
Submitted:
31 October 2025
Posted:
03 November 2025
You are already at the latest version
Abstract
Coronary artery disease remains the leading cause of cardiovascular morbidity and mortality worldwide, affecting millions of individuals each year. Coronary artery calcification is a common finding in patients with advanced atherosclerosis and represents an important determinant of procedural success during percutaneous coronary intervention. Severe calcifications are associated with increased procedural complexity and higher complication rates due to challenging lesion preparation, suboptimal stent expansion, and less favorable long-term outcomes. This review summarises the current understanding of vascular calcification mechanisms, diagnostic imaging modalities, and current plaque modification techniques used to optimize procedural results. Methods such as rotational, orbital, and laser atherectomy, as well as specialized balloon technologies and intravascular lithotripsy, are discussed with regard to their mechanisms of action, clinical effectiveness, and safety profiles. Particular emphasis is placed on the integration of advanced imaging for precise lesion assessment, improved patient selection, and the use of combination strategies in complex cases. Finally, emerging technologies and future directions are highlighted, aiming to enhance procedural safety, device deliverability, and treatment outcomes in the evolving field of interventional cardiology.
Keywords:
percutaneous coronary intervention
; coronary artery calcification
; coronary artery atherectomy
; intravascular imaging
1. Introduction
Cardiovascular diseases, including coronary artery disease (CAD), still represent the main cause of mortality, representing nearly one-third of total global fatalities [1]. The primary origin of coronary artery disease is atherosclerosis — a complex sequence of cellular mechanisms that drives plaque formation and gradual narrowing of the vascular lumen [2]. Coronary artery calcification represents an advanced manifestation of this process, reflecting both plaque burden and vascular degeneration, and acting as a robust predictor of adverse cardiovascular events [3]. Data from the large MESA cohort demonstrate that progression of coronary artery calcification is strongly associated with increased risk of acute coronary syndromes and cardiac arrest [4]. At the cellular level, coronary artery calcification arises from a complex interaction between endothelial injury, lipid accumulation, and chronic inflammation. Activated macrophages and inflammatory cytokines such as IL-6, TNF-, and IL-1- stimulate vascular smooth muscle cells to shift toward osteogenic differentiation through pathways involving RUNX2 and Wnt/-catenin signaling. Simultaneously, various forms of programmed cell death, including apoptosis and autophagy, contribute to release of matrix vesicle and dysmorphic calcium deposition within the arterial wall, ultimately promoting plaque mineralization and progression of atherosclerosis [5,6]. Intimal calcifications, most common in CAD, are considered to be associated particularly with age, diabetes mellitus, dyslipidemia, smoking, and systemic inflammation [3]. Assessment of plaque calcification severity may include non-invasive coronary artery calcification score (Agatston score) obtained from Coronary Computed Tomography Angiography (CCTA) or fluoroscopic and intravascular imaging (IVI) performed during percutaneous coronary intervention (PCI) procedure. Precise quantification of coronary artery calcification prior to PCI enables tailored procedural planning, selection of the most appropriate plaque-modification strategy, and optimization of clinical outcomes. IVI modalities such as intravascular ultrasound (IVUS) and optical coherence tomography (OCT) facilitate the assessment of calcium features and guide the choice of appropriate calcium debulking techniques [7]. Adequate lesion preparation reduces the risk of stent underexpansion, malapposition, and related complications such as thrombosis or target lesion failure, improving both procedural safety and long-term vessel patency [8,9,10].
2. Lesion Assessment
In fluoroscopy, calcified plaques appear as linear radiopaque or tramline-like densities that are clearly distinguishable even before contrast administration and without cardiac motion. When calcific deposits are observed bilateral along the vessel wall and extend over a cumulative length of at least 15 mm, they indicate a high calcium burden [10]. This allows a rough classification of calcification severity (mild, moderate, severe) [7,8]. Although highly specific, fluoroscopy lacks the sensitivity to precisely evaluate calcium depth, circumferential arc, and lesion length and therefore cannot effectively guide procedural decision making during PCI.
Accurate assessment of calcified coronary lesions requires the use of intravascular imaging. Intravascular ultrasound (IVUS) is a catheter-based modality that generates cross-sectional images of the vessel wall using ultrasound, enabling real-time evaluation of lumen, plaque, and calcium morphology. Calcifications are identified on IVUS as bright, hyperechoic regions with acoustic shadowing. Therefore, IVUS enables quick and appropriate measurement of calcific lesions: calcium arc, length, and location (superficial vs. deep). The extent of shadowing and the presence of reverberation artifacts on IVUS images allow assessing the estimated calcium thickness (reverberations suggest <0.5 mm, while complete shadowing suggests >1 mm calcium thickness). Moreover, IVUS provides an intraprocedural evaluation of the results of percutaneous coronary angioplasty, allowing confirmation of the proper modification of the plaque and correct stent apposition. The main limitation of IVUS is the relatively large catheter (approximately 3.2 F) that may not be able to cross highly calcified narrow lesions and its spatial resolution, typically 100-150 m for classical probes [11].
Optical coherence tomography (OCT) is an intracoronary imaging technique that uses near-infrared light to produce high-resolution (10–15 m) cross-sectional images of the vessel microstructure. In OCT, calcium is identified as a heterogeneous low-signal region with well-defined margins, minimal backscatter, deep light penetration, and no associated shadowing. OCT excels in delineating superficial calcium, measuring its thickness, arc, and longitudinal extent [12]. Simple OCT scoring systems such as the “rule of 5”—which considers arc >50% of vessel circumference, thickness >0.5 mm, and length >5 mm [13], or more recently “rule of 3”— which stands for 360° arc, thickness >0.3 mm, and length >3 mm - both correlate strongly with the likelihood of stent underexpansion [14]. Similarly to IVUS, OCT also enables visualization of real-time periprocedural plaque modification, such as fracture lines or tissue disruption, as well as confirmation of post-PCI optimal stent deployment criteria (e.g. minimum stent area, stent apposition, lack of edge dissections) [15].

Table 1.
Comparison of IVUS and OCT, adapted from Koganti et al. [16]
Table 1.
Comparison of IVUS and OCT, adapted from Koganti et al. [16]
| Aspect | IVUS | OCT |
|---|---|---|
| Imaging Modality | Ultrasound | Near-infrared light |
| Axial Resolution | 100-150 m (20–60 m for HD-IVUS) | 10–20 m |
| Lateral Resolution | 200 m | 20 m |
| Tissue Penetration Depth | >5 mm | 1–2 mm |
| Need for Blood Clearance | No | Yes |
| Need for Contrast Injection | No | Yes (may be replaced by dextran) |
| Catheter Size | Up to 3.2 Fr | 2.7 Fr |
| Assessment of Plaque Morphology | Moderate resolution for plaque assessment | Superior fine detail (fibrous cap, lipid core, thrombus) |
| Calcium Assessment | Semi-quantitative (measure calcium length and arc, but only estimates thickness) Microcalcifications not assessable Difficult differentiation between eruptive and non-eruptive CNs | Quantitative (measure calcium length, arc, and thickness) Microcalcifications assessable Accurate differentiation between eruptive and non-eruptive CNs Medial calcifications difficult to assess |
| Evaluation of Vessel Remodeling | Yes | Limited |
| Utility in Aorto-Ostial Lesions | Preferred (guideline-recommended) | Difficult, less preferred |
| Stent Expansion Assessment | Reliable, deeper wall visualization | Highly precise but limited by EEM 1 visibility |
| Detection of Malapposition/Dissection | Possible, less sensitive | Superior due to resolution |
1 EEM - external elastic membrane
The initial stage of coronary artery calcification involves microscopic deposits, typically observed in areas of intimal thickening, with dimensions ranging between 0.5 and 15 m. As calcification progresses, plaques often develop extensive calcium layers spanning more than one quadrant of the vessel wall. Mechanical disruption of these calcified plates may result in the emergence of very difficult-to-treat calcified nodules [17]. Certain morphologic features of calcified atherosclerotic plaques have been shown to significantly increase the risk of stent underexpansion and future in-stent restenosis. Consequently, dedicated scoring systems have been developed to evaluate such lesions and guide the need for plaque modification prior to stent implantation. Fujino et al. [18] proposed an OCT-based rating system, recently revised by Sato et al. [14], and similarly, Zhang et al. [19] established IVUS-derived criteria. Both scoring systems have been incorporated into the Expert Consensus Statement on the Management of Calcified Coronary Lesions [10] and are summarised in the Table 2.
