Submitted:
06 November 2025
Posted:
11 November 2025
You are already at the latest version
Abstract
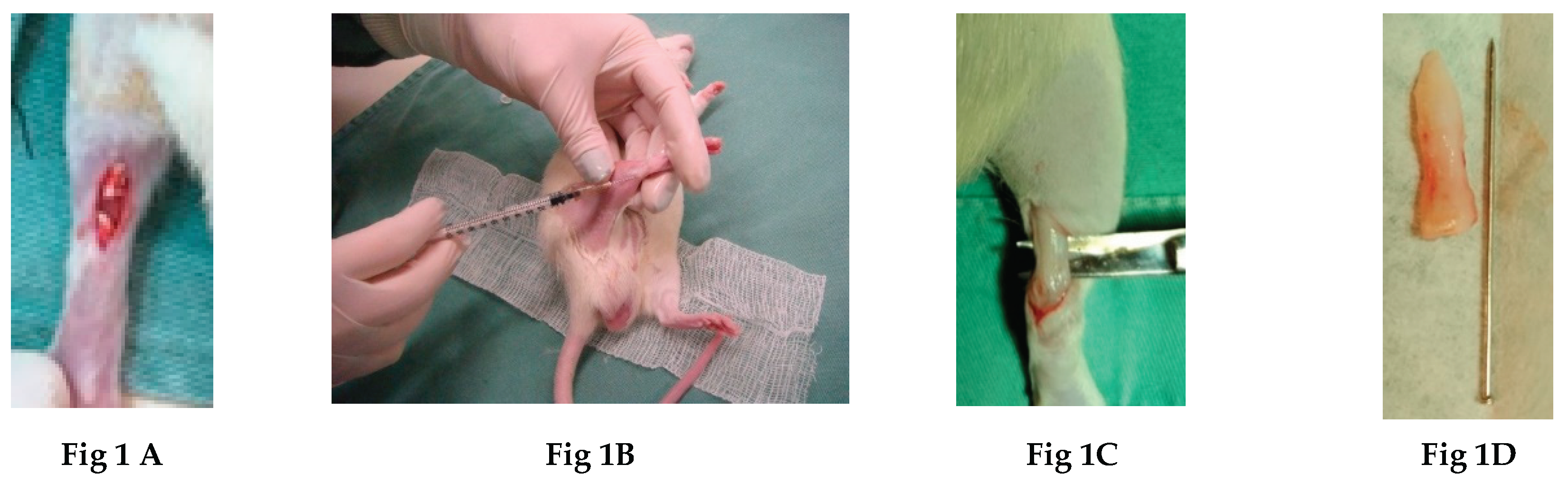
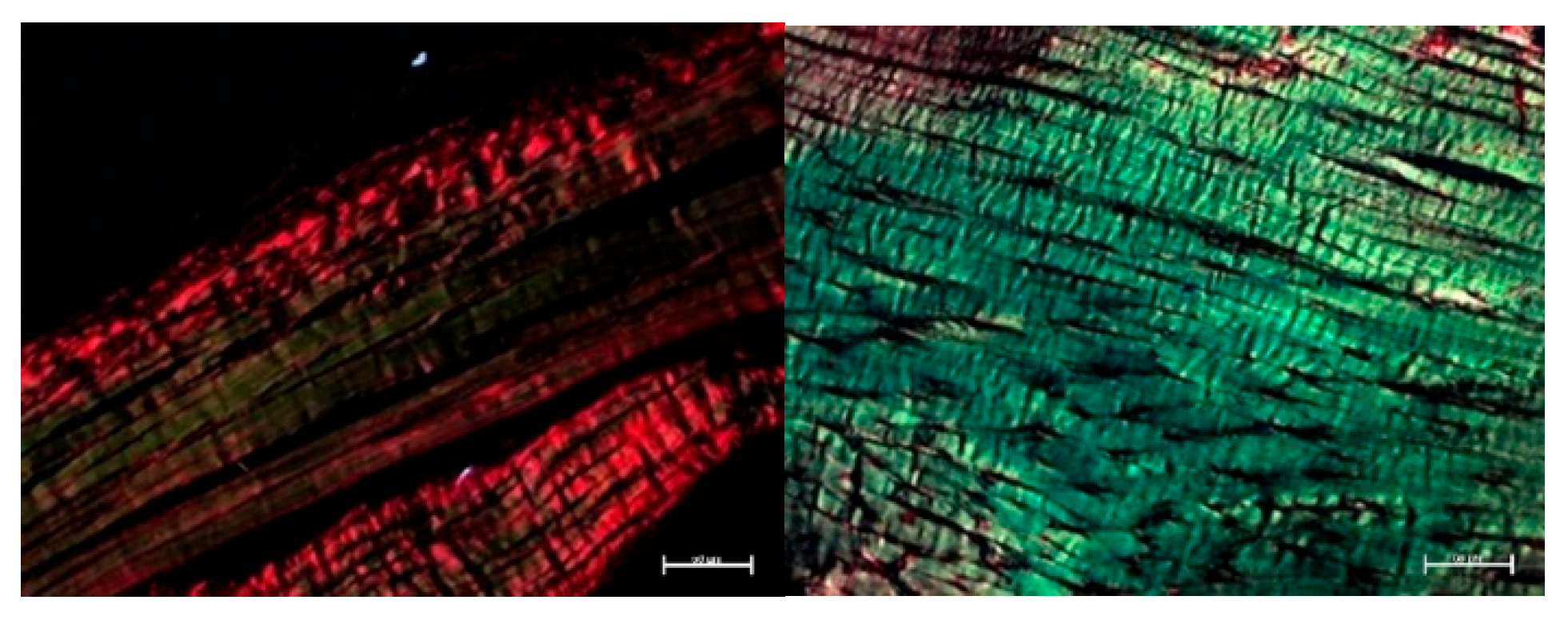
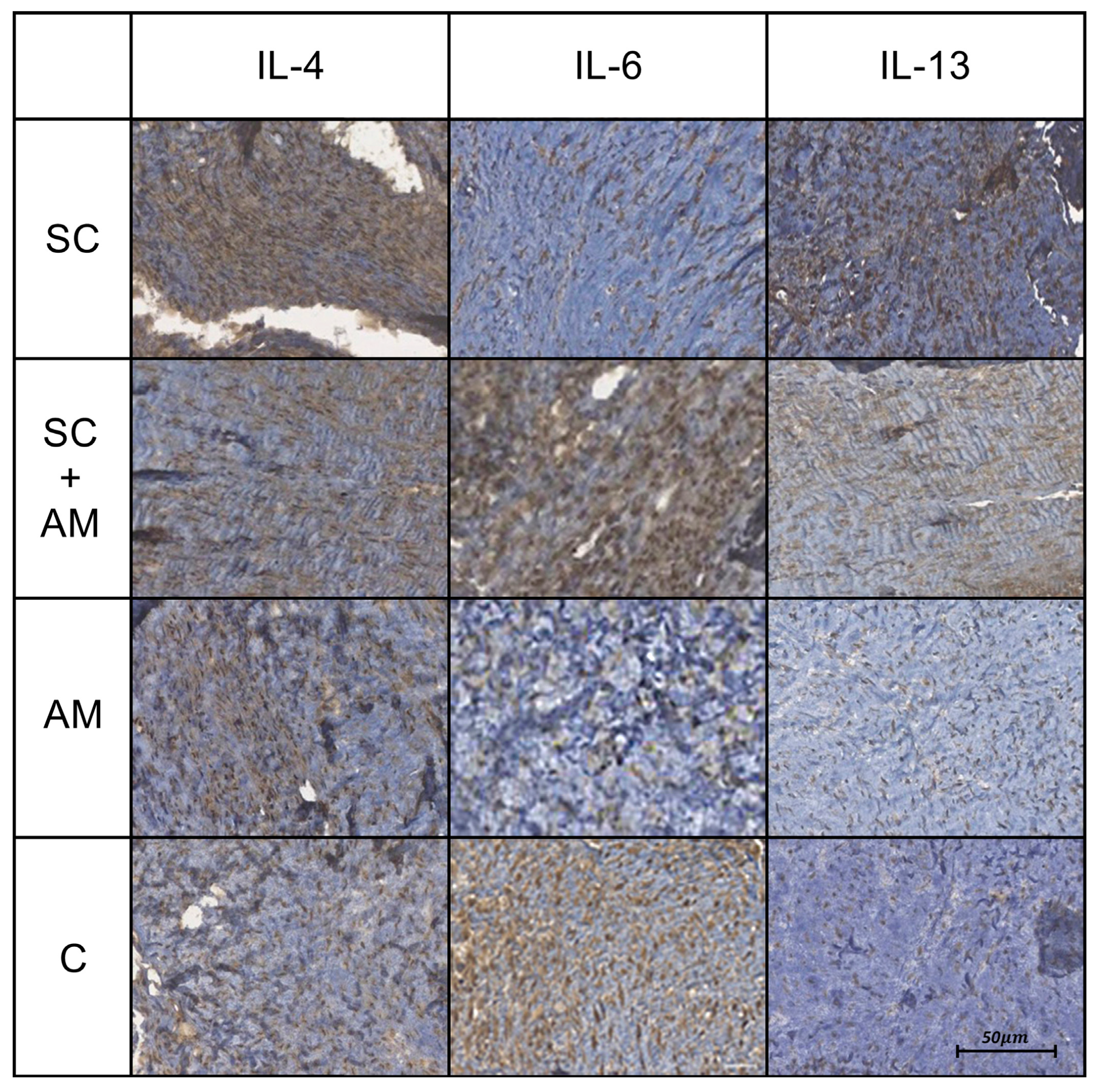
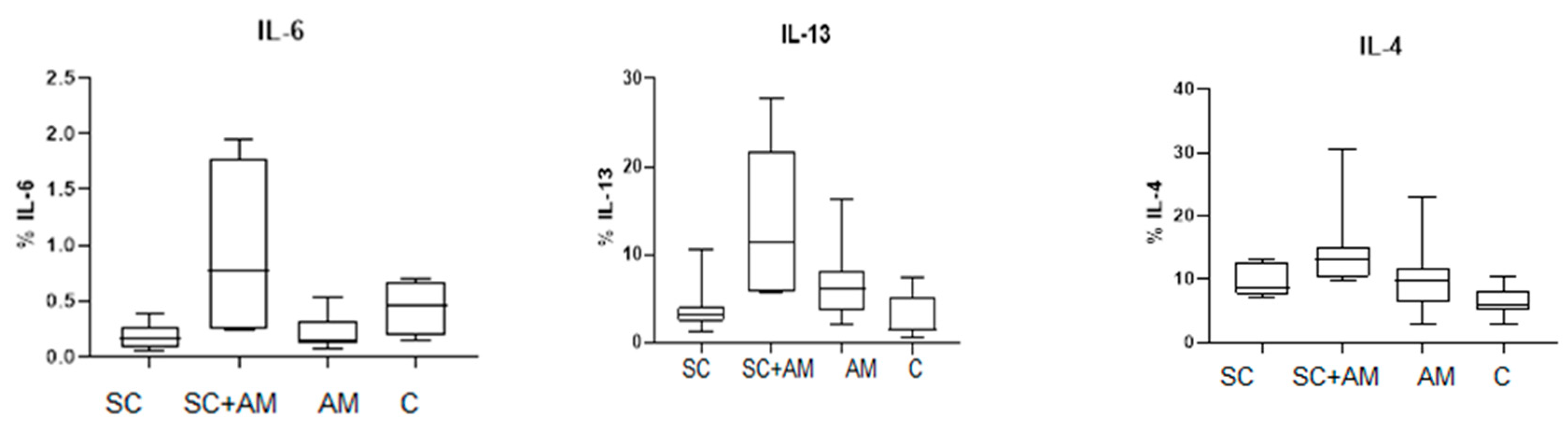
Tendon disorders are common and have a major socio-economic impact. Current treatments (drugs, physiotherapy, surgery) do not provide lasting relief, leading to chronicity and recurrence. In this context, studies on regenerative therapies, such as stem cells, platelet-rich plasma and natural and synthetic membranes, have shown promising results in the treatment of tendon lesions. The present study analyzes the tissue response to a combination of bone marrow mononuclear cells BMMCs) and human decellularized amniotic membrane for treatment of Achilles tendon lesions in rats. Forty male Wistar rats were randomized into four treatment groups: SC (stem cells), AM (amniotic membrane), SC + AM (stem cells + amniotic membrane) and C (control). All underwent Achilles tendon sectioning and tenorrhaphy. In the AM and SC + AM groups, amniotic membrane was sutured over the lesion after the tendon was sutured; in the SC and SC + AM groups, 2 ml of autologous blood from the iliac crest containing BMMCs was applied around the lesion. Group C animals received only 2 ml of 0.9% saline around the lesion. After four weeks, the animals were euthanized, and the tendons were sent for histological analysis (Picrosirius Red) and immunohistochemistry (IL-6, IL-4 and IL-13). Analysis of type I and type III collagen fibers showed no differences between groups. However, the SC + AM group showed a better immunohistochemical profile, with greater expression of IL-4 and IL-13. In this experiment, animals treated with amniotic membrane and autologous stem cells had a better immunohistochemical profile than controls, with increased expression of cytokines associated with tissue repair and organization.
