
Submitted:
26 November 2025
Posted:
27 November 2025
You are already at the latest version
Abstract
Pharmacy-based point-of-care (POC) services have evolved from pilot initiatives to an essential component of decentralized healthcare delivery. These services—ranging from rapid infectious-disease screening to chronic-disease monitoring—improve access, re-duce diagnostic delays and empower pharmacists as front-line healthcare providers. The present paper is the first comprehensive review of the evolution of pharmacy POC services worldwide, combined with the analysis of the regulatory and educational frameworks supporting implementation, technological drivers such as biosensors, mo-bile health and artificial intelligence and in-depth socioeconomic considerations. Bene-fits for patients, pharmacies and healthcare systems are contrasted with challenges in-cluding variable reimbursement, uneven regulatory oversight and workforce preparedness.

Keywords:
artificial intelligence
; community pharmacy
; biosensor
; diagnostics
; digital health
; pharmacy
; point-of-care testing
; quality control
; regulation
; telepharmacy
1. Introduction to Point-of-Care Services in Pharmacies
Community pharmacies are becoming vital nodes in the emerging analytical health network that connects diagnostic chemistry with decentralized clinical practice. Traditionally restricted to dispensing and counseling, pharmacies are now transitioning into localized analytical laboratories where rapid chemical and biochemical measurements are performed at or near the site of patient care. This transition is enabled by the miniaturization of analytical instrumentation, the development of robust biosensing chemistries and the evolution of regulatory frameworks that recognize pharmacists as qualified operators of analytical devices [1,2].
POC testing (POCT), in its strict analytical sense, refers to the in situ measurement of clinically relevant analytes in biological matrices such as blood, saliva or urine using portable or benchtop devices capable of producing quantitative or semi-quantitative results within minutes. The underlying analytical systems are frequently based on electrochemical, optical or immunochemical detection schemes that convert a biochemical recognition event into a measurable signal (Figure 1). Typical analytes encountered in community pharmacy practice include glucose, glycated hemoglobin (HbA1c), C-reactive protein (CRP), cholesterol, triglycerides, troponin I/T and markers of infectious diseases such as influenza or SARS-CoV-2 antigens [3,4].
The COVID-19 pandemic underscored the strategic relevance of distributed analytical capacity. During global lockdowns, pharmacies maintained open access and rapidly deployed antigen and antibody lateral-flow immunoassays under emergency authorization. Subsequent studies demonstrated that pharmacy-performed tests could achieve analytical sensitivities above 90 % and specificities exceeding 95 % when manufacturer protocols and external-quality controls were applied [5,6,7]. This experience catalyzed a paradigm shift: pharmacies are no longer viewed merely as dispensing outlets but as chemically competent micro-laboratories within the healthcare ecosystem [8].
The analytical rationale for integrating pharmacies into POC testing lies in both proximity and chemical fidelity. By reducing the pre-analytical delay—the interval between sample collection and analysis—the integrity of labile analytes (e.g., glucose, lactate, ammonia and certain enzymes) is preserved [9]. Consequently, analytical errors attributable to sample degradation or mishandling decrease dramatically compared with centralized laboratory workflows.
From an analytical chemistry perspective, the expansion of POC testing to pharmacies introduces a new class of end users—trained but non-specialist analytical operators—into the diagnostic value chain. This requires instrument designs that are chemically stable, reagent-integrated and largely automated in calibration and quality control [10]. Cartridge-based reagent systems employ lyophilized or micro-encapsulated chemistries that can withstand variable storage conditions and provide reproducible rehydration kinetics at the moment of testing. The analytical accuracy of such devices is sustained through built-in electrochemical reference systems, optical calibration curves stored on embedded chips and algorithmic temperature compensation [11].
The current review therefore examines the chemical and analytical foundations that enable point-of-care testing in pharmacies, the regulatory infrastructures that guarantee quality and safety and the technological architecture ranging from electrochemical transducers to AI-driven data analytics—that define next-generation diagnostic practice, along with challenges related to economic sustainability of POCT services and the pharmacists educational framework.
2. Evolution and Regulatory Context of Pharmacy-Based Point-of-Care Services
2.1. The Regulatory Landscape
Pharmacies have been a societal mainstay through the delivery of prescription drugs and, to a lesser extent, other products. There is, however, confusion among the public and even the health care community about the definition of and services available from pharmacies, which is a contributing factor to the slow acceptance of pharmacies as full-fledged providers of comprehensive health care [12,13].
The successful implementation of point-of-care services by pharmacies is predicated upon the existence of an appropriate regulatory framework that clearly delineates the scope of practice for pharmacies. The regulatory recognition of pharmacies as analytical testing environments has progressed unevenly across jurisdictions. Early legislative frameworks in Europe and North America focused primarily on good dispensing practice and the stability of pharmaceutical formulations rather than on analytical measurement performed on biological matrices [14]. The introduction of glucose self-testing in the 1980s marked the first major interface between clinical chemistry and community retail environments [15]. Subsequent regulatory milestones—such as the U.S. Clinical Laboratory Improvement Amendments (CLIA, 1988) and the European IVD Directive 98/79/EC (superseded by the IVDR 2017/746)—created the legal category of “waived” or “near-patient” tests [16,17,18]. The CLIA waiver is a certification granted by the Centers for Medicare & Medicaid Services (CMS) in the United States. It allows laboratories, including community pharmacies, to perform specific diagnostic tests that are categorized as "waived." [19]. In Europe, the IVD Directive 98/79/EC established the requirements for marketing in vitro diagnostic medical devices (IVDs) in the EU, allowing most devices to be self-certified with a CE mark. It has since been superseded by the more rigorous In Vitro Diagnostic Regulation (IVDR) 2017/746, which became fully applicable on May 26, 2022, to provide greater patient safety and address significant technological advancements in the field [20]. The IVDR introduces a risk-based classification system and requires more stringent conformity assessments, with the majority of IVDs now needing a Notified Body's involvement for certification. These tests are simple to perform, have a low risk of erroneous results and do not require specialized laboratory personnel or complex equipment. These categories permit operation by non-laboratory professionals provided that analytical systems meet predefined performance and risk criteria. In particular, CLIA-waived POCTs available for use in community pharmacies include (a) antibody/antigen-based lateral flow immunoassays and (b) molecular-based tests employing nucleic acid amplification technologies (NAATs), both for a variety of targets.

Table 1.
Main categories and target applications of CLA-waived POCT available in community pharmacies.
Table 1.
Main categories and target applications of CLA-waived POCT available in community pharmacies.
| Test category | Target application | Reference |
|---|---|---|
| Lateral flow immunoassay | Group A Streptococcus Influenza A & B COVID-19 Human immunodeficiency virus (HIV) Hepatitis C Virus (HCV) Helicobacter pylori Mononucleosis Syphilis |
[21] [22] [23] [24] [25] [26] [27] [28] |
| Molecular-based | Chlamydia Gonorrhea Trichomonas Group A Streptococcus Influenza A & B COVID-19 Respiratory Syncytial Virus (RSV) |
[29] [29] [29] [30] [31] [32] [33] |
Lateral flow assays offer the advantage of rapid results (usually 5-30 min), low cost and ease of use, although visual result interpretation may be subjective and the employment of a reader may be necessary for certain tests. Molecular methods, on the other hand, are highly sensitive and specific, offer multiplex capabilities and are considered more reliable than immunological methods. On the cons side, they are generally characterized by higher cost, longer run times, specific storage requirements for reagents and limited throughput capacity.
From a chemical-analytical standpoint, the challenge for regulators is to ensure that simplified devices still adhere to fundamental principles of metrology—traceability, accuracy, precision, linearity and detection limit—while being operable in non-controlled environments. For pharmacies, this translates into the need for standardized protocols addressing:
- Analytical validation – verification of calibration linearity, limit of detection (LOD), limit of quantification (LOQ) and coefficient of variation (CV %) against reference laboratory methods [34].
- External quality assessment (EQA) – participation in proficiency-testing schemes organized by accredited laboratories [35].
- Internal quality control (IQC) – routine checks using control materials of known concentration; statistical monitoring via Levey-Jennings plots [36].
- Documentation and traceability – use of barcode-encoded reagents and electronic result logging compliant with data-protection legislation [37].
The analytical reliability of pharmacy-based testing also depends on environmental control. Unlike centralized laboratories, pharmacies may experience fluctuating temperature and humidity, especially in resource-limiting settings [38]; thus, devices should ideally incorporate solid-state temperature sensors and correction algorithms. Reagent cartridges should be sealed in foil pouches with desiccants and on-board calibration curves should be periodically updated through software revisions approved by notified bodies [39].
Regulatory evolution increasingly recognizes the chemometric dimension of diagnostics—where measurement uncertainty is not only instrumental but also algorithmic. Under the new European IVDR, manufacturers must provide performance evaluation reports including statistical parameters such as slope, intercept, R² and bias versus reference methods, explicitly linking these to clinical-decision limits. Pharmacies implementing such systems must maintain a Quality Management System (QMS) comparable to ISO 15189 or ISO 22870, adapted to community settings.
Beyond the USA and Europe, regulations regarding POCT in pharmacies may vary. In Australia, for example, the Therapeutic Goods Administration (TGA) classifies pharmacy POC tests as Class 2 in vitro diagnostic devices requiring analytical performance data on sensitivity, specificity, repeatability and stability [40]. Canada’s Health Canada and the U.S. FDA employ similar frameworks but emphasize risk-based categorization (e.g., CLIA-waived, moderate or high complexity). Pharmacies usually operate within the CLIA-waived category, meaning the analytical method must be simple, with a negligible risk of erroneous results [41].
The implication for analytical chemists is profound: regulatory compliance becomes an extension of analytical validation. Instrument calibration, reagent formulation and chemometric algorithms are all audited for reproducibility under real-world use. This ensures that the chemical measurement principles—electrode potential, absorbance, luminescence or antigen-antibody binding kinetics—remain quantitatively traceable to national metrology standards even outside traditional laboratories.
2.2. Internal and External Quality Control
Quality control (QC) procedures in pharmacies mirror those in laboratories, adapted to smaller sample throughput. Two control levels (low/high) should be tested at least daily. Results are plotted on Levey–Jennings charts, enabling visual detection of systematic bias [42]. Westgard multirule criteria (1 2s, 1 3s, 2 2s, R 4s, 4 1s, 10 x) guide accept/reject decisions [43].
That said, participation in external-quality assessment (EQA) programs remains the hallmark of analytical credibility. All participating sites (labs or pharmacies) measure the same blinded control sample. Their results form a peer group distribution. The peer group mean and peer group standard deviation (SD_{peer}) describe how the group performed collectively.
EQA samples are blinded materials analyzed quarterly; z-scores are computed as
where |z| ≤ 2 indicates satisfactory performance [44]. WHO, IFCC and ISO jointly coordinate global EQA schemes. Pharmacies participating through national hubs send monthly QC results to central databases, where z-scores are computed and corrective actions recommended [45].
Global interoperability requires machine-readable analytical data using standardized metadata (analyte ID, method, device lot, calibration file checksum). HL7 FHIR and LOINC codes are now extended to POC devices; for example, LOINC 1558-6 denotes Glucose BldC POC [46] Chemometric compression algorithms (e.g., Principal Component Encoding) allow efficient cloud transfer of high-frequency amperometric data while preserving signal-to-noise ratios
2.3. Regional Implementation Models
Europe
In the EU, the Joint Committee for Traceability in Laboratory Medicine (JCTLM) lists reference methods for creatinine (IDMS), cholesterol (GC-MS) and HbA1c (HPLC) [47]. POC device manufacturers claiming equivalence must demonstrate analytical agreement (slope 0.95–1.05; intercept ±0.1 units; R² ≥ 0.97) versus these reference methods under ISO 17511.
