Submitted:
24 November 2025
Posted:
25 November 2025
You are already at the latest version
Abstract
Objectives
Telerehabilitation has emerged as a crucial modality in light of recent global challenges such as the COVID-19 pandemic. We examined the effectiveness of a mobile health telerehabilitation intervention developed for older adults with frailty and conducted
an article search on this topic in the context of Japan.
Methods
Six participants received a nursing care telerehabilitation intervention (Rehab Studio) that included exercise training videos. The participants were aged ≥65 years, had no history of dementia or psychiatric disorders, and had mild-to-moderate care needs. For 1 month, the participants received 1-h live online rehabilitation sessions with real-time communication with rehabilitation specialists. The quality of life (QoL) (EuroQol 5 dimensions 5-level [EQ-5D-5L] and self-rated health scores were recorded before and after the intervention and analysed to determine whether the service was effective. Data were analysed using paired t-tests.
Results
Significant differences were found in the total EQ-5D-5L and self-rated health scores (p< 0.05). The mean EQ-5D-5L score increased from 0.63±0.13 before the intervention to 0.77±0.14 after the intervention (p=0.010), while the mean self-rated health score increased from 66.0±18.0 to 83.3±10.3, respectively (p=0.019).
Conclusions
The telerehabilitation intervention is safe and can improve the QoL. However, the effectiveness of the intervention needs to be further investigated in patients with poor performance in activities of daily living. Telerehabilitation could help reduce the burden of nursing care in ageing societies with declining birthrates.
Keywords:
frailty
; telerehabilitation
; telehealth
; quality of life
; mHealth
; aged
; exercise
1. Introduction
Following the COVID-19 pandemic, methods such as telerehabilitation have been studied in recent years as an alternative to traditional face-to-face rehabilitation. Telerehabilitation involves the use of communication devices such as smartphones, tablets, personal computers, and telerehabilitation resource guides to facilitate communication and exercise when caregivers and users are physically separated. This type of therapy was designed according to the recommendations of the physiotherapists.
Although there are obvious cost advantages to providing telerehabilitation, whether this method is as effective as traditional methods for improving both clinical and quality-of-life (QoL)-related outcomes needs to be examined. Japan is considered a 'super-aging society'; by 2025, 6.8 million baby boomers will be aged over 65 years, and the number of single-person households and baby boomers requiring care is expected to increase according to the reports from the Ministry of Health, Labour and Welfare. Elderly people in Japan generally have a strong desire to live independently, and it is likely that their future care needs will differ from those currently addressed by conventional nursing care services. According to a report published by the Ministry of Economy, Trade, and Industry in April 2018, by 2035, the number of people requiring nursing care will reach 10 million, and the gap between the supply and demand for nursing care personnel will grow to approximately 680,000 people in Japan. As a result, a substantial number of 'nursing care refugees' will be unable to access nursing care services. Given this context, it is crucial to construct social infrastructure that addresses the physical, cognitive, and emotional needs of the elderly and ensures that they are not socially isolated. Such infrastructure must also incorporate technologies that are currently not covered by Japan's long-term care insurance (LTCI) system. The LTCI system includes seven levels of care: two levels of supportive care and five levels of nursing care. An individual can receive nursing care services if their certification results fall under one of the seven levels.
Exercise instructions for older adults using mobile technology have been suggested to improve physical activity, and older adults who have received telecare interventions have been reported to experience improvements in their QoL. Although many general systematic and scope reviews of telerehabilitation have focused on elderly people, none have focused on the effectiveness of exercise-based mHealth or telerehabilitation for frail older adults. Therefore, in this study, we aimed to investigate the QoL-related outcomes of simultaneous telerehabilitation in multiple users and conduct a literature search of the current state of the research on telerehabilitation.
1.1. Development of Interventions
In response to the increased need for telerehabilitation, a nursing care rehabilitation technology company developed Rehab Studio, an exercise-based remote rehabilitation service that can be used by many frail elderly people simultaneously (Figure 1). Rehab Studio uses a customised version of an online web-conferencing system.
This service allows the type and timing of exercises to be adjusted according to the user's physical condition and preferences. The training videos can be viewed at any time and are selected by rehabilitation specialists according to the users' current goals and physical condition so that the users can exercise daily (Figure 2).
The training videos include several exercises such as upper and lower limb and trunk muscle strengthening exercises, stretching, sitting, and standing balance exercises. A short video of approximately 5 min consists of three different exercises, while a video of 15–20 min consists of approximately 10 different exercises. More than 100 training videos and more than 2,000 different exercises are available in this resource. Training videos can be selected according to different objectives such as 'fall prevention', 'improving activity levels', and 'dementia prevention'.
Eligible persons receive weekly telerehabilitation and may also use a separate day service or other LTCI services. The training videos have no time constraints, and daily exercise opportunities can be created by using them as independent training on days when telerehabilitation and LTCI services are not scheduled. The effectiveness of this intervention was analysed in this study.
1.2. Pilot Test of Rehab Studio
Prior to the current study, short-term pilot tests of the service were conducted (first: May 2020, second: August 2020, third: November–December 2020, fourth: February 2021, fifth: August–September 2022). Although the pilot sample sizes ranged from a few to over 100 people, testing allowed the intervention to be refined and improved. A care provider supplied the tablet terminals, online videos, and live viewing tools to frail elderly individuals and physical and occupational therapists directly conducted exercise programs for the participants. This system allowed the users to perform exercises while watching an exercise program. Physical and occupational therapists provided individual feedback to the users and communicated interactively online.
For the fifth pilot test, in August 2022, four frail elderly individuals (two men and two women) who used a daycare service were provided with online exercise instructions and communication opportunities for 1 month. These users were certified as requiring long-term care under Japan's LTCI system (two required long-term care level 1 and two required support level 2). Two of the four users expressed a desire to continue using the service even if they had to pay for it. They also shared the following comments about the service: 'The instruction was very detailed and informative', 'I feel more positive mentally', and 'It is good to be able to interact with other people without going outside'.
