Submitted:
08 November 2025
Posted:
10 November 2025
You are already at the latest version
Abstract
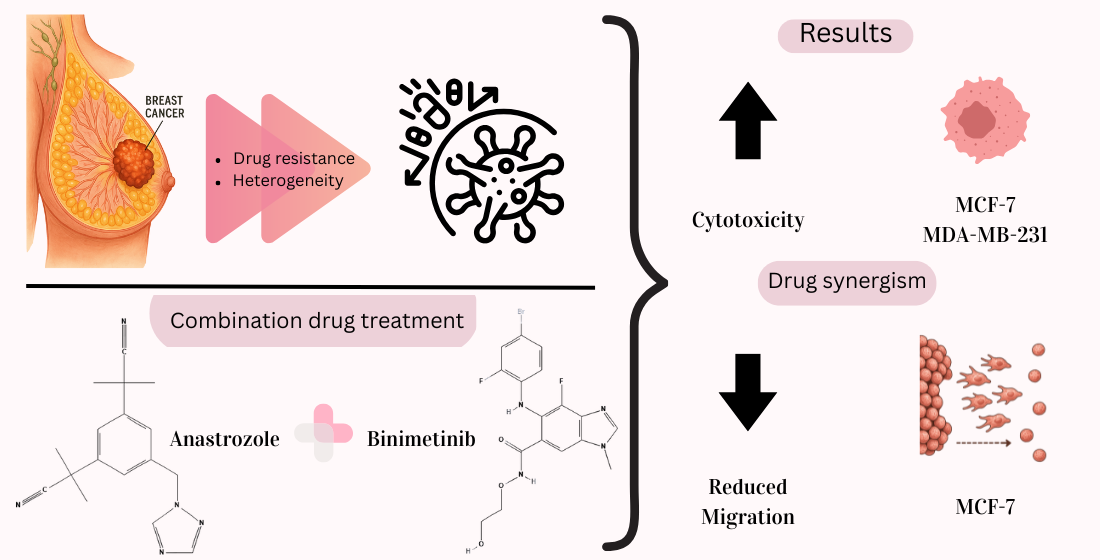
Background and Objectives: Worldwide, breast cancer affects more than 2.3 million women each year, and its treatment has been a challenge in the field of oncology. Its tendency to develop drug resistance, as well as the heterogeneity of the disease, poses a clinical challenge for its eradication. In order to overcome these barriers, this project focused on evaluating the response of breast cancer cells to exposure to an aromatase inhibitor (anastrozole) and a MEK inhibitor (binimetinib) as a combination drug treatment, in terms of their viability and migration. Materials and Methods: The cyto-toxicity of the treatment was evaluated in the 3T3-L1 cell line; viability and migration were evaluated in the MCF-7 and MDA-MB-231 breast cancer cell lines; and a synergy analysis of the combination of drugs was performed. Results: Synergy in cytotoxicity was observed with the combination of drugs at concentrations of 50 μg/mL for anastrozole and 6 μg/mL for binimetinib in MCF-7 and at concentrations of 100 μg/mL for anastrozole and 2 μg/mL for binimetinib in MDA-MB-231. Cytotoxicity was observed in breast cancer cell lines but not in 3T3-L1 fibroblast cells at the selected doses. A significant decrease in cell migration was obtained in the MCF-7 cell line with the combination of drugs compared to the control. Conclusions: In vitro results suggest that both binimetinib and its combination with anastrozole are potential treatments for future studies against hormone receptor-positive breast cancer.
Keywords:
breast cancer
; combinatorial therapies
; aromatase inhibitor
; MEK pathway inhibitor
1. Introduction
Worldwide, breast cancer affects more than 2.3 million women each year, and its treatment has been a challenge in the field of oncology [1]. As biomolecular and clinical research has deepened the understanding of the different characteristics of this disease, it has become increasingly evident that the approach to breast cancer treatment requires a multiple and highly personalized approach due to its diversity [2].
An important aspect to consider is breast cancer's tendency to develop drug resistance as well as the heterogeneity of the disease, since cancer cells constantly adapt to drug therapies, reducing their effectiveness, which presents a clinical challenge for its abatement [3]. One of the major contributors to resistance is the overexpression of ATP-binding cassette (ABC) transporters, such as P-glycoprotein (ABCB1), which actively pump chemotherapeutic agents out of cancer cells, reducing intracellular drug concentration [4]. Current research is focused on overcoming these barriers through combination therapies, targeted inhibitors, and epigenetic modulators to restore drug sensitivity and improve patient outcomes.
For this reason, combinatorial therapies have emerged as a potential treatment for this disease. These therapies involve the simultaneous administration of multiple drugs in a complementary manner. The importance of combinatorial therapies lies in their ability to avoid drug resistance, maximize efficacy, and personalize treatment, using the benefits of multiple therapies as an advantage. This strategy offers a promising option to improve patient prognosis [5]. For instance, the combination of endocrine therapy with CDK4/6 inhibitors has significantly improved progression-free survival in hormone receptor-positive (HR+) breast cancer by preventing cell cycle progression [6]. In HER2-positive breast cancer, using trastuzumab and pertuzumab, along with chemotherapy, has shown superior outcomes compared to single-agent HER2-targeted therapy [7].
One potential disadvantage of combining drugs to treat breast cancer is the increased risk of toxicity and adverse side effects due to overlapping mechanisms of action. However, these challenges can be mitigated through optimized dosing strategies, biomarker-guided patient selection, and supportive care measures.
This project sought to evaluate the response of breast cancer cells to the exposure of an aromatase inhibitor and a MEK inhibitor as a combinatorial drug treatment, in terms of their survival and migration. In vitro evidence of their efficacy represents a key guideline for developing a new therapy with the previously mentioned benefits of a combinatorial treatment.
2. Materials and Methods
2.1. Drugs
Anastrozole (a) and binimetinib (b) were purchased from Sigma-Aldrich (A2736; SML3385). Both drugs were resuspended in DMSO.
2.2. Cell Culture
The following cell lines were cultured: 3T3-L1 fibroblast cells, MCF-7 breast cancer cells (estrogen receptors) (donation Dr. Angelina Rodríguez Torres, School of Natural Sciences UAQ) and MDA-MB-231 breast cancer cells (triple negative) (donation Dr. Brenda Anguiano, Institute of Neurobiology UNAM) in DMEM medium (Dulbecco's Modified Eagle Medium, Gibco-L0093-500) supplemented with 10% fetal bovine serum (GIBCO-26140-079) and 1% penicillin-streptomycin (Caisson-PSL01) (ATCC, 2023). The cells were incubated at 37°C and 5% CO2.
2.3. Cytotoxicity Assay
Using an MTT (3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazole bromide) assay, cytotoxicity evaluation was carried out on the 3T3 cell line, with anastrozole treatment at concentrations of 100, 200, 300, 400 and 500 µg/mL, with binimetinib treatment at concentrations of 0.44, 2.2, 4.4, 8.8, 10 µg/mL and with the combination of anastrozole (a) and binimetinib (b) at concentrations of 50 µg/mL of anastrozole + 6 µg/mL of binimetinib (50a+6b), and 100 µg/mL of anastrozole + 2 µg/mL of binimetinib (100a+2b). In a 96-well plate, 8,000 cells per well were grown for 24 h to reach 80% confluence. After this time, the supplementation medium was removed, and the drugs were added at different concentrations; the cells were incubated for 48 h. Later, the cells were washed with 100 µL of PBS per well, after that 10 µL of MTT reagent and 100 µL of medium were added per well, and incubated for 4 h at 37°C. After this period, the MTT was removed with the medium, and 100 µL of DMSO was added per well. The plate was incubated for 10 min at 37°C protected from light, and absorbance was read in a spectrophotometer at 570 nm.
