adequate nutrition, growth, and neurodevelopment in the presence of severe malabsorption. Over recent decades, the prognosis of SBS has markedly improved owing to the availability and refinement of PN [26]. However, prolonged PN use is associated with multiple complications, including central line–associated bloodstream infections, intestinal failure–associated liver disease (IFALD), vascular thrombosis, metabolic disturbances, and multiorgan dysfunction [27]. To minimize PN-related complications, PN should be individualized according to the patient’s tolerated enteral intake and gradually reduced as enteral feeding improves. Whenever possible, enteral nutrition (EN) is preferred because it more closely mimics physiological nutrient delivery [10,28,29]. Enteral nutrients are also the primary drivers of intestinal adaptation. Both experimental and clinical studies have demonstrated that sustained nutrient contact with the intestinal mucosa stimulates epithelial proliferation and mucosal regrowth [21,22,23]. Nevertheless, rapid advancement of EN in patients with markedly reduced residual bowel length may be counterproductive. Excessive feeding may impair intestinal adaptation and contribute to dysmotility [30,31].
This review summarizes key physiological principles of enteral nutrition and offers practical guidance for advancing dietary therapy in children with SBS, with particular attention to anatomical variations and postoperative phases after bowel resection.
2. Methods
A structured, comprehensive literature search was conducted using the MEDLINE (PubMed), Scopus, Web of Science, Cochrane Central Register of Controlled Trials (CENTRAL), Scientific Electronic Library Online (SciELO), and Google Scholar databases for studies published between January 1975 and October 2025. In addition, a manual search of the reference lists of the retrieved publications was performed to identify additional relevant studies. The objective was to identify all human studies (clinical settings) in children directly addressing nutrition or specified nutrients in relation to SBS. Search terms included various combinations of the following keywords: “short bowel syndrome,” “intestinal failure,” “children,” “enteral nutrition,” “enteral feeding”, “parenteral nutrition weaning,” “phases of SBS,” “types of SBS,” and “intestinal adaptation.” Eligibility criteria were based on the PICO (Population, Intervention, Comparator, and Outcome) framework and were defined according to the inclusion and exclusion criteria summarized in Table 1.
Two authors independently screened the titles and abstracts of all identified studies. Full-text papers meeting the inclusion criteria-including analytical cross-sectional studies, prospective cohort studies, case-control studies, longitudinal studies, randomized controlled trials, case series, and retrospective cross-sectional studies-were retrieved for detailed assessment. Studies were excluded if they did not meet the review objectives, were not in English, or consisted of editorials, letters to the editor, conference abstracts, duplicate entries, or articles without freely available abstracts.
The following key questions were formulated for each phase of SBS (acute, adaptation, and maintenance phases):
- At what time should enteral nutrition (EN) be initiated? How should EN be advanced and administered?
- What type of EN should be used (focusing on specific macronutrients and micronutrients) during each post-surgical phase?
- What are the features of nutritional management depending on the type of SBS (e.g., site of resection, colon-in-continuity)?
To minimize bias at all stages of the review, several methodological safeguards were implemented: a/ Independent screening: Two authors independently conducted literature screening, data extraction, and quality assessment. Discrepancies were resolved by discussion or consultation with a third reviewer; b/ Duplicate removal and data verification: All datasets were cross-checked to avoid duplicate inclusion and confirm data accuracy; c/ Reporting standards: The review was conducted and reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) guidelines, ensuring methodological transparency and reproducibility [32]. d/Transparent inclusion criteria: The predefined PICO framework ensured objective selection and consistent eligibility decisions (Table 1); e/Quality appraisal: The STROBE Statement checklist was applied to cohort, case-control, and cross-sectional studies [33], and the Joanna Briggs Institute (JBI) checklist was used for systematic reviews and meta-analyses [34].
Definitions
The target population (referred to as children) included neonates, infants, and older children diagnosed with SBS. EN was defined as the delivery of nutrients to the gastrointestinal tract via oral or enteral tube feeding (nasoenteral, gastrostomy, or jejunostomy). Continuous administration typically employs an enteral infusion pump, with the hourly rate calculated by dividing the daily nutritional requirement by the total infusion time. Bolus feed volumes are determined by dividing the total daily requirement by the number of feedings. Minimal enteral feeding was defined as ≤12 mL/kg/day or <25 kcal/kg/d ay for 5–10 days in infants [35]. Extensively hydrolyzed (semi-elemental) formulas (EHFs) contain hydrolyzed proteins (oligopeptides and free amino acids). Amino-acid–based (elemental) formulas (AAFs) are similar but contain only free amino acids as the protein source. Polymeric (standard) formulas consist of intact proteins [36]. Short bowel syndrome (SBS) was defined as the need for parenteral nutrition (PN) for more than six weeks following massive intestinal resection or a residual intestinal length of <25% of the expected value for gestational age [1,3]. Enteral autonomy (EA) was defined as an achievement of adequate weight and height gain that are maintained using EN alone for more than three consecutive months [1]. Tolerance was defined as the ability to increase enteral or oral feeds without significant vomiting, diarrhea, or other signs of malabsorption.
3. Results
The literature search identified 130 pediatric clinical effect studies that had investigated the effects of different aspects of feeding strategies on clinical outcomes in children with SBS. Very few high-quality clinical randomized control studies are available on aspects of EN in children with SBS because of the relatively low incidence of the disorder and high variety of its manifestation in every patient. Consequently, dietary management is highly variable and depends on both clinical situation and Institutional policy. Five studies covered the timing of initiation of EN. Twenty-five papers covered method of administration (route of delivery). Forty-six studies covered type of nutrition (in first phase-38 papers, in second phase-20 papers, in third phase-7 papers). Ten studies were found on the advancement of EN (in first phase-3 papers, in second phase-5 papers, in third phase-2 papers). Eight papers focused on specific nutrients in relation to SBS (preventing hyperoxaluria, preventing osmotic diarrhea etc.). In addition, seven case reports and narrative review articles on feeding strategies in children with SBS were identified. Findings from those articles, if relevant, are listed under each key question.
4. Discussion
4.1. Enteral Nutrition at the First Phase of SBS (Acute Phase, Typically Lasts Weeks to Months).
The acute phase begins immediately postoperatively, before intestinal adaptation has occurred, when absorption is markedly impaired. During this period, delayed transit, reduced motility, diarrhea, and substantial fluid and electrolyte losses are frequent, increasing the risk of dehydration [37]. The acute phase typically lasts several days to a few weeks and is characterized by postoperative ileus and high gastrointestinal output [4]. The ESPGHAN Committee on Nutrition further delineates three stages within this phase: an early period (first 24–48 h), an intermediate postoperative period (up to ~1 week), and a recovery period (from ~day 7 until stabilization or transfer from intensive care) [38]. Throughout the early and intermediate stages, clinical priorities are maintenance of hydration and sodium balance, with close monitoring and replacement of losses using parenteral solutions that provide adequate sodium, as enteral tolerance is generally limited [39].
Parenteral Nutrition (PN).
As previously mentioned, PN is fundamental to immediate postoperative care in infants and children with SBS, regardless of etiology. Primary objectives are prevention of acute malnutrition, maintenance of fluid and electrolyte homeostasis, and support of growth during early adaptation, when enteral intake cannot meet requirements. In infants after extensive resection, PN is typically initiated within 48–72 h postoperatively [39]. Estimated energy needs are ~60–80 kcal/kg/day in preterm infants and 45–70 kcal/kg/day in term infants, with a minimum of 1.3–1.5 g/kg/day of parenteral amino acids to sustain positive nitrogen balance [39]. Fluid and electrolyte prescriptions should be individualized based on measured gastrointestinal and stoma losses, and routine micronutrient supplementation is required because deficiencies are common [39,40]. Close monitoring is essential: daily weights; meticulous intake/output; plasma sodium; and daily urinary sodium are recommended to ensure adequate replacement, with prompt correction of ongoing losses using appropriate sodium-containing solutions [39].
Timing of EN Initiation.
Early EN promotes intestinal adaptation from the acute phase by providing luminal nutrients that stimulate mucosal hyperplasia, support epithelial growth and absorptive capacity. It also enhances secretion of gastrointestinal and pancreaticobiliary hormones that drive gallbladder contraction, digestion, and intestinal motility [27,41]. EN helps reduce PN-associated cholestasis, supports microbiome development - particularly in preterm and high-risk infants [39,42] - and protects the mucosa from stress-related injury. Additionally, EN is simpler, safer, and more cost-effective than PN [36]. Because of these benefits, feeds should commence as soon as clinically feasible, often within the first days after resection-to promote adaptation and potentially reduce hospitalization [39,42]. Some centers begin once stool passage is documented [43], whereas others use more conservative criteria (e.g., clear, non-bilious tube drainage; audible bowel sounds; a soft, non-tender abdomen) before advancement [44].