Keywords:
1. Introduction
2. Materials and Methods
- -
- SC group, (BMMCs only;
- -
- AM group, AM only;
- -
- SC + AM group, BMMCs + AM;
- -
- C group (control), 0.9% saline solution.
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
| Grupo | Animal | % Col. type I | % Col. type III |
| SC | 1 | 88,67228 | 11,32772 |
| 2 | 94,68957 | 5,310428 | |
| 3 | 94,67009 | 5,329908 | |
| 4 | 71,99287 | 28,00713 | |
| 5 | 96,78912 | 3,210885 | |
| 6 | 97,76461 | 2,235387 | |
| 7 | 85,19644 | 14,80356 | |
| 8 | 91,76752 | 8,232476 | |
| 9 | 83,73942 | 16,26058 | |
| 10 | 37,24898 | 62,75102 | |
| AM +ST | 1 | 95,25195 | 4,748048 |
| 2 | 75,68604 | 24,31396 | |
| 3 | 83,30736 | 16,69264 | |
| 4 | - | - | |
| 5 | 85,80346 | 14,19654 | |
| 6 | 66,34731 | 33,65269 | |
| 7 | - | - | |
| 8 | 82,80798 | 17,19202 | |
| 9 | 81,30873 | 18,69127 | |
| 10 | 85,55754 | 14,44246 | |
| AM | 1 | 93,74026 | 6,259735 |
| 2 | 84,39343 | 15,60657 | |
| 3 | 82,02189 | 17,97811 | |
| 4 | 80,07587 | 19,92413 | |
| 5 | 90,08762 | 9,91238 | |
| 6 | 87,41478 | 12,58522 | |
| 7 | 73,04669 | 26,95331 | |
| 8 | 66,41677 | 33,58323 | |
| 9 | 55,63869 | 44,36131 | |
| 10 | 89,67368 | 10,32632 | |
| C (Control) | 1 | 68,02493 | 31,97508 |
| 2 | 97,72878 | 2,271217 | |
| 3 | 68,59478 | 31,40522 | |
| 4 | 97,01947 | 2,980529 | |
| 5 | 90,97798 | 9,022016 | |
| 6 | 96,26597 | 3,734033 | |
| 7 | 93,64437 | 6,355624 | |
| 8 | 97,96367 | 2,036329 | |
| 9 | 85,24229 | 14,75771 | |
| 10 | - | - |
Appendix B
| Group | Animal | IL-4 | IL-6 | IL-13 |
| Sc | 1 | 12,6851 | 0,09289 | 1,26152 |
| 2 | 7,08174 | 0,37515 | ||
| 3 | 7,71709 | 2,55785 | ||
| 4 | 8,97251 | 0,05649 | 2,39723 | |
| 5 | 6,95885 | 3,93043 | ||
| 6 | 12,5989 | 0,22803 | 2,54793 | |
| 7 | 7,68494 | |||
| 8 | 12,9734 | 3,78649 | ||
