Submitted:
04 December 2025
Posted:
05 December 2025
You are already at the latest version
Abstract
Background/Objectives: Caring for a child with Autism Spectrum Disorder (ASD) is often associated with elevated psychological distress and reduced life satisfaction. Mindfulness-based interventions may offer substantial benefits by enhancing emotional regulation, reducing maladaptive cognitive patterns, and strengthening mindful parenting. This randomized controlled trial (RCT) examined the effectiveness of an eight-week Mindfulness-Based Cognitive Therapy (MBCT) program, enriched with mindful parenting practices, on parental mental health and parent-reported child behavior outcomes. Methods: Fifty-six parents of children with ASD were randomly assigned to an MBCT intervention group (n = 30) or a waitlist-control group (n = 26). Participants completed assessments at baseline (T0), post-intervention (T1), and one-month follow-up (T2), including the DASS-21, PANAS, and SWLS. Parents rated the overall severity of their child’s behavior problems to explore indirect treatment effects. Results: All participants receiving MBCT (100%) completed the program successfully and reported high acceptability. At baseline, no significant differences were observed between groups. Compared to controls, the MBCT group demonstrated significant reductions in depression, anxiety, and stress, alongside increases in positive affect and life satisfaction at T1. These improvements were further strengthened or maintained at T2. However, the control group showed no significant changes across time. Additionally, parents in the MBCT group reported indirect improvements in their children’s behavioral adjustment at T1 and T2. Conclusions: Findings demonstrate that MBCT constitutes an effective intervention for reducing parental psychopathology and indirectly enhancing child positive behavior, emphasizing the importance of incorporating mindfulness and mindful parenting components into family-centered interventions for parents of children with ASD.
Keywords:
Mindfulness-Based Cognitive Therapy (MBCT)
; mindful parenting
; Autism Spectrum Disorder (ASD)
; parental mental health
; parenting stress
; child behavior
; family
; development
; psychopathology
1. Introduction
1.1. Parental Mental Health of Children with Autism Spectrum Disorder
Autism Spectrum Disorder (ASD) is a multifactorial and lifelong neurodevelopmental disability that not only affects the individuals diagnosed but also imposes substantial and persistent mental health challenges on their families. The core features of ASD—difficulties in social communication and interaction, along with restricted and repetitive patterns of behavior—often lead to considerable limitations in functional independence and sustained caregiving demands across the lifespan [1,2]. As many individuals with ASD require ongoing specialized health, educational, and rehabilitation services, a substantial body of research has documented significant psychological consequences for caregivers, including diminished quality of life, emotional exhaustion, and increased social isolation [3,4,5].
Parenting, even under typical conditions, is an inherently challenging and emotionally complex process. Although most parents undertake this role with dedication and warmth, they often experience elevated parenting-related stress that is further intensified when either the parent or the child presents with symptoms of psychopathology, such as anxiety, depression, or behavioral dysregulation [6]. Developmental disability research consistently shows that approximately one-third of parents of children with ASD report notably elevated levels of stress, anxiety, and depressive symptoms compared to parents of neurotypical children [7,8,9]. In fact, Davis and Carter [10] found that 33% of mothers and 17% of fathers raising a child with ASD endorsed clinically significant depressive symptoms, while 6% in both groups reported clinically significant anxiety. Additionally, Carter et al. [11] found that maternal depressive symptoms among mothers of young children with ASD remained relatively stable over time, and that children’s behavior problems emerged as a key predictor of subsequent increases in parental psychopathology. In this framework, parental depression has been consistently associated with disruptions in parent–child interactions, including increased intrusiveness and reduced emotional sensitivity [12], which in turn are linked to adverse developmental outcomes in children in emotional, behavioral and social domains [13,14,15] as well as in cognition and learning [16].
Raising a child with ASD is a chronic and enduring source of parental stress, often exceeding the burden reported by caregivers of children with other developmental disabilities such as Down syndrome, ADHD, and impairments in intellectual and adaptive functioning [17,18,19,20,21]. Consistent with these findings, Chen et al. [22], in a large cross-sectional study of 1,450 parents, demonstrated that caregivers of children with ASD experienced significantly greater mental health difficulties than parents of children with intellectual or sensory disabilities. More recently, Papadopoulos [23] found that parents of children with ASD experienced higher emotional burden compared to parents of children with ADHD or global developmental delay. Notably, the strongest predictors of parental psychopathology were lower socioeconomic status and dysfunctional child behaviors rather than ASD severity. These results align with extensive evidence showing that child behavioral dysregulation is one of the most potent and consistent contributors to parental stress, symptoms of depression, and emotional exhaustion in families of children with ASD [2,4]. Behavioral difficulties—such as irritability, aggression, tantrums, self--injury, and non-compliance—place sustained demands on caregivers, often exceeding the challenges associated with core ASD symptoms alone [24,25]. In this regard, previous studies have demonstrated that these behavior problems not only predict higher levels of parental stress and depression but also exacerbate feelings of helplessness, reduce parenting efficacy, and strain family functioning [26,27]. Moreover, child behavior problems are among the strongest predictors of caregiver burnout and service utilization, reflecting their pervasive and cumulative impact on daily routines and emotional well-being [28].
Psychological distress has also been related with increased marital dissatisfaction and a higher likelihood of marital dissolution [29,30]. Research consistently shows that the chronic psychological burden of raising a child with ASD can strain partner relationships, contributing to higher conflict, reduced emotional intimacy, and lower perceived relationship quality [31,32]. Couples raising children with ASD often report more disagreements about parenting responsibilities, financial strain, and reduced time for shared activities, all of which predict poorer marital functioning [33,34]. Marital distress, in turn, can exacerbate parenting stress and diminish the emotional resources available for effective caregiving. For single parents, the absence of co-parenting support may further intensify the stress associated with ASD-related caregiving demands, heightening vulnerability to psychological distress and burnout.
Parental psychological well-being represents a central component of the family’s developmental ecology [35]. Longitudinal research provides strong support for this transactional model, demonstrating that parental emotional functioning and child behavior dynamically influence each other over time [36,37]. A consistent bidirectional association has been documented between parenting stress and child behavior problems [38], forming a coercive and mutually reinforcing cycle of dysfunctional interaction. For example, Neece et al. [37] reported that parenting stress and child behavior problems significantly predicted one another through multiple developmental phases whereas elevated early parenting stress has been linked to poorer later child social skills [39].
Compared to parents of typically developing children, research suggests that parents of children with ASD exhibit distinct personality and socio-emotional profiles that may influence how they cope with the demands of caregiving. Li et al. [41] stressed that these parents tend to show lower levels of novelty seeking and adaptability to change, as well as reduced social engagement, characteristics that may heighten stress vulnerability in unpredictable caregiving environments. Earlier work by Wolff et al. [42] also found that fathers of children with ASD displayed higher levels of schizoid traits relative to comparison groups, potentially reflecting broader familial patterns of social withdrawal or interpersonal detachment. More recent studies corroborate these observations, noting elevated levels of neuroticism, introversion, and reduced emotional stability among parents of children with ASD [43,44]. These personality characteristics have been associated with increased psychopathology, greater sensitivity to child behavior problems, and a tendency toward less flexible coping strategies. Conversely, protective traits such as emotional intelligence, resilience, conscientiousness, and extraversion have been linked to lower parenting stress and more adaptive responses to daily challenges [45,46]. Collectively, this literature suggests that parents’ dispositional factors significantly shape their psychological adjustment and coping skills when raising a child with ASD.
1.2. Mindfulness and Parental Mental Health
Mindfulness—classified within the third wave of Cognitive–Behavioral Therapies (CBT) [47,48,49]—constitutes a set of practices aimed at cultivating present-moment awareness of thoughts, emotions, and bodily sensations with an attitude of openness and nonjudgmental acceptance [50,51]. These characteristics render mindfulness a particularly practical and relevant avenue for caregivers who face persistent stressors, chronic emotional demands, and elevated caregiving burdens associated with raising a child with ASD. At the neurocognitive level, mindfulness practices have been linked to systematic changes in neural circuits involved in attentional control, emotional regulation, and self-referential processing, contributing to improvements in affect, well-being, and adaptive behavioral functioning [52,53].
A growing body of evidence demonstrates that mindfulness training can reduce parental stress and depressive symptoms, improve parents’ perceptions of their interactions with their children, and decrease both internalizing and externalizing child behaviors [38,54,55]. Mindfulness-Based Cognitive Therapy (MBCT), originally developed as an eight-week relapse-prevention program for individuals with recurrent depression [56,57], integrates mindfulness meditation with cognitive therapy strategies to help individuals identify maladaptive cognitive patterns, interrupt ruminative thought cycles, and cultivate greater emotional flexibility. Research findings suggest that MBCT may also positively influence parenting by reducing emotional reactivity, promoting empathic attunement, and increasing constructive engagement in parent–child interactions [58].
Mindful Parenting, introduced by Kabat-Zinn and Kabat-Zinn [59], extends mindfulness principles into the parenting context by emphasizing intentional, present-centered, and compassionate engagement with both the child and the parenting experience. This relational framework highlights attunement, acceptance, emotional awareness, and non-reactivity as core mechanisms that support healthier family relationships. Empirical studies show that Mindful Parenting programs strengthen parent–child relationships, reduce parental preoccupation and parenting stress, enhance children’s executive functioning, and promote more adaptive co-parenting interactions [60]. Importantly, Mindful Parenting has been associated not only with improvements in parental functioning but also in children’s attention and behavioral regulation, especially among those with externalizing or attentional difficulties [54,61,62]. Moreover, studies suggests that parents of children with ASD who endorse elevated levels of dispositional mindfulness report lower levels of stress, anxiety, and depression, as well as fewer behavioral problems and ASD-related symptoms in their children [63,64].
In summary, mindfulness-based interventions appear theoretically well-grounded and clinically appropriate for parents of children with ASD, as well as for parents experiencing clinically significant depressive symptoms or heightened vulnerability to psychological distress. By fostering acceptance, emotional regulation, and present-focused awareness, mindfulness practices may help parents interrupt maladaptive cycles of experiential avoidance and reactive parenting while strengthening their capacity for attuned, sensitive, and compassionate caregiving. Nevertheless, further experimental research—particularly from diverse cultural contexts—is needed to clarify the direct and long-term effects of mindfulness interventions on parental well-being, parenting processes, and child developmental outcomes.
1.2. Current Study
According to the above evidence, the aim of the present randomized controlled trial (RCT) was to evaluate the preliminary efficacy of Mindfulness-Based Cognitive Therapy (MBCT) for parents of children aged 4–17 years with ASD who reported at least mild symptoms of depression, anxiety, or stress. The intervention preserved the core structure of standard MBCT while integrating mindful parenting elements designed to provide mindful awareness specifically with emphasis on reducing emotional reactivity, fostering acceptance and empathy, and strengthening parental engagement. Importantly, the program did not include explicit behavioral parenting strategies. However, it focused on applying mindfulness principles to daily parenting challenges which are often characterized by heightened emotional fatigue and may contribute to the intergenerational transmission of depressive vulnerability.
The present study examined the effects of MBCT on both parental mental health and parent-reported child behavioral outcomes in an outpatient mental health care setting. We hypothesized that: (a) parents in the MBCT group would exhibit significant reductions in depressive, anxiety, and stress symptoms, as well as significant increases in positive affect and life satisfaction, both immediately post-intervention and at one-month follow-up, compared to parents in the waitlist control group; (b) parents in the MBCT group would demonstrate high intervention acceptability; and (c) children of parents in the MBCT group would show greater improvements in parented reported severity of child’s behavior problems relative to those in the waitlist control group.