As infants transition into the late acute phase, EN should be gradually increased with recognition of persistent malabsorption due to reduced surface area. Typical targets are ~90–120 kcal/kg/day for preterm infants and ~75–85 kcal/kg/day for term infants, with routine monitoring and supplementation for micronutrient deficiencies [39]. To reduce risk of PN-associated liver disease, PN cycling should begin as tolerated in the late postoperative period—commonly once the infant is clinically stable and ~≥4 kg—to lessen hypoglycemia risk during PN-free intervals. Avoid overly rapid PN weaning or advancing EN faster than intestinal tolerance permits [37,39].
Route of Delivery.
Oral vs Tube Feeding.
Oral feeding should be encouraged when feasible because it provides physiological stimulation (including salivary epidermal growth factor release) and supports normal gastric and pancreatic secretions; luminal nutrient exposure triggers trophic enteral factors and hormones that aid adaptation [39,44,45]. Early oral experiences may also reduce the risk of later oral aversion, a complication that can delay transition from PN and affect quality of life (QOL) [44]. When oral feeding is not possible (e.g., mechanical ventilation, instability, immaturity, or dysfunction), early tube feeding is appropriate.
Gastric vs Post-pyloric Feeding.
Gastric delivery is physiologic, technically simpler, and can be given as intermittent boluses or continuous infusions, facilitating flexible strategies. Gastric feeding increases nutrient–mucosa contact and supports motility; in SBS it has been associated with improved transit and reduced diarrhea, thereby promoting adaptation [40,46]. Alternating feeding and fasting-together with cyclic PN-may avoid continuous insulin secretion and limit excessive fat synthesis and deposition [11,37]. Jejunal feeding can be useful in significant gastroesophageal reflux or aspiration risk and in selected patients with severe gastric dysfunction or anatomical barriers [47]. However, post-pyloric access is more technically demanding, costlier, and carries higher mechanical complication risks; it bypasses gastric/duodenal stimulation of biliary and pancreatic secretions and has been linked to intussusception [46,48,49]. Because post-pyloric feeding bypasses the stomach’s regulatory function in controlling the rate of nutrient entry into the small intestine, it must be administered continuously to prevent rapid intestinal delivery and dumping syndrome. Because post-pyloric feeding bypasses the stomach’s regulatory function in controlling the rate of nutrient entry into the small intestine, it must be administered continuously to prevent rapid intestinal delivery and dumping syndrome. This requirement further limits mobility and may affect QOL [44,47]. Current evidence does not show a clear advantage of post-pyloric over gastric feeding in pediatric SBS; practice varies, and ESPGHAN recommends individualized decision-making with gastric feeding as the default unless specific indications favor post-pyloric access [39,43,44,47].
Feeding Modality: Bolus vs Continuous.
Tube-based EN may be given as intermittent bolus, continuous, or mixed regimens. Continuous feeding prolongs luminal exposure, potentially enhancing absorption via transporter saturation and reduced osmotic load, and may reduce stool output and improve tolerance [27,50]. However, it eliminates fasting periods, which may impair motility and increase risks of small bowel bacterial overgrowth (SBBO) and IFALD [30,37,44]. No randomized trials directly compare continuous vs bolus EN in children with SBS; limited observational data suggest continuous feeding can improve tolerance, reduce stool volume, and support weight gain [51,52,53]. Adult SBS data indicate improved overall absorption with continuous vs oral/bolus feeding [54]. Bolus feeding mimics physiological meal–fast cycles, supporting normal gastric filling/emptying and stimulating motility; it may also promote bile flow and avoid continuous insulin secretion, potentially reducing hepatic steatosis and excess fat accretion [27,37]. In preterm infants, bolus feeding has been linked to better growth and tolerance [55], yet a meta-analysis did not show a consistent overall benefit over continuous feeding [56]. Given limited evidence, many centers employ bolus or mixed approaches tailored to anatomy, tolerance, clinical status, and goals [37,44].
Choice of Feed.
International guidelines (ASPEN, ESPGHAN, NASPGHAN, AGA) consistently recommend human breast milk as first-line EN for infants with SBS-associated IF [39,40,50]. Human milk (HM) provides long-chain fatty acids, free amino acids, growth factors, immunoglobulins, leukocytes, bioactive proteins (e.g., lactoferrin, lysozyme), cytokines, hormones (e.g., EGF), antimicrobial agents, immune and stem cells, and prebiotic oligosaccharides that collectively support mucosal growth/repair, immune function, microbiome development, and neurodevelopment [27,39,44,57,58]. This consensus is reflected in practice: an ERNICA survey reported 23/24 European centers use maternal milk as the primary regimen for infants with SBS-IF [43]. HM reduces necrotizing enterocolitis (NEC) in preterm infants [58], is associated with shorter PN duration [16], and may lower IFALD risk [59].
When maternal human milk (MHM) is unavailable, donor human milk (DHM) may be considered as an alternative for high-risk infants, including SBS-IF [27,57]. In very preterm and very low birth weight infants, DHM reduces NEC risk by ~50% compared with formula [60]. Although growth may be slower due to lower protein/energy after pasteurization, targeted fortification can achieve comparable growth while preserving protection against NEC [61]. In small bowel atresia or gastroschisis, DHM has been associated with shorter hospitalization and fewer central line days [62]. Despite reduced activity of some heat-labile components after pasteurization, DHM remains superior to formula for barrier maturation and microbiome profiles more similar to breastfeeding [63,64], and human milk oligosaccharides (HMOs) (e.g., 2′-fucosyllactose) may further augment adaptive responses after resection [65]. Pasteurization of DHM reduces the activity of several heat-sensitive components, including bile salt–stimulated lipase, lactoferrin, lysozyme, and some immunoglobulins, yet its protective benefits over formula are preserved, particularly regarding NEC risk [57,66,67,68]. In contrast, infant formula lacks the complex immunologic and trophic factors present in human milk and contains 3–5 times lower concentrations of HMOs, with markedly different compositional profiles [69,70]. Although DHM from accredited milk banks is considered low risk, with no serious adverse events causally linked in large biovigilance datasets [71,72], pasteurization does lead to nutrient loss, with protein content decreasing by up to 12% and fat by up to 25% [73,74]. Additionally, most DHM is produced by mothers of healthy term infants, and its composition may not fully meet the nutritional needs of preterm infants with SBS, including those with NEC.
Evidence to guide HM fortifier use in SBS is limited. Fortification increases osmolarity [75,76,77], which may worsen intolerance or may lead to metabolic acidosis in infants with compromised mucosa/absorption. If HM is unavailable or not tolerated, infant formula is the next option; optimal protein composition remains uncertain [37]. Animal models suggest polymeric formulas may increase diarrhea and prolong PN [78], whereas one clinical report associated AAFs with shorter PN duration [16]; however, a randomized trial of hydrolyzed vs non-hydrolyzed protein showed no differences in growth, energy intake, or nitrogen balance [13]. No clear advantage of EHFs over AAFs for adaptation has been demonstrated; a comparative review found no difference in time to enteral autonomy (EN) or PN duration across EHF-only, EHF + human milk, or AAF+HM regimens [18].
More complex proteins may theoretically enhance trophic signaling, yet reports describe possible associations between SBS and food-related immune responses, including cow’s-milk protein allergy (CMPA) [79,80] and noninfectious eosinophilic colitis [10,81,82]. Nevertheless, evidence remains limited: only two studies documented IgE-mediated CMPA in three pediatric SBS patients [79,80], and nonspecific postoperative symptoms may reflect intolerance rather than true allergy [83]. Routine avoidance of complex formulas is therefore not supported; individualized trials with careful monitoring are appropriate. Most EHF are lactose-free (exceptions exist, e.g., Nutrilon Pepti), which may be advantageous given reduced lactase activity in many infants with SBS due to proximal jejunal involvement [44,84]; however, the clinical relevance of universal lactose avoidance is uncertain. Adult SBS studies show similar tolerance between lactose-free diets and those containing up to ~20 g/day of lactose [85,86], though results may not extrapolate to early adaptation in infants.
Medium-chain triglycerides (MCTs) may improve fat absorption in rapid transit, bile acid depletion, or SBBO [44], but evidence is mixed. In one randomized trial, high-MCT formulas improved fat absorption with an intact colon but caused osmotic diarrhea without a colon [87]. Animal data suggest long-chain triglycerides (LCTs) may better stimulate adaptation than MCTs [88], implying very high-MCT formulas could blunt adaptive signaling. Consequently, choice between EHF and AAFs should be individualized based on anatomy (e.g., presence of colon), stool characteristics, growth needs, tolerance, and center experience.
Advancement of Enteral Feeding.
