Submitted:
12 November 2025
Posted:
14 November 2025
You are already at the latest version
Abstract
Objective. To evaluate the prevalence, risk factors, aetiology, and management of traumatic dental injuries (TDIs) among children aged 1–18 years attending the De-partment of Pediatric Dentistry, Damascus University, Syria, during 2023–2024, and to illustrate representative clinical cases with documented outcomes. Methods. This ret-rospective cross-sectional study reviewed 2,716 patient records (2023–2024) and identi-fied 301 children with TDIs. Demographic, clinical, and behavioural variables were ex-tracted and analysed using χ², t tests, ANOVA, and binary logistic regression (IBM SPSS v26). Results. The overall TDI prevalence was 11.08%. Males were over twice as likely as females to experience TDIs (OR = 2.30; 95% CI = 1.76–3.01; p < 0.001). Older age acted as a protective factor (OR = 0.56; 95% CI = 0.43–0.74; p < 0.001). Falls were the most common cause (63.7%), and injuries most often occurred at home (48.9%). The maxillary central incisors were most frequently affected (68.5% of cases). Children with special healthcare needs had significantly more traumatised teeth (mean = 2.61 ± 1.13) than healthy chil-dren (1.66 ± 0.92; p < 0.001). Nearly half of the patients (45.3%) presented > one month after injury, and asymptomatic apical periodontitis and reversible pulpitis were the most frequent diagnoses. Representative case presentations demonstrated multidisci-plinary management using restorative, endodontic, and orthodontic approaches with favourable follow-up outcomes. Conclusions. TDIs affected about one in nine children in this Syrian cohort. Male gender, younger age, and previous trauma were key risk factors. The predominance of delayed presentation underscores the need for community education, early referral systems, and targeted preventive programs within school and home environments.
Keywords:
traumatic dental injuries
; prevalence
; risk factors
; case presentations
; Syria
; pediatric dentistry
1. Introduction
Traumatic dental injuries (TDIs) represent a major public health concern worldwide, particularly among children and adolescents. They rank second only to dental caries in prevalence, preceding periodontal disease as a cause of oral morbidity and functional impairment [1,2,3]. Beyond their physical consequences, TDIs often result in significant psychological distress, aesthetic concerns, and economic burden for affected families, collectively diminishing children’s oral health–related quality of life [4,5,6].
Epidemiological studies indicate a wide variation in the global prevalence of TDIs, ranging from 4% to over 40%, depending on population characteristics, study design, diagnostic criteria, and sociocultural context [7,8,9]. A meta-analysis by Petti et al. [3] estimated that more than one billion people have experienced a TDI, with prevalence rates of 22.7% in primary dentition and 15.2% in permanent dentition. Such disparities across regions are influenced by behavioural, environmental, and systemic factors—including sports participation, unsafe environments, and socioeconomic inequality.
Risk factors for TDIs are multifactorial. Established determinants include male gender, increased overjet, inadequate lip coverage, history of previous trauma, and participation in contact sports [10,11,12,13]. Glendor [14] grouped these into three broad categories: (1) oral factors, such as dental malocclusion and overjet; (2) environmental factors, including material deprivation and unsafe surroundings; and (3) behavioural factors, such as aggression and exposure to violence. More recent literature has expanded this framework to include systemic conditions, developmental disorders, and sensory or motor impairments that increase susceptibility to trauma [15]. Children with special healthcare needs are especially vulnerable due to impaired motor coordination, limited protective reflexes, and behavioural challenges [16,17].
Favourable outcomes following TDIs depend on public awareness of emergency management and timely access to professional care [18,19]. Since prognosis worsens with delayed treatment, preventive education and organized emergency dental services are essential components of child oral health policy [20].
1.1. Local Context
In Syria, published data on TDIs are scarce. Over two decades ago, Marcenes et al. [21] surveyed 1087 Syrian schoolchildren aged 9–12 years and reported a prevalence of 5.2% at age 9 and 11.7% at age 12. More recently, Alshayeb et al. [22] reported a prevalence of 17.6% among Syrian children aged 9–12 years (2023–2024), attributing the rise to increased exposure to accidents and violence associated with prolonged conflict. The ongoing humanitarian crisis has profoundly influenced children’s living conditions—marked by overcrowding, unsafe play areas, and limited access to dental services—potentially elevating the risk and severity of TDIs [23]. However, national-level epidemiological data remain limited and fragmented, underscoring the need for updated institutional evidence.
1.2. Rationale and Aim
The Department of Pediatric Dentistry at Damascus University serves as a national referral center providing comprehensive dental care to children and individuals with special needs. Understanding the prevalence, etiology, and management of TDIs in this context is crucial for informing both academic curricula and public health initiatives. While the study was conducted in an institutional and urban setting (Damascus University), the diversity of patients referred from multiple governorates supports a cautious generalization beyond the Damascus population.
1.3. Hypothesis and Research Question
This study aimed to document the prevalence, risk factors, and treatment characteristics of TDIs among children attending Damascus University between 2023 and 2024, with selected case presentations illustrating typical clinical scenarios.
We hypothesized that the prevalence and patterns of TDI differ significantly by age, gender, and health status under post-conflict conditions in Syria.
2. Materials and Methods
2.1. Study Design and Ethical Approval
This retrospective cross-sectional study was conducted at the Department of Pediatric Dentistry, Faculty of Dentistry, Damascus University, Syria. It aimed to determine the prevalence, risk factors, and management patterns of traumatic dental injuries (TDIs) among children aged 1–18 years who attended the department between January 2023 and December 2024.
The study followed the Preferred Reporting Items for Observational Studies in Endodontics (PROBE 2023) guidelines [24]. Ethical approval was obtained from the Research Ethics Committee of Damascus University (Approval No. 2654/13.02.2023) and from the Ministry of Higher Education and Research. The research adhered to the principles of the Declaration of Helsinki (2013 revision). Caregivers of all patients had provided written informed consent at the time of initial treatment, allowing anonymized use of patient records for academic and research purposes.
2.2. Study Population and Sample Selection
The study population consisted of all pediatric patients (n = 2990) who received treatment at the Department of Pediatric Dentistry during the 2023–2024 period. The department functions as a tertiary public referral center, treating children from Damascus and surrounding governorates. All available patient records were reviewed.
Inclusion criteria were:
- Children aged 1–18 years,
- Diagnosed and treated for dental trauma during the study period, and
- Complete documentation of demographic, diagnostic, and treatment data.
Records with missing or illegible essential information (demographics, trauma diagnosis, or treatment details) were excluded (n = 64, ≈2%). The final analytical sample consisted of 2716 valid records, including 301 TDI cases (11.08%) and 2,415 non-trauma cases (control group). The control group, matched by age and gender, consisted of children who attended the same clinic during the same period for other dental conditions (caries, malocclusion, and preventive care) and were used for comparative statistical analysis.
2.3. Data Extraction and Calibration
Two trained examiners (Y.A.T. and M.A.) independently screened and extracted data from the records using a standardized form. Before data collection, both underwent a calibration process supervised by an experienced pediatric dentist (N.B.) to ensure diagnostic consistency. A pilot evaluation of 30 randomly selected records was conducted independently by both examiners, and discrepancies were resolved through discussion until full agreement was reached.
The inter-examiner reliability was assessed using Cohen’s kappa coefficient (κ = 0.89), indicating excellent agreement. Continuous supervision and periodic cross-checking were maintained throughout data collection to minimize observer bias.
2.4. Variables and Diagnostic Criteria
The following data were extracted:
- Demographic variables: age, gender, and governorate of residence.
- Health status: classified as healthy or special healthcare needs (SHCN). SHCN categories followed Almonaqel’s classification [25]: neurological disorders, sensory impairments, behavioural disabilities, medical disabilities, and developmental/congenital impairments. SHCN status was confirmed through medical documentation provided by caregivers and verified by the supervising pediatric dentist.
- Behavioural assessment: rated according to the Frankl Behaviour Rating Scale (definitely negative, negative, positive, definitely positive).