2. Methods
2.1. Evaluation of the Intervention
To determine the effectiveness of Rehab Studio, we selected 7 subjects. Inclusion criteria were: those attending day care with support levels 1 or 2, and care level 1; absence of dementia; ability to walk alone with a cane or walker; and agreement to participate within the study timeframe. Exclusion criteria included history of dementia or psychiatric disorders. Seven people agreed to participate, but one left due to ill health, resulting in six subjects who received 1-hour live online rehabilitation sessions with multiple participants. The participants engaged with the sessions in a sitting position with real-time communication with rehabilitation specialists, using Rehab Studio (Figure 3).
Rehab Studio has the following advantages: After participating in the exercise program, users can enter their satisfaction levels on a five-point scale, and physical and occupational therapists can check the results; the system is based on participant experiments and designed such that even elderly people who are not comfortable with technology can easily participate in the program; and this system has been tested for several years. In addition, the service is continually updated based on feedback (on pricing, exercise program design, and safety considerations) from users who participated in the intervention over the last several years (Table 1). Rehab Studio uses a customized version of the online web conferencing system, 'Whereby' (Norway), which is specifically designed to allow older adults to participate without the need for email addresses or passwords (Figure 4).
To assess the effectiveness and safety of the service, the EuroQol 5 dimensions 5-level (EQ-5D-5L) questionnaire was administered twice: before the intervention and 1 month after the intervention (Table 1). The EQ-5D-5L is a questionnaire with five items (walking, dressing, usual activities, pain/discomfort, and anxiety/blocked up) that are scored by the respondents on a five-point scale. We converted the responses obtained into a QoL score (maximum 1 point; minimum 0 points) using the conversion table of the Japanese version of the EQ-5D-5L.
3. Results
All six users exhibited improved EQ-5D-5L scores and self-rated health scores. The mean EQ-5D-5L score increased from 0.63±0.13 before the intervention to 0.77±0.14 after the intervention (p=0.010), while the mean self-rated health score increased from 66.0±18.0 to 83.3±10.3 (p=0.019). All statistical tests were two-sided. Data were analysed using paired t-tests. Significant differences were found in the total EQ-5D-5L and self-rated health scores (p<0.05). The significance level was set at p <0.05. Data were analysed using JMP pro ver18 (SAS Institute, Cary, NC, USA).
4. Discussion
4.1. Main Findings and Clinical Significance
In this pilot study, we found that a one-month multiuser exercise-based telerehabilitation intervention led to statistically significant improvements in both EQ-5D-5L scores and self-rated health scores among all six frail older adult participants. The mean EQ-5D-5L score increased from 0.63±0.13 to 0.77±0.14 (p=0.010), representing a 0.14-point improvement that exceeds the minimal clinically important difference (MCID) of 0.07-0.10 for the EQ-5D-5L in older populations [31,32]. The mean self-rated health score increased from 66.0±18.0 to 83.3±10.3 (p=0.019), indicating a 26% improvement in participants' subjective health perception. The EQ-5D-5L assesses five dimensions—mobility, self-care, usual activities, pain/discomfort, and anxiety/depression—capturing both physical and psychological components of health [33]. The improvements observed across these domains suggest that the intervention contributed to multidimensional well-being rather than isolated physical gains, which is particularly relevant for frail older adults whose health status is characterized by multisystem decline [34,35].
4.2. Social Engagement and Multiuser Format
The multiuser, group-based format represents a key distinguishing feature that may have contributed to the observed improvements. Social isolation has been identified as a significant risk factor for mortality and functional deterioration in older adults, with effect sizes comparable to established risk factors such as smoking [36,37]. In the context of frailty, social isolation can create a vicious cycle where physical limitations reduce opportunities for social engagement, which in turn accelerates functional decline [38,39]. The real-time video conferencing format employed in our study allowed participants to see and interact with both therapists and other participants, creating a virtual community. Research has demonstrated that group-based exercise interventions for frail older adults not only improve physical function but also enhance social networks and reduce depressive symptoms [40,41]. Our multiuser telerehabilitation format may disrupt the isolation-frailty cycle by providing both physical benefits through structured exercise and psychosocial benefits through shared online engagement.
4.3. Technological Accessibility
A critical success factor for telerehabilitation is technological accessibility for older adults, many of whom have limited digital literacy [42,43]. The Rehab Studio platform was specifically designed to address these barriers by eliminating the need for email addresses or passwords and providing pre-configured tablet devices that automatically connected to scheduled sessions. These design considerations align with principles of age-friendly technology design [44] and address usability barriers that have been identified as major obstacles to telehealth adoption among older adults [45,46].
4.4. Exercise and Frailty Management
The exercise component aligns with evidence that structured physical activity can prevent and potentially reverse frailty in older adults [47,48]. Frailty is increasingly recognized as a dynamic state that can be modified through appropriate interventions [49]. Multicomponent exercise programs addressing strength, balance, and endurance have emerged as effective interventions for frailty prevention and management [50,51]. Our platform incorporated all three components through a library of exercises covering strengthening, stretching, and balance activities, with personalization critical for the heterogeneous frail older adult population [52].
4.5. Healthcare Delivery Context
Telerehabilitation gained unprecedented attention during the COVID-19 pandemic [53,54], but its value extends beyond pandemic-related necessity. Many older adults face barriers to accessing traditional rehabilitation services, including transportation difficulties, geographical remoteness, and physical limitations [55]. The multiuser format leverages the scalability advantages of telehealth while maintaining social engagement benefits. This model is particularly relevant in Japan's healthcare system, which faces projected shortages of rehabilitation professionals due to population aging [56].
4.6. Study Limitations
This study has several important limitations. First, the small sample size (n=6) substantially limited statistical power and generalizability [57,58]. While we observed statistically significant improvements, these findings should be considered preliminary and hypothesis-generating. Second, the non-randomized design and absence of a control group limit causal inference [59,60]. Without a control group, we cannot definitively attribute improvements to the intervention rather than to placebo effects or temporal trends. Future studies should employ randomized controlled designs [61]. Third, the short intervention duration (one month) limited our ability to assess sustainability of benefits [62]. Long-term follow-up assessments are needed to evaluate durability of effects [63]. Fourth, reliance on self-reported measures introduces potential response bias [64]. Future studies should include objective measures such as gait speed, grip strength, or accelerometer-measured physical activity [65,66]. Fifth, we did not systematically assess intervention adherence, which is critical for understanding effectiveness [67]. Finally, our study was conducted in a single urban area in Japan with participants recruited from established day care services. Findings may not generalize to rural populations, other countries, or individuals not engaged with formal care services [68,69]. Cultural factors may influence both acceptability and effectiveness of telerehabilitation [70].