Early feeding practices vary widely [43]. Reported bolus advancement rates range from +1 mL/feed every 12 h in neonates [45] to 10–20 mL/kg/day [40,44]. For continuous feeding, descriptions range from +1 mL/h twice weekly [42] to +1–2 mL/h every 12 h [44]. Despite variability, most experts recommend advancing according to tolerance metrics-stool consistency, stoma output, and stool frequency-rather than fixed volumes [39,42,43,87]. Proposed upper limits for acceptable stool output vary from ~20 mL/kg/day (≈6 stools/day) to 40–50 mL/kg/day (≈10 stools/day) [39]. Decisions regarding rate and route of advancement should account for intestinal anatomy, gastroesophageal reflux/vomiting, stool/stoma patterns, and presence of feeding tubes [44]. Tolerance should be reassessed at least every 24 h, including stool volume/consistency, bloating, and any blood or mucus [30]. Feeds generally should not be advanced more than twice within that interval. Pharmacologic adjuncts (e.g., prokinetics, antidiarrheals) may improve tolerance in selected cases [44].
4.2. Enteral Nutrition at the Second Phase of SBS (Acute phase, Typically Lasts Weeks to 18 Months).
During the second phase of intestinal rehabilitation, feeding management in children with short bowel syndrome (SBS) has two principal objectives: (1) gradual escalation of EN with a parallel reduction of PN, and (2) stimulation of intestinal adaptation [26,27,28]. Solid foods are commonly introduced at 4–6 months corrected age to support oral motor development and mitigate aversion [89], with paced progression based on tolerance [7]. The efficiency of nutrients and fluid absorption is influenced by factors such as intestinal length, mucosal surface area, and the time nutrients remain in contact with the gut lining. Accordingly, nutritional approaches that help slow intestinal transit may improve absorption [44]. When tailoring the diet, it is important to account for the specific anatomy of the remaining bowel—including whether the colon is intact and how much jejunum or ileum remains, as well as the total length of functioning intestine [44].
Role of PN and Rationale for Progressive EN.
PN is life-saving in SBS and supports growth and neurodevelopment during severe malabsorption; it has contributed to improved survival over recent decades [26]. Nonetheless, prolonged PN is associated with complications, including CLABSIs, IFALD, vascular thrombosis, metabolic abnormalities, and organ dysfunction [26]. PN should therefore be titrated to the degree of enteral tolerance and reduced as EN advances. Rapid, enforced EN advancement in patients with markedly reduced residual bowel (less than one-third of expected length) may impair adaptation and precipitate dysmotility; a measured, tolerance-based approach is recommended [7,30,31].
Type of Enteral Nutrition
Second-phase feeding aims to provide adequate fluids, electrolytes, and calories for growth and neurodevelopment while supporting adaptation [44]. Given limited high-quality evidence, many centers rely on guiding principles based on expert consensus and clinical experience, rather than on formal standardized protocols [27,44].
Lipid composition.
Fat malabsorption is common in SBS due to reduced surface area, bile acid depletion, and relative pancreatic insufficiency. Nevertheless, dietary fat plays an important role in intestinal adaptation. Early introduction of a high-fat diet after resection promotes mucosal growth and villus lengthening [90,91], while low-fat diets are associated with impaired adaptation and poor weight gain [92,93]. MCTs can be useful in cholestasis or pancreatic insufficiency because they are absorbed without micellar solubilization and enter the portal system directly. However, formulas with >5% of total fat as MCT may increase stool output and limit advancement of enteral feeds [44]. A high-fat diet helps provide adequate calories without increasing feed volume [27], but may increase fecal losses of calcium, magnesium, copper, and zinc [94]. In patients with an intact colon, unabsorbed free fatty acids enhance oxalate absorption [95], raising the risk of hyperoxaluria and renal complications [36,44].
Carbohydrate quality.
Because simple sugars may exacerbate osmotic diarrhea in SBS, they should be limited [36]. Feeds that are starch-based rather than sugar-based are often better tolerated. In our experience, as well as in other centers, both artificial sweeteners and naturally occurring simple sugars can increase stool output, whether they are consumed in foods or present in compounded medications [36,44]. Lactose intake should be individualized based on tolerance. Children with proximal jejunal resection are more prone to lactose intolerance, and if symptoms occur, lactose-free or dairy-free alternatives can be recommended [36].
Soluble fibers (such as pectin or guar gum) may improve feeding tolerance by increasing viscosity, slowing intestinal transit, and serving as substrates for short-chain fatty acid (SCFA) production. Limited pediatric case data suggest they may help improve stool consistency and enhance nitrogen absorption [44,45,96,97]. For children without a colon, fiber may need to be reduced to limit stool bulk and ease emptying, and gas-producing foods may need to be restricted to reduce air accumulation in the ostomy bag [36].
Electrolyte and fluid considerations in older infants/children.
Fluid intake should be kept to the minimum necessary. Large intakes of free water without electrolytes should be avoided, as absorption is limited and may worsen diarrhea; small sips are preferred. Fluids should be consumed separately from meals to reduce nutrient malabsorption, as their rapid transit can increase stool losses and thereby worsen malabsorption when taken with food. To limit excess intake, some centers may offer ice chips or frozen oral rehydration solutions (ORS)/electrolyte popsicles [44]. Hyper-osmolar drinks (juice, soda, sweetened tea) should be avoided as they increase stool output and dehydration risk [36]. ORS is the preferred beverage for children with SBS; however, it is often poorly palatable, which may limit its acceptance. ORS should provide 20–25 g carbohydrate, 45–80 mEq/L sodium and have an osmolarity of ~300 mOsm [36].
Children with IF - especially those with stomas - are prone to total body sodium depletion [36,96,97,98], which can slow weight gain [98]. Low urine sodium (<10–30 mmol/L in a random urine sample) [36] may occur even with normal serum sodium levels. Sodium supplementation (enteral or parenteral) can improve growth [99]. Close monitoring of stoma output and sodium balance, including periodic urine sodium checks, is essential [7,100].
Hyperoxaluria.
In patients with ileal resection and colon in continuity, a low-oxalate, low-fat diet with high fluid intake is generally recommended to reduce the risk of hyperoxaluria [101,102]. In practice, further diet restriction can be challenging for patients who already limit simple carbohydrates. Many high-oxalate vegetables (e.g., celery, spinach, eggplant, green beans, okra, wax beans) are also low-sugar options commonly recommended for SBS, and several soluble, high-fiber legumes (such as chickpeas, green beans, kidney beans, and lentils) are likewise high in oxalate [36,44]. Potassium citrate may be used to reduce kidney stone formation but can increase stool output [44]. As noted earlier, dietary fat supports intestinal adaptation and should not be overly restricted, while fluid intake should be limited to prevent worsening diarrhea—yet kept sufficient to avoid dehydration [102]. Achieving this balance requires close clinical monitoring. A more practical approach is enteral calcium supplementation, which binds oxalate in the colon and reduces its absorption [45,101,102,103]. Additionally, because oral nutrition supplements and enteral formulas contain variable oxalate levels, attention should be paid to their oxalate content when selecting products [102].
Blenderized feeds.
Blenderized tube feeds (BTFs) are increasingly used as an alternative to commercial enteral formulas and have been associated with improvements in gastrointestinal tolerance (e.g., decreased reflux, gagging, retching, and feeding aversion), fewer hospitalizations for respiratory illnesses, and increased intestinal microbiome diversity [104]. However, evidence for their use in SBS remains limited. In a cohort of 58 children with SBS, of whom fewer than 10% were receiving PN, introducing BTFs to provide at least 5% of caloric intake was associated with improved stool consistency and gastrointestinal symptoms. Patients without an ICV or with colonic resection were more likely to experience weight loss [105]. Another small study of 12 children with intestinal failure reported a reduction in PN requirements after transitioning from amino acid or hydrolyzed formulas to BTFs [106]. Use of BTFs requires careful consideration: preparation is time-intensive, shelf life is short, enteral tubes may clog, and close dietitian oversight is necessary to ensure adequate macro- and micronutrient intake. Tube feeding formulas containing real food ingredients (TFRF) may offer a more standardized alternative. In a series of ten children with IF who had weaned off PN, TFRF use was associated with improved stool patterns [107]; however, palatability may limit oral use, making it more suitable for patients receiving full tube feeds. All available studies have been retrospective and uncontrolled, so further research is required to clarify the benefits and optimal use of BTF and real-food-based formulas in SBS.
4.3. Enteral Nutrition at the Third Phase of SBS (Maintenance phase, Typically Lasts from 18 -24 Months to Several Years).
The principal goal in the management of children with SBS during the third phase of intestinal rehabilitation is the achievement of EA. The process of weaning PN is complex and may take many years. Readiness to begin weaning from PN in pediatric patients is determined by a combination of clinical, nutritional, and biochemical criteria, with the overarching goal of ensuring sustained growth and nutritional adequacy through enteral or oral intake alone. Multiple factors influence the likelihood of achieving EA in children with SBS. Key predictors include residual small-bowel length and quality, presence of the ICV, remaining colonic length, gestational age, and underlying diagnosis (e.g., NEC as a positive predictor, gastroschisis as a negative one), as well as the absence of IFALD [108,109,110,111,112]. Additional factors associated with successful weaning include serum citrulline levels, enteral tolerance at six months post-resection, and consistent multidisciplinary follow-up [112]. Strong caregiver–provider relationships and good patient and caregiver adherence are also essential for achieving PN weaning [36].
