Submitted:
04 November 2025
Posted:
05 November 2025
You are already at the latest version
Abstract
Background: Healthcare systems generate nearly 4.4% of global greenhouse gas (GHG) emissions, making the transition toward low-carbon and circular economy models an urgent sustainability challenge. Public hospitals, as large energy and resource consumers, hold a strategic role in mitigating environmental impact and achieving the goals of the European Green Deal. Aim: This study develops and tests a reproducible methodological framework—the HULA Circular Decarbonization Model (HCDM)—designed to integrate circular economy principles into hospital operations and align institutional performance with carbon neutrality targets. Methods: The model was implemented at the Hospital Universitario Lucus Augusti (Spain) following the international GHG Protocol (Scopes 1–3) and ISO 14001 standards. It operationalizes decarbonization through five iterative axes: energy efficiency, clinical emissions control, waste and circular resource management, sustainable mobility, and governance engagement. The process followed a Plan–Do–Check–Act cycle with continuous monitoring of environmental indicators. Results: Between 2021 and 2023, total emissions were reduced by 35%, including a 95% decrease in anesthetic gases and a 17% reduction in plastic waste. The integrated strategy proved technically feasible and economically viable within a publicly funded system, fostering organizational awareness and interdisciplinary participation. Conclusions: The HCDM demonstrates that hospital-level decarbonization can be achieved through structured, low-cost, and replicable interventions. Policy implications: This model offers a transferable framework for public health systems seeking alignment with the European Green Deal, the WHO COP28 Health Report, and the UN 2030 Agenda, advancing the decarbonization of healthcare through circular economy innovation.
Keywords:
1. Introduction
2. Materials and Methods
2.1. Study Design and Conceptual Approach