European pharmacies integrate diagnostic chemistry within publicly funded health systems. The UK’s Community Pharmacy Consultation Service authorizes CRP, lipid and influenza POC testing under NHS accreditation [48]. Devices must comply with CE-marking under IVDR 2017/746, which now requires analytical-performance studies, risk analysis (ISO 14971) and clinical-evidence dossiers. Germany’s Apothekenlabor model emphasizes continuous external QC participation (Richtlinie BÄK 2021) [49]
North America
U.S. pharmacies operate under CLIA-waived classification. Analytical chemistry aspects include simplified calibration protocols and on-board controls validated against CLSI EP15 guidelines (precision evaluation using ≤5 replicates × 5 days) [50].
Canada’s provincial authorities (e.g., New Brunswick College of Pharmacists) require adherence to Good Laboratory Practice for Point-of-Care Testing, including traceability to IDMS methods for glucose and creatinine [51].
Asia-Pacific
Australia’s GuildCare POCT program mandates analytical validation prior to public reimbursement [52]. Japanese pharmacies integrate micro-spectrophotometric analyzers under Yakkyoku Shindan Senta (Pharmacy Diagnosis Centers), maintaining calibration certificates issued by the Japan Quality Assurance Organization (JQA) [53].
2.4. Risk Management and Chemical Safety
Pharmacies handling biological samples must adhere to biosafety levels 1–2. Chemical risk analysis includes proper disposal of reagents containing peroxides, azidesor chromogenic substrates (e.g., TMB, ABTS) [54]. Buffer solutions are neutralized before disposal; micro-quantities of heavy-metal salts from electrochemical reference systems are collected as hazardous waste. Integration of micro-total-analysis systems (µTAS) reduces chemical waste to microliter volumes, aligning with green-chemistry principles.
3. Biosensor Technologies and Diagnostic Integration
The technological basis of POC testing in pharmacies encompasses a broad spectrum of analytical, biosensor-based transduction mechanisms unified by the goal of rapid, accurate and miniaturized quantification. At the heart of each device is a chemical or biochemical recognition element coupled to a physical transducer that converts a molecular event into an electrical or optical signal (Figure 2).
3.1. Electrochemical Systems
Electrochemical biosensors dominate pharmacy-grade diagnostics because they combine chemical specificity with low cost and straightforward miniaturization. Amperometric glucose meters—based on glucose oxidase or glucose dehydrogenase catalysis—remain the canonical example. The enzymatic oxidation of glucose generates electrons transferred via mediators (ferricyanide, ferrocene derivatives) to screen-printed carbon electrodes. Modern devices incorporate nanostructured materials (graphene, carbon nanotubes, Au NPs) to enhance electron-transfer kinetics and lower detection limits [55].
Beyond glucose, amperometric or potentiometric principles are applied to cholesterol, lactate, uric acid and electrolytes. Disposable strip-based sensors utilize thin-film microfabrication and integrated reference electrodes (Ag/AgCl) for stability. Calibration is achieved via stored calibration coefficients derived from multi-point laboratory testing [56]. Analytical performance routinely reaches CV < 5 % with correlation coefficients > 0.98 versus standard clinical analyzers.
3.2. Optical and Spectrophotometric Methods
Optical POC systems convert chemical concentration into absorbance, fluorescence or luminescence signals. Photometric lateral-flow assays for infectious diseases use colloidal-gold or latex beads producing color changes detectable by smartphone cameras [57]. Quantitative reflectance photometry—employed in cholesterol and HbA1c meters—relies on LED sources and photodiode detectors calibrated for pathlength and wavelength drift. Chemiluminescent immunoassays (CLIA) are emerging in compact benchtop pharmacy analyzers, providing analytical sensitivity down to pg mL⁻¹ for hormonal or viral markers [58].
3.3. Immunochemical and Molecular Techniques
Pharmacies increasingly deploy immunochemical POC tests utilizing antibody-antigen specificity. The analytical chemistry of these systems depends on surface functionalization of nitrocellulose or polymer membranes with capture antibodies and on enzyme-labeled or nanoparticle-conjugated detection antibodies. Signal intensity correlates with analyte concentration through enzyme kinetics or nanoparticle optical density.
Molecular POC diagnostics—e.g., isothermal nucleic-acid amplification (LAMP, RPA)—are entering pharmacy settings for infectious-disease screening. These methods rely on strand-displacing polymerases and colorimetric indicators (hydroxynaphthol blue, SYBR Green) to report amplification products without thermal cycling. Analytical times of 15–30 min with LODs below 10² copies μL⁻¹ are typical [59]. Cartridge-integrated microheaters ensure precise temperature control critical for reaction fidelity.
3.4. Microfluidics and Lab-on-a-Chip Platforms
Microfluidic systems miniaturize entire analytical workflows—sample metering, reagent mixing, reaction, separation and detection—onto polymer chips fabricated via soft lithography. These devices handle microliter volumes, reducing reagent consumption and improving reaction kinetics through enhanced surface-to-volume ratios [60]. For pharmacy use, disposable microchips preloaded with reagents enable multiplex analysis of lipids, glucose and inflammatory markers. Capillary forces or centrifugal motion drive fluid transport; detection is performed electrochemically or optically [61].
Chemical compatibility and stability are key challenges: reagents must remain active over shelf lives exceeding one year under ambient storage. Encapsulation techniques (sol-gel matrices, sugar-based stabilizers) preserve enzymatic or antibody activity, while on-chip drying under controlled humidity ensures reproducible reconstitution upon sample addition [62].
3.5. Integration, Data Handling and Chemometrics
Modern pharmacy analyzers integrate sensors with microcontrollers capable of performing calibration, baseline correction and chemometric modeling. Algorithms based on partial-least-squares (PLS) regression, principal-component analysis (PCA) or neural-network classifiers interpret multivariate signals, distinguishing true analyte responses from background noise [63]. Such processing transforms raw amperometric or optical data into clinically actionable concentrations.
The chemical performance of POC devices is evaluated using key analytical metrics such as:
- -
- Sensitivity (S) = ΔSignal/ΔConcentration
- -
- Limit of Detection (LOD) = 3σ / S
- -
- Selectivity determined by cross-reactivity studies with structurally related analytes
- -
- Repeatability and Reproducibility expressed as intra- and inter-assay CVs
- -
- Analytical recovery using spiked control materials
Reported LODs for modern electrochemical POC sensors reach 10⁻⁶–10⁻⁹ M for metabolites and 10⁻¹² M for immunoassays, bridging the gap between benchtop analyzers and laboratory instruments [64].
Integration with telehealth systems allows pharmacists to transmit chemically validated results to physicians within minutes, closing the analytical loop between measurement and medical decision. Connectivity is achieved through Wi-Fi or Bluetooth modules, allowing automatic upload of anonymized data to cloud servers for epidemiological aggregation. Data integrity is ensured via checksum verification and encryption compliant with General Data Protection Regulation (GDPR) and Health Insurance Portability and Accountability Act (HIPAA). Pharmacies thus become chemical data nodes—autonomous yet networked laboratories contributing real-time analytical information to population-level health monitoring.
4. Benefits, Challenges and Economic Considerations of Point-of-Care Services in Pharmacies
4.1. Benefits and Challenges
An increasing number of pharmacies around the world are providing POC services, which include a variety of clinical services such as screening, diagnostic tests, health risk assessment and monitoring of disease or medication. Several studies suggested benefits of POC services related to the healthcare system, pharmacy sector, patients and society overall; yet, in contrast, numerous challenges have also been reported [65]. On a broader level, a healthcare system benefit involving POC services is the decrease in morbidity and mortality and better health management among the population. POC services in pharmacies have the potential to improve outcomes for patients with chronic illnesses, thereby reducing hospital admissions and the overall burden on health services [66]. With respect to pharmacy sector benefits, the competitive edge and profitability of pharmacies can be improved as a result of different revenue streams generated from POC services. Moreover, pharmacies providing professional POC services are likely to attract more foot traffic, increasing the sale of both medications and over-the-counter products [67]. From the perspective of patients, closer monitoring helps improve the effectiveness of drug therapy. Promptly receiving the test results and medical advice can benefit the patients' health status, particularly in emergency cases. The societal benefit stated is drug resistance prevention, currently an important global concern. POC tests help adhere to good prescribing practices, hence improving the quality and safety of treatment [68] (Figure 3).
Challenges of POC services in pharmacies are also numerous. One major issue is the unsound knowledge of existing POC technologies, devices, tests and services, which appears to be common among pharmacists as well as pharmacy owners. Other challenges include the lack of necessary facilities at pharmacies to set up POC services, inappropriate reimbursement policies in the case of unpaid professional service, concerns regarding false results from devices employed, poor perception of test inaccuracy among pharmacy staff and a shortage of trained staff to carry out the POC tests [69,70]. Lack of managerial vision as to how the pharmacy will be fitted into the delivery of healthcare services in terms of POC or non-POC testing was also cited as a barrier to the implementation of POC services with reference to the pharmacy owner [71,72]. Such barriers pointed at the pharmacy sector are likely to discourage pharmacists from using or implementing POC services. Despite the challenges mentioned above, pharmacy-based POC services present numerous advantages and great prospects in countries where pharmacies are easily reachable. As part of the larger healthcare team, pharmacists can contribute positively to improving health outcomes. To promote the sustainable development of pharmacy-based POC services, opportunities to increase awareness and understanding of POC services must be created among pharmacy staff.
Benefits and challenges of pharmacy-based POC services are summarized in the following Table 2:
4.2. Economic, Policy and Sustainability Considerations
The economics of POC diagnostics depend on the cost-per-test (CPT) and the cost-per-accurate-result (CPAR), where CPAR = CPT / (1 – p_error). If analytical error probability (p_error) = 0.05, a €5 test effectively costs €5.26 per reliable measurement. Thus, investments in calibration and QC reduce overall healthcare expenditure by lowering p_error [73].
In order to adopt a policy of providing POCT as a service, capital costs per pharmacy would include equipment costs (for molecular, automated and/or high throughput analysis), quality testing reagents, test reagents and associated software [74]. The estimated cost for said investment is broken down in the following Table 3:
For pharmacies offering POCT services, economic models show break-even at ~600 tests/year when reimbursement ≥ €7/test [75,76,77]. In addition, a cost–benefit meta-model shows return on investment > 300 % within 3 years for networks exceeding 100 pharmacies [78]. On the other hand, reducing diagnostic (analytical) uncertainty doubles the so-called Value-of-Information (VoI) index, as described by the following equation:
VoI = ΔHealth Outcome / Analytical Uncertainty
In other words, reducing analytical uncertainty from ±10 to ±5 % will double VoI, even if equipment costs rise by 20 %. Hence, public health funding agencies and insurance companies increasingly evaluate diagnostics through Value-of-Information rather than unit cost [79]. In the same context, chemometric analysis of national datasets report a cost elasticity with respect to analytical precision in the order of –€0.8 million per 1 % precision gain. Thus, for every 1 % improvement in CV a reduction of national diagnostic costs in the height of ca. €800 000/year could be expected for mid-size countries and economies [80]. Moreover, quantitative risk assessment models express Net Analytical Benefit (NAB) according to the following equation:
NAB= (Clinical Benefit × Accuracy) – (Cost × Error Probability)
whereas sensitivity analysis reveals a positive NAB at accuracy levels higher than 92 %, even at test cost levels of €10 [81]. In other words, improving diagnostic accuracy yields exponential societal and economic return.