The Parenteral Nutrition Dependence Index (PNDI)—the ratio of non-protein energy from HPN to resting energy expenditure using Schofield equations — provides a more accurate measure of intestinal sufficiency than enteral intake alone [113]. A PNDI >120% indicates very high PN dependence, 80–120% high dependence, and <80% mild dependence [114]. A recent study suggests that combining PNDI with serial citrulline levels may help predict PN weaning [115]. Belza et al. recently developed an SBS severity score to estimate the likelihood of achieving enteral autonomy. The score is based on four factors assessed six months after surgery: having >50% of expected small-bowel length remaining, presence of the ICV, conjugated bilirubin <34 µmol/L, and enteral intake >50% of total nutrition [116]. In infants with intestinal failure, lower PNDI% (e.g., 45% in weaned vs. 113% in not-weaned infants) and higher Belza scores at six months are both associated with successful weaning within 24 months [117].
Stepwise Weaning and Feeding Advancement.
EN should be advanced gradually, starting with small volumes and increasing as tolerated. Growth should be tracked using appropriate growth charts and z-scores, aiming for stable or improving weight and length/height. Tolerance is defined by the ability to increase enteral or oral feeds without significant vomiting, diarrhea, or other signs of malabsorption [118]. Laboratory tests should show stable electrolytes, glucose, renal function, and no major nutrient deficiencies or metabolic issues [111]. Close, individualized multidisciplinary follow-up is essential throughout the transition [27,111,119]. For PN weaning, some centers reduce the number of PN days per week [109,120], while others shorten daily PN infusion. There are no pediatric studies comparing these strategies. In adults, reducing PN days can improve quality of life and lower long-term complication rates, but it may also raise the risk of dehydration, electrolyte disturbances, and nutritional deficits if enteral or oral intake is inadequate [121,122].
Pharmacologic Support for PN Weaning.
Pharmacologic therapy can support nutrition management and aid PN weaning. Common agents include antisecretory drugs such as clonidine, antimotility medications like loperamide, prokinetics for delayed gastric emptying or motility disorders (e.g., in gastroschisis), and antibiotics for small-bowel bacterial overgrowth. Teduglutide, a GLP-2 analogue, may further enhance intestinal adaptation, reduce fluid losses, and decrease PN requirements [36,123].
Oral aversion.
Oral aversion is common in toddlers with SBS, especially those who rely on enteral tube feeding (ETF). Caregivers may avoid introducing new foods—particularly fruits—due to fear of diarrhea, while prolonged hospitalizations and fewer shared mealtime experiences limit normal social and developmental feeding opportunities [124]. This may result in limited dietary variety due to oral aversions. Additionally, early ETF as well as early prolonged periods of nil per os (NPO) have been thought to contribute to delayed acquisition of feeding skills in children with SBS-IF. Early ETF and long periods of NPO can delay acquisition of feeding skills, and late introduction of solids further increases the risk of oral aversion [111,125]. Oral feeding as opposed to ETF enhances acquisition of feeding skills, maintains self-regulation of hunger and satiety and enjoyment associated with eating, thus helps prevent feeding difficulties [111].
Establishing healthy eating behaviors requires active family involvement, including early safe oral experiences, oral-motor and sensorimotor interventions, offering developmentally appropriate foods, family mealtimes, and adjusting PN/EN schedules to allow participation in daily activities [117]. Effective implementation requires a coordinated multidisciplinary approach [124].
Nutritional status monitoring.
Micronutrient deficiencies are common—and often persist—after PN is discontinued, especially in children with SBS. Deficits in magnesium, calcium, fat-soluble vitamins (A, D, E, K), and vitamin B12 are frequently reported post-weaning [82,126,127]. Iron, zinc, selenium, and copper deficiencies are also prevalent; iron deficiency alone affects up to 61% of children after transitioning to full EN [127,128]. Children with intestinal failure are additionally at risk for essential fatty acid deficiency during PN weaning [129], and triene:tetraene ratio should be monitored. Close clinical, biochemical, and nutritional surveillance is required throughout PN weaning to prevent complications and ensure adequate growth. ASPEN and ESPGHAN recommend individualized monitoring based on age, underlying disease, and risk factors [118,127,130].
Hydration monitoring.
Caregivers should be taught how to track stool patterns and recognize early signs of dehydration—such as increased thirst, seeking extra fluids or salt, dark urine, fewer wet diapers, irritability, confusion, weakness, dizziness, fatigue, or excessive sleepiness [36].
Despite advances in care, evidence remains limited regarding the optimal strategy for PN weaning. Although mortality and intestinal transplantation rates have declined in recent years, the proportion of children achieving full EN has remained largely unchanged. A recent multicenter, retrospective study of 443 pediatric patients demonstrated a reduction in mortality and transplantation rates, yet no significant increase in EA attainment. The authors concluded that a growing proportion of children remain PN dependent, underscoring the need for new strategies to promote EA and improve long-term outcomes [8].
5. Conclusions
Nutritional management of children with short bowel syndrome remains variable and challenging. Although several small, randomized crossover studies in adults with SBS have examined different aspects of nutritional care, evidence to guide nutritional management in children with this complex condition remains scarce. Three phases of care typically emerge when considering appropriate nutritional support. During the first phase, EN administered orally or via a nasogastric tube-should be initiated whenever possible; however, PN remains the primary source of nutritional support, and advancement of enteral intake is generally gradual. While some studies favor continuous enteral feeding for patients with SBS, robust evidence to support this practice is still lacking. Feeding management during the second phase focuses on two key objectives: advancing enteral feeding and promoting intestinal adaptation. The use of specific nutrients has shown potential to enhance intestinal absorption and stimulate adaptive processes. The primary goal of the third phase is to achieve EA with concurrent weaning from PN, while ensuring appropriate weight gain and growth velocity. Management strategies in this stage rely largely on clinical experience rather than high-quality evidence.
Enteral nutrition remains a cornerstone of management in children with SBS. Multicenter, longitudinal studies are needed to strengthen the evidence base, refine therapeutic strategies, support centralized management, improve patient outcomes, and address existing knowledge gaps.
Author Contributions
Igor Sukhotnik and Inna Spector Cohen contributed to the conception and design of the review; to the acquisition and analysis of the data, and to original draft preparation. Hadar Moran-Lev, Reut Levi and Hofit Golden contributed to the design of the review; to reviewing and editing of the manuscript. All authors critically revised the manuscript, agreed to be fully accountable for ensuring the integrity and accuracy of the work, and read and approved the final manuscript.
Financial disclosure
None declared.
Institutional Review Board Statement
Ethical review and approval were waived for this study as it was a review of existing literature and did not involve the collection of new data from human subjects. Therefore, no direct contact with human participants was required, and there was no risk of harm or breach of confidentiality.
Informed Consent Statement
Patient consent was waived as this study did not involve the collection of new data from human subjects.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Modi, B.P.; Galloway, D.P.; Gura, K.; Nucci, A.; Plogsted, S.; Tucker, A.; Wales, P.W. ASPEN definitions in pediatric intestinal failure. JPEN J. Parenter. Enter. Nutr. 2022, 46, 42–59. [CrossRef]
- Duggan, C.P.; Jaksic, T. Pediatric intestinal failure. N. Engl. J. Med. 2017, 377, 666–675.
- Diamond, I.R.; de Silva, N.; Pencharz, P.B.; Kim, J.H.; Wales, P.W.; Group for the Improvement of Intestinal Function and Treatment. Neonatal short bowel syndrome outcomes after the establishment of the first Canadian multidisciplinary program. J. Pediatr. Surg. 2007, 42, 806–811.
- Premkumar, M.H.; Soraisham, A.; Bagga, N.; Massieu, L.A.; Maheshwari, A. Nutritional management of short bowel syndrome. Clin. Perinatol. 2022, 49, 557–572. [CrossRef]
- Lönnerdal, B. Bioactive proteins in human milk—Potential benefits for preterm infants. Clin. Perinatol. 2017, 44, 179–191. [CrossRef]
- Jaksic, T. Current short bowel syndrome management: An era of improved outcomes and continued challenges. J. Pediatr. Surg. 2023, 58, 789–798. [CrossRef]
- Scolapio, J.S.; Fleming, C.R. Short bowel syndrome. Gastroenterol. Clin. North Am. 1998, 27, 467–479.
- Gattini, D.; Roberts, A.J.; Wales, P.W.; et al. Trends in pediatric intestinal failure: A multicenter, multinational study. J. Pediatr. 2021, 237, 16–23.e4. [CrossRef]
- Bines, J.E.; Taylor, R.G.; Justice, F.; et al. Influence of diet complexity on intestinal adaptation. J. Gastroenterol. Hepatol. 2002, 17, 1170–1179. [CrossRef]
- Arai, Y.; Kinoshita, Y.; Kobayashi, T.; et al. A rare case of eosinophilic gastrointestinal disorders with short bowel syndrome after strangulated obstruction. Surg. Case Rep. 2022, 8, 168. [CrossRef]
- Goulet, O.; Abi Nader, E.; Pigneur, B.; Lambe, C. Short bowel syndrome as the leading cause of intestinal failure in early life. Pediatr. Gastroenterol. Hepatol. Nutr. 2019, 22, 303–329. [CrossRef]
- Bines, J.; Francis, D.; Hill, D. Reducing parenteral requirement with amino acid–based formula. J. Pediatr. Gastroenterol. Nutr. 1998, 26, 123–128.
