
Submitted:
06 November 2025
Posted:
07 November 2025
You are already at the latest version
Abstract
Background/Objectives
Oral health-related quality of life (OHRQoL) may influence mental health outcomes, yet longitudinal evidence on its association with depression remains limited. This study aimed to examine whether oral health status and OHRQoL are associated with the development of depression among adults in Japan.
Methods
We analyzed data from the Japan COVID-19 and Society Internet Survey (JACSIS), conducted in 2022 and 2023. A total of 15,068 participants aged ≥20 years without depression at baseline were included. Depression onset was identified by self-reported measures between the two survey waves. Logistic regression models estimated odds ratios (ORs) and 95% confidence intervals (CIs) for depression development in relation to OHRQoL and oral health status, adjusting for sociodemographic and behavioral factors.
Results
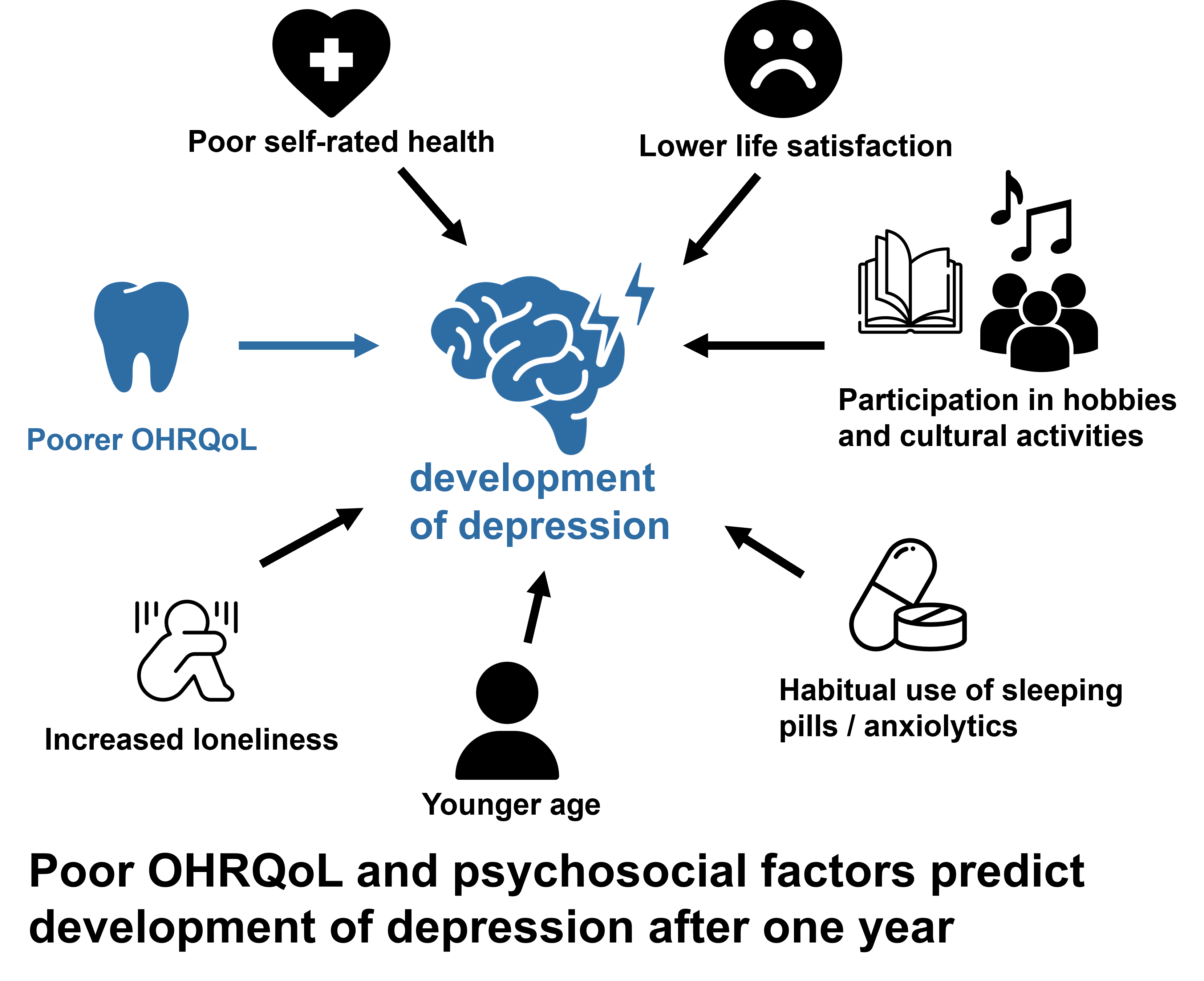
During follow-up, 218 participants (1.45%) developed depression. Poorer OHRQoL was significantly associated with development of depression (OR: 1.018; 95% CI: 1.001–1.036; p = 0.039). Additional risk factors included younger age (OR: 0.974; 95% CI: 0.964–0.985), participation in hobbies and cultural activities (OR: 2.224; 95% CI: 1.498–3.302), habitual use of sleeping pills or anxiolytics (current use OR: 3.512; 95% CI: 2.267–5.442), increased loneliness (OR: 1.217; 95% CI: 1.140–1.299), lower life satisfaction (OR: 0.900; 95% CI: 0.836–0.969), and poor self-rated health (OR: 2.921; 95% CI: 1.810–4.715).
Conclusions
Impaired OHRQoL was associated with depression development, potentially through psychosocial mechanisms. Maintaining good oral health and OHRQoL may help prevent depression, highlighting the need for integrated oral and mental health strategies in clinical practice.
Keywords:
oral health-related quality of life
; depression
; longitudinal study
1. Introduction
Depressive disorders are recognized as a major cause of adverse health effects from early adulthood to old age [1], with over 330 million people affected worldwide [2]. In recent years, there has been increasing global concern regarding mental health issues such as depression, anxiety, and stress. According to the disability-adjusted life years metric developed by the World Health Organization, depression ranked third in 2004, is projected to rise to second by 2020, and to become the leading cause of adverse health effects by 2030 [3]. This indicates that diseases and disabilities that rank higher impose a greater socioeconomic burden on society.
The etiology of depression is complex, involving a myriad of factors ranging from biological to lifestyle-related, which poses challenges for primary prevention strategies [4]. According to de Sousa et al. [5], in their review of longitudinal study, “the course of depression varies among individuals and is influenced by factors such as age and gender [6,7,8,9], social isolation [6,7,10], socioeconomic factors including childhood and current economic status [11], educational level [10,11,12,13,14], employment [9,13,15], chronic conditions and comorbidities [7,8,13,16,17] such as arthritis/rheumatism, asthma, stroke, coronary heart disease, mental health issues, and having more than three chronic diseases), health behaviors [18,19] such as sedentary lifestyles and smoking, self-rated health [7], and family support [20]. Additionally, factors such as participation in extracurricular activities [21], the use of sleeping medications [22], spousal loss [23], social networks [21,24], event participation, decreased life satisfaction [25], and health-related quality of life (HRQOL) [26,27] have also been reported to be associated with depression.
There have also been reports of an association between depression and oral health status. Factors such as tooth loss [26,28,29,30,31], oral pain [32,33], periodontal disease [34,35,36], dental caries [37], deterioration of oral function [30], worsening oral hygiene [38], dental anxiety [39], dental visits within the past year [40], and oral health-related quality of life (OHRQOL) [41,42] have been linked to depressive symptoms. In their review, Karimi et al. [30] suggested a strong correlation between oral health habits, general health practices, and unhealthy lifestyles. These factors are considered potential causes of depression [43,44]. Therefore, they discussed the possibility not only that depression affects oral health, but also that oral health may impact depression. However, most studies have been cross-sectional, leaving many questions unanswered about how oral health impacts the development of depression.
Therefore, we hypothesized that OHRQOL and oral health status are associated with the development of depression. The aim of this longitudinal study was to investigate the association between oral health status, OHRQOL, and the development of depression.
2. Materials and Methods
2.1. Participants
This longitudinal study utilized data from the Japan COVID-19 and Society Internet Survey (JACSIS) [45]conducted in 2022 and 2023, which surveyed 31,000 individuals aged 16–81 years. Sex was self-reported as male or female; gender identity was not assessed. Random sampling was performed based on sex, age, and prefecture, and then panel members were invited to participate in an online survey that included various questions on lifestyle, health, social interactions, and economic activities, as well as questions related to COVID-19. Participants provided web-based informed consent before answering the online survey and could withdraw consent at any time.
