Submitted:
19 November 2025
Posted:
21 November 2025
You are already at the latest version
Abstract
In Côte d’Ivoire, parent-child communication (PCC) about sexual and reproductive health (SRH) is often hindered by cultural and social norms. We aimed to explore pa-rental communication on sexual and reproductive health in the Haut-Sassandra re-gion, Côte d’Ivoire. We used an interpretive description approach. Participants were parents (mothers and fathers), recruited through purposive sampling. Data were col-lected through individual interviews. We performed a thematic analysis. Overall, 63 parents participated in the study. The mean age of parents was 41.2. Sexuality remains a taboo subject. Sociocultural factors that hinder PCC are tradition, the need for inter-generational respect, and the fear of incitement. Reasons that explain the gap between intention and actual practice are the young age of the child, low parental self-efficacy, child gender, shame and intergenerational respect. Parents who communicate address the following topics: relationships (e.g. stay away from boys); values, rights, culture and sexuality (e.g. don’t date someone else's husband); skills for health and well-being (e.g. sex has advantages and disadvantages); the human body and development (e.g. menstruation management); sexuality and sexual behaviour (e.g. practice abstinence); and sexual and reproductive health (e.g. protect oneself against disease). This study highlights the need to support parents in their educational role.
Keywords:
parent-child communication
; adolescents
; young adults
; sexual health
; reproductive health
; sex education
; sexuality
1. Introduction
In families, communication shapes parent-child relationships and supports children’s psychosocial development [1,2]. As children grow, their evolving needs require parents to adapt both the content and approach of their interactions, taking into account factors such as age, gender, and comprehension abilities [3]. Effective communication demands specific parental skills [1] and contributes to healthier socio-relational outcomes [4]. This is particularly crucial in the domain of sexual and reproductive health (SRH), where open and appropriate communication supports adolescents’ well-being [5], informs their sexual decision making [6], and promotes responsible, informed attitudes toward sexuality [7]. Evidence indicates that parent-child communication (PCC) on SRH plays a protective role and is associated with safer sexual behaviours among youth [5,7].
In Africa, PCC about SRH varies considerably and can sometimes be hindered by cultural and social norms. Barriers to open and constructive dialogue include parents’ lack of knowledge, skills and preparation [8,9], the discomfort in talking about sexual matters [9], and the fear of promoting behaviours deemed inappropriate [10] make it difficult for parents to broach these subjects. Also, cultural and traditional norms [8,11], religious norms [12] and taboos surrounding sexuality [8] further restrict communication. When sexuality is seen as a taboo, it limits discussion, narrows the scope of topics addressed, and prevents young people from accessing essential information [13]. In Côte d’Ivoire, PCC about sexual health is often limited by shame, concern about societal disapproval, and beliefs that youth are either too immature or will be encouraged to engage in sex [12,14].
Despite all the obstacles, PCC about sexual health occurs in some Ivorian families, though it often takes the form of threats and warnings [8,15,16]. Discussions may also be authoritarian, hostile and unidirectional [8,16,17], with a harsh and ambiguous tone of communication that does not encourage dialogue [16]. Furthermore, discussions may be characterised by inconsistent information and exaggeration of the consequences of sex [16,17] and thus, linked to poor outcomes [17]. Adolescents and young adults face multiple vulnerabilities related to SRH, including rising rates of school-based pregnancies [18,19,20], sexually transmitted infections, sexual violence, and limited understanding of consent [21,22]. These challenges are compounded by restrictive sociocultural norms and practices such as rigid gender roles and limited access to appropriate services [23,24,25]. Thus, we aimed to explore parental communication on SRH in the Haut-Sassandra region in Côte d’Ivoire.
This study is part of the Projet d’Appui à des Services de Santé Adaptés au Genre et Équitables (PASSAGE) implemented by a consortium of Ivorian and Canadian partners in the Haut-Sassandra region of the Côte d’Ivoire.
2. Methods
Study design and setting
This study adopts a qualitative research design using an interpretive description approach [26,27], which is well-suited to examining complex, context-dependent phenomena such as parental communication about SRH. The aim was to generate practical insights into the content and dynamics of PCC, in order to identify the types of support that could strengthen parents’ roles in SRH education.
Data were collected in three areas of the Haut-Sassandra region of Côte d’Ivoire: Daloa (main city of the region), Bonoufla (semi-urban locality) and Gonaté (rural area).
Study population
Study participants were parents (mothers and fathers). To be included, individuals had to meet the following criteria: 1) have at least one adolescent or young adult child (aged 10–24 years); 2) be in regular contact with their child or children, which may include cohabitation or frequent interactions (e.g., daily or weekly communication); 3) reside in one of the study’s selected localities (urban, semi-urban, or rural); and 4) be available and willing to participate in the study.
Recruitment and data collection
Recruitment and data collection have been previously reported [14]. We used a purposive sampling method with convenience and snowball sampling to recruit the participants in the study [28].
Data were collected through individual interviews, using an interview guide. Parents were asked if: 1) they think parents should communicate with their children about SRH; and 2) they communicate with their children about SRH. If so, what specifically do they tell them? If not, what justifies this? In addition, they were asked: 3) whether they feel comfortable communicating with their children about sexuality; 4) whether they have any need for support on this subject and 5) whether they had any other relevant information.
All participants read or received information about the research project, the research objectives, and the conditions of participation from the interviewer. They then signed an information and consent form, and answered a few sociodemographic questions and the questions presented above. No financial compensation was provided for participation in the study.
The interviews took place at the participants’ homes and lasted up to 30 minutes. The individual interviews were recorded with the participants’ permission.
Our approach was grounded in practical field saturation, seeking diverse and meaningful insights from parents across geographical contexts.
The recruitment and data collection took place between September 1 and October 31, 2023.
Data analysis
We reported this study using the consolidated criteria for reporting qualitative research (COREQ), a 32-item checklist for interviews and focus groups [29].