- Ksiazyk, J.; Piena, M.; Kierkus, J.; Lyszkowska, M. Hydrolyzed versus nonhydrolyzed protein diet in children with short bowel syndrome. J. Pediatr. Gastroenterol. Nutr. 2002, 35, 615–618.
- Shores, D.R.; Bullard, J.E.; Aucott, S.W.; et al. Implementation of feeding guidelines in infants at risk of intestinal failure. J. Perinatol. 2015, 35, 941–948. [CrossRef]
- De Greef, E.; Mahler, T.; Janssen, A.; et al. Influence of Neocate in pediatric short bowel syndrome on PN weaning. J. Nutr. Metab. 2010, 2010, 297575. [CrossRef]
- Andorsky, D.J.; Lund, D.P.; Lillehei, C.W.; Jaksic, T.; Dicanzio, J.; Richardson, D.S.; Collier, S.B.; Lo, C.; Duggan, C. Nutritional and Other Postoperative Management of Neonates with Short Bowel Syndrome Correlates with Clinical Outcomes. J. Pediatr. 2001, 139, 27–33. [CrossRef]
- van Goudoever, J.B.; Carnielli, V.; Darmaun, D.; et al. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Amino acids. Clin. Nutr. 2018, 37, 2315–2323. [CrossRef]
- Capriati, T.; Nobili, V.; Stronati, L.; Cucchiara, S.; Laureti, F.; Liguori, A.; Tyndall, E.; Diamanti, A. Enteral nutrition in pediatric intestinal failure: impact of initial feeding on adaptation. Expert Rev. Gastroenterol. Hepatol. 2017, 11, 741–748.
- Tappenden, K.A. Anatomical and physiological considerations in short bowel syndrome. Nutr. Clin. Pract. 2023, 38(Suppl. 1), S27–S34. [CrossRef]
- Le Beyec, J.; Billiauws, L.; Bado, A.; Joly, F.; Le Gall, M. Short bowel syndrome: A paradigm for intestinal adaptation. Annu. Rev. Nutr. 2020, 40, 299–321. [CrossRef]
- Venick, R.S. Predictors of intestinal adaptation in children. Gastroenterol. Clin. North Am. 2019, 48, 499–511. [CrossRef]
- Tappenden, K.A. Mechanisms of enteral nutrient-enhanced intestinal adaptation. Gastroenterology 2006, 130(Suppl. 1), S93–S99. [CrossRef]
- Sukhotnik, I.; Siplovich, L.; Shiloni, E.; et al. Intestinal adaptation in infants and children with SBS. Pediatr. Surg. Int. 2002, 18, 258–263.
- Pironi, L. Definition, classification, and causes of short bowel syndrome. Nutr. Clin. Pract. 2023, 38(Suppl. 1), S9–S16. [CrossRef]
- Pironi, L. Definitions of intestinal failure and short bowel syndrome. Best Pract. Res. Clin. Gastroenterol. 2016, 30, 173–185. [CrossRef]
- Muto, M.; Kaji, T.; Onishi, S.; et al. Current management of pediatric short-bowel syndrome. Surg. Today 2022, 52, 12–21.
- Puoti, M.G.; Köglmeier, J. Nutritional management of intestinal failure due to short bowel syndrome in children. Nutrients 2023, 15, 62. [CrossRef]
- Sondheimer, J.M.; Cadnapaphornchai, M.; Sontag, M.; Zerbe, G.O. Predicting PN duration after neonatal intestinal resection. J. Pediatr. 1998, 132, 80–84.
- Tappenden, K.A. Intestinal adaptation following resection. JPEN J. Parenter. Enter. Nutr. 2014, 38(Suppl. 1), 23S–31S. [CrossRef]
- Eshel Fuhrer, A.; Sukhotnik, S.; Moran-Lev, H.; et al. Motility disorders in children with intestinal failure. Pediatr. Surg. Int. 2022, 38, 1737–1743. [CrossRef]
- Hukkinen, M.; Mutanen, A.; Pakarinen, M.P. Small bowel dilation and risk of mucosal injury in SBS. Surgery 2017, 162, 670–679.
- Tricco, A.C.; Lillie, E.; Zarin, W.; et al. PRISMA-ScR extension. Ann. Intern. Med. 2018, 169, 467–473.
- von Elm, E.; Altman, D.G.; Egger, M.; et al. STROBE statement. Int. J. Surg. 2014, 12, 1495–1499.
- Moola, S.; Munn, Z.; Tufanaru, C.; et al. Systematic reviews of etiology and risk. In JBI Manual for Evidence Synthesis. 2020.
- Tyson, J.E.; Kennedy, K.A. Minimal enteral feeding for feeding tolerance. Cochrane Database Syst. Rev. 1997, CD000504.
- Bobo, E.; King, L.M. Techniques for advancing feeds in pediatric intestinal failure. Nutr. Clin. Pract. 2025, 40, 1000–1012.
- Goulet, O.; Olieman, J.; Ksiazyk, J.; et al. Neonatal short bowel syndrome as a model of intestinal failure. Clin. Nutr. 2013, 32, 162–171. [CrossRef]
- Moltu, S.J.; Bronsky, J.; Embleton, N.; et al. Nutritional management of the critically ill neonate. J. Pediatr. Gastroenterol. Nutr. 2021, 73, 274–289. [CrossRef]
- Norsa, L.; Goulet, O.; Alberti, D.; et al. Nutrition and intestinal rehabilitation of children with SBS: Part 1. J. Pediatr. Gastroenterol. Nutr. 2023, 77, 281–297.
- Iyer, K.; DiBaise, J.K.; Rubio-Tapia, A. AGA clinical practice update on SBS. Clin. Gastroenterol. Hepatol. 2022, 20, 2185–2194.e2.
- Olieman, J.; Kastelijn, W. Nutritional feeding strategies in pediatric intestinal failure. Nutrients 2020, 12, 177. [CrossRef]
- Olieman, J.F.; Penning, C.; IJsselstijn, H.; et al. Enteral nutrition in children with short-bowel syndrome. J. Am. Diet. Assoc. 2010, 110, 420–426. [CrossRef]
- Verlato, G.; Hill, S.; Jonkers-Schuitema, C.; et al. International survey on feeding in infants with SBS. J. Pediatr. Gastroenterol. Nutr. 2021, 73, 647–653.
- Avitzur, Y.; Courtney-Martin, G. Enteral approaches in malabsorption. Best Pract. Res. Clin. Gastroenterol. 2016, 30, 295–307. [CrossRef]
- Parvadia, J.K.; Keswani, S.G.; Vaikunth, S.; et al. VEGF and bowel adaptation. Am. J. Physiol. Gastrointest. Liver Physiol. 2007, 293, G591–G598.
- Micic, D.; Martin, J.A.; Fang, J. AGA clinical update on endoscopic enteral access. Gastroenterology 2025, 168, 164–168.
- Channabasappa, N.; Girouard, S.; Nguyen, V.; Piper, H. Enteral Nutrition in Pediatric Short-Bowel Syndrome. Nutrition in Clinical Practice 2020, 35, 848–854. [CrossRef]
- Mehta, N.M.; Skillman, H.E.; Irving, S.Y.; et al. Nutrition support in pediatric critical illness. JPEN J. Parenter. Enter. Nutr. 2017, 41, 706–742.
- Michaud, L.; Coopman, S.; Guimber, D.; et al. Percutaneous gastrojejunostomy in children. Arch. Dis. Child. 2012, 97, 733–734. [CrossRef]
- Braegger, C.; Decsi, T.; Dias, J.A.; et al. ESPGHAN comment on pediatric enteral nutrition. J. Pediatr. Gastroenterol. Nutr. 2010, 51, 110–122.
- Parker, P.; Stroop, S.; Greene, H. Continuous vs intermittent feeding in infants with intestinal disease. J. Pediatr. 1981, 99, 360–364.
- Levy, E.; Frileux, P.; Sandrucci, S.; et al. Continuous enteral nutrition during early adaptation in SBS. Br. J. Surg. 1988, 75, 549–553.
- Weizman, Z.; Schmueli, A.; Deckelbaum, R.J. Continuous nasogastric elemental feeding for prolonged diarrhea. Am. J. Dis. Child. 1983, 137, 253–255.