2. Materials and Methods
2.1. Study Design and Setting
The study used a two-arm randomized controlled trial (RCT) comparing an intervention group receiving MBCT with a waitlist-control group. Assessments were conducted at baseline (T0), immediately post-intervention (T1), and one-month follow-up (T2) to evaluate both the immediate effects and short-term maintenance of treatment outcomes. Participants were randomly allocated to conditions using simple randomization procedures to minimize selection bias and ensure comparable groups. The study design followed key CONSORT recommendations—such as random allocation and clearly defined assessment timepoints; thus, enhancing the methodological clarity and interpretability of the findings.
The study was conducted between February 2024 and April 2025 in an outpatient mental health clinic in Athens, Greece. This setting offered a structured, supportive, and therapeutically appropriate environment for family-focused interventions. All sessions and assessments were carried out in designated therapeutic rooms to ensure privacy, consistency, and adherence to professional standards.
This study was part of a postdoctoral research project and received ethical approval from the Ethics and Research Committee of the University of West Attica (Approval No. 8119/12-02-2024). Additional authorization for implementation of the intervention was granted by the administrative board of the collaborating mental health clinic (Approval No. 661/11-12-2023). All study procedures complied with the ethical principles outlined in the Declaration of Helsinki for research involving human participants.
2.2. Participants and Sample Size
A total of 78 Greek parents were initially screened for eligibility through multiple recruitment sources, including primary care settings, outpatient mental health clinics, parent associations in local primary schools, and community outreach initiatives (e.g., social media announcements, flyers, public advertisements). Eighteen individuals were excluded during screening due to insufficient DASS-21 symptom severity, concurrent psychotherapy participation, or refusal to provide informed consent. The remaining 60 eligible parents were enrolled and randomly assigned to either the MBCT intervention group (n = 30) or the waitlist-control group (n = 30). Figure 1 summarizes participant flow through the study following CONSORT guidelines.
An a priori power analysis was conducted using G*Power 3.1.9.4 [66] to determine the required sample size. The analysis was based on a repeated-measures ANOVA examining the group × time interaction (two groups; three assessment points: T0, T1, T2). Assuming a medium effect size (f = 0.25), α = 0.05, and desired power of 0.90, a minimum of 46 participants was required. Due to potential attrition, we sought to recruit at least 20% additional participants, targeting an overall sample of 56 parents.
2.3. Inclusion and Exclusion Criteria
To be included in the study, individuals were required to meet the following criteria: (a) be a parent and primary caregiver of at least one child diagnosed with ASD, aged 4 to 17 years, living in the same household; (b) be at least 18 years old; and (c) have sufficient fluency in Greek to understand instructions and complete all study procedures. To ensure parents most likely to benefit from the intervention, eligible participants were also required to present at least mild symptoms of depression, anxiety, or stress, based on the reliable DASS-21 cut-offs [67]: Depression ≥ 10, Anxiety ≥ 8, or Stress ≥ 15.
Exclusion criteria included participation in individual or group Cognitive Behavioral Therapy (CBT) within the previous 12 months, to maintain sample homogeneity and minimize confounding treatment effects. Participants were also required to attend at least 80% of MBCT sessions (i.e., ≥6 out of 8) to be included in post-intervention (T1) and follow-up (T2) assessments. However, the exclusion criterion based on attendance was not applied as no participants in the intervention group dropped out or failed to meet this attendance requirement.
2.4. Measures
2.4.1. Psychosocial and Demographic Questionnaire
Participants completed a social and demographic questionnaire developed by the researchers to provide a comprehensive assessment of individual and family characteristics. The first section collected parent-related information, including gender, age, marital and employment status, as well as educational attainment. The second section concerned the child, gathering data such as gender, age, and duration since diagnosis. Parents also rated child’s overall behavior using a four-point ordinal scale (0 = “no behavioral problems” to 3 = “severe behavioral problems”), a brief approach previously used in ASD research [28]. This rating reflected parents’ impressions of the child’s everyday behavioral functioning, considering common domains such as aggression, anxiety-related behaviors, regulatory difficulties, and noncompliance.
2.4.2. Parental Mental Health and Wellbeing
2.4.2.1. Depression Anxiety and Stress Scale (DASS-21) [67]
The DASS-21 is a self-report instrument comprising 21 items divided into three subscales: Depression, Anxiety, and Stress. Items are rated on a four-point Likert scale (0 = “Did not apply to me at all” to 3 = “Applied to me very much or most of the time”). Subscale scores are calculated by summing the relevant items and multiplying by two to ensure comparability with the full DASS-42. The DASS-21 has been widely used with parents of children with developmental disabilities [68,69] and has been validated in the Greek population [70]. In the present study, internal consistency coefficients (Cronbach’s α) were α = 0.75 for Depression, α = 0.64 for Anxiety, and α = 0.82 for Stress, indicating satisfactory reliability (see Table 1).
2.4.2.2. Satisfaction with Life Scale (SWLS) [71]
The SWLS assesses overall life satisfaction through five items rated on a seven-point Likert scale (1 = strongly disagree to 7 = strongly agree). Total scores range from 5 to 35, with higher scores indicating greater life satisfaction. Suggested interpretive categories include: 5–9 (extremely dissatisfied), 10–14 (dissatisfied), 15–19 (below average satisfaction), 20–24 (moderately satisfied), 25–29 (quite satisfied), and 30–35 (very satisfied). The Greek adaptation demonstrates satisfactory psychometric properties [72]. As shown in Table 1, Cronbach’s α in the present study was 0.82, indicating very good internal consistency.
2.4.2.3. Positive and Negative Affect Scale (PANAS) [73]
The PANAS consists of 20 items that measure the frequency of positive affect (10 items) and negative affect (10 items) on a five-point Likert scale (1 = very slightly or not at all to 5 = extremely). The instrument has been widely used in research involving parents of children with disabilities [74]. The scale has been translated and adapted in Greek with adequate psychometric properties [75]. Table 1 presents the internal consistency coefficients for the current study, which were α = 0.63 for Positive Affect and α = 0.77 for Negative Affect.
2.4.3. Intervention Acceptability
Acceptance of the intervention was assessed using a brief study-specific questionnaire developed by the researchers based on relevant literature on mindfulness interventions. Parents evaluated important program components (e.g., session structure, content relevance, home-practice activities, facilitator support) on a five-point Likert scale (1 = strongly disagree, 5 = strongly agree). Participants were asked to provide qualitative feedback on their overall experience by responding to two more open-ended questions about the program’s most and least beneficial elements.
2.5. Procedure
Parents who expressed interest in the study were contacted by email or telephone and completed an eligibility screening, which included confirmation of their child’s ASD diagnosis. The study’s objectives, methods, and procedure were thoroughly described to parents who met the inclusion criteria at an online or in-person briefing session. Informed consent was obtained prior to participation. The study followed CONSORT recommendations for randomized controlled trials.
After completing baseline assessments, participants were randomly allocated to the MBCT intervention group (n = 30) or the waitlist-control group (n = 30) using a computer-generated randomization sequence to minimize selection bias. Due to the nature of the intervention, blinding of participants and the MBCT instructor was not feasible; however, all data entry and dataset preparation were performed by a researcher blinded to group assignment to reduce analytic bias.
Participants allocated to the MBCT group proceeded to the intervention phase (described in Section 2.6). To maintain consistency and enhance group cohesion, the 30 participants allocated to the MBCT condition were organized into two fixed subgroups of 15 individuals each, which remained stable throughout the eight-week program. Participants in the waitlist-control group continued with treatment as usual.
Post-intervention assessments (T1) were conducted within one week following the final session, and follow-up assessments (T2) were administered four weeks later to examine short-term maintenance of treatment effects. All assessments were completed individually. All data were anonymized using unique identification codes and stored on encrypted, password-protected systems in accordance with GDPR requirements.
In the intervention group, all 30 parents initiated and completed the 8-week MBCT program without attrition and all participants satisfied the predefined ≥80% attendance criterion. In the waitlist-control group, 26 of 30 parents completed both T1 and T2 assessments; four participants withdrew immediately after randomization and completed only the baseline assessment. Thus, the final analytic sample comprised 56 parents (MBCT: n = 30; control: n = 26). All exclusions were due solely to missing follow-up data rather than intervention-related reasons.
2.6. Intervention
The intervention followed the standard eight-week Mindfulness-Based Cognitive Therapy (MBCT) protocol [56,57], delivered in weekly two-hour group sessions. MBCT integrates cognitive therapy principles with mindfulness meditation practices to cultivate present-moment awareness, reduce automatic negative thinking, enhance emotional regulation, and strengthen self-compassion, thereby enabling participants to experience greater psychological wellbeing.
To ensure relevance for parents of children with ASD, the program incorporated established mindful-parenting components [6,59,76], without altering the core MBCT curriculum. These additions emphasized applying mindfulness to real-time parenting challenges, including recognizing emotionally driven parenting reactions, increasing awareness of the parent–child relational dynamic, cultivating acceptance, and promoting nonreactive responding in high-stress caregiving situations.
Each session included guided mindfulness practices (e.g., body scan, sitting meditation, mindful movement), compassion-focused exercises toward self and child, cognitive-behavioral elements (identifying automatic thoughts, cognitive reactivity, and decentering), experiential activities, and structured group inquiry linking personal practice experiences to MBCT principles. Table 2 presents the program’s structure and content. Participants were assigned 30–40 minutes of daily home practice supported by Greek-translated audio recordings and written materials. To encourage participation and skill consolidation, home practice was reviewed weekly.
Sessions were facilitated by the first author, an academic specializing in developmental psychology and developmental psychopathology with accredited training in mindfulness-based interventions and clinical psychotherapeutic practice. Attendance was recorded, with an expectation of ≥80% participation to ensure adequate exposure. Participants in the waitlist-control group continued treatment-as-usual and were offered the MBCT program after completing T2. A minimum of 80% participation was required to guarantee sufficient exposure, and attendance was recorded. After completing T2, the MBCT program was offered to participants in the waitlist-control group who continued to receive standard treatment.
2.7. Statistical Analysis
All statistical analyses were conducted using IBM SPSS Statistics (Version 25). Assumptions of normality were evaluated through skewness and kurtosis values, all of which fell within the acceptable ±2 range, supporting the use of parametric procedures [77,78]. This approach aligns with other RCTs in the mindfulness literature [79].
Descriptive statistics were computed for all sociodemographic and baseline clinical variables, and internal consistency (Cronbach’s α) was examined for each psychometric instrument. Independent-samples t-tests for continuous variables and chi-square tests for categorical variables were used to evaluate baseline equivalency between the MBCT and waitlist-control groups.
Intervention effects were examined using repeated-measures ANOVAs with time (T0, T1, T2) as the within-subjects factor and group (MBCT vs. waitlist-control) as the between-subjects factor. The primary focus of inference was the group × time interaction. Partial eta squared (η²ₚ) was reported as the effect size for ANOVA models. When significant interactions were detected, post hoc paired-samples t-tests evaluated within-group changes across time, and independent-samples t-tests compared groups at each assessment point. Cohen’s d was reported for all t-test comparisons.
Changes in parent-reported child behavior problem severity over time and between groups were analyzed using chi-square tests, and effect sizes measured using Cramer’s V. Statistical significance was set at α = 0.05 (two-tailed).
3. Results
3.1. Sociodemographic and Clinical Characteristic
Table 3 presents the baseline sociodemographic characteristics of participating parents and their children. There were no statistically significant differences between the MBCT and waitlist-control groups on any demographic category (all p >.05), indicating appropriate baseline equivalency. Most parents (66.1%) were mothers and were married. Nearly half (42.9%) had received technical or technological education. The mean age of the parents was 40.67 years (SD = 6.45), and the two groups had no differences in age, gender distribution, or employment status. In terms of child characteristics, most children (80.4%) were males, with a mean age of 10.54 years and an average time since ASD diagnosis of 5.84 years. Similar to parental factors, no statistically significant between-group variations were found in child socio-demographic variables at baseline.