To evaluate the cytotoxicity on MCF-7 and MDA-MB-231 cell lines, the cells were treated with anastrozole at concentrations of 50, 100, 150, 200, 300 µg/mL; with binimetinib at concentrations of 2, 4, 6, 8, 10 µg/mL; and with the combination of anastrozole (a) and binimetinib (b) at concentrations of 50 µg/mL of anastrozole + 6 µg/mL of binimetinib (50a+6b), 50 µg/mL of anastrozole + 10 µg/mL of binimetinib (50a+10b), 100 µg/mL of anastrozole + 2 µg/mL of binimetinib (100a+2b), 100 µg/mL of anastrozole + 6 µg/mL of binimetinib (100a+6b), 100 µg/mL of anastrozole + 10 µg/mL of binimetinib (100a+10b), 200 µg/mL of anastrozole + 6 µg/mL of binimetinib (200a+6b); combinations based on the responses obtained from the evaluation of individual drugs. All concentrations of anastrozole and binimetinib had a final concentration of 1% DMSO in culture medium.
2.4. Migration Assay
Using a wound assay, migration evaluation was carried out in MCF-7 cell line with anastrozole at concentration of 50 µg/mL, binimetinib at concentration of 6 µg/mL, and the combination of both drugs concentrations; MDA-MB-231 cell line was treated with anastrozole at concentration of 100 µg/mL, with binimetinib at concentration of 2 µg/mL and with the combination of both drugs concentrations. All concentrations of anastrozole and binimetinib had a final concentration of 1% DMSO in culture medium.
In a 6-well plate, 400,000 MCF-7 cells and 500,000 MDA-MB-231 cells were grown for 24 h at 80% confluence. Three wounds per well were made, using a 200 µL micropipette tip. Each wound was measured at different points at 0 h, 6 h, 12 h, and 24 h.
2.5. Statistical Analysis
The statistical analysis of tis work was performer with the GraphPad Prism6® program using one-way analysis of variance (ANOVA) followed by the Tukey post hoc test (p<0.0
3. Results
3.1. Cell Cytotoxicity (MTT)
In 3T3-L1 cells, cell viability decreased as the dose of anastrozole was increased, with a minimum viability percentage of 64% at the highest dose (500 µg/mL) (Figure 1). In contrast, the lowest viability percentage for 3T3-L1 cells treated with binimetinib was 91% at a concentration of 4.4 µg/mL (Figure 2).
The results of the individual drug evaluation indicate higher cytotoxicity with anastrozole. Instead, evaluating the synergic combination treatment, viability remains high and exceeding 100%, indicating an absence of over cytotoxicity and a possible compensatory proliferative effect (Figure 3).
After 48 h exposure to anastrozole (a), binimetinib (b), or their combinations, MCF-7 cells showed a consistent, moderate reduction in viability across doses, with all combinations remaining below 80% of control (Figure 4A). In contrast, MDA-MB-231 cells exhibited a smaller decrement, with most combinations ranging between 80–90% viability; the exceptions were 100a+10b and 100a+2b, which fell below 80% (Figure 4B). No clear dose–response trend was observed.
