Submitted:
03 November 2025
Posted:
04 November 2025
You are already at the latest version
Abstract
Background/Objectives: Genital discomfort, manifested by vulvar itching and burning, is a frequent complaint among women of all ages and has multifactorial origins—including dermatoses, infections, allergies, and hormonal disorders. The study aimed to determine whether selected medical history factors—age, obstetric history, and body mass index (BMI)—influence the frequency of genital discomfort as a reason for gynecological consultation. Methods: A pilot study included 288 female patients aged 11–91 years who presented to outpatient gynecological clinics between September 2018 and February 2025 with symptoms of vulvar itching and genital discomfort. Qualitative data were expressed as numbers and percentages, and age was described using mean, median, quartiles, and range. Associations between categorical variables were assessed using Pearson’s chi-square test, with statistical significance set at p < 0.05. Results: The mean age of patients was 47.4 ± 20.3 years. Most were diagnosed with ICD-10 code N90 (82.6%), while 17.4% had N76. Genital discomfort was most frequently reported by women aged 41–50 years (p < 0.0001). Comorbidities (p < 0.0001) and obstetric history (p < 0.0001) significantly influenced the occurrence of genital discomfort, which was more prevalent among women with chronic conditions and those who had been pregnant. No significant associations were found with BMI (p = 0.2353) or menopausal status (p = 0.3458). Conclusions: Genital discomfort is a common and multifactorial condition requiring an interdisciplinary diagnostic and therapeutic approach. Collaboration among gynecologists, dermatologists, endocrinologists, and dietitians is crucial for effective management and prevention.
Keywords:
vulvar diseases
; pruritus vulvae
; genital diseases
; female
; gynecology
1. Introduction
In contemporary gynecology, a holistic approach that also includes aspects of sexual health is increasingly recommended for many clinical issues. Preventive measures such as maintaining a healthy lifestyle, physical activity, and appropriate diet play a significant role, with particular emphasis placed on dietotherapy—for example, in the context of the interdisciplinary nature of genital discomfort.
Vulvar discomfort, manifested by itching or burning sensations in the intimate area, reduces the quality of life of girls and women regardless of age [1]. In sexually active women, it is associated with dyspareunia and decreased libido, becoming a partnership problem that often requires sexological couples therapy [2]. In postmenopausal and elderly patients, due to the risk of vulvar cancer, it is not only a gynecological or geriatric issue but also an important dermatological and oncological concern [3].
The problem of genital discomfort may have multiple causes—from dermatoses, fungal and bacterial infections, and allergies, to hormonal disorders—and it affects patients of all ages, becoming a significant issue also in developmental-age gynecology (also referred to as pediatric and adolescent gynecology) [2,4,5].
The pilot study included 288 gynecological patients aged 11 to 91 years who presented to outpatient clinics with symptoms of vulvar itching and genital discomfort. All patients reported discomfort. It should be emphasized that this study did not analyze the subgroup of girls attending pediatric gynecology clinics, in whom such discomfort was an additional but not the primary problem; this group was analyzed separately in another study.
In the pilot analysis, typical correlations between discomfort and variables such as age group, comorbidities, pregnancy status, BMI (underweight/normal/overweight/obese), or menopausal status (<48 years / ≥48 years) were not examined. Instead, an attempt was made to determine whether any specific subcategory predominated among the studied gynecological patients. The patients underwent further diagnostic evaluation, including sexological and dermatological consultations. However, the results of these further diagnostic assessments are not the subject of this pilot report. It is worth emphasizing, nevertheless, the interdisciplinary nature of this issue.
Given the widespread nature of the problem of genital discomfort (vulvar itching), the aim of this study was to determine whether, and to what extent, selected factors from the medical history—such as age, obstetric history, and body mass index (BMI)—influence the frequency of this condition as a reason for visiting a gynecologist.
2. Materials and Methods
The study included 288 gynecological patients aged 11 to 91 years, who presented to outpatient clinics with symptoms of vulvar itching and genital discomfort between September 26, 2018, and February 18, 2025.
Qualitative data were described using numbers and frequencies, while age (in years) was characterized using the arithmetic mean, standard deviation (SD), median, lower quartile (Q25), upper quartile (Q75), minimum (Min.), and maximum (Max.) values.
To verify the equality of patient subgroup sizes, the Pearson chi-square test was applied.
A value of p < 0.05 was considered statistically significant. Statistical analyses were performed using the STATISTICA 10 PL software package.
3. Results
3.1. Characteristics of the Study Group
The patients’ ages ranged from 11 to 91 years. The mean age of the women was 47.4 ± 20.3 years. Half of the study participants were 46 years old or younger. Additionally, 25% of the patients were 30 years old or younger, while 75% were 67 years old or younger (Table 1).
In the vast majority of patients, the diagnosis was N90 – other noninflammatory disorders of the vulva and perineum, identified in 238 women (82.6%) (Table 2). The remaining patients were diagnosed with N76 – other inflammation of the vagina and vulva, observed in 50 women (17.4%).
3.2. Verification of Hypotheses
Is There a Relationship Between the Occurrence of Genital Discomfort and Patients’ Age or Comorbidities?
The Pearson chi-square test revealed a statistically significant difference in the distribution of women across age categories (p < 0.0001) (Table 3). The most numerous group consisted of women aged 41–50 years (Figure 1). Age was found to influence the occurrence of genital discomfort, which was most frequently reported by women aged 41–50 years and least frequently by women aged 81–91 years.
The Pearson chi-square test revealed a statistically significant difference between the number of women with comorbidities and those without such conditions (p < 0.0001) (Table 4). Women with comorbidities predominated in the study group (Figure 2). The presence of comorbidities was found to influence the occurrence of genital discomfort — women with comorbid conditions experienced genital discomfort more frequently.
Is There a Difference in the Frequency of Genital Discomfort Between Women Who Have Ever Been Pregnant and Those Who Have Not?