Baseline clinical outcomes are shown in Table 4. All mental health indicators showed no significant between-group differences (all p >.05). Parents were classified within mild to moderate symptom severity range on the DASS-21 (Mdepression= 17.32; Manxiety = 13.00, and Mstress = 26.14). Life satisfaction scores were low (M = 15.71) and fell into the category of “slightly dissatisfied.” Similarly, PANAS scores across groups showed a clinically significant trend of increased negative affect (M = 22.80) and decreased positive affect (M = 27.79). At baseline (T0) (p =.923), parent-reported severity of child behavioral problems did not differ significantly between groups, suggesting that both groups had comparable clinical profiles at the start of the study. The homogeneity of the overall sample strengthens the methodological validity of subsequent between-group comparisons.
3.2. Effect of the MBCT Program on Parental Mental Health Outcomes
3.2.1. Depression
Repeated-measures ANOVA revealed significant main effects of group (F = 22.950, p < .001, η²ₚ = .298) and time (F = 50.344, p < .001, η²ₚ = .482) on depressive symptoms. Importantly, a Group × Time interaction emerged (F = 64.126, p < .001, η²ₚ = .543). As presented in Table 5, within-group comparisons demonstrated that parents in the MBCT group experienced large and statistically significant reductions in depression from T0 to T1 (t(29) = 10.37, p < .001, d = 1.89) and from T0 to T2 (t(29) = 8.52, p < .001, d = 1.56). A smaller yet significant improvement also occurred between T1 and T2 (t(29) = 2.37, p = .030, d = 0.43), suggesting continued symptomatic relief during the follow-up period. In contrast, the waitlist-control group showed no significant changes in depression levels over time. As shown in Figure 1, between-group comparisons further indicated that, at T1, parents in the MBCT group reported substantially lower depressive symptoms than those in the control group (Mintervention = 11.77, SD = 2.67 vs. Mcontrol = 17.46, SD = 3.28; t(54) = −6.65, p < .001, d = −1.78). This difference was even more pronounced at T2 (Mintervention = 11.00, SD = 2.39 vs. Mcontrol = 17.69, SD = 3.47; t(54) = −8.02, p < .001, d = −2.15).
3.2.2. Anxiety
Repeated-measures ANOVA revealed significant main effects of group (F = 21.730, p < .001, η²ₚ = .287) and time (F = 18.462, p < .001, η²ₚ = .255), as well as a significant Group × Time interaction (F = 29.298, p < .001, η²ₚ = .352). As shown in Table 4, participants in the MBCT group exhibited substantial reductions in anxiety from baseline to post-intervention (t(29) = 7.53, p < .001, d = 1.37) and from T0 to T2 (t(29) = 6.72, p < .001, d = 1.23). No significant change was observed between T1 and T2 (p = .687), indicating that improvements were maintained over time. In contrast, the waitlist-control group showed no statistically significant changes across time. Between-group comparisons further supported that at T1, the MBCT group reported significantly lower anxiety scores than the control group (Mintervention = 9.30, SD = 2.09 vs. Mcontrol = 13.15, SD = 2.05; t(54) = –6.74, p < .001, d = –1.81). This difference remained significant at T2 (9.40 ± 2.24 vs. 13.46 ± 2.16; t(54) = –7.63, p < .001, d = –2.09) (see Figure 2).
3.2.3. Stress
A repeated-measures ANOVA revealed significant main effects of group (F = 25.530, p < .001, η²ₚ = .321) and time (F = 143.828, p < .001, η²ₚ = .727), as well as a significant Group × Time interaction (F = 188.515, p < .001, η²ₚ = .777) (Table 5). Within-group comparisons showed that parents in the MBCT group experienced significant reductions in stress from T0 to T1 (t(29) = 16.96, p < .001, d = 3.10) and from T0 to T2 (t(29) = 17.56, p < .001, d = 3.21). A smaller but still significant reduction was also observed between T1 and T2 (t(29) = 4.18, p < .001, d = 0.76), indicating continued improvement in stress levels during the follow-up period. In contrast, the waitlist-control group exhibited no significant changes in stress across any of the three assessment points. As illustrated in Figure 2, between-group comparisons further corroborated the intervention effects. At T1, the MBCT group reported significantly lower stress scores than the control group (Mintervention = 18.93, SD = 4.48 vs. Mcontrol = 26.46, SD = 4.09; t(54) = −6.44, p < .001, d = −1.73) and T2 (Mintervention = 17.30 ± 4.09 vs. Mcontrol = 26.85, SD = 3.76; t(54) = −9.28, p < .001, d = −2.49).
3.2.4. Life Satisfaction
Table 5 presents the significant main effects of group (F = 62.429, p < .001, η²ₚ = .536) and time (F = 87.903, p < .001, η²ₚ = .619), as well as a robust Group × Time interaction (F = 132.156, p < .001, η²ₚ = .710). Within-group comparisons demonstrated that parents in the MBCT group experienced large and statistically significant increases in life satisfaction from T0 to T1 (t(29) = −12.55, p < .001, d = −2.29), from T0 to T2 (t(29) = −14.87, p < .001, d = −2.71), and from T1 to T2 (t(29) = −4.71, p < .001, d = −0.86). No significant changes emerged at any time point in the waitlist-control group. As illustrated in Figure 2, between-group comparisons indicated that, at T1, the MBCT group reported significantly higher life satisfaction than the control group (Mintervention = 21.77, SD = 2.97 vs. Mcontrol = 15.31, SD = 1.69; t(54) = 9.55, p < .001, d = 2.56). This difference became even more pronounced at T2, with MBCT participants continuing to show substantial gains relative to controls (Mintervention = 23.07, SD = 2.49 vs. Mcontrol = 15.31, SD = 1.69; t(54) = 14.12, p < .001, d = 3.79).
3.2.5. Positive and Negative Affect
For positive affect, analyses revealed a significant main effect of group (F = 9.725, p = .003, η²ₚ = .153) and time (F = 23.866, p < .001, η²ₚ = .306), as well as a significant Group × Time interaction (F = 32.066, p < .001, η²ₚ = .373). Within-group results (Table 5) showed that parents in the MBCT group experienced significant increases in positive affect from T0 to T1 (t(29) = −6.38, p < .001, d = −1.16), from T1 to T2 (t(29) = −2.45, p = .020, d = −0.45), and from T0 to T2 (t(29) = −6.46, p < .001, d = −1.18). In contrast, the control group demonstrated no significant changes over time. Between-group comparisons confirmed that the MBCT group reported significantly higher positive affect at both T1 (Mintervention = 29.97, SD = 2.34 vs. Mcontrol = 27.77, SD = 1.70; t(54) = 3.82, p < .001, d = 1.02) and T2 (Mintervention = 30.43, SD = 2.39 vs. Mcontrol = 27.65, SD =1.65; t(54) = 5.10, p < .001, d = 1.37) (see Figure 2).
As illustrated in Table 5, a significant main effect of group (F = 7.292, p = .009, η²ₚ = .119) and time (F = 14.189, p < .001, η²ₚ = .208), as well as a significant Group × Time interaction (F = 25.267, p < .001, η²ₚ = .319) was revealed. Within-group analyses indicated that the MBCT group demonstrated significant reductions in negative affect from T0 to T1 (t(29) = 4.41, p < .001, d = 0.80), from T0 to T2 (t(29) = 5.34, p < .001, d = 0.98), and from T1 to T2 (t(29) = 3.67, p = .001, d = 0.67). No significant changes were observed within the control group across the three assessment points. Between-group comparisons (see Figure 2) further demonstrated that the MBCT group reported significantly lower negative affect relative to the control group at T1 (Mintervention = 20.83, SD = 1.72 vs. Mcontrol = 22.81, SD = 1.90; t(54) = −4.01, p < .001, d = −1.07) and T2 (Mintervention = 20.23, SD = 1.92 vs. Mcontrol = 22.96 ± 1.97; t(54) = −5.60, p < .001, d = −1.50).
3.3. Intervention Acceptability
Parents receiving MBCT intervention demonstrated very high levels of acceptability, with 96.4% reporting overall strong satisfaction with the program (M = 4.82, SD = 0.39). Regarding the structure and content of the intervention, 95.4% of participants indicated high satisfaction, reflecting strong approval of the program’s organization, session flow, and relevance to their personal and family needs. Similarly, 97.4% rated their overall experience and the suitability of the program as highly positive, highlighting the supportive group atmosphere, the facilitator’s guidance, and the practical usefulness of the skills taught. Open-ended responses also revealed that parents found the mindfulness practices highly appropriate to daily parenting and intended to continue using them beyond the program. The main obstacles identified were childcare needs and travel distance, while some parents suggested that future interventions could benefit from smaller group sizes to enhance interaction and personal sharing.
3.4. Child Behavioral Outcomes
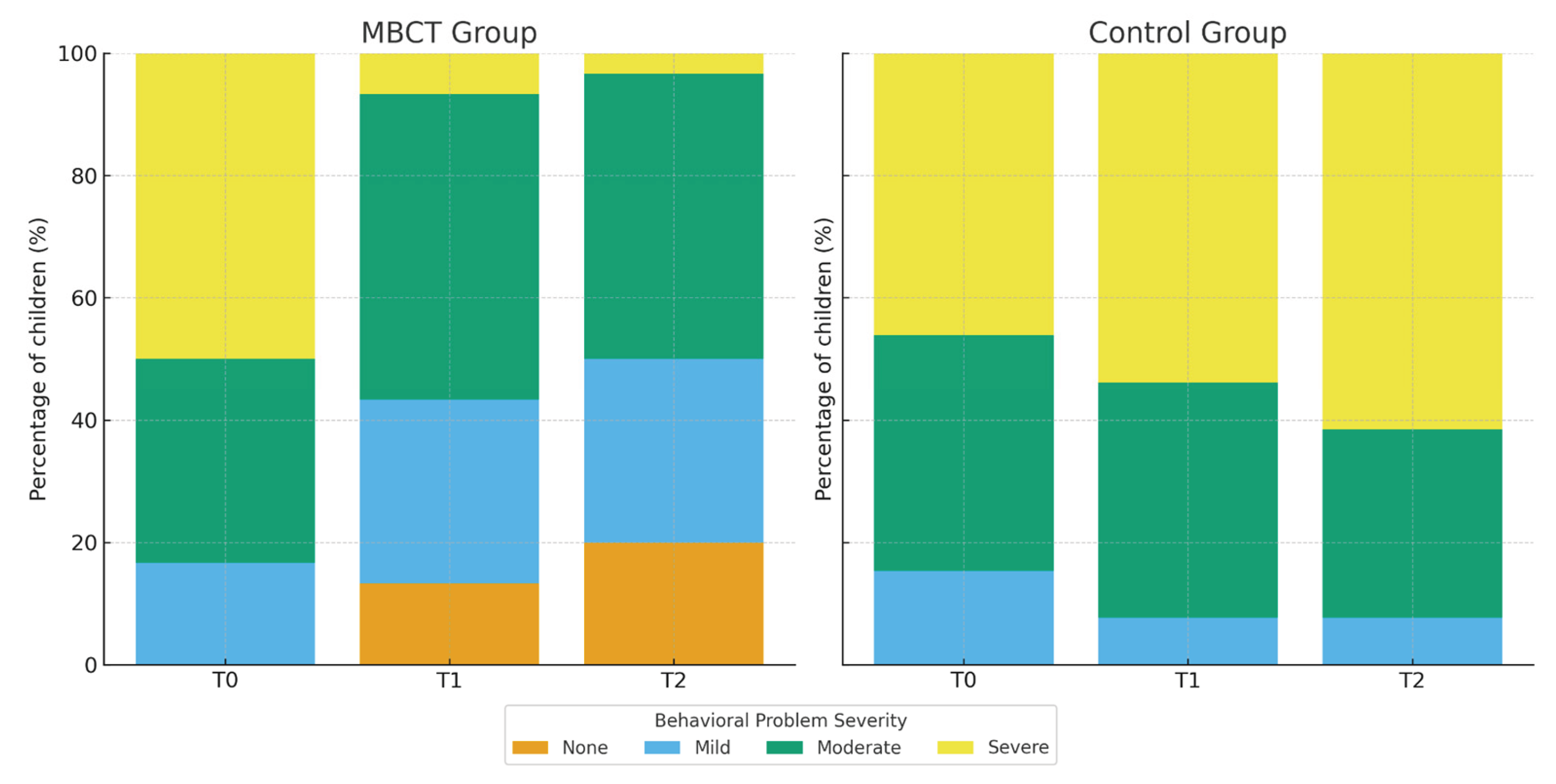
Because no significant between-group differences in parent-reported child behavioral problems were observed at baseline (T0) (p = .923; see Section 3.1), analyses focused on changes occurring at post-intervention (T1) and follow-up (T2). At T1, a significant difference observed between groups (χ²(3) = 18.262, p < .001), with a large effect (Cramer’s V = .57). In the MBCT group, only 6.7% of children remained in the severe range while 13.3% were rated as having no behavioral problems. In contrast, in the waitlist-control group, 53.8% of children continued to exhibit severe behavioral difficulties and no child was rated as problem-free. This pattern further strengthened at T2, where another significant group difference was revealed (χ²(3) = 25.169, p < .001; Cramer’s V = .67). The proportion of children rated as having no behavioral difficulties increased to 20% in the MBCT group, while only 3.3% remained in the severe category. Conversely, 61.5% of children in the control group continued to present with severe problems, and none were rated as having no difficulties.