- Occlusion type: assessed using Angle’s classification and primary molar relationships (flush terminal plane, distal step, mesial step).
- Caries experience: recorded as dmft/DMFT indices following WHO criteria [26].
- Previous history of trauma: yes/no, based on caregiver report and previous record review.
- Apex status: classified radiographically as open or closed, according to Gill et al. [27].
- Etiological and situational variables: time between trauma and dental visit, place of injury (home, school, street, etc.), and cause (falls, traffic accidents, collisions, fights).
Traumatic dental injuries were categorized according to the 2022 World Health Organization Classification of Traumatic Dental Injuries (NA0D) [28], which includes two major groups:
- 1.
- Fracture-related injuries (enamel fracture, enamel–dentin fracture, complicated crown fracture, crown–root fracture, root fracture).
- 2.
- Luxation-related injuries (concussion, subluxation, extrusive, lateral, and intrusive luxation, avulsion).
2.5. Data Management and Quality Control
All data were entered into Microsoft Excel 2021 and cross-checked for accuracy by an independent reviewer (R.M.). Each child was assigned a unique identification number to prevent duplication of cases or overcounting of multiple visits related to the same traumatic event. Only the first visit for each trauma episode was included; re-treatments and follow-ups were excluded.
Incomplete or unclear entries were flagged and discussed among the investigators. Random audits were performed to verify data integrity and minimize transcription errors.
2.6. Statistical Analysis
Data were analyzed using IBM SPSS Statistics version 26 (IBM Corp., Armonk, NY, USA). Descriptive statistics (frequencies, means, and standard deviations) were computed for all variables.
Inferential analyses included:
- Chi-square tests (χ2) for categorical variable comparisons,
- Independent-samples t tests and ANOVA with Bonferroni post hoc for continuous variables, and
- Binary logistic regression to identify independent predictors of TDIs (dependent variable: injury presence = yes/no).
Odds ratios (OR) with 95% confidence intervals (CI) were reported, and a p-value < 0.05 was considered statistically significant.
2.7. Methodological Considerations
Given the retrospective hospital-based design, findings reflect patterns among children seeking care at an academic dental institution and may not represent the full community prevalence of TDIs. However, the large sample size, rigorous calibration, and standardised classification enhance both internal validity and reproducibility.
3. Results
3.1. TDIs Prevalence and the Associated Risk Factors of the Sample
A total of 2716 patient records were analyzed, of which 301 children (11.08%) presented with traumatic dental injuries (TDIs)—the remaining 2415 served as the control grouMale children had a significantly higher prevalence (13.9%) compared with females (7.5%) (p < 0.001). The 12–18-year age group showed the highest rate (18.2%), compared with younger children (p < 0.001) (Table 1). Logistic regression identified male gender (OR = 2.30; 95% CI: 1.76–3.01) as a strong independent predictor, while increasing age (OR = 0.56; 95% CI: 0.43–0.74) was found to be protective (Table 2).
3.2. Caries Indices and Oral Health Correlates
The mean caries indices (DMFT/dmft) were significantly higher in non-trauma cases than in trauma cases (p < 0.001), suggesting that caries experience was not a risk factor for dental trauma. Children with TDIs generally showed good oral hygiene and predominantly exhibited positive or definitely positive behaviour, according to the Frankl scale (Table 3).
3.3. Injury Characteristics and Treatment
Table 4 summarizes the distribution of trauma type, pulp diagnosis, time to presentation, and treatment modality. Complicated crown fractures (39.1%) were the most frequent injuries among permanent teeth, whereas complicated crown–root fractures (23.1%) predominated in primary teeth. Falls represented the leading cause (63.7%), and nearly half the children (45.3%) presented more than one month after the injury, underscoring the delay in seeking care. Asymptomatic apical periodontitis (32.1%) and reversible pulpitis (29.6%) were the most frequent pulp diagnoses in permanent teeth.
3.4. Distribution by Age, Health Status, and Etiology
The mean number of traumatized teeth per child was 1.75 ± 0.98, ranging from one to five teeth. SHCN children had a significantly higher mean (2.61 ± 1.13; p < 0.001). Children under six years exhibited the highest mean number of affected teeth, reflecting the greater vulnerability of the primary dentition.
3.5. Illustrative Clinical Cases
Representative clinical cases managed within the department are presented in Figure 3, Figure 4 and Figure 5, demonstrating orthodontic–prosthodontic, surgical, and regenerative approaches, respectively, with follow-ups confirming functional and aesthetic success. All case images were published with documented parental consent and anonymization.
Case 1:
A 14-year-old adolescent presented to the Department of Pediatric Dentistry 18 months after a traumatic dental injury. The trauma had resulted in complete avulsion of tooth #21, accompanied by space loss due to the drift of teeth #11 and #22 into the edentulous area. The case was managed using a fixed orthodontic appliance to regain the lost space, followed by prosthetic rehabilitation with an adhesive bridge to replace the missing tooth. The overall treatment duration was seven months.
Case 2:
A 7-year-old child presented to the Department of Pediatric Dentistry three days after the injury with a complicated crown fracture involving pulp exposure in tooth #42. Radiographic examination revealed that the fractured crown fragment was embedded within the lower liAs the tooth had a closed apex, the fragment was surgically removed from the lip, followed by traditional endodontic treatment of tooth #42 in the same visit. The fractured crown segment was then successfully reattached to restore the tooth’s original form and function.
Case 3:
A 9-year-old child presented to the Department of Pediatric Dentistry with a history of recurrent dental trauma. The first injury, one year prior, had resulted in an uncomplicated crown fracture of tooth #11, still untreated. In contrast, the second trauma, one month earlier, caused an uncomplicated crown fracture of tooth #21. The child’s main complaint was pain associated with tooth #21. Routine radiographic examination revealed pulp necrosis in tooth #11. A vital pulp therapy using MTA was performed on tooth #21, whereas tooth #11 was managed with an MTA apical plug.
A two-year follow-up radiograph showed a marked reduction in the periapical radiolucency of tooth #11 and the formation of a mineralized apical barrier adjacent to the plug. In contrast, tooth #21 later developed symptoms of acute apical periodontitis, necessitating additional endodontic intervention.
3.6. TDI Risk Factors According to the Age Classification
In children with TDIs, a significant difference was found when comparing age classification and gender; both males and females in the 6–12-year age group were most frequently affected by TDIs. Although healthy children aged 6–12 years were the most commonly affected by TDIs, the incidence of TDIs among SHCN children was relatively evenly distributed across all age groups. No association was found between a previous traumatic injury and its recurrence in all age groups.
The highest percentages of traumas were due to falls and collisions with objects in the 6-<12 age group (43.3% and 9.0%, respectively). However, the highest percentage of trauma caused by fights was in the 12-year-old ≤ age grouTraffic accidents as a cause of dental trauma were similar across all age groups (Table 5).
3.7. TDIs’ Risk Factors According to the Number of Traumatized Teeth
The mean number of traumatized teeth was higher among SHCN children (2.61±1.133) compared to healthy children (1.66±0.918), with significant differences (p<0.001). The highest mean number of traumatized teeth was in the age group under 6 years (reflecting the primary dentition stage), with significant differences. Finally, the number of traumatized teeth varied significantly according to the cause of TDIs. Traffic accidents resulted in the highest number of affected teeth, followed by collisions with objects (2.93 ± 1.944 and 2.04 ± 1.105, respectively), with statistically significant differences (Table 6).
Significant differences in the mean number of traumatized teeth were found between primary dentition and mixed dentition, as well as between primary dentition and permanent dentition (p<0.05). The highest mean was observed in the under-6 age group (2.34 ± 1.234), with significant differences noted when post hoc tests were applied. The mean number of traumatized teeth due to traffic accidents was the highest among trauma causes, with significant differences (Table 7).