The Pearson chi-square test revealed a statistically significant difference between the number of women who had ever been pregnant and those who had never been pregnant (p < 0.0001) (Table 5). Women with a history of pregnancy predominated in the study group (Figure 3). Obstetric history was found to influence the occurrence of genital discomfort — women with a history of pregnancy experienced genital discomfort more frequently.
Is There a Relationship Between the Occurrence of Genital Discomfort and BMI?
The Pearson chi-square test did not reveal a statistically significant difference between the number of women with normal weight or underweight and those with overweight or obesity (p > 0.05) (Table 6) (Figure 4). BMI was not found to influence the occurrence of genital discomfort in the studied group of patients.
Is There a Relationship Between the Occurrence of Genital Discomfort and Menopausal Status (Before or After the Last Menstrual Period)?
Women were divided into two groups according to menopausal status: Yes (aged 48 years and older) and No (under 48 years of age) (Figure 5). The Pearson chi-square test did not show a statistically significant difference between the number of women in the menopausal group (≥48 years) and those in the premenopausal group (<48 years) (p > 0.05) (Table 7). Menopausal status was not found to influence the occurrence of genital discomfort among the studied patients.
4. Discussion
Genital discomfort, manifested by burning and vaginal irritation, is a condition that can significantly reduce the quality of life of girls and women. This problem affects patients of all ages and may have various etiologies—ranging from dermatoses, fungal and bacterial infections, and allergies to hormonal disorders. Although itching is usually transient and mild, in some cases it may indicate more complex and serious health problems, often associated with metabolic disturbances [1]. In this context, attention should also be drawn to the importance of probiotics, prebiotics, symbiotics, and dietotherapy, which play a role in maintaining genital health [6].
Genital discomfort and vulvar diseases represent conditions for which patients commonly seek consultation with gynecologists and dermatologists. The symptoms of vulvar disorders frequently require combined gynecological and dermatological management. A significant group in this regard consists of dermatoses that may involve not only the genital area—the vulva may be just one of several affected sites [7,8,9].
In sexually active women, genital discomfort is often associated with dyspareunia and reduced libido, becoming a relationship problem that may require sexological couples therapy [2]. In postmenopausal and elderly women, due to the risk of vulvar cancer, this condition represents not only a gynecological and geriatric issue but also a dermatological and oncological concern [3].
Genital discomfort, with its diverse causes—dermatoses, infections (fungal or bacterial), allergies, and hormonal disturbances—affects women across all age groups and constitutes an important problem also in developmental-age gynecology [5].
The pilot study included 288 gynecological patients aged 11 to 91 years who presented to outpatient clinics with symptoms of vulvar itching and genital discomfort. All patients reported the presence of discomfort. It should be emphasized that the study did not include a group of girls attending pediatric gynecology clinics, in whom such discomfort was an additional but not the primary reason for consultation; this subgroup was analyzed separately in another study.
In this pilot analysis, typical correlations between genital discomfort and variables such as age (age groups), comorbidities (yes/no), pregnancy history (yes/no), body mass index (underweight/normal/overweight/obese), or menopausal status (<48 years / ≥48 years) were not examined. Instead, the analysis focused on identifying whether any specific subcategory predominated among the gynecological patients studied. The participants underwent further diagnostic evaluation, including sexological and dermatological consultations; however, the results of those additional assessments are beyond the scope of this pilot report. It is worth underscoring once again the interdisciplinary character of this issue.
The discomfort experienced by the patients was characterized primarily by intense itching in the intimate area. This symptom could involve both the vaginal interior and the external parts of the vulva, such as the labia, clitoris, and vestibule of the vagina. The itching sensation could make sitting uncomfortable, cause distraction, provoke scratching, and—as emphasized—may even prevent sexual activity. The discomfort was often accompanied by burning, skin irritation, and changes in vaginal discharge, all of which may significantly affect a woman’s well-being and daily quality of life. A more detailed differentiation of these symptoms is planned for subsequent analyses.
It should be reiterated that genital discomfort as a gynecological complaint may result from minor irritations, but can also be a sign of more serious health conditions requiring diagnosis and treatment. It may be a manifestation of dermatoses [5,7,8,9], hypoestrogenism typical of postmenopausal and senium periods [3], or various medical disorders, including fungal and bacterial infections [10], allergies, endocrine diseases [11] and vulvodynia [12].
Although the applied therapy in the studied patients was not the subject of analysis, it is important to emphasize that in order to select an appropriate treatment, it is essential to determine which microorganism is responsible for the symptoms. This requires a detailed medical history, including information about other symptoms accompanying the itching—such as the type of discharge, presence of pain, and skin changes in the intimate area. It is also necessary to perform appropriate diagnostic tests and, when indicated, refer patients for specialist consultations, including dermatology, oncology, and other relevant disciplines [1].
In some patients, genital discomfort and intense itching of the vagina and vulva are the only noticeable symptoms of an allergy or genital infection. However, the vast majority of women experience additional symptoms, such as:
- Redness in the intimate area, including the labia, clitoral region, and vaginal introitus,
- Swelling of both the minor and major labia,
- Pain and tenderness in the genital area, particularly during intercourse, washing, or touch,
- Vaginal discharge with unpleasant odor, abnormal consistency (e.g., curd-like or foamy), or color (white, gray, greenish),
- Burning sensation during urination and increased urinary frequency,
- Nighttime discomfort associated with itching and urgency,
- Postcoital vaginal itching,
Genital discomfort and the accompanying itching may have numerous causes, which can be broadly divided into infectious and non-infectious origins. The most important among them include:
- Allergic reactions to components present in products such as sanitary pads, panty liners, or tampons—especially those containing fragrances or dyes. Allergies may also be triggered by the materials used in underwear, particularly synthetic, non-breathable fabrics. In addition, laundry detergents, including strongly perfumed washing powders and fabric softeners, may provoke allergic irritation [5,10].