Data analysis was conducted by MMN, LGK and TTA under the supervision of MJD. We acknowledge LGK’s contribution as an Ivorian analyst with deep insight into the social context and local terminologies. To facilitate coding and thematic organization, we structured the data in tables using Word and Excel.
We guided the analysis process according to the interpretive description approach adopted for this study. This approach allowed us not only to identify patterns in the data but also to generate contextually grounded interpretations relevant to the lived experiences of participants. We transcribed all interview audio recordings verbatim and conducted a thematic analysis of the transcripts. Codes were generated inductively from the data and grouped into broader themes that reflected recurring ideas, social dynamics, and culturally embedded meanings.
Interpretation was guided by iterative thematic analysis and team-based reflection, integrating both local and external perspectives. We did not conduct member checking.
To categorize the messages communicated by parents, we used the International Technical Guidance on Sexuality Education developed by UNESCO. This framework proposes eight key concepts to guide the development of sexual education programs for children, adolescents, and young adults aged 5 to 18 and older. These concepts that are Relationships; Values, Rights, Culture and Sexuality; Understanding Gender; Violence and Staying Safe; Skills for Health and Well-being; The Human Body and Development; Sexuality and Sexual Behaviour; and Sexual and Reproductive Health, served as an analytical lens to classify and interpret the content of parental messages [30].
Ethical considerations
The project was approved by the Comité National d’Éthique des Sciences de la Vie et de la Santé in Côte d’Ivoire (N/Réf: 114-23/MSHPCMU/CNESVS-km) and by the Research Ethics Committee of the CHU de Québec-Université Laval in Canada (Project 2024-7017).
3. Results
This section presents the characteristics of the participants and the main results.
3.1. Characteristics of Participants
Overall, 63 parents (31 mothers and 32 fathers) participated in the study. The mean age of parents was 41.2. In each locality, 21 parents took part in the study: 11 fathers and 10 mothers in Daloa, 11 fathers and 10 mothers in Bonoufla, and 10 fathers and 11 mothers in Gonaté.
3.2. Main Results
This section, presents the different dimensions of parental communication about sexuality, highlighting the perceptions, practices, and needs expressed.
Figure 1 summarizes participants’ answers to the various questions.
3.2.1. Sexuality: Still a Taboo Subject
According to participants, sexuality remains a largely taboo subject in the Haut-Sassandra region of Côte d’Ivoire. While most parents acknowledge the importance of discussing SRH with their children, they point to several sociocultural factors that hinder open dialogue and reinforce the taboo. These include deeply rooted traditions, the need to uphold intergenerational respect, and the fear that such conversations might be seen as encouraging early sexual activity.
For some parents, sexuality is simply not considered an appropriate topic for discussion with children. One mother expressed this sentiment clearly: “... you see that well, it’s not a conversation to have with a child, maybe with my generation, but with children... it doesn’t show respect. That’s how it is with us.” (Mother, Participant #13).
Other parents, while more open to the idea of communication, remain ambivalent. A father explained the dilemma many face: “... but when you talk to children about this, it’s as if you’re telling them to do it. Often parents are right too, because when you talk to them about it, it’s like you’re giving them the opportunity to do it, and that’s what scares parents, which is why they don’t talk about it, I think...” (Father, participant #46).
Despite these concerns, many parents recognize the negative consequences of avoiding the topic. The lack of guidance at home often leads children to seek information elsewhere, particularly from peers or the streets, which can result in misinformation and risky behaviours. As one mother lamented:
“Yes, of course, that’s true, especially here in Africa. It’s very difficult to talk about this. Parents don’t sit down to talk about it; it’s a taboo subject, so... it’s the street that teaches them [children]. it’s the street that does everything, so that leads them to do stupid things.” Mother, participant #7
3.2.2. Communication: Recognized as Important, Yet Often Absent
Although most parents interviewed recognize the importance of discussing SRH with their children, many do not engage in such conversations, or do so only partially. Participants identified several reasons that explain this gap between intention and practice (see Figure 1).
Child’s Age as a Barrier
Some parents refrain from discussing sexuality because they consider their children too young. Three parents explicitly stated that they had not yet initiated conversations due to age. Others reported communicating only with their older children, postponing discussions with younger ones until they reach what is perceived as an appropriate age. One father explained that he was waiting until his daughter reached adulthood before addressing sexual health precautions.
“Well, the two who are at home, because the youngest is now 13, I haven’t talked to her much yet, but I talk to the boys [who are older].” Mother, participant #14
Low Parental Self-Efficacy
Another barrier is low self-efficacy. Some parents feel unprepared or lack the necessary knowledge to engage in SRH discussions. One father expressed a willingness to break the taboo but admitted he did not know how to begin:
“Well, right now, I don’t know if I can find anyone to teach me about this, but it would be helpful because I don’t know where to start... I need training. I need someone to teach me how to approach and explain things to children so that I can understand better.” Father, participant #48
Gender Norms and Role Division
Several fathers reported avoiding SRH conversations with their daughters, believing that such discussions should be handled by mothers.
“Personally, I can’t talk to my daughter about sexual health... I don’t think that’s right... Normally, it’s the woman who should talk to her daughters… We, men, can advise boys... I am Senufo, and in our culture, we don’t approve of that.” Father, Participant #45
Shame and Discomfort
Shame also emerged as a significant barrier, particularly among fathers communicating with daughters. Four fathers expressed embarrassment when discussing sexuality with their daughters. One father, whose two daughters became pregnant while in school, admitted that he still felt uncomfortable addressing the topic, fearing a loss of respect and also because the damage has already been done. Another participant highlighted the general discomfort parents feel when approaching sensitive subjects:
“No, because it’s a bit awkward, and parents avoid sensitive words.” Parent – Father – participant #50
Despite these barriers, many parents do communicate with their children about SRH. For some, especially mothers, this communication is viewed as essential. One mother reflected on how the absence of dialogue in her own upbringing left her vulnerable. She explained that, in the absence of parental guidance, she engaged in relationships with men as a means of coping with financial hardship and securing material support. Today, she takes on a mentoring role with teens and young women in her community, determined to help them avoid the same mistakes and navigate adolescence with greater awareness.
