
Submitted:
20 October 2025
Posted:
21 October 2025
You are already at the latest version
Abstract
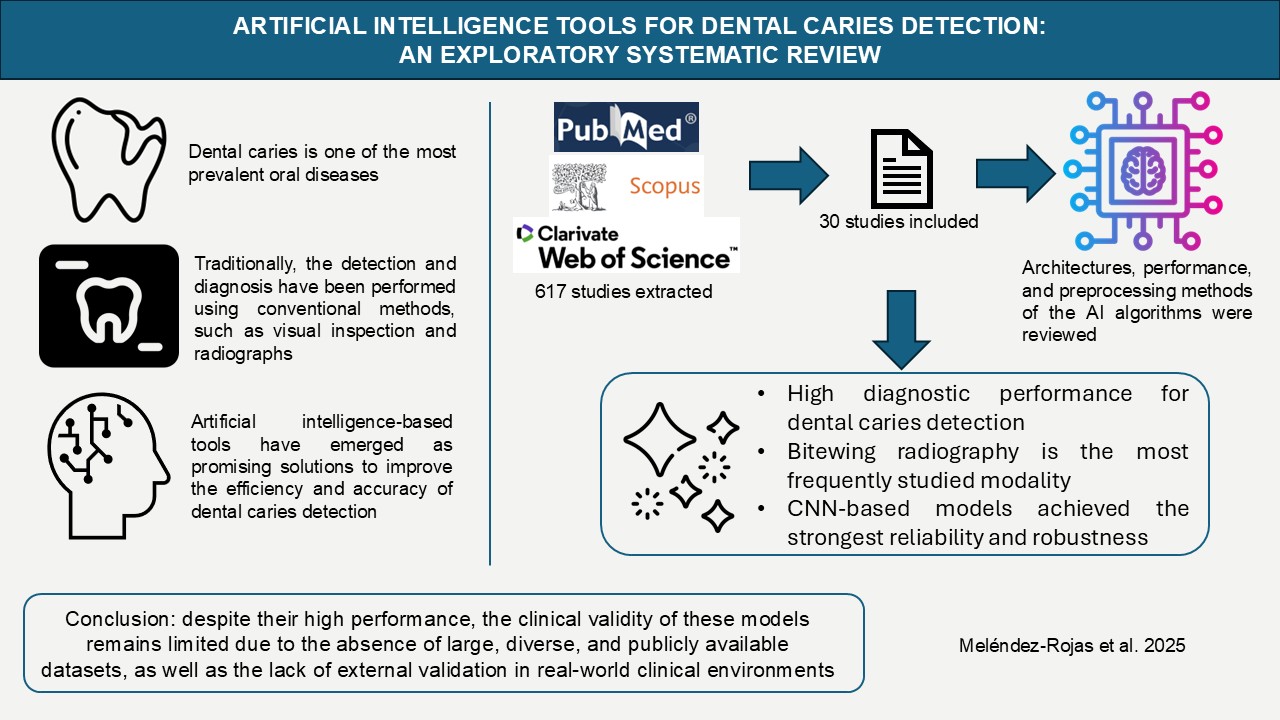
Background/Objectives: Dental caries is one of the most prevalent oral diseases. Traditionally, the detection and diagnosis have been performed using conventional methods, such as visual inspection and radiographs. In this context, artificial intelligence-based tools have emerged as promising solutions to improve the efficiency and accuracy of dental caries detection. The objective of this scoping review was to map the scientific evidence available in the literature on the use of artificial intelligence tools for the detection of dental caries. Methods: This review was conducted following the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews) guidelines. A literature search was performed in the PubMed, Scopus, and Web of Science (WoS) databases using the search expression "artificial intelligence AND dental caries". Inclusion criteria were articles published in the last five years, in English or Spanish and available in full text. Results: The initial search yielded 617 records. After reviewing titles, 143 articles were selected, and upon removing duplicates, 93 unique entries remained. Following abstract evaluation, 40 articles were chosen for full-text review. Finally, 30 publications were included in this review. Conclusions: The evidence shows that artificial intelligence (AI) tools applied to dental caries detection have demonstrated significant improvements in diagnostic accuracy, with sensitivity and specificity values that are comparable to or even exceed those of traditional methods. Thus, the evidence indicates that the integration of AI is no longer a question of if, but how profoundly it will reshape the existing paradigms of dental diagnostics.
Keywords:
dental caries/diagnosis
; artificial intelligence
; machine learning
; deep learning
; diagnostic imaging
1. Introduction
Dental caries continues to represent a major public health problem in Chile, with a prevalence of 73.9% among 15-year-olds and 99.2% in adults aged 35 to 44 years [1]. Traditionally, its detection and diagnosis have been based on conventional methods such as visual inspection [2], the use of dental probes [3], and radiographic imaging [3]. Although these approaches remain widely implemented in daily practice, they present inherent limitations in terms of sensitivity, reproducibility, and standardization. In this context, artificial intelligence (AI) has emerged as a promising technological innovation, relying on algorithms capable of simulating human learning and decision-making processes [4] for the analysis of a wide range of dental images [5].
The incorporation of AI into dentistry has demonstrated multiple advantages. These include reductions in diagnostic time [5], decreases in error rates [6], and improvements in diagnostic accuracy [7], all of which contribute to optimized treatment planning [8], enhanced clinical efficiency [3], and the reduction of risks associated with diagnostic uncertainty [7]. More specifically, techniques such as machine learning (ML), artificial neural networks (ANN) and convolutional neural networks (CNN) have exhibited the ability to process and analyze large volumes of data with high precision [9], accelerate evaluation processes [5,10], reduce inter-professional variability [4], facilitate the early identification of incipient lesions that allow for minimally invasive interventions [11], and ultimately improve the overall efficiency of dental practice [12].