In the context of public health policy, a model proposed by OECD in 2024 showed that adoption of a nationwide pharmacy-based POC testing (by shortening treatment initiation by 1.2 days on average) could reduce diagnostic-delay associated health costs by €2.8 billion/year in the EU. Using a productivity-loss coefficient of €160/day, an economic benefit of ca. €192/patient has been calculated [82].
Clinical trials, albeit few, have demonstrated the societal impact of POCT in improving primary health in the general population, in particular by improving control of diabetes, lipidemia and respiratory infection, as shown in the following Table 4:
5. Pharmacist Training and Education for POCT Services
The provision of POCT services in pharmacies necessitates adequate training and education for pharmacists. Both pre-service and in-service training programs are essential for equipping pharmacists with the necessary skills and competencies to effectively deliver point-of-care services. Training programs should cover a range of topics, including clinical knowledge, point-of-care testing procedures, quality control, data interpretation, communication skills and patient management [86]. Pre-service education should be integrated into pharmacy curricula to ensure that future pharmacists are adequately prepared to provide point-of-care services.
The introduction of analytical measurement into community pharmacies represents not only a regulatory expansion of professional scope but also a profound shift in the epistemology of pharmaceutical science: the pharmacist must acquire analytical literacy comparable to that of a laboratory technologist [87].
Unlike traditional compounding or dispensing activities, POC testing requires quantitative reasoning, calibration control and understanding of chemical interferences—skills typically associated with analytical chemistry curricula.
Undergraduate pharmacy programs increasingly integrate applied analytical chemistry modules that cover the principles of spectrophotometry, electrochemistry and immunoassay kinetics. However, global curricula audits reveal that fewer than 40 % of accredited programs dedicate more than one semester to practical diagnostic chemistry [88].
A competency-based model for diagnostic education in pharmacy should include:
- Analytical Chemistry Core – stoichiometry of assays, Beer–Lambert law, electrochemical potentials and reaction equilibria.
- Instrumental Analysis – calibration curves, signal processing, blank subtraction and sensitivity calculation.
- Bioanalytical Techniques – enzyme kinetics, antibody–antigen binding thermodynamics (Ka, Kd) and enzyme-linked detection.
- Quality Management – statistical process control, uncertainty estimation and ISO 15189 principles.
- Clinical Correlation – translation of numerical results to therapeutic decisions.
Educational institutions should collaborate with relevant stakeholders to develop standardized training programs and guidelines for the integration of point-of-care services into pharmacy education. Continuing education programs should be developed and implemented to provide ongoing training and support for practicing pharmacists. These programs can be delivered through various formats, including workshops, seminars, online courses and on-the-job training. Collaboration between pharmacy organizations and educational institutions is crucial for the successful implementation of continuing education programs. Support and resources should be provided to facilitate the implementation of training and education programs [89]. This includes the development of training materials, guidelines and resources for pharmacists and educational institutions. Financial and logistical support may also be necessary, particularly for low-resource settings. Collaboration and partnerships among stakeholders are vital for the successful training and education of pharmacists in point-of-care services. By working together, stakeholders can share resources, knowledge and expertise, ensuring that pharmacists are adequately trained and supported in their delivery of point-of-care services.
6. Integration of Digital Technologies, Mobile Health (mHealth) and Artificial Intelligence in Point-of-Care Services
6.1. Integration with Telepharmacy and Remote Supervision
Advancements in technology have facilitated the development and utilization of innovative tools that enhance the efficiency and effectiveness of point-of-care services. These technologies can be broadly categorized into telemedicine, mobile health applications and health information systems, which provide unique advantages to pharmacies and their clientele. Telemedicine allows for real-time remote consultations between healthcare professionals and patients, resulting in time, cost and convenience savings, especially for those living in rural areas [90,91]. Telepharmacy, a unique aspect of telemedicine, enables the provision of pharmaceutical care through digital means, allowing pharmacists to perform medication reviews, provide counseling and confirmation of prescriptions and assess the appropriateness of therapy, dosage and potential drug interactions. Telepharmacy has improved medication adherence rates and the overall health of patients in several states and various countries [92].
Health information systems, comprising equipment and processes that collect, manage and analyze healthcare data, provide valuable benefits such as automation that enhances efficiency and control over data management, improved operational performance and the ability to aggregate information and analyze it statistically to improve the quality of services [93,94]. These systematic and automatic approaches to managing health information help minimize errors associated with manual handling and provide abundant and quick access to telecommunication possibilities. These widely used systems merit further exploration.
Despite the evident social benefits of POCT services, their uptake and development among pharmacies remain inadequate. Barriers such as insufficient knowledge of the services, concerns regarding the impact on patient health and pharmacy workload and doubts about the viability and profitability of point-of-care services impede the widespread implementation of these services. [65] Young and newly graduated pharmacists perceive greater potential for expanding these services compared to older pharmacists nearing retirement, suggesting a viewpoint influenced by their professional experience. While it is considered vital to actively promote the development of point-of-care services, attempts to increase awareness, participation or professional capacity must be tailored to the unique characteristics of target populations [95].
6.2. Artificial Intelligence and Decision Support for Pharmacy-Based Point-of-Care Testing
The increasing digitalization of diagnostic workflows in community pharmacies creates fertile ground for the integration of artificial intelligence (AI) and advanced chemometric decision-support systems [96]. While POC devices already incorporate embedded algorithms for calibration and signal interpretation, AI extends this analytic layer toward multivariate pattern recognition, risk stratification and individualized therapeutic recommendations. In the context of pharmacy-based POCT, AI can operate at three main levels: (i) signal-level processing, (ii) result-level interpretation and (iii) population-level learning and feedback [97].
At the lowest level, AI and machine-learning (ML) models enhance the interpretation of raw analytical signals generated by electrochemical, optical or immunochemical sensors [98]. Traditional calibration approaches rely on linear or polynomial regression linking signal intensity to analyte concentration; however, real-world pharmacy environments introduce non-linearities, matrix effects and time-dependent drift that are not always well modeled by simple functions.
Machine-learning algorithms such as support-vector regression (SVR), random forests and artificial neural networks (ANNs) can be trained on large datasets of POC signals and corresponding reference laboratory values to learn complex, non-linear mapping functions. These models correct for temperature fluctuations, lot-to-lot variation of reagents and interfering species by implicitly capturing multidimensional relationships between sensor responses and experimental conditions [99]. In voltammetric and amperometric sensing, for example, convolutional neural networks (CNNs) can ingest full current–potential curves and return calibrated analyte concentrations with higher robustness than single-point peak analysis.
Such AI-driven chemometric engines are particularly relevant for multiplex POC platforms, where multiple analytes are measured simultaneously and overlapping spectral or electrochemical signatures occur. By using multivariate calibration (partial least squares, principal-component regression) combined with non-linear ML models, the system can deconvolute overlapping responses and maintain analytical performance—expressed as low bias and coefficient of variation (CV)—even in more complex panels.
At the result level, AI acts as a clinical decision-support system (CDSS) embedded in pharmacy workflows. Once a quantitative value (e.g., HbA1c, CRP, lipid profile, troponin) is produced by the POC device, it must be interpreted in the context of patient-specific factors such as age, comorbidities, medication history and previous test results [100]. Rule-based systems, often derived from clinical guidelines, can encode thresholds and decision trees (e.g., “if CRP < 20 mg/L and no severe symptoms, defer antibiotics”).
However, more sophisticated AI approaches can identify patterns across multiple biomarkers and time points, better reflecting the multi-dimensional nature of disease. Gradient-boosted decision trees and Bayesian networks can integrate POC measurements with electronic health record (EHR) summaries to compute individualized risk scores—for example, estimating the probability of poor glycaemic control, imminent cardiovascular events or bacterial vs viral etiology in respiratory infections [101]. For pharmacists, these outputs can be visualized as traffic-light indicators (green/amber/red) or quantitative risk probabilities that support clinical judgment rather than replace it.
This AI-assisted interpretation is particularly relevant in community settings where pharmacists may have limited time and incomplete access to full medical records [102]. By embedding evidence-based algorithms—derived from clinical-trial and real-world outcome data—into the pharmacy information system, the POC result can immediately trigger suggested actions: intensification of lifestyle counselling, recommendation to consult a physician, medication review or repeat testing after a defined interval.
The different levels of AI integration across the three analytical and clinical layers of pharmacy-based POCT are graphically summarized in the following Figure 4.
6.3. Population-Level Learning and Continuous Performance Optimization
Telepharmacy and mHealth applications further enhance communication, enabling remote consultations and electronic record integration. AI and machine learning support decision-making through automated result interpretation, risk stratification and clinical recommendations. Health-information systems interlink data from pharmacy tests with national surveillance networks, improving epidemic response and pharmacovigilance. At the population level, pharmacy POC networks generate large volumes of high-frequency analytical data [103]. AI-based analytics applied at this scale can detect trends that are invisible at the individual-pharmacy level, such as emerging outbreaks, systematic device drift or geographically clustered anomalies [104].
Unsupervised learning methods (e.g., clustering, anomaly detection) can identify pharmacies whose QC performance deviates from the peer distribution, prompting targeted technical support or recalibration. Similarly, time-series models applied to anonymized POC markers (e.g., CRP, influenza antigen tests) across regions can serve as early-warning systems for respiratory epidemics or other public-health threats [105]. Crucially, these AI models can be continuously updated through federated-learning frameworks, where model training occurs locally at each node (pharmacy) and only model parameters, not raw patient data, are shared [106]. This approach enhances privacy while still allowing global improvement of predictive performance.
7. Future Directions, Implementation Barriers and Opportunities for Pharmacies in Point-of-Care Services
The future of pharmacies in point-of-care services appears promising amidst a dynamic and evolving healthcare landscape. The COVID-19 pandemic has underscored the importance of pharmacies in public health response and community-based care. This pivotal role creates new opportunities for pharmacies to expand and enhance healthcare services, particularly in testing and monitoring. With growing consumer demand for healthcare services that are convenient, efficient and accessible, the use of portable testing devices or kits for screening and monitoring health and disease is increasing. To take advantage of this growth, there are significant opportunities for pharmacies to establish themselves as competent entrepreneurs in their communities, particularly in chronic disease management, wellness and preventive care and infectious disease screening.
With digital technologies advancing rapidly and poised to reconfigure the pharmacy landscape, a revolutionary transformation of pharmacy services is becoming more probable, facilitated by emerging technologies such as AI, big data analytics, mHealth and digital health. There is an opportunity for pharmacies to embrace these emerging technologies to redesign traditional pharmacy services to become more value-added. Big data analytics can help analyze health data at the population level to generate insights to improve wellness and preventive healthcare services. Digital health and affiliated technologies can help automate the drug dispensing process and the flow of drug-related information, thereby improving the efficiency and effectiveness of pharmacy services and freeing up pharmacists to perform healthcare services.
