
Submitted:
13 November 2025
Posted:
17 November 2025
You are already at the latest version
Abstract
Background: Avascular wounds represent a significant challenge in medical care due to impaired blood flow. Synthetic matrices, such as poly-lactic acid (PLA), have demonstrated promising results in promoting wound healing in complex wounds, including those with restricted blood supply, such as diabetic foot and venous leg ulcers. Objective: This case series presents the outcomes of five patients with avascular wounds of various etiologies successfully treated with PLA matrices. Case description: Five patients presented complex wounds involving exposure of bone, tendon, fascia, or osteosynthetic material. Wound bed preparation included debridement followed by PLA application covered with additional layers (non-adherent dressing, absorbent dressing, and compression bandage) as needed. Weekly assessments were conducted until full wound closure was achieved. Results: All cases showed successful outcomes, with PLA promoting granulation tissue formation and re-epithelialization, contributing to wound closure. One patient required skin grafts for complete healing. No local infections were reported before or after PLA application. Conclusion: PLA matrices are a practical and effective option for managing complex avascular wounds, promoting tissue regeneration and optimizing wound bed quality for skin grafts or flaps. While these findings are promising, further studies are needed to confirm the broader applicability and efficacy of PLA in avascular wound management.
Keywords:
avascular wounds
; polylactic acid
; synthetic biomaterials
; tissue regeneration
1. Introduction
Wounds with avascular components, such as exposed bone, joint surfaces, tendons, and orthopedic hardware, pose significant challenges in wound care due to the lack of blood flow to these structures. This absence hinders revascularization and the formation of regenerative tissue, which is crucial for healing. Historically, the gold standard for treating such complex soft tissue defects has been the transfer of vascularized tissue through microsurgical procedures or regional muscle, skin, or fascia transposition [1]. However, recent technologies such as negative wound pressure therapy and cellular, acellular and matrix-like products (CAMPs) have allowed the closure of these defects through less invasive procedures via a combination of wound bed temporization and skin grafting [2].
CAMPs are a heterogeneous group of advanced wound care therapies comprising living cells, tissues and/or engineered materials derived from diverse sources. These products are designed to promote wound healing and tissue regeneration by providing bioactive components, growth factors, and structural support to the wound healing [3]. Within CAMPs, synthetic dermal closure matrices, a novel category of alloplastic skin substitutes, are increasingly used for wound closure. Specifically, poly-lactic acid (PLA) wound closure matrices have consistently demonstrated favorable closure outcomes for patients with complex vascular wounds and burns by restoring the interaction of the key elements involved in the wound-healing process [4,5]. Most of these outcomes can be directly attributed to the fact that the degradation product of PLA matrices is lactate, which in turn is a potent signaling molecule that enhances neo-angiogenesis in wounds [6].
Given these promising results, we believe PLA matrices have significant potential for treating wounds with avascular components. Here, we present a case series of five patients successfully treated with a novel PLA dermal matrix to enhance wound repair over complex soft tissue defects with exposed avascular structures.