| 9 | 8,27816 | 0,14316 | 10,5361 | |
| 10 | 12,9734 | 0,19234 | 4,18266 | |
| SC + AM | 1 | 13,9265 | 27,8312 | |
| 2 | 13,0249 | 1,93656 | ||
| 3 | 11,5018 | 19,8547 | ||
| 4 | 30,5643 | 0,25865 | 7,75376 | |
| 5 | ||||
| 6 | 10,2099 | 15,0871 | ||
| 7 | 9,64392 | 0,24008 | 5,59404 | |
| 8 | 15,1371 | 1,28579 | 5,70805 | |
| AM | 1 | |||
| 2 | 10,0641 | 0,53462 | 7,75376 | |
| 3 | 6,86066 | 6,01953 | ||
| 4 | 22,988 | 0,30739 | 8,3792 | |
| 5 | 7,11552 | 0,1392 | 4,30523 | |
| 6 | 5,60763 | 0,07892 | 3,03288 | |
| 7 | 13,5096 | 0,16221 | 1,98716 | |
| 8 | 9,81983 | 0,11303 | 7,86464 | |
| 9 | 10,1212 | 0,1319 | 5,00698 | |
| 10 | 2,97585 | 0,32952 | 16,3635 | |
| C | 1 | |||
| 2 | 2,8693 | 0,15288 | 0,51087 | |
| 3 | 7,73207 | 5,13824 | ||
| 4 | 10,5307 | 0,28865 | 1,49216 | |
| 5 | 8,21829 | 0,69733 | 1,19455 | |
| 6 | ||||
| 7 | 6,01073 | 0,63131 | 7,3027 | |
| 8 | 4,98184 | 1,2504 | ||
| 9 | 5,5838 | 2,10399 |
References
- Mafulli, N.; Kader, D. Tendinopathy of Tendo Achillis. J. Bone Joint. Surg. 2002, 84-B, 1–8. [Google Scholar] [CrossRef]
- Christensen, I.B. Rupture of the Achilles tendon: Analysis of 57 cases. Acta Chir. Scand. 1953, 106, 50–60. [Google Scholar]
- Lopez, R.G.L.; Jung, H.-G. Achilles tendinosis: Treatment options. Clin. Orthop. Surg. 2015, 7, 1–7. [Google Scholar] [CrossRef]
- Laffite, C.D.; Soslowski, L.J.; Goff, B. Molecular and structural effects of percutaneous interventions in chronic Achilles tendinopathy. Int. J. Mol. Sci. 2020, 21, 7000. [Google Scholar] [CrossRef]
- Young, M. Stem Cell Applications in Tendon Disorders: A Clinical Perspective; Hindawi Publishing Corporation, Stem Cells International: Washington, DC, USA, 2012. [Google Scholar]
- Yin, Z.; Chen, X.; Chen, J.L.; Ouyang, H.W. Stem cells for tendon tissue engineering and regeneration. Expert Opin. Biol. Ther. 2010, 10, 689–700. [Google Scholar] [CrossRef]