Despite the many opportunities in point-of-care services, there are several potential challenges that may inhibit the growth and sustainability of these services in pharmacies. These potential challenges include deficiencies in pharmacy management and operation, pharmacy and pharmacist reimbursement, pharmacy and pharmacist education and trainingand pharmacy-facilitated patient education and information. Because these services are pharmacy-based, management and operation are crucial to the success of these services [107]. There is a lack of management policies, strategies and guidelines to help pharmacy managers run and administer pharmacy-based services effectively and efficiently [108]. This deficiency may become a stumbling block to the initiation and operation of pharmacy-based services. Lack of reimbursement for pharmacy-based services is one of the main barriers to the growth and sustainability of these services worldwide, along with knowledge gaps regarding device accuracy and maintenance and the resistance from other healthcare providers unaware of pharmacists’ diagnostic competencies [109]. In this context organized interprofessional collaboration between pharmacies and other healthcare providers is scarce. Non-collaborative pharmacy practices are a barrier to pharmacists' participation in established collaborative roles. Lack of knowledge regarding other providers' collaborative roles is a barrier for healthcare providers, especially physicians, to refer patients to collaborative pharmacy services. Thus, raising awareness is vital to implement potential interprofessional collaboration practices. Finally, professional associations could play a crucial role in establishing accreditation and continuous professional-development pathways.
Patient perspectives and satisfaction with pharmacy point-of-care services are equally important factors that can affect the effectiveness of these services. Understanding patient perspectives and factors that predict satisfaction is necessary to ensure the continuous provision of these services by community pharmacies in the future [114]. Previous research indicated that offering an easy definition and providing examples of services can enhance patient understanding. Respondents expressed a strong desire for more decentralized health services, especially those covered by the health insurance system [115]. However, desired services providing free treatments caused a negative reaction. While patients wanting more services tended to be older and have a higher number of prescriptions, these characteristics could not be directly linked to desired pharmacy point-of-care services. Services classified as important did not correlate with a high percentage of respondents desiring the service [116].
8. Conclusions
The expanded role of the pharmacy workforce, including pharmacists as direct care providers, is a growing trend throughout the world. Pharmacy-based point-of-care services redefine the pharmacist’s role as a clinical decision-support professional. They can deliver faster diagnostics, personalized interventions and improved public-health outcomes.
Technological progress and favorable policy will continue to expand this domain. The challenge for the coming decade is ensuring consistent education, equitable reimbursement and digital interoperability, transforming every community pharmacy into a connected health hub. The Global Strategy on Human Resources for Health includes the expansion of practice roles and responsibilities, in conjunction with an increase in the number of students entering pharmacy education programs and the establishment of pharmacy schools, as key global workforce strategies addressing medication-related health problems [117]. Pharmacists will need to implement direct patient care services, including but not limited to medication therapy management, immunizations, smoking cessation counseling, disease management, health screenings and other patient care services. The ability to provide expanded patient care services will depend on the practice environment and workplace setting, regulations and laws governing pharmacists’ scope of practice and reimbursement policies governing the payment for pharmacy services.
Author Contributions
Conceptualization, M.D. and S.K.; methodology, M.D.; investigation, M.D.; writing—original draft preparation, M.D.; writing—review and editing, S.K.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AI ANNs CLIA CMS CLIA CDSS CV % CNNs CPT CPAR CRP EHR EQA GDPR Hba1c HIPAA HIV HCV IQC IVDR JCTLM LOD LOQ ML μTAS mHealth NAB NAATs PLS POC POCT PCA QC QMS RSV SVR TGA VOI |
Artificial Intelligence Artificial Neural Networks Clinical Laboratory Improvement Amendments Centers For Medicare & Medicaid Services Chemiluminescent Immunoassays Clinical Decision-Support System Coefficient Of Variation Convolutional Neural Networks Cost-Per-Test Cost-Per-Accurate-Result C-Reactive Protein Electronic Health Record External Quality Assessment General Data Protection Regulation Glycated Hemoglobin Health Insurance Portability and Accountability Act Human Immunodeficiency Virus Hepatitis C Virus Internal Quality Control In Vitro Diagnostic Regulation Joint Committee For Traceability In Laboratory Medicine Limit Of Detection Limit Of Quantification Machine Learning Micro-Total-Analysis Systems Mobile Health Net Analytical Benefit Nucleic Acid Amplification Technologies Partial-Least-Squares Regression Point-Of-Care Point-Of-Care Testing Principal-Component Analysis Quality Control Quality Management System Respiratory Syncytial Virus Support-Vector Regression Therapeutic Goods Administration Value-Of-Information |
References
- Chan, J.T.N.; Nguyen, V.; Tran, T.N.; Nguyen, N.V.; Do, N.T.T.; van Doorn, H.R.; Lewycka, S. Point-of-care testing in private pharmacy and drug retail settings: A narrative review. BMC Infect. Dis. 2023, 23, 551. [Google Scholar] [CrossRef] [PubMed]
- Santana, C.R.; de Oliveira, M.G.G.; Camargo, M.S.; Moreira, P.M.B.; de Castro, P.R.; Aguiar, E.C.; Mistro, S. Improving pharmaceutical practice in diabetes care using point-of-care glycated haemoglobin testing in the community pharmacy. Int. J. Pharm. Pract. 2024, 32, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Ihekoronye, R.M.; Akande, O.-O.D.; Osemene, K.P. Management of Point-of-Care Testing (POCT) Services by Community Pharmacists in Osun State Nigeria. Innov. Pharm. 2023, 14, 5576. [Google Scholar] [CrossRef] [PubMed]
- Figueira, I.; Teixeira, I.; Rodrigues, A.T.; Gama, A.; Dias, S. Point-of-care HIV and hepatitis screening in community pharmacies: A quantitative and qualitative study. Int. J. Clin. Pharm. 2022, 44, 1–12. [Google Scholar] [CrossRef]
- Widayanti, A.W.; Haulaini, S.; Kristina, S.A. Pharmacists’ roles and practices in pharmaceutical services during COVID-19 pandemic: A qualitative study. Indones. J. Pharm. 2022, 401–411. [Google Scholar] [CrossRef]
- Hoti, K.; Jakupi, A.; Hetemi, D.; Raka, D.; Hughes, J.; Desselle, S. Provision of community pharmacy services during COVID-19 pandemic: A cross-sectional study of community pharmacists’ experiences with preventative measures and sources of information. Int. J. Clin. Pharm. 2020, 42, 1197–1206. [Google Scholar] [CrossRef]
- Dzierba, A.L.; Pedone, T.; Patel, M.K.; Ciolek, A.; Mehta, M.; Berger, K.; Ramos, L.G.; Patel, V.D.; Littlefield, A.; Chuich, T.; et al. Rethinking the Drug Distribution and Medication Management Model: How a New York City Hospital Pharmacy Department Responded to COVID-19. J. Am. Coll. Clin. Pharm. 2020, 3, 1471–1479. [Google Scholar] [CrossRef]
- Klepser, D.G.; Klepser, N.S.; Adams, J.L.; Adams, A.J.; Klepser, M.E. The impact of the COVID-19 pandemic on addressing common barriers to pharmacy-based point-of-care testing. Expert Rev. Mol. Diagn. 2021, 21, 751–755. [Google Scholar] [CrossRef]
- Auvet, A.; Espitalier, F.; Grammatico-Guillon, L.; Nay, M.A.; Elaroussi, D.; Laffon, M.; Andres, C.R.; Legras, A.; Ehrmann, S.; Dequin, P.F.; et al. Preanalytical conditions of point-of-care testing in the intensive care unit are decisive for analysis reliability. Ann. Intensive Care 2016, 6, 57. [Google Scholar] [CrossRef]
- Nayak, S.; Blumenfeld, N.R.; Laksanasopin, T.; Sia, S.K. Point-of-care diagnostics: Recent developments in a connected age. Anal. Chem. 2017, 89, 102–123. [Google Scholar] [CrossRef]
- Hitzbleck, M.; Gervais, L.; Delamarche, E. Controlled release of reagents in capillary-driven microfluidics using reagent integrators. Lab Chip 2011, 11, 2680–2685. [Google Scholar] [CrossRef]
- Cunha Leal, M.L.G.; Rodrigues, A.R.; Bell, V.; Forrester, M. Exploring the evolving role of pharmaceutical services in community pharmacies: Insights from the USA, England, and Portugal. Healthcare 2025, 13, 1786. [Google Scholar] [CrossRef] [PubMed]
- Policarpo, V.; Romano, S.; António, J.H.C.; et al. A new model for pharmacies? Insights from a quantitative study regarding the public’s perceptions. BMC Health Serv. Res. 2019, 19, 186. [Google Scholar] [CrossRef]
- Minghetti, P.; Pantano, D.; Gennari, C.G.; Casiraghi, A. Regulatory framework of pharmaceutical compounding and actual developments of legislation in Europe. Health Policy 2014, 117, 328–333. [Google Scholar] [CrossRef] [PubMed]
- Olczuk, D.; Priefer, R. A history of continuous glucose monitors (CGMs) in self-monitoring of blood glucose. Diagnostics 2024, 14, 2223. [Google Scholar]
- Adusumalli, R.; Banala, R.R. Advancements in prenatal diagnostics and the effects of EU regulatory frameworks, including the IVDR and MDR: A systematic review. Egypt J. Med. Hum. Genet. 2025, 26, 164. [Google Scholar] [CrossRef]
- Klepser, M.; Koski, R.R. Molecular point-of-care testing in the community pharmacy setting: Current status and future prospects. Expert Rev. Mol. Diagn. 2022, 22, 1–12. [Google Scholar] [CrossRef]
- Adams, A.J.; Klepser, D.G.; Klepser, M.E.; Adams, J.L. Pharmacy-based point-of-care testing: How a “standard of care” approach can facilitate sustainability. Innov. Pharm. 2021, 12, 4290. [Google Scholar] [CrossRef]
- Rivers, P.A.; Dobalian, A.; Germinario, F.A. A review and analysis of the Clinical Laboratory Improvement Amendments of 1988: Compliance plans and enforcement policy. Health Care Manag. Rev. 2005, 30, 93–102. [Google Scholar] [CrossRef]
- Kahles, A.; Goldschmid, H.; Volckmar, A.L.; Ploeger, C.; Kazdal, D.; Penzel, R.; Budczies, J.; Flechtenmacher, C.; Gassner, U.M.; Brüggemann, M.; et al. Regulation (EU) 2017/746 (IVDR): Practical implementation of Annex I in pathology. Pathologie 2023, 44, 86–95. [Google Scholar] [CrossRef]
- Fraser, H.; Gallacher, D.; Achana, F.; et al. Rapid antigen detection and molecular tests for group A streptococcal infections: Systematic reviews and economic evaluation. Health Technol. Assess. 2020, 24, 1–262. [Google Scholar] [CrossRef] [PubMed]
- Damhorst, G.L.; Lam, W.A. Point-of-care and home-use influenza diagnostics for advancing therapeutic and public health strategies. J. Infect. Dis. 2025, 232, S314–S326. [Google Scholar] [CrossRef] [PubMed]
- Goux, H.; Green, J.; Wilson, A.; Sozhamannan, S.; Richard, S.A.; Colombo, R.; Lindholm, D.A.; Jones, M.U.; Agan, B.K.; Larson, D.; et al. Performance of rapid antigen tests to detect SARS-CoV-2 variant diversity and correlation with viral culture positivity. mBio 2024, 15, e02737–24. [Google Scholar] [CrossRef] [PubMed]
- Stevens, D.R.; Vrana, C.J.; Dlin, R.E.; Korte, J.E. A global review of HIV self-testing: Themes and implications. AIDS Behav. 2018, 22, 497–512. [Google Scholar] [CrossRef]