4.7. Future Research and Clinical Implications
Large-scale randomized controlled trials with adequate statistical power are needed to definitively establish effectiveness of multiuser exercise-based telerehabilitation for frail older adults [71,72]. These trials should include appropriate control groups and comprehensive outcome assessments including quality of life, physical function, cognitive function, and healthcare utilization [73]. Research should also examine dose-response relationships to identify optimal intervention parameters [74], investigate subpopulation differences [75], and assess cost-effectiveness [76,77]. Despite limitations, this pilot study provides preliminary evidence supporting feasibility, safety, and potential efficacy of multiuser exercise-based telerehabilitation for frail older adults. The positive outcomes add to evidence supporting policy reforms to expand insurance coverage for telerehabilitation services [78,79]. The multiuser format offers a scalable model that could help address workforce shortages and improve access to rehabilitation services [80].

Table 2.
Overview of the literature search.
| Study | Country | Subject No. | older adult, frail/ other | telehealth/ mHealth | multiuser/ group | QOL outcome |
|---|---|---|---|---|---|---|
| Tsai et al., 20177 | Australia | 36 | yes, with COPD | Yes | Yes | Yes |
| Bernocchi et al., 201821 | Italy | 112 | yes, with heart failure and COPD | Yes | No | Yes |
| Lin et al., 201414 | Taiwan | 43 | yes, stroke | Yes | Yes | not evident |
| Kwan et al., 202016 | China | 99 | yes, cognitive frailty | Yes | Yes | not evident |
| Murukesu et al., 202122 | Malaysia | 42 | yes, cognitive frailty | No | Yes | Yes |
| Oursler et al., 202215 | USA | 80 | yes, with HIV | Yes | Yes | Yes |
| Daniel, 201223 | USA | 23 | yes, prefrail | No | Yes | not evident |
| Cabrita et al., 201724 | the Netherlands | 10 | yes (not frail-specific, but frailty assessed) | Yes | Yes | Yes |
| Zengin Alpozgen et al., 202217 | Turkey | 30 | yes (not frail-specific, with no other conditions specified) | Yes | No | Yes |
| Geraedts et al., 202125 | the Netherlands | 40 | yes, prefrail | Yes | Yes | not evident |
| Dekker-van Weering et al., 201726 | the Netherlands | 37 | yes, prefrail | Yes | Yes | Yes |
| Li et al., 202027 | USA | 8 | yes, cognitively intact | Yes | Yes | not evident |
| Osuka et al., 202228 | Japan | 58 | yes, frail | Partly | Yes | Yes |
| Tekin, 202229 | Turkey | 255 | Yes | Yes | No | Yes |
| Tosi et al., 202130 | Brazil | 43 | yes, frail | Partly | No | not evident |
COPD: chronic obstructive pulmonary disease, QOL: quality of life.
5. Conclusions
This pilot study provides preliminary evidence that a one-month multiuser exercise-based telerehabilitation intervention can improve quality of life in frail older adults. All six participants showed improvements in EQ-5D-5L and self-rated health scores, and the intervention was safe with no reported adverse events. However, the small sample size, absence of a control group, short intervention duration, and reliance on self-reported outcomes limit conclusions regarding causality and generalizability. Multiuser telerehabilitation could help address challenges such as limited healthcare resources, workforce shortages, and increased demand for rehabilitation services in aging societies. By enabling healthcare providers and older adults to collaborate in virtual spaces, these technologies have potential to improve health outcomes, enhance access to care, reduce isolation, and provide continuous support. With continued research, refinement, and policy support, multiuser exercise-based telerehabilitation may become an important component of comprehensive care for frail older adults, complementing traditional in-person services and helping older adults maintain independence, function, and quality of life as they age. New telemedicine, telerehabilitation, and mHealth technologies for elderly people can improve their QoL. Multiuser telerehabilitation could address problems such as limited healthcare resources and increased demand for rehabilitation services. By allowing healthcare providers, caregivers, and older adults to collaborate in real or virtual spaces, these new technologies can improve health outcomes and provide continuous support to users.
Author Contributions
NY and IS conceptualised this study. NY, AM, ST, and TN conducted the literature review. IS was involved in protocol development, gaining ethical approval, patient recruitment, and data analysis. RO and TN were responsible for data analysis. NY wrote the first draft of the manuscript. All authors were involved in the study design and research questions. All authors reviewed and edited the manuscript and approved the final version.
Funding
This work was supported by the Japan Society for the Promotion of Science JSPS, KAKENHI [grant number JP19K20018].
Institutional Review Board Statement
The Ethics Committee of Eisei Hospital approved this study (approval number E-2023-04).
Informed Consent Statement
We have obtained written informed consent to participate and for publication from all participants.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the Japan medical association Database Of clinical MEdicine (J-DOME).