“I feel comfortable myself when there are girls around or we see that, I call them because my parents didn’t do that, so I made a commitment to myself not to let it become difficult.” Parent – Mother – participant #12
3.2.3. Parents’ Message About Sexuality
Table 1 presents the content of parents’ messages broken down by UNESCO themes and sub-themes. We found messages on 6 topics. Each parent gives an average of two to three of the messages presented in the table. A parent covers on average one or two themes. The themes most frequently addressed by parents are theme 7 on Sexuality and Sexual Behaviour followed by theme 8 on SRH.
Theme 1: Relationships
In this theme, the messages were related to the sub-theme “Friendship, Love, and Romantic Relationships.” They focused on avoiding relationships or controlling partner choices. There was no content related to the sub-themes “Families,” “Tolerance, Inclusion and Respect,” and “Long-term Commitments and Parenting.”
Theme 2: Values, Rights, Culture, and Sexuality
In this theme, the messages were related to the sub-theme “Values and Sexuality.” All messages are formulated negatively and in the form of prohibitions. There was no content related to the sub-themes “Human Rights and Sexuality” or “Culture, Society and Sexuality.”
Theme 3: Understanding Gender
There were no messages related to this theme and its sub-themes.
Theme 4: Violence and Staying Safe
There were no messages related to this theme and its sub-themes.
Theme 5: Skills for Health and Well-being
In this theme, the messages were related to two sub-themes: “Decision-making” and “Finding Help and Support.” For the first sub-theme, the messages provided some knowledge about the benefits and consequences of the decision to have sex. For the second sub-theme, only one source of support was mentioned. No messages addressed “Norms and Peer Influence on Sexual Behaviour,” “Communication, Refusal, and Negotiation Skills,” or “Media Literacy and Sexuality.”
Figure 1.
Parental typology and barriers to communication about SRH with adolescents and young adults. Analysis of the findings reveals three distinct categories of parental attitudes toward SRH: parents who oppose such discussions, parents who are ambivalent, and parents who consider communication important. The first group typically justifies their reluctance by citing cultural traditions and the imperative to maintain intergenerational respect. The second group expresses concern that discussing these topics may encourage early sexual activity among youth. While the third group acknowledges the importance of engaging in dialogue with their children, not all members communicate systematically. Several factors may inhibit them, including the perceived young age of the child, low parental self-efficacy, discomfort related to the child’s gender, feelings of shame or embarrassment, and intergenerational norms. Even among those who do initiate communication, various challenges persist. These include discomfort stemming from generational gaps, perceptions of children’s lack of receptiveness, and the context of poverty. Moreover, the content of the messages conveyed is often incomplete, sometimes inaccurate, prescriptive in nature, and predominantly focused on risks.
Figure 1.
Parental typology and barriers to communication about SRH with adolescents and young adults. Analysis of the findings reveals three distinct categories of parental attitudes toward SRH: parents who oppose such discussions, parents who are ambivalent, and parents who consider communication important. The first group typically justifies their reluctance by citing cultural traditions and the imperative to maintain intergenerational respect. The second group expresses concern that discussing these topics may encourage early sexual activity among youth. While the third group acknowledges the importance of engaging in dialogue with their children, not all members communicate systematically. Several factors may inhibit them, including the perceived young age of the child, low parental self-efficacy, discomfort related to the child’s gender, feelings of shame or embarrassment, and intergenerational norms. Even among those who do initiate communication, various challenges persist. These include discomfort stemming from generational gaps, perceptions of children’s lack of receptiveness, and the context of poverty. Moreover, the content of the messages conveyed is often incomplete, sometimes inaccurate, prescriptive in nature, and predominantly focused on risks.
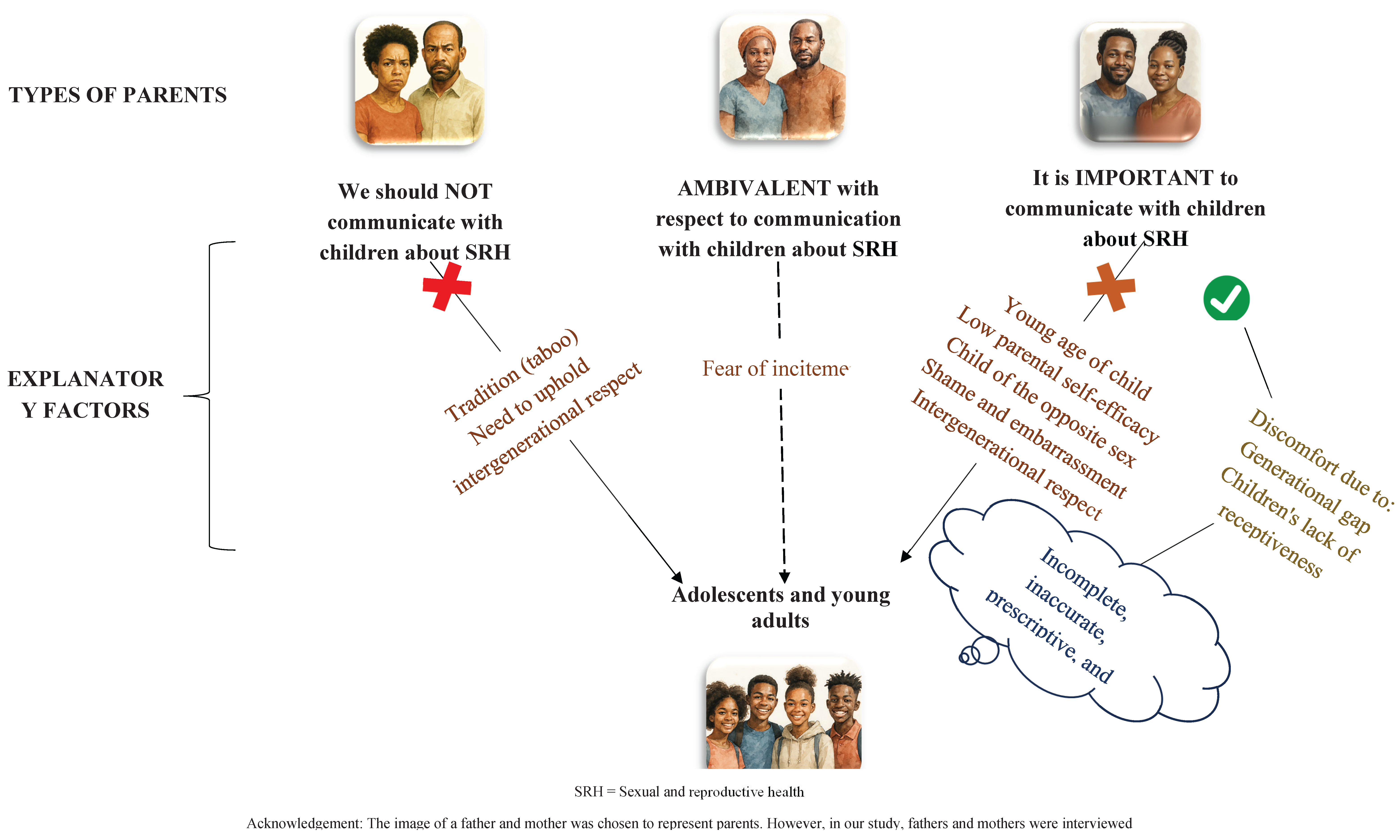

Table 1.
Content of parents’ messages broken down by UNESCO topics.
| UNESCO Topics [30] | UNESCO Subtopics [30] |
Content of parents’ message | Number of parents who communicated the message | Quote |
|---|---|---|---|---|
| Relationships | Families |
S/O | S/O | S/O |
| Friendship, Love and Romantic Relationships |