- Awad, H.A.; Butler, D.L.; Boivin, G.P.; Smith, F.N.; Malaviya, P.; Huibregtse, B.; Caplan, A.I. Autologous mesenchymal stem cell-mediated repair of tendon. Tissue Eng. 1999, 5, 267–277. [Google Scholar] [CrossRef]
- Gible, J.; Guilak, F.; Nuttall, M.E.; Sathishkumar, S.; Vidal, M.; Bunnell, B.A. In vitro Differentiation Potential of Mesenchymal Stem Cells. Transfus. Med. Haemother. 2008, 35, 228–238. [Google Scholar] [CrossRef]
- Sachs, B.P.; Stern, C.M. Activity and characterization of a low molecular fraction present in human amniotic fluid with broad-spectrum antibacterial activity. Br. J. Obstet. Gynaecol. 1979, 86, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Werber, B. Amniotic Tissues for the Treatment of Chronic Plantar Fasciitis and Achilles Tendinosis. J. Sports Med. 2015, 2015, 219896. [Google Scholar] [CrossRef] [PubMed]
- Nicodemo, M.C.; Neves, L.R.; Aguiar, J.C.; Brito, F.S.; Ferreira Sant`Anna, L.B.; Raniero, L.J.; Martins, R.A.L.; Barja, P.R.; Arisawa, E.A.L.S. Amniotic membrane as an option for treatment of acute Achilles tendon injury in rats. Acta Cirúrgica Bras./Soc. Bras. Para Desenvolv. Pesqui. Em Cir. 2017, 32, 125–139. [Google Scholar] [CrossRef] [PubMed]
- Oxlund, H.; Helmig, R.; Halaburt, J.; Uldbjerg, N. Biomechanical analysis of human chorioamniotic membranes. Eur. J. Obstet. Gynecol. Reprod. Biol. 1990, 34, 247–255. [Google Scholar] [CrossRef] [PubMed]
- Abetov, D.; Mustapova, Z.; Saliev, T.; Bulanin, D. Biomarkers and signaling pathways of colorectal cancer stem cells. Tumor Biol. 2015, 36, 1339–1353. [Google Scholar] [CrossRef]
- Yuan, F.L.; Hu, W.; Lu, W.G.; Li, X.; Li, J.P.; Xu, R.S.; Li, C.W.; Chen, F.H.; Jin, C. Targeting interleukin-21 in rheumatoid arthritis. Mol. Biol. Rep. 2011, 38, 1717–1721. [Google Scholar] [CrossRef] [PubMed]