Nevertheless, despite the considerable potential of AI, its implementation in dentistry continues to face significant challenges. The quality, diversity, and representativeness of training data are decisive factors, since biased or insufficient datasets may compromise the performance and generalizability of algorithms [4]. Moreover, appropriate technological infrastructure and professional training are indispensable for the effective adoption of these tools [13]. In parallel, the establishment of robust regulatory frameworks is required to promote responsible and ethical integration of AI, ensuring both patient safety and the preservation of professional standards. This scenario explains the heterogeneity observed in the existing literature, which complicates the systematic synthesis of knowledge regarding these emerging technologies.
The justification for addressing this problem stems from the pressing need to overcome such barriers while capitalizing on the proven benefits of AI to transform dental practice. A systematic analysis and organization of the available scientific evidence are therefore essential to maximize the clinical applicability of these tools and to contribute to the global advancement of oral health. Accordingly, the objective of this study is to provide a comprehensive overview of the current landscape of AI in the detection of dental caries, emphasizing its potential to reshape conventional diagnostic paradigms and strengthen evidence-based decision making in dentistry.
In alignment with this objective, the study specifically aims to: (i) compile the scientific evidence published in the last five years on AI tools for the detection of dental caries; (ii) compare the architectures employed in the development of the algorithms; (iii) analyze the functioning and reported performance of AI tools; and (iv) examine the preprocessing methods applied in the included studies.
2. Materials and Methods
This scoping review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines. The present review incorporated academic publications and scientific articles published within the last five years, indexed in PubMed, Scopus, and Web of Science (WoS), and available up to June 2024. Eligible studies were required to investigate the use of AI for the detection of dental caries, provide access to the full text, and be published in either English or Spanish. In contrast, opinion pieces, editorials, review articles, and studies that employed AI for pedagogical purposes were excluded, as were articles related to periodontics, endodontics, or oral cancer.
The search was conducted in June 2024 using the electronic databases PubMed, Scopus, and Web of Science. The strategy was based on standardized Medical Subject Headings (MeSH) terms, specifically “Artificial Intelligence” and “Dental Caries,” combined with the Boolean operator “AND,” resulting in the query “Artificial Intelligence AND Dental Caries.” This process generated a set of records that, after the removal of duplicates across databases, were subjected to an initial screening by title to retain those potentially relevant to the research question. Subsequently, the remaining publications underwent a more detailed evaluation, during which studies that did not meet the predefined inclusion criteria or for which full-text access was not available were excluded.
The selection process was independently conducted by two authors, and in cases where discrepancies arose, these were resolved through discussion with a third author. The remaining studies were then subjected to abstract screening, after which only those that directly addressed the research question were retained. The final pool of documents underwent critical appraisal in accordance with the TRIPOD-AI guidelines [14], with particular emphasis on methodological rigor, ethical considerations, and the clarity and reproducibility of the reported results, ensuring that each study adequately addressed the research objectives. The use of TRIPOD-AI served as a framework for bias control, ensuring that the included studies provided transparent, reliable, and verifiable evidence that adequately addressed the research objectives.
3. Results
The systematic search identified a total of 617 records, of which 159 were retrieved from PubMed, 290 from Scopus, and 166 from Web of Science, along with two additional studies identified outside the automated search strategy (Figure 1).
After the removal of duplicate entries across databases, the records were screened by title, resulting in the selection of publications that were potentially relevant to the research question. In the subsequent evaluation phase, studies that did not meet the inclusion criteria were excluded, as well as those for which full-text access was not available. Following abstract review, only studies that directly addressed the research objectives were retained, ultimately leading to the inclusion of 30 publications in this review (Table 1).
The temporal analysis of the included studies shows a steady increase in research output between 2019 and 2024, with a notable peak in 2022 (Figure 2). The geographic distribution of publications, highlighting the countries contributing the most to this research field, is presented in Figure 3.
The average compliance with the TRIPOD-AI checklist among studies developing and evaluating prediction models for dental caries was estimated between 80% and 85%. However, several recurrent deficiencies were identified. The most critical was the lack of a definitive gold standard for ground truth, as most studies relied on expert clinical annotation and consensus—often with high inter-rater agreement (Kappa > 0.75)—instead of histological or micro-CT verification. In addition, formal sample size calculations were generally absent, and the generalizability of results was limited by the predominant use of data from single institutions or ex vivo settings. Finally, a recurring shortcoming was the inadequate handling and reporting of class imbalance, particularly regarding the low prevalence of rare or severe lesions, which contributed to reduced model performance in minority classes despite high overall metrics (Table 1).
The studies included in this review assessed a wide spectrum of artificial intelligence applications for dental caries detection across different imaging modalities and diagnostic techniques (Figure 4). The performance of these approaches varied depending on the type of input data, the architecture employed, and the methodological rigor of the studies. Below, the main findings are summarized by technique, highlighting the strengths, limitations, and clinical implications of each approach.
The analysis of intraoral photography revealed heterogeneous performance across architectures, with models such as MobileNetV2 (sensitivity 0.925; specificity 0.896) and VGG-16 (AUC 0.8565; sensitivity 0.819) standing out for their accessibility and clinical potential, though their accuracy was strongly influenced by image quality [18,20,27,32]. More advanced frameworks, including Cascade R-CNN (specificity 0.96; sensitivity 0.732) and Mask R-CNN (accuracy 0.889), demonstrated higher robustness but required considerable computational resources, limiting their applicability [10]. In contrast, UV absorption spectroscopy, applied to salivary samples, achieved perfect sensitivity and specificity, highlighting its potential for noninvasive diagnosis [15].