The survey for FY2022 started on September 12, 2022 and ended on October 19, 2022. The survey for FY2023 started on September 25, 2023 and concluded on November 17, 2023. The inclusion criteria were reporting no diagnosis of depression at baseline in 2022, age 20 years or older, and providing valid responses to all question items. The exclusion criteria were having been diagnosed with depression presently or in the past, taking less than 15 minutes to respond, answering “yes” to all drug use items, answering “yes” to all systemic disease items, age less than 20 years, and having missing data. Sex was included as a covariate in all statistical analyses. The study protocol was approved by the Osaka International Cancer Institute Research Ethics Committee (approved on June 19, 2020; approval No. 20084) as well as the Ethics Review Board of Okayama University (approval Nos.: 2403-044, 2408-009).
Figure 1.
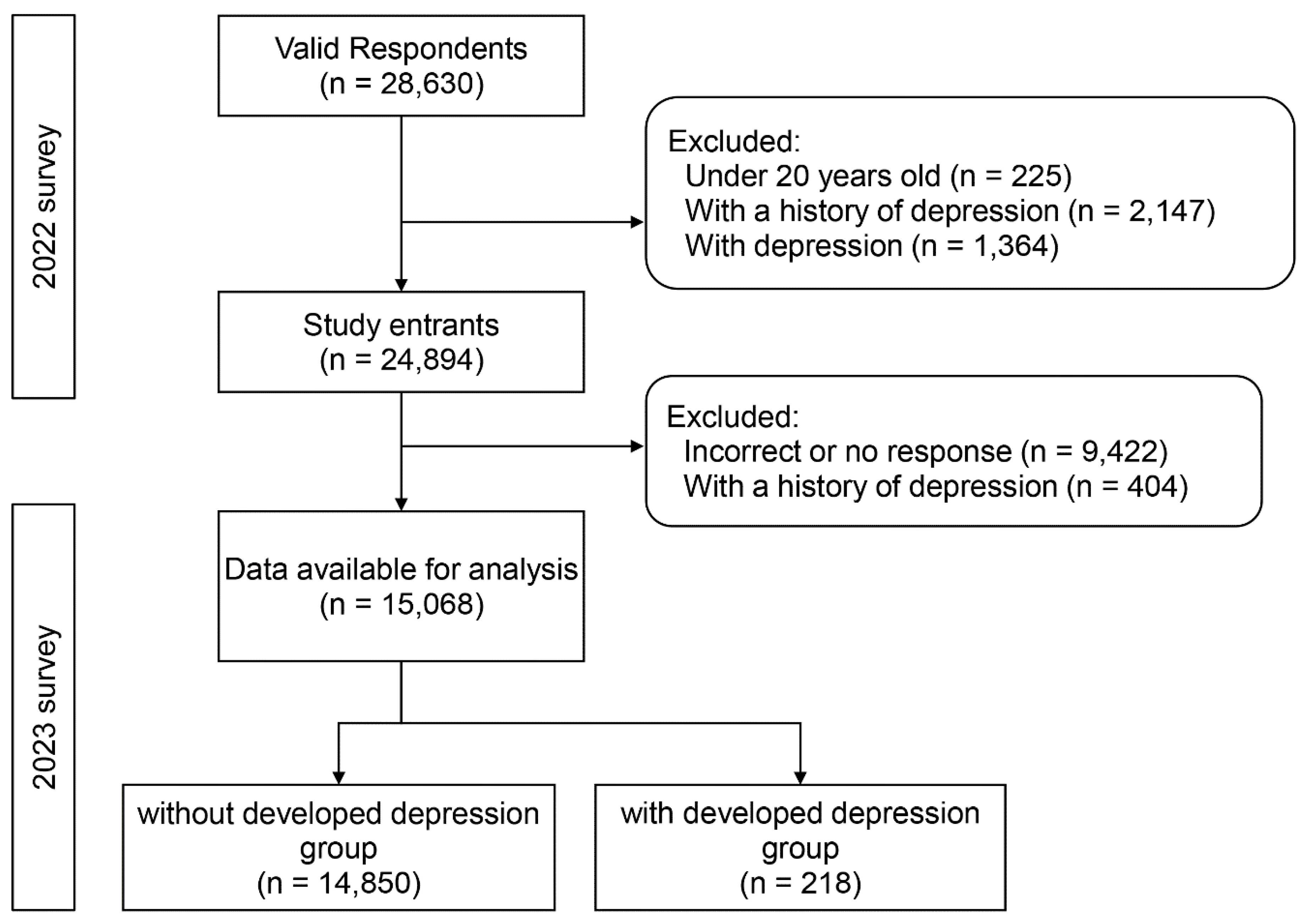
Flowchart of the study. Flowchart illustrating the participant selection process for the study conducted in 2022 and 2023. The diagram shows inclusion and exclusion criteria applied to respondents from the 2022 survey (n = 28,630) and the subsequent 2023 follow-up. Participants under 20 years old, those with a history of depression, or those with depression at baseline were excluded, resulting in 24,894 entrants. Further exclusions for incorrect or missing responses and history of depression during follow-up yielded 15,068 participants for analysis. These were categorized into two groups: without developed depression (n = 14,850) and with developed depression (n = 218). Abbreviations: n = number of participants.
Figure 1.
Flowchart of the study. Flowchart illustrating the participant selection process for the study conducted in 2022 and 2023. The diagram shows inclusion and exclusion criteria applied to respondents from the 2022 survey (n = 28,630) and the subsequent 2023 follow-up. Participants under 20 years old, those with a history of depression, or those with depression at baseline were excluded, resulting in 24,894 entrants. Further exclusions for incorrect or missing responses and history of depression during follow-up yielded 15,068 participants for analysis. These were categorized into two groups: without developed depression (n = 14,850) and with developed depression (n = 218). Abbreviations: n = number of participants.
2.2. Measures
2.2.1. Depression
We asked the participants, “Do you currently have depression?”, to which they were instructed to respond with one of the following options: “Never had it”, “Not currently depressed but have had it in the past”, “Currently have depression (under treatment with medication)”, “Currently have depression (under treatment without medication)”, or “Currently have depression (not under treatment)”. Responses indicating “Currently have depression (under treatment with medication)”, “Currently have depression (under treatment without medication)”, or “Currently have depression (not under treatment)” were classified as “depression present”.
2.2.2. Oral Health-Related Quality of Life (OHRQOL)
Many studies have shown that OHRQOL is influenced by factors such as the number of teeth, the presence of dentures, the need for dental treatment, and the awareness of oral dryness [46,47,48,49]. Among the evaluation indicators for OHRQOL, the Oral Health Impact Profile (OHIP) and the General Oral Health Assessment Index (GOHAI) have been translated into Japanese and are frequently used. However, while the GOHAI is affected by functional disabilities and pain, the OHIP is influenced by psychosocial factors [46,48]. Therefore, in this study, we used the Japanese version of the OHIP-14, a short version of the OHIP (see Table 1 for the English version), as a measure of OHRQOL.
The OHIP-14 consists of 14 questions, each with five response options regarding experiences within the past month. The respondents were asked to select the option that best applied to them, with the scoring as follows: “Always” = 4, “Often” = 3, “Sometimes” = 2, “Rarely” = 1, and “Never” = 0. The OHIP-14 total score is calculated by summing the scores from each question, with a maximum possible score of 56. A higher score indicates poorer OHRQOL.
2.2.3. Oral Health Status
Oral health status was assessed for tooth loss, periodontal disease and oral pain.
Tooth Loss
We asked the participants, “Have you ever had permanent teeth extracted because of cavities or periodontal disease? If so, please specify the number of teeth extracted (excluding teeth extracted because of an external cause such as injury or orthodontic treatment)”. They were instructed to respond with one of the following options: “0 teeth, 1 tooth, 2 teeth, 3 teeth, 4 teeth, 5 teeth, 6–9 teeth, 10–19 teeth, 20–27 teeth, or 28 teeth or more (edentulous)”. Responses were categorized into three groups: 0–5 teeth, 6–9 teeth, and 10 or more teeth.
Periodontal Disease Screening
For the assessment of periodontal status, we used the periodontal screening index developed by Yamamoto et al. [50]. We asked the participants the following questions: “Do you experience bleeding from your gums (such as when brushing your teeth)?”, “Do you feel that your gums have receded compared with before, making your teeth appear longer?”, “Have you ever been told by a dental clinic that you need treatment for periodontal disease or gum issues?”, and “Are you currently a smoker or have you smoked in the past?” Participants who answered “Yes” to three or more of these questions were classified as “having periodontal disease”.
Oral Pain
We asked the participants, “Have you experienced tooth pain because of cavities in the past 2 months?” and “Have you experienced gum pain because of periodontal disease in the past 2 months?” They were instructed to answer “Yes” or “No”. Participants who answered “Yes” to one or more of these questions were classified as having “oral pain”.
Oral Health Behavior
We also asked the participants, “Have you visited a dentist in the past year?” They were instructed to respond with either “Yes” or “No”.