- Saifullah, M.; Khan, M.; Usman, M.A.; Mehmood, Q.; Mehdi, A.M. OraQuick hepatitis C virus self-test: A new frontier in hepatitis C screening. World J. Virol. 2025, 14, 109614. [Google Scholar] [CrossRef]
- Graham, D.Y.; Evans, D.J., Jr.; Peacock, J.; Baker, J.T.; Schrier, W.H. Comparison of rapid serological tests with ELISA for detection of Helicobacter pylori. Am. J. Gastroenterol. 1996, 91, 942–948. [Google Scholar]
- Kiiskinen, S.J.; Luomala, O.; Häkkinen, T.; Lukinmaa-Åberg, S.; Siitonen, A. Evaluation of serological point-of-care testing of infectious mononucleosis by external quality samples. Microbiol. Insights 2020, 13, 1178636120977481. [Google Scholar] [CrossRef]
- Goza, M.; Kulwicki, B.; Akers, J.M.; Klepser, M.E. Syphilis screening: A review of the Syphilis Health Check rapid immunochromatographic test. J. Pharm. Technol. 2017, 33, 53–59. [Google Scholar] [CrossRef]
- Reddy, K.; Hao, J.; Sigcu, N.; Govindasami, M.; Matswake, N.; Jiane, B.; et al. Validation of rapid point-of-care STI diagnostic tests for self-testing among adolescent girls and young women. Diagnostics 2025, 15, 1604. [Google Scholar] [CrossRef]
- Touitou, R.; Bidet, P.; Dubois, C.; Partouche, H.; Bonacorsi, S.; Jung, C.; Cohen, R.; Levy, C.; Cohen, J.F. Diagnostic accuracy of a rapid nucleic acid test for group A streptococcal pharyngitis using saliva samples: Protocol for a multicenter study in primary care. Diagn. Progn. Res. 2023, 7, 13. [Google Scholar] [CrossRef]
- Kanwar, N.; Michael, J.; Doran, K.; Montgomery, E.; Selvarangan, R. Comparison of the ID Now Influenza A & B 2, Cobas Influenza A/B, and Xpert Xpress Flu Point-of-Care Nucleic Acid Amplification Tests for Influenza A/B Virus Detection in Children. J. Clin. Microbiol. 2020, 58, e01611–19. [Google Scholar] [PubMed]
- Bruijns, B.; Folkertsma, L.; Tiggelaar, R. FDA-authorized molecular point-of-care SARS-CoV-2 tests: A critical review on principles, systems, and clinical performances. Biosens. Bioelectron. X 2022, 11, 100158. [Google Scholar] [CrossRef] [PubMed]
- Jensen, C.B.; Schneider, U.V.; Madsen, T.V.; Nielsen, X.C.; Ma, C.M.G.; Severinsen, J.K.; Hoegh, A.M.; Botnen, A.B.; Trebbien, R.; Lisby, J.G. Evaluation of the analytical and clinical performance of two RT-PCR based point-of-care tests; Cepheid Xpert® Xpress CoV-2/Flu/RSV plus and SD BioSensor STANDARD™ M10 Flu/RSV/SARS-CoV-2. J. Clin. Virol. 2024, 172, 105674. [Google Scholar] [CrossRef] [PubMed]
- Shrivastava, A. Methods for the determination of limit of detection and limit of quantitation of analytical methods. Chron. Young Sci. 2011, 2, 21–25. [Google Scholar] [CrossRef]
- Laudus, N.; Nijs, L.; Nauwelaers, I.; Dequeker, E.M.C. The significance of external quality assessment schemes for molecular testing in clinical laboratories. Cancers 2022, 14, 3686. [Google Scholar] [CrossRef]
- Gruber, L.; Hausch, A.; Mueller, T. Internal quality controls in the medical laboratory: A narrative review of the basic principles of an appropriate quality control plan. Diagnostics 2024, 14, 2223. [Google Scholar] [CrossRef]
- Zhang, R.; Chiron, S.; Tyree, R.; Carson, K.; Raber, L.; Ramadass, K.; Gao, C.; Kim, M.E.; Zuo, L.; Li, Y.; et al. Enhancing clinical data management through barcode integration and REDCap: A scalable and adaptable implementation study. JMIR Form. Res. 2025, 9, e70016. [Google Scholar] [CrossRef]
- Khuluza, F.; Chiumia, F.K.; Nyirongo, H.M.; Kateka, C.; Hosea, R.A.; Mkwate, W. Temperature variations in pharmaceutical storage facilities and knowledge, attitudes, and practices of personnel on proper storage conditions for medicines in southern Malawi. Front. Public Health 2023, 11, 1209903. [Google Scholar] [CrossRef]
- Barbé, B.; Gillet, P.; Beelaert, G.; Fransen, K.; Jacobs, J. Assessment of desiccants and their instructions for use in rapid diagnostic tests. Malar. J. 2012, 11, 326. [Google Scholar] [CrossRef]
- Yoffe, A.; Liu, J.; Smith, G.; Chisholm, O. Regulatory reform outcomes and accelerated regulatory pathways for new prescription medicines in Australia. Ther. Innov. Regul. Sci. 2023, 57, 271–286. [Google Scholar] [CrossRef]
- Kardjadj, M. Regulatory approved point-of-care diagnostics (FDA & Health Canada): A comprehensive framework for analytical validity, clinical validity, and clinical utility in medical devices. J. Appl. Lab. Med. 2025, 10, 1622–1637. [Google Scholar] [PubMed]
- Padmore, R.; Petersen, K.; Campbell, C.; Chennette, M.; Sabourin, A.; Shaw, J. Practical application of mathematical calculations and statistical methods for the routine haematology laboratory. Int. J. Lab. Hematol. 2022, 44, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Cristelli, L.; Occhipinti, F.; Tumiatti, D.; Antonia, L.; Jani, E.; Daves, M. Implementation of new Westgard rules suggested by the Westgard Advisor software for five immunological parameters. Biochem. Med. 2025, 35, 010701. [Google Scholar] [CrossRef] [PubMed]
- Vierbaum, L.; Kaiser, P.; Spannagl, M.; Wenzel, F.; Thevis, M.; Schellenberg, I. Experiences and challenges for EQA providers in assessing the commutability of control materials in accuracy-based EQA programs. Front. Med. 2024, 11, 1416642. [Google Scholar] [CrossRef] [PubMed]
- Haliassos, A. Inter-Laboratory Comparisons and EQA in the Mediterranean Area. EJIFCC 2018, 29, 253–258. [Google Scholar]
- Gimah, M.; Eli, L.; Johnson, E. Towards seamless data integration: A comparative study of HL7, FHIR, and LOINC in SaaS laboratory systems. Preprint, 2024. [Google Scholar]
- Armbruster, D.; Miller, R.R. The Joint Committee for Traceability in Laboratory Medicine (JCTLM): A global approach to promote the standardisation of clinical laboratory test results. Clin. Biochem. Rev. 2007, 28, 105–113. [Google Scholar]
- NHS England; NHS Improvement. Point of Care Testing in Community Pharmacies: Guidance for Commissioners and Community Pharmacies Delivering NHS Services; NHS Publications: London, UK, 2022. [Google Scholar]
- Bundesärztekammer. Richtlinie der Bundesärztekammer zur Qualitätssicherung in medizinischen Laboratorien (Rili-BÄK); German Medical Association, 2021.
- Chakravarthy, S.N.; Ramanathan, S.; S.S.; Nallathambi, T.; S.M. EP15A3-based precision and trueness verification of the VITROS HbA1c immunoassay. Indian J. Clin. Biochem. 2019, 34, 89–94.
- Hutchings, L.; Shiamptanis, A. Evaluation of point-of-care testing in pharmacy to inform policy writing by the New Brunswick College of Pharmacists. Pharmacy 2022, 10, 159. [Google Scholar] [CrossRef]
- Tirimacco, R. Evolution of point-of-care testing in Australia. Clin. Biochem. Rev. 2010, 31, 75–80. [Google Scholar]
- Fujita, K.; Kushida, K.; Okada, H.; Moles, R.J.; Chen, T.F. Developing and testing quality indicators for pharmacist home-visit services: A mixed methods study in Japan. Br. J. Clin. Pharmacol. 2021, 87, 1940–1952. [Google Scholar] [CrossRef]
- Burnett, L.C.; Lunn, G.; Coico, R. Biosafety: Guidelines for working with pathogenic and infectious microorganisms. Curr. Protoc. Microbiol. 2009, 1, Unit 1A.1. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Liu, H.; Chen, W.; Ma, B.; Ju, H. Device integration of electrochemical biosensors. Nat. Rev. Bioeng. 2023, 1, 346–360. [Google Scholar] [CrossRef] [PubMed]
- Kumari, M.N.S.K.S.; Thankappan, S.X. Sensing the future—Frontiers in biosensors: Classifications, principles, and recent advances. ACS Omega 2024, 9, 48918–48987. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Qin, W.; Hou, Y.; Xiao, K.; Yan, W. The application of lateral flow immunoassay in point-of-care testing: A review. Nano Biomed. Eng. 2016, 8, 172–183. [Google Scholar] [CrossRef]
- Kılıç, E.; Şahin, E.A.; Tunçcan, Ö.G.; Yıldız, Ş.; Özkurt, Z.N.; Yeğin, Z.A.; Kalkancı, A. Comparative analysis of chemiluminescence immunoassay (CLIA)-based tests in diagnosing invasive aspergillosis in hematologic malignancies. Mycoses 2025, 68, e70064. [Google Scholar] [CrossRef]
- Srivastava, P.; Prasad, D. Isothermal nucleic acid amplification and its uses in modern diagnostic technologies. 3 Biotech 2023, 13, 200. [Google Scholar] [CrossRef]
- Ferreira, M.; Carvalho, V.; Ribeiro, J.; Lima, R.A.; Teixeira, S.; Pinho, D. Advances in microfluidic systems and numerical modeling in biomedical applications: A review. Micromachines 2024, 15, 873. [Google Scholar] [CrossRef]
- Berlanda, S.F.; Breitfeld, M.; Dietsche, C.L.; Dittrich, P.S. Recent advances in microfluidic technology for bioanalysis and diagnostics. Anal. Chem. 2021, 93, 311–331. [Google Scholar] [CrossRef]
- Zucca, P.; Fernandez-Lafuente, R.; Sanjust, E. Agarose and its derivatives as supports for enzyme immobilization. Molecules 2016, 21, 1577. [Google Scholar] [CrossRef]
- Goicoechea, H.C.; Collado, M.S.; Satuf, M.L.; Olivieri, A.C. Complementary use of partial least-squares and artificial neural networks for non-linear spectrophotometric analysis of pharmaceutical samples. Anal. Bioanal. Chem. 2002, 374, 460–465. [Google Scholar] [CrossRef]
- Macovei, D.-G.; Irimes, M.; Hosu, O.; Cristea, C.; Tertis, M. Point-of-care electrochemical testing of biomarkers involved in inflammatory and inflammation-associated medical conditions. Anal. Bioanal. Chem. 2023, 415, 1–25. [Google Scholar] [CrossRef]
- Alshorman, K.; Hussain, R. Community pharmacy-led point-of-care testing (POCT): Expanding roles and strengthening health systems in low- and middle-income countries. J. Pharm. Policy Pract. 2025, 18, 2578803. [Google Scholar] [CrossRef] [PubMed]
- Khatri, R.; Endalamaw, A.; Erku, D.; Wolka, E.; Nigatu, F.; Zewdie, A.; Assefa, Y. Continuity and care coordination of primary health care: A scoping review. BMC Health Serv. Res. 2023, 23, 750. [Google Scholar] [CrossRef] [PubMed]
- Bilka, M.; Duarte, A.; Lábaj, M. Entry and competition of retail pharmacies: A case study of OTC drugs sales and ownership deregulation. Ceska Slov. Farm. 2023, 72, 11–20. [Google Scholar] [PubMed]
- Serrano, L.P.; Maita, K.C.; Avila, F.R.; Torres-Guzman, R.A.; Garcia, J.P.; Eldaly, A.S.; Haider, C.R.; Felton, C.L.; Paulson, M.R.; Maniaci, M.J.; et al. Benefits and challenges of remote patient monitoring as perceived by health care practitioners: A systematic review. Perm. J. 2023, 27, 100–111. [Google Scholar] [CrossRef]
- Chakma, N.; Ali, S.B.; Islam, M.S.; Momtaz, T.; Farzana, N.; Amzad, R.; Khan, S.I.; Khan, M.I.H.; Azad, A.K.; Babar, Z.-U.-D.; et al. Exploration of challenges and opportunities for good pharmacy practices in Bangladesh: A qualitative study. Pharmacy 2025, 13, 26. [Google Scholar] [CrossRef]
- Clement, M. Challenges and opportunities in pharmacy-based test-and-treat models for infectious diseases: A framework for future implementation. Preprint 2019. [Google Scholar]
- Albasri, A.; Van den Bruel, A.; Hayward, G.; McManus, R.J.; Sheppard, J.P.; Verbakel, J.Y.J. Impact of point-of-care tests in community pharmacies: A systematic review and meta-analysis. BMJ Open 2020, 10, e034298. [Google Scholar] [CrossRef]
- Gallimore, C.E.; Porter, A.L.; Barnett, S.G.; Portillo, E.; Zorek, J.A. A state-level needs analysis of community pharmacy point-of-care testing. J. Am. Pharm. Assoc. 2021, 61, e93–e98. [Google Scholar] [CrossRef]
- Foster, K.; Despotis, G.; Scott, M. Point-of-care testing: Cost issues and impact on hospital operations. Clin. Lab. Med. 2001, 21, 269–284. [Google Scholar] [CrossRef]
- Nosanchuk, J.S.; Keefner, R. Cost analysis of point-of-care laboratory testing in a community hospital. Am. J. Clin. Pathol. 1995, 103, 240–243. [Google Scholar] [CrossRef]
- International Pharmaceutical Federation (FIP). Pharmacy-Based Point-of-Care Testing: A Global Intelligence Report. FIP Self-Care; The Hague, The Netherlands, 2023.