CBCT yielded high diagnostic values (accuracy 0.953; sensitivity 0.921; specificity 0.963), though its integration into routine practice remains constrained by the high technical and resource requirements of this imaging modality [11]. Dental (periapical) radiography studies reported variable outcomes: while Faster R-CNN demonstrated moderate accuracy (0.7349) with rapid processing times (0.1923 s per image), Deeplabv3 achieved very high average accuracy (0.994) but poor segmentation performance (IoU mean 0.5073), reflecting challenges in lesion delineation [6,16].
Emerging methods, such as TFSNs, supported by U-Net and NASNet, reported moderate diagnostic performance (sensitivity 0.8026; PPV 0.7636), particularly for early-stage caries [8]. In panoramic radiographs, architectures such as ResNet18 (accuracy 82.72%; sensitivity 0.8538; specificity 0.877), MobileNetV2 (accuracy 0.87; specificity 0.88), and DCDNet (accuracy 0.72) showed variable but promising results for large-scale screening, with MobileNetV2 offering practical advantages for resource-limited environments [17,18,19].
NILT emerged as a radiation-free alternative, with ResNet18–ResNeXt50 combinations achieving moderate accuracy (0.69) and AUC (0.74), while U-Net with VGG-16 improved segmentation performance (mIoU 0.727). Nonetheless, the sensitivity remained relatively low (0.59), limiting its reliability despite favorable AUC values in vivo (0.78) compared to in vitro settings (0.65) [20,21,22]. Studies exploring clinical data and salivary biomarkers through neural networks also demonstrated encouraging performance, with accuracy values above 83%, reinforcing their potential role in complementary diagnosis [23].
Bitewing radiographs, the most frequently studied modality (13 publications), confirmed the versatility of deep learning architectures. U-Net models consistently reached high accuracy (0.9491) and F1-scores (0.8818), while AlexNet (accuracy 0.903) and VGG19 (accuracy 0.94) underscored the potential of classical CNNs (24,25,26,27). Advanced models such as Faster R-CNN and VGG-16 reported robust metrics (accuracy 0.861; specificity 0.985; AUC 0.948), and DarkNet-53 achieved strong discriminatory power (AUC 0.9564; specificity 98.18%) despite a lower sensitivity (72.26%) (7,28,29). RetinaNet, YOLOv5, and EfficientDet applied in the HUNT4 Oral Health Study reached a mean Average Precision (mAP) of 0.647, supporting the utility of large datasets for model validation [4]. Finally, Mask R-CNN obtained consistent AUC values (>0.80) for both primary and secondary caries, with data augmentation improving sensitivity and robustness across clinical conditions [12].
4. Discussion
This review highlights a research field in notable expansion, driven by technological advancements and a growing interest in its integration into dental practice. A multidisciplinary effort is evident to identify the most effective AI applications, exploring a variety of imaging techniques and analytical methods. While bitewing radiographs are the most used, there is a trend towards investigating new imaging technologies, seeking advantages in early and non-invasive detection.
The analyzed studies underscore the transformative potential of AI, especially CNNs, in caries diagnosis, enhancing clinical accuracy and efficiency. Deep learning (DL) algorithms such as U-Net, Faster R-CNN, and Mask R-CNN have demonstrated substantial improvements in diagnostic accuracy, with models like U-Net achieving superior sensitivity (0.75) compared to professionals (0.36) in certain contexts. These automated systems can distinguish between primary and secondary caries and identify incipient lesions with greater sensitivity than traditional methods, also optimizing workflow by directing the clinician’s attention to relevant areas of interest.
The premise of this review regarding the ability of AI models, such as the U-Net architecture, to surpass clinical performance is validated by the literature, which consistently reports that AI enhances the accuracy and sensitivity of dentists [30,31]. For example, AI sensitivity (0.75) has been shown to be significantly higher than the average dentist sensitivity (0.36) in the detection of proximal caries on bitewings [30,32]. This improved sensitivity is particularly relevant, as AI assistance has been observed to substantially increase clinicians’ ability to identify initial or moderate lesions (the categories most easily overlooked) with significant improvements in sensitivity for these subgroups [33]. Nonetheless, this high diagnostic precision must be weighed against reported limitations: AI often shows weaker performance for caries detection (lower sensitivity and lower AUC) compared to other dental pathologies, such as residual roots or crowns, in both panoramic radiographs and CBCT [34,35]. For instance, in a multi-diagnostic framework, AI demonstrated very high specificity (0.990) but the lowest sensitivity (0.554) for caries, with an AUC significantly lower than that achieved by highly experienced dentists [34]. In line with the methodological shortcomings identified in this review, the literature confirms that the lack of a strict ground truth (e.g., histology or micro-CT) is the most critical limitation [5,33,35], since most models are trained on expert consensus as the gold standard, which can introduce biases inherent to human judgment [5,35]. Generalizability is further limited by the predominant use of single-source data [34]. Unlike the earlier review by Mohammad-Rahimi et al. [36], which highlighted promising results but limited study quality, our work not only applies TRIPOD-AI criteria to mitigate bias but also provides clinically oriented insights into the applicability of AI tools for caries detection in real-world practice.
Regarding clinical workflow impact, beyond the optimization noted in this manuscript, eye-tracking studies confirm that dentists assisted by AI display more efficient visual behavior, focusing on relevant regions (caries and restorations) in significantly less time [31]. This efficiency translates into substantial time savings: one AI system for panoramic radiographs achieved an average diagnostic time of 1.5 seconds per radiograph, compared with 53.8 seconds for dentists [34]. Finally, although AI increases diagnostic precision, its cost-effectiveness is only realized when early detection leads to non-restorative, minimally invasive management rather than an increase in invasive interventions [30].
Nevertheless, clinical implementation faces important challenges, mainly the generalizability of models and variability in image quality. This underscores the need for extensive, high-quality datasets representative of diverse clinical scenarios. Other obstacles include the transparency and explainability of AI models (the “black box” problem), the requirement for large volumes of data for training, and the imperative need to establish robust ethical and regulatory frameworks to ensure safe and effective use. Interdisciplinary collaboration between AI developers and dental professionals is indispensable to ensure that the tools meet clinical requirements and are of practical utility.