A final score of ≥2 points in the OCT scale [14] or ≥2 points in the IVUS scale indicates the necessity of appropriate plaque preparation with advanced calcium modification techniques to provide optimal stent deployment [19].
A calcified nodule (CN) is a protruding mass of calcium within the coronary lumen, typically overlying a heavily calcified plaque, often observed in the proximal and medial segments of the right coronary artery, which are exposed to high flexural stress or in lipid-rich and necrotic-core–dominant areas, including the left main bifurcation and proximal parts of epicardial arteries [20]. CNs tend to occur more frequently in older individuals, women, and patients with comorbidities such as diabetes mellitus, prior CABG, or those receiving chronic hemodialysis [21]. CNs are histologically categorized as either eruptive — with fibrous cap disruption, irregular surface and thrombus formation — or non-eruptive, which present a smooth surface and intact cap [22]. CNs are associated with an elevated risk of long-term cardiovascular events and poor invasive treatment results due to suboptimal stent expansion and a high percentage of in-stent restenosis. Non-eruptive calcium nodules are less susceptible to balloon deformation and require accurate, often multi-stage lesion modification to avoid stent underexpansion. On the other hand, eruptive CNs may allow for more symmetrical acute stent deployment, but they are linked to worse long-term outcomes due to early in-stent restenosis caused by reprotrusion of nodular debris into the vessel lumen [10]. Intraprocedural differentiation of CN subtypes is achievable using IVI — particularly with HD-IVUS or more precisely with OCT because of its superior resolution.
Figure 1.
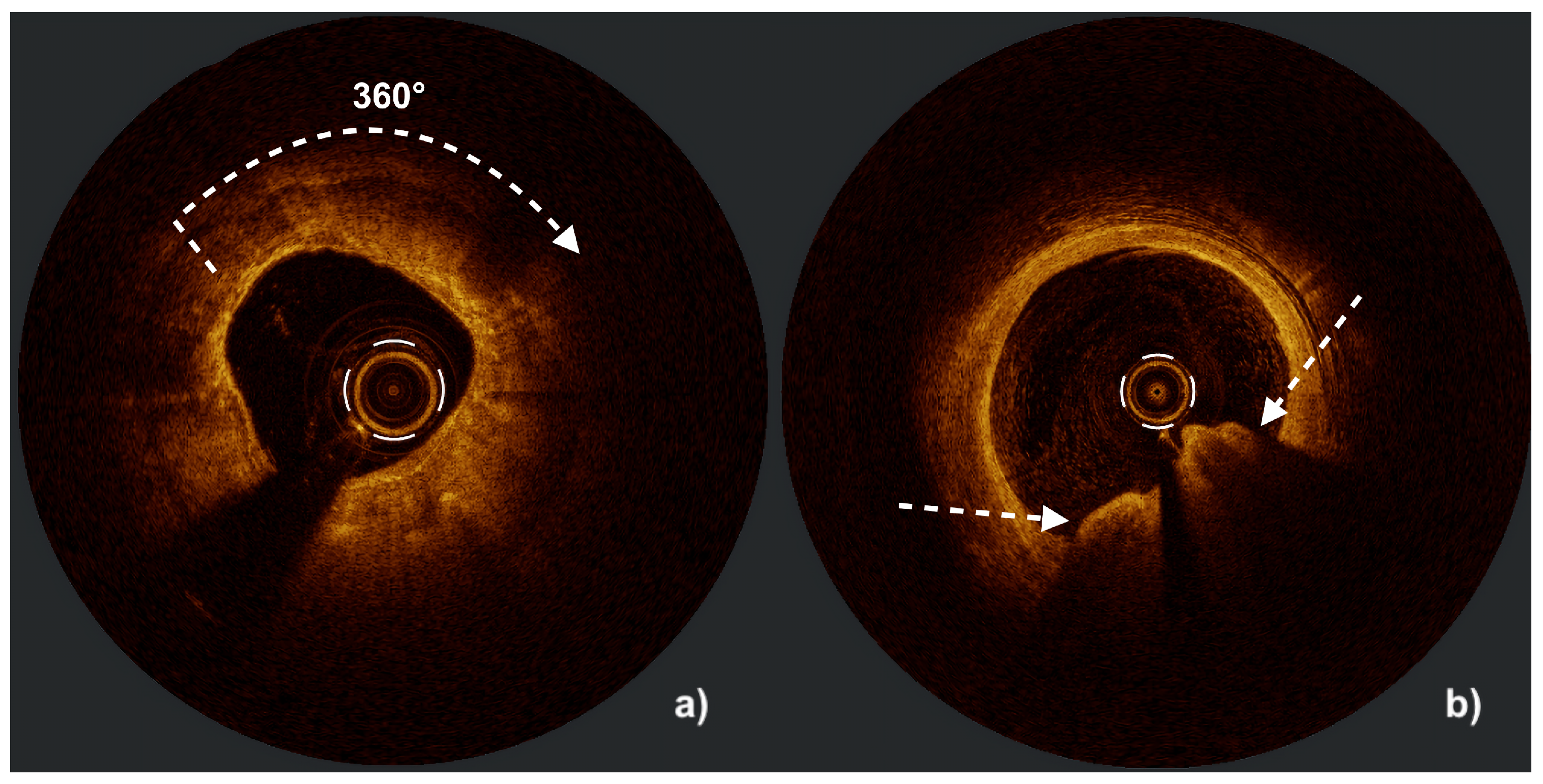
High-definition intravascular ultrasound (HD-IVUS) images illustrating severe coronary calcification: (a) a circumferential (360°) calcified lesion appearing as a bright ring with an acoustic shadow behind (white arrow), and (b) an eruptive calcified nodule represented by an irregular, protruding calcified mass extending into the vessel lumen with an acoustic shadow (white arrows indicate the proximal and distal margins of the calcified nodule).
Figure 1.
High-definition intravascular ultrasound (HD-IVUS) images illustrating severe coronary calcification: (a) a circumferential (360°) calcified lesion appearing as a bright ring with an acoustic shadow behind (white arrow), and (b) an eruptive calcified nodule represented by an irregular, protruding calcified mass extending into the vessel lumen with an acoustic shadow (white arrows indicate the proximal and distal margins of the calcified nodule).

Figure 2.
Optical coherence tomography (OCT) images illustrating severe coronary calcification: (a) a circumferential (360°) calcified lesion appearing as a heterogeneous, low-signal region with well-defined borders, minimal backscatter, deep light penetration, and no shadowing (white arrow), and (b) an eruptive calcified nodule visualized as a heterogeneous, low-signal mass protruding into the vessel lumen with similar optical characteristics (white arrows indicate the margins of the calcified nodule). Figure courtesy of Professor Maciej Lesiak and Sylwia Iwańczyk, PhD.
Figure 2.
Optical coherence tomography (OCT) images illustrating severe coronary calcification: (a) a circumferential (360°) calcified lesion appearing as a heterogeneous, low-signal region with well-defined borders, minimal backscatter, deep light penetration, and no shadowing (white arrow), and (b) an eruptive calcified nodule visualized as a heterogeneous, low-signal mass protruding into the vessel lumen with similar optical characteristics (white arrows indicate the margins of the calcified nodule). Figure courtesy of Professor Maciej Lesiak and Sylwia Iwańczyk, PhD.