3.2. Drug–Drug Interaction (Combination Index)
Drug interaction was quantified using the Combination Index (CI; CompuSyn; Chou–Talalay model). In MCF-7 cells (Figure 5A), 50a+6b was synergistic (CI = 0.82796), 100a+2b was borderline additive (CI = 0.99869), and higher-dose pairs were antagonistic (200a+6b, CI = 1.27568; 100a+10b, CI = 1.54273; 100a+6b, CI = 1.13934; 50a+10b, CI = 1.60385). In MDA-MB-231 cells (Figure 5B), synergy was detected at 100a+2b (CI = 0.79897), whereas all other tested combinations were antagonistic (200a+6b, CI = 3.16859; 100a+10b, CI = 1.27197; 100a+6b, CI = 2.83590; 50a+10b, CI = 3.96390; 50a+6b, CI = 1.96763). Values above CI=2 are not shown in the combination index plot as they exceed the limits plotted. Where a CI < 1 indicates a synergistic effect, CI = 1 indicates an additive effect, and CI > 1 indicates an antagonistic effect.
3.3. Cell Migration by Wound-Healing Assay
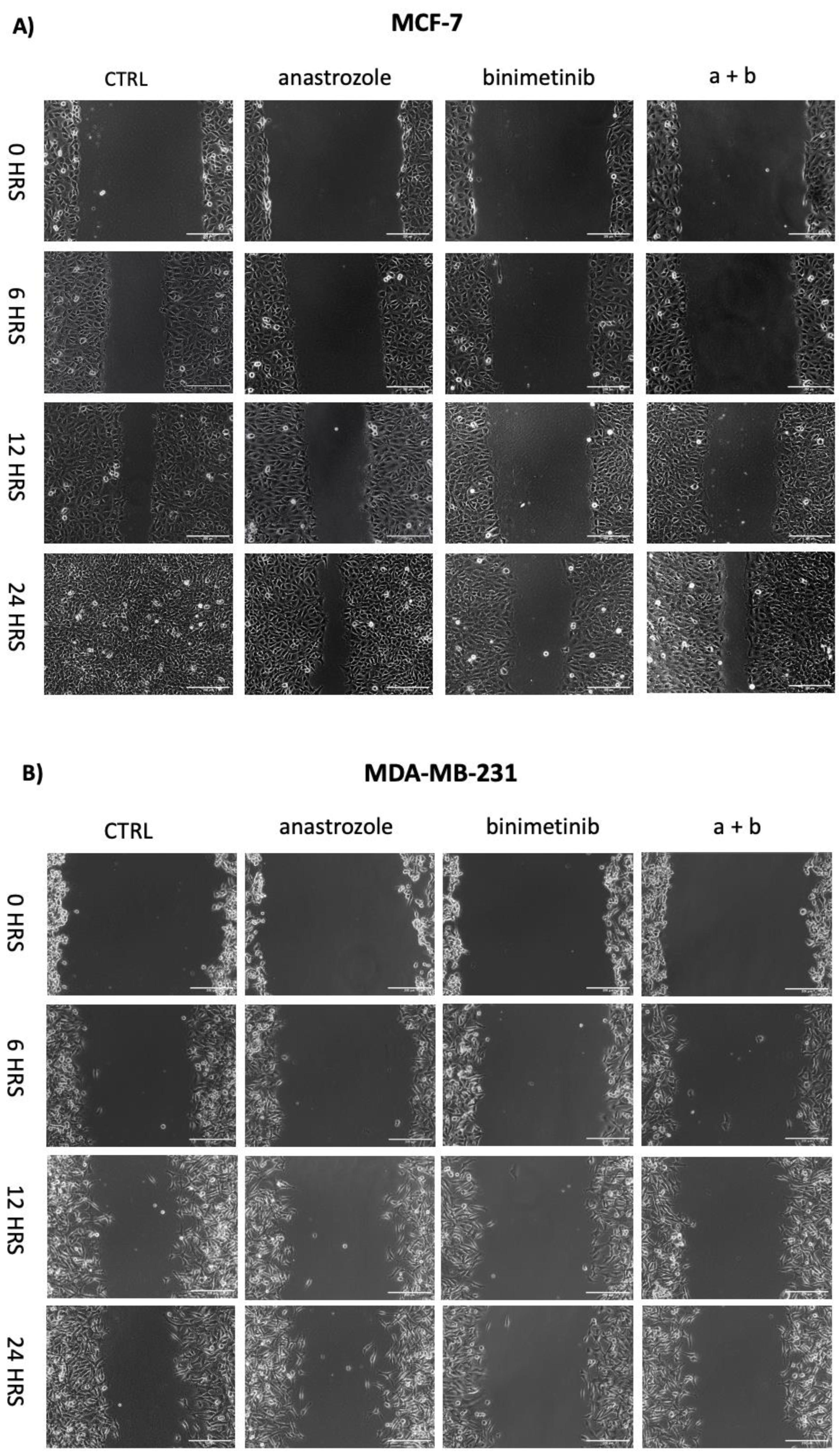
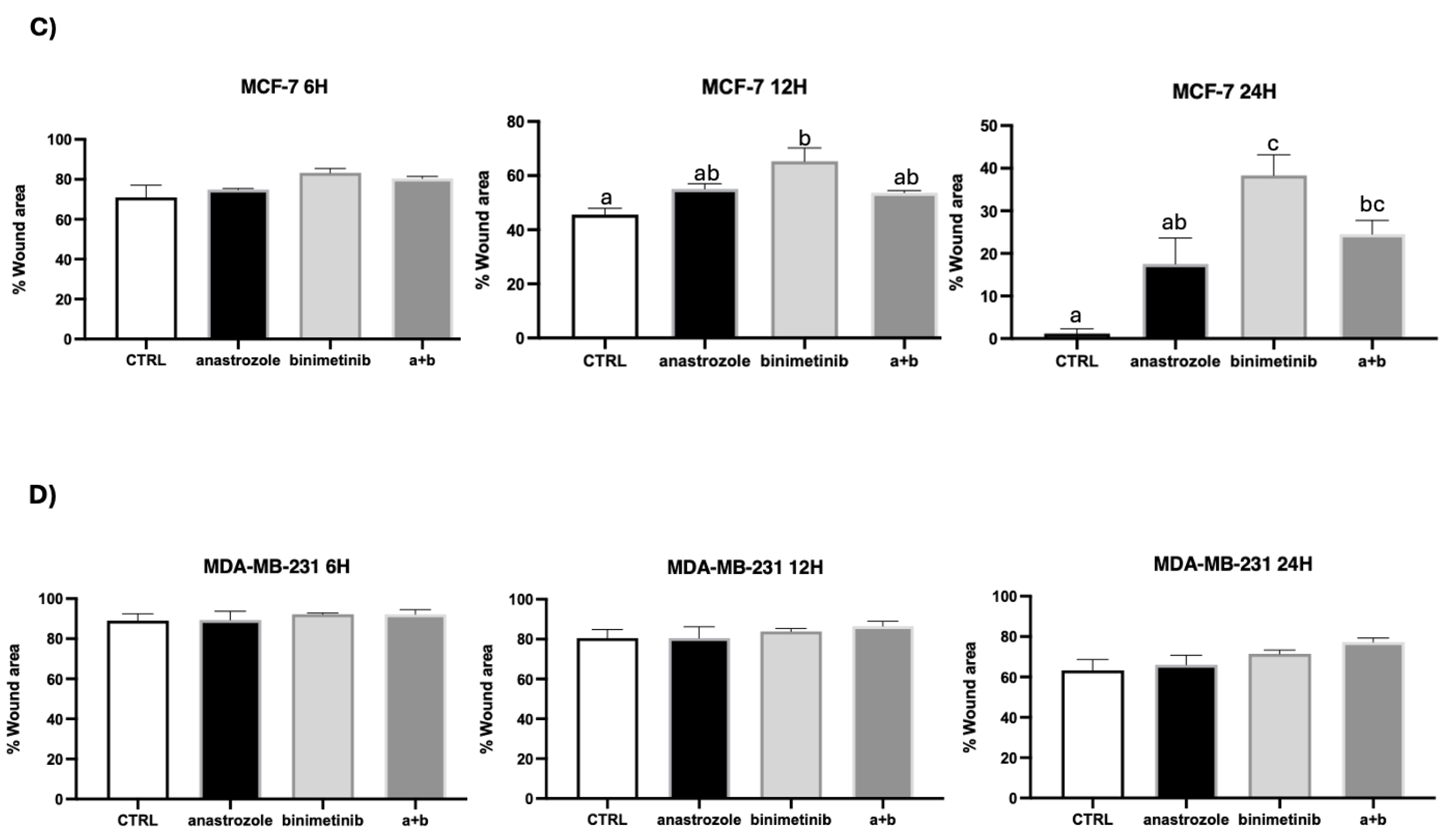
Wound closure was quantified as the percentage of uncovered area at 0, 6, 12, and 24 h using ImageJ. In MCF-7 cells (Figure 6A, Figure 6C), differences were minimal and not statis-tically significant at 6 h; by 12 h, all treatments increased the percentage of wound (re-duced closure) versus control, with binimetinib showing a significant effect. At 24 h, the control monolayer was nearly closed, while binimetinib maintained the largest and sta-tistically significant inhibition versus control; the combination anastrozole + binimetinib (a+b) and individual treatment with anastrozole (a) also reduced closure but to a lesser magnitude, with anastrozole reaching significance only relative to binimetinib. In MDA-MB-231 cells (Figure 6B, Figure 6D), wound closure was similar across groups at all-time points; the combination showed a slight trend toward reduced closure, but no statistically significant differences versus control were detected for anastrozole, binimetinib, or the combination.
Figure 1.
Cytotoxicity of anastrozole in the 3T3-L1 cell line. Evaluation of the cytotoxic effect of anastrozole at concentrations of: 100, 200, 300, 400, 500 µg/mL in the 3T3-L1 cell line after 48 hours of treatment. Data are presented as mean ± standard error (n=3). One-way ANOVA analysis with Tukey's post-hoc analysis.
Figure 1.
Cytotoxicity of anastrozole in the 3T3-L1 cell line. Evaluation of the cytotoxic effect of anastrozole at concentrations of: 100, 200, 300, 400, 500 µg/mL in the 3T3-L1 cell line after 48 hours of treatment. Data are presented as mean ± standard error (n=3). One-way ANOVA analysis with Tukey's post-hoc analysis.
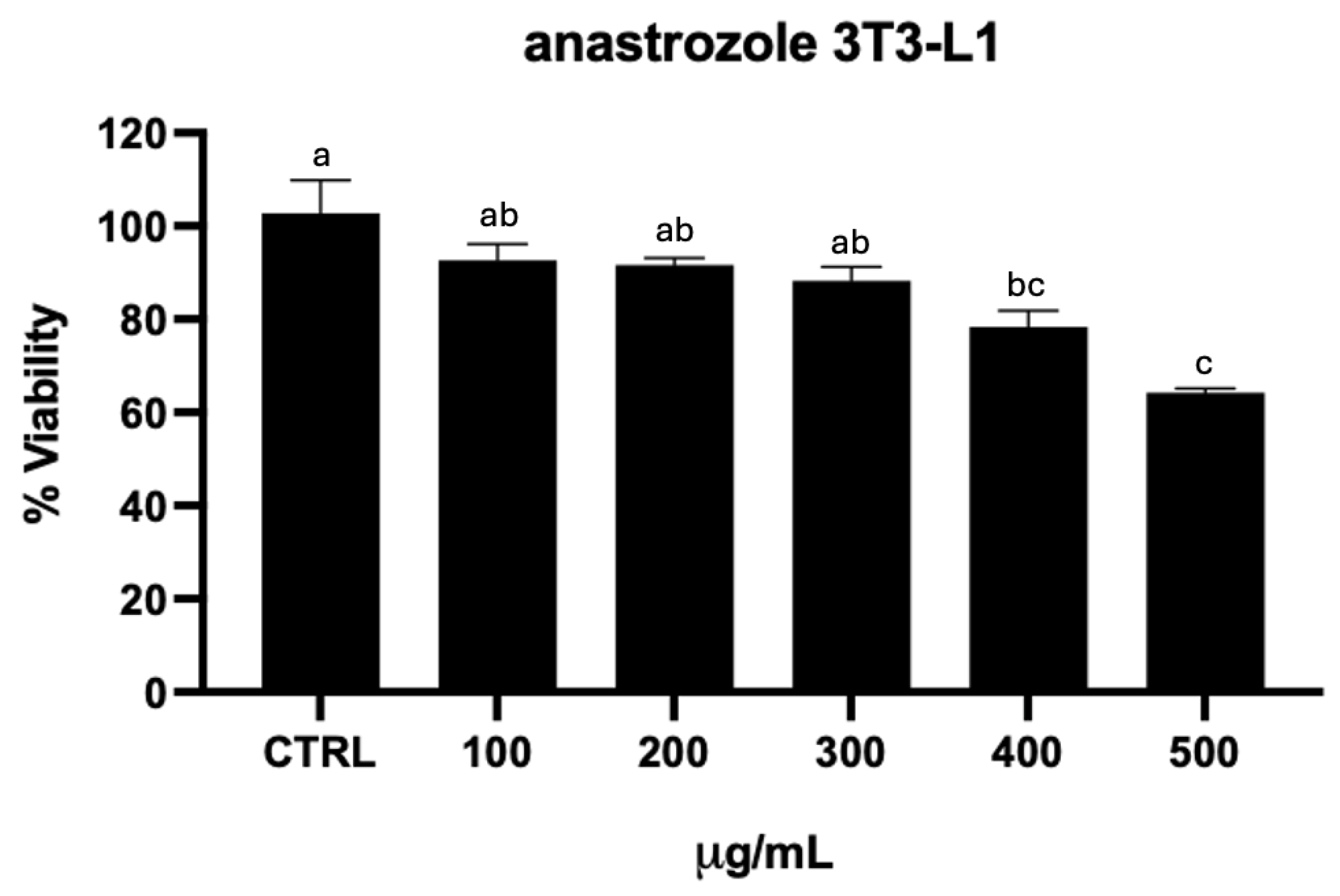
Figure 2.