2.2. Data Collection and Carbon Accounting
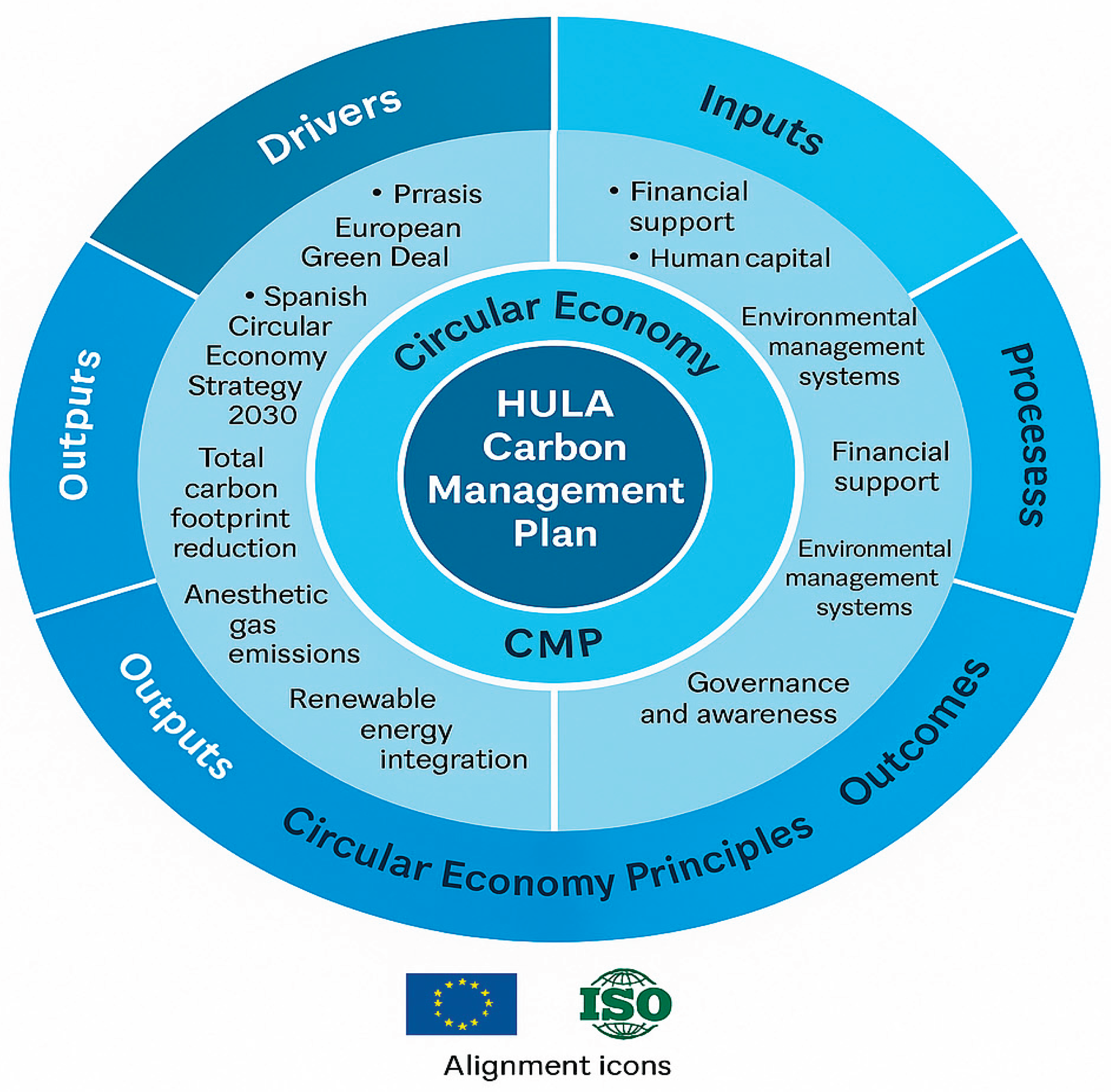
2.3. The HULA Circular Decarbonization Model (HCDM)
- Energy and infrastructure: efficiency and photovoltaic self-consumption.
- Clinical emissions: anesthetic gas capture and sustainable prescribing.
- Waste and circular economy: plastic reduction and food waste prevention.
- Mobility and logistics: low-emission transport and supply-chain optimization.
- Governance and awareness: capacity-building and staff engagement.
2.4. Implementation and Monitoring
2.5. Data Analysis and Model Validation
3. Results
3.1. Overall carbon footprint reduction
3.2. Key decarbonization projects
Organizational outcomes and awareness
4. Discussion
4.1. Lessons Learned from Implementation
4.2. Integrating Circular Economy Principles into Healthcare
4.3. Governance, Engagement, and Policy Alignment
4.4. International Context and Comparative Insights
4.5. Challenges and Future Directions
5. Conclusions
Relevance statement
References
- Pichler PP, Jaccard IS, Weisz U, Weisz H. International comparison of healthcare carbon footprints. Environ Res Lett. 2019;14(6):064004. [CrossRef]
- United Nations. Paris Agreement of the United Nations Framework Convention on Climate Change (UNFCCC). 2015. Available at: https://unfccc.int/sites/default/files/english_paris_agreement.pdf.
- European Commission. The European Green Deal. COM(2019) 640 final. 2019. https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX:52019DC0640.
- Eckelman MJ, Sherman JD. Environmental impacts of the US health care system and effects on public health. PLoS One. 2016;11(6):e0157014. [CrossRef]
- Rodríguez-Jiménez L, González-Díaz C, Álvarez-Martín E, et al. The carbon footprint of healthcare settings: a systematic review. J Adv Nurs. 2023;79(12):e1–e20. [CrossRef]
- Health Care Without Harm (HCWH). Health Care’s Climate Footprint: How the Health Sector Contributes to the Global Climate Crisis and Opportunities for Action. Brussels: HCWH Europe; 2019. https://noharm-global.org/documents/health-cares-climate-footprint.