4. Discussion
4.1. Overview and Key Findings
This study provides updated epidemiological evidence on traumatic dental injuries (TDIs) among children and adolescents in Syria—one of the few national-level datasets collected in a post-conflict setting. The overall prevalence of 11.08% aligns with global averages (10–15%) and demonstrates the continuing public health burden of dental trauma in low- and middle-income contexts. Male gender, younger age, and a history of previous trauma were significant predictors of TDIs. Falls at home were the most common cause (63.7%), and nearly half of the patients (45.3%) presented for treatment more than one month after injury—delays associated with increased risk of pulpal and periapical complications. The findings also confirm the heightened vulnerability of children with special healthcare needs (SHCN), who sustained a significantly higher mean number of traumatised teeth.
4.2. Global Comparisons
The prevalence observed in this study is consistent with international reports: India (13%) [29], Turkey (10–15%) [30], and Saudi Arabia (12%) [9], yet notably lower than Sweden (37.6%) [31] and some European urban cohorts where organized sports and outdoor activities increase exposure to injury [32].
Gender distribution (71% male, 29% female) mirrors results from Lebanon (male-to-female ratio 2.1:1) [12] and Jordan (2.3:1) [33], reaffirming that male children are more likely to experience trauma due to greater physical activity and risk-taking behaviour.
Age-related trends in the present study, with a peak between 6–12 years, also correspond with studies from Greece [34] and India [11], reflecting the developmental stage of mixed dentition when increased mobility and participation in sports coincide with incomplete motor coordination.
When comparing the time to presentation, the proportion of delayed visits (more than one month, 45.3%) was substantially higher than reported in Jordan (12.5%) [33] and Lebanon (17%) [12], highlighting critical barriers to timely trauma care in Syria. Delayed management likely contributed to the high rates of asymptomatic apical periodontitis (32.1%) and irreversible pulpitis (9%) observed, emphasizing the urgent need for public awareness campaigns on early intervention.
4.3. Sociopolitical and Environmental Context
The results must be interpreted within the broader sociopolitical and environmental context of Syria. More than a decade of conflict has disrupted urban infrastructure, public safety, and access to healthcare. Children’s exposure to unsafe environments—damaged playgrounds, overcrowded housing, and unregulated streets—has increased both accidental and intentional injury risks [23].
Hard flooring materials, such as marble or stone, are widely used in many urban residences in Damascus and may exacerbate the severity of facial and dental trauma following falls. Additionally, decreased parental supervision due to economic hardship, combined with limited access to emergency dental facilities, exacerbates delays in seeking care.
This context helps explain the predominance of home-based injuries (48.9%) and falls (63.7%) as etiological factors. Moreover, adolescents may face increased interpersonal violence, as reflected by a higher proportion of trauma caused by fights among children aged ≥12 years. The compounding effects of conflict, displacement, and reduced access to recreational safety infrastructure likely underline these patterns.
4.4. Clinical Implications
The findings have several implications for pediatric dental practice.
First, the maxillary central incisors were the most frequently injured teeth (68.5%), consistent with their anterior position and limited lip protection. This underscores the importance of early orthodontic and occlusal assessments, especially for children with increased overjet or inadequate lip coverage—conditions consistently associated with TDI risk [18,35].
Second, the inclusion of clinical case presentations in this study highlights the multidisciplinary nature of pediatric trauma management, where orthodontic, restorative, and endodontic interventions are often integrated. Modern regenerative and bioceramic-based techniques, as illustrated in the presented cases, have achieved promising outcomes even in delayed presentations [36], supporting the role of advanced materials (e.g., MTA, Biodentine, BioCeramic Putty) in promoting pulp healing and root development in immature teeth [37]. These developments form part of the continuum of care that Baghdadi [38] highlighted in his 2000 publication, which documented the evolution of materials, concepts, and techniques in the management of traumatic dental injuries (TDIs). The notion of a “biological continuum,” as originally articulated by Baghdadi (2000), underscored the dynamic interaction between injured dental tissues and the materials used for their restoration. The present study advances that concept within the broader Preservation-to-Precision paradigm, where the emphasis shifts from mechanical repair to biologically congruent healing. This theoretical bridge situates traumatic dental injury management along a continuum that begins with tissue preservation, extends through regenerative potential, and culminates in individualized, precision-based care—mirroring the “Rethink, Reform, Rise” (3R) framework guiding modern pediatric dental philosophy.
Third, SHCN children showed a higher mean number of traumatised teeth (2.61 vs. 1.66; p < 0.001). This finding highlights the need for specialized preventive programs and caregiver education that focus on motor coordination, protective devices, and supervised play.
4.5. Preventive and Policy Implications
The high proportion of delayed visits and home-related injuries indicates significant gaps in awareness, emergency response, and intersectoral coordination. Prevention must therefore operate at multiple levels:
- 1.
-
School-based Programs
- ○
- Introduce injury-prevention curricula that include dental first-aid education (e.g., management of avulsed teeth, proper storage media).
- ○
- Teachers and school nurses should receive annual first-responder training, supported by the Ministries of Education and Health.
- 2.
-
Parental and Community Education
- ○
- Launch nationwide awareness campaigns on dental trauma prevention and early care—via television, social media, and community centers.
- ○
- Encourage the use of mouthguards during sports activities and promote safer play environments.
- 3.
-
Health System Strengthening
- ○
- ntegrate dental trauma management protocols within emergency departments and pediatric hospitals.
- ○
- Establish a national TDI registry and reporting system to monitor incidence, guide resource allocation, and evaluate interventions.
- 4.
-
Urban and Infrastructure Planning
- ○
- Advocate for child-safe environments through collaboration between the Ministry of Housing, local municipalities, and NGOs.
- ○
- Encourage the use of shock-absorbent materials (e.g., rubberized flooring) in schools and playgrounds, replacing hard marble or stone surfaces prevalent in Damascus (Syrian) homes.
Such coordinated action can significantly reduce the frequency and severity of TDIs while improving prognosis through prompt care and follow-uAs conflict-affected MENA countries experience breakdowns in infrastructure and systems, heightening children’s exposure to preventable injuries [39], rebuilding child oral-health programs must move beyond emergency repair toward resilience-based models. Aligning prevention with the Rethink-Reform-Rise (3R) philosophy and the Preservation-to-Precision continuum ensures that restorative, educational, and policy efforts evolve together to safeguard children’s health in both post-conflict and recovery settings.
4.6. Limitations
The retrospective and hospital-based nature of this study restricts its generalizability to the broader community, as it only includes children who sought care at a university clinic. Additionally, relying on recorded data may introduce reporting bias or missing variables (e.g., socioeconomic status). Despite these limitations, the large sample size, standardized WHO classification, and excellent inter-examiner reliability (κ = 0.89) ensure strong internal validity. Future prospective and community-based studies are warranted to complement these findings and assess long-term outcomes of TDI management in Syrian children.
4.7. Summary
In summary, this study confirms that TDIs remain a significant but preventable pediatric health issue in Syria. The combination of post-conflict environmental risks, delayed care, and limited public awareness calls for urgent integration of dental trauma prevention into national child health strategies. The multidisciplinary treatment outcomes presented further illustrate that with proper intervention and training, functional and aesthetic recovery can be successfully achieved even in resource-limited settings.
5. Conclusions
This study provides updated institutional data on traumatic dental injuries (TDIs) among Syrian children and adolescents, revealing a prevalence of 11.08%. Males, younger children, and those with a history of previous trauma were at significantly higher risk. Falls within the home environment remained the predominant cause, while maxillary central incisors were the most frequently affected teeth. Delayed presentation—observed in nearly half of all cases—was strongly associated with pulpal and periapical complications, underscoring a critical gap in emergency response and public awareness.
The findings also highlight the increased burden among children with special healthcare needs, who sustained more severe and multiple injuries. These insights necessitate a multifaceted prevention approach that encompasses school safety programs, caregiver education, and structured emergency referral systems.
At the clinical level, the study’s case presentations illustrate the effectiveness of integrated, multidisciplinary management using contemporary biomaterials and regenerative protocols. Such approaches can significantly enhance prognosis, even when the initial presentation is delayed.