Cytotoxicity of binimetinib in the 3T3-L1 cell line. Evaluation of the cytotoxic effect of binimetinib at concentrations of: 0.44, 2.2, 4.4, 8.8, 10 µg/mL in the 3T3-L1 cell line after 48 hours of treatment. Data are presented as mean ± standard error (n=3). One-way ANOVA analysis with Tukey's post-hoc analysis.
Figure 2.
Cytotoxicity of binimetinib in the 3T3-L1 cell line. Evaluation of the cytotoxic effect of binimetinib at concentrations of: 0.44, 2.2, 4.4, 8.8, 10 µg/mL in the 3T3-L1 cell line after 48 hours of treatment. Data are presented as mean ± standard error (n=3). One-way ANOVA analysis with Tukey's post-hoc analysis.
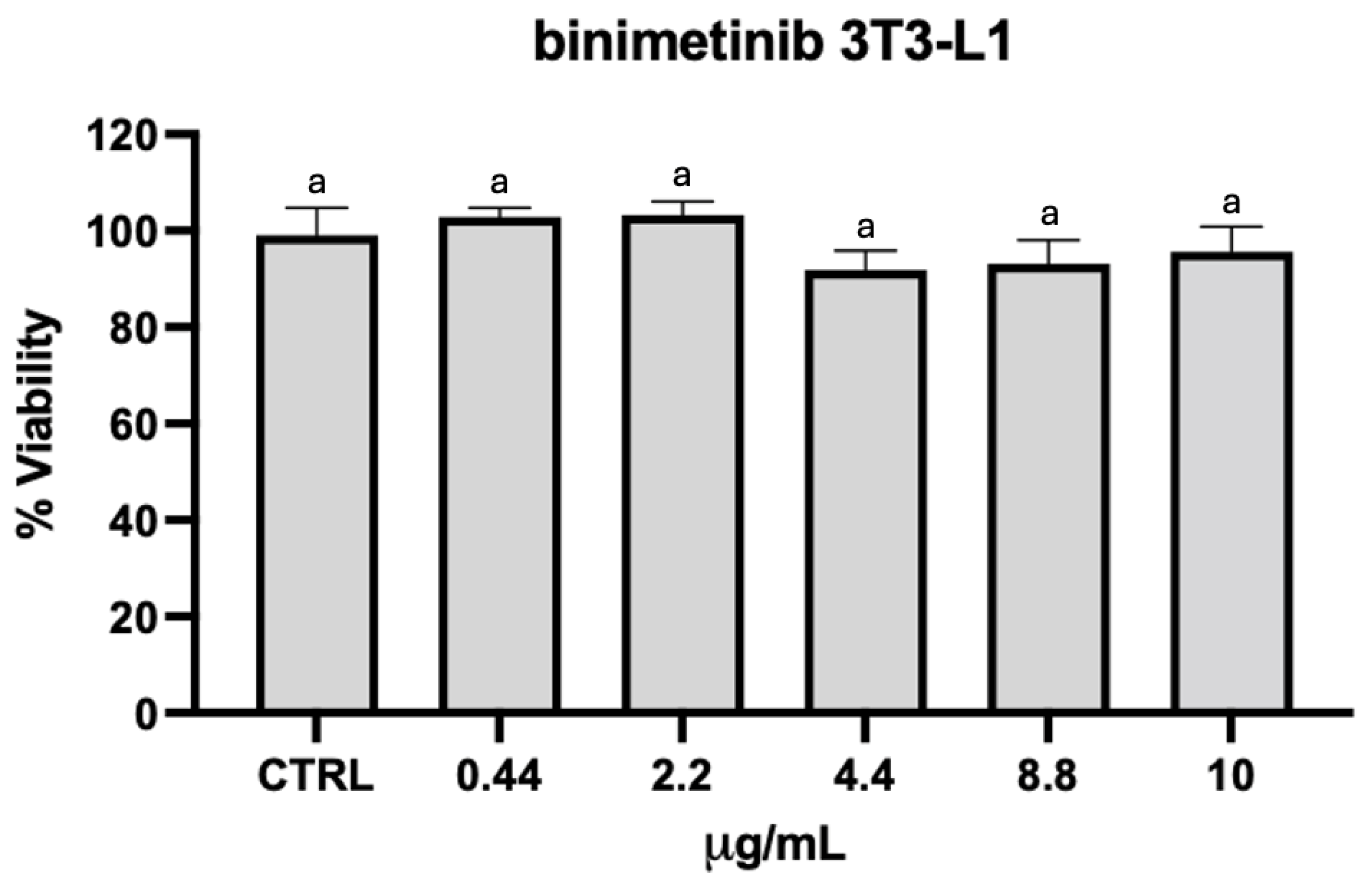
Figure 3.
Cytotoxicity of the synergic drug combination in the 3T3-L1 cell line. Evaluation of the cytotoxic effect of the synergic combination treatment of anastrozole and binimetinib at concentrations of: 50 µg/mL of anastrozole + 6 µg/mL of binimetinib (50a+6b), based on MCF-7 synergic results, and 100 µg/mL of anastrozole + 2 µg/mL of binimetinib (100a+2b), based on MDA-MB-231 synergic results; in the 3T3-L1 cell line after 48 hours of treatment. Data are presented as mean ± standard error (n=3).
Figure 3.
Cytotoxicity of the synergic drug combination in the 3T3-L1 cell line. Evaluation of the cytotoxic effect of the synergic combination treatment of anastrozole and binimetinib at concentrations of: 50 µg/mL of anastrozole + 6 µg/mL of binimetinib (50a+6b), based on MCF-7 synergic results, and 100 µg/mL of anastrozole + 2 µg/mL of binimetinib (100a+2b), based on MDA-MB-231 synergic results; in the 3T3-L1 cell line after 48 hours of treatment. Data are presented as mean ± standard error (n=3).