- Fungal infection (candidiasis, yeast infection) of the vagina: it is estimated that up to 75% of women experience vaginal and vulvar candidiasis at least once in their lifetime, and approximately 40–50% of cases are recurrent. The infection is most often caused by Candida albicans, responsible for 80–92% of cases. Symptoms include white, curd-like discharge, irritation of the vaginal and vulvar mucosa, swelling, pain, and intense itching, particularly during sexual intercourse and urination. Predisposing factors include pregnancy, diabetes, obesity, antibiotic or corticosteroid therapy, immunosuppression, hormonal disturbances, poor hygiene, and the use of intrauterine devices (IUDs) [1,6,10,14].
- Trichomoniasis, an infection caused by Trichomonas vaginalis, manifests as profuse, frothy, greenish vaginal discharge with a foul, musty odor, pain during urination, burning, dyspareunia (pain during intercourse), and swelling of the vagina and vulva. In severe cases, the swelling may be so pronounced that it impedes sexual intercourse or gynecological examination. Trichomoniasis is primarily sexually transmitted [1,10,14].
- Bacterial infection – bacterial vaginosis: in such cases, itching is usually mild, but there is a characteristic fishy odor of the vaginal discharge. The condition results from an imbalance in the vaginal microbiota and excessive proliferation of anaerobic bacteria, such as Prevotella spp., Gardnerella vaginalis, and Mycoplasma hominis [1,10,14].
- Another important risk factor, as analyzed, is obstetric history, with multiparity playing a notable role.
- Viral infections caused by herpes simplex virus type 2 (HSV-2)—less commonly HSV-1—lead to genital herpes. Early symptoms include pain, burning, and itching, followed by redness, vesicles, and ulcerations. The disease is often accompanied by painful urination, vaginal discharge, joint and muscle pain, and fever. Symptoms may persist for several weeks, and the infection tends to recur. Genital herpes is particularly dangerous during pregnancy, as it can lead to preterm delivery and neonatal infection [14].
- Hormonal changes, occurring particularly during the perimenopausal and senium periods, have been shown to play a significant role. A low level of estrogens may lead to atrophy of the vaginal and vulvar mucosa. As a result, the epithelium becomes thinner, less hydrated, and more prone to irritation, leading to dryness, burning, and itching. Contact spotting and dyspareunia may also occur. A reduced estrogen level increases vaginal pH, thereby raising the risk of infection. Treatment includes estrogen supplementation, the use of moisturizing preparations, and attention to proper hygiene and lifestyle, including smoking cessation [3].
- Other, less common causes of vaginal itching (not analyzed in this study) include: mechanical irritation, e.g., during sexual intercourse or the use of erotic devices; excessive hygiene practices, leading to dryness of the intimate area, including vaginal douching; sexually transmitted diseases (STDs) such as chlamydia, genital herpes, HPV (condylomata acuminata), gonorrhea, and others [14], which can cause characteristic symptoms including skin lesions, abnormal discharge, and persistent itching; hemorrhoids, whose itching and irritation may extend to the vaginal area; dermatoses such as lichen sclerosus [17], psoriasis, or atopic dermatitis, which can manifest with itching of the intimate regions; diabetes mellitus [18], which increases susceptibility to fungal infections due to altered microflora and elevated glucose levels promoting yeast growth; chronic stress and emotional tension, which may affect the skin and mucous membranes, leading to itching; and vulvar cancer, which may present with severe itching, nodules, or ulcerations in the vulvar region.
It should be emphasized that in all these contexts, the cooperation between gynecologists and dermatologists is of particular importance.
Failure to undertake diagnosis and treatment of conditions associated with genital discomfort may lead to serious and irreversible consequences, which tend to worsen the longer the problem persists. It is essential to emphasize the need for histopathological verification of vulvar skin lesions, especially in postmenopausal and elderly patients, as this stage of life carries an increased risk not only of dystrophic changes but also of vulvar cancer [3].
Another non-oncological concern is that inflammatory processes, particularly those of bacterial origin, may spread to the urethra, cervix, and fallopian tubes, leading to adhesion formation and, consequently, infertility [19]. Untreated genital infections may also result in the development of pelvic abscesses, which often require surgical intervention, since conservative antibiotic therapy is usually insufficient in such cases.
During a gynecological consultation, a detailed medical history is crucial, with attention paid to the circumstances under which symptoms occur, their intensity, duration, and any additional manifestations related to sexual activity. A thorough examination of the vulva and vagina using a speculum is necessary, with a focus on redness, mucocutaneous changes, and the character of vaginal discharge. It is also important to perform a transvaginal ultrasound (TVUS) and collect a vaginal swab for cytology, as well as refer the patient for blood or urine tests and, when indicated, specialist consultations, particularly dermatologicts [1].
The treatment of genital discomfort depends on its underlying cause. If symptoms appear after the introduction of new hygienic or washing products, their use should be immediately discontinued; in many cases, symptoms will resolve spontaneously. If they persist, oral antihistamines may be indicated [5].
In cases of candidiasis, topical antifungal creams or vaginal suppositories are used, and in more severe cases, oral antifungal therapy may be required for a longer duration. Bacterial infections are treated with metronidazole, administered both orally and topically. Trichomoniasis is treated with antiprotozoal agents, such as nifuratel [1].
In the case of genital herpes, no treatment can completely eliminate the virus; however, during exacerbations, antiviral medications such as acyclovir are used to inhibit viral replication [1,14].
Itching resulting from vulvar dystrophy, caused by a decrease in estrogen levels during the perimenopausal and senium periods, can be alleviated with creams, tablets, or vaginal rings containing estriol. If the itching is due to insufficient lubrication leading to microtraumas and abrasions, the use of moisturizing and mucosal-regenerating preparations is recommended—these most often contain hyaluronic acid or its salts and are available in the form of vaginal suppositories, creams, or gels [3].