Stay away from boys, don’t hang out with boys to avoid getting pregnant | 1 | “I talk about sexuality and tell them not to spend too much time with boys and get pregnant because they’re not ready yet. They’re 14 and 15 years old, and you can see for yourself that it’s not a good idea to spend time with boys, so I give them advice to stay away from boys like this, like that.” Parent – Mother – participant #43 | |
| Don’t chase boys, don’t follow boys, don’t follow boys into the dark | 2 | |||
| Show off your boyfriend, tell people who are courting her to see if they are good people | 3 | |||
| Tolerance, Inclusion and Respect |
S/O | S/O | S/O | |
| Long-term commitments and Parenting | S/O | S/O | S/O | |
| Values, Rights, Culture and Sexuality | Values and Sexuality | It is not right to date other people’s husbands | 1 | “... so, when she came to tell me, I told her straight up that it’s not right, first of all, because you’re not old enough, you’re too young, and second, because you’re dating someone else’s husband, which is just not right.” Parent – Mother – Participant #15 |
| Don’t take the easy way out | 1 | |||
| Don’t give yourself to the first guy who comes along | 1 | |||
| Don’t let yourself be taken advantage of for money | 1 | |||
| Don’t do anything that isn’t right | 1 | |||
| It is not good to spoil someone else’s child | 1 | |||
| Human Rights and Sexuality | S/O | S/O | S/O | |
| Culture, Society and Sexuality | S/O | S/O | S/O | |
| Understanding Gender | The Social Construction of Gender and Gender Norms |
S/O | S/O | S/O |
| Gender Equality, Stereotypes and Bias | S/O | S/O | S/O | |
| Gender-based Violence | S/O | S/O | S/O | |
| Violence and Staying Safe | Violence | S/O | S/O | S/O |
| Consent, Privacy, and Bodily Integrity | S/O | S/O | S/O | |
| Safe use of Information and Communication Technologies (ICTs) |
S/O | S/O | S/O | |
| Skills for Health and Well-being | Norms and Peer Influence on Sexual Behaviour | S/O | S/O | S/O |
| Decision-making | Consequences of having sex (eg. it can spoil your future...) | 2 | “I tell children that sex is good… I say it’s good when you’re old enough to know, but when you’re not old enough and you want to do it, it’s not good… they should know that one day they will learn about it because there are advantages and disadvantages.” Parent – Father – participant #16. | |
| Sex has advantages and disadvantages | 1 | |||
| Communication, Refusal and Negotiation Skills | S/O | S/O | S/O | |
| Media Literacy and Sexuality | S/O | S/O | S/O | |
| Finding Help and Support | Exhortation to ask their parents questions | 1 | “...he just has to ask Dad or Mom. If I have any advice, I’ll give it to my child.” Parent - Father - Participant #34 | |
| Inform her mum when she (daughter) is going to have sex for the first time | 2 | |||
| Inform their parents if they become pregnant, instead of seeking an abortion | 1 | |||
| The Human Body and Development | Sexual and Reproductive Anatomy and Physiology |
Menstruation | 3 | “... I only focus on sex because we shouldn’t hide our faces, because if the child doesn’t know her own body it’s difficult, she’ll be exposed to a lot being outside, so it’s all that and then also her school life, everything, so it’s a bit of everything that she and I talk about.” Parent - Father - Participant #9 |
| Knowing your body | 1 | |||
| Reproduction | Knowing your cycle | 1 | ||
| Puberty | S/O | S/O | S/O | |
| Body Image | S/O | S/O | S/O | |
| Sexuality and Sexual Behaviour | Sex, Sexuality and the Sexual Life Cycle | Abstain, avoid giving oneself to a boy, wait until they are of age to have sex, abstain until they have finished their studies | 7 | “I tell them to take care of themselves, not to ask the little boys for money. If they need money, all they have to do is ask me, and if I don’t have any, I’ll do everything I can to give it to them. Asking young boys for money is what often leads to sexual relations between adolescents, that’s what happens.” Parent - Father - Participant #28” |
| No need to rush | 1 | |||
| Sexual Behaviour and Sexual Response | Protecting yourself to avoid early pregnancy and falling ill, advice on how not to get pregnant (eg. using the pill) | 14 | ||
| Avoid multi-partnering, have only one partner, remain faithful, don’t sleep with everyone | 4 | |||
| Don’t ask little boys for money | 1 | |||
| Sexual and Reproductive Health | Pregnancy and Pregnancy Prevention | Pregnancy, early pregnancy during schooling and its consequences for girls and all those involved | 8 | “That’s what I tell my daughters here, I tell them that work comes first because if you’re pregnant maybe the person isn’t ready yet that’s going to spoil your work and if you try to have an abortion you can die so let them be patient, let them work and tomorrow you have your work. Necessarily you’re going to have a husband.” Parent - Father - Participant #48 |
| Don’t get girls pregnant (for boys), consequences and responsibilities of impregnating a girl (for boys) | 3 | |||