2. Case Description
Five patients (3 females, 2 males) with wounds of various etiologies and exposed avascular structures were treated with PLA matrices at the Wound Clinic of a tertiary level trauma care center in the city of San Luis Potosi, Mexico. The management protocol for these wounds included a comprehensive clinical and wound assessment, with particular attention to the use of medications affecting wound healing, nutritional optimization when needed, and assessment of the vascular and infectious status of the wounds following the “prepare to repair” paradigm [7]. In all cases, major vascular pathology was ruled out using a combination of infrared thermography, ankle-brachial index, and clinical evaluation [8]. Bacterial contamination or infection was excluded through fluorescence-based assessments and bacterial culture [9]. Wound bed preparation included surgical debridement and hemostasis, followed by the application of PLA matrices (Supra SDRM, PolyMedics Innovations, Kirchheim unter Teck, Germany) using the “sandwich technique” (Figure 1). Briefly, the PLA matrix was applied directly onto the wound bed without extending beyond the edges. For undermined areas or deep soft tissue defects, the material was layered in up to two or three layers. Next, a self-adherent, non-contact dressing (Supra Net, Polymedics Innovations) was added, and an outer layer of absorbent dressings (i.e., gauze pads or silver foam dressings) was applied on top. Finally, a mild compression bandage was used to secure all the layers below. This dressing technique allows the changing of the outermost layers as often as needed without disturbing the inner layers containing the PLA matrix and non-contact layer. Outer dressing changes were performed every seven days and wound assessments were performed on a weekly basis until healing. In all cases, PLA matrices were applied only once and remained untouched until complete degradation, which occurred between days 7 and 14, depending on the moisture of the wound and the number of layers applied
Case 1
A 62-year-old male with no significant medical history developed a surgical site infection and dehiscence after fixation of an exposed tibial fracture (Figure 2A). The wound bed was necrotic and covered with slough. After undergoing drainage, debridement, and a course of IV antibiotics, exposed osteosynthetic material was identified. PLA matrices were applied to the wound bed, covering the fixation hardware. By week five, granulation tissue covered the metal implants, leading to complete healing of the wound at week eight with no major scarring or mobility limitation after a 10-month follow-up.
Case 2
An 82-year-old female patient with a mild malnutrition status, bedridden due to a previous stroke, and exhibiting signs of dementia, presented with a one-week-old wound on the anterior region of the left leg exposing the extensor hallucis longus tendon caused by rubbing one leg against the other (Figure 2B). During the initial assessment, debridement of the wound and application of a single layer of PLA matrices were performed. Over the following weeks, progressive granulation tissue formation over the peritendon was observed, and by the fourth week, re-epithelialization of the wound edges was completed. The patient was followed for six additional months, during which the healed site had good skin quality and only minor pigmentation changes in the scar tissue.
Case 3
A 56-year-old female with controlled type 2 diabetes mellitus was referred to our clinic for a surgical wound dehiscence following an Achilles tendon repair (Figure 2C). The wound resulted in significant exposure of the peritendon. PLA matrices were applied to the wound and outer dressings were changed weekly. Complete wound closure was achieved within 10 weeks, with excellent skin quality and preserved range of motion, suggesting no adherence of the tendon to the skin at the closure site.
Case 4
A 57-year-old female patient with a medical history of uncontrolled diabetes and lupus erythematosus under chronic high-dose corticosteroid therapy was referred to the Wound Clinic after experiencing a fall that resulted in an ulcer on her right leg with exposure of the underlying bone (Figure 3). The ulcer failed to heal with standard wound care management and the bone’s periosteum eventually became necrotic. The patient reported severe pain and expressed concerns regarding potential further tissue damage, ultimately refusing any surgical intervention, such as a tissue flap. The decision to apply PLA matrices was made in response to this, and the material was applied to the wound to cover the defect. Interestingly, over the course of the initial week of treatment, the patient reported pain relief. Over the following course of five weeks, granulation tissue and epithelium formed from the wound edges, leading to complete cover of the bone defect, closure of the ulcer, and successful healing.
Case 5
A 32-year-old healthy male patient presented to the emergency department with a frontal region trauma caused by a sharp-blunt weapon (machete), resulting in an avulsive injury with exposed bone (Figure 4). The patient was admitted for wound bed preparation, which involved the debridement of devitalized tissue and intraoperative application of PLA matrices. After two weeks of treatment and despite the initial size of the wound, more than 15% size reduction was observed without significant tissue contraction. The periosteum was found to be covered with well-vascularized repair tissue, making the patient a candidate for reconstruction using a scalp advancement flap and a full-thickness skin graft over the residual wound site. This large soft tissue defect healed with good skin quality and without adverse sequelae.
3. Discussion
The case series presented in this manuscript involves five patients treated with PLA-guided matrices for various wounds with exposed avascular structures. Among these patients, one presented with an avulsive wound in the frontal region that involved exposure of the underlying bone. The remaining four cases involved wounds in the lower extremities, characterized by exposure of osteosynthetic material, bone, tendon, or fascia. The cases presented in the current manuscript demonstrate that PLA matrices are a suitable material for promoting adequate repair of wounds with avascular components.