2.2.4. Covariates
Developmental Factors
As developmental factors, we evaluated childhood socioeconomic status and experiences of abuse during childhood.
Regarding childhood socioeconomic status, we asked the participants, “Did you experience financial hardship before turning 18?” [51]. They were instructed to respond with “Yes” or “No”.
Regarding childhood abuse, we asked the following questions [51]: “Have you ever been injured by being severely beaten by a parent before turning age 18?”, “Have you ever lacked necessary care, such as meals or clothing, before turning age 18?”, “Has a parent ever said hurtful or insulting things to you before turning age 18?”, and “Did you feel suffocated because your opinions were never respected by your parents before turning age 18?”. The participants were instructed to answer “Yes” or “No” to each question. Those who answered “Yes” to one or more questions were classified as having experienced abuse.
Sociodemographic and Relationship Characteristics
We also evaluated age, gender, years of education, and annual income. We classified annual income into the following categories: “Less than 3 million yen”, “3 million yen to less than 6 million yen”, “6 million yen to less than 9 million yen”, and “9 million yen or more” [52].
We inquired about educational background (junior high school, high school, vocational school, junior college, university, and graduate school) and assigned the following years of education: “Junior high school” = 9 years, “High school” = 12 years, “Vocational school” = 13 years, “Junior college” = 14 years, “University” = 16 years, and “Graduate school” = 18 years [53]. Responses that fell outside these categories or were marked as “unknown” were excluded from the analysis.
Lifestyle Factors
Regarding lifestyle factors, we evaluated participation in extracurricular activities, physical activity, sitting for more than 240 minutes per day, smoking history, and excessive alcohol intake.
We asked the participants about extracurricular activities and light exercise with the following questions: “Do you participate in hobby, learning, or educational groups or clubs?” and “Do you engage in walking or equivalent physical activity for more than 1 hour per day in your daily life?”. The participants were instructed to respond with “Yes” or “No”.
Regarding sitting for more than 240 minutes per day, we asked the participants, “What was your average sitting time per day in the past month?”. Those who reported sitting for more than 240 minutes were classified as sitting for over 240 minutes per day.
Regarding smoking history, we asked the participants to respond with one of the following options: “Currently smoking”, “I used to smoke but do not smoke now”, or “I have never smoked”.
Regarding excessive drinking, daily alcohol consumption was converted into sake, with the threshold set at more than 3 gou (a traditional Japanese measurement for sake) per day for men and more than 2 gou per day for women [54].
Physical Health Status
We evaluated physical health status by assessing the number of diseases and the habitual use of sleeping pills and antianxiety medications.
We assessed the number of diseases by asking about the current prevalence of the following conditions: hypertension, diabetes, hyperlipidemia, pneumonia/bronchitis, asthma, heart disease, cerebrovascular disease, chronic obstructive pulmonary disease, kidney disease, liver disease, immune disorders, and cancer/malignant tumors. The total number of diseases for which the participants answered “currently present” was classified as the number of diseases.
With regard to the habitual use of sleeping pills, the participants were asked whether they “currently use sleeping pills”, “never used them”, “used them at least once but not habitually”, “used them habitually but not anymore”, “used them occasionally some days”, or “used them almost every day”. Respondents who answered “never used them” or “used them at least once but not habitually” were defined as “never used them habitually”, and those who answered “used them occasionally on some days” or “used them almost every day” were defined as “used them habitually”.
2.3. Statistical Analysis
Among individuals who reported no depression in the 2022 survey, those who reported having depression in the 2023 survey were classified as the “with developed depression” group, and those who reported no depression were classified as the “without developed depression” group. Correlations with covariates were analyzed using the chi-square test and the Mann–Whitney U test. Items with a p-value <0.1 were treated as independent variables, and the presence or absence of depression was treated as a dependent variable in a multivariate binary logistic regression analysis. Sex (male/female) was included as a covariate in all models. SPSS (ver. 26, IBM Japan, Tokyo, Japan) was used for all statistical analyses, with the level of significance set at 5%.
3. Results
Table 2 shows the characteristics of the respondents, including sex distribution (male/female). The “with developed depression” group consisted of 218 individuals (1.5%). The results of the comparison between the with developed depression and without developed depression groups are presented in Table 3. The items that showed a significant correlation between the two groups (p<0.1) included: dental visits within the past year; OHIP-14 score; age; gender; income; smoking history; participation in hobbies, learning, and cultural activities; walking or equivalent physical activity for more than 1 hour a day; chatting with non-cohabiting family members; economic situation until age 18; abuse until age 18; frequency of eating alone; habitual use of sleeping pills or antianxiety medications; family social capital; UCLA-LS3-SF-3 score; risk of social isolation; life satisfaction; and CDC HRQOL-4 score.
Table 4 shows the results of the multivariate binomial logistic regression analysis with these items as independent variables and with or without developed depression as the dependent variable. The items found to be associated with incident depression after adjusting for other items were: “OHIP-14: (odds ratio [OR]: 1.02, 95% confidence interval [CI]: 1.00–1.04, p=0.039)”, “Age (OR: 0.97, 95%CI: 0.96–0.99, p<0.001)”, “Participation in hobbies, learning, and cultural activities: Yes (OR: 2.22, 95%CI: 1.50–3.30, p<0.001)”, “Habitual use of sleep or antianxiety medications: Ever (OR: 1.97, 95%CI: 1.06–3.68, p=0.033) and Currently (OR 3.51, 95%CI: 2.27–5.44, p<0.001)”, “UCLA-LS3-SF-3 (OR: 1.22, 95%CI: 1.14–1.30, p<0.001)”, “Life satisfaction (OR: 0.90, 95%CI: 0.84–0.97, p=0.005)”, and “CDC HRQOL-4: Poor (OR: 2.92: 95%CI: 1.81–4.72, p<0.001)”.
4. Discussion
In this study, we investigated developed depression and associated factors among adults aged 20 years and older. The findings revealed that younger age, participation in hobbies, learning, and cultural activities, habitual use of sleeping pills and anxiolytics, lower scores on the UCLA-LS3-SF-3 (indicating feelings of loneliness), higher scores on the CDC HRQOL-4 (indicating poor self-rated health), lower life satisfaction scores (indicating low satisfaction), and higher scores on the OHIP-14 (indicating poor OHRQOL) were significantly associated with the development of depression. These results suggest that maintaining good OHRQOL may help prevent the development of depression.
In this study, a significant association was observed between OHRQOL and developed depression. The potential pathways from OHRQOL impairment to the onset of depressive symptoms may include the deterioration of social activities and psychosocial issues. Ohi et al. [26] investigated whether OHRQOL impairment at baseline was associated with the development of depressive symptoms 4 years later among participants without depressive symptoms by conducting a questionnaire survey on adults aged 55 years and older. They reported that baseline OHRQOL impairment was significantly associated with an increased risk of depressive symptoms, independent of potential confounding factors such as dental status and dental visits. Those findings suggest that a deterioration of social activities and psychosocial issues may be involved in the pathway from OHRQOL impairment to the development of depressive symptoms. In a cross-sectional study, Zhang et al. [65] reported that college students with inadequate OHRQOL are more likely to exhibit depressive symptoms. Their findings suggest that OHRQOL may influence the prevalence of depressive symptoms through a decrease in self-esteem and life satisfaction caused by barriers to interpersonal communication. These previous reports investigated the relationship between self-assessment depression scales and OHRQOL. By contrast, the present study, aiming to clarify the association with the development of depression more clearly, longitudinally examined the correlation between the presence or absence of a depression diagnosis and OHRQOL. In the present study, OHRQOL may also have influenced the development of depression through the deterioration of social activities, psychosocial problems, impaired interpersonal communication, and decreased self-esteem and life satisfaction.
No significant association was found between missing teeth and the development of depression. Kusama et al. [66] conducted a 3-year longitudinal study involving participants with an average age of 72.7 years to investigate the relationship between tooth loss and depressive symptoms. They found that having 19 or fewer teeth significantly increased the risk of depressive symptoms by 1.3 times. This relationship was notably mediated by difficulties in speaking, smiling, and chewing. Ohi et al. [26] examined the association between depressive symptoms and the number of teeth among Japanese older individuals aged 55 years and older. While a cross-sectional study revealed a correlation, a 4-year longitudinal study did not. Chu et al. [28] reported a connection between the number of teeth and the onset of depression in a 20-year cohort study with an average participant age of 58.8 years. They considered the potential involvement of nutritional status and social participation in this relationship. This may be because the study period was short and the study population did not comprise only older adults.