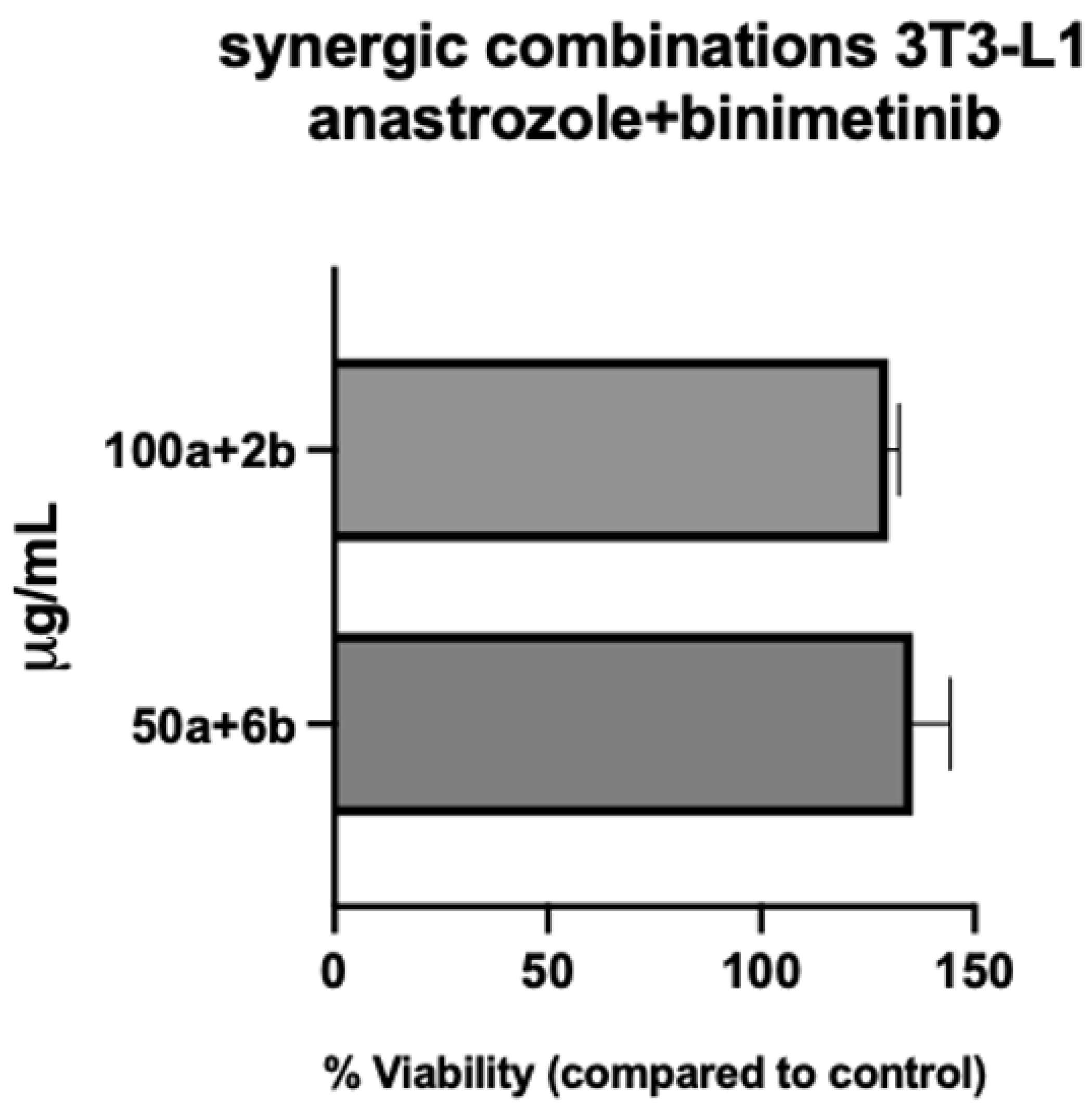
Figure 4.
Cell viability assessment in cancer cells treated with anastrozole and binimetinib. A) MCF-7 and B) MDA-MB-231 cells were treated for 48 hours with anastrozole, binimetinib and its combination at different concentrations (µg/mL), and cell viability was assessed using an MTT assay. Data are presented as mean ± standard error (n=3).
Figure 4.
Cell viability assessment in cancer cells treated with anastrozole and binimetinib. A) MCF-7 and B) MDA-MB-231 cells were treated for 48 hours with anastrozole, binimetinib and its combination at different concentrations (µg/mL), and cell viability was assessed using an MTT assay. Data are presented as mean ± standard error (n=3).
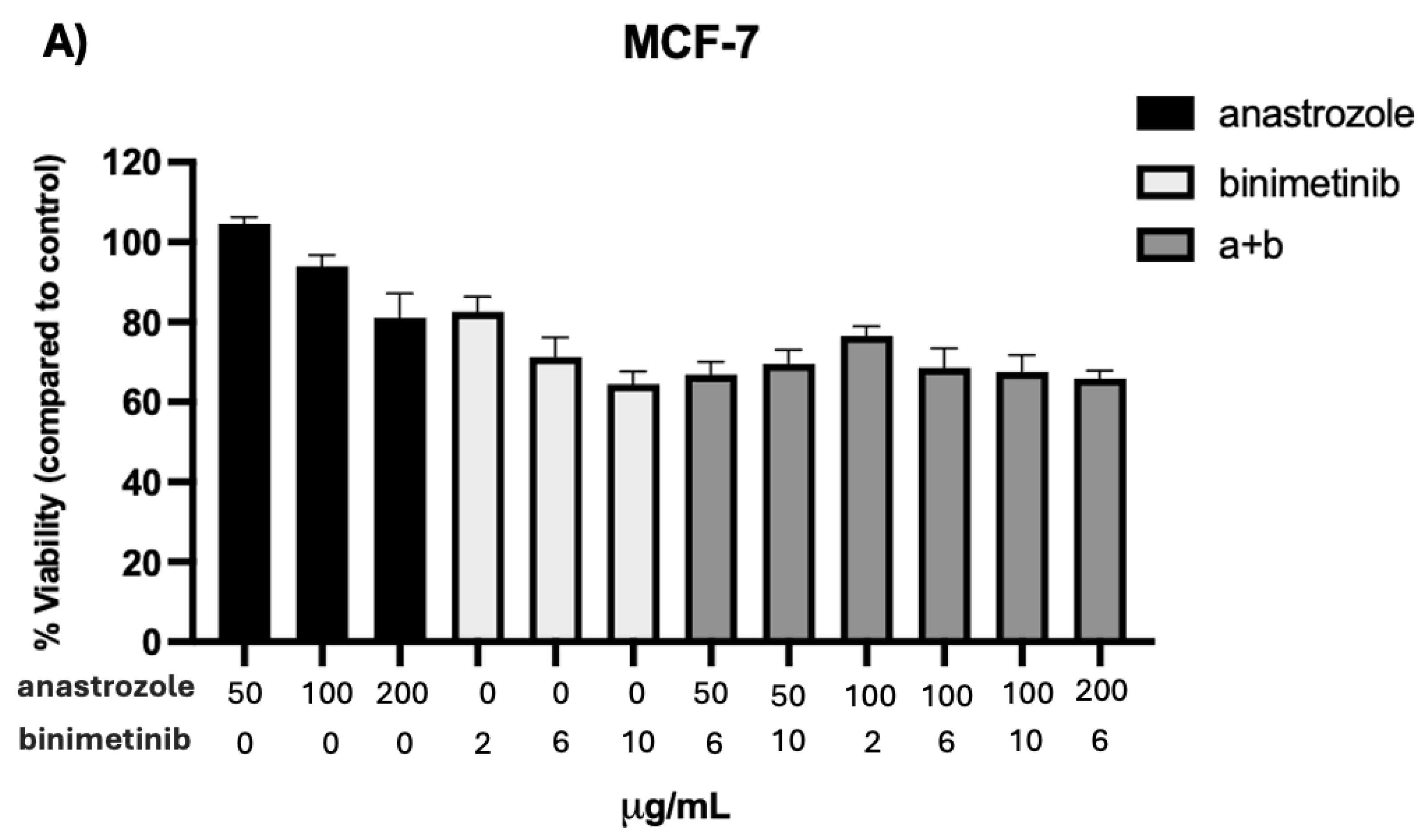
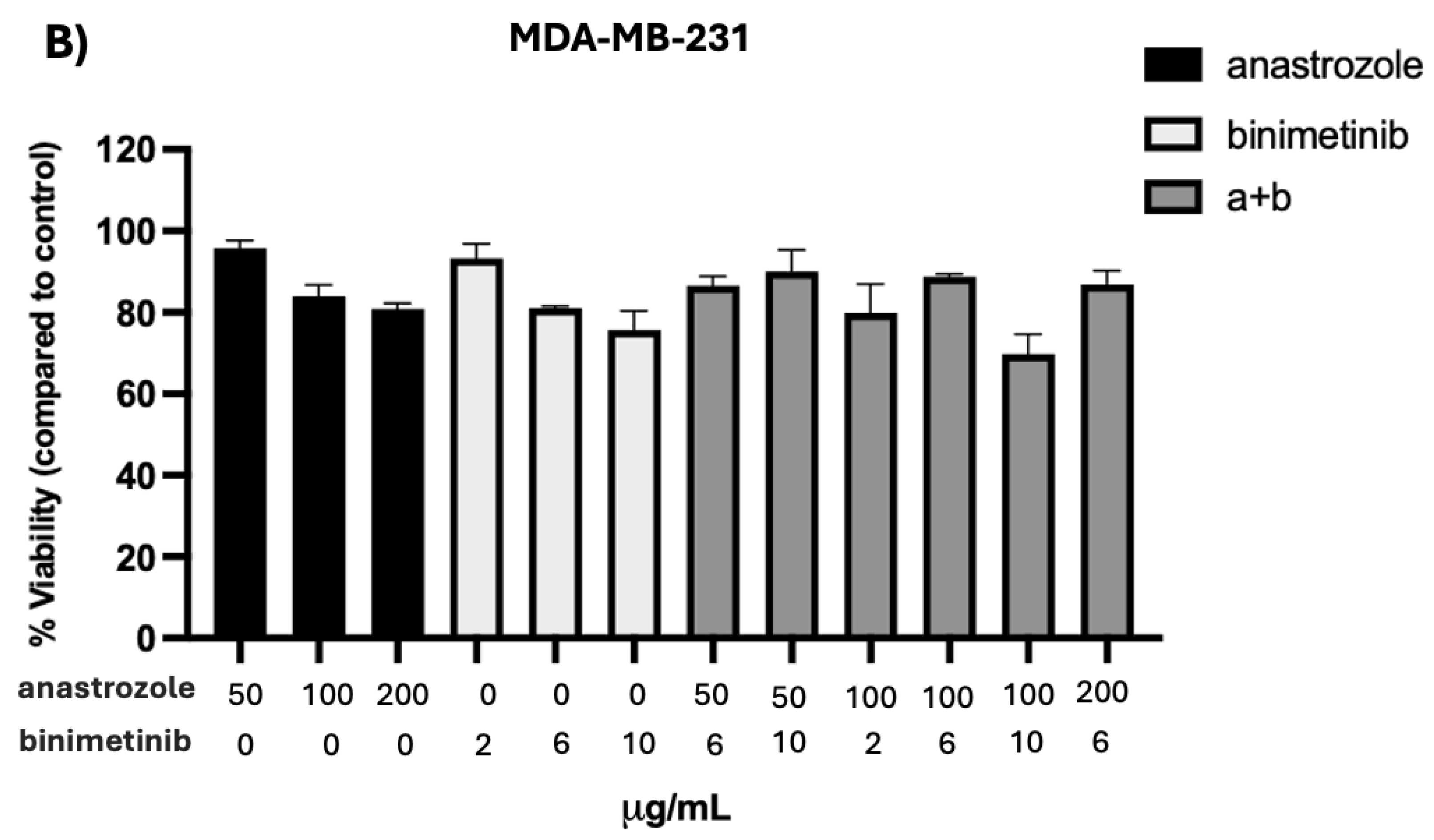
Figure 5.