| Avoid rushing into motherhood | 1 | |||
| Consequences of abortion | 1 | |||
| HIV and AIDS Stigma, Care, Treatment and Support | S/O | S/O | S/O | |
| Understanding, Recognizing and Reducing the Risk of STIs, including HIV |
Health, diseases (e.g., STIs) | 5 | “I tell him that AIDS kills. There are pills for it, but often even if you’re sick, you have simple malaria, and taking the medication is a problem, but for AIDS, it’s a matter of opinion, so you have to take the HIV pill every day. You can’t miss a dose, because if you do, the virus multiplies, and that’s how it can kill you. It’s better to abstain or protect yourself until you find the man you want to spend your life with.” Parent - Mother - Participant #37 | |
| Other | Studies first | Concentrate on their studies and prepare for the future (“think about your future, sex comes after, work comes first”). After your studies, you’ll get married. | 10 | “I told my wife to tell our daughter, I don’t approve of going out... going out as a girl, giving yourself to a boy is useless. You have to calm down first. My priority is the children; you have to study. Tomorrow you’re going to grow up to be somebody and then you’re going to get married and then have your wedding and then you don’t have any problems with anybody. We didn’t have the chance to go far in school, so if today they have parents who support them, they should leave the wife’s things there to work first. Whatever the expenses, even if I don’t work, I’ll manage to pay for their studies. They’ll make it far. Even if I’m not there, they’re comfortable.” Parent - Father - participant #36 |
| Be careful | Be careful with sex, be careful outside, be wary, be careful if you’re on your way to school and a young person calls out to you… |
7 | ||
| No secret |
Don’t hide anything from your parents | 1 |
Theme 6: The Human Body and Development
In this theme, the messages were related to two sub-themes: “Sexual and Reproductive Anatomy and Physiology” and “Reproduction.” These messages enabled girls to learn how to manage their periods, understand their menstrual cycle, and learn about their bodies. There were no messages related to the sub-themes “Puberty” and “Body Image.”
Theme 7: Sexuality and Sexual Behaviour
In this theme, the messages were related to the two sub-themes: “Sex, Sexuality, and the Sexual Life Cycle” and “Sexual Behaviour and Sexual Response.” The messages urged young people to practice abstinence, take their time before engaging in sexual relations, protect themselves against sexually transmitted diseases and pregnancies, and avoid sexual multi-partnership and transactional sex.
Theme 8: Sexual and Reproductive Health
In this theme, the messages were related to two sub-themes: “Pregnancy and Pregnancy Prevention” and “Understanding, Recognizing and Reducing the Risk of STIs, including HIV.” Communication was about pregnancy, early pregnancy during schooling and its consequences, the consequences of abortion and sexually transmitted diseases. There were no messages related to the sub-theme “HIV and AIDS Stigma, Care, Treatment and Support.”
Other themes
Other communications consisted of encouraging adolescents and young adults to focus on their studies instead of sexual relationships. There was also the “be careful” message often used by parents to encourage young adults to be cautious, and in particular young women to be wary of men and sex.
3.2.4. Communication Experience: Between Comfort and Discomfort
Discussing sexuality with children is not always straightforward, as reported by participants. Although many parents indicated feeling comfortable addressing SRH with their children, many parents expressed discomfort, which they attributed to various factors including generational gaps in values and experiences, limited receptivity from children, and socioeconomic insecurity (see Figure 1).
Parental Adaptation to Evolving Generational Norms in Sexuality
Some parents described the challenge of adapting to the realities of their children’s generation. They acknowledged that norms and expectations around sexuality have evolved significantly, making it difficult to rely on the parenting models they themselves experienced. One father, for instance, admitted that although he does not feel at ease discussing sexuality, he recognizes the urgency of the issue in today’s context.
“No, I’m not comfortable with it, but since it’s a current issue, we have to talk about it, otherwise I don’t feel comfortable.” Father, participant #47
Lack of Receptivity from Children
Discomfort is also associated with children’s level of receptiveness. Some parents, particularly mothers, observed that daughters who are already sexually active tend to be less responsive to parental guidance. One father expressed frustration over the lack of observable change despite repeated attempts to engage in dialogue, which ultimately led him to reduce communication in order to avoid tension and conflict.