In the present study, no significant association was found between periodontal disease screening and the development of depression. In an 11-year cohort study, Hsu et al. [67] found that periodontitis (International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9-CM] 523.4x and 523.5x) was associated with the onset of depression (ICD-9-CM 296.2x, 296.3x, 300.4x, and 311.xx). They considered that periodontitis leads to the release of proinflammatory cytokines such as interleukin (IL)-1β, IL-6, and tumor necrosis factor into systemic circulation, and that psychological stress in patients with periodontitis promotes disturbances in the hypothalamic–pituitary–adrenal (HPA) axis and related hypercortisolism. This, in turn, affects immune dysfunction and neuroinflammation, potentially leading to the development of depression. In the present study, the lack of an association may be due to the use of questionnaire-based screening indicators rather than oral examinations for periodontal disease. Additionally, the short follow-up period of 1 year may have contributed to the absence of observed associations.
In a systematic review, Anita et al. [33] suggested a correlation between oral-facial pain (e.g., temporomandibular joint pain, stomatitis) and depression. It is noted that oral-facial pain activates the HPA axis, which is involved in the release of cortisol hormones in patients with depressive symptoms. In this study, only the presence or absence of pain related to caries and periodontal disease was investigated, and temporomandibular joint pain was not included, which may explain the lack of observed associations.
In this study, no significant association was observed between regular dental visits and the onset of depression. In a cross-sectional survey, Peltzer et al. [40] reported a correlation between depression and regular dental visits. Although they did not discuss the mechanisms, it is generally considered that lower socioeconomic status can lead to poorer oral health behaviors. It has also been suggested that university students with lower socioeconomic status may be less likely to attend regular dental check-ups because of their inability to afford dental treatment [68]. In the present study, a significant association was found between income and the presence of regular dental visits (not shown), but neither income nor the presence of regular dental visits was associated with the onset of depression.
This study was based on a large web-based survey of residents in 47 prefectures throughout Japan, which is a strength in ensuring high generalizability. Furthermore, the large sample size from the JACSIS is a strength of this study.
The incidence of depression in this study was 1.45%. Büchtemann et al. [69] reported in a systematic review of elderly individuals aged 70 and older that the incidence of major depression ranged from 1.7% to 7.6%. Although the definitions of depression and the age groups of the subjects differ, it cannot be conclusively stated that the incidence of depression in this population is low.
Limitations
This study has several limitations. First, it relied entirely on self-reporting and was not an objective survey. As a result, the actual outcomes may have been either underestimated or overestimated. Second, there are confounding factors that could not be surveyed. Genetic factors and stress resilience have not been investigated. Third, due to limitations regarding the statistical analysis, binary variables were used for exposure, mediators, and outcomes, which may have led to an overestimation or underestimation of the results. Fourth, because this study depended on an online survey, there is a possibility that the sample was overrepresented by individuals with high Internet literacy [70]. This may have led to selection bias; however, it has been confirmed that this population is not disproportionate compared with census data. In future research, objective measurements such as oral examinations and the use of medical records should be used in addition to self-reported evaluations.
5. Conclusion
In a longitudinal study of participants who had not been diagnosed with depression, we investigated whether OHRQOL and oral health status were associated with the development of depression. The results indicated that OHRQOL is associated with incident depression, even after adjusting for other related factors.
Author Contributions
Conceptualization, Noriko Takeuchi, Takayuki Maruyama, Naoki Toyama, Daisuke Ekuni; Formal analysis, Noriko Takeuchi, Yuzuki Katsube; Investigation, Takahiro Tabuchi; Data curation, Takahiro Tabuchi; Writing – original draft, Noriko Takeuchi; Writing – review & editing, Takayuki Maruyama, Naoki Toyama, Daisuke Ekuni, Takahiro Tabuchi, Yuzuki Katsube; Funding acquisition, Noriko Takeuchi, Takahiro Tabuchi.
Funding
This study was supported by the Mental Health Okamoto Memorial Foundation; the Japan Society for the Promotion of Science (grant numbers 20K10467, 20K13721, 20K19633, 21H04856, 22K02116, 22H03225, 23H03160, 23K07492, 23K16245, 23K18370); the Japan Science and Technology Agency (grant number JPMJPF2017); the Health and Labor Sciences Research Grants (grant numbers 21HA2016, 22JA1005, 23EA1001, 23FA1004); the Strategic Research Promotion of Yokohama City University (2021–2022, grant number SK202116); the Children and Families Agency Program (grant number JPCA20CA2053); the National Institute for Environmental Studies, Intramural Fund; and the Tokyo Foundation for Policy Research. The funding sources were not involved in the study design, data collection, analysis, interpretation, writing of the manuscript, or decision to submit the article for publication.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Osaka International Cancer Institute Research Ethics Committee (approval No. 20084, approved on June 19, 2020) and the Ethics Review Board of Okayama University (approval Nos.: 2403-044, 2408-009).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data used in the present study are not deposited in a public repository due to containing personally identifiable or potentially sensitive information. In accordance with ethical guidelines in Japan, dissemination of the data is restricted by the Research Ethics Committee of the Osaka International Cancer Institute. Any inquiries regarding data use should be directed to Dr. Takahiro Tabuchi (tabuchitak@gmail.com). More details of data availability can be found on the JACSIS website (https://jacsis-study.jp/howtouse/).
Acknowledgments
The authors thank all participants for their time and contribution to this study.
AI Software Disclosure
The authors employed ChatGPT (OpenAI) as an ancillary instrument to verify the coherence and logical consistency of the manuscript. The AI tool was solely responsible for proposing suggestions; the decision regarding acceptance or rejection of these suggestions was at the discretion of the authors.
Conflicts of Interest
Takahiro Tabuchi has disclosed receipt of research funding, consulting fees, or lecture fees from the following entities within the past 36 months: Daiichi Sankyo Healthcare Co., Ltd.; Johnson & Johnson K.K.; Data Seed Inc.; Workout-Plus LLC; and EMMA Co., Ltd. No conflicts of interest are held by any of the other authors.
References
- GBD 2019 Mental Disorders Collaborators. Global, Regional, and National Burden of 12 Mental Disorders in 204 Countries and Territories, 1990-2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet Psychiatry 2022, 9 (2), 137–150. [CrossRef]
- Global Health Data Exchange (GHDx). 2021. Institute of Health Metrics and Evaluation. https://vizhub.healthdata.org/gbd-results (accessed 2025-03-12).
- World health organization. Mental health of older adults. https://www.who.int/news-room/fact-sheets/detail/mental-health-of-older-adults (accessed 2025-04-03).