In other cases of irritation and itching, such as those caused by lichen sclerosus, topical steroid therapy may be necessary.
In terms of prevention, it is important to follow basic hygiene principles: intimate areas should be washed at least twice daily with neutral cleansing agents, and sanitary pads or panty liners should be changed regularly. It is also advisable to increase the consumption of dairy products, which are a natural source of probiotics that support the colonization of beneficial bacteria [6].
During treatment of genital infections, alcohol consumption should be avoided, and sexual abstinence is recommended; in some cases, simultaneous treatment of the partner may be necessary.
Symptoms such as discomfort, itching of the vulva and vagina tend to recur, which highlights the importance of preventive measures, including:
- Using gentle, hypoallergenic intimate hygiene products that do not cause irritation, while avoiding excessive hygiene practices (especially vaginal douching), which may disturb the natural microbiota;
- Avoiding perfumed cosmetics, toilet paper, and sanitary products, as well as potential allergens such as new laundry detergents;
- Using pads instead of tampons, particularly during the last days of menstruation;
- Washing the perineal area with warm water, always from the vaginal vestibule toward the anus;
- Wiping from front to back after bowel movements;
- Avoiding prolonged moisture in the genital area, such as sitting in a wet swimsuit;
- Wearing loose, breathable cotton underwear [10];
- Using condoms during sexual intercourse [14];
- Taking probiotics to support the restoration of the vaginal microbiota [6];
- Applying gentle vaginal moisturizers, such as vaginal suppositories [1].
5. Conclusions
Genital discomfort is an important issue not only in the field of gynecology, but one that also requires close collaboration with specialists in dermatology, internal medicine, diabetology, dietetics, and, in some cases, oncology.
Author Contributions
Conceptualization, G.J.B., A.P. and M.P; methodology, K.P.G.; validation, A.P, M.P., Y.Y; formal analysis, G.J.P, W.K.; investigation, M.M, M.P.K, J.M.; resources, W.K.; data curation, A.P., M.P.; writing—original draft preparation, G.J.B, K.P.R, M.M, M.P,K, J.M.; writing—review and editing, A.P.; supervision, G.J.B, W.K.; project administration, G.J.B.; funding acquisition, G.J.P, W.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding. Funding is sourced from the resources of the Department of Gyneacology.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. The study did not meet the criteria of a medical experiment and was therefore exempt from approval by the Bioethics Committee.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The original data presented in the study are openly available in Zenodo at: https://doi.org/10.5281/zenodo.17469511 (published on 28th October 2005).
Conflicts of Interest
The authors declare no conflicts of interest.
References
- American College of Obstetricians and Gynecologists (ACOG). Vaginitis in Nonpregnant Patients: ACOG Practice Bulletin, Number 215. Obstet. Gynecol. 2020, 135(1), e1–e17. [CrossRef]
- Pawlaczyk, M.; Jarząbek, G.; Pawlaczyk, M.; Friebe, Z.; Ochmańska, K.; Kapczuk, K.; Sowińska-Przepiera, E. Inflammatory Conditions of the Vulva and Vagina (Vulvovaginitis) in Pediatric and Adolescent Patients. In Xth European Pediatric and Adolescent Gynecological Congress – Abstracts; Budapest, Hungary, 2006.
- Pawlaczyk, M.; Jarząbek-Bielecka, G. Vulvar Diseases in Postmenopausal Women. Prz. Derm. 2016, 103(Suppl. 1), S54.
- Jarząbek, G.; Pawlaczyk, M.; Pawlaczyk, M.; Friebe, Z.; Ochmańska, K.; Kapczuk, K.; Sowińska, E. Vulvar Diseases in Adolescent Girls. In 14th World Congress on Pediatric & Adolescent Gynecology “The Young Athlete Woman” – Final Programme & Book of Abstracts; Athens, Greece, 8–11 May 2004; p. 163.
- Pawlaczyk, M.; Jarząbek, G.; Pawlaczyk, M.; Friebe, Z.; Ochmańska, K.; Sowińska-Przepiera, E.; Kapczuk, K. Childhood Vulvar Dermatoses. J. Eur. Acad. Dermatol. Venereol. 2004, 18(Suppl. 2), 153.
- Mizgier, M.; Jarząbek-Bielecka, G.; Mruczyk, K.; Kędzia, W. The Role of Diet and Probiotics in the Prevention and Treatment of Bacterial Vaginosis and Vulvovaginal Candidiasis in Adolescent Girls and Nonpregnant Women. Ginekol. Pol. 2020, 91(7), 412–416. [CrossRef]
- Boroch, J.; Jarząbek-Bielecka, G.; Mizgier, M.; Pawlaczyk, M.; Pisarska-Krawczyk, M.; Wojtyła-Buciora, P.; Wojtyła, A.; Chuchracki, M.; Kędzia, W. Selected Dermatological and Gynecological Problems Including Some Dietary Aspects in Girls. Med. Rodz. 2018, 21(4), 344–348.
- Pawlaczyk, M.; Jarząbek-Bielecka, G.; Pawlaczyk, M.; Sowińska-Przepiera, E.; Ochmańska, K.; Kapczuk, K.; Friebe, Z. Inflammatory and Dermatological Conditions of the Vulva and Vagina in Girls. Ginekol. Prakt. 2006, 14(1), 16–18.
- Boroch, J.; Jarząbek-Bielecka, G.; Mizgier, M.; Pawlaczyk, M.; Pisarska-Krawczyk, M.; Wojtyła-Buciora, P.; Wojtyła, A.; Chuchracki, M.; Kędzia, W. Dermatological–Gynecological Problems in Girls with Emphasis on Dietary Aspects. Med. Rodz. 2018, 21(4), 344–348.