- Ellis, M.; Schnabel, L.V.; Berglund, A.K. Defining the profile: Characterizing cytokines in tendon injury to improve clinical therapy. J. Immunol. Regen. Med. 2022, 16, 100059. [Google Scholar] [CrossRef]
- Legerlotz, K.; Jones, E.R.; Screen, H.R.; Riley, G.P. Increased expression of IL-6 family members in tendon pathology. Rheumatology 2012, 51, 1161–1165. [Google Scholar] [CrossRef]
- Andersen, M.B.; Pingel, J.; Kjaer, M.; Langberg, H. Interleukin-6: A growth factor stimulating collagen synthesis in human tendon. J. Appl. Physiol. 2011, 110, 1549–1554. [Google Scholar] [CrossRef]
- Aoudjehane, L.; Pissaia, A., Jr.; Scatton, O.; Podevin, P.; Massault, P.P.; Chouzenoux, S.; Soubrane, O.; Calmus, Y.; Conti, F. Interleukin-4 induces the activation and collagen production of cultured human intrahepatic fibroblasts via the STAT-6 pathway. Mod. Pathol. 2008, 88, 973–985. [Google Scholar] [CrossRef] [PubMed]
- Courneya, J.P.; Luzina, I.G.; Zeller, C.B.; Rasmussen, J.F.; Bocharov, A.; Schon, L.C.; Atamas, S.P. Interleukins 4 and 13 modulate gene expression and promote proliferation of primary human tenocytes. Fibrogenesis Tissue Repair 2010, 3, 9. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Farvind, V.; Huang, A.H. Reparative and Maladaptive Inflammation in Tendon Healing. Front. Bioeng. Biotechnol. 2021, 9, 719047. [Google Scholar] [CrossRef]
- Boyum, A. Separation of lymphocytes, granulocytes, and monocytes from human blood using iodinated density gradient media. Methods Enzymol. 1984, 108, 88–102. [Google Scholar]
- Hopper, R.A. Acellularization of human placenta with preservation of the basement membrane: A potential matrix for tissue engineering. Ann. Plast. Surg. 2003, 51, 598–602. [Google Scholar] [CrossRef]
- Blume, G.G.; Machado-Junior, P.A.B.; Simeoni, R.B.; Bertinato, G.P.; Tonial, M.S.; Nagashima, S.; Pinho, R.A.; de Noronha, L.; Olandoski, M.; de Carvalho, K.A.T.; et al. Bone-Marrow Stem Cells and Acellular Human Amniotic Membrane in a Rat Model of Heart Failure. Life 2021, 11, 958. [Google Scholar] [CrossRef]