“Really... that’s what I always say, when you give girls advice, they don’t want to listen to you, so what can you do? ... At home, I talk to my children, but you can’t feel comfortable when you talk to your children and they don’t listen to you.” Mother, participant #54
Socioeconomic Constraints and Pessimism
For certain parents, financial insecurity heightens discomfort. Two fathers noted that children tend to be more receptive when parents have sufficient financial means. One father expressed this view clearly:
“Well, we communicate with them, we talk to them, but if we communicate with them, they don’t understand. Well, we know it’s always about the means. If we have the means right away, we know how to manage young people, they will understand us. But if we don’t always have the means, we talk to them tomorrow, they will still go out... so it’s always about the means. If we have the means, nothing will happen, they will always listen to us, they will stay calm. It’s the means that we lack.” Father, participant #26
Choosing Discomfort Over Risk
Despite these challenges, some parents expressed a willingness to confront their discomfort for the sake of their children’s well-being. One participant emphasized that the unease of discussing sexuality was preferable to the consequences of silence, such as early pregnancy or illness.
3.2.5. Needs Expressed by Parents
Most participants expressed their needs. Some parents recognize that the message they convey is implicit, that their knowledge is limited, and that the message may not be adequate, or effective. For example, one mother’s understanding of ovulation was inaccurate. One mother also noticed that her daughters are reserved, and therefore she believes that the intervention of other people could be helpful. They would like to have support in educating their children about sexuality (including from teachers and others to supplement their message). Parents have a limited understanding of sex education, like the mother who says she doesn’t talk to her children about sexuality, even though she talks to her daughters about menstruation. They want to be made aware of and informed about the subject (eg., informational materials) and trained on how to broach the subject with their children. A few parents mentioned the need for courage to talk to their children and the need for their children to pay attention when they talk to them; and training could be useful in addressing this need by helping them to be ready to tackle the subject.
“Well, I need help because it’s true that I’m speaking for myself, but if there’s someone else who can add something, because I can’t know everything, that’s true, but we need someone else to add more.” Parent – Mother – participant #7
“For me, when I talk about sexuality with my children, I often get the impression that they feel a little ashamed, they are a little reserved, so I prefer to go through another person to talk to them. Maybe with another person they will feel comfortable enough to talk properly, so I prefer to go through other people to broach this subject.” Parent – Mother – participant #43
Other parents emphasized the need for financial resources. Some parents also think they don’t need anything. When it comes to adolescents and young adults, parents believe that the government and nongovernmental organizations should run awareness campaigns in schools and neighborhoods. They also believe that adolescents and young adults should be given advice on various topics (e.g., the dangers of sexual relations, avoiding bad company, not being envious, taking control of their lives, and taking school seriously). Parents also suggest regularly following up with adolescents and young adults, showing films, providing physical spaces for young people to exchange ideas and discuss issues, and offering free healthcare.
“... for general needs, there is a real need for awareness-raising by certain NGOs, we really need to communicate with children, I think that’s part of it.” Parent – Father – participant #9
Other needs include communication on social media and networks, government funding for youth awareness campaigns, the inclusion of sexual health concepts in the student training curriculum, and teacher training for this purpose.
4. Discussion
In this study, we explored parental communication on SRH in the Haut-Sassandra region in Côte d’Ivoire. Sociocultural factors hinder PCC. Many reasons explain the gap between intention to communicate with a child and actual practice (eg. low parental self-efficacy). Analysis of messages communicated to adolescents and young adults by parents reveals some gaps. Parents expressed their needs, for themselves, and for the adolescents and young adults in their families.
First, in Haut-Sassandra, sexuality is a taboo structuring intergenerational relation, limiting PCC despite growing recognition of the importance of SRH education. Beyond its educational dimension, sexuality reveals the tensions between tradition and modernity, authority and dialogue, control and autonomy. In this sense, sex education can be seen as a lever for social transformation, capable of redefining family relationships and parental roles from a more inclusive perspective. The prevailing silence, based on socio-cultural norms that prioritize verbal restraint and uphold parental authority, generates educational ambivalence. Parents oscillate between their role of transmission and the fear of encouraging sexuality deemed precocious. Yet international recommendations, notably those of UNESCO, advocate sex education from childhood onwards [30]. Delaying these conversations only reinforces the taboo and complicates future dialogue. Findings from this study indicate that both parents and children experience shame when addressing the topic, underscoring not only the persistence of the taboo but also its intergenerational transmission. Research further suggests that preadolescence is a particularly receptive period for SRH education, as children in this age group are more open to discussion and less likely to respond negatively than adolescents [31]. The absence of dialogue encourages young people to turn to informal sources, revealing an involuntary delegation of educational responsibility and a tension between traditional values and contemporary demands. Addressing these challenges requires strengthening parental competencies, establishing safe spaces for dialogue, deconstructing restrictive gender norms, and implementing culturally sensitive approaches.
Second, there is a notable gap between parents’ recognition of the importance of SRH education and their actual communicative practices. This disconnect stems from a range of psychosocial and cultural constraints, including the belief that early adolescence is an inappropriate time to discuss SRH. Such perceptions significantly delay PCC and are not limited to local contexts. For example, an American study identified a daughter’s age as a key predictor of parental engagement in sex-related discussions, with findings showing that as daughters grow older, mothers tend to cover more topics and initiate conversations at later ages [32]. These beliefs reinforce avoidance behaviours and contribute to the intergenerational transmission of silence. Our study highlights that, beyond the prevailing taboo around sexuality, other significant factors hinder PCC, particularly parental lack of knowledge and personal efficacy. In fact, for many parents, the challenge lies in initiating the conversation (22). Evidence suggests that parents are more likely to engage when they feel confident in their understanding of the topic [17]. Gender dynamics add another layer of complexity, particularly for fathers, who often struggle to discuss sex education with their daughters. As demonstrated by Lavoie (2014), many fathers report feeling underinformed and uncomfortable compared to mothers [31], which exacerbates feelings of shame and discourages open dialogue. The perception that such discussions are inappropriate for men deepens emotional discomfort and perpetuates silence within families. It is essential to multiply initiatives aimed at strengthening parents’ knowledge and self-confidence, so they can engage in meaningful and age-appropriate discussions on sexual health with their children, regardless of gender. By strengthening parents’ skills and creating safe spaces for discussion, it is possible to improve the transmission of information and promote sex education that is adapted to the realities of young people.