3. Calcified Plaque Modification Methods
Percutaneous treatment of heavily calcified coronary lesions remains challenging, with increased periprocedural risk, higher incidence of early complications, and suboptimal success rates. Selection of appropriate calcium modification techniques seems to be crucial for effective lesion preparation, optimal stent deployment, and avoiding adverse events.
3.1. SC and NC Balloons
Semi-compliant balloons are thin-wall angioplasty devices constructed from soft, flexible polymers. They are commonly used for lesion predilatation in soft, non-calcified coronary stenoses, plain old balloon angioplasty (POBA), or as carriers for antiproliferative agents in drug-coated balloon therapy. Due to their trackability and conformability, they are advantageous for crossing tight or tortuous lesions. However, in heavily calcified plaques, under high inflation pressures, SC balloons may expand asymmetrically - widening at the proximal and distal edge while remaining constricted at the lesion site - often referred to as a “dog-bone” or “dumbbell” effect. This phenomenon not only indicates insufficient plaque modification but may also lead to serious complications such as balloon rupture, vessel perforation, or dissection, especially at the balloon edges [23].
Non-compliant balloons are composed of thick, rigid walls of durable polymers. These balloons exhibit limited expansion in response to increasing inflation pressure, resulting in a more controlled and predictable diameter. This feature allows for application of high radial force against the lesion with minimal risk of overexpansion, which makes them a first-line tool for predilatation of calcified lesions, especially when intravascular imaging or advanced plaque modification devices are not insertable through tight coronary stenosis. However, in asymmetrical, sharp, or deep calcifications, even NC balloons may still display deficient inflation, structural compromise or even a rupture at very high pressures [23].
Clinical data suggest that even in relatively simple lesions, the use of non-compliant balloons for lesion preparation results in more uniform expansion and better procedural outcomes compared to semi-compliant alternatives. These findings have contributed to a paradigm shift in predilatation strategy, favoring high-pressure, non-compliant balloon inflation for optimal stent bed preparation, regardless of lesion complexity [24].
3.2. Super High-Pressure Non-Compliant Balloons
Super high-pressure non-compliant balloons, such as the OPN (SIS Medical, Switzerland), are designed with a dual-layer architecture to withstand inflation pressures up to 30-45 atmospheres [25] and apply significant forces to modify severely resistant lesions, including undilatable de novo calcifications and in-stent restenoses. Their reinforced structure distributes pressure between the inner and outer layers, reducing the risk of vessel perforation in the event of balloon rupture. Super high-pressure NC balloons are relatively easy to use and do not require additional operator training. However, due to their bulky design and a larger crossing profile, in complex narrow lesions, adjunctive methods such as a "buddy wire" technique or guide extension catheter may be necessary to advance the device to the target site [23]. Compared with standard non-compliant balloons, the use of OPN devices in complex, non-dilatable lesions was associated with a significantly lower residual diameter stenosis. [26].
3.3. Scoring and Cutting Balloons
Scoring balloons are modified balloon devices equipped with an external nitinol net designed to focus contact force without provoking vessel wall pressure injury. Force transmission through the nitinol struts generates controlled microfractures within the plaque, resulting in efficient calcium disruption at lower inflation pressures. The structural design also provides anchoring during inflation, which helps to prevent slippage and ensure stable balloon expansion. Because the majority of scoring balloons are based on semicompliant platforms, they maintain favorable crossability and trackability, offering advantages in anatomies where bulky devices are difficult to deliver [27]. Slightly different technology is applied in Scoreflex (OrbusNeich, Hong Kong, China) NC balloon family, where a single nitinol wire and a segment of standard workhorse guidewire are used as scoring components [23]. A combination of hydrophilic and hydrophobic coatings reduces friction to improve deliverability of the NC-based device to the lesion site [13].
Cutting balloons are specialized non-compliant angioplasty devices equipped with three or four longitudinal microsurgical blades. Cutting edges focus contact force to create controlled shallow incisions in fibrotic or calcified plaques at relatively low pressures, improving balloon expansion and facilitating optimal stent delivery [28]. Reduction of applied pressures limits the risk of uncontrolled dissection or vessel injury. The main limitation of cutting balloons’ wide application is their bulky profile, which has poor lesion crossability. Newer designs - such as the Wolverine (Boston Scientific, USA) balloon - have improved deliverability through lower profile shafts and more flexible distal tips [29]. In the COPS trial, patients with calcified plaques randomized to cutting balloon predilatation achieved a greater final minimum stent area than those treated with standard NC balloons [30]. Other studies comparing scoring and cutting balloons suggest better stent deliverability after cutting balloon predilatation, even in more challenging anatomies [31].
3.4. Coronary Atherectomy
Atherectomy is a percutaneous intervention designed to partially remove atherosclerotic plaque responsible for vascular obstruction. In contrast to angioplasty, which compresses plaque into the arterial wall, this approach physically eliminates part of the lesion. Coronary atherectomy is an important modality for the modification of calcified lesions, especially in tight, balloon-uncrossable stenoses. Available atherectomy methods include rotational, orbital, and laser atherectomy.
3.4.1. Rotational Atherectomy
Rotational atherectomy (RA), also known as rotablation, is one of the oldest and most established techniques for modifying calcified coronary plaques. Despite its long history, it remains underused due to its procedural complexity and the relatively long time operator training required.
The most popular ROTAPRO™ system (Boston Scientific, USA) requires specialized 0.009” guidewires, such as the ROTAWIRE or ROTAWIRE Drive from a newer guidewire family with improved trackability. A diamond-coated elliptical burr that spins over the wire at an operating speed of 140,000 to 180,000 revolutions per minute allows for cutting fragments of calcific plaque. A burr-to-artery ratio of approximately 0.6 is recommended [32,33], with smaller burrs (1.25-1.5 mm) favored for long or tortuous segments and the larger ones reserved for proximal or aorto-ostial disease. Most procedures can be performed with burr sizes up to 1.75 mm via radial approach with a 6 Fr guiding catheter. Burrs of 2.0 mm diameter necessitate a 7 Fr system or sheathless radial approach, while the biggest devices may need an 8 Fr guiding catheter and subsequent femoral approach [34]. A continuous flush solution, typically composed of heparinized saline with vasodilators like verapamil or nitrates, is administered through the side port of the device to cool the turbine, prevent vasospasm, and reduce debris accumulation during the procedure [33].
Unlike balloon techniques, RA removes plaque by mechanical abrasion, reducing vessel walls barotrauma and the risk of deep dissections. The most frequent complication of RA (5-20%) is the coronary slow flow phenomenon (CSFP), usually resulting from the accumulation of atherosclerotic debris in the distal coronary circulation. The incidence of this complication is related to anatomical features like low vessel diameter, its angulation, and atherosclerotic lesion length, but also with procedural factors such as high burr to vessel ratio, long ablation runs [35], and excessive drops in rotational speed. Although current, less aggressive burr to vessel ratio recommendations have reduced the incidence of CSFP, operators should remain cautious about the possibility of this complication. The moment the drop of flow is noticed, rotational atherectomy should be suspended until normal TIMI-3 flow is re-established [34]. ST-segment elevation on ECG monitoring often precedes the onset of CSFP and can be valuable for intraprocedural surveillance during rotational atherectomy. Proper pre-procedural hydration combined with maintaining systolic blood pressure above 100 mmHg are important maneuvers in the prevention of CSFP [36]. Although rare, coronary artery perforations (1–2% of cases) [37,38] remain a potentially fatal adverse event of RA. Increased vigilance for perforation is required, especially when performing procedures on eccentric calcifications — such as calcified nodules — or within narrow, tortuous coronary vessels [36]. Another major complication is burr entrapment, reported in 0.4 - 0.8% of cases. It can arise from anatomical angulation or the so-called “Kokesi phenomenon,” where the burr slips behind the lesion and becomes stuck due to its fusiform silhouette [39]. In some cases, this complication requires surgical intervention and coronary artery bypass grafting. Experienced operators emphasize the importance of monitoring for early signs of rising resistance, such as alterations in ablation sound pitch and fluctuations in rotational speed, as prompt recognition and response can prevent device lodging, vessel injury, or other serious complications [33].