- Itriyeva, K. Evaluation of Vulvovaginitis in the Adolescent Patient. Curr. Probl. Pediatr. Adolesc. Health Care 2020, 50(7), 100836. [CrossRef]
- Mizgier, M.; Jarząbek-Bielecka, G.; Wendland, N.; Jodłowska-Siewert, E.; Nowicki, M.; Brożek, A.; Kędzia, W.; Formanowicz, D.; Opydo-Szymaczek, J. Relation between Inflammation, Oxidative Stress, and Macronutrient Intake in Normal and Overweight Adolescent Girls with Clinical Features of Polycystic Ovary Syndrome. Nutrients 2021, 13(3), 896. [CrossRef]
- Bergeron S, Reed BD, Wesselmann U, Bohm-Starke N. Vulvodynia. Nat Rev Dis Primers. 2020 Apr 30;6(1):36.
- Jarząbek-Bielecka, G.; Pawlaczyk, M.; Pawlaczyk, M.; Pawlaczyk, M.; Pisarska-Krawczyk, M.; Wojtyła-Buciora, P.; Mizgier, M.; Boroch, J.; Kędzia, W. Inflammatory Conditions of Female Genital Organs—Assessment of Girls’ Knowledge about Prevention and Treatment. Med. Rodz. 2018, 21(1A), 29–36.
- Skłodowska, A.; Pawlaczyk, M.; Jarząbek, G.; Friebe, Z.; Pawlaczyk, M. Clinical Aspects of Vulvovaginitis in Prepubertal Girls. Prz. Derm. 2011, 98(1), 48–49.
- Pawlaczyk, M.; Jarząbek, G.; Pawlaczyk, M.; Sowińska-Przepiera, E.; Ochmańska, K.; Kapczuk, K.; Friebe, Z. Inflammatory Diseases of the Vulva and Vagina (Vulvovaginitis) in Girls at Different Developmental Stages. Ginekol. Prakt. 2006, 14(1), 16–18.
- Jarząbek, G.; Pawlaczyk, M.; Pawlaczyk, M.; Friebe, Z.; Ochmańska, K.; Kapczuk, K.; Sowińska-Przepiera, E. Vulvovaginitis in Adolescent Girls. In Xth European Pediatric and Adolescent Gynecological Congress – Abstracts; Budapest, Hungary, 10–13 May 2006. Available online: http://www.new-instant.hu/pag/abstracts.html (accessed on 28 October 2025).
- Jarząbek-Bielecka, G.; Mizgier, M.; Boroch, J.; Pisarska-Krawczyk, M.; Pawlaczyk, M.; Jakubek, E.; Kędzia, W. Patient Suffering from Lichen Sclerosus Together with Partial Labial Fusion (Adhesion) and Inflammatory Infection of the Vulva, Vagina, and Anal Area. Clin. Exp. Obstet. Gynecol. 2020, 47(2), 315–319. [CrossRef]
- Mizgier, M.; Jarząbek-Bielecka, G.; Mruczyk, K.; Cisek-Woźniak, A. Maternal Diet and Gestational Diabetes Mellitus Development. In 6th International Conference on Nutrition and Growth – Abstract Book; Vaencia, Spain, 7–9 March 2019;. [CrossRef]
- Mizgier, M.; Jarząbek-Bielecka, G.; Mruczyk, K.; Kędzia, W. The Role of Obesity and Environmental Factors such as Diet and Physical Activity in the Etiopathogenesis of Fertility Disorders. Clin. Exp. Obstet. Gynecol. 2019, 46(4), 516–520. [CrossRef]
Figure 1.
Age Groups of Women Experiencing Genital Discomfort.
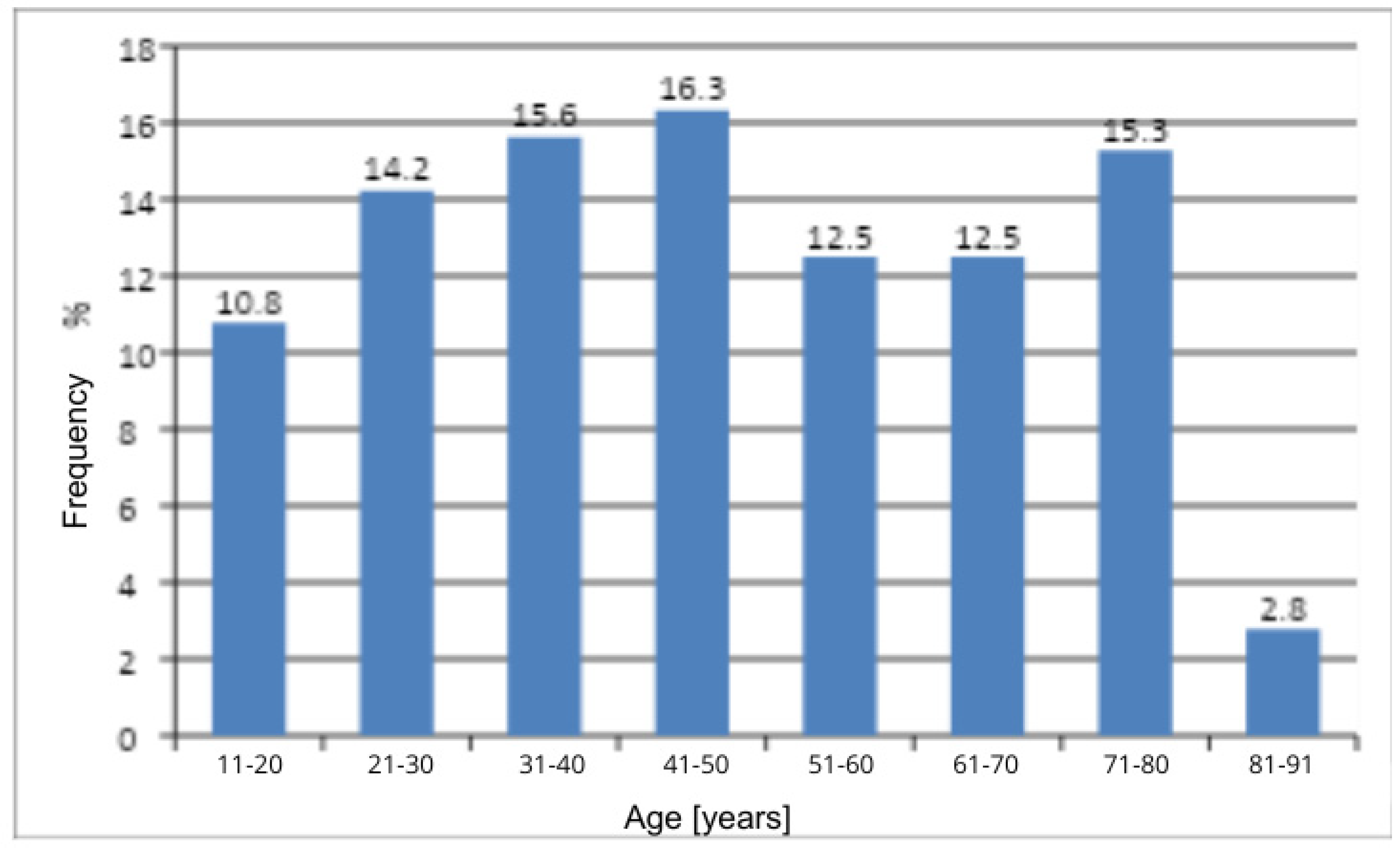
Figure 2.