This review confirms that AI (particularly CNN-based DL architectures) has considerably improved sensitivity, specificity, and reduced inter-observer variability, addressing a persistent challenge in conventional dentistry. However, despite the promising performance reported in controlled studies, validation in real-world clinical settings remains imperative. Future research should focus on the development of more robust, clinically applicable, transparent, and reproducible models, trained on large and diverse datasets. Moreover, improving the interpretability of AI to foster clinician trust, together with the establishment of ethical and regulatory frameworks that safeguard safety and privacy, will be essential for translating these advances into sustainable clinical practice.
5. Conclusions
The AI frameworks, particularly those leveraging DL and CNN architectures, exhibit robust diagnostic efficacy in the detection of dental caries. This efficacy is demonstrated across a spectrum of imaging modalities, with bitewing radiography being the most extensively investigated. The aggregated findings substantiate that these computational models consistently yield performance metrics (notably accuracy, sensitivity, and specificity) that are commensurate with, and in several instances surpass, the diagnostic benchmarks of conventional clinical assessment. Consequently, this work systematically fulfills its primary objectives by not only charting the predominant algorithmic architectures and data preprocessing pipelines but also by critically evaluating their reported efficacy. Finally, this review positions AI not merely as a technological novelty but as a validated and increasingly integral adjunct poised to redefine the paradigms of diagnostic accuracy in contemporary dentistry.
Author Contributions
Conceptualization, P.M.-R., M.R.-L., M.D.-A., S.N.-E., M.F.V.-D., J.J.-R. and A.V.-B.; methodology, P.M.-R., M.R.-L. and S.N.-E..; validation, P.M.-R., M.R.-L., M.D.-A. and S.N.-E.; formal analysis, P.M.-R., M.R.-L., M.D.-A., S.N.-E., M.F.V.-D., J.J.-R. and A.V.-B.; investigation, P.M.-R., M.R.-L. and M.D.-A.; writing—original draft preparation, P.M.-R.; writing—review and editing, P.M.-R., M.R.-L., M.D.-A., S.N.-E., M.F.V.-D., J.J.-R. and A.V.-B.; project administration, P.M.-R.; funding acquisition, P.M.-R.. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the Agencia Nacional de Investigación y Desarrollo (ANID), Chile, through the Doctorado en Chile Scholarship Program, Academic Year 2025 (Grant No. 1340/2025).
Data Availability Statement
All data supporting the findings of this systematic review are derived from previously published articles that are publicly available in their corresponding databases (PubMed, Scopus, and WoS). As this study did not generate or analyze primary datasets, no new data was created. The full list of publications included in this review is provided in the manuscript and serves as a direct reference to the original data sources.
Conflicts of Interest
The authors declare no financial or non-financial conflicts of interest that could be perceived as influencing the work reported in this manuscript.
Abbreviations
The following abbreviations are used in this manuscript:
| PRISMA-ScR | Preferred reporting items for systematic reviews and meta-analyses extension for scoping reviews |
| WoS | Web of science |
| AI | Artificial intelligence |
| ML | Machine learning |
| ANN | Artificial neural network |
| CNN | Convolutional neural network |
| MeSH | Medical subject headings |
| TRIPOD-AI | Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis |
| IoU | Intersection over union |
| AUC | Area under the curve |
| SE | Sensitivity |
| SP | Specificity |
| PPV | Positive predictive value |
| NPV | Negative predictive value |
| NILT | Near-infrared light transillumination |
| TFSNs | Targeted fluorescent nanoparticles |
| UV | Ultraviolet |
| CD | Caries detection |
| CBCT | Cone beam computed tomography |
| Micro-CT | Micro computed tomography |
| DL | Deep learning |
References
- Phillips M, Bernabé E, Mustakis A. (2020). Radiographic assessment of proximal surface carious lesion progression in Chilean young adults. Community dentistry and oral epidemiology, 48(5), 409–414. [CrossRef]
- Kühnisch J, Meyer O, Hesenius M, Hickel R, Gruhn V. (2022). Caries Detection on Intraoral Images Using Artificial Intelligence. Journal of dental research, 101(2), 158–165. [CrossRef]
- Chan EK, Wah YY, Lam WY, Chu CH, Yu OY. (2023). Use of Digital Diagnostic Aids for Initial Caries Detection: A Review. Dentistry journal, 11(10), 232. [CrossRef]
- Pérez de Frutos J, Holden Helland R, Desai S, Nymoen LC, Langø T, Remman T, Sen A. (2024). AI-Dentify: deep learning for proximal caries detection on bitewing x-ray - HUNT4 Oral Health Study. BMC oral health, 24(1), 344. [CrossRef]
- Arsiwala-Scheppach LT, Castner NJ, Rohrer C, Mertens S, Kasneci E, Cejudo Grano de Oro JE, Schwendicke F. (2024). Impact of artificial intelligence on dentists’ gaze during caries detection: A randomized controlled trial. Journal of dentistry, 140, 104793. [CrossRef]
- Zhu Y, Xu T, Peng L, Cao Y, Zhao X, Li S, Zhao Y, Meng F, Ding J, Liang S. (2022). Faster-RCNN based intelligent detection and localization of dental caries. Displays. 74. 102201. 10.1016/j.displa.2022.102201.