- Katsma, M.S.; Patel, S.H.; Eldon, E.; Corbell, K.A.; Shimkus, K.L.; Fluckey, J.D.; Carroll, C.C. The influence of chronic il-6 exposure, in vivo, on rat achilles tendon extracellular matrix. Cytokine 2017, 93, 10–14. [Google Scholar] [CrossRef]
- Chen, S.; Deng, G.; Li, K.; Zheng, H.; Wang, G.; Yu, B.; Zhang, K. Interleukin-6 Promotes Proliferation but Inhibits Tenogenic Differentiation via the Janus Kinase/Signal Transducers and Activators of Transcription 3 (JAK/STAT3) Pathway in Tendon Derived Stem Cells. Med Sci. Monit. 2018, 24, 1567–1573. [Google Scholar] [CrossRef]
- Stauber, T.; Moschini, G.; Hussien, A.A.; Jaeger, P.K.; De Bock, K.; Snedeker, J.G. IL-6 signaling exacerbates hallmarks of chronic tendon disease by stimulating progenitor proliferation & migration to damage. eLife. 2025, 12, RP87092. [Google Scholar] [PubMed]
- Tang, C.; Chen, Y.; Huang, J.; Zhao, K.; Chen, X.; Yin, Z.; Heng, B.C.; Chen, W.; Shen, W. Review article: The roles of inflammatory mediators and immunocytes in tendinopathy. J. Orthop. Transl. 2018, 14, 23–33. [Google Scholar]
- Chisari, E.; Rehak, L.; Khan, W.S.; Maffulli, N. Tendon healing is adversely affected by low-grade inflammation. J. Orthop. Surg. Res. 2021, 16, 700. [Google Scholar] [CrossRef]
- Jiang, L.; Liu, T.; Lyu, K.; Chen, Y.; Lu, J.; Wang, X.; Long, L.; Li, S. Inflammation-related signaling pathways in tendinopathy. Open Life Sci. 2023, 18, 20220729. [Google Scholar] [CrossRef] [PubMed]
- Tony WLin Luis Cardenas David LGlaser Louis, J. Soslowsky, Tendon healing in interleukin-4 and interleukin-6 knockout mice. J. Biomech. 2006, 39, 61–69. [Google Scholar] [CrossRef]