- McAllister-Williams, R. H.; Arango, C.; Blier, P.; Demyttenaere, K.; Falkai, P.; Gorwood, P.; Hopwood, M.; Javed, A.; Kasper, S.; Malhi, G. S.; Soares, J. C.; Vieta, E.; Young, A. H.; Papadopoulos, A.; Rush, A. J. The Identification, Assessment and Management of Difficult-to-Treat Depression: An International Consensus Statement. J Affect Disord 2020, 267, 264–282. [CrossRef]
- de Sousa, R. D.; Zagalo, D. M.; Costa, T.; de Almeida, J. M. C.; Canhão, H.; Rodrigues, A. Exploring Depression in Adults over a Decade: A Review of Longitudinal Studies. BMC Psychiatry 2025, 25, 378. [CrossRef]
- Briggs, R.; McDowell, C. P.; De Looze, C.; Kenny, R. A.; Ward, M. Depressive Symptoms Among Older Adults Pre– and Post–COVID-19 Pandemic. J Am Med Dir Assoc 2021, 22 (11), 2251–2257. [CrossRef]
- Chondros, P.; Davidson, S.; Wolfe, R.; Gilchrist, G.; Dowrick, C.; Griffiths, F.; Hegarty, K.; Herrman, H.; Gunn, J. Development of a Prognostic Model for Predicting Depression Severity in Adult Primary Patients with Depressive Symptoms Using the Diamond Longitudinal Study. J Affect Disord 2018, 227, 854–860. [Google Scholar] [CrossRef]
- Cheng, Y.; Thorpe, L.; Kabir, R.; Lim, H. J. Latent Class Growth Modeling of Depression and Anxiety in Older Adults: An 8-Year Follow-up of a Population-Based Study. BMC Geriatr 2021, 21, 550. [Google Scholar] [CrossRef]
- Lo Coco, G.; Salerno, L.; Albano, G.; Pazzagli, C.; Lagetto, G.; Mancinelli, E.; Freda, M. F.; Bassi, G.; Giordano, C.; Gullo, S.; Di Blasi, M. Psychosocial Predictors of Trajectories of Mental Health Distress during the COVID-19 Pandemic: A Four-Wave Panel Study. Psychiatry Res 2023, 326, 115262. [Google Scholar] [CrossRef]
- Luo, M. S.; and Li, L. W. Trajectories of Social Isolation and Depressive Symptoms in Mid- and Later Life: A Parallel Process Latent Growth Curve Analysis. Aging & Mental Health 2023, 27, 2211–2219. [Google Scholar] [CrossRef]
- Kim, W.; Kim, T. H.; Lee, T.-H.; Ju, Y. J.; Park, E.-C. The Effect of Childhood and Current Economic Status on Depressive Symptoms in South Korean Individuals: A Longitudinal Study. Int J Equity Health 2016, 15 (1), 111. [CrossRef]
- Cheval, B.; Maltagliati, S.; Saoudi, I.; Fessler, L.; Farajzadeh, A.; Sieber, S.; Cullati, S.; Boisgontier, M. P. Physical Activity Mediates the Effect of Education on Mental Health Trajectories in Older Age. J Affect Disord 2023, 336, 64–73. [Google Scholar] [CrossRef]
- Shin, J.; Cho, E. Trajectories of Depressive Symptoms among Community-Dwelling Korean Older Adults: Findings from the Korean Longitudinal Study of Aging (2006-2016). BMC Psychiatry 2022, 22 (1), 246. [CrossRef]
- Zhang, W.; Wang, T.; Wang, A. Impact of Physical Activity Intensity on Longitudinal Trajectories of Cognitive Function and Depressive Symptoms in Middle-Aged and Older Chinese Adults: Eight-Year Prospective Study. J Affect Disord 2022, 315, 64–69. [Google Scholar] [CrossRef]
- Handley, T. E.; Rich, J.; Lewin, T. J.; Kelly, B. J. The Predictors of Depression in a Longitudinal Cohort of Community Dwelling Rural Adults in Australia. Soc Psychiatry Psychiatr Epidemiol 2019, 54, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Leung, J.; Fan, V. S.; Mahadevan, R. How Do Different Chronic Condition Comorbidities Affect Changes in Depressive Symptoms of Middle Aged and Older Adults? J Affect Disord 2020, 272, 46–49. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-M.; Lee, I.-C.; Su, Y.-Y.; Mullan, J.; Chiu, H.-C. The Longitudinal Relationship between Mental Health Disorders and Chronic Disease for Older Adults: A Population-Based Study. International Journal of Geriatric Psychiatry 2017, 32, 1017–1026. [Google Scholar] [CrossRef] [PubMed]
- Feter, N.; Rocha, J. Q. S.; Leite, J. S.; Delpino, F. M.; Caputo, E. L.; Cassuriaga, J.; de Almeida Paz, I.; Silveira da Silva, L.; Vieira, Y. P.; Schröeder, N.; Nascimento da Silva, C.; Baptista Gonçalves, J. C.; da Costa Pereira, H.; Barbosa, T. A.; Reichert, F. F.; Silva, M. C.; Rombaldi, A. J. Using Digital Platform for Physical Activity Practice Attenuated the Trajectory of Depressive Symptoms during the Covid-19 Pandemic: Findings of the PAMPA Cohort. Mental Health and Physical Activity 2023, 25, 100543. [Google Scholar] [CrossRef]
- Yang, G.; D’Arcy, C. The Changing Relationship between Health Risk Behaviors and Depression among Birth Cohorts of Canadians 65+, 1994–2014. Front Psychiatry 2022, 13, 1078161. [Google Scholar] [CrossRef]
- Wang, J.; Wu, Bei; Pei, Yaolin; and Zhong, R. Instrumental Support Primarily Provided by Adult Children and Trajectories of Depressive Symptoms among Older Adults with Disabilities in Rural China. Aging & Mental Health 2023, 27 (3), 646–652. [CrossRef]
- Uemura, K.; Makizako, H.; Lee, S.; Doi, T.; Lee, S.; Tsutsumimoto, K.; Shimada, H. Behavioral Protective Factors of Increased Depressive Symptoms in Community-Dwelling Older Adults: A Prospective Cohort Study. International Journal of Geriatric Psychiatry 2018, 33, e234–e241. [Google Scholar] [CrossRef]
- Tsutsumimoto, K.; Makizako, H.; Doi, T.; Hotta, R.; Nakakubo, S.; Shimada, H.; Suzuki, T. Prospective Associations between Sedentary Behaviour and Incident Depressive Symptoms in Older People: A 15-Month Longitudinal Cohort Study. International Journal of Geriatric Psychiatry 2017, 32, 193–200. [Google Scholar] [CrossRef]
- Schoevers, R. A.; Deeg, D. J. H.; van Tilburg, W.; Beekman, A. T. F. Depression and Generalized Anxiety Disorder: Co-Occurrence and Longitudinal Patterns in Elderly Patients. Am J Geriatr Psychiatry 2005, 13, 31–39. [Google Scholar] [CrossRef]
- Luppa, M.; Luck, T.; König, H.-H.; Angermeyer, M. C.; Riedel-Heller, S. G. Natural Course of Depressive Symptoms in Late Life. An 8-Year Population-Based Prospective Study. J Affect Disord 2012, 142, 166–171. [Google Scholar] [CrossRef] [PubMed]
- Lue, B.-H.; Chen, L.-J.; Wu, S.-C. Health, Financial Stresses, and Life Satisfaction Affecting Late-Life Depression among Older Adults: A Nationwide, Longitudinal Survey in Taiwan. Arch Gerontol Geriatr 2010, 50 Suppl 1, S34–38. [Google Scholar] [CrossRef]
- Ohi, T.; Murakami, T.; Komiyama, T.; Miyoshi, Y.; Endo, K.; Hiratsuka, T.; Satoh, M.; Asayama, K.; Inoue, R.; Kikuya, M.; Metoki, H.; Hozawa, A.; Imai, Y.; Watanabe, M.; Ohkubo, T.; Hattori, Y. Oral Health-Related Quality of Life Is Associated with the Prevalence and Development of Depressive Symptoms in Older Japanese Individuals: The Ohasama Study. Gerodontology 2022, 39, 204–212. [Google Scholar] [CrossRef] [PubMed]
- Sivertsen, H.; Bjørkløf, G. H.; Engedal, K.; Selbæk, G.; Helvik, A.-S. Depression and Quality of Life in Older Persons: A Review. Dement Geriatr Cogn Disord 2015, 40, 311–339. [Google Scholar] [CrossRef] [PubMed]
- Chu, W.-M.; Nishita, Y.; Tange, C.; Zhang, S.; Furuya, K.; Shimokata, H.; Otsuka, R.; Lee, M.-C.; Arai, H. Association of a Lesser Number of Teeth with More Risk of Developing Depressive Symptoms among Middle-Aged and Older Adults in Japan: A 20-Year Population-Based Cohort Study. J Psychosom Res 2023, 174, 111498. [Google Scholar] [CrossRef]
- Ehrenthal, J. C.; Graetz, C.; Plaumann, A.; Dörfer, C. E.; Herzog, W. Number of Teeth Predict Depressive Symptoms in a Longitudinal Study on Patients with Periodontal Disease. J Psychosom Res 2016, 89, 16–19. [Google Scholar] [CrossRef]
- Karimi, P.; Zojaji, S.; Fard, A. A.; Nateghi, M. N.; Mansouri, Z.; Zojaji, R. The Impact of Oral Health on Depression: A Systematic Review. Spec Care Dentist 2024. [Google Scholar] [CrossRef]
- Weng, S.; Hou, S.; Jiao, X.; Sun, Y. Adverse Impacts of Temporomandibular Disorders Symptoms and Tooth Loss on Psychological States and Oral Health-Related Quality of Life During the COVID-19 Pandemic Lockdown. Front Public Health 2022, 10, 899582. [Google Scholar] [CrossRef]
- Karamat, A.; Smith, J. G.; Melek, L. N. F.; Renton, T. Psychologic Impact of Chronic Orofacial Pain: A Critical Review. J Oral Facial Pain Headache 2022, 36, 103–140. [Google Scholar] [CrossRef]
- Anita, H.; Asnely Putri, F.; Maulina, T. The Association Between Orofacial Pain and Depression: A Systematic Review. J Pain Res 2024, 17, 785–796. [Google Scholar] [CrossRef] [PubMed]
- Shin, H.-S.; Ahn, Y.-S.; Lim, D.-S. Association Between Chewing Difficulty and Symptoms of Depression in Adults: Results from the Korea National Health and Nutrition Examination Survey. J Am Geriatr Soc 2016, 64, e270–e278. [Google Scholar] [CrossRef]
- Dibello, V.; Custodero, C.; Cavalcanti, R.; Lafornara, D.; Dibello, A.; Lozupone, M.; Daniele, A.; Pilotto, A.; Panza, F.; Solfrizzi, V. Impact of Periodontal Disease on Cognitive Disorders, Dementia, and Depression: A Systematic Review and Meta-Analysis. GeroScience 2024, 46, 5133–5169. [Google Scholar] [CrossRef] [PubMed]