- Joly, F.; Dray, X.; Corcos, O.; Barbot, L.; Kapel, N.; Messing, B. Tube Feeding Improves Intestinal Absorption in Short Bowel Syndrome Patients. Gastroenterology 2009, 136, 824–831. [CrossRef]
- Schanler, R.J.; Shulman, R.J.; Lau, C.; Smith, E.O.; Heitkemper, M.M. Feeding strategies for premature infants: randomized trial of GI priming and tube-feeding method. Pediatrics 1999, 103, 434–439.
- Premji, S.S.; Chessell, L. Continuous nasogastric milk feeding versus intermittent bolus feeding for premature infants <1500 g. Cochrane Database Syst. Rev. 2002, CD001819.
- Parker, M.G.; Stellwagen, L.M.; Noble, L.; Kim, J.H.; Poindexter, B.B.; Puopolo, K.M. Promoting human milk and breastfeeding for the very low birth weight infant. Pediatrics 2021, 148, e2021054272. [CrossRef]
- Manea, A.; Boia, M.; Iacob, D.; Dima, M.; Iacob, R.E. Benefits of early enteral nutrition in extremely low birth weight infants. Singapore Med. J. 2016, 57, 616–618. [CrossRef]
- Kulkarni, S.; Mercado, V.; Rios, M.; Arboleda, R.; Gomara, R.; Muinos, W.; Reeves-Garcia, J.; Hernandez, E. Breast milk vs formula in preventing PN-associated liver disease. J. Pediatr. Gastroenterol. Nutr. 2013, 57, 383–388.
- Quigley, M.; Embleton, N.D.; Meader, N.; McGuire, W. Donor human milk for preventing NEC in very preterm infants. Cochrane Database Syst. Rev. 2024, CD002971.
- Li, Y.; Chi, C.; Li, C.; Song, J.; Song, Z.; Wang, W.; Sun, J. Efficacy of donated milk in early nutrition of preterm infants: A meta-analysis. Nutrients 2022, 14, 1724. [CrossRef]
- Hoban, R.; Khatri, S.; Patel, A.; Unger, S.L. Supplementation of mother’s own milk with donor milk in infants with gastroschisis or intestinal atresia. Nutrients 2020, 12, 589. [CrossRef]
- Roskes, L.; Chamzas, A.; Ma, B.; Medina, A.E.; Gopalakrishnan, M.; Viscardi, R.M.; Sundararajan, S. Early human milk feeding: intestinal barrier maturation and growth. Pediatr. Res. 2025, 97, 2065–2073.
- Parra-Llorca, A.; Gormaz, M.; Alcántara, C.; Cernada, M.; Nuñez-Ramiro, A.; Vento, M.; Collado, M.C. Preterm gut microbiome depending on feeding type: significance of donor milk. Front. Microbiol. 2018, 9, 1376. [CrossRef]
- Mezoff, E.A.; Hawkins, J.A.; Ollberding, N.J.; Karns, R.; Morrow, A.L.; Helmrath, M.A. 2’-Fucosyllactose augments adaptive response to intestinal resection. Am. J. Physiol. Gastrointest. Liver Physiol. 2016, 310, G427–G438.
- Burge, K.; Vieira, F.; Eckert, J.; Chaaban, H. Lipid composition and absorption differences among neonatal feeding strategies. Nutrients 2021, 13, 1–19.
- Peila, C.; Moro, G.E.; Bertino, E.; et al. Effect of Holder pasteurization on donor human milk nutrients and bioactive components. Nutrients 2016, 8, 477.
- Colaizy, T.T. Effects of milk banking procedures on donor human milk components. Semin. Perinatol. 2021, 45, 151382.
- Cheng, L.; Akkerman, R.; Kong, C.; Walvoort, M.T.C.; de Vos, P. Human milk oligosaccharides as essential bioactive molecules. Crit. Rev. Food Sci. Nutr. 2021, 61, 1184–1200. [CrossRef]
- Liu, F.; van der Molen, J.; Kuipers, F.; van Leeuwen, S.S. Quantitation of bioactive components in infant formulas. Food Res. Int. 2023, 174, 113589.
- Clifford, V.; Klein, L.D.; Brown, R.; et al. Donor and recipient safety in human milk banking. J. Paediatr. Child Health 2022, 58, 1629–1634. [CrossRef]
- Coutsoudis, I.; Adhikari, M.; Nair, N.; Coutsoudis, A. Feasibility of donor breastmilk bank in resource-limited neonatal units. BMC Public Health 2011, 11, 356.
- Adhisivam, B., Vishnu Bhat, B., Rao, K., Kingsley, S.M., Plakkal, N., Palanivel, C. Effect of Holder pasteurization on macronutrients and immunoglobulin profile of pooled donor human milk. J, Matern, Fetal, Neonatal, Med. 2019,32(18):3016-3019. [CrossRef]
- Piemontese, P., Mallardi, D., Liotto, N., Tabasso, C., Menis, C., Perrone, M., Roggero, P., Mosca, F. Macronutrient content of pooled donor human milk before and after Holder pasteurization. BMC. Pediatr. 2019, 19(1):58. [CrossRef]
- Kreissl, A.; Zwiauer, V.; Repa, A.; et al. Effect of fortifiers and protein on human milk osmolarity. J. Pediatr. Gastroenterol. Nutr. 2013, 57, 432–437.
- Chinnappan, A.; Sharma, A.; Agarwal, R.; Thukral, A.; Deorari, A.; Sankar, M.J. Breast milk fortification with preterm formula vs HMF. JAMA Pediatr. 2021, 175, 790.
- Herranz Barbero, A.; Rico, N.; Oller-Salvia, B.; et al. Fortifier selection and dosage enables control of breast milk osmolarity. PLoS One 2020, 15, e0233924. [CrossRef]
- Hua, Z.; Turner, J.M.; Mager, D.R.; et al. Polymeric vs elemental formula in neonatal piglets with SBS. JPEN J. Parenter. Enter. Nutr. 2014, 38, 498–506.
- El Hassani, A.; Michaud, L.; Chartier, A.; et al. Cow’s milk protein allergy after neonatal intestinal surgery. Arch. Pediatr. 2005, 12, 134–139.
- Diamanti, A.; Fiocchi, A.G.; Capriati, T.; et al. Cow’s milk allergy and neonatal SBS. Eur. J. Clin. Nutr. 2015, 69, 102–106.
- Stamm, D.A.; Hait, E.; Litman, H.J.; Mitchell, P.D.; Duggan, C. High prevalence of eosinophilic GI disease in intestinal failure. J. Pediatr. Gastroenterol. Nutr. 2016, 63, 336–339.
- Masumoto, K.; Esumi, G.; Teshiba, R.; et al. Cow’s milk allergy in extremely short bowel syndrome. e-SPEN 2008, 3, e147–e150.
- Neelis, E.G.; Olieman, J.F.; Hulst, J.M.; et al. Promoting intestinal adaptation by nutrition and medication. Best Pract. Res. Clin. Gastroenterol. 2016, 30, 249–261. [CrossRef]
- Matarese, L.E. Nutrition and fluid optimization for short bowel syndrome. JPEN J. Parenter. Enter. Nutr. 2013, 37, 161–170.
- Arrigoni, E.; Marteau, P.; Briet, F.; et al. Lactose tolerance and absorption in short bowel syndrome. Am. J. Clin. Nutr. 1994, 60, 926–929.
- Marteau, P.; Messing, B.; Arrigoni, E.; et al. Do SBS patients need a lactose-free diet? Nutrition 1997, 13, 13–16.
- Jeppesen, P.B.; Mortensen, P.B. Influence of preserved colon on medium-chain fat absorption. Gut 1998, 43, 478–483.
- Vanderhoof, J.A.; Grandjean, C.J.; Kaufman, S.S.; et al. High–medium-chain triglyceride diet and mucosal adaptation. JPEN J. Parenter. Enter. Nutr. 1984, 8, 685–689.
- Fewtrell, M.; Bronsky, J.; Campoy, C.; et al. Complementary feeding: ESPGHAN guidelines. J. Pediatr. Gastroenterol. Nutr. 2017, 64, 119–132.
- Sukhotnik, I.; Mor-Vaknin, N.; Drongowski, R.A.; et al. Effect of dietary fat on intestinal adaptation in SBS rats. Pediatr. Surg. Int. 2004, 20, 419–424.
- Choi, P.M.; Sun, R.C.; Guo, J.; Erwin, C.R.; Warner, B.W. High-fat diet enhances villus growth after massive resection. J. Gastrointest. Surg. 2014, 18, 286–294.
- Sukhotnik, I.; Shiloni, E.; Krausz, M.M.; et al. Low-fat diet impairs postresection adaptation. J. Pediatr. Surg. 2003, 38, 1182–1187.
- Sukhotnik, I.; Gork, A.S.; Chen, M.; et al. Low-fat diet and fatty-acid transport after resection. Pediatr. Surg. Int. 2001, 17, 259–264.
- Ovesen, L.; Chu, R.; Howard, L. Influence of dietary fat on jejunostomy output in severe SBS. Am. J. Clin. Nutr. 1983, 38, 270–277.