PLA matrices have demonstrated effectiveness in treating other complex wounds, including burns, diabetic foot ulcers, and venous leg ulcers [3]. Yet, evidence regarding their use in soft tissue defects with avascular components remains limited. In recent studies conducted by our group, PLA treatment reduced the time to complete healing by 44% in diabetic foot ulcers and by 95% in venous leg ulcers compared to collagen, and 40% compared to fish grafts. 80% of PLA-treated patients achieved full healing within 12 weeks, as opposed to 33% in the collagen group [10,11]. Other synthetic materials, such as polyglycolic acid and boron-based glass fibrous matrices, have also been reported in case reports addressing avascular wounds, but further evidence is needed to establish their efficacy [3]. Polyurethane matrices have also been explored in complex wounds with exposed bone or tendon. A case series by Solanki et al. [12] reported positive outcomes in 25 patients, including 18 with complex wounds, treated with a two-stage reconstruction approach that required skin grafting, although infections were commonly encountered. In our series, one case required skin grafts, but no infections were observed after applying the PLA matrices, suggesting that PLA matrices may offer comparable benefits with potentially fewer complications.
The therapeutic effect of the PLA matrices can be mainly attributed to the release of lactate, which acts as a paracrine agent (referred to as a lactormone) with potent signaling effects that promote neo-vascularization through stimulation of vascular endothelial growth factor (VEGF), leading to granulation in the wound bed and facilitating collagen synthesis and fibroblast migration [5,6,13]. Lactate also lowers the local pH levels, which in turn inhibits bacterial growth and prevents the matrix degradation caused by bacterial activity [5,13]. Furthermore, the microporous structure of the PLA matrices serves as a supportive scaffold and maintains a moist environment with high vapor permeability [4]. These mechanisms contribute to the preservation of tissue viability and integrity, assisting in secondary closure or preparing the wound bed for definitive surgical repair.
Synthetic matrices, such as PLA, offer a promising, practical, and simple alternative for optimizing the wound bed prior to flap or graft placement, thereby enhancing outcomes, reducing complications, and potentially allowing spontaneous closure in selected small, non-recurrent wounds.
In this case series, one out of five patients required skin grafts after receiving PLA matrix treatment. Therefore, it is reasonable to propose that PLA matrices could be used initially for one to two weeks to assess wound healing progress, potentially decreasing the need for more complex therapies.
Limitations
As we present our case series, it is important to acknowledge that our findings may not yet be generalizable and instead, reflect the clinical experiences of practitioners using PLA matrices for avascular wounds. Based on our observations, we strongly believe in the efficacy of the product for managing patients with complex wounds, but it remains essential to emphasize the need for further evidence. Additional research focusing on complex soft tissue defects and comparative studies is necessary to thoroughly evaluate the effectiveness of PLA and support its wider applications in clinical practice.
4. Conclusions
This case series highlights the potential of PLA matrices as an effective and practical option for the management of avascular wounds. Across five cases involving various complex wound etiologies, PLA matrices promoted granulation tissue formation, supported re-epithelialization, and achieved successful wound closure. The favorable outcomes observed suggest that PLA matrices may represent a promising alternative to more complex therapies, such as negative pressure wound therapy and skin transplantation, while remaining accessible to a wide range of health care providers. While these observations offer valuable insights into the potential applications of PLA for avascular wounds, further research is needed to confirm these observations and establish the broader clinical efficacy of this approach.