- García-Cañas Á, Bonfanti-Gris M, Paraíso-Medina S, Martínez-Rus F, Pradíes G. (2022). Diagnosis of Interproximal Caries Lesions in Bitewing Radiographs Using a Deep Convolutional Neural Network-Based Software. Caries research, 56(5-6), 503–511. [CrossRef]
- Schwendicke F, Mertens S, Cantu AG, Chaurasia A, Meyer-Lueckel H, Krois J. (2022). Cost-effectiveness of AI for caries detection: randomized trial. Journal of dentistry, 119, 104080. [CrossRef]
- Panyarak W, Wantanajittikul K, Suttapak W, Charuakkra A, Prapayasatok S. (2023). Feasibility of deep learning for dental caries classification in bitewing radiographs based on the ICCMS™ radiographic scoring system. Oral surgery, oral medicine, oral pathology and oral radiology, 135(2), 272–281. [CrossRef]
- Moutselos K, Berdouses E, Oulis C, Maglogiannis I. (2019). Recognizing Occlusal Caries in Dental Intraoral Images Using Deep Learning. Annual International Conference of the IEEE Engineering in Medicine and Biology Society. IEEE Engineering in Medicine and Biology Society. Annual International Conference, 2019, 1617–1620. [CrossRef]
- Esmaeilyfard R, Bonyadifard H, Paknahad M. (2024). Dental Caries Detection and Classification in CBCT Images Using Deep Learning. International dental journal, 74(2), 328–334. [CrossRef]
- Chaves ET, Vinayahalingam S, van Nistelrooij N, Xi T, Romero VHD, Flügge T, Saker H, Kim A, Lima GDS, Loomans B, Huysmans MC, Mendes FM, Cenci MS. (2024). Detection of caries around restorations on bitewings using deep learning. Journal of dentistry, 143, 104886. [CrossRef]
- Cantu AG, Gehrung S, Krois J, Chaurasia A, Rossi JG, Gaudin R, Elhennawy K, Schwendicke F. (2020). Detecting caries lesions of different radiographic extension on bitewings using deep learning. Journal of dentistry, 100, 103425. [CrossRef]
- Collins GS, Moons KGM, Dhiman P, Riley RD, Beam AL, Van Calster B, Ghassemi M, Liu X, Reitsma JB, van Smeden M, Boulesteix AL, Camaradou JC, Celi LA, Denaxas S, Denniston AK, Glocker B, Golub RM, Harvey H, Heinze G, Hoffman MM, et al. (2024). TRIPOD+AI statement: updated guidance for reporting clinical prediction models that use regression or machine learning methods. BMJ (Clinical research ed.), 385, e078378. [CrossRef]
- Basri KN, Yazid F, Mohd Zain MN, Md Yusof Z, Abdul Rani R, Zoolfakar AS. (2024). Artificial neural network and convolutional neural network for prediction of dental caries. Spectrochimica acta. Part A, Molecular and biomolecular spectroscopy, 312, 124063. [CrossRef]
- Qayyum A, Tahir A, Butt MA, Luke A, Abbas HT, Qadir J, Arshad K, Assaleh K, Imran MA, Abbasi QH. (2023). Dental caries detection using a semi-supervised learning approach. Scientific reports, 13(1), 749. [CrossRef]
- Zhou X, Yu G, Yin Q, Liu Y, Zhang Z, Sun J. (2022). Context Aware Convolutional Neural Network for Children Caries Diagnosis on Dental Panoramic Radiographs. Computational and mathematical methods in medicine, 2022, 6029245. [CrossRef]
- Dayı B, Üzen H, Çiçek İB, Duman ŞB. (2023). A Novel Deep Learning-Based Approach for Segmentation of Different Type Caries Lesions on Panoramic Radiographs. Diagnostics (Basel, Switzerland), 13(2), 202. [CrossRef]
- Vinayahalingam S, Kempers S, Limon L, Deibel D, Maal T, Hanisch M, Bergé S, Xi T. (2021). Classification of caries in third molars on panoramic radiographs using deep learning. Scientific reports, 11(1), 12609. [CrossRef]
- Holtkamp A, Elhennawy K, Cejudo Grano de Oro JE, Krois J, Paris S, Schwendicke F. (2021). Generalizability of Deep Learning Models for Caries Detection in Near-Infrared Light Transillumination Images. Journal of clinical medicine, 10(5), 961. [CrossRef]
- Schwendicke F, Elhennawy K, Paris S, Friebertshäuser P, Krois J. (2020). Deep learning for caries lesion detection in near-infrared light transillumination images: A pilot study. Journal of dentistry, 92, 103260. [CrossRef]
- Casalegno F, Newton T, Daher R, Abdelaziz M, Lodi-Rizzini A, Schürmann F, Krejci I, Markram H. (2019). Caries Detection with Near-Infrared Transillumination Using Deep Learning. Journal of dental research, 98(11), 1227–1233. [CrossRef]
- Udod OA, Voronina HS, Ivchenkova OY. (2020). Application of neural network technologies in the dental caries forecast. Wiadomosci lekarskie (Warsaw, Poland : 1960), 73(7), 1499–1504.
- Ahmed W, Azhari A, Fawaz K, Ahmed H, Alsadah Z, Majumdar A, Carvalho R. (2023). Artificial intelligence in the detection and classification of dental caries. The Journal of Prosthetic Dentistry. 133. 10.1016/j.prosdent.2023.07.013.