- Saletu, A.; Pirker-Frühauf, H.; Saletu, F.; Linzmayer, L.; Anderer, P.; Matejka, M. Controlled Clinical and Psychometric Studies on the Relation between Periodontitis and Depressive Mood. J Clin Periodontol 2005, 32, 1219–1225. [Google Scholar] [CrossRef] [PubMed]
- Cademartori, M. G.; Demarco, F. F.; Freitas da Silveira, M.; Barros, F. C.; Corrêa, M. B. Dental Caries and Depression in Pregnant Women: The Role of Oral Health Self-Perception as Mediator. Oral Dis 2022, 28, 1733–1740. [Google Scholar] [CrossRef]
- Chen, R.-J.; Lai, K.-H.; Lee, C.-H.; Lin, H.-Y.; Lin, C.-C.; Chen, C.-H.; Chen, W.; Chen, W.-Y.; Vo, T. T. T.; Lee, I.-T. Exploring the Link between Xerostomia and Oral Health in Mental Illness: Insights from Autism Spectrum Disorder, Depression, Bipolar Disorder, and Schizophrenia. Healthcare (Basel) 2024, 12 (20), 2018. [CrossRef]
- Halonen, H.; Nissinen, J.; Lehtiniemi, H.; Salo, T.; Riipinen, P.; Miettunen, J. The Association Between Dental Anxiety And Psychiatric Disorders And Symptoms: A Systematic Review. Clin Pract Epidemiol Ment Health 2018, 14, 207–222. [Google Scholar] [CrossRef]
- Peltzer, K.; Pengpid, S. Oral Health Behaviour and Social and Health Factors in University Students from 26 Low, Middle and High Income Countries. Int J Environ Res Public Health 2014, 11, 12247–12260. [Google Scholar] [CrossRef]
- Gemp, S.; Ziebolz, D.; Haak, R.; Mauche, N.; Prase, M.; Dogan-Sander, E.; Görges, F.; Strauß, M.; Schmalz, G. Oral Health-Related Quality of Life in Adult Patients with Depression or Attention Deficit Hyperactivity Disorder (ADHD). J Clin Med 2023, 12, 7192. [Google Scholar] [CrossRef]
- Rouxel, P.; Tsakos, G.; Chandola, T.; Watt, R. G. Oral Health-A Neglected Aspect of Subjective Well-Being in Later Life. J Gerontol B Psychol Sci Soc Sci 2018, 73, 382–386. [Google Scholar] [CrossRef]
- Ouanounou, A. Xerostomia in the Geriatric Patient: Causes, Oral Manifestations, and Treatment. Compend Contin Educ Dent 2016, 37, 306–311;quiz312. [Google Scholar]
- Zahedi, H.; Kelishadi, R.; Heshmat, R.; Motlagh, M. E.; Ranjbar, S. H.; Ardalan, G.; Payab, M.; Chinian, M.; Asayesh, H.; Larijani, B.; Qorbani, M. Association between Junk Food Consumption and Mental Health in a National Sample of Iranian Children and Adolescents: The CASPIAN-IV Study. Nutrition 2014, 30, 1391–1397. [Google Scholar] [CrossRef]
- Saito, K.; Kawai, Y.; Ishikawa, H.; Tabuchi, T.; Kuwahara, K. Combined Associations of Education and Health Literacy with Preventive Dental Visits in Patients with Diabetes: A Nationwide Cross-Sectional Study. Diabetol Int 2025, 16, 145–152. [Google Scholar] [CrossRef]
- Ikebe, K.; Watkins, C. A.; Ettinger, R. L.; Sajima, H.; Nokubi, T. Application of Short-Form Oral Health Impact Profile on Elderly Japanese. Gerodontology 2004, 21, 167–176. [Google Scholar] [CrossRef] [PubMed]
- John, M. T.; Koepsell, T. D.; Hujoel, P.; Miglioretti, D. L.; LeResche, L.; Micheelis, W. Demographic Factors, Denture Status and Oral Health-Related Quality of Life. Community Dentistry and Oral Epidemiology 2004, 32, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Locker, D.; Matear, D.; Stephens, M.; Lawrence, H.; Payne, B. Comparison of the GOHAI and OHIP-14 as Measures of the Oral Health-Related Quality of Life of the Elderly. Community Dentistry and Oral Epidemiology 2001, 29, 373–381. [Google Scholar] [CrossRef] [PubMed]
- Slade, G. D. Derivation and Validation of a Short-Form Oral Health Impact Profile. Community Dent Oral Epidemiol 1997, 25, 284–290. [Google Scholar] [CrossRef]
- Yamamoto, T.; Koyama, R.; Tamaki, N.; Maruyama, T.; Tomofuji, T.; Ekuni, D.; Yamanaka, R.; Azuma, T.; Morita, M. Validity of a Questionnaire for Periodontitis Screening of Japanese Employees. Journal of Occupational Health 2009, 51, 137–143. [Google Scholar] [CrossRef]
- Fujiwara, T. Impact of Adverse Childhood Experience on Physical and Mental Health: A Life-Course Epidemiology Perspective. Psychiatry and Clinical Neurosciences 2022, 76, 544–551. [Google Scholar] [CrossRef]
- Usami, K.; Sasahara, S.; Yoshino, S.; Tomotsune, Y.; Hayashi, M.; Matsuzaki, I. Association between Perceptions of Post-Retirement and Mental Health Status of Middle-Aged Workers in Tsukuba Research Park City. Journal of Physical Fitness, Nutrition and Immunology 2008, 18, 205–212. [Google Scholar]
- Yanagisawa, S.; Sugisawa, H.; Harada, K.; Sugihara, Y. [Psychosocial mediators between socioeconomic status and oral health among urban-dwelling older adults]. Nihon Koshu Eisei Zasshi 2023, 70, 433–441. [Google Scholar] [CrossRef]
- Suzuki, T.; Eguchi, A.; Shigefuku, R.; Nagao, S.; Morikawa, M.; Sugimoto, K.; Iwasa, M.; Takei, Y. Accuracy of Carbohydrate-Deficient Transferrin as a Biomarker of Chronic Alcohol Abuse during Treatment for Alcoholism. Hepatol Res 2022, 52, 120–127. [Google Scholar] [CrossRef]
- Fujiwara, T.; Doi, S.; Isumi, A.; Ochi, M. Association of Existence of Third Places and Role Model on Suicide Risk Among Adolescent in Japan: Results From A-CHILD Study. Front Psychiatry 2020, 11, 529818. [Google Scholar] [CrossRef]
- Hughes, M. E.; Waite, L. J.; Hawkley, L. C.; Cacioppo, J. T. A Short Scale for Measuring Loneliness in Large Surveys. Res Aging 2004, 26, 655–672. [Google Scholar] [CrossRef]
- Russell, D. W. UCLA Loneliness Scale (Version 3): Reliability, Validity, and Factor Structure. J Pers Assess 1996, 66, 20–40. [Google Scholar] [CrossRef] [PubMed]
- Imamura, K.; Kamide, N.; Sakamoto, M.; Sato, H.; Shiba, Y.; Matsunaga, A. Association Between Social Network and Physical Function in Community-Dwelling Older Adults in Japan. Phys Ther Res 2020, 23, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Kurimoto, A.; Awata, S.; Ohkubo, T.; Tsubota-Utsugi, M.; Asayama, K.; Takahashi, K.; Suenaga, K.; Satoh, H.; Imai, Y. [Reliability and validity of the Japanese version of the abbreviated Lubben Social Network Scale]. Nihon Ronen Igakkai Zasshi 2011, 48, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Lubben, J.; Blozik, E.; Gillmann, G.; Iliffe, S.; von Renteln Kruse, W.; Beck, J. C.; Stuck, A. E. Performance of an Abbreviated Version of the Lubben Social Network Scale among Three European Community-Dwelling Older Adult Populations. Gerontologist 2006, 46, 503–513. [Google Scholar] [CrossRef]
- Chimed-Ochir, O.; Mine, Y.; Okawara, M.; Ibayashi, K.; Miyake, F.; Fujino, Y. Validation of the Japanese Version of the CDC HRQOL-4 in Workers. J Occup Health 2020, 62, e12152. [Google Scholar] [CrossRef]
- Kurogi, K.; Ikegami, K.; Eguchi, H.; Tsuji, M.; Tateishi, S.; Nagata, T.; Matsuda, S.; Fujino, Y.; Ogami, A.; CORoNaWork Project. A Cross-Sectional Study on Perceived Workplace Health Support and Health-Related Quality of Life. Journal of Occupational Health 2021, 63 (1). [CrossRef]
- Ford, E. S.; Moriarty, D. G.; Zack, M. M.; Mokdad, A. H.; Chapman, D. P. Self-Reported Body Mass Index and Health-Related Quality of Life: Findings from the Behavioral Risk Factor Surveillance System. Obes Res 2001, 9, 21–31. [Google Scholar] [CrossRef]
- Dumas, S. E.; Dongchung, T. Y.; Sanderson, M. L.; Bartley, K.; Levanon Seligson, A. A Comparison of the Four Healthy Days Measures (HRQOL-4) with a Single Measure of Self-Rated General Health in a Population-Based Health Survey in New York City. Health Qual Life Outcomes 2020, 18, 315. [Google Scholar] [CrossRef]
- Zhang, Z.; Tian, Y.; Zhong, F.; Li, C.; Dong, S.; Huang, Y.; Liu, X.; Huang, C. Association between Oral Health-Related Quality of Life and Depressive Symptoms in Chinese College Students: Fitness Improvement Tactics in Youths (FITYou) Project. Health Qual Life Outcomes 2019, 17, 96. [Google Scholar] [CrossRef] [PubMed]
- Kusama, T.; Kiuchi, S.; Umehara, N.; Kondo, K.; Osaka, K.; Aida, J. The Deterioration of Oral Function and Orofacial Appearance Mediated the Relationship between Tooth Loss and Depression among Community-Dwelling Older Adults: A JAGES Cohort Study Using Causal Mediation Analysis. J Affect Disord 2021, 286, 174–179. [Google Scholar] [CrossRef]
- Hsu, C.-C.; Hsu, Y.-C.; Chen, H.-J.; Lin, C.-C.; Chang, K.-H.; Lee, C.-Y.; Chong, L.-W.; Kao, C.-H. Association of Periodontitis and Subsequent Depression: A Nationwide Population-Based Study. Medicine 2015, 94, e2347. [Google Scholar] [CrossRef]
- Lopez, R.; Baelum, V. Factors Associated with Dental Attendance among Adolescents in Santiago, Chile. BMC Oral Health 2007, 7, 4. [Google Scholar] [CrossRef] [PubMed]
- Büchtemann, D.; Luppa, M.; Bramesfeld, A.; Riedel-Heller, S. Incidence of Late-Life Depression: A Systematic Review. J Affect Disord 2012, 142, 172–179. [Google Scholar] [CrossRef] [PubMed]
- Andrade, C. The Limitations of Online Surveys. Indian J Psychol Med 2020, 42, 575–576. [Google Scholar] [CrossRef]

Table 1.