Synergy analysis of the combination of anastrozole and binimetinib treatment in MCF-7 and MDA-MB-231. Analysis of the combination index (CI) calculated using CompuSyn software in (A) MCF-7 and (B) MDA-MB-231 cells. Dose a (µg/mL): Anastrozole and dose b (µg/mL): binimetinib. The Fa-CI graphs show the nature of the interactions according to the effect (Fa) achieved. CI < 1 indicates a synergistic effect, CI = 1 indicates an additive effect, and CI > 1 indicates an antagonistic effect. .
Figure 5.
Synergy analysis of the combination of anastrozole and binimetinib treatment in MCF-7 and MDA-MB-231. Analysis of the combination index (CI) calculated using CompuSyn software in (A) MCF-7 and (B) MDA-MB-231 cells. Dose a (µg/mL): Anastrozole and dose b (µg/mL): binimetinib. The Fa-CI graphs show the nature of the interactions according to the effect (Fa) achieved. CI < 1 indicates a synergistic effect, CI = 1 indicates an additive effect, and CI > 1 indicates an antagonistic effect. .
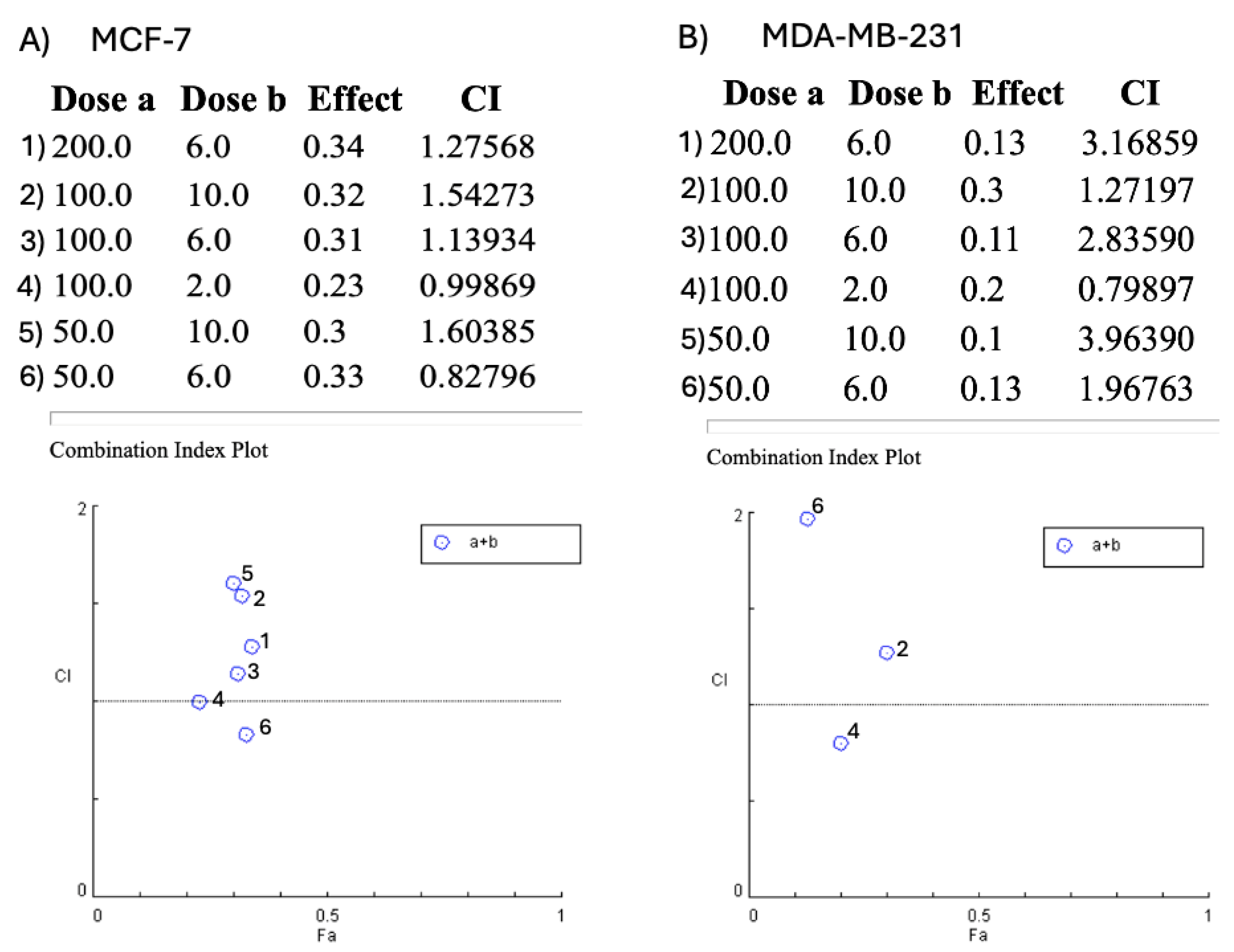
Figure 6.