Third, although some parents do engage in conversations about sexuality with their children, these messages often reveal significant limitations in both content and form. The topics addressed tend to be narrow, with a focus on risk avoidance rather than the development of relational competencies. Messages are frequently normative, centered on abstinence and prohibition (e.g., “don’t do this or that”), and rarely include positive dimensions such as consent, and self-respect. The commonly used “be careful” message, for instance, remains vague and lacks actionable guidance. These findings align with a review of studies on parent-child communication about sexuality in sub-Saharan Africa, which highlights the prevalence of warnings and threats in parental discourse [8]. This pattern may reflect broader parenting styles, as communication approaches are closely linked to parental attitudes [33]. A study conducted among mothers of daughters aged 9 to 15 years in Iowa found that those with an authoritarian parenting style do engage in conversations about sexuality, but tend to avoid sensitive topics such as sexual orientation and condom use [32]. Even in more open contexts like Quebec, certain themes (eg. human development and sexual behaviour) remain difficult to address, as reported by francophone parents of preadolescents aged 9 to 12 [31]. This suggests that parents require targeted support to improve both the scope and quality of their communication.
Fourth, the needs expressed by parents reflect a desire to be involved in their children’s sex education, while revealing a keen awareness of the individual and structural limitations that stand in the way of this approach. Far from being merely ad hoc requests, these needs highlight levers for action to strengthen parenting skills, improve the transmission of SRH knowledge, and promote an educational approach based on co-responsibility between families, institutions and communities. The results of the study reveal a gap between the educational reference points of parents and the contemporary realities of young people, not least because of increased access to digital information. Many parents have not benefited from formal sex education, and express the need for structured support. The results of this study highlight the relevance of several activities planned for this project, such as the parents’ school, which aims to improve knowledge and strengthen parents’ capacities in terms of their children’s sex education. However, this study also makes it possible to specifically identify the parental typology and barriers to communication about SRH that need to be addressed.
5. Conclusions
The results of this study reveal that parent-child communication about sexuality in Haut-Sassandra is hampered by taboos, cultural norms and a lack of skills. To meet these challenges, structured interventions aimed at training parents are recommended, notably through adapted programs that reinforce their knowledge, communication skills and sense of efficacy. It is also essential to involve adolescents and young adults in the next research phases. Their perspective will enable us to assess the reception of parental messages, identify unmet needs and co-construct more relevant and inclusive educational approaches.
Author Contributions
Funding acquisition, conceptualization, and methodology: A.A., J.R., S.D., and M.J.D.; Data curation: M.K. and S.D.; Formal analysis: T.T.A., M.M.N., L.G.K., and M.J.D.; Writing—original draft: T.T.A. and M.J.D.; Writing—review and editing: All authors have read and agreed to the published version of the manuscript.
Funding
The PASSAGE project is funded by Global Affairs Canada under approval number P-010344
Institutional Review Board Statement
The project was approved by the Comité National d’Éthique des Sciences de la Vie et de la Santé in Côte d’Ivoire (N/Réf: 114–23/MSHPCMU/CNESVS-km) on 3 July 2023, and by the Research Ethics Committee of the CHU de Québec-Université Laval in Canada (Project 2024–7017), on 8 August 2023.
Informed Consent Statement
Informed consent for participation was obtained from all subjects involved in the study.
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author.
Acknowledgments
The authors would like to thank all partners, in particular the field team in the Ivory Coast, the interviewers and transcribers, for their contribution to this study.
Conflicts of Interest
The authors declare that this study received funding from Global Affairs Canada. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article, or the decision to submit it for publication.
Abbreviations
The following abbreviations are used in this manuscript:
| PCC | Parent-child communication |
| SRH | Sexual and reproductive health |
| PASSAGE | Projet d’Appui à des Services de Santé Adaptés au Genre et Équitables |
References
- Runcan, P.L., et al., The role of communication in the parent-child interaction. Procedia-Social and Behavioral Sciences, 2012. 46: p. 904-908. [CrossRef]
- Zhang, Y., Quality matters more than quantity: Parent–child communication and adolescents’ academic performance. Frontiers in Psychology, 2020. 11: p. 1203. [CrossRef]
- Vangelisti, A.L., The Routledge handbook of family communication. 2013: Routledge UK.
- Zapf, H., et al., A systematic review of parent–child communication measures: Instruments and their psychometric properties. Clinical child and family psychology review, 2023. 26(1): p. 121-142. [CrossRef]
- Evans, R., et al., Gender differences in parents’ communication with their adolescent children about sexual risk and sex-positive topics. The Journal of Sex Research, 2020. 57(2): p. 177-188. [CrossRef]
- Hurst, J.L., et al., Parent–child communication and adolescent sexual decision making: An application of family communication patterns theory. Journal of Family Psychology, 2022. 36(3): p. 449. [CrossRef]
- Widman, L., et al., Parent-adolescent sexual communication and adolescent safer sex behavior: A meta-analysis. JAMA pediatrics, 2016. 170(1): p. 52-61.
- Bastien, S., Kajula, L.J., Muhwezi, W.W., A review of studies of parent-child communication about sexuality and HIV/AIDS in sub-Saharan Africa. Reproductive health, 2011. 8: p. 1-17. [CrossRef]
- Vilanculos, E., and Mzikazi N., “The child can remember your voice”: parent–child communication about sexuality in the South African context. African Journal of AIDS Research, 2017. 16(1): p. 81-89.