English version of the OHIP-14 questionnaire. The Oral Health Impact Profile (OHIP-14) assesses oral health-related quality of life across 14 items. Participants responded based on experiences during the past 7 days. Response options: 0 = Never, 1 = Hardly ever, 2 = Occasionally, 3 = Fairly often, 4 = Very often.
Table 1.
English version of the OHIP-14 questionnaire. The Oral Health Impact Profile (OHIP-14) assesses oral health-related quality of life across 14 items. Participants responded based on experiences during the past 7 days. Response options: 0 = Never, 1 = Hardly ever, 2 = Occasionally, 3 = Fairly often, 4 = Very often.
| For the past 7 days, have you… |
| …had trouble pronouncing any words because of problems with your teeth or mouth? …felt that your sense of taste has worsened because of problems with your teeth or mouth? …had painful aching in your mouth? …found it uncomfortable to eat any foods because of problems with your teeth or mouth? …been self-conscious because of your teeth or mouth? …felt tense because of problems with your teeth or mouth? …had to interrupt meals because of problems with your teeth or mouth? …found it difficult to relax because of problems with your teeth or mouth? …been a bit embarrassed because of problems with your teeth or mouth? …been a bit irritable with other people because of problems with your teeth or mouth? …had difficulty doing your usual jobs because of problems with your teeth or mouth? …felt that life in general was less satisfying because of problems with your teeth or mouth …been totally unable to function because of problems with your teeth or mouth? Has been your diet been unsatisfactory because of problems with your teeth of mouth? |
Table 2.
Characteristics of participants at baseline (n=15068). Baseline characteristics of study participants, including oral health-related variables (OHIP-14 score, oral health status), sociodemographic factors, and behavioral covariates. Continuous variables are presented as mean ± standard deviation (SD), and categorical variables as n (%). OHIP: Oral Health Impact Profile; UCLA: University of California, Los Angeles; CDC HRQOL-4: Centers for Disease Control and Prevention Health-Related Quality of Life.
Table 2.
Characteristics of participants at baseline (n=15068). Baseline characteristics of study participants, including oral health-related variables (OHIP-14 score, oral health status), sociodemographic factors, and behavioral covariates. Continuous variables are presented as mean ± standard deviation (SD), and categorical variables as n (%). OHIP: Oral Health Impact Profile; UCLA: University of California, Los Angeles; CDC HRQOL-4: Centers for Disease Control and Prevention Health-Related Quality of Life.
| Variables | Categories | n (%) /average ± SD |
|---|---|---|
| OHIP-14 score | 3.8 ± 6.9* | |
| Oral health status | ||
| Number of tooth loss | None | 7,553 (50.1)† |
| 1~5 | 6,903 (45.8) | |
| 10 or more | 612 (4.1) | |
| Periodontal disease | None | 13,346 (88.6) |
| Yes | 1,722 (11.4) | |
| Oral pain | None | 13,379 (88.8) |
| Yes | 1,689 (11.2) | |
| Dental visits within 1 year | Yes | 9,010 (59.8) |
| None | 6,058 (40.2) | |
| Covariates | ||
| Age (years) | 51.9 ± 16.8 | |
| Gender | Male | 7,715 (51.2) |
| Female | 7,353 (48.8) | |
| Years of Education (years) | 14.4 ± 2.0 | |
| Annual income | < 3 million yen | 2,560 (21.0) |
| 3-6 million yen | 4,819 (39.6) | |
| 6-9 million yen | 2,631 (21.6) | |
| >9 million yen | 2,155 (17.7) | |
| Smokin history | Never | 9,439 (62.6) |
| Past | 3,058 (20.3) | |
| Currently | 2,571 (17.1) | |
| Excessive alcohol intake | None | 13,795 (91.6) |
| Yes | 1,273 (8.4) | |
| Number of diseases | 0.6 ± 1.0 | |
| Participation in hobbies, study, and culture-related activities | Nonparticipation | 13,112 (87.0) |
| Participation | 1,956 (13.0) | |
| Walking ≥1 hour/day or equivalent physical activity | Yes | 6,096 (40.5) |
| No | 8,972 (59.5) | |
| Relationship with Neighbors | None | 8,338 (55.3) |
| Yes | 6,730 (44.7) | |
| Chatting/mingling with non-family members | None | 2,962 (19.7) |
| Yes | 12,106 (80.3) | |
| Sitting ≥240 minutes/day | Yes | 5,639 (38.7) |
| None | 8,924 (61.3) | |
| Loss of spouse | None | 13,627 (90.4) |
| Yes | 1,441 (9.6) | |
| Financial situation up to age 18 | Not poor | 11,852 (78.7) |
| Poor | 3,216 (21.3) | |
| Abuse experience up to age 18 | None | 12,606 (83.7) |
| Yes | 2,462 (16.3) | |
| Frequency of eating alone | <1 time/week | 6,005 (39.9) |
| 1-5 times/week | 4,768 (31.6) | |
| 6-7 times/week | 4,295 (28.5) | |
| Habitual use of sleeping pills/anxiolytics | No | 13,911 (92.3) |
| Past use | 354 (2.3) | |
| Current use | 803 (5.3) | |
| Family social capital | 14.6 ± 6.1 | |
| UCLA Loneliness Scale (3-item) | 5.4 ± 2.6 | |
| Risk of social isolation | None | 8,686 (57.6) |
| Yes | 6,382 (42.4) | |
| CDC HRQOL-4 | Good | 14,650 (97.2) |
| Poor | 418 (2.8) | |
| Life satisfaction | 7.4 ± 2.3 |
*: average±SD, †: n(%).
Table 3.
Comparison of depressed and healthy groups by each indicator. Baseline characteristics and oral health-related variables compared between participants who developed depression and those who did not during follow-up. Continuous variables are presented as mean ± standard deviation (SD), and categorical variables as n (%). Statistical tests: Student’s t-test for continuous variables (‡) and Chi-square test for categorical variables (§).OHIP: Oral Health Impact Profile; UCLA: University of California, Los Angeles; LSNS: Lubben Social Network Scale; CDC HRQOL-4: Centers for Disease Control and Prevention Health-Related Quality of Life.
Table 3.