Assessment of cell migration by wound healing assay in breast cancer cells treated with anastrozole and binimetinib. Representative images of the wound healing assay at 0, 6, 12, and 24 hours after wounding and treatment with anastrozole at concentration of 50 µg/mL, binimetinib at concentration of 6 µg/mL, and the combination of both drugs concentrations, in (A,C) MCF-7 cells; and treatment with anastrozole at concentration of 100 µg/mL, with binimetinib at concentration of 2 µg/mL and with the combination of both drugs concentrations in (B,D) MDA-MB-231 cells. The bar corresponds to 200 μm. (C–D) Statistical data for wound area are expressed as mean ± standard error (n = 3). One-way ANOVA analysis with Tukey's post-hoc analysis, different letters stand for statistical significance, p<0.05.
Figure 6.
Assessment of cell migration by wound healing assay in breast cancer cells treated with anastrozole and binimetinib. Representative images of the wound healing assay at 0, 6, 12, and 24 hours after wounding and treatment with anastrozole at concentration of 50 µg/mL, binimetinib at concentration of 6 µg/mL, and the combination of both drugs concentrations, in (A,C) MCF-7 cells; and treatment with anastrozole at concentration of 100 µg/mL, with binimetinib at concentration of 2 µg/mL and with the combination of both drugs concentrations in (B,D) MDA-MB-231 cells. The bar corresponds to 200 μm. (C–D) Statistical data for wound area are expressed as mean ± standard error (n = 3). One-way ANOVA analysis with Tukey's post-hoc analysis, different letters stand for statistical significance, p<0.05.
4. Discussion
The heterogeneity of breast cancer and the predominant signaling pathways in different cell lines are crucial factors that determine the response to therapies [8,9]. The observed differences in cell viability between MCF-7 and MDA-MB-231 cell lines following the combined treatment with anastrozole and binimetinib can be explained by their distinct molecular subtypes and the predominant signaling pathways involved in their proliferation and survival.
The MCF-7 cell line represents a subtype of breast cancer characterized by estrogen receptor (ER) and progesterone receptor (PR) positivity. In these cells, proliferation and growth are heavily reliant on estrogen-mediated signaling [10,11]. Anastrozole, as an aromatase inhibitor, reduces endogenous estrogen levels, directly suppressing the growth and proliferation of ER-positive breast cancer cells [12]. This mechanism underpins the fundamental principle of endocrine therapy used for this subtype of cancer.
Simultaneously, binimetinib, an inhibitor of MEK, blocks MEK phosphorylation, dis-rupting the MAPK/ERK signaling pathway, which is critical for cell proliferation and survival [13]. The combination of anastrozole, which decreases the availability of estrogen, and the inhibition of the MAPK/ERK pathway by binimetinib, provides a dual attack on critical signaling pathways in MCF-7 cells. The proposed combinatorial strategy aligns with the literature supporting the therapeutic synergy between drugs, enhancing the antitumor effect by targeting multiple biological mechanisms [14,15]. In fact, previous studies with MCF-7 cells and other agents have shown significant reductions in proliferation and increased apoptosis, suggesting that the moderate response observed in MCF-7 cells is expected and reflects their estrogen dependence [16].
In contrast, the MDA-MB-231 cell line represents a triple-negative breast cancer (TNBC) model, characterized by the absence of estrogen, progesterone, and HER2 receptors. TNBC is known for being one of the most aggressive and poor-prognosis subtypes due to the lack of specific molecular targets for targeted therapies and a high resistance rate to drugs [17, 18]. In this context, the response of MDA-MB-231 cells to the combined treatment of anastrozole and binimetinib mainly relies on MEK inhibition and its impact on the MAPK/ERK pathway, which is frequently altered in TNBC [19]. One way in which these cells could respond to anastrozole is through membrane estrogen receptors coupled to G proteins, such as GPER (GPR30), which can stimulate RAS activation [20], so aromatase inhibition would interfere with the availability of free estrogens for binding to these receptors. However, TNBC, including the MDA-MB-231 line, is characterized by the frequent activation of alternative survival pathways, such as the PI3K/AKT/mTOR pathway [21], which may compensate for MEK inhibition, explaining the smaller decrease in cell viability observed compared to MCF-7 cells. The ability of these cells to activate alternative signaling networks in response to MEK inhibition underscores the complexity of their treatment and the need for more complex and personalized therapeutic strategies.
The combination of therapies in TNBC cell lines needs to be extensively studied due to the difficulty in eradicating these cells with monotherapies. In this regard, the analysis of pharmacodynamic synergy using mathematical models, such as the Chou-Talalay method [22], enables the evaluation of drug interactions, identifying optimal therapeutic regimens that maximize efficacy and minimize toxicity. The results obtained in this study, which show a synergistic effect of the combination, support the idea that the joint inhibition of aromatase and MEK may provide a more effective treatment than monotherapy approaches.
The inhibition of the MAPK/MEK/ERK pathway and its relationship with therapeutic efficacy in cancers such as TNBC has been documented [23,24]. The aberrant activation of this pathway in TNBC could promote cell proliferation and metastasis. Combination treatments, addressing multiple signaling pathways, have the potential to more effectively block tumor growth and metastatic progression, emphasizing the need for combinatorial therapies for this cancer subtype.
Finally, tumor heterogeneity, driven by genetic mutations, epigenetic alterations, and microenvironmental variations, contributes to the variability in response to treatments [25]. Combination therapy offers the potential to reduce the dose of each drug, which may minimize toxicity in normal cells while maximizing efficacy in tumor cells. This ap-proach, focused on tailoring treatment to the specific characteristics of each tumor, is essential for improving clinical outcomes, particularly in TNBC, an extremely complex subtype.
The study of cellular migration inhibition, mediated by anastrozole in MCF-7 cells, highlights the importance of hormonal modulation in the migration of tumor cells. This behavior can be explained by the role of aromatase in cancer regulation, whereby, by inhibiting the signaling pathway that is activated when estradiol is synthesized, it cannot bind to its receptors or translocated to the nucleus to bind to the regulatory regions of target genes involved, among other processes, in cell proliferation and migration [26]. In the case of MDA-MB-231 cells, inhibition of other signaling pathways, such as PI3K/AKT/mTOR and WNT [27,28], has also been shown to suppress cell migration, underscoring the importance of developing therapies targeting multiple pathways to improve the TNBC response.
5. Conclusions
The results obtained show that the synergic combination of anastrozole and binimetinib has a favorable preliminary safety profile in non-tumor cells (3T3-L1). The differential response of MCF-7 and MDA-MB-231 cell lines to the combination of anastrozole and binimetinib in its viability and cell migration, is consistent with their molecular profiles and underlying signaling pathways. The estrogen dependency of MCF-7 makes it more susceptible to aromatase inhibition, while the complex network of survival pathways in MDA-MB-231 (TNBC) confers greater resistance and a lower overall response to this combination, despite MEK inhibition. This underscores the need for personalized strategies and drug combinations that address the complexity and heterogeneity of breast cancer subtypes, particularly triple-negative breast cancer (TNBC).
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/doi/s1, Figure S1: title; Table S1: title; Video S1: title.
Author Contributions
Conceptualization, P.D. and E.C.; methodology, P.D. and E.C.; software, P.D.; validation, B.S., G.A. and E.C.; formal analysis, B.S.; investigation, P.D.; resources, P.D.; data curation, B.S.; writing—original draft preparation, P.D.; writing—review and editing, E.C.; visualization, G.A.; supervision, E.C.; project administration, P.D.; funding acquisition, E.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available upon request from the corresponding author.
Acknowledgments
The authors are thankful for the support of a grant #1312392 from SECIHTI to Karla Denisse Portilla Dominguez.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ABC | ATP-binding cassette |
| ABCB1 | ATP-binding cassette P-glycoprotein |
| DMSO | Dimethyl sulfoxide |
| ER | Estrogen receptor |
| MTT | 3-(4,5-Dimethylthiazol-2-yl)-2,5-Diphenyltetrazolium Bromide |
| TNBC | triple-negative breast cancer |
References
- Oms, 2022.