- Baydar O, Różyło-Kalinowska I, Futyma-Gąbka K, Sağlam H. (2023). The U-Net Approaches to Evaluation of Dental Bite-Wing Radiographs: An Artificial Intelligence Study. Diagnostics (Basel, Switzerland), 13(3), 453. [CrossRef]
- Mao YC, Chen TY, Chou HS, Lin SY, Liu SY, Chen YA, Liu YL, Chen CA, Huang YC, Chen SL, Li CW, Abu PAR, Chiang WY. (2021). Caries and Restoration Detection Using Bitewing Film Based on Transfer Learning with CNNs. Sensors (Basel, Switzerland), 21(13), 4613. [CrossRef]
- ForouzeshFar P, Safaei AA, Ghaderi F, Hashemikamangar SS. (2024). Dental Caries diagnosis from bitewing images using convolutional neural networks. BMC oral health, 24(1), 211. [CrossRef]
- Bayraktar Y, Ayan E. (2022). Diagnosis of interproximal caries lesions with deep convolutional neural network in digital bitewing radiographs. Clinical oral investigations, 26(1), 623–632. [CrossRef]
- Estai M, Tennant M, Gebauer D, Brostek A, Vignarajan J, Mehdizadeh M, Saha S. (2022). Evaluation of a deep learning system for automatic detection of proximal surface dental caries on bitewing radiographs. Oral surgery, oral medicine, oral pathology and oral radiology, 134(2), 262–270. [CrossRef]
- Schwendicke F, Rossi JG, Göstemeyer G, Elhennawy K, Cantu AG, Gaudin R, Chaurasia A, Gehrung S, Krois J. (2021). Cost-effectiveness of Artificial Intelligence for Proximal Caries Detection. Journal of dental research, 100(4), 369–376. [CrossRef]
- Arsiwala-Scheppach LT, Castner NJ, Rohrer C, Mertens S, Kasneci E, Cejudo Grano de Oro JE, Schwendicke F. (2024). Impact of artificial intelligence on dentists’ gaze during caries detection: A randomized controlled trial. Journal of Dentistry, 140, 104793. [CrossRef]
- Amasya H, Alkhader M, Serindere G, Futyma-Gąbka K, Aktuna Belgin C, Gusarev M, Ezhov M, Różyło-Kalinowska I, Önder M, Sanders A, Costa ALF, Castro Lopes SLP, Orhan K. (2023). Evaluation of a Decision Support System Developed with Deep Learning Approach for Detecting Dental Caries with Cone-Beam Computed Tomography Imaging. Diagnostics (Basel, Switzerland), 13(22), 3471. [CrossRef]
- Lee S, Oh SI, Jo J, Kang S, Shin Y, Park JW. (2021). Deep learning for early dental caries detection in bitewing radiographs. Scientific reports, 11(1), 16807. [CrossRef]
- Zhu J, Chen Z, Zhao J, Yu Y, Li X, Shi K, Zhang F, Yu F, Shi K, Sun Z, Lin N, Zheng Y. (2023). Artificial intelligence in the diagnosis of dental diseases on panoramic radiographs: a preliminary study. BMC oral health, 23(1), 358. [CrossRef]
- Amasya H, Alkhader M, Serindere G, Futyma-Gąbka K, Aktuna Belgin C, Gusarev M, Ezhov M, Różyło-Kalinowska I, Önder M, Sanders A, Ferreira Costa AL, Pereira de Castro Lopes SL, Orhan K. (2023). Evaluation of a decision support system developed with deep learning approach for detecting dental caries with cone-beam computed tomography imaging. Diagnostics, 13(22), 3471. [CrossRef]
- Mohammad-Rahimi H, Motamedian SR, Rohban MH, Krois J, Uribe SE, Mahmoudinia E, Rokhshad R, Nadimi M, Schwendicke F. (2022). Deep learning for caries detection: A systematic review. Journal of Dentistry, 122, 104115. [CrossRef]
- Yoon K, Jeong HM, Kim JW, Park JH, Choi J. (2024). AI-based dental caries and tooth number detection in intraoral photos: Model development and performance evaluation. Journal of dentistry, 141, 104821. [CrossRef]
- Jones KA, Jones N, Tenuta LMA, Bloembergen W, Flannagan SE, González-Cabezas C, Clarkson B, Pan LC, Lahann J, Bloembergen S. (2022). Convolution Neural Networks and Targeted Fluorescent Nanoparticles to Detect and ICDAS Score Caries. Caries research, 56(4), 419–428. [CrossRef]
- Chen X, Guo J, Ye J, Zhang M, Liang Y. (2022). Detection of Proximal Caries Lesions on Bitewing Radiographs Using Deep Learning Method. Caries research, 56(5-6), 455–463. [CrossRef]
- Moran M, Faria M, Giraldi G, Bastos L, Oliveira L, Conci A. (2021). Classification of Approximal Caries in Bitewing Radiographs Using Convolutional Neural Networks. Sensors (Basel, Switzerland), 21(15), 5192. [CrossRef]
- Zhang X, Liang Y, Li W, Liu C, Gu D, Sun W, Miao L. (2022). Development and evaluation of deep learning for screening dental caries from oral photographs. Oral diseases, 28(1), 173–181. [CrossRef]
- Park EY, Cho H, Kang S, Jeong S, Kim EK. (2022). Caries detection with tooth surface segmentation on intraoral photographic images using deep learning. BMC oral health, 22(1), 573. [CrossRef]
Figure 1.
PRISMA flow diagram illustrating the selection process of studies included in the systematic review, from the initial identification of 617 records to the final inclusion of 30 publications.
Figure 1.
PRISMA flow diagram illustrating the selection process of studies included in the systematic review, from the initial identification of 617 records to the final inclusion of 30 publications.