ROTAPRO™ rotablation system (Boston Scientific, USA), as it is equipped with diamond coating only on the front half of the spinning burr, is a typical “front cutting device”. Due to the mechanism of action, it is especially effective in treating very tight or even balloon-uncrossable calcified lesions. In moderate stenoses, eccentric lesions, and calcified nodules, the use of RA, although possible, is less effective. Spinning burr can “shave” the calcium surface and even cause cracking in calcific nodules, but techniques such as OA or IVL tend to be more effective in such cases. [40].
A recent advancement in RA technology, such as the FireRaptor System (MicroPort Rota Pace, China), features an eccentric and fully diamond-coated burr. Therefore, unlike ROTAPRO, the FireRaptor System permits bidirectional plaque modification. Forward and reverse device movement not only decreases the risk of burr entrapment but also enhances cutting efficiency. Moreover, adjustable rotational speed allows operators to tailor the ablation diameter to vessel size and lesion characteristics, reducing the need for multiple device exchanges [41].
3.4.2. Orbital Atherectomy
Orbital atherectomy (OA) is another technique within the atherectomy family. The Diamondback 360® Coronary Orbital Atherectomy System (Abbott Cardiovascular, USA) features a diamond-coated, eccentrically mounted 1.25 mm crown that rotates over a specialized 0.012” ViperWire with a 0.014" tip. The mechanism of OA relies on centrifugal force generated by the spinning crown, which orbits as it advances through a coronary artery and preferentially ablates calcified tissue while displacing softer structures. This unique mechanism of action allows for the continuous blood flow during atheroablation and generates very small, submicron debris (~2 m), which passes safely through the microcirculation, resulting in a low risk of distal embolization and slow-flow phenomenon [42]. The system utilizes only one size “fit all” 1.25 mm crown, delivered through a 6 Fr guide catheter. Changes in rotational speed (from 80,000 rpm to 120,000 rpm) translate into an increased sanding radius, thereby enabling treatment of different-sized vessels from 2.5 to 4 mm in diameter [43]. The procedure is aided by the infusion of ViperSlide specific lubricant to reduce friction between the crown and vessel wall. Lesion preparation typically begins at the lower rotational speed, with careful advancement at 1 mm/s and no forward force applied. The operator is encouraged to monitor acoustic feedback from the spinning crown to evaluate engagement with the lesion. Each run should be slow but time-limited to a maximum of 30 seconds, and the total duration of atherectomy should not exceed 5 minutes due to the equipment wear off [44]. The incidence of complications with orbital atherectomy is comparable to that observed with rotational atherectomy [45].
3.4.3. Laser Atherectomy
Excimer laser coronary atherectomy (ELCA) is an atherectomy modality that uses high-energy ultraviolet light to ablate atherosclerotic tissue. The most popular CVX-300 Laser Excimer System (Philips, Netherlands) generates short pulses at a wavelength of 308 nm by passing an electrical discharge through a rare gas–halogen mixture, producing excimer molecules that emit photons. Lesion modification occurs through combined photochemical bond disruption, photomechanical shockwave generation, and localized photothermal effects. This tri-modal action enables precise ablation of plaque with minimal thermal injury to surrounding tissue and formation of low particulate debris (<10 m), reducing the risk of distal embolization and no-reflow phenomenon [46].
A key advantage of ELCA over rotational or orbital atherectomy is the fact that it is compatible with any standard 0.014-inch guidewire. Catheters are available in various sizes ranging from 0.9 mm to 2.0 mm and should not exceed two-thirds of the vessel’s reference diameter. The most common 0.9 mm device is deliverable through a 6 Fr guide catheter, facilitating performing the ELCA procedure from radial access [47]. Device operation requires heparinised saline or contrast flushing to prevent bubble formation. Each 10-second activation is followed by a 5-second pause, repeated until the lesion is crossed or adequately modified for balloon passage or expansion [48]. For safety, each personnel member and the patient must wear protective tinted eyewear to prevent retinal injury from UV light exposure.
ELCA can be applied to native calcified lesions, balloon-uncrossable stenoses, chronic total occlusions, and in-stent restenoses (ISR), especially with significant peri-stent calcification [49]. Clinical outcome data in ELCA studies regarding ISR lesions showed no significant effect on stent structural integrity or polymer release [50]. Another advantage of ELCA is the ability to use side branch wire protection in resistant coronary bifurcation lesion treatment [10]. In certain heavily calcified lesions, when RotaWire™ advancement is not possible, ELCA may be applied first to create a channel that facilitates wire passage, allowing RA to be performed and the procedure to be completed successfully in the so-called “RASER” technique [51]. This complex intervention procedure offers a valuable bailout option for patients with lesions resistant to conventional PCI, however, due to higher baseline and peri-procedural risk, its introduction should be guided by the multi-disciplinary heart team consultation and patient input [52].
3.5. Intravascular Lithotripsy
Intravascular lithotripsy (IVL) is one of the newer calcium modification techniques that delivers pulsatile acoustic pressure waves from an external power source via spherical emitters integrated into a semicompliant balloon. The device is monorail over a standard 0.014” guidewire. The system applies low-pressure balloon inflation — typically around 4 atmospheres — ensuring vessel wall contact while minimizing barotrauma. Once apposed, a controlled electrical discharge within the fluid-filled balloon generates rapidly expanding vapor bubbles. Their collapse emits circumferential shockwaves that traverse soft tissue without damage, but produce focal mechanical stress when encountering calcific deposits. The peak wave pressure is equivalent to approximately 50 atmospheres [53]. The targeted stress leads to multiplane microfractures in both superficial and deep layers of calcium, improving vessel compliance. The shockwaves are delivered at a consistent frequency of one pulse per second, with a maximum number of 120 pulses for the new C2+ Generation Shockwave System (Shockwave Medical, USA). The integrated balloon serves multiple purposes: it stabilizes the system during energy delivery, facilitates coupling of acoustic energy through fluid-tissue impedance matching, and provides thermal protection to vascular structures and device components by dispersing generated heat [53]. Given the IVL balloon’s limited length of 12 mm and minimum diameter of 2.5 mm, small vessels are unattainable for treatment, while long, calcified segments require sequential inflations. Other limitation of IVL is its relatively bulky profile, which can hinder delivery across tight or tortuous lesions. In such cases, auxiliary techniques or devices—such as guide extensions or preceding atherectomy—may be required [54].
IVL is particularly effective in lesions with circumferential calcium, where acoustic pressure waves can disrupt concentric calcified rings and restore vessel compliance. Clinically, its key advantage is observed in the treatment of eccentric calcifications and calcified nodules, where conventional techniques—such as high-pressure non-compliant, scoring, or cutting balloons—carry an elevated risk of arterial dissection. In these challenging morphologies, rotational atherectomy is further limited by wire bias, often resulting in superficial “shaving” or lesion guttering rather than sufficient calcium modification. In contrast, IVL catheters deliver acoustic energy selectively toward dense calcific deposits while sparing healthy soft vessel wall regions, enabling safer and more uniform lesion preparation. [55]. IVL has also been successfully used in managing underexpanded stents, with evidence from registries showing significant increases in stent area and luminal gain [56]. Unlike RA or OA, the IVL catheter allows for the use of side branch protection wire during impulse delivery, which makes it very convenient in the treatment of coronary bifurcation lesions [57]. Due to its safety profile and lower risk of complications, IVL is also recommended over atherectomy in balloon-crossable calcified aorto-ostial lesions [10].
DISRUPT CAD III, a large prospective study involving 384 patients with severe coronary calcification, assessed IVL procedural success at over 92%, with perforation and slow flow rates of 0.3% and 0.5% [58]. IVL safety profile with minimal incidence of adverse events was later confirmed in other studies, also including patients with acute coronary syndromes [59,60].