Conflicts of Interest
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
- Cordeiro ALL, da Silva Miranda A, de Almeida HM, et al. Quality of life in patients with heart failure assisted by telerehabilitation: A systematic review and meta-analysis. Int J Telerehabil 2022, 14, e6456. [Google Scholar] [CrossRef]
- Arian M, Valinejadi A, Soleimani M. Quality of life in heart patients receiving telerehabilitation: An overview with meta-analyses. Iran J Public Health 2022, 51, 2388–2403. [Google Scholar] [CrossRef]
- Giovannini S, Coraci D, Loreti C, et al. Prehabilitation and heart failure: main outcomes in the COVID-19 era. Eur Rev Med Pharmacol Sci 2022, 26, 4131–4139. [Google Scholar] [CrossRef]
- Koike A, Sobue Y, Kawai M, et al. Safety and feasibility of a telemonitoring-guided exercise program in patients receiving cardiac resynchronization therapy. Ann Noninvasive Electrocardiol 2022, 27, e12926. [Google Scholar] [CrossRef]
- Piotrowicz E, Mierzyńska A, Jaworska I, et al. Relationship between physical capacity and depression in heart failure patients undergoing hybrid comprehensive telerehabilitation vs. usual care: Subanalysis from the TELEREH-HF Randomized Clinical Trial. Eur J Cardiovasc Nurs 2022, 21, 568–577. [Google Scholar] [CrossRef]
- Skov Schacksen C, Dyrvig AK, Henneberg NC, et al. Patient-reported outcomes from patients with heart failure participating in the future patient telerehabilitation program: Data from the intervention arm of a randomized controlled trial. JMIR Cardio 2021, 5, e26544. [Google Scholar] [CrossRef] [PubMed]
- Tsai LL, McNamara RJ, Moddel C, et al. Home-based telerehabilitation via real-time videoconferencing improves endurance exercise capacity in patients with COPD: The randomized controlled TeleR Study. Respirology 2017, 22, 699–707. [Google Scholar] [CrossRef]
- Velayati F, Ayatollahi H, Hemmat M. A systematic review of the effectiveness of telerehabilitation interventions for therapeutic purposes in the elderly. Methods Inf Med 2020, 59, 104–109. [Google Scholar] [CrossRef]
- Saare M, Hussain, A, Seng Yue W. Investigating the effectiveness of mobile peer support to enhance the quality of life of older adults: a systematic literature review. Int J Interact Mob Technol 2019, 13, 130–139. [Google Scholar] [CrossRef]
- Aslam AS, van Leunen S, Aslam S, et al. A systematic review on the use of mHealth to increase physical activity in older people. Clinical eHealth 2020, 3, 31–39. [Google Scholar] [CrossRef]
- Tam ACY, Chan AWY, Cheung DSK, et al. The effects of interventions to enhance cognitive and physical functions in older people with cognitive frailty: a systematic review and meta-analysis. Eur Rev Aging Phys Act 2022, 19, 19. [Google Scholar] [CrossRef] [PubMed]
- Md Fadzil NH, Shahar S, Rajikan R, et al. A scoping review for usage of telerehabilitation among older adults with mild cognitive impairment or cognitive frailty. Int J Environ Res Public Health 2022, 19, 4000. [Google Scholar] [CrossRef]
- Linn N, Goetzinger C, Regnaux JP, et al. Digital health interventions among people living with frailty: a scoping review. J Am Med Dir Assoc 2021, 22, 1802–1812.e21. [Google Scholar] [CrossRef]
- Lin KH, Chen CH, Chen YY, et al. Bidirectional and multi-user telerehabilitation system: clinical effect on balance, functional activity, and satisfaction in patients with chronic stroke living in long-term care facilities. Sensors 2014, 14, 12451–12466. [Google Scholar] [CrossRef]
- Oursler KK, Marconi VC, Briggs BC, et al. Telehealth exercise intervention in older adults with HIV: protocol of a multisite randomized trial. J Assoc Nurses AIDS Care 2022, 33, 168–177. [Google Scholar] [CrossRef]
- Kwan RY, Lee D, Lee PH, et al. Effects of an mHealth brisk walking intervention on increasing physical activity in older people with cognitive frailty: pilot randomized controlled trial. JMIR Mhealth Uhealth 2020, 8, e16596. [Google Scholar] [CrossRef]
- Zengin Alpozgen A, Kardes K, Acikbas E, et al. The effectiveness of synchronous tele-exercise to maintain the physical fitness, quality of life, and mood of older people - A randomized and controlled study. Eur Geriatr Med 2022, 13, 1177–1185. [Google Scholar] [CrossRef]
- Van der Vorst A, Zijlstra GAR, De Witte N, et al. Explaining discrepancies in self-reported quality of life in frail older people: a mixed-methods study. BMC Geriatr 2017, 17, 251. [Google Scholar] [CrossRef]
- Rizzoli R, Reginster JY, Arnal JF, et al. Quality of life in sarcopenia and frailty. Calcif Tissue Int 2013, 93, 101–120. [Google Scholar] [CrossRef]
- Baraković S, Baraković Husić J, van Hoof J, et al. Quality of life framework for personalised ageing: a systematic review of ICT solutions. Int J Environ Res Public Health 2020, 17, 2940. [Google Scholar] [CrossRef]
- Bernocchi P, Vitacca M, La Rovere MT, et al. Home-based telerehabilitation in older patients with chronic obstructive pulmonary disease and heart failure: a randomised controlled trial. Age Ageing 2018, 47, 82–88. [Google Scholar] [CrossRef]
- Murukesu RR, Singh DKA, Shahar S, et al. Physical activity patterns, psychosocial well-being and coping strategies among older persons with cognitive frailty of the "WE-RISE" trial throughout the COVID-19 movement control order. Clin Interv Aging 2021, 16, 415–429. [Google Scholar] [CrossRef] [PubMed]
- Daniel, K. Wii-hab for pre-frail older adults. Rehabil Nurs 2012, 37, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Cabrita M, Lousberg R, Tabak M, et al. An exploratory study on the impact of daily activities on the pleasure and physical activity of older adults. Eur Rev Aging Phys Act 2017, 14, 1. [Google Scholar] [CrossRef] [PubMed]
- Geraedts HAE, Dijkstra H, Zhang W, et al. Effectiveness of an individually tailored home-based exercise programme for pre-frail older adults, driven by a tablet application and mobility monitoring: A pilot study. Eur Rev Aging Phys Act 2021, 18, 10. [Google Scholar] [CrossRef]
- Dekker-van Weering M, Jansen-Kosterink S, Frazer S, et al. User experience, actual use, and effectiveness of an information communication technology-supported home exercise program for pre-frail older adults. Front Med (Lausanne) 2017, 4, 208. [Google Scholar] [CrossRef]
- Li J, Hodgson N, Lyons MM, et al. A personalized behavioral intervention implementing mHealth technologies for older adults: a pilot feasibility study. Geriatr Nurs 2020, 41, 313–319. [Google Scholar] [CrossRef]
- Osuka Y, Sasai H, Kojima N, et al. Adherence, safety and potential effectiveness of a home-based Radio-Taiso exercise program in older adults with frailty: a pilot randomized controlled trial. Geriatr Gerontol Int 2023, 23, 32–37. [Google Scholar] [CrossRef]
- Tekin F, Nilufer CK. Effectiveness of a telerehabilitative home exercise program on elder adults' physical performance, depression and fear of falling. Percept Mot Skills 2022, 129, 714–730. [Google Scholar] [CrossRef]
- Tosi FC, Lin SM, Gomes GC, et al. A multidimensional program including standing exercises, health education, and telephone support to reduce sedentary behavior in frail older adults: Randomized clinical trial. Exp Gerontol 2021, 153, 111472. [Google Scholar] [CrossRef]
- Walters SJ, Brazier JE. Comparison of the minimally important difference for two health state utility measures: EQ-5D and SF-6D. Qual Life Res 2005, 14, 1523–1532.