Call to Action
Given the post-conflict reconstruction phase in Syria, dental trauma prevention should be embedded within broader child health and safety policies. Collaboration among the Ministries of Health, Education, and Housing, supported by professional bodies such as the Syrian Dental Association and university faculties, is crucial to:
- Establish a national TDI surveillance registry,
- Implement school-based first-aid and mouthguard education programs, and
- Promote safe urban design with shock-absorbent flooring in schools and playgrounds.
By integrating dental trauma management into national child welfare and educational frameworks, Syria can substantially reduce preventable injuries and advance the long-term oral health and quality of life of its youngest generation.
Author Contributions
Y.A.T., M.A. and M.N.A. conceptualized the research idea, screened the clinical records, and contributed to data interpretation, documentation, and manuscript drafting. R.E.M. performed the statistical analyses and assisted in data validation. N.B., M.B.A., and O.A. provided conceptual input, methodological oversight, and academic supervision throughout the project. Z.D.B. led the scientific framing, critical revision, and editorial refinement of the manuscript; ensured methodological and ethical compliance; maintained the continuity and integrity of the study from conception to publication; and provided senior mentorship that shaped its analytical depth and overall excellence in presentation. All authors have read and approved the final version of the manuscript for publication.
Funding
The project was funded by Damascus University (funder No. 501100020595).
Institutional Review Board Statement
The study was conducted in accordance with the guidelines of the Declaration of Helsinki and was approved by the Institutional Review Board of Damascus University (document number 2654, dated 13 February 2023).
Informed Consent Statement
Informed consent was obtained from all parents of the children involved in the study.
Data Availability Statement
The data are available upon request from the authors.
Acknowledgments
The presented article is a part of the PhD study of Yasser Alsayed Tolibah, approved by the IRB, Damascus University College of Dentistry, Damascus, Syria (UDDS-361-13032023/SRC-2654).
Conflicts of Interest
All authors declare no conflict of interest.
References
- Liu, F.; Wu, T.-T.; Lei, G.; Fadlelseed, A.F.A.; Xie, N.; Wang, D.-Y.; Guo, D.Q.-Y. Worldwide tendency and perspectives in traumatic dental injuries: A bibliometric analysis over two decades (1999–2018). Dent. Traumatol. 2020, 36, 489–497. [Google Scholar] [CrossRef]
- Glendor, U. Epidemiology of traumatic dental injuries–a 12-year review of the literature. Dent. Traumatol. 2008, 24, 603–611. [Google Scholar] [CrossRef]
- Petti, S.; Glendor, U.; Andersson, L. World traumatic dental injury prevalence and incidence, a meta-analysis—One billion living people have had traumatic dental injuries. Dent. Traumatol. 2018, 34, 71–86. [Google Scholar] [CrossRef] [PubMed]
- Magno, M.B.; de Paiva Cabral Tristão, S.K.; Jural, L.A.; Aguiar Sales Lima, S.O.; Coqueiro, R.D.S.; Maia, L.C.; Pithon, M.M. Does dental trauma influence the social judgment and motivation to seek dental treatment by children and adolescents? Development, validation, and application of an instrument for the evaluation of traumatic dental injuries and their consequences. Int. J. Paediatr. Dent. 2019, 29, 474–488. [Google Scholar] [CrossRef] [PubMed]
- Verma, S.K.; Jha, A.K.; Prakash, O.; Ekram, S.; Tigga, C.; Noorani, M.K.; Mehta, V.; Meto, A.; Meto, A.; Fiorillo, L.; et al. Impact of dental and orofacial trauma on oral health-related quality of life in adults: A systematic review. Chin. J. Traumatol. 2024, 27, 249–253. [Google Scholar] [CrossRef]
- da Silva, R.L.C.; Dias Ribeiro, A.P.; Almeida, J.C.F.; Sousa, S.J.L.; Garcia, F.C.P. Impact of dental treatment and the severity of traumatic dental injuries on the quality of life of Brazilian schoolchildren. Dent. Traumatol. 2021, 37, 562–567. [Google Scholar] [CrossRef]
- Zengin, A.Z.; Celenk, P.; Sumer, A.P.; Cankaya, S. Evaluation of traumatic dental injuries in a group of Turkish population. Niger. J. Clin. Pract. 2015, 18, 86–89. [Google Scholar] [CrossRef]
- Alshammary, F.; Alhur, T.; Alshammari, K.N.; Siddiqui, A.A.; Abideen, M.Z.U.; Alghaythi, K.S.; Ilyas, M.; Alam, M.K. Prevalence and Risk Factors of Dental Trauma in Ha’il, Saudi Arabia. J. Contemp. Dent. Pract. 2022, 23, 628–633. [Google Scholar]
- Andreasen, J.O.; Andreasen, F.M. Classification, etiology and epidemiology. In Textbook and Color Atlas of Traumatic Injuries to the Teeth, 5th ed.; Wiley Blackwell: Hoboken, NJ, USA, 2019; pp. 252–282. [Google Scholar]
- Magno, M.B.; Nadelman, P.; Leite, K.L.F.; Ferreira, D.M.; Pithon, M.M.; Maia, L.C. Associations and risk factors for dental trauma: A systematic review of systematic reviews. Community Dent. Oral. Epidemiol. 2020, 48, 447–463. [Google Scholar] [CrossRef] [PubMed]
- Tewari, N.; Mathur, V.P.; Siddiqui, I.; Morankar, R.; Verma, A.R.; Pandey, R.M. Prevalence of traumatic dental injuries in India: A systematic review and meta-analysis. Indian J. Dent. Res. 2020, 31, 601–614. [Google Scholar] [CrossRef] [PubMed]
- Abdel Malak, C.; Chakar, C.; Romanos, A.; Rachidi, S. Prevalence and Etiological Factors of Dental Trauma among 12- and 15-Year-Old Schoolchildren of Lebanon: A National Study. ScientificWorldJournal 2021, 2021, 5587431. [Google Scholar] [CrossRef] [PubMed]
- Martin, A.G.; Shivashakarappa, P.G.; Adimoulame, S.; Sundaramurthy, N.; G, E. Prevalence, Etiology, and Risk Factors of Traumatic Dental Injuries in Children with Special Needs of Puducherry. Int. J. Clin. Pediatr. Dent. 2022, 15, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Glendor, U. Aetiology and risk factors related to traumatic dental injuries—A review of the literature. Dent. Traumatol. 2009, 25, 19–31. [Google Scholar] [CrossRef] [PubMed]
- Born, C.D.; Jackson, T.H.; Koroluk, L.D.; Divaris, K. Traumatic dental injuries in preschool-age children: Prevalence and risk factors. Clin. Exp. Dent. Res. 2019, 5, 151–159. [Google Scholar] [CrossRef]