- Lingervelder, D.; Koffijberg, H.; Kusters, R.; IJzerman, M.J. Health economic evidence of point-of-care testing: A systematic review. Pharmacoecon. Open 2021, 5, 157–173. [Google Scholar] [CrossRef] [PubMed]
- St John, A.; Price, C.P. Economic evidence and point-of-care testing. Clin. Biochem. Rev. 2013, 34, 61–74. [Google Scholar] [PubMed]
- Alsetohy, W.; El-Fass, K.; Hadidi, S.; Zaitoun, M.F.; Badary, O.; Ali, K.; Ezz-Elden, A.; Ibrahim, M.; Makhlouf, B.; Hamdy, A.; et al. Economic impact and clinical benefits of clinical pharmacy interventions: A six-year multicenter study using an innovative medication management tool. PLoS ONE 2025, 20, e0311707. [Google Scholar] [CrossRef] [PubMed]
- Bindels, J.; Ramaekers, B.; Ramos, I.C.; Mohseninejad, L.; Knies, S.; Grutters, J.; Postma, M.; Al, M.; Feenstra, T.; Joore, M. Use of value-of-information in healthcare decision-making: Exploring multiple perspectives. Pharmacoeconomics 2016, 34, 315–322. [Google Scholar] [CrossRef]
- Chen, W.; Wong, N.C.B.; Wang, Y.; Zemlyanska, Y.; Butani, D.; Virabhak, S.; Matchar, D.B.; Prapinvanich, T.; Teerawattananon, Y. Mapping the value for money of precision medicine: A systematic literature review and meta-analysis. Front. Public Health 2023, 11, 1151504. [Google Scholar] [CrossRef]
- Pennello, G.; Pantoja-Galicia, N.; Evans, S. Comparing diagnostic tests on benefit-risk. J. Biopharm. Stat. 2016, 26, 1083–1097. [Google Scholar] [CrossRef]
- OECD. The Economics of Diagnostic Safety: Setting the Scene. OECD Publishing: Paris, France, 2024.
- Hirst, J.A.; McLellan, J.H.; Price, C.P.; English, E.; Feakins, B.G.; Stevens, R.J.; Farmer, A.J. Performance of point-of-care HbA1c test devices: Implications for use in clinical practice—a systematic review and meta-analysis. Clin. Chem. Lab. Med. 2017, 55, 167–180. [Google Scholar] [CrossRef]
- Lourdes, R.; Gayle, T.; Chong, Z.; Saminathan, T.; Abd Hamid, H.A.; Rifin, H.M.; Wan, K.S.; Majid, N.L.B.; Ratnam, K.; Riyadzi, M.R.; et al. Diagnostic accuracy of the CardioChek PA point-of-care testing analyser with a 3-in-1 lipid panel for epidemiological surveys. Lipids Health Dis. 2024, 23, 2702. [Google Scholar]
- Martínez-González, N.A.; Keizer, E.; Plate, A.; Coenen, S.; Valeri, F.; Verbakel, J.Y.J.; Rosemann, T.; Neuner-Jehle, S.; Senn, O. Point-of-care C-reactive protein testing to reduce antibiotic prescribing for respiratory tract infections in primary care: Systematic review and meta-analysis. Antibiotics 2020, 9, 610. [Google Scholar] [CrossRef]
- Ozucelik, Y.; Collins, J.; Pace, J. Identifying the educational needs of pharmacists engaging in professional development: A global systematic review. J. Am. Pharm. Assoc. 2025, 65, 102418. [Google Scholar] [CrossRef]
- Saeed, H.; Scahill, S.; Kim, J.; Moyaen, R.; Natarajan, D.; Soga, A.; Wong, M.; Martini, N. Pharmacist perceptions and future scope of telepharmacy in New Zealand: A qualitative exploration. Int. J. Telemed. Appl. 2024, 2024, 2667732. [Google Scholar] [CrossRef] [PubMed]
- Vanderbush, R.; Anderson, H.; Fant, W.; Fujisaki, B.; Malone, P.; Price, P.; Pruchnicki, M.; Sterling, T.; Weatherman, K.; Williams, K. Implementing pharmacy informatics in college curricula. Am. J. Pharm. Educ. 2007, 71, 117. [Google Scholar] [CrossRef] [PubMed]
- Kehrer, J.; James, D. The role of pharmacists and pharmacy education in point-of-care testing. Am. J. Pharm. Educ. 2016, 80, 129. [Google Scholar] [CrossRef] [PubMed]
- El-Tallawy, S.N.; Pergolizzi, J.V.; Vasiliu-Feltes, I.; Ahmed, R.S.; LeQuang, J.K.; Alzahrani, T.; Varrassi, G.; Awaleh, F.I.; Alsubaie, A.T.; Nagiub, M.S. Innovative applications of telemedicine and other digital health solutions in pain management: A literature review. Pain Ther. 2024, 13, 791–812. [Google Scholar] [CrossRef]
- Haleem, A.; Javaid, M.; Singh, R.; Suman, R. Medical 4.0 technologies for healthcare: Features, capabilities, and applications. Internet Things Cyber-Phys. Syst. 2022, 2, 100–120. [Google Scholar] [CrossRef]
- Sarasmita, M.A.; Sudarma, I.W.; Jaya, M.K.A.; Irham, L.M.; Susanty, S. Telepharmacy implementation to support pharmaceutical care services during the COVID-19 pandemic: A scoping review. Can. J. Hosp. Pharm. 2024, 77, e3430. [Google Scholar] [CrossRef]
- Apostolakis, A.; Barmpakos, D.; Mavrikou, S.; Papaioannou, G.M.; Tsekouras, V.; Hatziagapiou, K.; et al. System for classifying antibody concentration against SARS-CoV-2 S1 spike antigen with automatic QR code generation for integration with health passports. Explor. Digit. Health Technol. 2024, 2, 20–29. [Google Scholar] [CrossRef]
- Daoutakou, M.; Kintzios, S. Point-of-care testing (POCT) for cancer and chronic disease management in the workplace: Opportunities and challenges in the era of digital health passports. Appl. Sci. 2025, 15, 6906. [Google Scholar] [CrossRef]
- Abdellatife, O.E.; Makowsky, M.J. Factors influencing implementation of point-of-care testing for acute respiratory infectious diseases in community pharmacies: A scoping review using the CFIR framework. Res. Social Adm. Pharm. 2024, 20, 1–24. [Google Scholar] [CrossRef]
- Alsanosi, S.M.; Padmanabhan, S. Potential applications of artificial intelligence (AI) in managing polypharmacy in Saudi Arabia: A narrative review. Healthcare 2024, 12, 788. [Google Scholar] [CrossRef] [PubMed]