Driven by increasing clinical demand, next-generation devices based on established mechanisms of action are being developed and introduced worldwide. Several new IVL platforms are currently undergoing clinical evaluation (Abbott, Lepumedical, Shunmei), including the first laser-based IVL system with one, but movable optical transmitter, Sola (FastWave Medical, USA, IDE trial starts in mid-2026), and a single distal emitter device that enables calcium modification beyond the catheter tip and facilitating treatment of tight, non-crossable stenoses, Javelin Coronary IVL (Shockwave Medical, USA) [61].
Figure 3.
Intravascular ultrasound (IVUS) images of a severely calcified coronary lesion with circumferential (360°) calcification before (a) and after (b) intravascular lithotripsy (IVL) using the Shockwave C2+ catheter (Shockwave Medical, USA), demonstrating an increase in minimal lumen area and multiple calcium fractures indicated with white arrows.
Figure 3.
Intravascular ultrasound (IVUS) images of a severely calcified coronary lesion with circumferential (360°) calcification before (a) and after (b) intravascular lithotripsy (IVL) using the Shockwave C2+ catheter (Shockwave Medical, USA), demonstrating an increase in minimal lumen area and multiple calcium fractures indicated with white arrows.
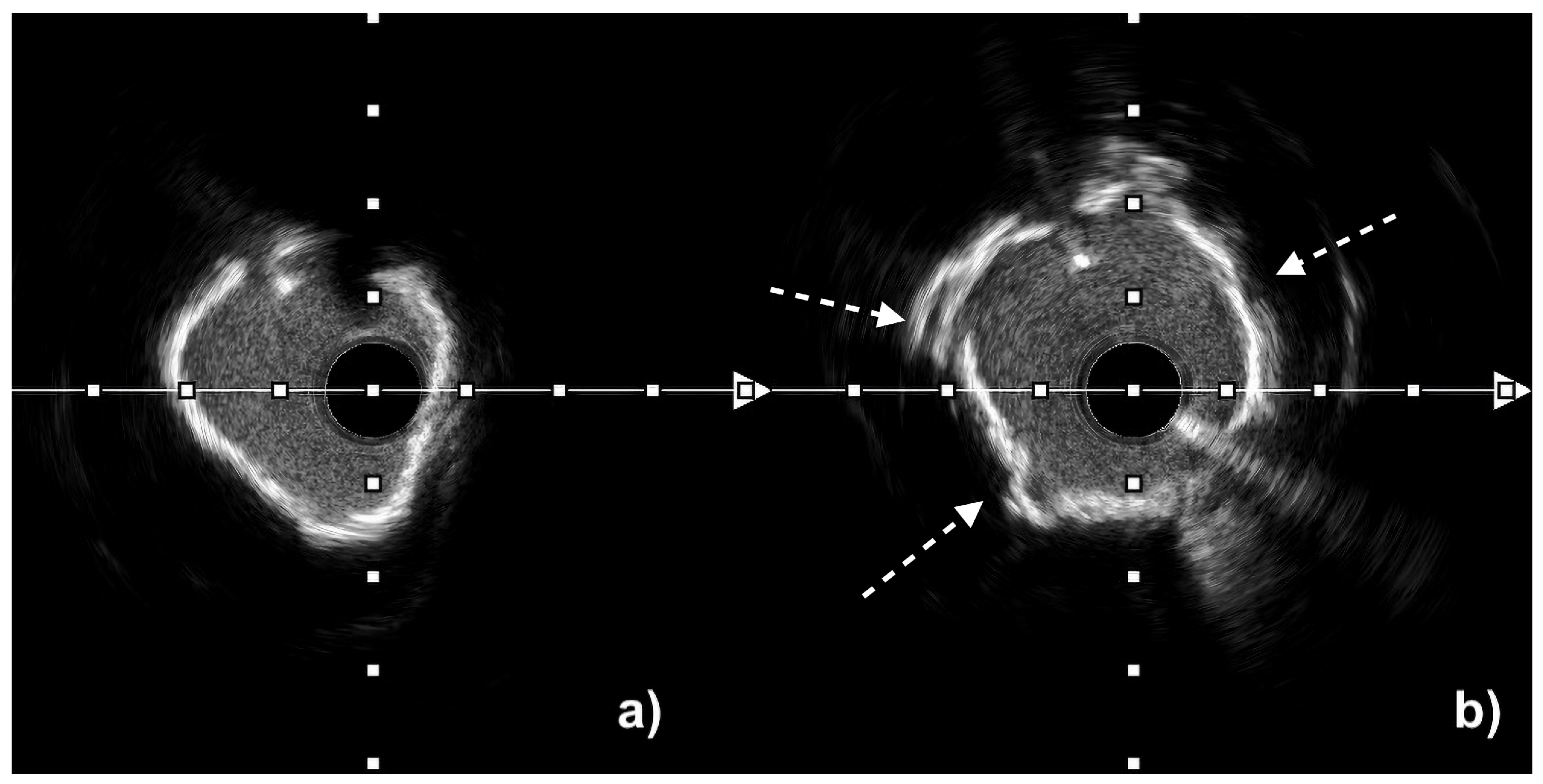
Figure 4.
Optical coherence tomography (OCT) images of a severely calcified coronary lesion with circumferential (360°) calcification before (a) and after (b) plaque modification, demonstrating an increase in minimal lumen area and calcium fracture indicated with white arrow. Figure courtesy of Professor Maciej Lesiak and Sylwia Iwańczyk, PhD.
Figure 4.
Optical coherence tomography (OCT) images of a severely calcified coronary lesion with circumferential (360°) calcification before (a) and after (b) plaque modification, demonstrating an increase in minimal lumen area and calcium fracture indicated with white arrow. Figure courtesy of Professor Maciej Lesiak and Sylwia Iwańczyk, PhD.
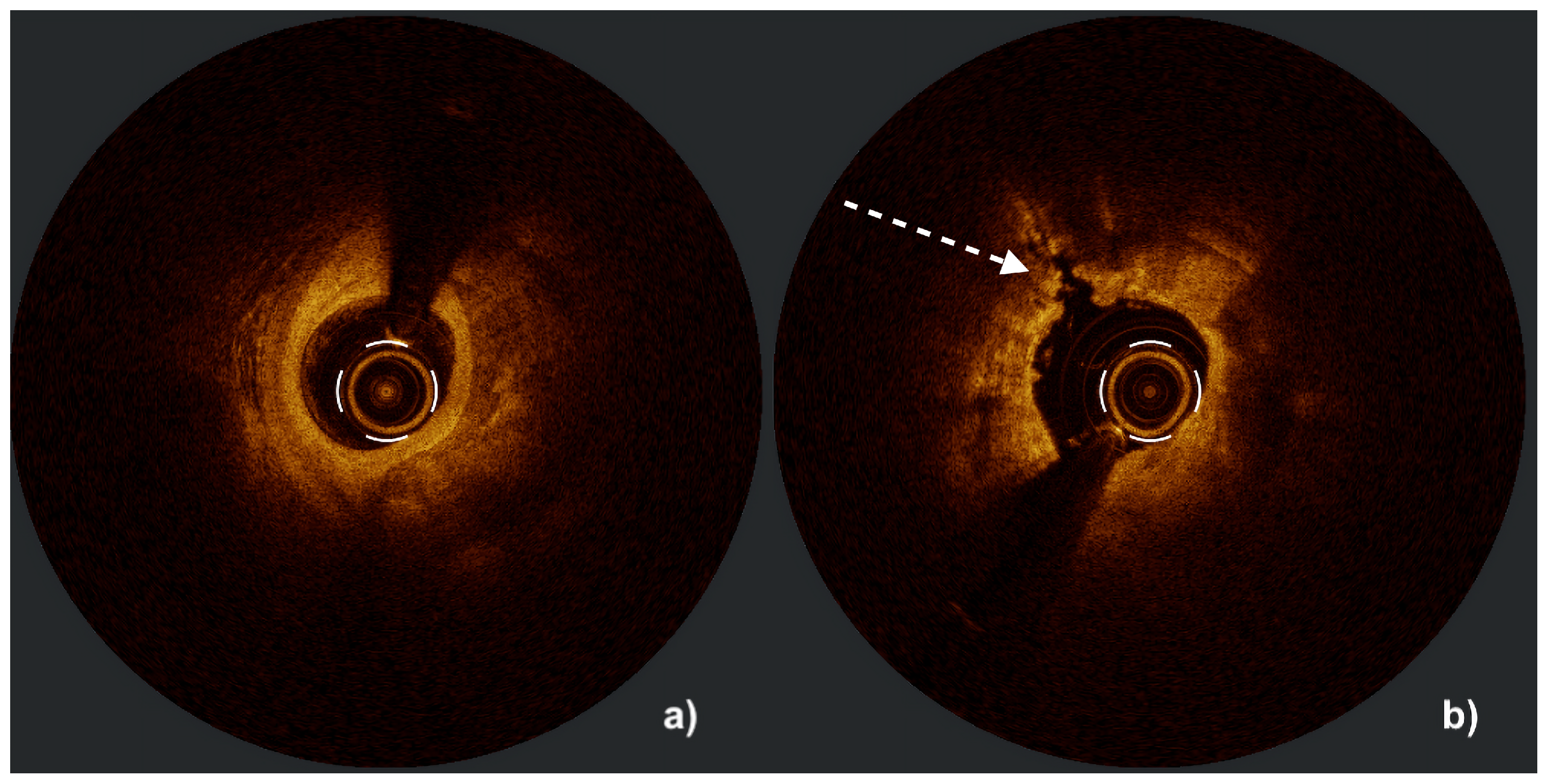
Table 3.