Comparison of depressed and healthy groups by each indicator. Baseline characteristics and oral health-related variables compared between participants who developed depression and those who did not during follow-up. Continuous variables are presented as mean ± standard deviation (SD), and categorical variables as n (%). Statistical tests: Student’s t-test for continuous variables (‡) and Chi-square test for categorical variables (§).OHIP: Oral Health Impact Profile; UCLA: University of California, Los Angeles; LSNS: Lubben Social Network Scale; CDC HRQOL-4: Centers for Disease Control and Prevention Health-Related Quality of Life.
| Without developed depression group (n=14850) |
With developed depression group (n=218) |
P value | ||
|---|---|---|---|---|
| OHIP-14 score | 3.7 ± 6.9* | 6.0 ± 9.0 | <0.001‡ | |
| Oral health status | ||||
| Number of tooth loss | None | 7437 (50.1)† | 116 (53.2) | 0.471§ |
| 1~5 | 6807 (45.8) | 96 (44.0) | ||
| 10 or more | 606 (4.1) | 6 (2.8) | ||
| Periodontal disease | None | 13157 (88.6) | 189 (86.7) | 0.393 |
| Yes | 1693 (11.4) | 29 (13.3) | ||
| Oral pain | None | 13193 (88.8) | 186 (85.3) | 0.101 |
| Yes | 1657 (11.2) | 32 (14.7) | ||
| Dental visits within 1 year | Yes | 8894 (59.9) | 116 (53.2) | 0.051 |
| None | 5956 (40.1) | 102 (46.8) | ||
| Covariates | ||||
| Age (years) | 52.0 ± 16.8 | 43.9 ± 15.3 | <0.001 | |
| Gender | Male | 7590 (51.1) | 125 (57.3) | 0.076 |
| Female | 7260 (48.9) | 93 (42.7) | ||
| Years of Education (years) | 14.4 ± 2.0 | 14.2 ± 2.1 | 0.262 | |
| Annual income | < 3 million yen | 2513 (21.0) | 47 (26.6) | 0.082 |
| 3-6 million yen | 4746 (39.6) | 73 (41.2) | ||
| 6-9 million yen | 2605 (21.7) | 26 (14.7) | ||
| >9 million yen | 2124 (17.7) | 31 (17.5) | ||
| Smoking history | Never | 9317 (62.7) | 122 (56.0) | 0.009 |
| Past | 3016 (20.3) | 42 (19.3) | ||
| Currently | 2517 (16.9) | 54 (24.8) | ||
| Excessive alcohol intake | None | 13597 (91.6) | 198 (90.8) | 0.724 |
| Yes | 1253 (8.4) | 20 (9.2) | ||
| Number of diseases | 0.6 ± 1.0 | 0.8 ± 1.6 | 0.960 | |
| Participation in hobbies, study, and culture-related activities | Nonparticipation | 12943 (87.2) | 169 (77.5) | <0.001 |
| Participation | 1907 (12.8) | 49 (22.5) | ||
| Walking ≥1 hour/day or equivalent physical activity | Yes | 6025 (40.6) | 71 (32.6) | 0.019 |
| No | 8825 (59.4) | 147 (67.4) | ||
| Relationship with Neighbors | None | 8205 (55.3) | 133 (61.0) | 0.100 |
| Yes | 6645 (44.7) | 85 (39.0) | ||
| Chatting/mingling with non-family members | None | 2902 (19.5) | 60 (27.5) | 0.004 |
| Yes | 11948 (80.5) | 158 (72.5) | ||
| Sitting ≥240 minutes/day | Yes | 5549 (38.7) | 90 (43.3) | 0.174 |
| None | 8806 (61.3) | 118 (56.7) | ||
| Loss of spouse | None | 13428 (90.4) | 199 (91.3) | 0.805 |
| Yes | 1422 (9.6) | 19 (8.7) | ||
| Financial situation up to age 18 | Not poor | 11695 (78.8) | 157 (72.0) | 0.018 |
| Poor | 3155 (21.2) | 61 (28.0) | ||
| Abuse experience up to age 18 | None | 12456 (83.9) | 150 (68.6) | <0.001 |
| Yes | 2394 (16.1) | 68 (31.2) | ||
| frequency of eating alone | <1 time/week | 5949 (40.1) | 56 (25.7) | <0.001 |
| 1-5 times/week | 4683 (31.5) | 85 (39.0) | ||
| 6-7 times/week | 4218 (28.4) | 77 (35.3) | ||
| Habitual use of sleeping pills/anxiolytics | No | 13749 (92.6) | 162 (74.3) | <0.001 |
| Past use | 340 (2.3) | 14 (6.4) | ||
| Current use | 761 (5.1) | 42 (19.3) | ||
| Family social capital | 14.6 ± 6.1 | 17.3 ± 6.9 | <0.001 | |
| UCLA Loneliness Scale (3-item) | 5.4 ± 2.6 | 7.7 ± 3.0 | <0.001 | |
| Risk of social isolation | None | 6322 (42.6) | 60 (27.5) | <0.001 |
| Yes | 8528 (57.4) | 158 (72.5) | ||
| CDC HRQOL-4 | Good | 14468 (97.4) | 162 (83.5) | <0.001 |
| Poor | 382 (2.6) | 36 (16.5) | ||
| Life satisfaction | 7.4 ± 2.3 | 5.6 ± 2.8 | <0.001 | |
*: Mean ± SD; †: n (%); ‡: Student’s t-test; §: Chi-square test.
Table 4.
Binomial logistic regression analysis with developed depression as dependent variable. Odds ratios (ORs) and 95% confidence intervals (CIs) for factors associated with the development of depression, adjusted for sociodemographic and behavioral covariates. OHIP = Oral Health Impact Profile; UCLA = University of California, Los Angeles; LSNS = Lubben Social Network Scale; CDC HRQOL-4 = Centers for Disease Control and Prevention Health-Related Quality of Life; Ref = Reference category.
Table 4.
Binomial logistic regression analysis with developed depression as dependent variable. Odds ratios (ORs) and 95% confidence intervals (CIs) for factors associated with the development of depression, adjusted for sociodemographic and behavioral covariates. OHIP = Oral Health Impact Profile; UCLA = University of California, Los Angeles; LSNS = Lubben Social Network Scale; CDC HRQOL-4 = Centers for Disease Control and Prevention Health-Related Quality of Life; Ref = Reference category.
| Independent variable | Category | Odds Ratio | 95% CI | p-value |
|---|---|---|---|---|
| OHIP-14 score | — | 1.02 | 1.00-1.04 | 0.039 |
| Dental visits within 1 year | Yes (Ref) | — | ||
| None | 1.17 | 0.85-1.60 | 0.329 | |
| Age (years) | — | 0.97 | 0.96-0.99 | <0.001 |
| Gender | Male (Ref) | — | ||
| Female | 1.08 | 0.78-1.52 | 0.637 | |
| Annual income | >9 million yen (Ref) | — | ||
| 6–9 million yen | 0.64 | 0.38-1.10 | 0.106 | |
| 3–6 million yen | 0.97 | 0.62-1.51 | 0.883 | |
| <3 million yen | 1.07 | 0.65-1.77 | 0.787 | |
| Smoking history | Never (Ref) | — | ||
| Past | 1.28 | 0.83-1.96 | 0.268 | |
| Current | 1.28 | 0.86-1.92 | 0.221 | |
| Participation in hobbies, study, and culture-related activities | Nonparticipation (Ref) | — | ||
| Participation | 2.22 | 1.50-3.30 | <0.001 | |
| Walking ≥1 hour/day or equivalent physical activity | Yes (Ref) | — | ||
| No | 0.96 | 0.69-1.32 | 0.783 | |
| Chatting/mingling with non-family members | None (Ref) | — | ||
| Yes | 1.05 | 0.72-1.55 | 0.788 | |
| Financial situation up to age 18 | Not poor (Ref) | — | ||
| Poor | 0.97 | 0.67-1.41 | 0.864 | |
| Abuse experience up to age 18 | None (Ref) | — | ||
| Yes | 1.09 | 0.75-1.59 | 0.653 | |
| Frequency of eating alone | <1 time/week (Ref) | — | ||
| 1–5 times/week | 1.41 | 0.96-2.08 | 0.084 | |
| 6–7 times/week | 0.87 | 0.56-1.34 | 0.518 | |
| Habitual use of sleeping pills/anxiolytics | No (Ref) | — | ||
| Past use | 1.97 | 1.06-3.68 | 0.033 | |
| Current use | 3.51 | 2.27-5.44 | <0.001 | |
| Family social capital | — | 1.01 | 0.98-1.03 | 0.715 |
| UCLA Loneliness Scale (3-item) | — | 1.22 | 1.14-1.30 | <0.001 |
| Risk of social isolation | None (Ref) | — | ||
| Yes | 1.17 | 0.81-1.68 | 0.408 | |
| CDC HRQOL-4 | Good (Ref) | — | ||
| Poor | 2.92 | 1.81-4.72 | <0.001 | |
| Life satisfaction | — | 0.90 | 0.84-0.97 | 0.005 |
OR = Odds Ratio; CI = Confidence Interval.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