- Council, O. Guideline on management of acute dental trauma. Dent. Traumatol. 2009, 1. [Google Scholar]
- Levin, L.; Day, P.F.; Hicks, L.; O’Connell, A.; Fouad, A.F.; Bourguignon, C.; Abbott, P.V. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: General introduction. Dent. Traumatol. 2020, 36, 309–313. [Google Scholar] [CrossRef]
- Fouad, A.F.; Abbott, P.V.; Tsilingaridis, G.; Cohenca, N.; Lauridsen, E.; Bourguignon, C.; O’Connell, A.; Flores, M.T.; Day, P.F.; Hicks, L.; et al. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 2. Avulsion of permanent teeth. Dent. Traumatol. 2020, 36, 331–342. [Google Scholar] [CrossRef]
- Marcenes, W.; al Beiruti, N.; Tayfour, D.; Issa, S. Epidemiology of traumatic injuries to the permanent incisors of 9-12-year-old schoolchildren in Damascus, Syria. Endod. Dent. Traumatol. 1999, 15, 117–123. [Google Scholar] [CrossRef]
- Alshayeb, L.; Al-Shiekh, M.N.; Dashash, M. Prevalence and Risk Factors of Traumatic Dental Injuries among Conflict-Affected Schoolchildren in Syria (2023–2024). J. Epidemiol. Glob. Health 2025, 15, 1–10. [Google Scholar] [CrossRef]
- Dashash, M.; Omar, K. CRISIS criteria for effective continuous education in traumatic dental injuries during syrian crisis. Am. J. Health Res. 2016, 4, 1–6. [Google Scholar]
- Nagendrababu, V.; Duncan, H.F.; Fouad, A.F.; Kirkevang, L.L.; Parashos, P.; Pigg, M.; Vaeth, M.; Jayaraman, J.; Suresh, N.; Arias, A.; et al. PROBE 2023 guidelines for reporting observational studies in endodontics: A consensus-based development study. Int. Endod. J. 2023, 56, 308–317. [Google Scholar] [CrossRef] [PubMed]
- Organization, W.H. Oral Health Surveys: Basic Methods; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Almonaqel, M.B.; Makieh, R.E. Health status and visit reasons for children attending the Pediatric Dentistry department in damascus university, damascus, Syria: A retrospective study. Saudi Dent. J. 2024, 36, 1025–1030. [Google Scholar] [CrossRef]
- Gill, I.; Mittal, S.; Kumar, T.; Keshav, V. Open Apex and its Management: Review Article. J. Pharm. Bioallied. Sci. 2024, 16 (Suppl. S1), S31–S34. [Google Scholar] [CrossRef] [PubMed]
- Petti, S.; Andreasen, J.O.; Glendor, U.; Andersson, L. NA0D—The new Traumatic Dental Injury classification of the World Health Organization. Dent. Traumatol. 2022, 38, 170–174. [Google Scholar] [CrossRef]
- Habal, W.; Alkattan, R.; Hajeer, M.Y.; Alkhouli, M.; Al-Nerabieah, Z.; Habal, T.; Awawdeh, M. Impact of Syrian Conflict on the Oral Health of Adolescents: A Cross-Sectional Study. Cureus 2024, 16, e54613. [Google Scholar] [CrossRef]
- Petti, S.; Glendor, U.; Andersson, L. World traumatic dental injury prevalence and incidence, a meta-analysis-One billion living people have had traumatic dental injuries. Dent. Traumatol. 2018, 34, 71–86. [Google Scholar] [CrossRef]
- Goswami, M.; Aggarwal, T. Prevalence of Traumatic Dental Injuries among 1- to 14-year-old Children: A Retrospective Study. Int. J. Clin. Pediatr. Dent. 2021, 14, 467–470. [Google Scholar] [CrossRef]
- Eyuboglu, O.; Yilmaz, Y.; Zehir, C.; Sahin, H. A 6-year investigation into types of dental trauma treated in a paediatric dentistry clinic in Eastern Anatolia region, Turkey. Dent. Traumatol. 2009, 25, 110–114. [Google Scholar] [CrossRef]
- Oldin, A.; Lundgren, J.; Nilsson, M.; Norén, J.G.; Robertson, A. Traumatic dental injuries among children aged 0–17 years in the BITA study—A longitudinal Swedish multicenter study. Dent. Traumatol. 2015, 31, 9–17. [Google Scholar] [CrossRef]
- Ogunmayowa, O.; Baker, C. Neighborhood risk factors for sports and recreational injuries: A systematic review of studies applying multilevel modeling techniques. Inj. Epidemiol. 2022, 9, 6. [Google Scholar] [CrossRef] [PubMed]
- ElKarmi, R.F.; Hamdan, M.A.; Rajab, L.D.; Abu-Ghazaleh, S.B.; Sonbol, H.N. Prevalence of traumatic dental injuries and associated factors among preschool children in Amman, Jordan. Dent. Traumatol. 2015, 31, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Agouropoulos, A.; Pavlou, N.; Kotsanti, M.; Gourtsogianni, S.; Tzanetakis, G.; Gizani, S. A 5-year data report of traumatic dental injuries in children and adolescents from a major dental trauma center in Greece. Dent. Traumatol. 2021, 37, 631–638. [Google Scholar] [CrossRef]
- Kramer, P.F.; Pereira, L.M.; Ilha, M.C.; Borges, T.S.; Freitas, M.P.M.; Feldens, C.A. Exploring the impact of malocclusion and dentofacial anomalies on the occurrence of traumatic dental injuries in adolescents. Angle Orthod. 2017, 87, 816–823. [Google Scholar] [CrossRef] [PubMed]
- Alsayed Tolibah, Y.; Bshara, N.; Aljabban, O.; Abbara, M.T.; Alhaji, M.; Almasri, I.A.; Baghdadi, Z.D. Randomized Trial of Bioceramic Apical Barrier Methods in Necrotic Immature Incisors: Effects on Pain, Extrusion, and Procedure Duration. Children 2025, 12, 1423. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Alsayed Tolibah, Y.; Bshara, N.; Abbara, M.T.; Alhaji, M.; Aljabban, O.; Ahmad, I.A.; Baghdadi, Z.D. Root Development Following Bioceramic Material Application in Immature Permanent Teeth: A Case Series With 24-Month Follow-U. Case Rep. Dent. 2025, 2025, 1530438. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Baghdadi, Z.D. Crown fractures: New concepts, materials, and techniques. Compend. Contin. Educ. Dent. 2000, 21, 831 832, 834, 836 passim; quiz 851. [Google Scholar] [PubMed]
- UNICEF Middle East; North Africa Regional Office. Humanitarian Situation Report: Middle East & North Africa (Jan–Dec 2023); UNICEF MENA: Amman, Jordan, 2023; p. 2. [Google Scholar]
Figure 1.
Mean (± SD) number of traumatized teeth by age group (< 6 years, 6–12 years, ≥12 years). The highest mean was observed among children < 6 years (2.34 ± 1.23). Error bars represent standard deviations. p < 0.05 is considered significant.
Figure 1.
Mean (± SD) number of traumatized teeth by age group (< 6 years, 6–12 years, ≥12 years). The highest mean was observed among children < 6 years (2.34 ± 1.23). Error bars represent standard deviations. p < 0.05 is considered significant.
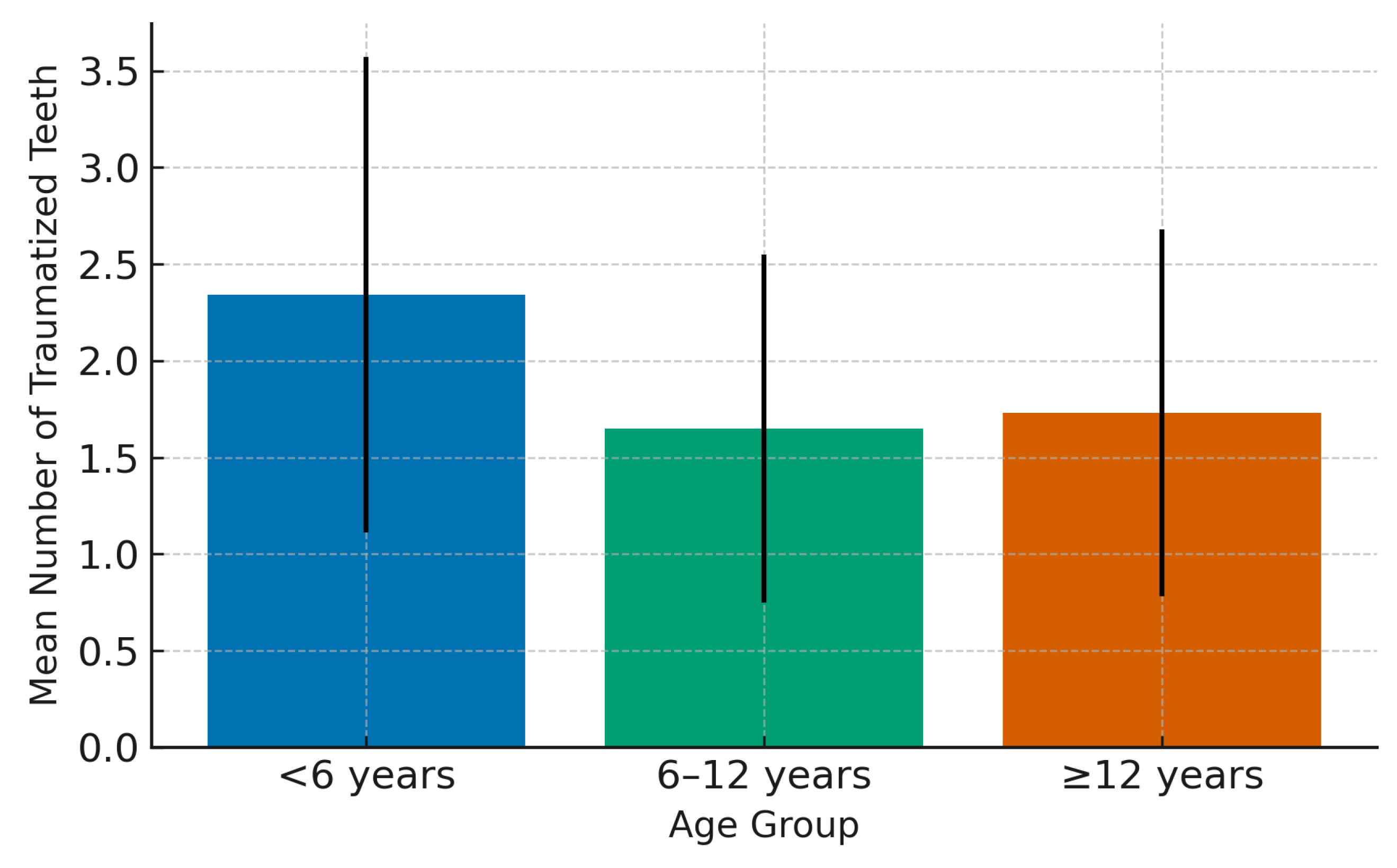
Figure 2.