Comparison of calcified lesion modification methods adapted from Russo et al. [62], Sasi et al. [63] and Yeung et al. [64].
| Aspect | IVL | RA | OA | ELCA |
|---|---|---|---|---|
| Mechanism of action | Lithotripsy via acoustic pressure waves | Atheroablation via front abrasion | Atheroablation via sanding | Photoablation (light, acoustic pressure waves, cavitation microbubbles) |
| Guidewire | Elective 0.014” wire | Dedicated 0.009”/0.014” tip wire | Dedicated 0.012”/0.014” tip wire | Elective 0.014” wire |
| Device size | 2.5 - 4.0 mm x 12 mm | 1.25 - 2.5 mm (5-8 Fr) | One crown size 1.25 mm (6 Fr) | 0.9 - 2.0 mm with concentric and eccentric tip designs |
| Course of action | Forward and backward On the balloon’s adhesion surface | Forward only Outside curve only | Forward and backward Outside and inside curve | Forward only |
| Effect of wire bias | Independent | Dependent | Less-dependent | Limited by vessel curvature (UV light does not deflect) |
| Side branch protection | Yes | No | No | Yes |
| Distal embolization | No or very low risk of no/slow-reflow | Higher risk of no/slow-reflow | Medium risk of no/slow-reflow | Very low risk of no/slow-relow |
| Perforation | Low <1% | Up to 1.5% | Up to 1.8% | 1.5-2% |
| Effect on calcium | Affect superficial and deep calcium | Affects only superficial calcium | Affects only superficial calcium | Different effect on superficial and deep calcium |
The latest and different approach method is Hertz Contact Intravascular Lithotripsy (HC-IVL). The technique is based on the Hertzian contact stress principle, where force concentrated at small contact points generates sufficient stress to fracture rigid structures while sparing surrounding soft tissues. The system consists of a semicompliant balloon catheter with multiple rows of metallic hemispheres. When inflated, these hemispheres apply discrete, high-intensity contact forces to the calcified plaque, producing controlled fractures without the need for any external energy source, which significantly reduces procedural complexity. The semicompliant platform of HC-IVL provides improved deliverability, especially when compared to standard IVL and other calcified lesion dedicated devices. Moreover, this design enables treatment of various lesion morphologies, adjusting to the size of the vessel during inflation. Repeated HC-IVL inflations allow effective management of long segments, including eccentric and concentric calcification, while maintaining a favorable safety profile [65].
LithiX™ HC-IVL (Elixir Medical Corporation, USA) was assessed in the PINNACLE I trial, a prospective, multicenter, single-arm study that included 60 patients with moderate to severely calcified coronary lesions, and demonstrated very high clinical success rate for the combined primary safety and efficacy endpoint (98.3%) with 100% angiographic success and residual diameter stenosis <30% in all lesions. The target lesion failure rate was 1.7%, with a single perioperative non–Q-wave myocardial infarction. No cases of severe dissection, perforation, or abrupt vessel closure were observed [66,67].
4. Conclusions
Coronary artery calcification remain a major determinant of procedural success and long-term outcomes in percutaneous coronary intervention. The choice of calcium modification technique should be guided by intravascular imaging findings, lesion morphology, and operator expertise and experience. Despite significant progress, evidence from randomized trials comparing different calcium modification strategies is still limited. Future studies are required to establish standardized algorithms integrating multimodal imaging and combination therapies to optimize stent expansion and improve patient prognosis in complex coronary disease with advanced atherosclerosis.
Author Contributions
Conceptualization, P.K., P.S. and T.S.; writing—original draft preparation, P.S. and P.K.; writing—review and editing, T.S. and A.B.; visualization, P.S.; supervision, T.S.and A.B.; funding acquisition, T.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
During the preparation of this manuscript, the authors used ChatGPT-4 (OpenAI, https://openai.com/, accessed on 24 October 2025) for language and style editing, paraphrasing, and improving the clarity and structure of sentences. The authors have reviewed and edited the output and take full responsibility for the content of this publication
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Di Cesare, M.; Perel, P.; et al. The Heart of the World. Glob. Heart 2024, 19, 11. [Google Scholar] [CrossRef]
- Jebari-Benslaiman, S.; Galicia-García, U.; et al. Pathophysiology of Atherosclerosis. Int. J. Mol. Sci. 2022, 23, 3346. [Google Scholar] [CrossRef]
- Onnis, C.; Virmani, R.; et al. Coronary Artery Calcification: Current Concepts and Clinical Implications. Circulation 2024, 149, 251–266. [Google Scholar] [CrossRef]
- Budoff, M.J.; Young, R.; et al. Progression of Coronary Calcium and Incident Coronary Heart Disease Events: MESA (Multi-Ethnic Study of Atherosclerosis). J. Am. Coll. Cardiol. 2013, 61, 1231–1239. [Google Scholar] [CrossRef]
- Pugliese, G.; Iacobini, C.; et al. The Dark and Bright Side of Atherosclerotic Calcification. Atherosclerosis 2015, 238, 220–230. [Google Scholar] [CrossRef]
- Mitsis, A.; Khattab, E.; et al. From Cells to Plaques: The Molecular Pathways of Coronary Artery Calcification and Disease. J. Clin. Med. 2024, 13, 6352. [Google Scholar] [CrossRef] [PubMed]
- Petousis, S.; Skalidis, E.; et al. The Role of Intracoronary Imaging for the Management of Calcified Lesions. J. Clin. Med. 2023, 12, 4622. [Google Scholar] [CrossRef]
- Caiazzo, G.; Di Mario, C.; et al. Current Management of Highly Calcified Coronary Lesions: An Overview of the Current Status. J. Clin. Med. 2023, 12, 4844. [Google Scholar] [CrossRef] [PubMed]
- Ikari, Y.; Saito, S.; et al. Device Indication for Calcified Coronary Lesions Based on Coronary Imaging Findings. Cardiovasc. Interv. Ther. 2023, 38, 163–165. [Google Scholar] [CrossRef] [PubMed]
- Riley, R.F.; Patel, M.P.; et al. SCAI Expert Consensus Statement on the Management of Calcified Coronary Lesions. J. Soc. Cardiovasc. Angiogr. Interv. 2024, 3, 101259. [Google Scholar] [CrossRef]
- Dawood, M.; Elwany, M.; et al. Coronary Calcifications, the Achilles Heel in Coronary Interventions. Postępy w Kardiologii Interwencyjnej Adv. Interv. Cardiol. 2024, 20, 1–17. [Google Scholar] [CrossRef]