- Asleh, K.; Riaz, N.; Nielsen, T.O. Heterogeneity of triple negative breast cancer: Current advances in subtyping and treatment implications. J. Exp. Clin. Cancer Res. 2022, 41, 265. [CrossRef]
- Kinnel, B.; Singh, S.K.; Oprea-Ilies, G.; Singh, R. Targeted Therapy and Mechanisms of Drug Resistance in Breast Cancer. Cancers 2023, 15, 1320. [CrossRef]
- Gervasini G, Jara C, Olier C, Romero N, Martínez R, Carrillo JA. Polymorphisms in ABCB1 and CYP19A1 genes affect anastrozole plasma concentrations and clinical outcomes in postmenopausal breast cancer patients. Br J Clin Pharmacol. 2017 Mar;83(3):562-571. doi: 10.1111/bcp.13130.
- Wang, Y.; Minden, A. Current Molecular Combination Therapies Used for the Treatment of Breast Cancer. Int. J. Mol. Sci. 2022, 23, 11046. [CrossRef]
- Herrera-Abreu, M.T.; Guan, J.; Khalid, U.; et al. Inhibition of GPX4 enhances CDK4/6 inhibitor and endocrine therapy activity in breast cancer. Nat. Commun. 2024, 15, 9550. [CrossRef]
- Swain, S.M.; Shastry, M.; Hamilton, E. Targeting HER2-positive breast cancer: advances and future directions. Nat. Rev. Drug Discov. 2023, 22, 101–126. [CrossRef]
- Ye, J.; Wu, J.; Liu, B. Therapeutic strategies of dual-target small molecules to overcome drug resistance in cancer therapy. Biochim. Biophys. Acta Rev. Cancer 2023, 1878, 188866. [CrossRef]
- Gautam, S.; Maurya, R.; Vikal, A.; Patel, P.; Thakur, S.; Singh, A.; Gupta, G.D.; Kurmi, B.D. Understanding drug resistance in breast cancer: Mechanisms and emerging therapeutic strategies. Med. Drug Discov. 2025, 26, 100210. [CrossRef]
- Zivadinovic, D.; Gametchu, B.; Watson, C.S. Membrane estrogen receptor-α levels in MCF-7 breast cancer cells predict cAMP and proliferation responses. Breast Cancer Res. 2004, 7, R101. [CrossRef]
- Telang, N.T. The Divergent Effects of Ovarian Steroid Hormones in the MCF-7 Model for Luminal A Breast Cancer: Mechanistic Leads for Therapy. Int. J. Mol. Sci. 2022, 23, 4800. [CrossRef]
- Cairns, J.; Ingle, J.N.; Dudenkov, T.M.; Kalari, K.R.; Carlson, E.E.; Na, J.; Buzdar, A.U.; Robson, M.E; Ellis, M.J.; Goss, P.E.; Shepherd, L.E.; Goodnature, B.; Goetz, M.P.; Weinshilboum, R.M.; Li, H.; Bari, M.G.; Wang, L. Pharmacogenomics of aromatase inhibitors in postmenopausal breast cancer and additional mechanisms of anastrozole action. JCI Insight 2020, 5, e137571. [CrossRef]
- Kun, E.; Tsang, Y.T.M.; Ng, C.W.; Gershenson, D.M.; Wong, K.K. MEK inhibitor resistance mechanisms and recent developments in combination trials. Cancer Treat. Rev. 2021, 92, 102137. [CrossRef]
- Correia, A.S.; Gärtner, F.; Vale, N. Drug combination and repurposing for cancer therapy: the example of breast cancer. Heliyon 2021, 7, e05948. [CrossRef]
- Chu, Y.H.; Huang, Y.C.; Chiu, P.Y.; Kuo, W.H.; Pan, Y.R.; Kuo, Y.T.; Wang, R.H.; Kao, Y.C.; Wang, Y.H.; Lin, Y.F.; Lin, K.T. Combating breast cancer progression through combination therapy with hypomethylating agent and glucocorticoid. iScience 2023, 26, 106597. [CrossRef]
- Thornton, D.; Heck, K.; Patrick, M.; Kromtit, R.; Benedict, C.; Pondugula, S.R.; Shen, J.; Calderón, A.I. Açaí extract and anticancer drug combination promotes synergistic toxicity and apoptosis in MCF-10A cells of breast cancer model. J. Ethnopharmacol. 2025, 353, 120361. [CrossRef]
- Rushing, B.R.; Molina, S.; Sumner, S. Metabolomics Analysis Reveals Altered Metabolic Pathways and Response to Doxorubicin in Drug-Resistant Triple-Negative Breast Cancer Cells. Metabolites 2023, 13, 865. [CrossRef]
- Obidiro, O.; Battogtokh, G.; Akala, E.O. Triple Negative Breast Cancer Treatment Options and Limitations: Future Outlook. Pharmaceutics 2023, 15, 1796. [CrossRef]
- Moon, A. Ras Signaling in Breast Cancer. In Translational Research in Breast Cancer; Noh, D.Y., Han, W., Toi, M., Eds.; Advances in Experimental Medicine and Biology; Springer: Singapore, 2021; Volume 1187. [CrossRef]
- Lei, B.; Sun, S.; Zhang, X.; Feng, C.; Xu, J.; Wen, Y.; Huang, Y.; Wu, M.; Yu, Y. Bisphenol AF exerts estrogenic activity in MCF-7 cells through activation of Erk and PI3K/Akt signals via GPER signaling pathway. Chemosphere 2019, 220, 122–131. [CrossRef]
- Zhang, H.P.; Jiang, R.Y.; Zhu, J.Y.; Sun, K.N.; Huang, Y.; Zhou, H.H.; Zheng, Y.B.; Wang, X.J. PI3K/AKT/mTOR signaling pathway: an important driver and therapeutic target in triple-negative breast cancer. Breast Cancer 2024, 31, 539–551. [CrossRef]
- Elwakeel, A.; Soudan, H.; Eldoksh, A.; Shalaby, M.; Eldemellawy, M.; Ghareeb, D.; Abouseif, M.; Fayad, A.; Hassan, M.; Saeed, H. Implementation of the Chou-Talalay method for studying the in vitro pharmacodynamic interactions of binary and ternary drug combinations on MDA-MB-231 triple negative breast cancer cells. Synergy 2019, 8, 100047. [CrossRef]
- Acosta-Casique, A.; Montes-Alvarado, J.B.; Barragán, M.; Larrauri-Rodríguez, K.A.; Perez-Gonzalez, A.; Delgado-Magallón, A.; Millán-Perez-Peña, L.; Rosas-Murrieta, N.H.; Maycotte, P. ERK activation modulates invasiveness and Reactive Oxygen Species (ROS) production in triple negative breast cancer cell lines. Cell. Signal. 2023, 101, 110487. [CrossRef]
- Yoshikawa, Y. RAS Inhibition Suppresses the Progression and Metastasis of Triple-Negative Breast Cancer. Ph.D. Thesis, Kobe University, Kobe, Japan, 2024.
- Wang, D.; Zhang, Y.; Li, Q.; Li, Y; Li, W.; Zhang, A.; Xu, J.; Meng, J.; Tang, L.; Lyu, S. Epigenetics: Mechanisms, potential roles, and therapeutic strategies in cancer progression. Genes Dis. 2023, 11, 101020. [CrossRef]
- Molehin, D.; Rasha, F.; Rahman, R.L.; et al. Regulation of aromatase in cancer. Mol. Cell. Biochem. 2021, 476, 2449–2464. [CrossRef]
- Bilir, B.; Kucuk, O.; Moreno, C.S. Wnt signaling blockage inhibits cell proliferation and migration, and induces apoptosis in triple-negative breast cancer cells. J. Transl. Med. 2013, 11, 280. [CrossRef]
- Xu, X.; Zhang, M.; Xu, F.; et al. Wnt signaling in breast cancer: biological mechanisms, challenges and opportunities. Mol. Cancer 2020, 19, 165. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