Relative distribution of etiological causes of TDIs. Falls (63.7%) were the predominant cause, followed by collisions (21.0%), traffic accidents (8.5%), and fights (6.9%). The predominance of falls reflects household environments as the primary setting of injury.
Figure 2.
Relative distribution of etiological causes of TDIs. Falls (63.7%) were the predominant cause, followed by collisions (21.0%), traffic accidents (8.5%), and fights (6.9%). The predominance of falls reflects household environments as the primary setting of injury.
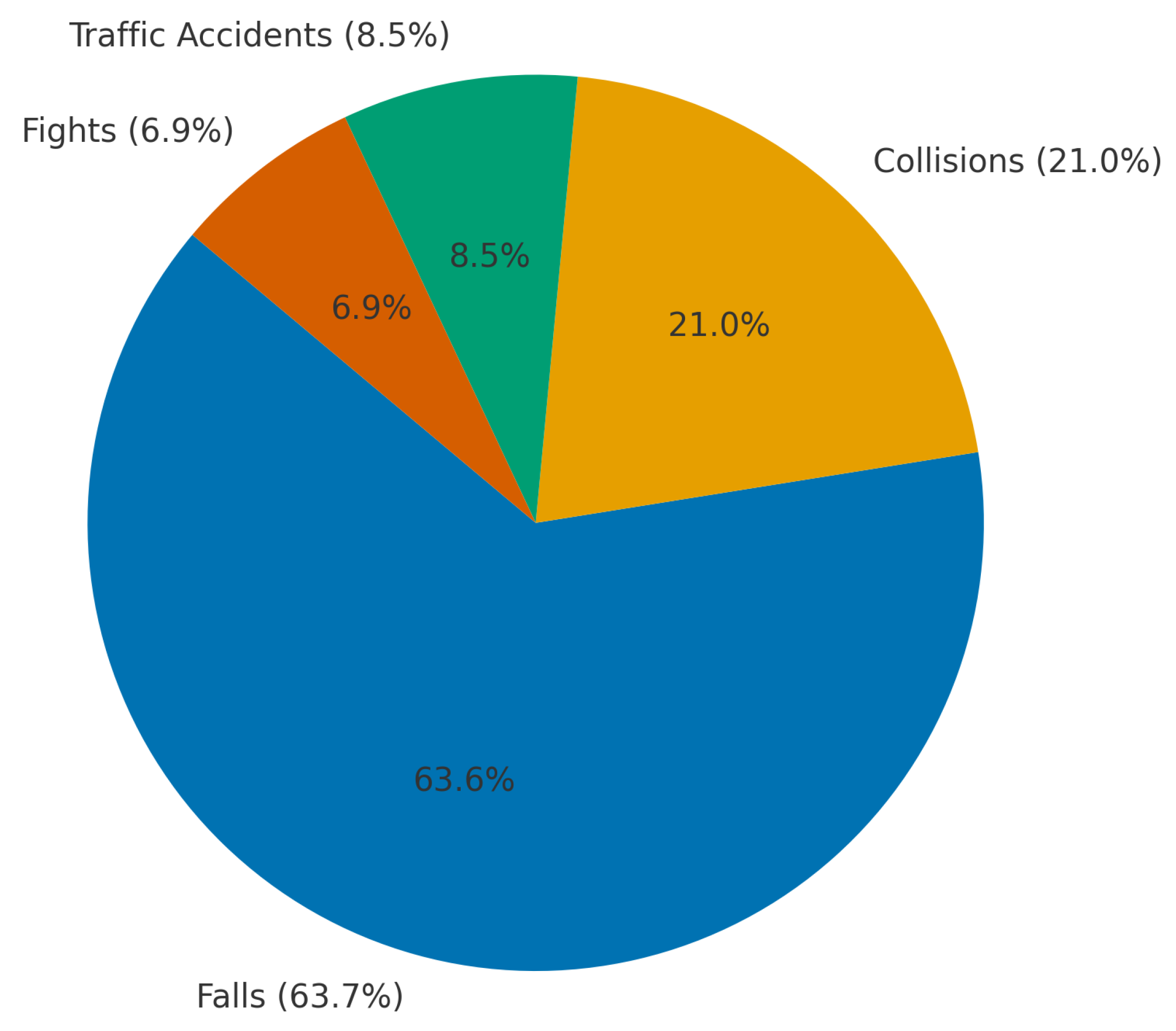
Figure 3.
A case of anterior teeth axis correction using fixed orthodontic treatment to redistribute the space of a missing lateral incisor, followed by replacement with an adhesive bridge: A: Before treatment, B: After appliance placement, C: Completion of orthodontic treatment, D: Adhesive bridge application, and D: the final result.
Figure 3.
A case of anterior teeth axis correction using fixed orthodontic treatment to redistribute the space of a missing lateral incisor, followed by replacement with an adhesive bridge: A: Before treatment, B: After appliance placement, C: Completion of orthodontic treatment, D: Adhesive bridge application, and D: the final result.

Figure 4.
A case of managing a complicated crown fracture with the fractured fragment retained within the lower lip: A: Preoperative view, B: Radiograph showing the location of the broken fragment within the lower lip, C: Surgical removal of the fractured fragment, D: Isolation, endodontic treatment, and reattachment of the broken fragment in a single visit, and E: 6 months follow-up.
Figure 4.
A case of managing a complicated crown fracture with the fractured fragment retained within the lower lip: A: Preoperative view, B: Radiograph showing the location of the broken fragment within the lower lip, C: Surgical removal of the fractured fragment, D: Isolation, endodontic treatment, and reattachment of the broken fragment in a single visit, and E: 6 months follow-up.