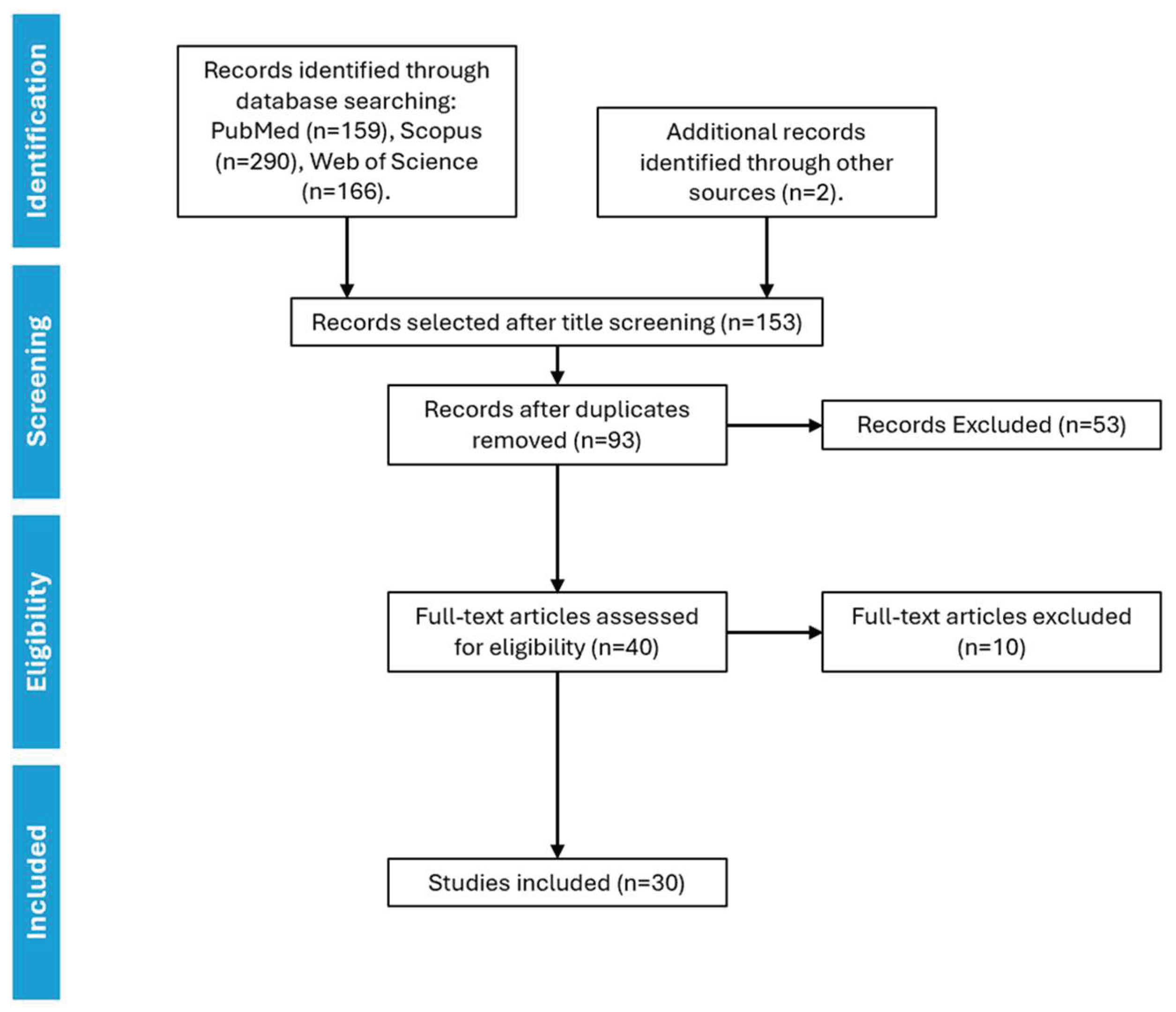
Figure 2.
Temporal distribution of the included studies published between 2019 and 2024, showing a steady increase in research output with a peak in 2022.
Figure 2.
Temporal distribution of the included studies published between 2019 and 2024, showing a steady increase in research output with a peak in 2022.
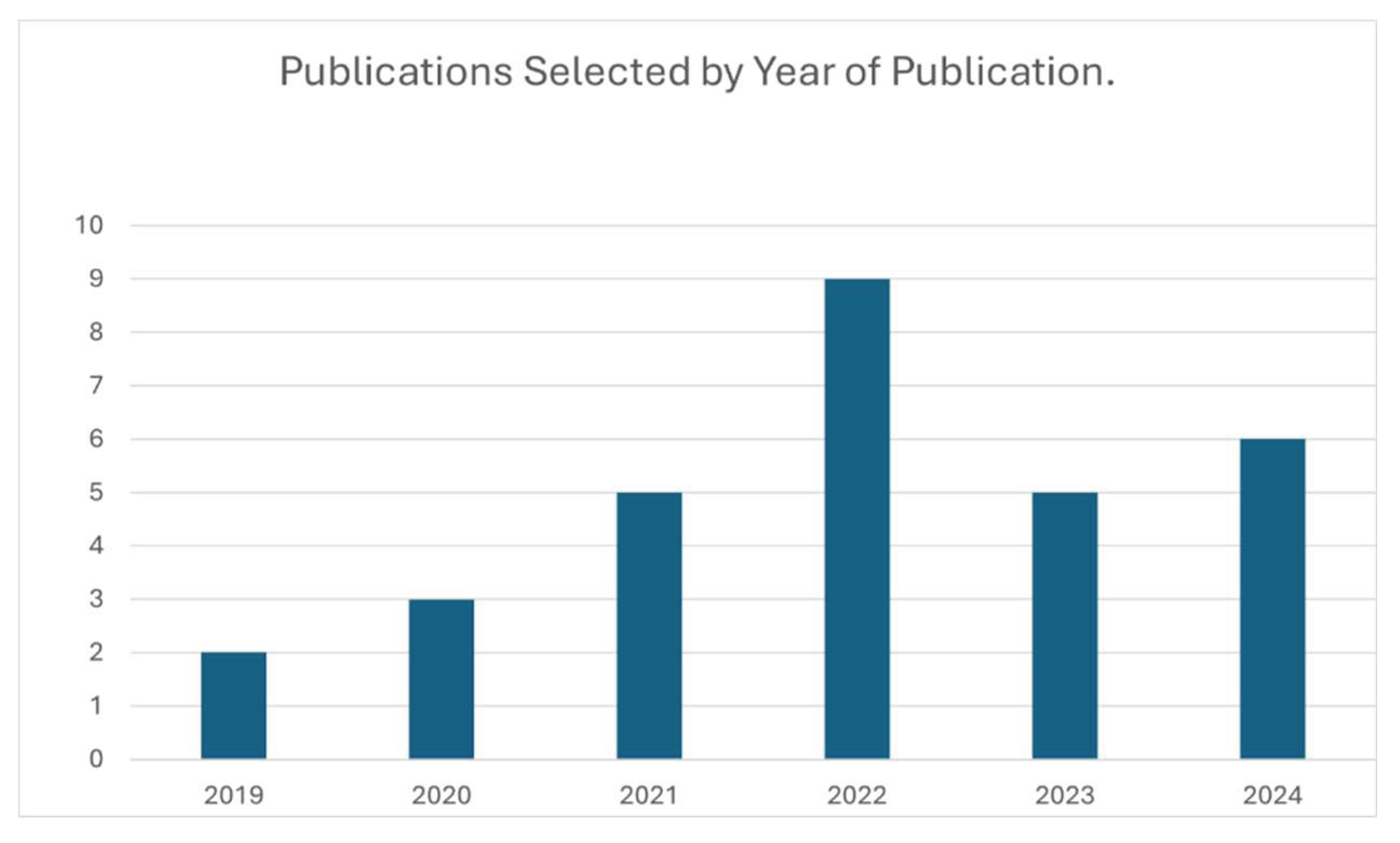
Figure 3.