- Wu, W.; Zhao, S.; et al. High-Definition Intravascular Ultrasound Versus Optical Coherence Tomography: Lumen Size and Plaque Morphology. J. Soc. Cardiovasc. Angiogr. Interv. 2025, 4, 102520. [Google Scholar] [CrossRef]
- Jurado-Román, A.; Gómez-Menchero, A.; et al. Plaque Modification Techniques to Treat Calcified Coronary Lesions: Position Paper from the ACI-SEC. REC Interv. Cardiol. (Engl. Ed.) 2023, 9672. [Google Scholar] [CrossRef]
- Sato, T.; Matsumura, M.; et al. A Revised Optical Coherence Tomography–Derived Calcium Score to Predict Stent Underexpansion in Severely Calcified Lesions. JACC Cardiovasc. Interv. 2025, 18, 622–633. [Google Scholar] [CrossRef]
- Shlofmitz, E.; Croce, K.; et al. The MLD MAX OCT Algorithm: An Imaging-Based Workflow for Percutaneous Coronary Intervention. Catheter. Cardiovasc. Interv. 2022, 100, S7–S13. [Google Scholar] [CrossRef] [PubMed]
- Koganti, S.; Kotecha, T.; et al. Choice of Intracoronary Imaging: When to Use Intravascular Ultrasound or Optical Coherence Tomography. Interv. Cardiol. 2016, 11, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Mori, H.; Torii, S.; et al. Coronary Artery Calcification and Its Progression: What Does It Really Mean? JACC Cardiovasc. Imaging 2018, 11, 127–142. [Google Scholar] [CrossRef] [PubMed]
- Fujino, A.; Mintz, G.S.; et al. A New Optical Coherence Tomography-Based Calcium Scoring System to Predict Stent Underexpansion. EuroIntervention 2018, 13, e2182–e2189. [Google Scholar] [CrossRef]
- Zhang, M.; Matsumura, M.; et al. Intravascular Ultrasound-Derived Calcium Score to Predict Stent Expansion in Severely Calcified Lesions. Circ. Cardiovasc. Interv. 2021, 14, e010296. [Google Scholar] [CrossRef]
- Shin, D.; Karimi Galougahi, K.; et al. Calcified Nodule in Percutaneous Coronary Intervention: Therapeutic Challenges. JACC Cardiovasc. Interv. 2024, 17, 1187–1199. [Google Scholar] [CrossRef]
- Lee, T.; Mintz, G.S.; et al. Prevalence, Predictors, and Clinical Presentation of a Calcified Nodule as Assessed by Optical Coherence Tomography. JACC Cardiovasc. Imaging 2017, 10, 883–891. [Google Scholar] [CrossRef]
- Sato, T.; Matsumura, M.; et al. Impact of Eruptive vs Noneruptive Calcified Nodule Morphology on Acute and Long-Term Outcomes After Stenting. JACC Cardiovasc. Interv. 2023, 16, 1024–1035. [Google Scholar] [CrossRef]
- Maffey, M.W.; Bagur, R. Dedicated Balloon Techniques for Coronary Calcium Modification. Interv. Cardiol. (Lond. Engl.) 2024, 19, e13. [Google Scholar] [CrossRef] [PubMed]
- Cuculi, F.; Bossard, M.; et al. Performing Percutaneous Coronary Interventions with Predilatation Using Non-Compliant Balloons at High-Pressure versus Conventional Semi-Compliant Balloons: Insights from Two Randomised Studies Using Optical Coherence Tomography. Open Heart 2020, 7, e001204. [Google Scholar] [CrossRef] [PubMed]
- Bulluck, H.; McEntegart, M. Contemporary Tools and Devices for Coronary Calcium Modification. JRSM Cardiovasc. Dis. 2022, 11, 20480040221089760. [Google Scholar] [CrossRef] [PubMed]
- Secco, G.G.; Ghione, M.; et al. Very High-Pressure Dilatation for Undilatable Coronary Lesions: Indications and Results with a New Dedicated Balloon. EuroIntervention 2016, 12, 359–365. [Google Scholar] [CrossRef]
- Perfetti, M.; Fulgenzi, F.; et al. Calcific Lesion Preparation for Coronary Bifurcation Stenting. Cardiol. J. 2019, 26, 429–437. [Google Scholar] [CrossRef]
- Scalamogna, M.; Kuna, C.; et al. Modified Balloons to Prepare Severely Calcified Coronary Lesions before Stent Implantation: A Systematic Review and Meta-Analysis of Randomized Trials. Clin. Res. Cardiol. 2024, 113, 995–1005. [Google Scholar] [CrossRef]
- Shah, M.; Najam, O.; et al. Calcium Modification Techniques in Complex Percutaneous Coronary Intervention. Circ. Cardiovasc. Interv. 2021, 14, e009870. [Google Scholar] [CrossRef]
- Mangieri, A.; Nerla, R.; et al. Cutting Balloon to Optimize Predilation for Stent Implantation: The COPS Randomized Trial. Catheter. Cardiovasc. Interv. 2023, 101, 798–805. [Google Scholar] [CrossRef]
- Ishihara, T.; Iida, O.; et al. Improved Crossability with Novel Cutting Balloon versus Scoring Balloon in the Treatment of Calcified Lesion. Cardiovasc. Interv. Ther. 2021, 36, 198–207. [Google Scholar] [CrossRef] [PubMed]
- Nowak, A.; Ratajczak, J.; et al. Long-Term Outcome of Rotational Atherectomy According to Burr-to-Artery Ratio and Changes in Coronary Artery Blood Flow: Observational Analysis. Cardiol. J. 2023, 30, 361–368. [Google Scholar] [CrossRef]
- Barbato, E.; Carrié, D.; et al. European Expert Consensus on Rotational Atherectomy. EuroIntervention 2015, 11, A6. [Google Scholar] [CrossRef]
- Sakakura, K.; Ito, Y.; et al. Clinical Expert Consensus Document on Rotational Atherectomy from the Japanese Association of Cardiovascular Intervention and Therapeutics: Update 2023. Cardiovasc. Interv. Ther. 2023, 38, 141–162. [Google Scholar] [CrossRef]
- Sakakura, K.; Taniguchi, Y.; et al. Modifiable and Unmodifiable Factors Associated with Slow Flow Following Rotational Atherectomy. PLOS ONE 2021, 16, e0250757. [Google Scholar] [CrossRef]
- Mattaroccia, G.; Redivo, M.; et al. The New Era of Coronary Angioplasty: How Cutting-Edge Technologies Are Redefining Complex Interventions. Heart Surg. Forum 2025, 28, E107–E119. [Google Scholar] [CrossRef]
- Kini, A.; Marmur, J.D.; et al. Rotational Atherectomy: Improved Procedural Outcome with Evolution of Technique and Equipment. Single-Center Results of First 1,000 Patients. Catheter. Cardiovasc. Interv. 1999, 46, 305–311. [Google Scholar] [CrossRef]
- Januszek, R.; Siudak, Z.; et al. Predictors of In-Hospital Effectiveness and Complications of Rotational Atherectomy (from the ORPKI Polish National Registry 2014–2016). Catheter. Cardiovasc. Interv. 2018, 92, E278–E287. [Google Scholar] [CrossRef]
- Mechery, A.; Jordan, P.J.; et al. Retrieval of a Stuck Rotablator Burr (“Kokeshi Phenomenon”) and Successful Percutaneous Coronary Intervention. J. Cardiol. Cases 2015, 13, 90–92. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Wang, P.; et al. Comparison of Intravascular Lithotripsy versus Rotational Atherectomy for the Treatment of Severe Coronary Artery Calcification. BMC Cardiovasc. Disord. 2024, 24, 311. [Google Scholar] [CrossRef]
- MicroPort. MicroPort extregistered RotaPace Receives Approval for FireRaptor extregistered in China, 2025. MicroPort News.