- Pickard AS, Neary MP, Cella D. Estimation of minimally important differences in EQ-5D utility and VAS scores in cancer. Health Qual Life Outcomes 2007, 5, 70. [Google Scholar] [CrossRef] [PubMed]
- Janssen MF, Pickard AS, Golicki D, et al. Measurement properties of the EQ-5D-5L compared to the EQ-5D-3L across eight patient groups: a multi-country study. Qual Life Res 2013, 22, 1717–1727. [Google Scholar] [CrossRef]
- Clegg A, Young J, Iliffe S, et al. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef]
- Dent E, Morley JE, Cruz-Jentoft AJ, et al. Physical frailty: ICFSR international clinical practice guidelines for identification and management. J Nutr Health Aging 2019, 23, 771–787. [Google Scholar] [CrossRef]
- Holt-Lunstad J, Smith TB, Baker M, et al. Loneliness and social isolation as risk factors for mortality: a meta-analytic review. Perspect Psychol Sci 2015, 10, 227–237. [Google Scholar] [CrossRef] [PubMed]
- Steptoe A, Shankar A, Demakakos P, et al. Social isolation, loneliness, and all-cause mortality in older men and women. Proc Natl Acad Sci USA 2013, 110, 5797–5801. [Google Scholar] [CrossRef] [PubMed]
- Gale CR, Westbury L, Cooper C. Social isolation and loneliness as risk factors for the progression of frailty: the English Longitudinal Study of Ageing. Age Ageing 2018, 47, 392–397. [Google Scholar] [CrossRef]
- Hoogendijk EO, Suanet B, Dent E, et al. Adverse effects of frailty on social functioning in older adults: results from the Longitudinal Aging Study Amsterdam. Maturitas 2016, 83, 45–50. [Google Scholar] [CrossRef]
- Coll-Planas L, Nyqvist F, Puig T, et al. Social capital interventions targeting older people and their impact on health: a systematic review. J Epidemiol Community Health 2017, 71, 663–672. [Google Scholar] [CrossRef]
- Czaja SJ, Boot WR, Charness N, et al. Improving social support for older adults through technology: findings from the PRISM randomized controlled trial. Gerontologist 2018, 58, 467–477. [Google Scholar] [CrossRef]
- Choi NG, Dinitto DM. The digital divide among low-income homebound older adults: internet use patterns, eHealth literacy, and attitudes toward computer/internet use. J Med Internet Res 2013, 15, e93. [Google Scholar] [CrossRef]
- Nymberg VM, Bolmsjö BB, Wolff M, et al. 'Having to learn this so late in our lives...' Swedish elderly patients' beliefs, experiences, attitudes and expectations of e-health in primary health care. Scand J Prim Health Care 2019, 37, 41–52. [Google Scholar] [CrossRef]
- Wildenbos GA, Peute L, Jaspers M. Aging barriers influencing mobile health usability for older adults: a literature based framework (MOLD-US). Int J Med Inform 2018, 114, 66–75. [Google Scholar] [CrossRef] [PubMed]
- Kruse C, Fohn J, Wilson N, et al. Utilization barriers and medical outcomes commensurate with the use of telehealth among older adults: systematic review. JMIR Med Inform 2020, 8, e20359. [Google Scholar] [CrossRef] [PubMed]
- van Houwelingen CT, Ettema RG, Antonietti MG, et al. Understanding older people's readiness for receiving telehealth: mixed-method study. J Med Internet Res 2018, 20, e123. [Google Scholar] [CrossRef]
- de Labra C, Guimaraes-Pinheiro C, Maseda A, et al. Effects of physical exercise interventions in frail older adults: a systematic review of randomized controlled trials. BMC Geriatr 2015, 15, 154. [Google Scholar]
- Apóstolo J, Cooke R, Bobrowicz-Campos E, et al. Effectiveness of interventions to prevent pre-frailty and frailty progression in older adults: a systematic review. JBI Database System Rev Implement Rep 2018, 16, 140–232. [Google Scholar] [CrossRef]
- Puts MTE, Toubasi S, Andrew MK, et al. Interventions to prevent or reduce the level of frailty in community-dwelling older adults: a scoping review of the literature and international policies. Age Ageing 2017, 46, 383–392. [Google Scholar]
- Cruz-Jentoft AJ, Bahat G, Bauer J, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Sherrington C, Michaleff ZA, Fairhall N, et al. Exercise to prevent falls in older adults: an updated systematic review and meta-analysis. Br J Sports Med 2017, 51, 1750–1758. [Google Scholar] [CrossRef]
- Cesari M, Vellas B, Hsu FC, et al. A physical activity intervention to treat the frailty syndrome in older persons—results from the LIFE-P study. J Gerontol A Biol Sci Med Sci 2015, 70, 216–222. [Google Scholar] [CrossRef]
- Hollander JE, Carr BG. Virtually perfect? Telemedicine for COVID-19. N Engl J Med 2020, 382, 1679–1681.
- Smith AC, Thomas E, Snoswell CL, et al. Telehealth for global emergencies: implications for coronavirus disease 2019 (COVID-19). J Telemed Telecare 2020, 26, 309–313. [Google Scholar] [CrossRef] [PubMed]
- Ahmed T, Vafaei A, Belanger E, et al. Trajectories of limitations in activities of daily living among older adults in the International Mobility in Aging Study: persistence, recovery, and mortality. Age Ageing 2021, 50, 939–945. [Google Scholar]
- Ministry of Health, Labour and Welfare. Annual health, labour and welfare report 2019-2020. Tokyo: Ministry of Health, Labour and Welfare, 2020.