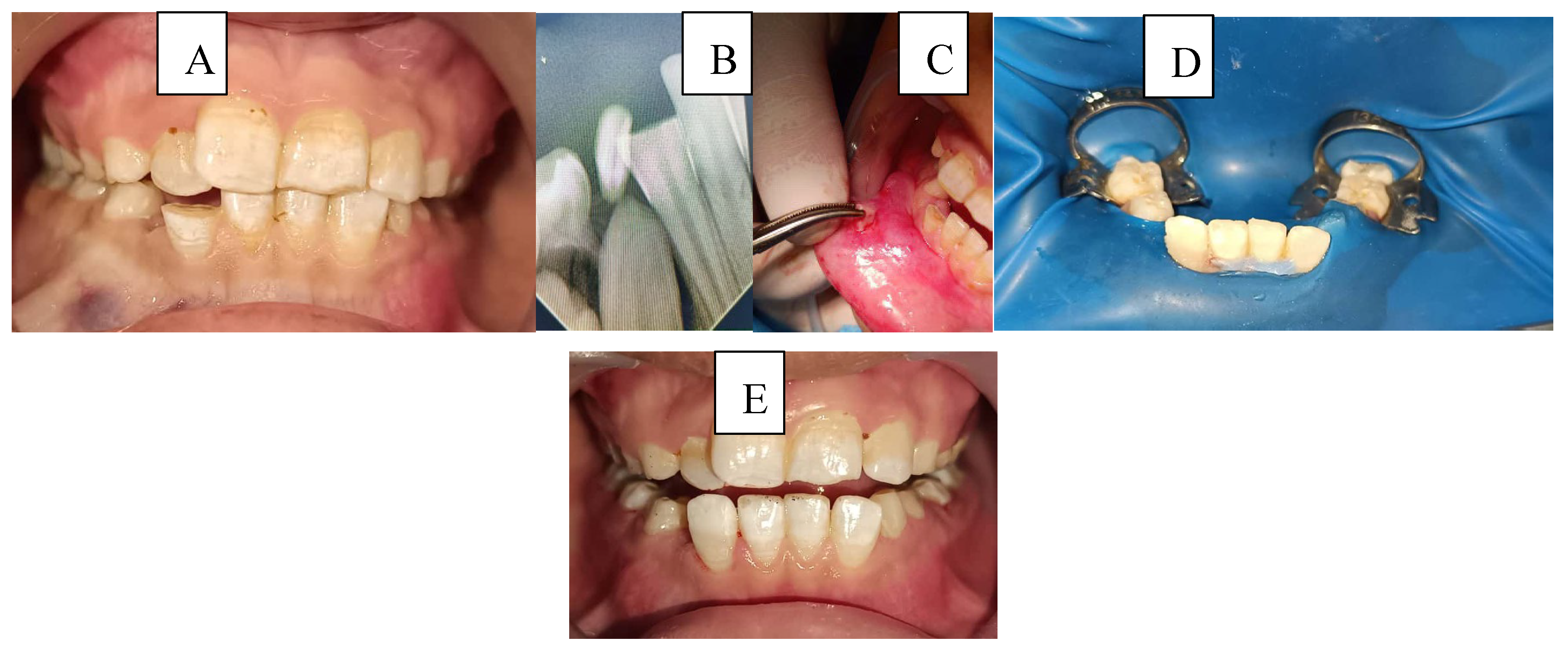
Figure 5.
A case of managing anterior teeth with a history of repeated trauma: A: Diagnostic radiograph, B: Radiograph showing working length determination for tooth #11 and MTA pulpotomy for tooth #21 C: Radiograph showing the placement of MTA apical plug and final restorations, and D: Two-year follow-up radiograph showing successful treatment outcome of tooth #11 and failure of tooth #21.
Figure 5.
A case of managing anterior teeth with a history of repeated trauma: A: Diagnostic radiograph, B: Radiograph showing working length determination for tooth #11 and MTA pulpotomy for tooth #21 C: Radiograph showing the placement of MTA apical plug and final restorations, and D: Two-year follow-up radiograph showing successful treatment outcome of tooth #11 and failure of tooth #21.
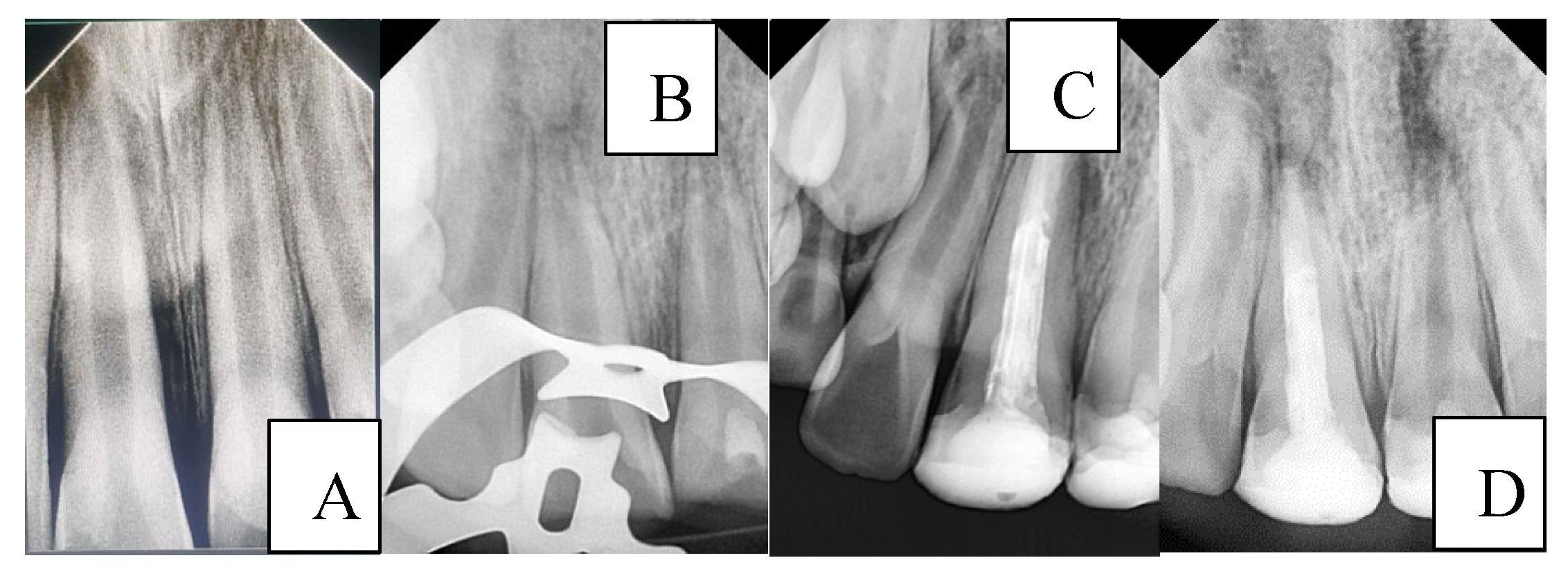

Table 1.
Demographic and behavioural characteristics associated with traumatic dental injuries (TDIs).
Table 1.
Demographic and behavioural characteristics associated with traumatic dental injuries (TDIs).
| Variable | With Injuries (n=301) | No Injuries (n=2415) | TDI Prevalence (%) | p-value |
|---|---|---|---|---|
| Gender (Male/Female) | 213/88 | 1323/1092 | 13.9/7.5 | <0.001 |
| Age group (<6/6–12/≥12) | 32/165/104 | 441/1507/467 | 6.8/8.4/18.2 | <0.001 |
| Health status (Healthy/SHCN) | 273/28 | 2169/246 | 11.8/10.2 | 0.631 |
| Frankl’s behaviour (Neg/Pos) | 104/197 | 1125/1290 | 8.1/17.6 | <0.001 |
| Previous trauma (Yes/No) | 17/284 | 53/2354 | 24.3/10.8 | <0.001 |
| Occlusion (Class I/II/III) | 212/53/6 | 1447/309/146 | 12.8/14.6/4.0 | <0.001 |
| Note: SHCN = special healthcare needs. Bold p-values indicate significant associations (p < 0.05). | ||||
Table 2.