- APESSA-Bénin, Guide de référence pour la conduite du dialogue parent-enfant en santé sexuelle et reproductive. Available at: https://apessa.net/wp-content/uploads/2019/03/Guide-pour-la-conduite-du-dialogue-parent-enfant-en-sant%C3%A9-sexuelle-et-reproductive.pdf. Consulted on June 6 2025. 2018.
- Kamangu, A.A., John, M.R., Nyakoki, S.J., Barriers to parent-child communication on sexual and reproductive health issues in East Africa: A review of qualitative research in four countries. Journal of African Studies and Development, 2017. 9(4): p. 45-50.
- Breakthrough RESEARCH, Quels sont les principaux obstacles et facteurs de facilitation associés à la communication intergénérationnelle sur la SSR au Niger et en Côte d’Ivoire ? Breakthrough RESEARCH Sommaire de Recherche. Washington DC: Population Council. Available at: https://breakthroughactionandresearch.org/wp-content/uploads/2022/09/BR_IntergenerationalComm_Brief_Fr.pdf. 2022.
- Houndjo, A., Dialogue parents-enfants sur la sexualité: clé de l’épanouissement des adolescents et jeunes. Le partenariat de Ouagadougou. Available at: https://partenariatouaga.org/dialogue-parents-enfants-sur-la-sexualite-cle-de-lepanouissement-des-adolescents-et-jeunes/. Consulted on June 6, 2025. 2020.
- Agbadje, T.T., et al., Freedom with regard to sexual and reproductive health and rights for adolescents and young adults of Haut-Sassandra, Ivory Coast: A study of stakeholders’ opinion. Sexes 2025, 6(4), 61.
- Wamoyi, J., et al., Parent-child communication about sexual and reproductive health in rural Tanzania: Implications for young people’s sexual health interventions. Reproductive health, 2010. 7: p. 1-18. [CrossRef]
- Mabunda, A.a.S.M., The context of parent-child communication about sexuality and HIV prevention: The perspectives of high school learners in gauteng province, South Africa. Botswana Journal of African Studies Vol. 31, No. 1, 2017 2017.
- Grey, E., et al., A systematic review of the evidence on the effect of parental communication about health and health behaviours on children’s health and wellbeing. Preventive Medicine, 2022. 159: p. 107043. [CrossRef]
- Conseil National des Droits de l’Homme (CNDH), Rapport Annuel CNDH 2023. Available from: https://cndh.ci/wp-content/uploads/2015/10/RAP-ANNUEL-2023-CNDH.pdf. Consulted on September 17, 2025. 2023. p. 67.
- Conseil National des Droits de l’Homme (CNDH), Communiqué de presse numéro 3. Available from: https://cndh.ci/wp-content/uploads/2015/10/COMMUNIQUE-DE-PRESSE-N%C2%B003.pdf. Consulted on September 17, 2025. 2024.
- Ministère de l’éducation nationale et de l’alphabétisation, Statistiques scolaires de poche, Rapport 2023-2024. MENA/DESPS. Direction des stratégies, de la planification et des statistiques. . 2024.
- Tisseron, C., et al., Exploring the sexual and reproductive health knowledge, practices and needs of adolescents living with perinatally acquired HIV in Côte d’Ivoire: a qualitative study. Reproductive Health, 2024. 21(1): p. 180. [CrossRef]
- UNICEF Côte d’Ivoire, Les adolescent(e)s et les jeunes – Analyse de la situation des enfants et des femmes en Côte d’Ivoire. Available from: https://www.unicef.org/cotedivoire/media/3106/file/Les%20adolescent%28e%29s%20et%20les%20jeunes.pdf. Consulted on September 17, 2025. 2020.
- N’Dri, M.K., et al., Trends and determinants of risky sexual behavior among adolescents and young adults in Côte d’Ivoire from 1998 to 2021. International Journal of Epidemiology and Health Sciences, 2025. 6(Continuous): p. e725382. [CrossRef]
- AGIR, Improving access to sexual and reproductive health rights for young people and adolescents in Côte d’Ivoire. Available from: https://solthis.org/wp-content/uploads/2024/12/AGIR-EN.pdf. Consulted on September 17, 2025. s.a.
- Ministère de la Santé et de l’Hygiène Publique (MSHP), Politique Nationale de la Santé Sexuelle, Reproductive et Infantile, Côte d’Ivoire. Available from: https://natlex.ilo.org/dyn/natlex2/natlex2/files/download/111964/CIV-111964.pdf. Consulted on September 22, 2025. 2020.
- Thompson J.B., Thorne S., Gurjit S., Interpretive description: A flexible qualitative methodology for medical education research. Medical education, 2021. 55(3): p. 336-343.
- Thorne, S., Interpretive description, in Routledge international handbook of qualitative nursing research. 2013, Routledge. p. 295-306.
- Creswell, J.W. and Poth C.N., Qualitative inquiry and research design: Choosing among five approaches. Fourth Edition. Sage publications. ISBN 978-1-5063-3020-4. 2016.
- Tong, A., Sainsbury P., and Craig J., Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. International journal for quality in health care, 2007. 19(6): p. 349-357. [CrossRef]
- UNESCO, International technical guidance on sexuality education: an evidence-informed approach. UNESCO Publishing. Available at: https://www.unfpa.org/sites/default/files/pub-pdf/266214fre.pdf. Consulted on June 11, 2025. 2018.
- Lavoie, G., Discuter de sexualité avec son préadolescent: les connaissances perçues et le sentiment d’autoefficacité des parents. 2014, Université du Québec à Montréal.
- Askelson, N.M., Campo S., and Smith S., Mother–daughter communication about sex: The influence of authoritative parenting style. Health Communication, 2012. 27(5): p. 439-448. [CrossRef]
- Isaksen, K.J., Musonda P., and Sandøy I.F., Parent-child communication about sexual issues in Zambia: a cross sectional study of adolescent girls and their parents. BMC public health, 2020. 20: p. 1-12. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