- Button KS, Ioannidis JP, Mokrysz C, et al. Power failure: why small sample size undermines the reliability of neuroscience. Nat Rev Neurosci 2013, 14, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Faber J, Fonseca LM. How sample size influences research outcomes. Dental Press J Orthod 2014, 19, 27–29. [Google Scholar] [CrossRef]
- Schulz KF, Altman DG, Moher D. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c332.
- Moher D, Hopewell S, Schulz KF, et al. CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c869. [Google Scholar] [CrossRef]
- Eldridge SM, Chan CL, Campbell MJ, et al. CONSORT 2010 statement: extension to randomised pilot and feasibility trials. BMJ 2016, 355, i5239. [Google Scholar] [CrossRef]
- Simek EM, McPhate L, Haines TP. Adherence to and efficacy of home exercise programs to prevent falls: a systematic review and meta-analysis of the impact of exercise program characteristics. Prev Med 2012, 55, 262–275. [Google Scholar] [CrossRef]
- Dishman RK, Buckworth J. Increasing physical activity: a quantitative synthesis. Med Sci Sports Exerc 1996, 28, 706–719. [Google Scholar] [CrossRef] [PubMed]
- McCambridge J, Witton J, Elbourne DR. Systematic review of the Hawthorne effect: new concepts are needed to study research participation effects. J Clin Epidemiol 2014, 67, 267–277. [Google Scholar] [CrossRef]
- Guralnik JM, Simonsick EM, Ferrucci L, et al. A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. J Gerontol 1994, 49, M85–M94. [Google Scholar] [CrossRef] [PubMed]
- Bohannon RW, Wang YC, Gershon RC. Two-minute walk test performance by adults 18 to 85 years: normative values, reliability, and responsiveness. Arch Phys Med Rehabil 2015, 96, 472–477. [Google Scholar] [CrossRef]
- Essery R, Geraghty AW, Kirby S, et al. Predictors of adherence to home-based physical therapies: a systematic review. Disabil Rehabil 2017, 39, 519–534. [Google Scholar] [CrossRef] [PubMed]
- Bashshur RL, Shannon GW, Smith BR, et al. The empirical foundations of telemedicine interventions for chronic disease management. Telemed J E Health 2014, 20, 769–800. [Google Scholar] [CrossRef]
- Kruse CS, Krowski N, Rodriguez B, et al. Telehealth and patient satisfaction: a systematic review and narrative analysis. BMJ Open 2017, 7, e016242. [Google Scholar] [CrossRef]
- Greenhalgh T, Wherton J, Papoutsi C, et al. Beyond adoption: a new framework for theorizing and evaluating nonadoption, abandonment, and challenges to the scale-up, spread, and sustainability of health and care technologies. J Med Internet Res 2017, 19, e367. [Google Scholar] [CrossRef]
- Campbell MK, Piaggio G, Elbourne DR, et al. Consort 2010 statement: extension to cluster randomised trials. BMJ 2012, 345, e5661. [Google Scholar] [CrossRef]
- Zwarenstein M, Treweek S, Gagnier JJ, et al. Improving the reporting of pragmatic trials: an extension of the CONSORT statement. BMJ 2008, 337, a2390. [Google Scholar] [CrossRef]
- Chan AW, Tetzlaff JM, Altman DG, et al. SPIRIT 2013 statement: defining standard protocol items for clinical trials. Ann Intern Med 2013, 158, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Nelson ME, Rejeski WJ, Blair SN, et al. Physical activity and public health in older adults: recommendation from the American College of Sports Medicine and the American Heart Association. Med Sci Sports Exerc 2007, 39, 1435–1445. [Google Scholar] [CrossRef] [PubMed]
- Inouye SK, Studenski S, Tinetti ME, et al. Geriatric syndromes: clinical, research, and policy implications of a core geriatric concept. J Am Geriatr Soc 2007, 55, 780–791. [Google Scholar] [CrossRef]
- Drummond MF, Sculpher MJ, Claxton K, et al. Methods for the economic evaluation of health care programmes. 4th ed. Oxford: Oxford University Press, 2015.
- Husereau D, Drummond M, Petrou S, et al. Consolidated Health Economic Evaluation Reporting Standards (CHEERS) statement. BMJ 2013, 346, f1049. [Google Scholar] [CrossRef]
- Tamiya N, Noguchi H, Nishi A, et al. Population ageing and wellbeing: lessons from Japan's long-term care insurance policy. Lancet 2011, 378, 1183–1192. [Google Scholar] [CrossRef] [PubMed]
- Mitchell UA, Chebli PG, Ruggiero L, et al. The digital divide in health-related technology use: the significance of race/ethnicity. Gerontologist 2019, 59, 6–14. [Google Scholar] [CrossRef]
- Cottrell MA, Galea OA, O'Leary SP, et al. Real-time telerehabilitation for the treatment of musculoskeletal conditions is effective and comparable to standard practice: a systematic review and meta-analysis. Clin Rehabil 2017, 31, 625–638. [Google Scholar] [CrossRef]
Figure 1.
Overview of the telerehabilitation service provision.