Occurrence of comorbidities among women.
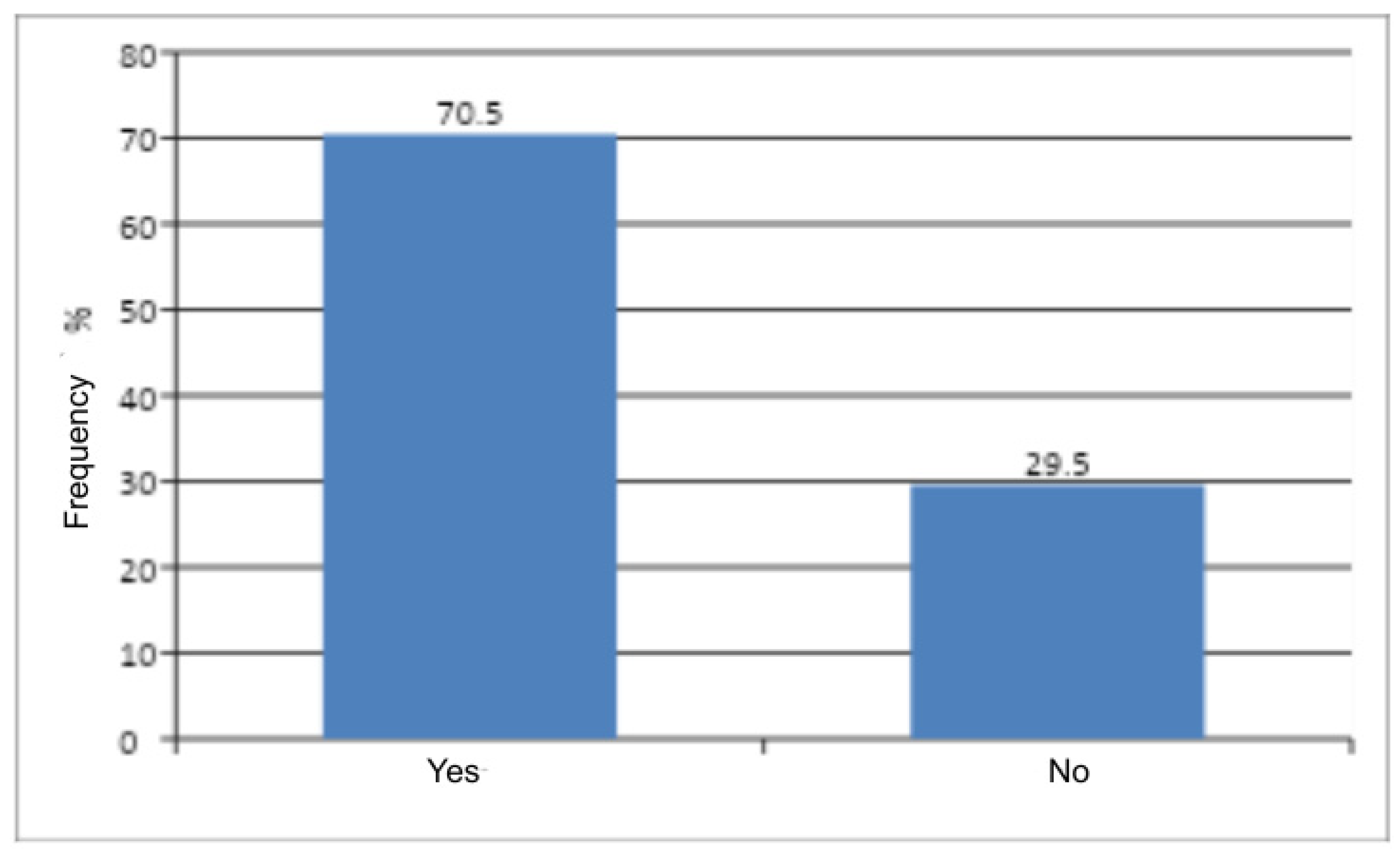
Figure 3.
Obstetric history among women.