- Awala, E.; Olutimehin, D. Revolutionizing remote patient care: The role of machine learning and AI in enhancing telepharmacy services. World J. Adv. Res. Rev. 2024, 24, 1–15. [Google Scholar] [CrossRef]
- Flynn, C.D.; Chang, D. Artificial intelligence in point-of-care biosensing: Challenges and opportunities. Diagnostics 2024, 14, 1100. [Google Scholar] [CrossRef] [PubMed]
- Dou, B.; Zhu, Z.; Merkurjev, E.; Ke, L.; Chen, L.; Jiang, J.; Zhu, Y.; Liu, J.; Zhang, B.; Wei, G.W. Machine learning methods for small data challenges in molecular science. Chem. Rev. 2023, 123, 8736–8780. [Google Scholar] [CrossRef]
- Horta-Velázquez, A.; Arce, F.; Rodríguez-Sevilla, E.; Morales-Narváez, E. Toward smart diagnostics via AI-assisted surface-enhanced Raman spectroscopy. TrAC Trends Anal. Chem. 2023, 169, 117378. [Google Scholar] [CrossRef]
- Zhao, Q.; Zhang, C.; Zhang, W.; Zhang, S.; Liu, Q.; Guo, Y. Applications and challenges of biomarker-based predictive models in proactive health management. Front. Public Health 2025, 13, 1633487. [Google Scholar] [CrossRef]
- Hatem, N.A.H. Advancing pharmacy practice: The role of intelligence-driven pharmacy practice and the emergence of pharmacointelligence. Integr. Pharm. Res. Pract. 2024, 13, 139–153. [Google Scholar] [CrossRef]
- Thacharodi, A.; Singh, P.; Meenatchi, R.; Tawfeeq Ahmed, Z.H.; Kumar, R.R.S.; V. N.; Kavish, S.; Maqbool, M.; Hassan, S. Revolutionizing healthcare and medicine: The impact of modern technologies for a healthier future—A comprehensive review. Health Care Sci. 2024, 3, 329–349. [Google Scholar] [CrossRef]
- Olabiyi, W.; Clark, J.; Bliss, M. Predictive analytics for disease outbreaks: Using artificial intelligence to analyze patterns in health data for early detection of outbreaks. Preprint 2025. [Google Scholar]
- Hemingway, H.; Feder, G.S.; Fitzpatrick, N.K.; Denaxas, S.; Shah, A.D.; Timmis, A.D. Using nationwide ‘big data’ from linked electronic health records to help improve outcomes in cardiovascular disease: 33 studies from the CALIBER programme. Health Technol. Assess. 2017, 21, 1–200. [Google Scholar]
- Madathil, N.T.; Dankar, F.K.; Gergely, M.; Belkacem, A.N.; Alrabaee, S. Revolutionizing healthcare data analytics with federated learning: A comprehensive survey of applications, systems, and future directions. Comput. Struct. Biotechnol. J. 2025, 28, 217–238. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.; Joyce, S.; Schembri, R.; Swain, J.; Turiano, R.; Glass, B.D. Transforming care: Exploring consumer and pharmacist perceptions of expanded pharmacy practice in rural and remote communities. Pharmacy 2025, 13, 71. [Google Scholar] [CrossRef] [PubMed]
- Roberto, J. Challenges and opportunities of local pharmacies in Talavera, Nueva Ecija: A basis for an operational plan. Preprint 2025. [Google Scholar]
- Kroenert, A.C.; Bertsche, T. Implementation, barriers, solving strategies and future perspectives of reimbursed community pharmacy services: A nationwide survey in Germany. BMC Health Serv. Res. 2024, 24, 1463. [Google Scholar] [CrossRef]
- Luppa, P.B.; Müller, C.; Schlichtiger, A.; Schlebusch, H. Point-of-care testing (POCT): Current techniques and future perspectives. TrAC Trends Anal. Chem. 2011, 30, 887–898. [Google Scholar] [CrossRef]
- Zalupski, B.; Elroumi, Z.; Klepser, D.G.; Klepser, N.S.; Adams, A.J.; Klepser, M.E. Pharmacy-based CLIA-waived testing in the United States: Trends, impact, and the road ahead. Res. Social Adm. Pharm. 2024, 20, 146–151. [Google Scholar] [CrossRef]
- Dingwoke, J.; Onuzulike, I.; Egwu, K.; Duru, P.; Ezeanolue, C.; Onyekwere, F.; Agu, P.; Nweke, G.; Onyia, E.; Ajibo, O.; et al. Implementation of point-of-care testing in community pharmacies in Enugu State, Nigeria: A cross-sectional study. Pharm. Educ. 2025, 25, 422–433. [Google Scholar] [CrossRef]
- Ortblad, K.F.; Kuo, A.P.; Mogere, P.; Roche, S.D.; Kiptinness, C.; Wairimu, N.; Gakuo, S.; Baeten, J.M.; Ngure, K. Low selection of HIV PrEP refills at private pharmacies among clients who initiated PrEP at public clinics: A mixed-methods study in Kenya. BMC Health Serv. Res. 2024, 24, 618. [Google Scholar] [CrossRef]
- Ferreira, D.C.; Vieira, I.; Pedro, M.I.; Caldas, P.; Varela, M. Patient satisfaction with healthcare services and techniques used for its assessment: A systematic literature review and bibliometric analysis. Healthcare 2023, 11, 639. [Google Scholar] [CrossRef]
- Ojha, A.; Bista, D.; Kc, B. Patients’ perceptions on community pharmacy services in Kathmandu Metropolitan. Patient Prefer. Adherence 2023, 17, 1487–1499. [Google Scholar] [CrossRef]
- Dougherty, S.; Lorenzoni, L.; Marino, A.; Murtin, F. The impact of decentralization on the performance of healthcare systems: A nonlinear relationship. Eur. J. Health Econ. 2022, 23, 705–715. [Google Scholar] [CrossRef] [PubMed]
- McIsaac, M.; Buchan, J.; Abu-Agla, A.; et al. Global Strategy on Human Resources for Health: Workforce 2030—A Five-Year Check-In. Hum. Resour. Health 2022, 20, 94. [Google Scholar] [CrossRef]
Figure 1.
Key examples of analytical and biosensing POCTs applied in pharmacy sensing.
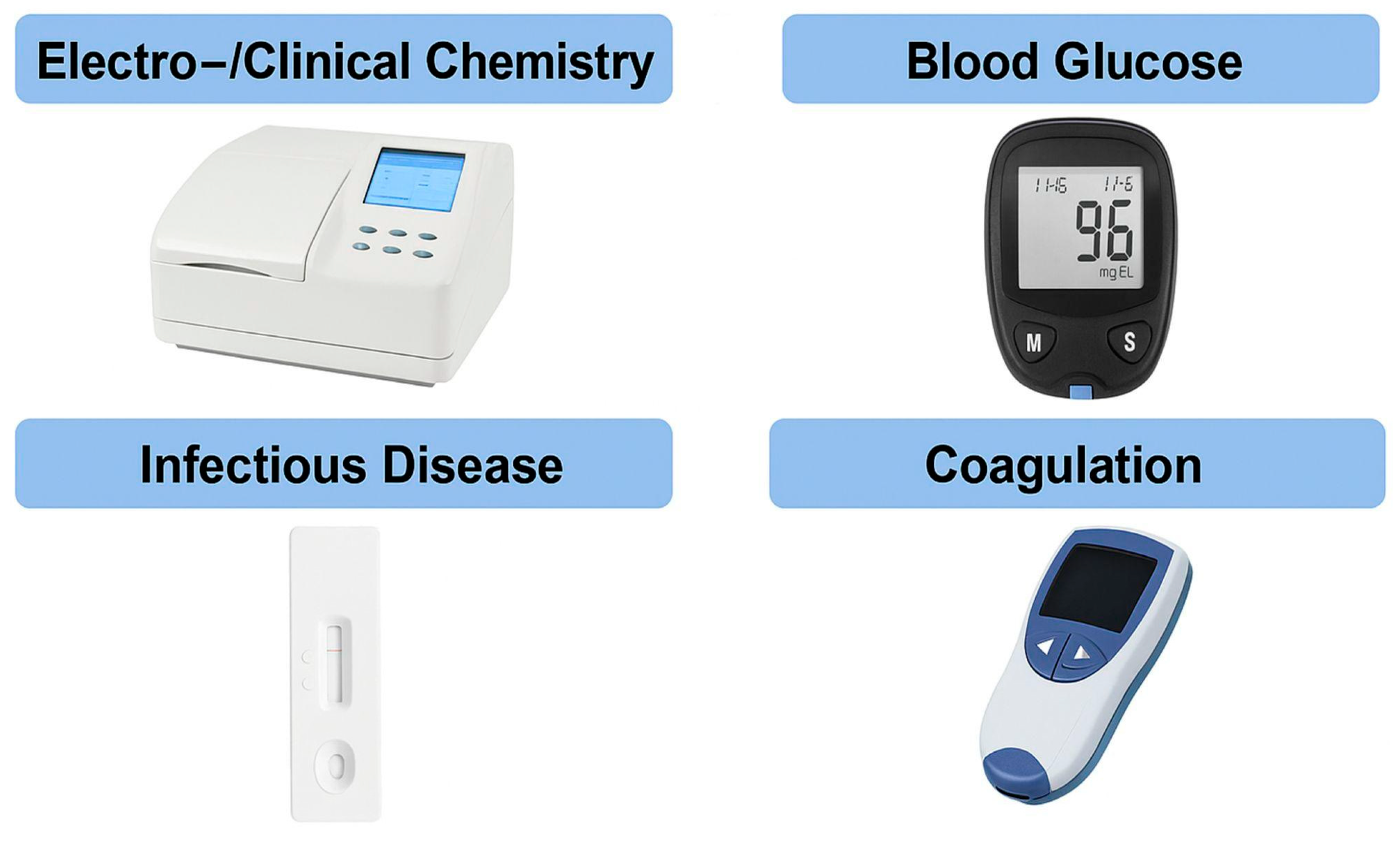
Figure 2.
Overview of different biosensor technologies used in pharmacy-based POCT.
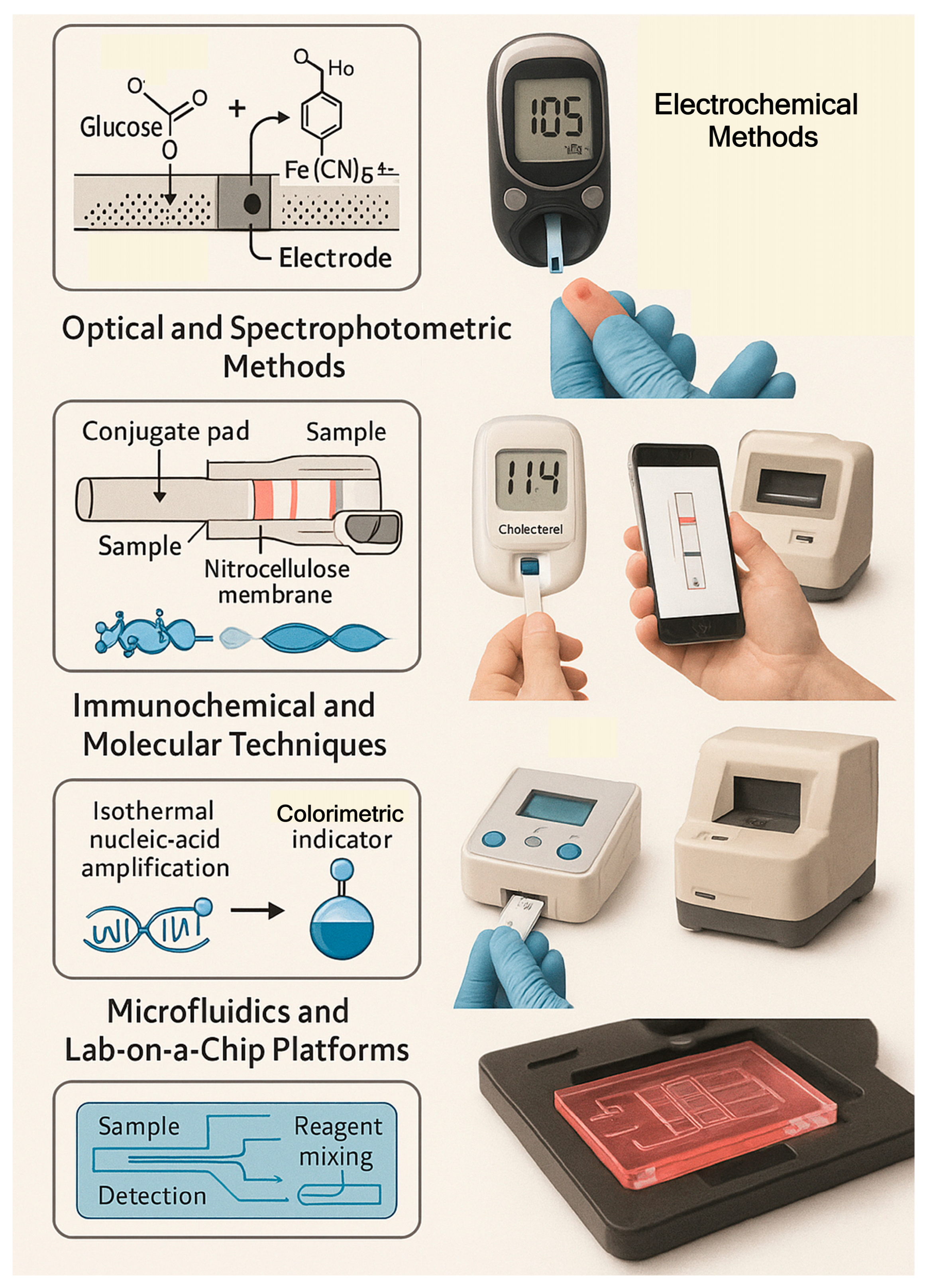
Figure 3.
Workflow of pharmacy-based POCT service delivery.