- Shlofmitz, E.; Jeremias, A.; et al. Lesion Preparation with Orbital Atherectomy. Interv. Cardiol. Rev. 2019, 14, 169–173. [Google Scholar] [CrossRef]
- Khattak, S.; Sharma, H.; et al. Atherectomy Techniques: Rotablation, Orbital and Laser. Interv. Cardiol. (Lond. Engl.) 2024, 19, e21. [Google Scholar] [CrossRef] [PubMed]
- Shipman, J.N.; Agasthi, P. Orbital Atherectomy. In StatPearls; StatPearls Publishing: Treasure Island (FL), 2025. [Google Scholar]
- Goel, S.; Pasam, R.T.; et al. Orbital Atherectomy versus Rotational Atherectomy: A Systematic Review and Meta-Analysis. Int. J. Cardiol. 2020, 303, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Rawlins, J.; Din, J.N.; et al. Coronary Intervention with the Excimer Laser: Review of the Technology and Outcome Data. Interv. Cardiol. Rev. 2016, 11, 27–32. [Google Scholar] [CrossRef]
- Jawad-Ul-Qamar, M.; Sharma, H.; et al. Contemporary Use of Excimer Laser in Percutaneous Coronary Intervention with Indications, Procedural Characteristics, Complications and Outcomes in a University Teaching Hospital. Open Heart 2021, 8, e001522. [Google Scholar] [CrossRef]
- Fernandez, J.P.; Hobson, A.R.; et al. Beyond the Balloon: Excimer Coronary Laser Atherectomy Used Alone or in Combination with Rotational Atherectomy in the Treatment of Chronic Total Occlusions, Non-Crossable and Non-Expansible Coronary Lesions. EuroIntervention 2013, 9, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Ai, H.; et al. The Therapeutic Effects of Excimer Laser Coronary Atherectomy Therapy for In-Stent Restenosis Chronic Total Occlusions. BMC Cardiovasc. Disord. 2021, 21, 399. [Google Scholar] [CrossRef]
- Giri, S.; Ito, S.; et al. Clinical and Angiographic Outcome in the Laser Angioplasty for Restenotic Stents (LARS) Multicenter Registry. Catheter. Cardiovasc. Interv. 2001, 52, 24–34. [Google Scholar] [CrossRef]
- Protty, M.B.; Gallagher, S.; et al. Combined Use of Rotational and Excimer Laser Coronary Atherectomy (RASER) during Complex Coronary Angioplasty—An Analysis of Cases (2006–2016) from the British Cardiovascular Intervention Society Database. Catheter. Cardiovasc. Interv. 2021, 97, E911–E918. [Google Scholar] [CrossRef]
- Hesse, K.; Mehta, S.; et al. Combined Rotational Excimer Laser Coronary Atherectomy (RASER) in Non-Crossable, Non-Dilatable Coronary Artery Disease: Observations from a Single Center. [CrossRef]
- Kereiakes, D.J.; Virmani, R.; et al. Principles of Intravascular Lithotripsy for Calcific Plaque Modification. JACC Cardiovasc. Interv. 2021, 14, 1275–1292. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, C.; Vilela, M.; et al. Coronary Intravascular Lithotripsy Effectiveness and Safety in a Real-World Cohort. J. Pers. Med. 2024, 14, 438. [Google Scholar] [CrossRef]
- Honton, B.; Monsegu, J. Best Practice in Intravascular Lithotripsy. Interv. Cardiol. (Lond. Engl.) 2022, 17, e02. [Google Scholar] [CrossRef]
- Forero, M.T.; Sardella, G.; et al. Coronary Lithotripsy for the Treatment of Underexpanded Stents: The International Multicentre CRUNCH Registry. EuroIntervention 2022. [Google Scholar] [CrossRef]
- Kaul, A.; Dhalla, P.S.; et al. Current Treatment Modalities for Calcified Coronary Artery Disease: A Review Article Comparing Novel Intravascular Lithotripsy and Traditional Rotational Atherectomy. Cureus 2020, 12, e10922. [Google Scholar] [CrossRef]
- Hill, J.M.; Kereiakes, D.J.; et al. Intravascular Lithotripsy for Treatment of Severely Calcified Coronary Artery Disease. J. Am. Coll. Cardiol. 2020, 76, 2635–2646. [Google Scholar] [CrossRef]
- Wu, T.; Yang, H.; et al. The Safety and Efficacy of Intravascular Lithotripsy in the Treatment of Severe Coronary Artery Calcification in 261 Cases: A Retrospective Study. Health Sci. Rep. 2025, 8, e70474. [Google Scholar] [CrossRef]
- van Oort, M.J.H.; Al Amri, I.; et al. Evolving Use and Clinical Outcomes of Coronary Intravascular Lithotripsy: Insights from an International, Multicentre Registry. Heart 2024, 111, 62–68. [Google Scholar] [CrossRef]
- Shockwave Medical, I. Prospective, Multicenter, Single-Arm, Investigational Device Exemption (IDE) Study of the Shockwave Intravascular Lithotripsy (IVL) System with the Shockwave Javelin Coronary IVL Catheter (FORWARD CAD IDE Study); Clinical trial registration NCT06662500; clinicaltrials.gov, 2025.
- Russo, D.; Massaro, G.; et al. Contemporary Approach to Heavily Calcified Lesions: Tools of the Trade, Challenges, and Pitfalls. Vessel Plus 2024, 8. [Google Scholar] [CrossRef]
- Sasi, V.; Szántó, G.; et al. Combination of Laser Atherectomy and Super High-Pressure Non-Compliant Balloon to Treat Stent Under-Expansion in Cases of Failed Interventional Options. Interv. Cardiol. 2023, 18, e23. [Google Scholar] [CrossRef]
- Yeung, J.Y.K.; Chiang, M. Current Role of Excimer Laser Coronary Angioplasty Atherectomy in Calcified Coronary Artery Disease Management. JACC Case Rep. 2025, 30, 103025. [Google Scholar] [CrossRef] [PubMed]
- Medical, E. LithiX HC-IVL: Advanced Intravascular Lithotripsy for Calcified Coronary Lesions, 2025. Elixir Medical Website.
- PCR. EuroPCR 2024: Primary Outcomes from PINNACLE I Clinical Trial Establish Safety and Effectiveness of Elixir Medical’s Hertz Contact Intravascular Lithotripsy System for Calcium Fragmentation in Moderate to Severe Calcified Coronary Artery Lesions, 2024. Press Release, PCR Online.
- Bennett, J.; Hamer, B.; et al. TCT-381 Safety and Effectiveness of a Novel Intravascular Lithotripsy Device Using the Hertz Contact Stress Mechanism for Calcium Fragmentation: Six-Month Outcomes of the PINNACLE I Clinical Trial. J. Am. Coll. Cardiol. 2024, 84, B104–B104. [Google Scholar] [CrossRef]
Table 2.
Calcified coronary lesions scoring systems for OCT and IVUS reproduced from Sato et al. [14] and Jurado-Román et al. [13].
| OCT | IVUS | |||||||
| Calcium arc | <360° | 0 | Calcium arc | ≤270° | 0 | |||
| 360 ° | 1 | >270° and >5 mm length | 1 | |||||
| Calcium thickness | ≤0.3 mm | 0 | Calcified nodule | No | 0 | |||
| >0.3 mm | 1 | Yes | 1 | |||||
| Length of calcium >270° | ≤3 mm | 0 | Coronary artery diameter | ≥3.5 mm | 0 | |||
| >3 mm | 1 | <3.5 mm | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