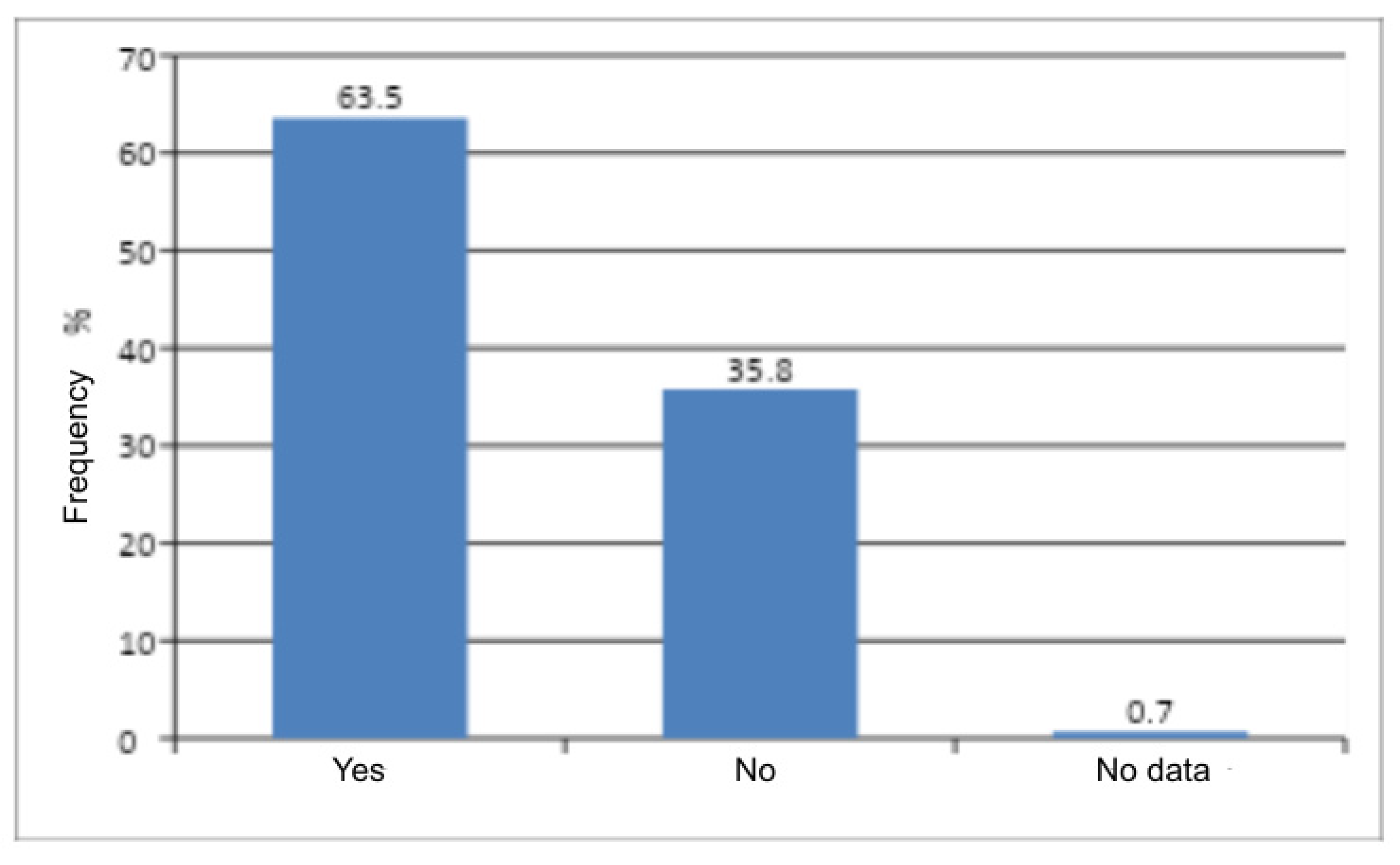
Figure 4.
Distribution of BMI in the study group.
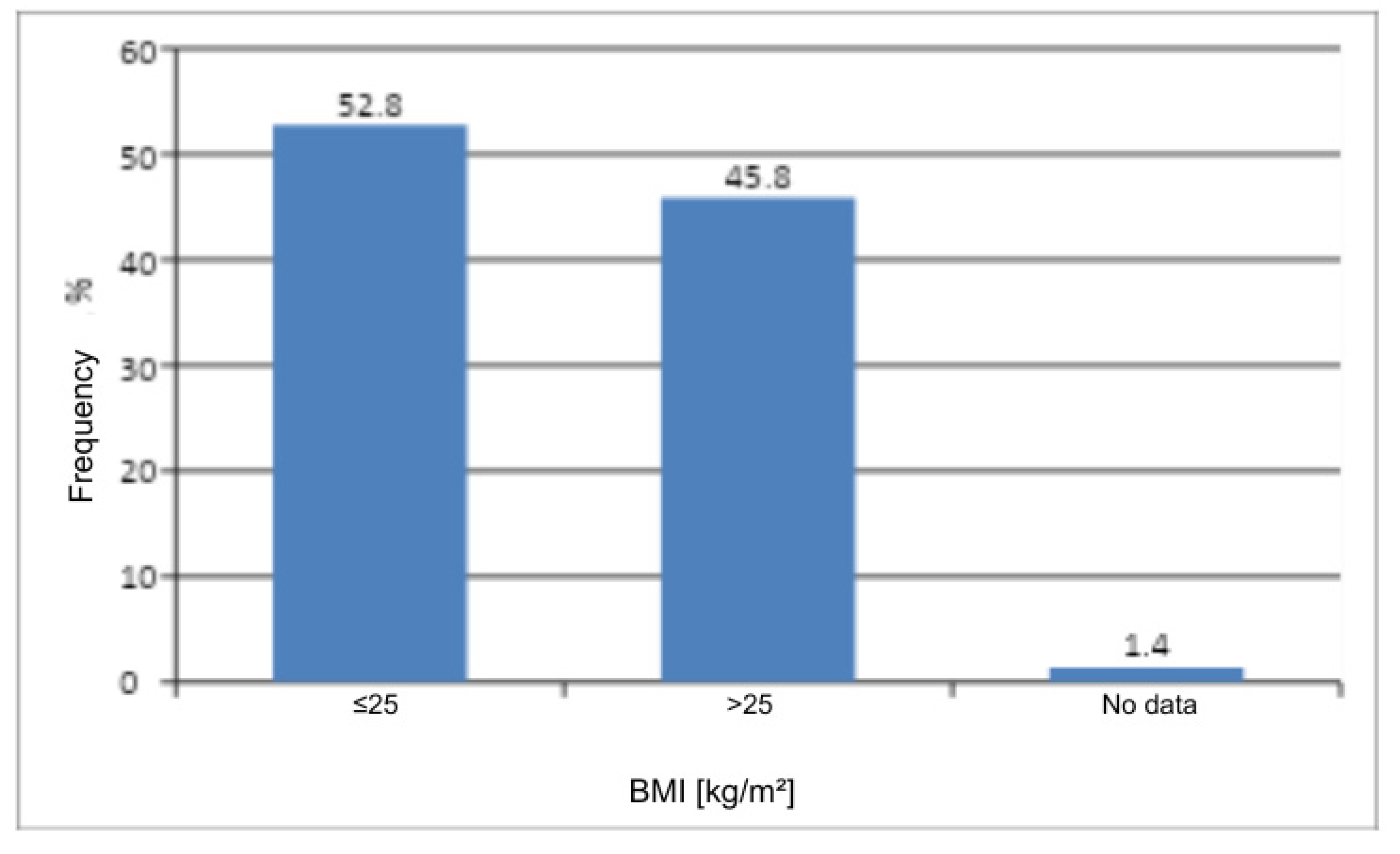
Figure 5.