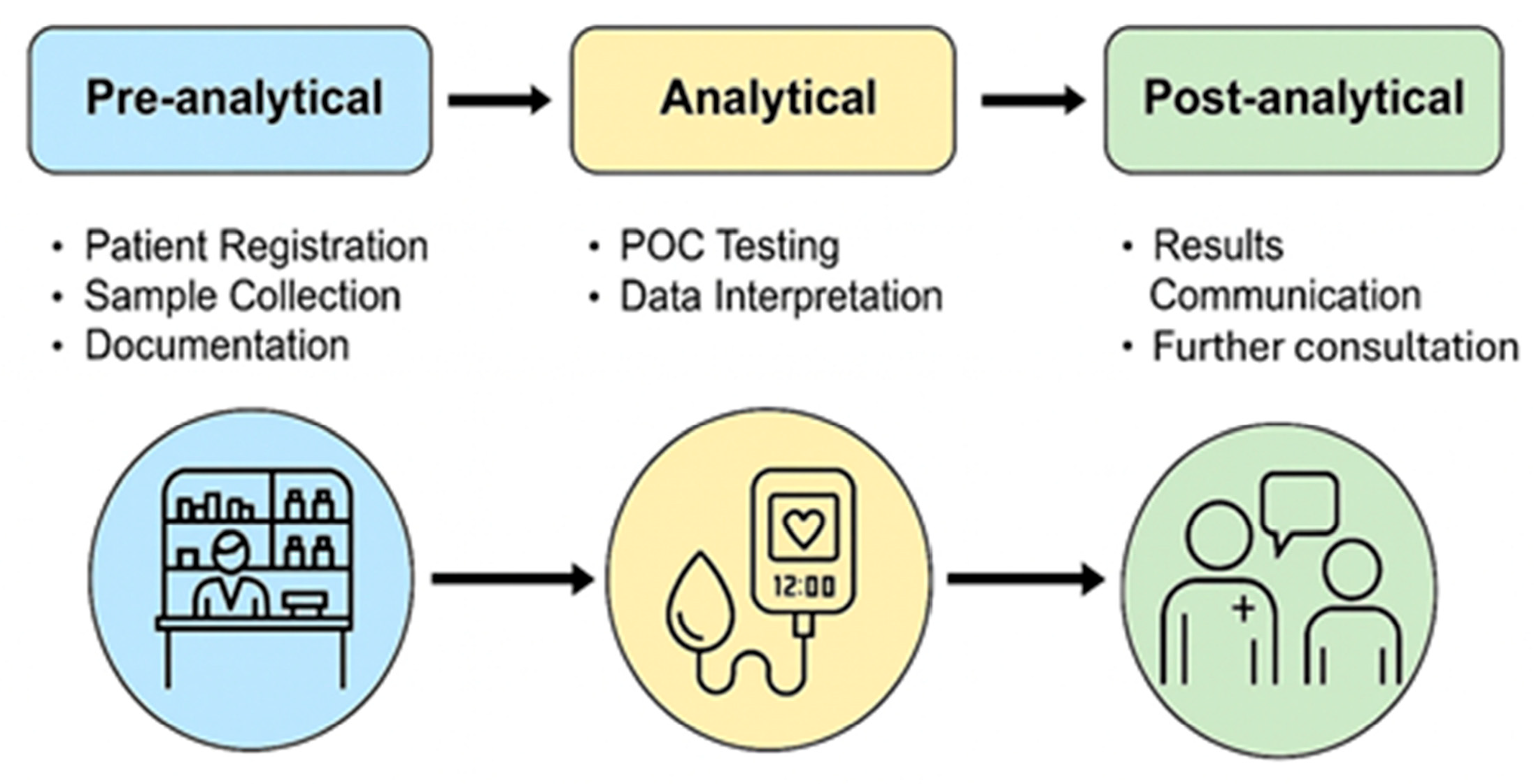
Figure 4.
Schematic representation of AI integration across the three analytical and clinical layers of pharmacy-based point-of-care testing POCT. At the signal-processing level, machine-learning models enhance raw electrochemical, optical and immunochemical signals by correcting for drift, matrix effects and non-linearities. At the result-interpretation level, AI-driven clinical decision-support systems combine biomarker values (e.g., HbA1c, CRP, lipid profile) with patient-specific factors and electronic health records to generate individualized risk estimates. At the population-learning level, aggregated POCT data contribute to network-wide surveillance, anomaly detection and continuous model improvement, transforming pharmacies into nodes of a learning diagnostic ecosystem.
Figure 4.
Schematic representation of AI integration across the three analytical and clinical layers of pharmacy-based point-of-care testing POCT. At the signal-processing level, machine-learning models enhance raw electrochemical, optical and immunochemical signals by correcting for drift, matrix effects and non-linearities. At the result-interpretation level, AI-driven clinical decision-support systems combine biomarker values (e.g., HbA1c, CRP, lipid profile) with patient-specific factors and electronic health records to generate individualized risk estimates. At the population-learning level, aggregated POCT data contribute to network-wide surveillance, anomaly detection and continuous model improvement, transforming pharmacies into nodes of a learning diagnostic ecosystem.
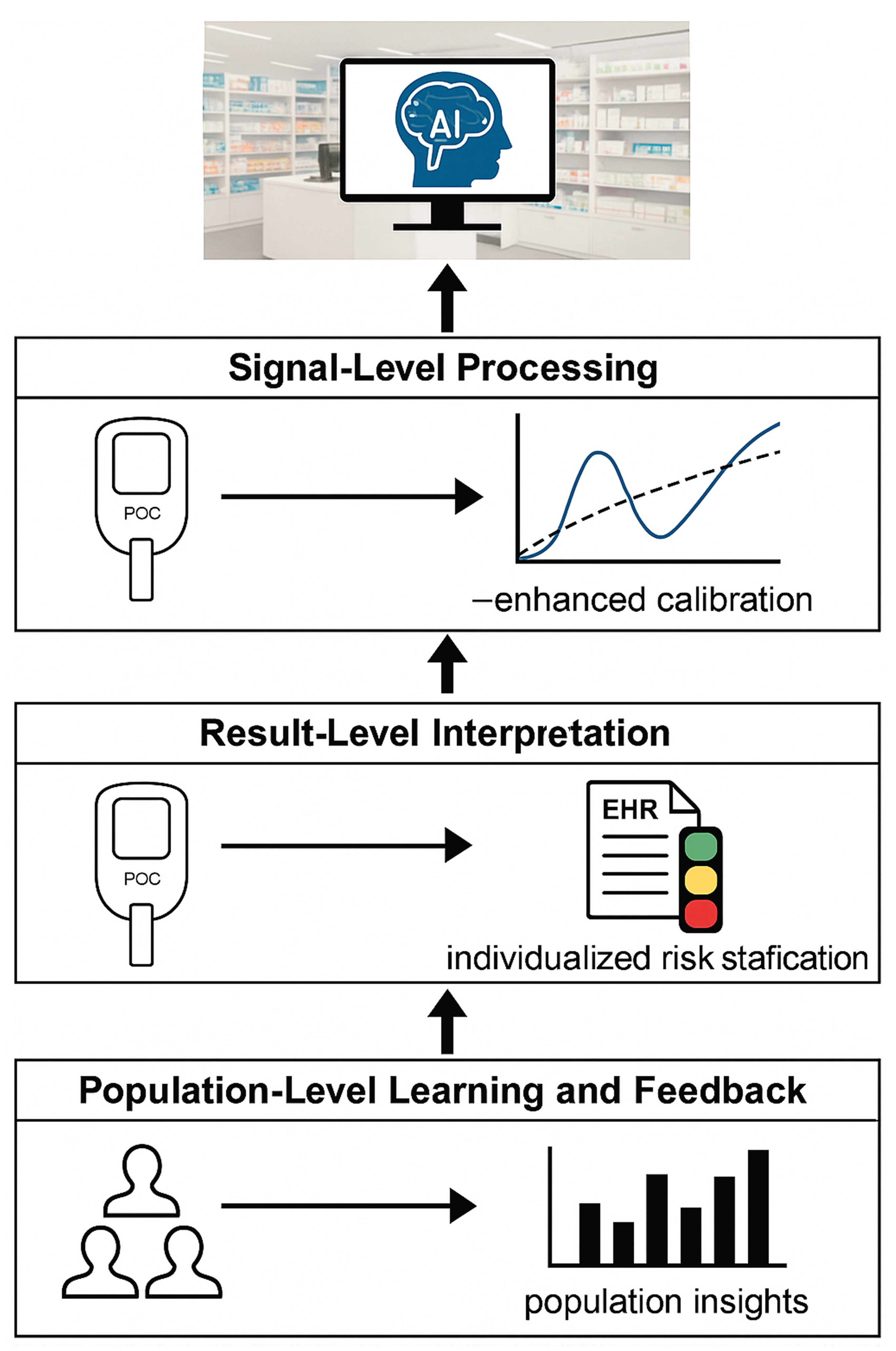
Table 2.
Anticipated key benefits and challenges of pharmacy-based POC services.
| Domain | Benefits | Challenges |
|---|---|---|
| Healthcare system | Reduced hospital burden; faster diagnosis | Variable reimbursement; policy gaps |
| Pharmacy sector | Diversified revenue; enhanced visibility | Infrastructure investment |
| Patients | Convenience; improved adherence | Perception of test reliability |
| Society | Better disease control; antimicrobial stewardship | Need for regulation and data protection |
Table 3.
Cost breakdown for adopting a POCT service at the pharmacy (estimates).
| Cost category | Cost (in €) |
|---|---|
| Equipment (read-out device) | 2000-6000 |
| Quality control | 300/year |
| Test reagents | 1-2/test |
| Software licence & update, IoT connectivity | 200/year |
Table 4.
Representative clinical trials assessing the impact of validated pharmacy-compatible POCT systems on primary health improvement.
Table 4.
Representative clinical trials assessing the impact of validated pharmacy-compatible POCT systems on primary health improvement.
| Analyte | Device Type | Analytical R² vs Laboratory | Clinical Outcome Improvement | Reference |
|---|---|---|---|---|
| HbA1c | Optical photometry | 0.97–0.99 | Same-visit HbA1c testing improved diabetes control; ~7–10% more patients reached target HbA1c | [83] |
| Total Cholesterol | Electrochemical | 0.95–0.98 | Immediate lipid results increased statin treatment adherence by ~10–15% | [84] |
| CRP | Lateral-flow immunoassay | 0.93–0.97 | Reduced unnecessary antibiotic prescribing in respiratory infections | [85] |
Table 5.
Core pharmacist competencies and implementation barriers for POC services.
| Category | Key Competencies | Common Barriers |
|---|---|---|
| Clinical interpretation | Result analysis, referral decisions | Lack of training, time constraints |
| Technical skills | Device operation, QC procedures | Cost of equipment, maintenance |
| Communication | Counseling, confidentiality | Space limitations, privacy issues |
| Management | Record keeping, workflow integration | Inconsistent reimbursement |
Table 6.
Summary of reimbursement and policy frameworks by region.
| Region | Reimbursement Mechanism | Policy Instruments | References |
|---|---|---|---|
| European Union | National health service contracts | Standardized accreditation, IVDR 2017/746 | [110] |
| North America | Insurance & Medicare billing codes | CLIA-waived classification; collaborative practice | [111] |
| Asia-Pacific | Mixed private/public schemes | Pharmacy-led screening programs, national POCT standards | [112] |
| Africa | NGO & donor support | Capacity-building projects, malaria/HIV POCT policies | [113] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