- Nikovics, K.; Favier, A.L.; Rocher, M.; Mayinga, C.; Gomez, J.; Dufour-Gaume, F.; Riccobono, D. In Situ Identification of Both IL-4 and IL-10 Cytokine-Receptor Interactions during Tissue Regeneration. Cells 2023, 12, 1522. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chamberlain, C.S.; Leiferman, E.M.; Frisch, K.E.; Wang, S.; Yang, X.; Brickson, S.L.; Vanderby, R. The influence of interleukin-4 on ligament healing. Wound Repair Regen 2011, 19, 426–435. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gasparini, G.; Cozzani, E.; Parodi, A. Interleukin-4 and interleukin-13 as possible therapeutic targets in systemic sclerosis. Cytokine 2020, 125, 154799. [Google Scholar] [CrossRef] [PubMed]
- Fedato, R.A.; Francisco, J.C.; Sliva, G.; Noronha, L.; Olandoski, M.; Faria Neto, J.R.; Ferreira, P.E.; Simioni, R.B.; Abdelwahid, E.; Carvalho, K.A.T.; et al. Stem Cells and Platelet-Rich Plasma Enhance the Healing Process of Tendinitis in Mice. Gama Res. Artic. 2019, 2019, 1497898. [Google Scholar] [CrossRef] [PubMed]
- Silini, R.; Cargnoni, A.; Magatti, M.; Pianta, S.; Parolini, O. The Long Path of Human Placenta, and its Derivatives, in Regenerative Medicine. Front. Bioeng. Biotechnol. 2015, 3, 162. [Google Scholar] [CrossRef] [PubMed]
- Chopra, A.; Thomas, B.S. Amniotic membrane: A novel material for regeneration and repair. J. Biomim. Biomater. Tissue Eng. 2013, 18, 106–113. [Google Scholar]
- Kim, S.S. Effects of human amniotic membrane grafts combined with marrow mesenchymal stem cells on healing of full-thickness skin defects in rabbits. Cell Tissue Res. 2009, 336, 59–66. [Google Scholar] [CrossRef] [PubMed]


| Group | N | Mean | Standard deviation | Median | Minimum | Maximum | p* | |
|---|---|---|---|---|---|---|---|---|
| Col. I (%) | SC | 10 | 84.3 | 18.2 | 90.2 | 37.2 | 97.8 | |
| SC + AM | 8 | 82.0 | 8.4 | 83.1 | 66.3 | 95.3 | ||
| AM | 10 | 80.3 | 12.0 | 83.2 | 55.6 | 93.7 | ||
| C | 9 | 88.4 | 12.1 | 93.6 | 68.0 | 98.0 | 0.147 | |