Figure 3.
Comparison of Children’s Behavioral Problems Across Time by Group.
4. Discussion
4.1. Preliminary Findings
At baseline, the two groups were comparable in terms of all sociodemographic and clinical factors, confirming the adequacy of randomization. More specifically, parents had significantly higher levels of depression, anxiety, and stress, accompanied by reduced life satisfaction. These scores fell within clinically relevant ranges across important mental health indices and were significantly higher than normal population norms [80]. Such findings have been consistently reported in previous studies which demonstrates the elevated psychological burden experienced by parents of children with ASD and underline the clinical relevance of evaluating interventions specifically targeting this population [74,81,82]. Moreover, this high level of initial distress provided substantial scope for therapeutic improvement.
4.2. Effectiveness of MBCT on Parental Mental Health
The current study’s results suggest that the MBCT program was highly effective in reducing depression symptoms, with parents in the MBCT group exhibiting significant gains both at immediately post-intervention and at follow-up. These findings align with a large body of research showing that MBCT reliable improves depressive symptoms and prevents relapse [56,57,85,86] while also enhancing psychological flexibility and resilience [83,84]. Depression is typically characterized by rigid negative schemas, ruminative thinking, and heightened attentional focus on distressing emotional states [88]. MBCT can reduce depressive symptomatology by interrupting the repetitive negative cognitive cycles that sustain emotional distress and depressive episodes; thereby fostering metacognitive awareness, cognitive flexibility, acceptance, and self-compassion [56,87,88]. Accordingly, this cognitive shift enables individuals to cope with difficult situations with less automatic reactivity and greater psychological flexibility, functioning as a broad regulatory mechanism that yields downstream benefits across anxiety- and stress-related processes.
Within the context of parenting a child with ASD—an environment marked by chronic stressors and heightened emotional demands—these internal regulatory gains are likely further reinforced by the mindful parenting components embedded in the MBCT protocol. These practices foster present-moment awareness, emotional attunement, and compassion in parent–child interactions [60,76,89,90], which, in turn, help disrupt entrenched reactive patterns and reduce the likelihood that everyday challenges will elicit negative interpretations or self-critical rumination. Through this dual pathway—targeting both internal emotion-regulation processes and the interpersonal quality of parent–child exchanges—the combined MBCT and mindful parenting approach fosters a more regulated, attuned, and compassionate caregiving stance.
In terms of parental stress, the MBCT group showed both immediate post-intervention and long-term gains, with stress levels decreasing significantly from the severe range at baseline to the mild range at T1 and falling within the normative range by T2. These results are consistent with previous studies revealing that mindfulness-based interventions reliably reduce stress and enhance emotional functioning among caregivers of children with ASD [91,92,93,94]. Mindfulness may serve as a protective factor particularly for parents who must balance demanding caregiving responsibilities alongside professional pressures, financial strain, and persistent work–family conflict [95]. Parents receiving MBCT learn to interrupt automatic stress responses and shift attention toward more adaptive interpretations through practices that cultivate a non-judgmental present-moment stance, mindful disengagement from “autopilot,” and greater sensitivity to internal cues [96]. This in turn expands their capacity to cope with daily challenges in more flexible and adaptive ways. Indeed, such cognitive–emotional shifts reduce reliance on fight-or-flight patterns—commonly associated with anxiety and heightened reactivity [97]—and foster more deliberate, emotionally regulated parenting behaviors.
Significant improvements in perceived positive affect and life satisfaction were observed among participants in the MBCT group, who shifted from “somewhat dissatisfied” at baseline to “somewhat satisfied” at post-intervention and follow-up. Such findings align with evidence indicating that mindfulness practice reduces self-criticism, enhances positive emotion, and supports broader psychological flourishing [98,99,100]. According to the Mindfulness-to-Meaning Theory [96], mindfulness practices that foster decentering and broaden attentional scope may initiate an upward spiral of adaptive cognitive–affective processing that progressively transforms how individuals respond to stress. This shift enables individuals to engage in more constructive cognitive reappraisal and to flexibly reinterpret both internal and external experiences, thereby enhancing their capacity to cope with adversity with greater clarity, emotional calmness, and sense of purpose. More specifically, such cognitive changes enhance well-being primarily through their influences on affective process, namely by elevating positive affect and reducing negative affect [101]. For families raising a child with ASD, this process functions as core mechanisms linking mindfulness practice to greater life satisfaction [102] as parents become more capable of re-experiencing positive emotions and evaluating daily life more favorably. This, in turn can foster a more positive stance and meaning in their caregiving role while also shifting parents away from automatic negative interpretations, such as guilt or self-blame, regarding their child’s disability and challenging behaviors.
Contemporary neuroscientific models describing the therapeutic mechanisms underlying mindfulness practice provide a coherent explanatory framework for understanding the treatment gains observed in the current study. Research evidence indicates that MBCT induces functional and structural neuroplastic changes in brain system supporting attentional and cognitive control, emotional regulation, and self-referential processing [103]. Indeed, mindfulness practice has been found to enhance activation in prefrontal and anterior cingulate regions, which are critical for top-down emotion regulation [53]. Additionally, it reduces amygdala reactivity, thereby improving threat sensitivity and strengthening emotional resilience [104,105]. In parallel, mindfulness practices modulate the hypothalamic–pituitary–adrenal (HPA) axis, contributing to reductions in cortisol levels [106,107] and counteracting the chronic stress dysregulation frequently reported among parents of children with ASD [108].
4.3. Acceptance of the Intervention
All 30 parents (100%) in the MBCT group completed the eight-week program and consistently attended sessions, engaged in daily mindfulness practice (30–45 minutes), and applied mindful parenting skills at home. Participants’ consistent involvement throughout the program reflects high commitment and strong feasibility to the intervention protocol. Acceptability ratings were constantly positive with parents reporting that the program’s structure, content, and relevance aligned closely to their needs. They also identified the supportive group environment and the facilitator’s guidance as key strengths of the program. Open-ended responses further revealed the practical value of mindfulness practices for managing everyday increased. Reported obstacles were primarily associated with increased childcare demands and travel distance to and from the intervention setting. These findings align with international research demonstrating high satisfaction and strong engagement with mindfulness-based programs [74,109,110], confirming MBCT as a feasible and well-accepted intervention for ASD caregivers.
4.4. Indirect Effects on Children’s Behavior
Despite the fact that children did not receive direct intervention, parent reports at post-intervention and follow-up revealed substantial between-group differences in behavioral outcomes, with the MBCT group showing notable reductions in problem severity. Consistent with the transactional model of development [35] and with prior evidence [55,61,111] these gains in children’s behavior outcomes may reflect parents improved emotional regulation and increased use of adaptive and appropriate parenting skills. Reductions in parental stress may interrupt maladaptive parent–child transactional cycles and promote a calmer, more supportive caregiving environment that facilitates children’s self-regulation. As parents become more regulated, attentive, and responsive to their child’s needs and behaviors, the parent child relationship improves, and daily interactions tend to become less reactive and more supportive. In turn, parents are more able to create a caregiving environment characterized by emotional stability and consistency that fosters the child’s behavioral self-regulation and contributes to reductions in behavior problems over time. Therefore, mindful parenting functions as a key mechanism through which parental well-being translates into measurable improvements in children’s behavioral adjustment, underscoring the reciprocal interplay between parental wellbeing and child behavior.
4.5. Strengths, Limitations, and Future Research
This study has several methodological strengths. The use of a randomized controlled trial with an experimental and a waitlist-control group enhances the rigor of the study and supports robust conclusions about the effectiveness of MBCT on parental mental health. Importantly, there was no attrition in the MBCT group, indicating high acceptability, strong engagement, and good feasibility which are all critical factors for interventions targeting parents of children with ASD. Additionally, the inclusion of parents of children aged 4 to 17 years may enhance the applicability of the findings to a broad spectrum of ASD caregiving experiences.
Despite these strengths, several limitations need consideration. First, although the sample size exceeded a priori power criteria, it remained relatively modest, that may limit the precision of effect size estimates and the generalizability of the findings [112]. Future studies should recruit larger and more socioeconomically and geographically diverse samples, including families from rural settings and varied cultural backgrounds, to enhance the applicability of results [84]. Second, conclusions regarding the long-term sustainability of treatment gains are limited by the one-month follow-up period [113]. Future studies should incorporate follow-up assessments extending several months or years post-intervention., as evidence suggests that the benefits of mindfulness may change over time. Third, outcomes were assessed using quantitative self-report measures. Although these instruments have strong psychometric properties [67,71], they may not fully capture the subjective complexity of parents’ lived experiences or provide insights into how mindfulness skills influence daily parenting behaviors. Mixed-methods approaches, incorporating interviews, observational assessments, or ecological momentary assessment (EMA), would provide a richer understanding of the mechanisms through which MBCT intervention exert their effects. Finally, parent-reported child behavioral outcomes may be subject to cognitive biases [114] and do not account for co-occurring psychopathology (e.g., ADHD), which can influence the child’s behavioral presentation [115]. To improve the validity of child outcome measurement, future research should incorporate multi-informant reports (e.g., from teachers and clinicians), structured behavioral observations, and standardized assessment tools.
5. Conclusions
This randomized controlled study provides robust evidence that MBCT, combined with mindful parenting practices, is an effective and acceptable intervention for parents of children with ASD. Parents who received MBCT demonstrated significant improvements in overall mental health and wellbeing, with particularly notable reductions in parental psychopathology along with strong gains in positive affect and life satisfaction. These improvements were evident immediately post-intervention and either further increased or, in the case of anxiety, remained stable at follow-up, revealing both the direct impact and short-term durability of treatment gains. In contrast, the waitlist-control group showed no meaningful changes, underscoring both the efficacy of MBCT and the persistent psychological burden experienced by parents caring for a child with ASD.