Menopausal status in the study group.

Table 1.
Statistics of age for female patients.
| n | Age (years) | ||||||
|---|---|---|---|---|---|---|---|
| Mean | SD | Median | Q25 | Q75 | Min. | Max. | |
| 288 | 47.4 | 20.3 | 46.0 | 30.5 | 67.5 | 11 | 91 |
Table 2.
Number and frequency of female patients by diagnosis (ICD-10 Code).
| Diagnosis | n | % | |
|---|---|---|---|
| N76 | 50 | 17.4 | |
| including | N76.0 | 10 | 3.5 |
| N76.1 | 8 | 2.8 | |
| N76.2 | 1 | 0.3 | |
| N76.4 | 7 | 2.4 | |
| N76.5 | 3 | 1.0 | |
| N76.6 | 5 | 1.7 | |
| N76.8 | 16 | 5.6 | |
| N90 | 238 | 82.6 | |
| including | N90.0 | 5 | 1.7 |
| N90.1 | 2 | 0.7 | |
| N90.2 | 15 | 5.2 | |
| N90.3 | 10 | 3.5 | |
| N90.4 | 8 | 2.8 | |
| N90.5 | 7 | 2.4 | |
| N90.6 | 18 | 6.3 | |
| N90.7 | 5 | 1.7 | |
| N90.8 | 27 | 9.4 | |
| N90.9 | 141 | 49.0 | |
| All | 288 | 100 | |
Table 3.
Number and frequency of women by age and the result of Pearson’s Chi-Square Test of Independence.
Table 3.
Number and frequency of women by age and the result of Pearson’s Chi-Square Test of Independence.
| Age | n | % | χ2 | df | p | |
|---|---|---|---|---|---|---|
| 11-20 | 31 | 10.8 | 30.56 | 7 | <0.0001 | |
| 21-30 | 41 | 14.2 | ||||
| 31-40 | 45 | 15.6 | ||||
| 41-50 | 47 | 16.3 | ||||
| 51-60 | 36 | 12.5 | ||||
| 61-70 | 36 | 12.5 | ||||
| 71-80 | 44 | 15.3 | ||||
| 81-91 | 8 | 2.8 | ||||
| All | 288 | 100 | ||||
* χ² – chi-square statistic; df – degrees of freedom; p – probability level (p-value).
Table 4.
Number and frequency of women by the presence of comorbidities and the result of Pearson’s Chi-Square Test of Independence.
Table 4.
Number and frequency of women by the presence of comorbidities and the result of Pearson’s Chi-Square Test of Independence.
| Comorbidities | n | % | χ2 | df | p |
|---|---|---|---|---|---|
| Yes | 203 | 70.5 | 48.35 | 1 | <0.0001 |
| No | 85 | 29.5 | |||
| All | 288 | 100 | |||
Table 5.
Number and frequency of women by the presence of obstetric history and the result of Pearson’s Chi-Square Test of Independence.
Table 5.
Number and frequency of women by the presence of obstetric history and the result of Pearson’s Chi-Square Test of Independence.
| History of pregnancy | n | % | χ2 | df | p |
|---|---|---|---|---|---|
| Yes | 183 | 63.5 | 22.38 | 1 | <0.0001 |
| No | 103 | 35.8 | |||
| No data | 2 | 0.7 | |||
| All | 288 | 100 | |||
Table 6.
Number and frequency of women by BMI and the result of Pearson’s Chi-Square Test of Independence.
Table 6.
Number and frequency of women by BMI and the result of Pearson’s Chi-Square Test of Independence.
| BMI | n | % | χ2 | df | p |
|---|---|---|---|---|---|
| <25 | 152 | 52.8 | 1.41 | 1 | 0.2353 |
| >25 | 132 | 45.8 | |||
| No data | 4 | 1.4 | |||
| All | 288 | 100 | |||
Table 7.
Number and frequency of women by menopausal status and the result of Pearson’s Chi-Square Test of Independence.
Table 7.
Number and frequency of women by menopausal status and the result of Pearson’s Chi-Square Test of Independence.
| Menopausal status | n | % | χ2 | df | p |
|---|---|---|---|---|---|
| Yes | 136 | 47.2 | 0.89 | 1 | 0.3458 |
| No | 152 | 52.8 | |||
| All | 288 | 100 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