| Col. III (%) | SC | 10 | 15.7 | 18.2 | 9.8 | 2.2 | 62.8 | |
| SC + AM | 8 | 18.0 | 8.4 | 16.9 | 4.7 | 33.7 | ||
| AM | 10 | 19.7 | 12.0 | 16.8 | 6.3 | 44.4 | ||
| C | 9 | 11.6 | 12.1 | 6.4 | 2.0 | 32.0 | 0.147 |
| Variable | Group | N |
|---|---|---|
| IL-4 | SC | 10 |
| SC + AM | 7 | |
| AM | 9 | |
| C | 7 | |
| IL-6 | SC | 6 |
| SC + AM | 4 | |
| AM | 8 | |
| C | 4 | |
| IL-13 | SC | 8 |
| SC + AM | 6 | |
| AM | 9 | |
| C | 7 |
| Variable | Group | N | Mean | Standard deviation | Median | Minimum | Maximum | p* |
|---|---|---|---|---|---|---|---|---|
| IL-6 | SC | 6 | 0.18 | 0.11 | 0.17 | 0.06 | 0.38 | |
| SC + AM | 4 | 0.93 | 0.83 | 0.77 | 0.24 | 1.94 | ||
| AM | 8 | 0.22 | 0.15 | 0.15 | 0.08 | 0.53 | ||
| C | 4 | 0.44 | 0.26 | 0.46 | 0.15 | 0.70 | 0.084 | |
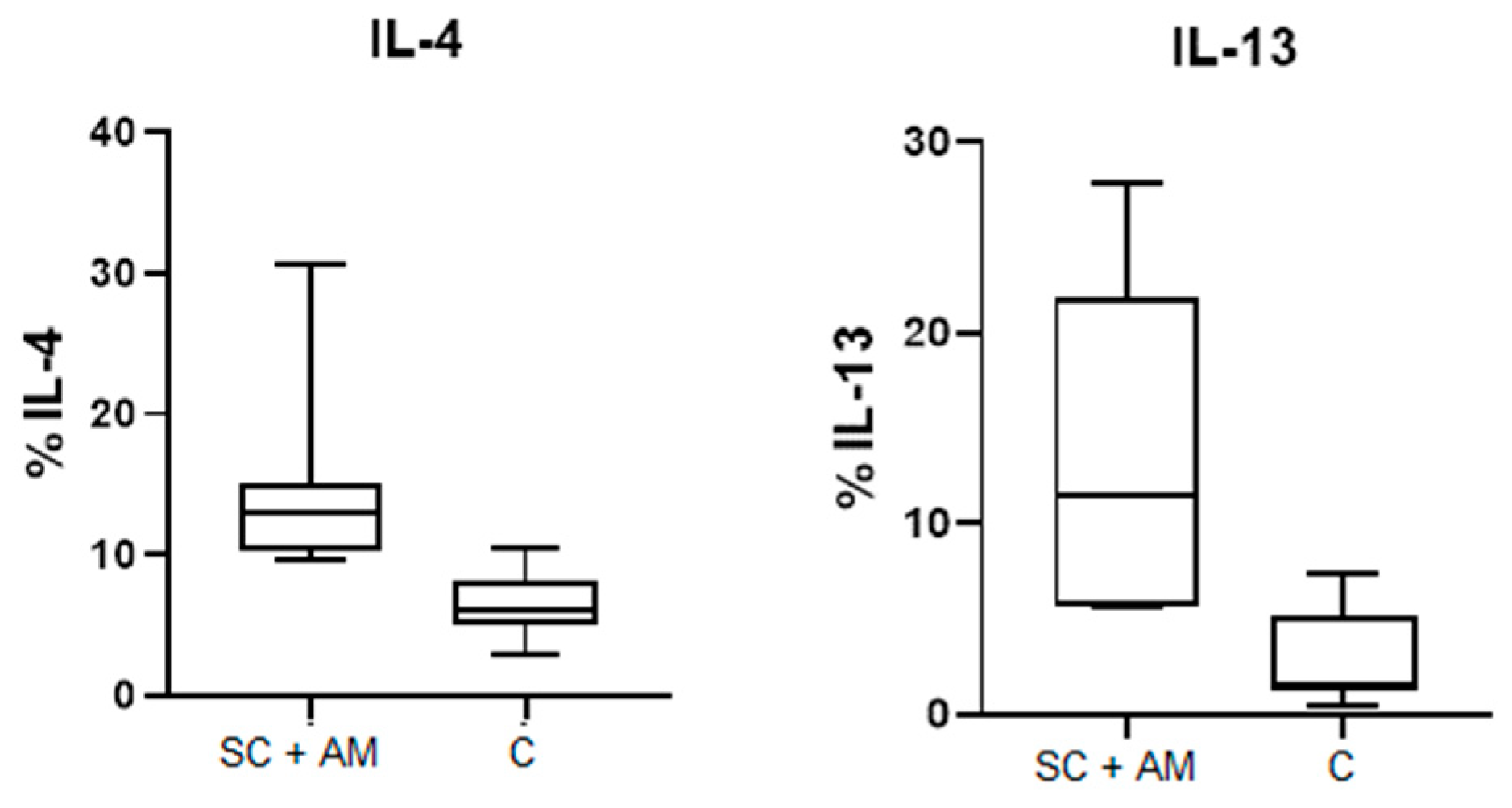
| IL-13 | SC | 8 | 3.9 | 2.9 | 3.2 | 1.3 | 10.5 | |
| SC + AM | 6 | 13.6 | 9.0 | 11.4 | 5.6 | 27.8 | ||
| AM | 9 | 6.8 | 4.2 | 6.0 | 2.0 | 16.4 | ||
| C | 7 | 2.7 | 2.5 | 1.5 | 0.5 | 7.3 | 0.004 | |
| IL-4 | SC | 10 | 9,8 | 2.7 | 8.6 | 7.0 | 13.0 | |
| SC + AM | 7 | 14.9 | 7.2 | 13.0 | 9.6 | 30.6 | ||
| AM | 9 | 9.9 | 5.8 | 9.8 | 3.0 | 23.0 | ||
| C | 7 | 6.6 | 2.5 | 6.0 | 2.9 | 10.5 | 0.011 |
| Compared groups | IL-13 | IL-4 |
|---|---|---|
| SC × C | 1 | 0.489 |
| SC × AM | 0.733 | 1 |
| SC × SC + AM | 0.060 | 0.381 |
| C × AM | 0.101 | 0.985 |
| C × SC + AM | 0.005 | 0.005 |
| AM × SC + AM | 1 | 0.200 |
| Group | Variables analyzed | n | Spearman’s correlation coefficient | p-value |
|---|---|---|---|---|
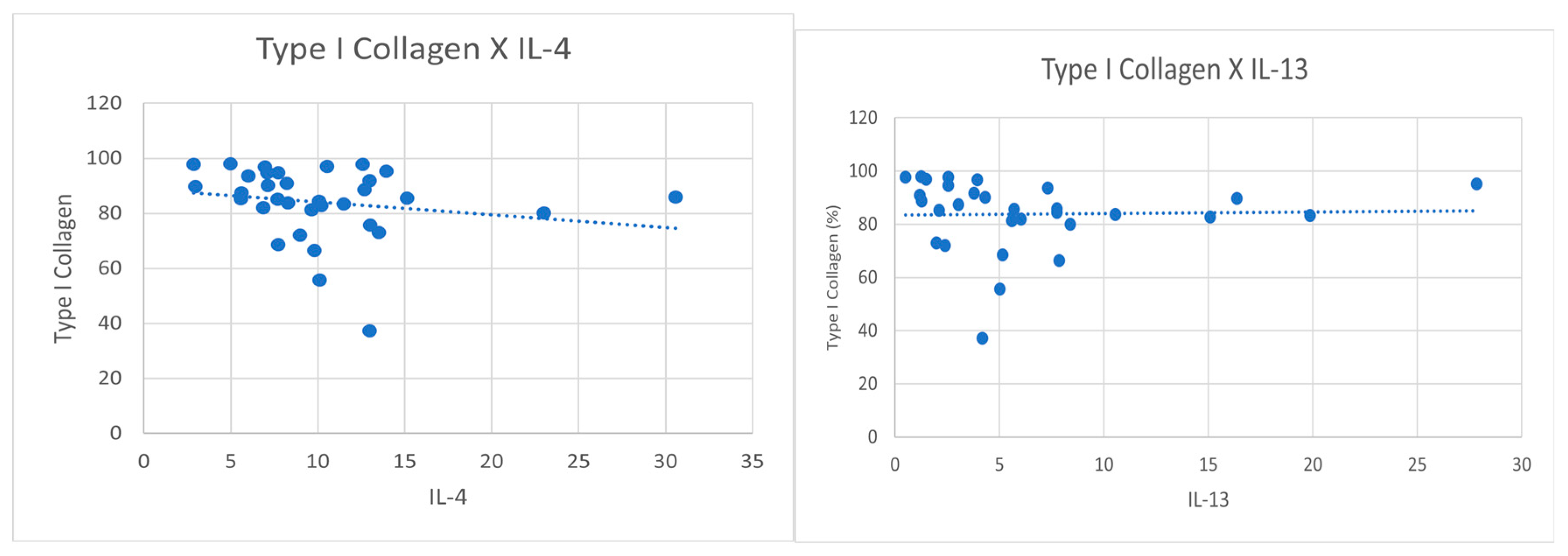
| MA | IL-4 x collagen I (%) | 9 | -0.65 | 0.058 |
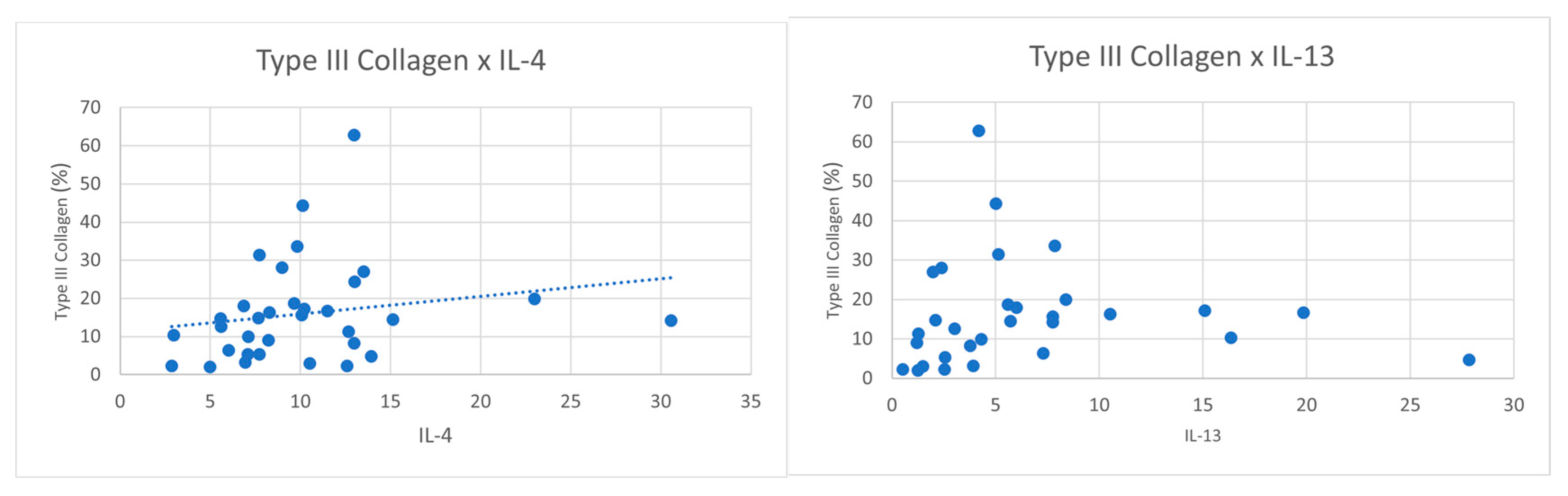
| IL-4 x collagen III (%) | 9 | 0.65 | 0.058 | |
| All | IL-13 x collagen I (%) | 30 | -0.35 | 0.057 |
| IL-13 x collagen III (%) | 30 | 0.35 | 0.057 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