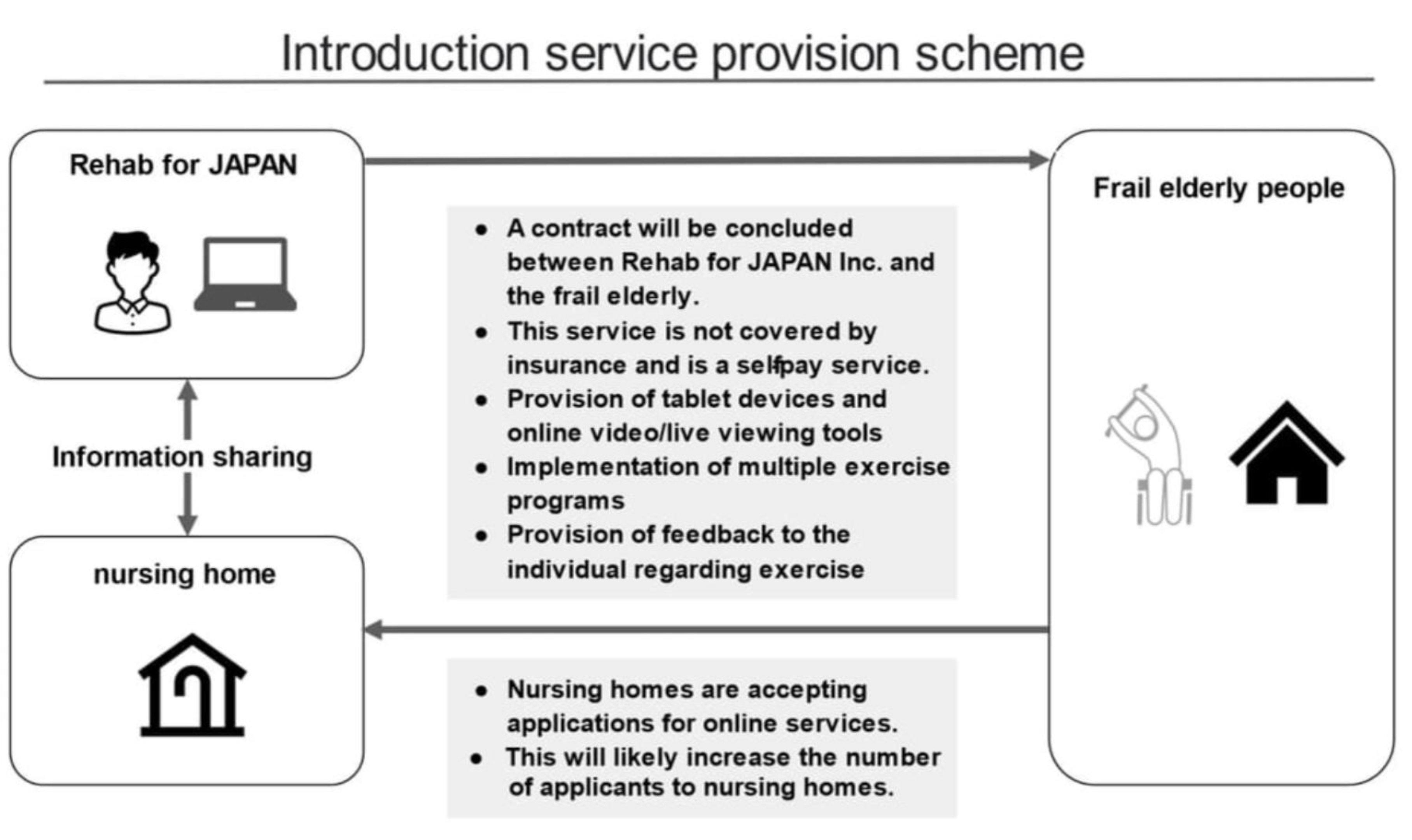
Figure 2.
Home implementation of the telerehabilitation intervention.
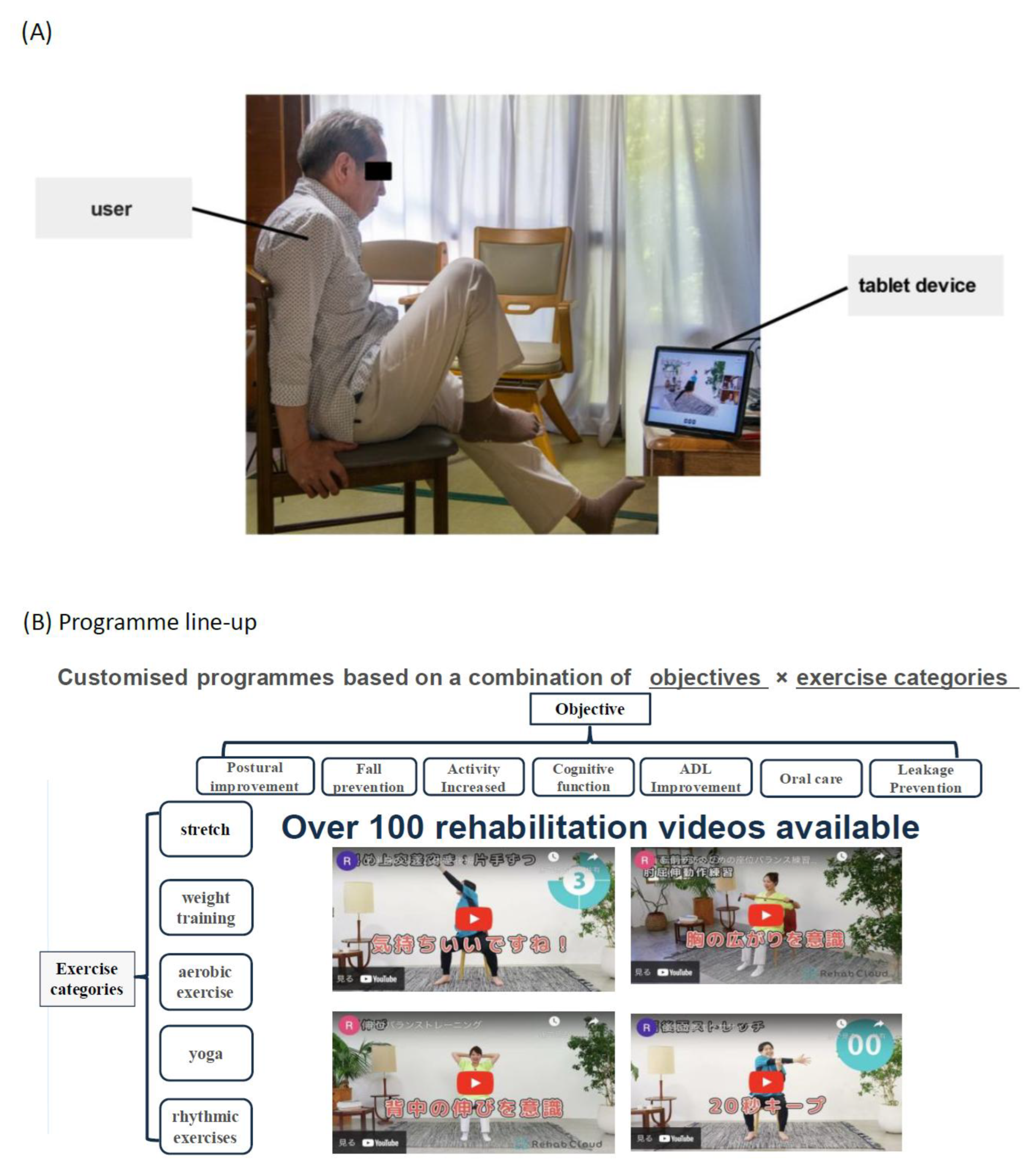
Figure 3.