- Schaefer, J.T.; Schulz-Heise, S.; Rueckel, A.; et al. Enteric hyperoxaluria in pediatric SBS. Front. Pediatr. 2023, 11, 1157696.
- Atia, A.; Girard-Pipau, F.; Hébuterne, X.; et al. Macronutrient absorption in SBS with jejunocolonic anastomosis. JPEN J. Parenter. Enter. Nutr. 2011, 35, 229–240.
- Drenckpohl, D.; Hocker, J.; Shareef, M.; et al. Green beans resolving diarrhea after neonatal bowel surgery: case study. Nutr. Clin. Pract. 2005, 20, 674–677.
- Brindle, M.E.; McDiarmid, C.; Short, K.; et al. ERAS guidelines for neonatal intestinal surgery. World J. Surg. 2020, 44, 2482–2492.
- O’Neil, M.; Teitelbaum, D.H.; Harris, M.B. Sodium depletion and poor weight gain in ileostomy patients. Nutr. Clin. Pract. 2014, 29, 397–401.
- Schwarz, K.B.; Ternberg, J.L.; Bell, M.J.; Keating, J.P. Sodium needs in infants with ileostomy. J. Pediatr. 1983, 102, 509–513.
- Hoppe, B.; Leumann, E.; von Unruh, G.; et al. Diagnostic and therapeutic approaches in secondary hyperoxaluria. Front. Biosci. 2003, 8, e437–e443.
- Adler, M.; Millar, E.C.; Deans, K.A.; Torreggiani, M.; Moroni, F. Nutrition and CKD-related hyperoxaluria in SBS. Nutrients 2022, 14, 3441.
- Sundaram, A.; Koutkia, P.; Apovian, C.M. Nutritional management of short bowel syndrome in adults. Curr. Opin. Clin. Nutr. Metab. Care 2002, 5, 267–275. [CrossRef]
- Weston, S.; Algotar, A.; Karjoo, S.; et al. State-of-the-art review of blenderized diets. J. Pediatr. Gastroenterol. Nutr. 2025, 81, 376–386.
- Zong, W.; Troutt, R.; Merves, J. Blenderized enteral nutrition in pediatric short gut syndrome. Nutr. Clin. Pract. 2022, 37, 913–920. [CrossRef]
- DePaula, B.; Mitchell, P.D.; Reese, E.; Gray, M.; Duggan, C.P. Parenteral nutrition dependence and growth in pediatric intestinal failure after transition to blenderized feeds: case series. Nutr. Clin. Pract. 2025, 40, 188–194.
- Samela, K.; Mokha, J.; Emerick, K.; Davidovics, Z.H. Transition to real-food ingredient tube formulas in pediatric intestinal failure. Nutr. Clin. Pract. 2017, 32, 277–281.
- Gutierrez, I.M.; Kang, K.H.; Jaksic, T. Neonatal short bowel syndrome. Semin. Fetal Neonatal Med. 2011, 16, 157–163. [CrossRef]
- Hill, S. Practical management of home parenteral nutrition in infancy. Early Hum. Dev. 2019, 138, 104876. [CrossRef]
- Enman, M.A.; Wilkinson, L.T.; Meloni, K.B.; Shroyer, M.C.; Jackson, T.F.; Aban, I.; Dimmitt, R.A.; Martin, C.A.; Galloway, D.P. Determinants of enteral autonomy and reduced PN exposure in pediatric intestinal failure. JPEN J. Parenter. Enter. Nutr. 2020, 44, 1263–1270.
- Norsa, L.; Goulet, O.; Alberti, D.; et al. Nutrition and intestinal rehabilitation in children with SBS: Part 2, long-term follow-up on home PN. J. Pediatr. Gastroenterol. Nutr. 2023, 77, 298–314.
- Khan, F.A.; Squires, R.H.; Litman, H.J.; et al. Predictors of enteral autonomy in pediatric intestinal failure: multicenter cohort. J. Pediatr. 2015, 167, 29–34.e1.
- Schofield, W.N. Predicting basal metabolic rate, new standards and review of previous work. Human Nutrition: Clinical Nutrition.1985, 39 Suppl 1: 5–41.
- Abi Nader, E.; Lambe, C.; Talbotec, C.; Acramel, A.; Pigneur, B.; Goulet, O. Metabolic bone disease in pediatric intestinal failure is not associated with PN dependency. Clin. Nutr. 2021, 40, 1974–1982.
- Proli, F.; Faragalli, A.; Talbotec, C.; Bucci, A.; Zemrani, B.; Chardot, C.; Abi Nader, E.; Goulet, O.; Lambe, C. Plasma citrulline variation predicts PN-weaning in neonatal short bowel syndrome. Clin. Nutr. 2021, 40, 4941–4947.
- Belza, C.; Fitzgerald, K.; de Silva, N.; Avitzur, Y.; Wales, P.W. Early predictors of enteral autonomy in pediatric intestinal failure: development of a severity scoring tool. JPEN J. Parenter. Enter. Nutr. 2019, 43, 961–969.
- Roggero, P.; Liotto, N.; Piemontese, P.; Menis, C.; Perrone, M.; Tabasso, C.; et al. Neonatal intestinal failure: growth pattern and nutrition during PN weaning. JPEN J. Parenter. Enter. Nutr. 2023, 47, 236–244.
- Worthington, P.; Balint, J.; Bechtold, M.; Bingham, A.; Chan, L.N.; Durfee, S.; Jevenn, A.K.; Malone, A.; Mascarenhas, M.; Robinson, D.T.; et al. When is parenteral nutrition appropriate? JPEN J. Parenter. Enter. Nutr. 2017, 41, 324–377.
- Tannuri, U.; Barros, F. de; Tannuri, A.C.A. Treatment of short bowel syndrome in children: value of intestinal rehabilitation program. Rev. Assoc. Med. Bras. 2016, 62, 575–583. [CrossRef]
- Puntis, J.W.L.; Hojsak, I.; Ksiazyk, J.; Braegger, C.; Bronsky, J.; Cai, W.; Carnielli, V.; Darmaun, D.; Decsi, T.; et al. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: organizational aspects. Clin. Nutr. 2018, 37, 2392–2400. [CrossRef]
- Stanner, H.; Zelig, R.; Rigassio Radler, D. Impact of infusion frequency on quality of life in home PN patients. JPEN J. Parenter. Enter. Nutr. 2022, 46, 757–770.
- Dibaise, J.K.; Matarese, L.E.; Messing, B.; Steiger, E. Strategies for PN weaning in adult SBS. J. Clin. Gastroenterol. 2006, 40(Suppl. 2), S94–S98.
- Kaenkumchorn, T.K.; Lampone, O.; Huebner, K.; Cramer, J.; Karls, C. When PN is the answer: pediatric intestinal rehabilitation case series. Nutr. Clin. Pract. 2024, 39, 991–1002.
- Hopkins, J.; Cermak, S.A.; Merritt, R.J. Oral feeding difficulties in children with short bowel syndrome: narrative review. Nutr. Clin. Pract. 2018, 33, 99–106. [CrossRef]
- Boctor, D.L.; Jutteau, W.H.; Fenton, T.R.; Shourounis, J.; Galante, G.J.; Eicher, I.; Goulet, O.; Lambe, C. Feeding difficulties and risk factors in pediatric intestinal failure. Clin. Nutr. 2021, 40, 5399–5406.
- Ubesie, A.C.; Kocoshis, S.A.; Mezoff, A.G.; Henderson, C.J.; Helmrath, M.A.; Cole, C.R. Multiple micronutrient deficiencies during and after transition to enteral nutrition. J. Pediatr. 2013, 163, 1692–1696.
- Neelis, E.; Olieman, J.; Rizopoulos, D.; Wijnen, R.; Rings, E.; de Koning, B.; Hulst, J. Growth, body composition, and micronutrient abnormalities after weaning off home PN. J. Pediatr. Gastroenterol. Nutr. 2018, 67, e95–e100.
- Tuokkola, J.; Olkkonen, E.; Gunnar, R.; Pakarinen, M.; Merras-Salmio, L. Vitamin and trace element status in children with SBS being weaned off PN. J. Pediatr. Gastroenterol. Nutr. 2025, 80, 318–325.
- Gunnar, R.; Lumia, M.; Pakarinen, M.; Merras-Salmio, L. Essential fatty acid deficiency risk during intestinal rehabilitation. JPEN J. Parenter. Enter. Nutr. 2018, 42, 1203–1210.
- Durfee, S.M.; Adams, S.C.; Arthur, E.; Corrigan, M.L.; Hammond, K.; Kovacevich, D.S.; McNamara, K.; Pasquale, J.A. A.S.P.E.N. standards for nutrition support: home and alternate site care. Nutr. Clin. Pract. 2014, 29, 542–555.
Figure 1.
Anatomical types of SBS according to the presence or absence of a small-bowel ostomy, preservation of the ileocecal valve, and colonic continuity.
Figure 1.