Author Contributions
Conceptualization, supervision and writing:—review and editing, Martinez-Jimenez MA; visualization and writing—original draft preparation, Novoa-Moreno AL.; data curation, Loza-González VM.; writing—review and editing, Perez-MedinaCarballo R.; investigation, Cervantes-Báez PA. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. Ethical review and approval were waived, as the research involved only anonymized data obtained from routine clinical practice and posed no additional risk to participants.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patients to publish this paper.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| PLA | Polylactic Acid |
| CAMP’s | Cellular, acellular and matrix-like products |
| IV | Intra venous |
| VEGF | Vascular endothelial growth factor |
References
- Simman, R. and M.H.E. Hermans, Managing Wounds with Exposed Bone and Tendon with an Esterified Hyaluronic Acid Matrix (eHAM): A Literature Review and Personal Experience. J Am Coll Clin Wound Spec, 2017. 9(1-3): p. 1-9. [CrossRef]
- Bogdasarian, R.N., et al., Treating Wounds With an Avascular Component With a Dermal Regenerative Template. Wounds, 2020. 32(1): p. 1-10.
- Horn, C.P., A.L. Fierro, and J.C. Lantis, 2nd, The Shift to Synthetics: A Review of Novel Synthetic Matrices for Wound Closure. Surg Technol Int, 2023. 42: p. 75-86.
- Haller, H.L., et al., Made in Germany: A Quality Indicator Not Only in the Automobile Industry But Also When It Comes to Skin Replacement: How an Automobile Textile Research Institute Developed a New Skin Substitute. Medicina (Kaunas), 2021. 57(2). [CrossRef]
- Haller, H.L., et al., Oxygen, pH, Lactate, and Metabolism-How Old Knowledge and New Insights Might Be Combined for New Wound Treatment. Medicina (Kaunas), 2021. 57(11). [CrossRef]
- Porporato, P.E., et al., Lactate stimulates angiogenesis and accelerates the healing of superficial and ischemic wounds in mice. Angiogenesis, 2012. 15(4): p. 581-92. [CrossRef]
- Regulski, M. Preparing to Repair in Diabetic Wound Care: Insights from an Expert. 2023; 36(5):[Available from: https://www.hmpgloballearningnetwork.com/site/podiatry/diabetes-watch/preparing-repair-diabetic-wound-care-insights-expert.
- Martinez-Jimenez, M.A., et al., Development and validation of an algorithm to predict the treatment modality of burn wounds using thermographic scans: Prospective cohort study. PLoS One, 2018. 13(11): p. e0206477. [CrossRef]
- Andersen, C.A., K. McLeod, and R. Steffan, Diagnosis and treatment of the invasive extension of bacteria (cellulitis) from chronic wounds utilising point-of-care fluorescence imaging. Int Wound J, 2022. 19(5): p. 996-1008. [CrossRef]
- Liden, B.A., et al., A multicenter retrospective study comparing a polylactic acid CAMP with intact fish skin graft or a collagen dressing in the management of diabetic foot ulcers and venous leg ulcers. Wounds, 2024. 36(9): p. 297-302. [CrossRef]
- Liden, B.A. and J.L. Ramirez-GarciaLuna, Efficacy of a polylactic acid matrix for the closure of Wagner grade 1 and 2 diabetic foot ulcers: a single-center, prospective randomized trial. Wounds, 2023. 35(8): p. E257-E260.
- Solanki, N.S., et al., A consecutive case series of defects reconstructed using NovoSorb(Ⓡ) Biodegradable Temporising Matrix: Initial experience and early results. J Plast Reconstr Aesthet Surg, 2020. 73(10): p. 1845-1853. [CrossRef]
- Certo, M., et al., Understanding lactate sensing and signalling. Trends Endocrinol Metab, 2022. 33(10): p. 722-735. [CrossRef]
Figure 1.
“Sandwich technique.” Description of the method used for covering a wound by layering multiple materials.
Figure 1.
“Sandwich technique.” Description of the method used for covering a wound by layering multiple materials.