Presentation of the telerehabilitation intervention.
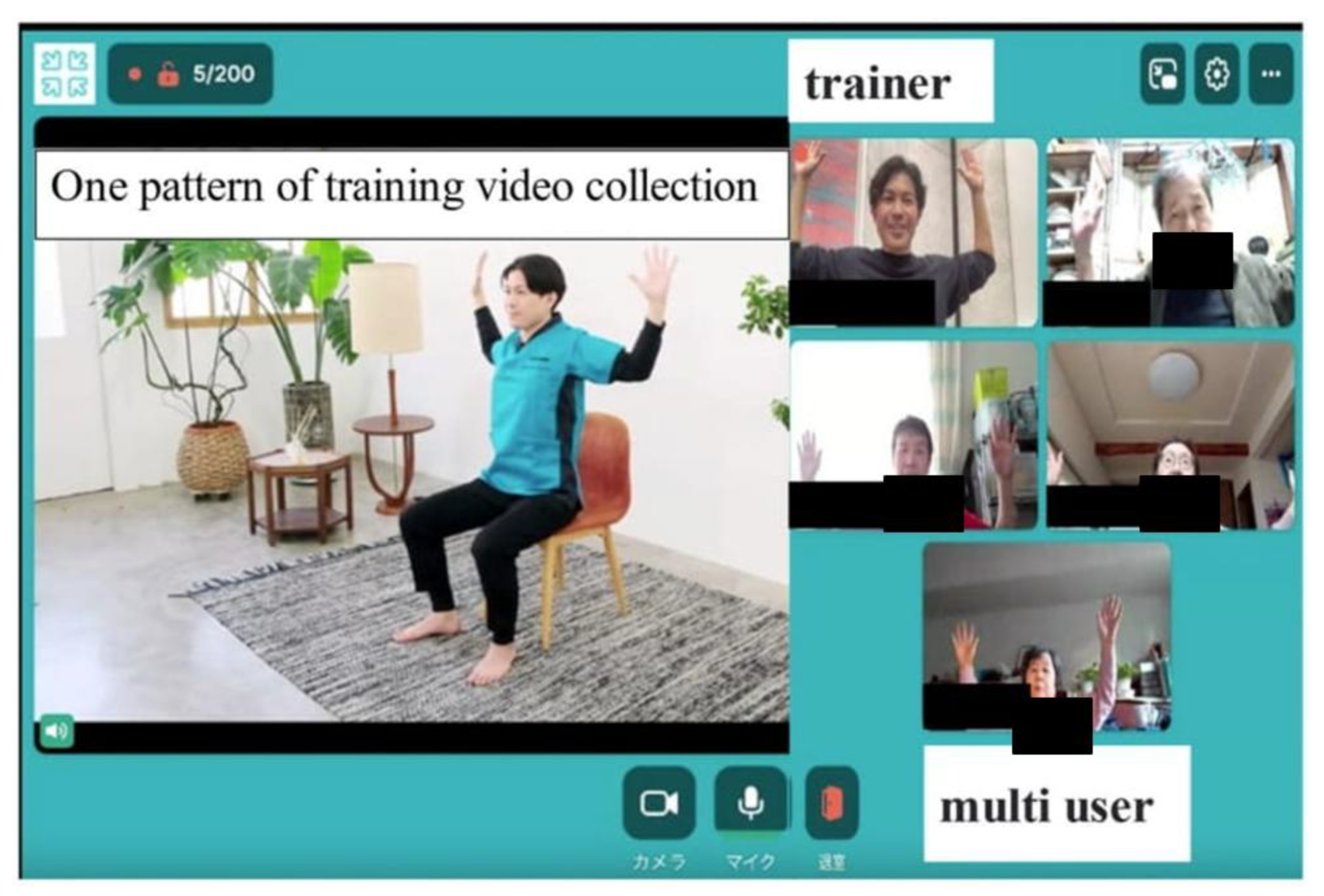
Figure 4.
Dedicated tablet device configured for ease of use with online web conferencing system: 'Whereby' (Norway).
Figure 4.
Dedicated tablet device configured for ease of use with online web conferencing system: 'Whereby' (Norway).

Table 1.
EQ-5D-5L scores before and 1 month after the start of the intervention for frail elderly patients (N=6).
Table 1.
EQ-5D-5L scores before and 1 month after the start of the intervention for frail elderly patients (N=6).
| No | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|
| Age | 67 | 82 | 80 | 80 | 82 | 81 |
| Sex | Male | Female | Female | Female | Female | Female |
| Disease name | OPLL, LDH | Hip osteoarthritis | LDH, DM | SAH | LCS, Lumbar Kyphosis | Lumbar compression fracture |
| Nursing care certification | Needs level 2 support | Needs level 2 support | Needs level 2 support | Needs level 1 support | Needs level 2 support | Needs level 2 support |
| EQ-5D-5L score pre-intervention | 0.55 | 0.76 | 0.52 | 0.48 | 0.82 | 0.66 |
| EQ-5D-5L score post-intervention | 0.60 | 0.78 | 0.73 | 0.61 | 1.00 | 0.88 |
EQ-5D-5L: EuroQol 5 dimensions 5-level quality of life scale OPLL: ossification of the posterior longitudinal ligament LDH: lumbar disc herniation DM: diabetes mellitus SAH: subarachnoid haemorrhage LCS: lumbar spinal canal stenosis.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