Preliminary indications of improvement in parent-reported child behavior further suggest that enhancing parental emotional regulation may positively influence family dynamics and parent–child relationships. These improvements are likely explained by gains in present-moment awareness, acceptance, and self-compassion all of which are central mechanisms cultivated through MBCT and mindful parenting. As a result, through these practices parents experience neurocognitive changes which interrupt maladaptive cognitive patterns and reduce emotional reactivity while enhancing prefrontal control processes involved in psychological flexibility and emotional regulation. Thus, these changes enable parents to respond to caregiving demands in a more adaptive and flexible manner rather than relying on habitual stress or emotional-driven reactions [6,116].
In clinical practice, MBCT represents a well-accepted intervention that can be integrated into individual therapy, group-based parent support, and broader psychoeducational programs. By strengthening parental mental health, MBCT has the potential to indirectly support children’s positive behavioral, highlighting its value as a family-centered approach to promoting psychological well-being and healthier parent–child interactions.
Author Contributions
Conceptualization, D.P. and K.M.; methodology, D.P.; software, D.P.; validation, D.P., and K.M.; formal analysis, D.P.; investigation, D.P.; writing—original draft preparation, D.P.; writing—review and editing, K.M. and D.P.; supervision, K.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of West Attica (8119/12-02-2024) for studies involving humans.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data is available upon reasonable request from the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Marsack-Topolewski, C.N.; Samuel, P.S.; Tarraf, W. Empirical evaluation of the association between daily living skills of adults with autism and parental caregiver burden. PLoS ONE 2021, 16, e0244844. [Google Scholar] [CrossRef]
- Lecavalier, L.; Leone, S.; Wiltz, J. The impact of behavior problems on caregiver stress in young people with autism spectrum disorders. J. Intellect. Disabil. Res. 2006, 50, 172–183. [Google Scholar] [CrossRef] [PubMed]
- Sánchez Amate, J.J.; Luque de la Rosa, A. The Effect of Autism Spectrum Disorder on Family Mental Health: Challenges, Emotional Impact, and Coping Strategies. Brain Sci. 2024, 14, 1116. [Google Scholar] [CrossRef]
- Estes, A.; Olson, E.; Sullivan, K.; Greenson, J.; Winter, J.; Dawson, G.; Munson, J. Parenting-related stress and psychological distress in mothers of toddlers with autism spectrum disorders. Brain Dev. 2013, 35, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Papadopoulos, D. Mothers’ experiences and challenges raising a child with autism spectrum disorder: A qualitative study. Brain Sci. 2021, 11, 309. [Google Scholar] [CrossRef] [PubMed]
- Bögels, S.; Restifo, K. Mindful Parenting: A Guide for Mental Health Practitioners; Springer: New York, NY, USA, 2014. [Google Scholar]
- van der Lubbe, A.; Swaab, H.; Vermeiren, R.; et al. Chronic Parenting Stress in Parents of Children with Autism: Associations with Chronic Stress in Their Child and Parental Mental and Physical Health. J. Autism Dev. Disord. 2025. [Google Scholar] [CrossRef]
- Ekas, N.V.; Lickenbrock, D.M.; Whitman, T.L. Optimism, social support, and well-being in mothers of children with autism spectrum disorder. J. Autism Dev. Disord. 2010, 40, 1274–1284. [Google Scholar] [CrossRef]
- Gambetti. Full reference details not provided in the current draft; please complete according to MDPI style. 2024. [Google Scholar]
- Davis, N.O.; Carter, A.S. Parenting stress in mothers and fathers of toddlers with autism spectrum disorders: Associations with child characteristics. J. Autism Dev. Disord. 2008, 38, 1278–1291. [Google Scholar] [CrossRef]
- Carter, A.S.; Martínez-Pedraza, F. de L.; Gray, S.A. Stability and individual change in depressive symptoms among mothers raising young children with ASD: Maternal and child correlates. J. Clin. Psychol. 2009, 65, 1270–1280. [Google Scholar] [CrossRef]
- Lovejoy, M.C.; Graczyk, P.A.; O’Hare, E.; Neuman, G. Maternal depression and parenting behavior: A meta-analytic review. Clin. Psychol. Rev. 2000, 20, 561–592. [Google Scholar] [CrossRef]
- Gladstone, T.R.G.; Beardslee, W.R.; Diehl, A. The impact of parental depression on children. In Parental Psychiatric Disorder: Distressed Parents and Their Families, 3rd ed.; Reupert, A., Maybery, D., Nicholson, J., Göpfert, M., Seeman, M.V., Eds.; Cambridge University Press: Cambridge, UK, 2015; pp. 117–126. [Google Scholar] [CrossRef]
- Goodman. Full reference details not provided in the current draft; please complete. 2011. [Google Scholar]
- Pan, B.; Gong, Y.; Wang, Y.; et al. The impact of maternal parenting stress on early childhood development: the mediating role of maternal depression and the moderating effect of family resilience. BMC Psychol. 2025, 13, 277. [Google Scholar] [CrossRef] [PubMed]
- Chad-Friedman, S.; Zhang, I.; Donohue, K.; Chad-Friedman, E.; Rich, B.A. Reciprocal associations between parental depression and child cognition: Pathways to children’s internalizing and externalizing symptoms. Dev. Psychopathol. 2025, 37, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Abbeduto. Full reference details not provided in the current draft; please complete. 2004. [Google Scholar]
- Dabrowska, A.; Pisula, E. Parenting stress and coping styles in mothers and fathers of preschool children with autism and Down syndrome. J. Intellect. Disabil. Res. 2010, 54, 266–280. [Google Scholar] [CrossRef]
- Hayes, S.A.; Watson, S.L. The impact of parenting stress: A meta-analysis of studies comparing the experience of parenting stress in parents of children with and without autism spectrum disorder. J. Autism Dev. Disord. 2013, 43, 629–642. [Google Scholar] [CrossRef] [PubMed]
- Yesilkaya, M.; Magallón-Neri, E. Parental Stress Related to Caring for a Child With Autism Spectrum Disorder and the Benefit of Mindfulness-Based Interventions for Parental Stress: A Systematic Review. SAGE Open 2024, 14, 1–15. [Google Scholar] [CrossRef]
- Dijkstra-de Neijs, L.; Swaab, H.; van Berckelaer-Onnes, I.A.; et al. Resilience Within Families of Young Children with ASD. J. Autism Dev. Disord. 2025. [Google Scholar] [CrossRef]
- Chen, S.-Q.; Chen, S.-D.; Li, X.-K.; Ren, J. Mental health of parents of special needs children in China during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2020, 17, 9519. [Google Scholar] [CrossRef]
- Papadopoulos, D. Impact of child and family factors on caregivers’ mental health and psychological distress during the COVID-19 pandemic in Greece. Children 2023, 11, 7. [Google Scholar] [CrossRef]
- Lovell, B.; Wetherell, M.A. Child behaviour problems mediate the association between coping and perceived stress in caregivers of children with autism. Res. Autism Spectr. Disord. 2015, 20, 17–23. [Google Scholar] [CrossRef]
- Soke, G.N.; Rosenberg, S.A.; Rosenberg, C.R.; Vasa, R.A.; Lee, L.C.; DiGuiseppi, C. Brief Report: Self-injurious Behaviors in Preschool Children with Autism Spectrum Disorder Compared to Other Developmental Delays and Disorders. J. Autism Dev. Disord. 2018, 48(7), 2558–2566. [Google Scholar] [CrossRef]
- Kim, I.; Ekas, N.V.; Hock, R. Associations between child behavior problems, family management, and depressive symptoms for mothers of children with autism spectrum disorder. Res. Autism Spectr. Disord. 2016, 26, 80–89. [Google Scholar] [CrossRef]
- Postorino, V.; Sanges, V.; Giovagnoli, G.; Fatta, L.M.; De Peppo, L.; Armando, M.; Vicari, S.; Mazzone, L. Clinical differences in children with autism spectrum disorder with and without food selectivity. Appetite 2015, 92, 126–132. [Google Scholar] [CrossRef]
- Karst, J.S.; Van Hecke, A.V. Parent and family impact of autism spectrum disorders: A review and proposed model for intervention evaluation. Clin. Child Fam. Psychol. Rev. 2012, 15(3), 247–277. [Google Scholar] [CrossRef] [PubMed]
- Hartley, S.L.; Barker, E.T.; Seltzer, M.M.; Floyd, F.; Greenberg, J.; Orsmond, G.; Bolt, D. The relative risk and timing of divorce in families of children with an autism spectrum disorder. J. Fam. Psychol. 2010, 24, 449–457. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.K.S.; Leung, D.C.K. The Impact of Child Autistic Symptoms on Parental Marital Relationship: Parenting and Coparenting Processes as Mediating Mechanisms. Autism Res. 2020, 13, 1516–1526. [Google Scholar] [CrossRef] [PubMed]
- Saini, M.; Stoddart, K.P.; Gibson, M.; Morris, R.; Barrett, D.; Muskat, B.; Nicholas, D.; Rampton, G.; Zwaigenbaum, L. Couple relationships among parents of children and adolescents with Autism Spectrum Disorder: Findings from a scoping review of the literature. Res. Autism Spectr. Disord. 2015, 17, 142–157. [Google Scholar] [CrossRef]