Binary logistic regression analysis for predictors of traumatic dental injuries.
| Predictor Variable | B | SE | Wald | OR (95% CI) | p-value |
|---|---|---|---|---|---|
| Gender (Male) | 0.834 | 0.137 | 37.262 | 2.30 (1.76–3.01) | <0.001 |
| Age (Increasing) | -0.570 | 0.138 | 17.064 | 0.56 (0.43–0.74) | <0.001 |
| Behaviour (Frankl) | -0.140 | 0.090 | 2.415 | 0.87 (0.73–1.04) | 0.120 |
| Previous trauma | 0.017 | 0.120 | 0.019 | 1.02 (0.80–1.29) | 0.889 |
| Angle’s classification | 0.095 | 0.059 | 2.574 | 1.10 (0.98–1.23) | 0.109 |
| Model χ2 = 62.45, p < 0.001; Nagelkerke R2 = 0.118; Hosmer–Lemeshow test p = 0.47; Overall classification accuracy = 78.2%. OR = odds ratio; CI = confidence interval. | |||||
Table 3.
Comparison of mean caries indices (DMFT/dmft) between children with and without TDIs.
| Index | With Injuries (Mean ± SD) | No Injuries (Mean ± SD) | Mean Difference (95% CI) | p-value |
|---|---|---|---|---|
| dmft (Primary) | 1.96 ± 2.15 | 5.92 ± 3.79 | -3.96 (-4.35, --3.57) | <0.001 |
| DMFT (Permanent) | 2.94 ± 2.33 | 5.57 ± 4.00 | -2.63 (-3.05, -2.21) | <0.001 |
| DMFT + dmft (Mixed) | 4.45 ± 2.82 | 5.51 ± 3.44 | -1.06 (-1.45, -0.67) | <0.001 |
Table 4.
Injury characteristics, pulp diagnosis, and treatment modalities among permanent and primary teeth (n = 521).
Table 4.
Injury characteristics, pulp diagnosis, and treatment modalities among permanent and primary teeth (n = 521).
| Variable | Permanent teeth (n = 430) | Primary teeth (n = 91) | Notes/p-value |
|---|---|---|---|
| Apex status—open | 40.1% | – | 40.1% overall open apex rate |
| Most affected teeth | #11 (36.1%), #21 (32.4%) | #51 (5.4%), #61 (5.0%) | — |
| Complicated crown fracture | 39.1% | 9.9% | Most frequent type overall |
| Avulsion | 4.9% | 25.3% | p < 0.001 (primary > permanent) |
| Healthy/Reversible pulpitis | 22.0%/29.6% | 16.4%/6.0% | — |
| Asymptomatic apical periodontitis | 32.1% | 17.9% | — |
| >one month delay | 45.3% | 45.1% | 45% delayed overall |
| Restorations | 26.1% | 1.9% | |
| Re-bonding fractured segment | 1.2% | — | |
| Traditional root canal treatment | 7.7% | 1.7% | |
| Apexogenesis | 7.8% | 0.3% | |
| Apical barrier, Regeneration | 18.3%, 2.7% | — | — |
| Note: Percentages refer to teeth within each dentition grouBold values indicate major categories. p < 0.05 is considered significant. | |||
Table 5.
Statistical tests to study the differences between the following variables: gender, health status, previous traumatic injury, cause, and the age classification in children with TDIs.
Table 5.
Statistical tests to study the differences between the following variables: gender, health status, previous traumatic injury, cause, and the age classification in children with TDIs.
| Variables | Age Classification | p-value | |||||
|---|---|---|---|---|---|---|---|
| <6 | 6–<12 | 12≤ | Total | ||||
| Gender | Male | N | 15 | 121 | 77 | 213 | 0.007 a |
| % of Total | 5.0% | 40.2% | 25.6% | 70.8% | |||
| Female | N | 17 | 44 | 27 | 88 | ||
| % of Total | 5.6% | 14.6% | 9.0% | 29.2% | |||
| Total | N | 32 | 165 | 104 | 301 | ||
| % of Total | 10.6% | 54.8% | 34.6% | 100.0% | |||
| Health status | Healthy | N | 22 | 157 | 94 | 273 | <0.001 a |
| % of Total | 7.3% | 52.2% | 31.2% | 90.7% | |||
| SHCN | N | 10 | 8 | 10 | 28 | ||
| % of Total | 3.3% | 2.7% | 3.3% | 9.3% | |||
| Total | N | 32 | 165 | 104 | 301 | ||
| % of Total | 10.6% | 54.8% | 34.6% | 100.0% | |||
| Previous traumatic injury | No | N | 29 | 160 | 95 | 284 | 0.094 a |
| % of Total | 9.6% | 53.2% | 31.6% | 94.4% | |||
| Yes | N | 3 | 5 | 9 | 17 | ||
| % of Total | 1.0% | 1.7% | 3.0% | 5.6% | |||
| Total | N | 32 | 165 | 104 | 301 | ||
| % of Total | 10.6% | 54.8% | 34.6% | 100.0% | |||
| Cause | Falls | N | 20 | 130 | 60 | 210 | <0.001 a |
| % of Total | 6.7% | 43.3% | 20.0% | 70.0% | |||
| Traffic accident | N | 5 | 5 | 5 | 15 | ||
| % of Total | 1.7% | 1.7% | 1.7% | 5.0% | |||
| Collisions with objects | N | 6 | 27 | 22 | 55 | ||
| % of Total | 2.0% | 9.0% | 7.3% | 18.3% | |||
| Fight | N | 1 | 2 | 17 | 20 | ||
| % of Total | 0.3% | 0.7% | 5.7% | 6.7% | |||
| Total | N | 32 | 164 | 104 | 300 | ||
| % of Total | 10.7% | 54.7% | 34.7% | 100.0% | |||
| |||||||
Table 6.
Statistical tests to study the differences between the following variables: gender, health status, occlusion type, place, and age.
Table 6.
Statistical tests to study the differences between the following variables: gender, health status, occlusion type, place, and age.
| variables | Number of traumatized teeth | p-value | |||
|---|---|---|---|---|---|
| N | Mean | SD | |||
| Gender | Male | 213 | 1.71 | .955 | 0.305 a |
| Female | 88 | 1.84 | 1.027 | ||
| Health status | Healthy | 273 | 1.66 | .918 | <0.001 a |
| SHCN | 28 | 2.61 | 1.133 | ||
| Place | Home | 148 | 1.74 | .897 | 0.469 b |
| Street | 46 | 1.98 | 1.483 | ||
| School | 62 | 1.65 | .812 | ||
| Sport | 19 | 1.79 | .855 | ||
| Garden | 25 | 1.64 | .700 | ||
| Total | 300 | 1.75 | .978 | ||
| Age | <6 | 32 | 2.34 | 1.234 | 0.001 b |
| 6–<12 | 165 | 1.65 | .903 | ||
| 12 ≤ | 104 | 1.73 | .947 | ||
| Total | 301 | 1.75 | .977 | ||
| Cause | Falls | 210 | 1.59 | .760 | <0.001 b |
| Traffic accident | 15 | 2.93 | 1.944 | ||
| Collision with objects | 55 | 2.04 | 1.105 | ||
| Fight | 20 | 1.80 | .894 | ||
| Total | 300 | 1.75 | .978 | ||
| |||||
Table 7.
Post hoc tests for significant differences between the mean number of traumatized teeth and the variables: occlusion type, age, and trauma cause.
Table 7.
Post hoc tests for significant differences between the mean number of traumatized teeth and the variables: occlusion type, age, and trauma cause.
| Age | Mean Difference | Std. Error | p-value a | |
|---|---|---|---|---|
| <6 | 6–<12 | .695 | .185 | .001 |
| 12 ≤ | .613 | .194 | .005 | |
| 6–<12 | 12 ≤ | -.082 | .120 | 1.000 |
| Cause | Mean Difference | Std. Error | p-value a | |
| Falls | Traffic accident | -1.343 | .248 | 0.000 |
| Collisions with objects | -.446 | .141 | 0.010 | |
| Fight | -.210 | .217 | 1.000 | |
| Traffic accident | Collisions with objects | .897 | .270 | 0.006 |
| Fight | 1.133 | .317 | 0.002 | |
| Collisions with objects | Fight | .236 | .242 | 1.000 |
| ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