Anatomical types of SBS according to the presence or absence of a small-bowel ostomy, preservation of the ileocecal valve, and colonic continuity.
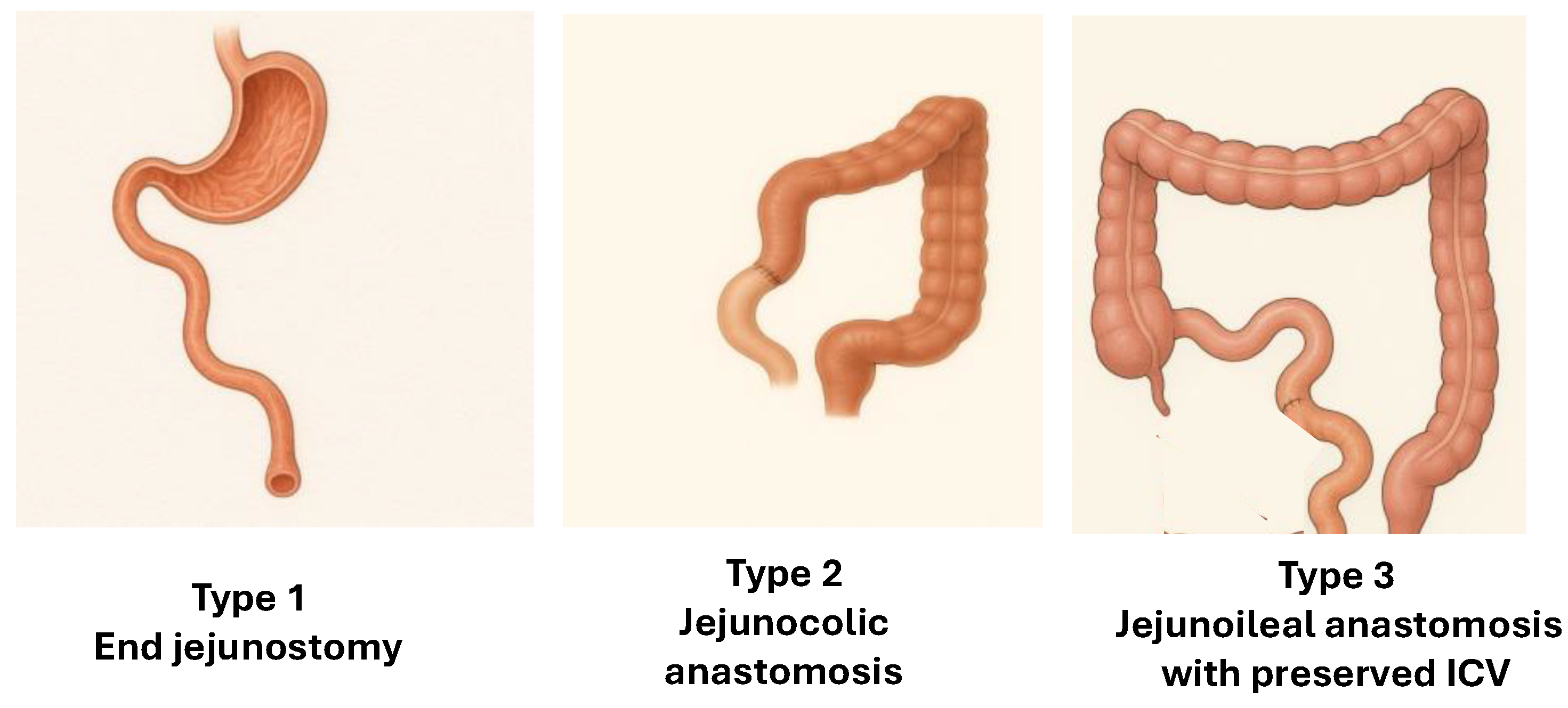
Figure 3.
Key postoperative phases of SBS.
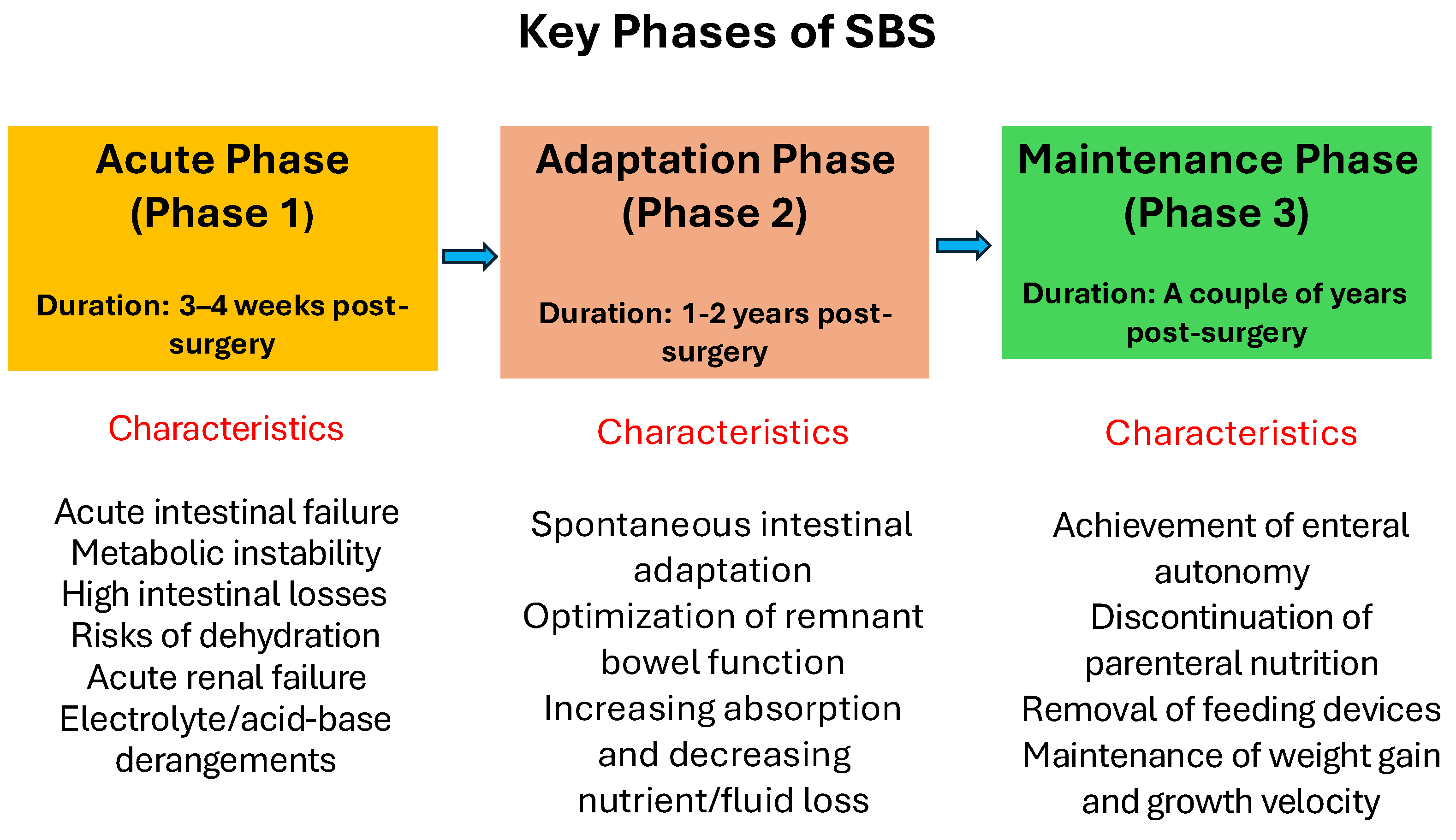

Table 1.
Inclusion and Exclusion Criteria According to the PICOS Model.
| PICOS Category | Inclusion Criteria | Exclusion Criteria |
| P (Population) | Neonates, infants, and older children with SBS | Children with intestinal failure due to motility disorders; children with SBS >5 years of follow-up |
| I (Intervention) | Full-text papers, including RCTs, prospective cohort, analytical cross-sectional, case–control, longitudinal, case series, and retrospective cross-sectional studies | Studies using incompatible virtual methods; studies primarily focused on medical or surgical management of SBS |
| C (Comparators) | Studies comparing outcomes of nutritional management during different SBS phases or between anatomical SBS types | Studies comparing nutritional management in children vs. adults with SBS |
| O (Outcomes) | Survival, achievement of EA (weaning off PN), and complication rates | Incomplete results |
| S (Study Design) | Studies published in English between January 1974 and December 2024, indexed in PubMed, Scopus, Web of Science, CENTRAL, SciELO, and Google Scholar | Duplicates, conference papers, abstracts, and non-English case reports |
Abbreviations: SBS, short bowel syndrome; RCT, randomized controlled study; EA, enteral autonomy; PN, parenteral nutrition; CENTRAL, Cochrane Central Register of Controlled Trials; SciELO, Scientific Electronic Library Online.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