- Weitlauf, A.S.; McPheeters, M.L.; Peters, B.; Sathe, N.; Travis, R.; Aiello, R.; Williamson, E.; Veenstra-VanderWeele, J.; Krishnaswami, S.; Jerome, R.; Warren, Z. Report No. 14-EHC036-EF; Therapies for Children with Autism Spectrum Disorder: Behavioral Interventions Update. Agency for Healthcare Research and Quality: Rockville, MD, USA, 2014. [PubMed]
- Kersh, J.; Hedvat, T.T.; Hauser-Cram, P.; Warfield, M.E. The contribution of marital quality to the well-being of parents of children with developmental disabilities. J. Intellect. Disabil. Res. 2006, 50(12), 883–893. [Google Scholar] [CrossRef]
- Brobst, J.B.; Clopton, J.R.; Hendrick, S.S. Parenting children with Autism Spectrum Disorders: The couple’s relationship. Focus Autism Other Dev. Disabil. 2009, 24(1), 38–49. [Google Scholar] [CrossRef]
- Sameroff, A.J. The Transactional Model of Development: How Children and Contexts Shape Each Other; American Psychological Association: Washington, DC, USA, 2009. [Google Scholar] [CrossRef]
- Baker, J.K. Full reference details not provided in the current draft; please complete. 2003. [Google Scholar]
- Neece, C.L.; Green, S.A.; Baker, B.L. Parenting stress and child behavior problems: A transactional relationship across time. Am. J. Intellect. Dev. Disabil. 2012, 117, 48–66. [Google Scholar] [CrossRef]
- Neece, C.L. Mindfulness-based stress reduction for parents of young children with developmental delays: Implications for parental mental health and child behavior problems. J. Appl. Res. Intellect. Disabil. 2014, 27, 174–186. [Google Scholar] [CrossRef] [PubMed]
- Neece, C.L.; Baker, B. Predicting maternal parenting stress in middle childhood: The roles of child intellectual status, behavior problems, and social skills. J. Intellect. Disabil. Res. 2008, 52, 1114–1128. [Google Scholar] [CrossRef]
- Baker, J.K.; Messinger, D.S.; Lyons, K.K.; Grantz, C.J. A pilot study of maternal sensitivity in the context of emergent autism. J. Autism Dev. Disord. 2010, 40, 988–999. [Google Scholar] [CrossRef]
- Li, X.; Wang, Q.; Wu, Y.; Wang, S.; Huang, Y.; Li, T. Personality Characteristics and Neurocognitive Functions in Parents of Children with Autism Spectrum Disorder. Shanghai Arch. Psychiatry 2017, 29, 41–47. [Google Scholar] [CrossRef]
- Wolff, S.; Narayan, S.; Moyes, B. Personality characteristics of parents of autistic children: A controlled study. J. Child Psychol. Psychiatry 1988, 29, 143–153. [Google Scholar] [CrossRef]
- Pottie, C.G.; Ingram, K.M. Daily stress, coping, and wellbeing in parents of children with autism: A multilevel modeling approach. J. Fam. Psychol. 2008, 22, 855–864. [Google Scholar] [CrossRef]
- Benson, P.R.; Karlof, K.L. Anger, stress proliferation, and depressed mood among parents of children with ASD: A longitudinal replication. J. Autism Dev. Disord. 2009, 39, 350–362. [Google Scholar] [CrossRef]
- Smith, B.W.; Tooley, E.M.; Christopher, P.J.; Kay, V.S. Resilience as the ability to bounce back from stress: A neglected personal resource? J. Posit. Psychol. 2010, 5, 166–176. [Google Scholar] [CrossRef]
- Phelps, K.W.; McCammon, S.L.; Wuensch, K.L.; Golden, J.A. Enrichment, stress, and growth from parenting an individual with an autism spectrum disorder. J. Intellect. Dev. Disabil. 2009, 34, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Haddock, L.R. Third-wave cognitive behavioral theories with mindfulness-based interventions. In Counseling and Psychotherapy: Theories and Interventions, 7th ed.; Capuzzi, D., Stauffer, M.D., Eds.; American Counseling Association: Alexandria, VA, USA, 2022; pp. 217–236. [Google Scholar]
- Hayes, S.C.; Hofmann, S.G. “Third-wave” cognitive and behavioral therapies and the emergence of a process-based approach to intervention in psychiatry. World Psychiatry 2021, 20, 363–375. [Google Scholar] [CrossRef]
- Whittingham, K. Parents of children with disabilities, mindfulness and acceptance: A review and a call for research. Mindfulness 2014, 5, 704–709. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Wherever You Go, There You Are: Mindfulness Meditation in Everyday Life; Hyperion: New York, NY, USA, 1994. [Google Scholar]
- Marlatt, G.A.; Kristeller, J.L. Mindfulness and meditation. In Integrating Spirituality into Treatment: Resources for Practitioners; Miller, W.R., Ed.; American Psychological Association: Washington, DC, USA, 1999; pp. 67–84. [Google Scholar] [CrossRef]
- Davidson, R.J.; Kabat-Zinn, J.; Schumacher, J.; Rosenkranz, M.; Muller, D.; Santorelli, S.F.; Urbanowski, F.; Harrington, A.; Bonus, K.; Sheridan, J.F. Alterations in brain and immune function produced by mindfulness meditation. Psychosom. Med. 2003, 65, 564–570. [Google Scholar] [CrossRef]
- Jha, A.P.; Stanley, E.A.; Kiyonaga, A.; Wong, L.; Gelfand, L. Examining the protective effects of mindfulness training on working memory capacity and affective experience. Emotion 2010, 10, 54–64. [Google Scholar] [CrossRef]
- Bögels, S.; Hoogsteder, A.; van Tadjen, L. Mindful parenting to reduce parenting stress: Results from a pilot study. J. Child Fam. Stud. 2008, 17, 313–324. [Google Scholar] [CrossRef]
- Singh, N.N.; Lancioni, G.E.; Winton, A.S.; Singh, J. Mindfulness training for parents and their children with ADHD increases the children’s compliance. J. Child Fam. Stud. 2006, 15, 302–315. [Google Scholar]
- Segal, Z.V.; Williams, J.M.G.; Teasdale, J.D. Mindfulness-Based Cognitive Therapy for Depression: A New Approach to Preventing Relapse; Guilford Press: New York, NY, USA, 2002. [Google Scholar]
- Segal, Z.V.; Williams, J.M.G.; Teasdale, J.D. The Mindful Way Workbook: An 8-Week Program to Free Yourself from Depression and Emotional Distress; Guilford Press: New York, NY, USA, 2014. [Google Scholar]
- Bailie, C.; Smith, S.; Garbutt, J. Mindfulness-based cognitive therapy for parents of children with autism spectrum disorders: A qualitative evaluation. J. Child Fam. Stud. 2011, 20, 347–357. [Google Scholar]
- Kabat-Zinn, J.; Kabat-Zinn, M. Everyday Blessings: The Inner Work of Mindful Parenting; (Original work published 1997); Hachette Books: New York, NY, USA, 2014. [Google Scholar]
- Bögels, S.; Hellemans, J.; van Deursen, S.; Römer, M.; van der Meulen, R. Mindful parenting in mental health care: Effects on parental and child psychopathology, parental stress, parenting, co-parenting, and marital functioning. Mindfulness 2010, 1, 107–120. [Google Scholar] [CrossRef] [PubMed]
- Bögels. Full reference details not provided in the current draft; please complete. 2014. [Google Scholar]
- van der Oord, S.; Bögels, S.M.; Peijnenburg, D. The effectiveness of mindfulness training for children with ADHD and mindful parenting for their parents. J. Child Fam. Stud. 2012, 21, 139–147. [Google Scholar] [CrossRef]
- Beer, J.; Fernández, S.; Slusarchuk, C. Mindful parenting and maternal well-being in parents of children with autism spectrum disorder. Mindfulness 2013, 4, 220–233. [Google Scholar] [CrossRef]
- Conner, C.M.; White, S.W. Parenting stress among parents of individuals with autism spectrum disorder: The roles of child characteristics and parental emotional functioning. J. Autism Dev. Disord. 2014, 44, 1862–1868. [Google Scholar] [CrossRef]
- Hanington, L.; Ramchandani, P.; Stein, A. Parental depression and child temperament: Assessing child-to-parent effects in a longitudinal population study. Infant Behav. Dev. 2010, 33, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- Lovibond, S.H.; Lovibond, P.F. Manual for the Depression Anxiety Stress Scales, 2nd ed.; Psychology Foundation of Australia: Sydney, Australia, 1995. [Google Scholar]
- Rayan, A.; Ahmad, M. Mindfulness and parenting distress among parents of children with disabilities: The mediating role of parental self-efficacy. Res. Dev. Disabil. 2017, 69, 52–61. [Google Scholar]
- Tellegen, C.L.; Sanders, M.R. A randomized controlled trial evaluating a brief parenting program with children with autism spectrum disorders. J. Consult. Clin. Psychol. 2014, 82, 1193–1200. [Google Scholar] [CrossRef]
- Lyrakos, G.N.; Arvaniti, C.; Smyrnioti, M.; Kostopanagiotou, G. Translation and validation study of the Depression Anxiety Stress Scale in the Greek general population and in a psychiatric patient’s sample. Eur. Psychiatry 2011, 26(S2), 1731. [Google Scholar] [CrossRef]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The Satisfaction With Life Scale. J. Pers. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef]
- Lyrakos. Greek adaptation of SWLS—full bibliographic details not provided; please complete. 2013. [Google Scholar]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J. Pers. Soc. Psychol. 1988, 54, 1063–1070. [Google Scholar] [CrossRef]
- Benn, R.; Akiva, T.; Arel, S.; Roeser, R.W. Mindfulness training effects for parents and educators of children with special needs. Dev. Psychol. 2012, 48, 1476–1487. [Google Scholar] [CrossRef]
- Daskalou, V.; Sigkollitou, E. Positive and Negative Affect Scale (PANAS). In Psychometric Instruments in Greece, 2nd ed.; Stalikas, A., Triliva, S., Roussi, P., Eds.; Pedio: Athens, Greece, 2012; p. 526. [Google Scholar]
- Duncan, L.G.; Coatsworth, J.D.; Greenberg, M.T. A model of mindful parenting: Implications for parent–child relationships and prevention research. Clin. Child Fam. Psychol. Rev. 2009, 12, 255–270. [Google Scholar] [CrossRef]