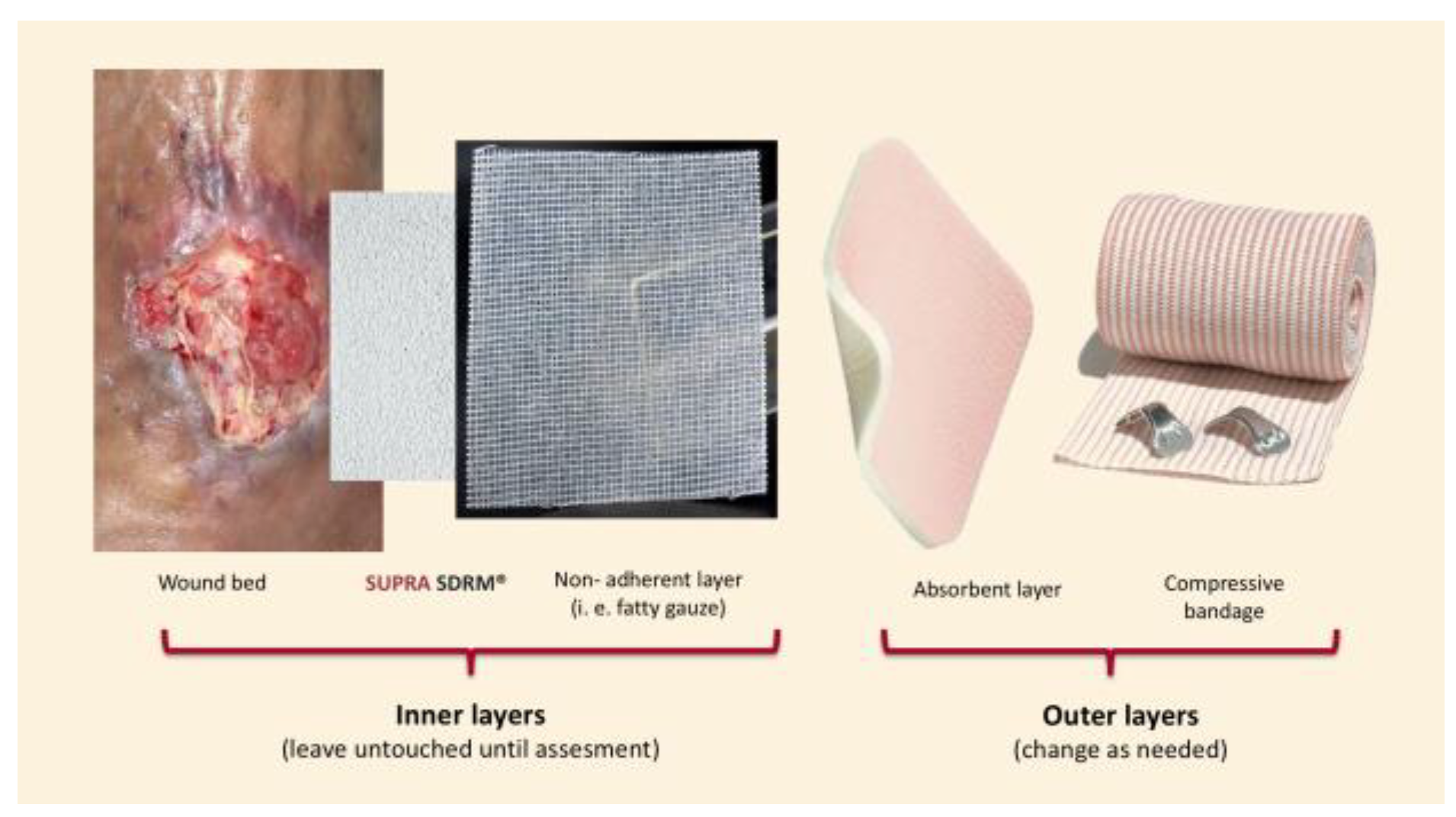
Figure 2.
Sequential presentation of lower-leg injuries: (A) tibial fracture wound with osteosynthesis material, (B) friction wound with exposed tendon, and (C) postoperative wound showing Achilles tendon exposure.
Figure 2.
Sequential presentation of lower-leg injuries: (A) tibial fracture wound with osteosynthesis material, (B) friction wound with exposed tendon, and (C) postoperative wound showing Achilles tendon exposure.

Figure 3.
Right leg ulcer with exposed bone.

Figure 4.
Frontal region wound with exposed bone caused by a machete impact.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