- Kirchherr J, Reike D, Hekkert M. Conceptualizing the circular economy: an analysis of 114 definitions. Resour Conserv Recycl. 2017;127:221–232. [CrossRef]
- D’Alessandro C, Bianchi G, Romano A, et al. Circular economy practices in the healthcare sector: a comprehensive review. Sustainability. 2024;16(1):401. [CrossRef]
- Rizan C, Bhutta MF, Reed M, Lillywhite R. The carbon footprint of waste streams in a UK hospital. J Clean Prod. 2021;286:125446. [CrossRef]
- Orsini LP, Del Giudice M, Marra A, et al. Towards greener hospitals: the effect of green practices on hospital performance. J Clean Prod. 2024;441:140987. [CrossRef]
- Bizzarri G, Morini GL. New technologies for an effective energy retrofit of hospitals: results of a case study. Energy Build. 2006;38(10):1130–1139. [CrossRef]
- De Masi RF, Palumbo A, Clemente C, et al. Energy retrofit design optimization for hospitals in Mediterranean climate: a multistage approach. Sustainability. 2023;15(14):11450. [CrossRef]
- Aquino ACT de, Menezes PR, Carmo AC. Healthcare waste and circular economy principles: it is time for action. Int J Environ Res Public Health. 2024;21(7):792. [CrossRef]
- Andersen MPS, Molander L, Shah A, et al. The climate impact of inhalational anaesthetic gases: a review. Lancet Planet Health. 2023;7(8):e667–e676. [CrossRef]
- Ministerio para la Transición Ecológica y el Reto Demográfico. Estrategia Española de Economía Circular: España Circular 2030. Madrid: Gobierno de España; 2020. https://www.miteco.gob.es/es/.
- Xunta de Galicia. Estrategia Gallega de Economía Circular 2020–2030. Santiago de Compostela: Xunta de Galicia; 2019. https://medioambiente.xunta.gal.
- World Health Organization (WHO). COP28 Special Report on Climate Change and Health. Geneva: WHO; 2023. https://www.who.int/publications/i/item/cop28-special-report.
- Mermillod B, Faye B, Hernandez D, et al. Estimating the carbon footprint of healthcare in France. Int J Environ Res Public Health. 2024;21(6):690. [CrossRef]
- van Straten B, Butler P, van den Dobbelsteen J, et al. Towards circular hospitals: feasibility of reusing surgical stainless-steel instruments. Sustain Mater Technol. 2021;29:e00297. [CrossRef]
- Reuters. Big Pharma pulls together to shrink healthcare’s outsized carbon footprint. 14 Feb 2024. https://www.reuters.com/sustainability/big-pharma-carbon-footprint-2024-02-14.

| Phase | Core Actions | Expected Outcomes |
|---|---|---|
| 1. Institutional Commitment | Formation of a multidisciplinary Carbon Management Team; integration of circular principles into hospital governance. | Governance structure and policy alignment. |
| 2. Baseline Assessment | Comprehensive quantification of Scopes 1–3 emissions following GHG Protocol; ISO 14,001 validation. | Verified carbon inventory. |
| 3. Strategic Design | Development of the Carbon Management Plan (CMP) with measurable targets (Scope 1: −16% by 2025; Scope 3: −19% by 2030); identification of operational axes. | Strategic roadmap for emission reduction. |
| 4. Implementation | Deployment of prioritized interventions in energy efficiency, anesthetic gas recovery, waste valorization, mobility, and green procurement. | Tangible carbon reduction and circular resource use. |
| 5. Monitoring and Continuous Improvement | Evaluation under the Plan–Do–Check–Act cycle; annual reporting to hospital management and regional health authorities. | Verified performance indicators and feedback loop. |
| Indicator | 2021 (Baseline) | 2023 | Change (%) | Main Contributing Actions |
|---|---|---|---|---|
| Total GHG emissions (tCO2e) | 7,262.9 | 4,687.1 | −35.4 | Implementation of Carbon Management Plan; energy efficiency upgrades; renewable electricity supply |
| Scope 1 emissions (tCO2e) | 6,459.7 | 4,116.6 | −36.3 | Reduction of stationary combustion and anesthetic gas recovery system (Contrafluran®) |
| Scope 2 emissions (tCO2e) | 0 | 0 | – | 100 % renewable electricity from certified supplier |
| Scope 3 emissions (tCO2e) | 803.3 | 570.6 | −29.0 | Waste reduction, green procurement, food waste prevention program |
| Plastic waste reduction (t/year) | – | −30 | – | Reusable containers, elimination of single-use items, textile logistics |
| Anesthetic gas emissions (tCO2e) | 367 | 17 | −95 | Activated-carbon capture system (Contrafluran®) and low-flow anesthesia |
| Paper consumption (kg) | 100 % baseline | 59 % | −41 | “Paperless Hospital” project (Escriba digital forms) |
| Renewable energy capacity (kW) | 0 | 997.9 | +997.9 | Installation of photovoltaic panels (INEGA program) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