- George, D.; Mallery, P. SPSS for Windows Step by Step: A Simple Guide and Reference, 10th ed.; Pearson/Allyn & Bacon: Boston, MA, USA, 2010. [Google Scholar]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E.; Tatham, R.L. Multivariate Data Analysis, 8th ed.; Cengage Learning: Andover, UK, 2019. [Google Scholar]
- Cengiz, Kılıç. RCT in mindfulness literature—full reference details not provided; please complete. 2025. [Google Scholar]
- Alibekova, R.; Chan, C.K.; Crape, B.; Kadyrzhanuly, K.; Gusmanov, A.; An, S.; Bulekbayeva, S.; Akhmetzhanova, Z.; Ainabekova, A.; Yerubayev, Z.; et al. Stress, anxiety and depression in parents of children with autism spectrum disorders in Kazakhstan: Prevalence and associated factors. Global Ment. Health 2022, 9, 472–482. [Google Scholar] [CrossRef] [PubMed]
- Bazzano, A.; Wolfe, C.; Zylowska, L.; Wang, S.; Schuster, E.; Barrett, C. Mindfulness-based stress reduction (MBSR) for parents and caregivers of individuals with developmental disabilities: A community-based approach. J. Child Fam. Stud. 2015, 24, 298–308. [Google Scholar] [CrossRef]
- Lunsky, Y.; Albaum, C.; Baskin, A.; Hastings, R.P.; Hutton, S.; Steel, L.; Wang, W.; Weiss, J. Group Virtual Mindfulness-Based Intervention for Parents of Autistic Adolescents and Adults. J. Autism Dev. Disord. 2021, 51, 3959–3969. [Google Scholar] [CrossRef] [PubMed]
- Azizi, M.; Sanaat, Z.; Jafarnejad, F.; Dadkhah, F. Increasing the tolerance of mothers with children with autism: The effectiveness of cognitive therapy based on mindfulness—experimental research. Ann. Med. Surg. 2023, 86, 207–211. [Google Scholar] [CrossRef]
- Greenberg, J.; Reiner, K.; Meiran, N. “Mind the trap”: Mindfulness practice reduces cognitive rigidity. PLoS ONE 2012, 7, e36206. [Google Scholar] [CrossRef]
- Teasdale, J.D.; Segal, Z.V.; Williams, J.M.G.; Ridgeway, V.A.; Soulsby, J.M.; Lau, M.A. Prevention of relapse/recurrence in major depression by mindfulness-based cognitive therapy. J. Consult. Clin. Psychol. 2000, 68, 615–623. [Google Scholar] [CrossRef] [PubMed]
- Ma, S.H.; Teasdale, J.D. Mindfulness-based cognitive therapy for depression: Replication and exploration of differential relapse prevention effects. J. Consult. Clin. Psychol. 2004, 72, 31–40. [Google Scholar] [CrossRef]
- Sommerhoff, A.; Ehring, T.; Takano, K. Effects of induced mindfulness at night on repetitive negative thinking: Ecological momentary assessment study. JMIR Ment. Health 2023, 10, e44365. [Google Scholar] [CrossRef]
- Hick, S.F.; Chan, L. Mindfulness-Based Cognitive Therapy for Depression: Effectiveness and Limitations. Soc. Work Ment. Health 2010, 8, 225–237. [Google Scholar] [CrossRef]
- Cachia, R.L.; Anderson, A.; Moore, D.W. Mindfulness, stress and well-being in parents of children with autism spectrum disorder: A systematic review. J. Child Fam. Stud. 2016, 25, 1–14. [Google Scholar] [CrossRef]
- Bluth, K.; Wahler, R.G. Does effort matter in mindful parenting? Mindfulness 2011, 2, 175–178. [Google Scholar] [CrossRef]
- Benn. Mindfulness-based program for parents—full reference details not provided; please complete. 2021. [Google Scholar]
- Burgdorf, W.; Szabó, M.; Abbott, M.J. Mindful parenting: A meta-analytic review of effects on parents, children, and parenting. Clin. Psychol. Rev. 2019, 75, 101799. [Google Scholar] [CrossRef]
- Singh, N.N.; Lancioni, G.E.; Karazsia, B.T.; Myers, R.E.; Hwang, Y.S.; Anālayo, B. Effects of mindfulness-based positive behavior support training are equally beneficial for mothers and their children with autism spectrum disorder or with intellectual disabilities. Front. Psychol. 2019, 10, 385. [Google Scholar] [CrossRef] [PubMed]
- Weitlauf, A.S.; Vehorn, A.C.; Taylor, J.L.; Hampton, L.H. A pilot study of a remote parent-mediated early intervention for children with autism. Autism 2020, 24, 1288–1301. [Google Scholar] [CrossRef]
- Cheung, R.Y.M.; Chan, S.K.C.; Chui, H.; et al. Enhancing parental well-being: Initial efficacy of a 21-day online self-help mindfulness-based intervention for parents. Mindfulness 2022, 13, 2812–2826. [Google Scholar] [CrossRef]
- Garland, E.L.; Farb, N.A.; Goldin, P.R.; Fredrickson, B.L. The mindfulness-to-meaning theory: Extensions, applications, and challenges at the attention–appraisal–emotion interface. Psychol. Inq. 2015, 26, 377–387. [Google Scholar] [CrossRef]
- Kunimatsu, M.M.; Marsee, M.A. Examining the presence of anxiety in aggressive individuals: The illuminating role of fight-or-flight mechanisms. Child Youth Care Forum 2012, 41, 247–258. [Google Scholar] [CrossRef]
- Harnett, P.H.; Whittingham, K.; Puhakka, E.; Hodges, J.; Spry, C.; Dob, R. The short-term impact of a brief group-based mindfulness therapy program on depression and life satisfaction. Mindfulness 2010, 1, 183–188. [Google Scholar] [CrossRef]
- Zhang, L. Mindfulness-based interventions and life satisfaction among parents of children with developmental disorders: A systematic review. Int. J. Environ. Res. Public Health 2023, 20. [Google Scholar] [CrossRef]
- Alvarado-García, P.A.A.; Soto-Vásquez, M.R.; Infantes Gomez, F.M.; Guzman Rodriguez, N.M.; Castro-Paniagua, W.G. Effect of a mindfulness program on stress, anxiety, depression, sleep quality, social support, and life satisfaction: A quasi-experimental study in college students. Front. Psychol. 2025, 16, 1508934. [Google Scholar] [CrossRef]
- Li, X.; Ma, L.; Li, Q. How mindfulness affects life satisfaction: Based on the mindfulness-to-meaning theory. Front. Psychol. 2022, 13, 887940. [Google Scholar] [CrossRef]
- Extremera, N.; Rey, L. Ability emotional intelligence and life satisfaction: Positive and negative affect as mediators. Pers. Individ. Dif. 2016, 102, 98–101. [Google Scholar] [CrossRef]
- Hölzel, B.K.; Carmody, J.; Vangel, M.; Congleton, C.; Yerramsetti, S.M.; Gard, T.; Lazar, S.W. Mindfulness practice leads to increases in regional brain gray matter density. Psychiatry Res. Neuroimaging 2011, 191, 36–43. [Google Scholar] [CrossRef]
- Zheng, M.; Hong, T.; Zhou, H.; Garland, E.L.; Hu, Y. The acute effect of mindfulness-based regulation on neural indices of cue-induced craving in smokers. Addict. Behav. 2024, 159, 108134. [Google Scholar] [CrossRef]
- Laurent, H.K.; Duncan, L.G.; Lightcap, A.; Khan, F. Mindful parenting predicts mothers’ and infants’ hypothalamic–pituitary–adrenal activity during a dyadic stressor. Dev. Psychol. 2017, 53, 417–424. [Google Scholar]
- Bergen-Cico, D.; Possemato, K.; Pigeon, W. Reductions in cortisol associated with primary care brief mindfulness program for veterans with PTSD. Med. Care 2014, 52 Suppl. 5, S25–S31. [Google Scholar] [CrossRef]
- González-Martín. Mindfulness and cortisol—full reference details not provided; please complete. 2023. [Google Scholar]
- Ruiz-Robledillo, N.; Moya-Albiol, L. Emotional intelligence modulates cortisol awakening response and self-reported health in caregivers of people with autism spectrum disorders. Res. Autism Spectr. Disord. 2014, 8, 1535–1543. [Google Scholar] [CrossRef]
- Ahmed, A.N.; Raj, S.P. Self-compassion intervention for parents of children with developmental disabilities: A feasibility study. Adv. Neurodev. Disord. 2023, 7, 277–289. [Google Scholar] [CrossRef] [PubMed]
- Ferraioli, S.; Harris, S.L. The impact of mindfulness-based interventions on the well-being of parents of children with autism spectrum disorders: A review. Res. Autism Spectr. Disord. 2013, 7, 1318–1331. [Google Scholar]
- Chan, N.; Neece, C.L. Parenting stress and emotion dysregulation among children with developmental delays: The role of parenting behaviors. J. Child Fam. Stud. 2018, 27, 4071–4082. [Google Scholar] [CrossRef]
- Button, K.S.; Ioannidis, J.P.; Mokrysz, C.; Nosek, B.A.; Flint, J.; Robinson, E.S.; Munafo, M.R. Power failure: Why small sample size undermines the reliability of neuroscience. Nat. Rev. Neurosci. 2013, 14, 365–376. [Google Scholar] [CrossRef]
- Mo, Y.; Lei, Z.; Chen, M.; Deng, H.; Liang, R.; Yu, M.; Huang, H. Effects of self-help mindfulness-based cognitive therapy on mindfulness, symptom change, and suicidal ideation in patients with depression: A randomized controlled study. Front. Psychol. 2023, 14, 1287891. [Google Scholar] [CrossRef] [PubMed]
- De Los Reyes, A.; Kazdin, A.E. Informant discrepancies in the assessment of childhood psychopathology: A critical review, theoretical framework, and recommendations for further study. Psychol. Bull. 2005, 131, 483–509. [Google Scholar] [CrossRef]
- Kuhlthau, K.; Payakachat, N.; Delahaye, J.; Hurson, J.; Pyne, J.M.; Kovacs, E.; Tilford, J.M. Quality of life for parents of children with autism spectrum disorders. Res. Autism Spectr. Disord. 2014, 8, 1339–1350. [Google Scholar] [CrossRef]
- Kabat-Zinn, J.; Kabat-Zinn, M. Mindful Parenting: Guide to Raising Compassionate Kids; Piatkus: London, UK, 2021. [Google Scholar]
Figure 1.
Participants flow chart.
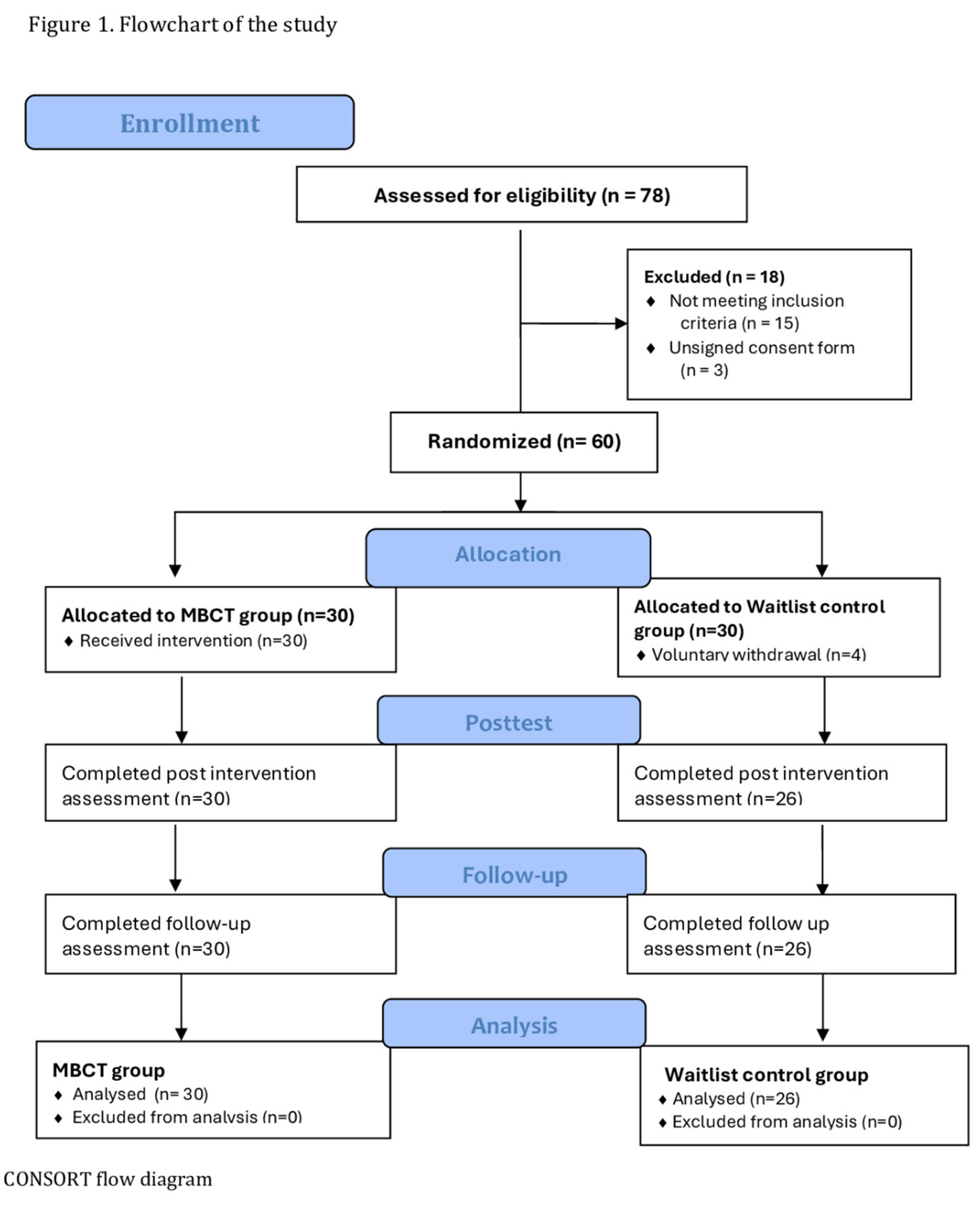
Figure 2.
Changes in Parental Mental Health Outcomes Across Time by Group.
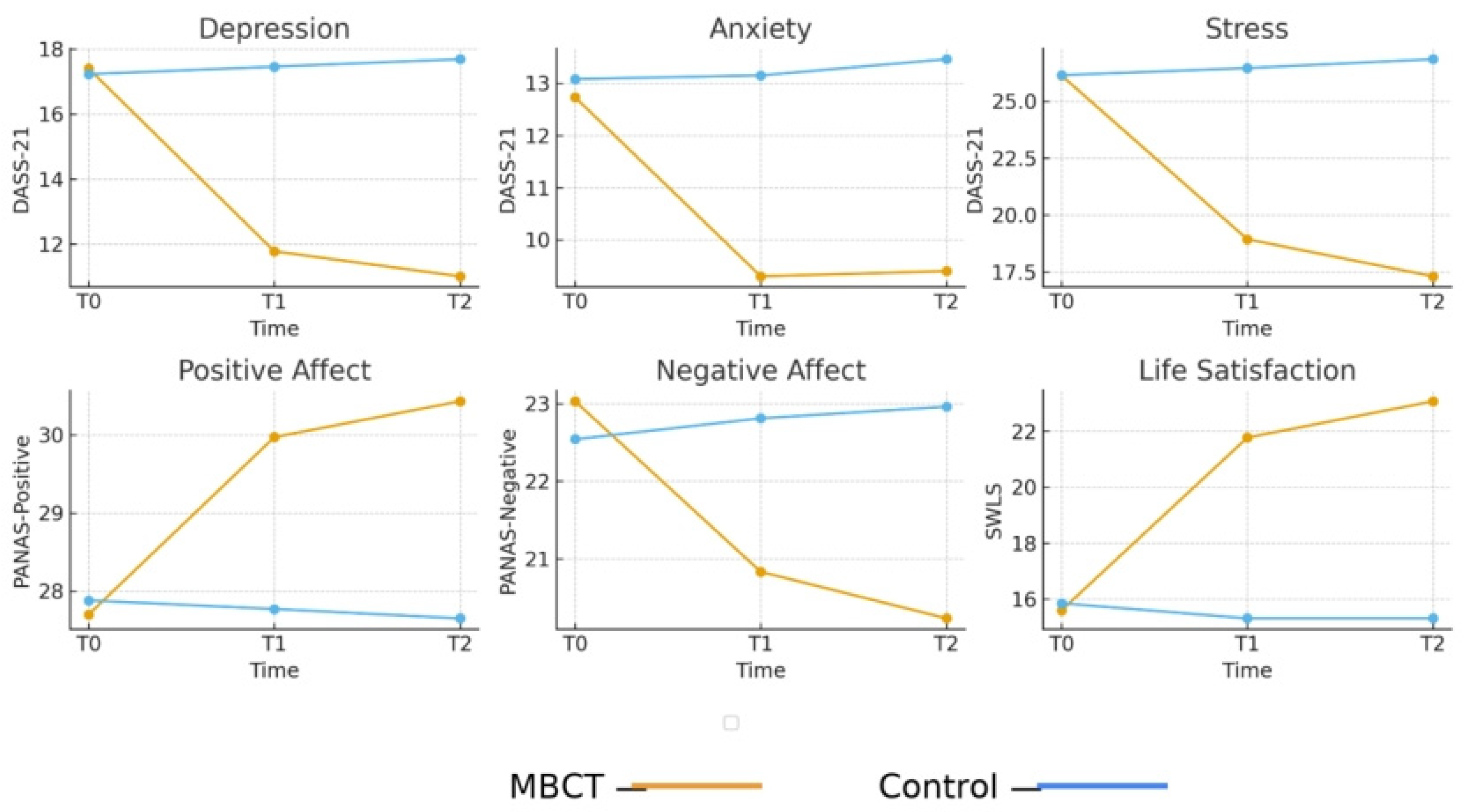

Table 1.
Summary of instruments used in the study.
| Instruments | Items/Subscales | Scoring and Interpretation |
Cronbach’s α (Present Study) |
| DASS-21 [67] (Depression, Anxiety, Stress) |
21 3 subscales (7 items each) |
4-point Likert scale (0–3); subscale scores multiplied by 2; higher scores indicate greater symptom severity. |
Depression=0.75, Anxiety=0.64, Stress=0.82 |
| PANAS [71] (Positive–Negative Affect) |
20; 2 subscales (10 items each) |
5-point Likert scale (1–5); higher PA = greater positive affect, higher NA = greater distress. |
Pos.=0.63 Neg.=0.77 |
| SWLS [73] (Satisfaction with Life) |
5 | 7-point Likert scale (1–7); higher total scores reflect greater life satisfaction. |
Life satisfaction = 0.82 |
Table 2.
Overview of the MBCT Intervention: Session-by-Session Protocol.
| Week / Session | Core Theme | Primary Mindfulness Practices | MBCT / Mindful Parenting Components |
| Week 1 | Awareness and Autopilot | Mindful eating (raisins task); Introduction to body scan | Recognizing automatic parenting reactions; introducing the program structure and group guidelines |
| Week 2 | Facing Obstacles / A Different Way of Knowing | Body scan; Short mindful breathing | Distinguishing “doing” vs. “being” mode; observing difficult parenting thoughts/emotions as mental events |
| Week 3 | Focusing the Scattered Mind | Extended mindful breathing; Mindful movement; 3-minute breathing space | Applying attentional focus before/after challenging parent–child interactions |
| Week 4 | Responding to Experience / Recognizing Aversion | Sitting meditation (breath, body, sounds, thoughts) | Noticing pleasant and unpleasant events in parenting; cultivating nonjudgmental awareness toward the child |
| Week 5 | Allowing and Letting Be | Acceptance-focused meditation (observing difficult emotions) | Allowing parental emotions (guilt, frustration, sadness) to arise without avoidance or suppression |
| Week 6 | Thoughts Are Not Facts | Sitting meditation emphasizing thought awareness | Decentering from self-critical thoughts (e.g., “I am not a good parent”); reframing automatic interpretations |
| Week 7 | Self-Care and Relapse Prevention | Extended sitting meditation | Identifying personal stress triggers; developing a self-care and mindful parenting maintenance plan |
| Week 8 | Maintaining and Extending New Learning | Review of core practices; Choice of preferred meditation | Creating individualized mindful parenting plans; integrating mindfulness into daily routines |
Table 3.
Social and Demographic Characteristics of Participants.
| Variables |
Total participants (n=56) |
MBCT group (n=30) |
Waitlist Control group (n=26) |
χ2/T | P |
| Parental characteristics | |||||
| Gender, n (%) | |||||
| Male | 19 | 9 | 10 | ||
| Female | 37 | 21 | 16 | .445 | .505 |
| Age in years (M/SD) | 40.67 | 40.52 | 40.85 | -.194 | .846 |
| Marital status, n (%) | |||||
| Married | 42 | 22 | 20 (76.9%) | ||
| Divorced | 9 | 4 | 5 | ||
| Single parent | 5 | 4 | 1 | 1 | .421 |
| Education level, n (%) | |||||
| Secondary | 10 | 3 | 7 | ||
| Technical/Technological | 24 | 15 | 9 | ||
| University | 22 | 12 | 10 | 3,011 | .222 |
| Employment status, n (%) |
|||||
| Public employee | 16 | 7 | 9 | ||
| Private employee | 27 | 15 | 12 | ||
| Self-employed | 13 | 8 | 5 | .995 | .608 |
| Child characteristics | |||||
| Gender, n (%) | |||||
| Boy | 45 | 24 | 21 | ||
| Girl | 11 | 6 | 5 | .005 | .942 |
| Age in years (M/SD) | 10.54 | 10.51 | 10.59 | .072 | .942 |
| Duration since diagnosis (M/SD) |
5.84 | 5.78 | 5.9 | -.129 | .897 |
| Severity of child’s behavior problem, n (%) |
|||||
| Mild | 9(16.1%) | 5(16.7%) | 4(15.4%) | ||
| Moderate | 20(35.7%) | 10(33.3%) | 10(38.5%) | ||
| Severe | 27(48.2%) | 15(50%) | 12(46.2%) | .160 | .923 |
Table 4.
Baseline Clinical Characteristics of Participants.
| Indicators | Total Participants (n=56) | MBCT Group (n=30) |
Control Group (n=26) |
t | p |
| M/SD | M/SD | M/SD | |||
| DASS-21 | |||||
| Depression | 17.32±4.29 | 17.4±4.85 | 17.23±3.63 | 3.573 | .168 |
| Anxiety | 13±2.7 | 12.93±3.27 | 13.08±1.90 | 3.098 | .377 |
| Stress | 26.14±4.73 | 26.13±5.01 | 26.15±4.49 | .219 | .896 |
| PANAS | |||||
| Positive Affect | 27.79±2.10 | 27.70±2.45 | 27.88±1.65 | -.334 | .740 |
| Negative Affect | 22.80±2.70 | 23.03±3.35 | 22.54±1.70 | .711 | .481 |
| SWLS | |||||
| Life satisfaction | 15.71±2.81 | 15.6±3.16 | 15.85±2.41 | 1.811 | .770 |
Table 5.
Comparisons of Parental Mental Health Outcomes by Group and Time.
| Indicator | Group |
Μ. ± S.D. (T0) |
Μ. ± S.D. (T1) |
Μ. ± S.D. (T2) |
T0 vs T1 | T0 vs T2 | T1 vs T2 |
Group x Time Interaction (F, p, ) |
| Depression | MBCT | 17.40 ± 4.85 | 11.77 ± 2.67 | 11.00 ± 2.39 | t(29)=10.37,p=<.001, d=1.89 | t(29)=8.52, p=<.001, d=1.56 |
t(29)=2.37, p=0.02, d=0.43 |
F=64.126, p<.001, η²p=0.543 |
| Control | 17.23 ± 3.63 | 17.46 ± 3.28 | 17.69 ± 3.47 | t(25)=−1.14,p=0.265, d=−0.22 | t(25)=−1.54,p=0.136, d=−0.30 |
t(25)=−0.90,p=0.376, d=−0.18 |
||
| Anxiety | MBCT | 12.73 ± 3.50 | 9.40 ± 2.24 | 9.30 ± 2.09 | t(29)=7.53, p=<.001, d=1.37 |
t(29)=6.72, p=<.001, d=1.23 |
t(29)=0.4. p=0.687, d=0.07 |
F=29.298, p< .001, η²p=0.352 |
| Control | 12.92 ± 2.05 | 13.15 ± 2.05 | 13.46 ± 2.16 | t(25) =-1.14, p = 0.265 d=-0.22 |
t(25)=−1.54,p=0.136, d=−0.30 |
t(25)=−0.90, p=0.376, d=−0.18 |
||
| Stress | MBCT | 26.13 ± 5.01 | 18.93 ± 4.48 | 17.30 ± 4.09 | t(29)=16.96,p=<.001, d=3.10 | t(29)=17.56,p=<.001, d=3.21 |
t(29)=4.18, p=<.001, d=0.76 |
F=188.515, p< .001, η²p=0.777 |
| Control | 26.15 ± 4.09 | 26.46 ± 4.09 | 26.85 ± 3.76 | t(25)=-0.39, p=.80, d=-0.047 |
t(25)=−1.17,p=0.025, d=−0.23 | t(25)=−0.65, p=0.50, d=−0.13 |
||
|
Positive Affect |
MBCT | 27.70 ± 2.45 | 29.97 ± 2.34 | 30.43 ± 2.39 | t(29)=−6.38,p=<.001, d=−1.16 |
t(29)=−6.46,p=<.00, d=−1.18 |
t(29)=−2.45,p=0.020, d=−0.45 |
F= 32.066, p < .001, η²p = 0.373 |
| Control | 26.69 ± 3.96 | 27.88 ± 1.66 | 27.65 ± 1.65 | t(25)=−1.28,p=0.211, d=−0.25 | t(25)=−1.01,p=0.323, d=−0.20 |
t(25)=1.19, p=0.247, d=0.23 |
||
| Negative Affect | MBCT | 23.03 ± 3.35 | 20.83 ± 1.72 | 20.23 ± 1.92 | t(29)=4.41, p=<.001, d=0.80 |
t(29)=5.34, p=<.001, d=0.98 |
t(29)=3.67, p=0.001, d=0.67 |
F= 25.267, p < .001, η²p = 0.319 |
| Control | 22.54 ± 1.70 | 22.81 ± 1.90 | 22.96 ± 1.97 | t(25)=0.97, p=0.341, d=-0.19 |
t(25)=−1.53,p=0.139, d=−0.30 | t(25)=−1.69,p=0.103, d=−0.33 |
||
| Life Satisfaction | MBCT | 15.60 ± 3.16 | 21.77 ± 2.97 | 23.07 ± 2.49 | t(29)=−12.5,p=<.001, d=−2.29 | t(29)=−14.8,p=<.001, d=−2.71 |
t(29)=−4.71,p=<.001, d=−0.86 |
F=132.156, p<.001, η²p=0.710 |
| Control | 15.31 ± 1.69 | 15.12 ± 1.53 | 15.04 ± 1.93 | t(25)=0.48, p=0.638, d=0.09 |
t(25)=1.32, p=0.199, d=0.26 |
t(25)=0.20, p=0.844, d=0.04 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