Geographic distribution of publications by country, highlighting the regions with the highest contribution to the research field on artificial intelligence for dental caries detection.
Figure 3.
Geographic distribution of publications by country, highlighting the regions with the highest contribution to the research field on artificial intelligence for dental caries detection.
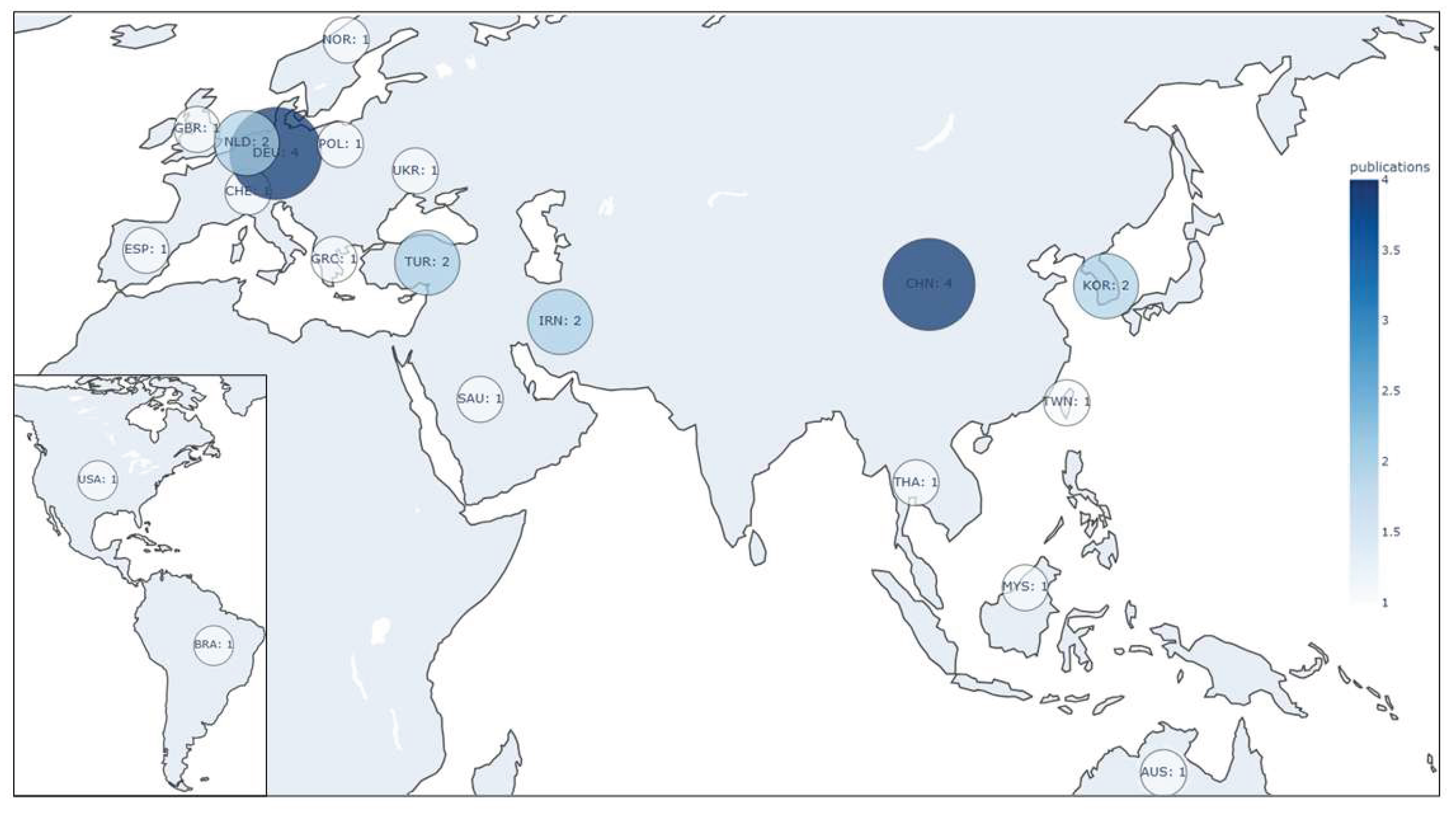
Figure 4.
Overview of the artificial intelligence applications and imaging and data modalities analyzed in the included studies, summarizing their diagnostic performance and methodological characteristics.
Figure 4.
Overview of the artificial intelligence applications and imaging and data modalities analyzed in the included studies, summarizing their diagnostic performance and methodological characteristics.
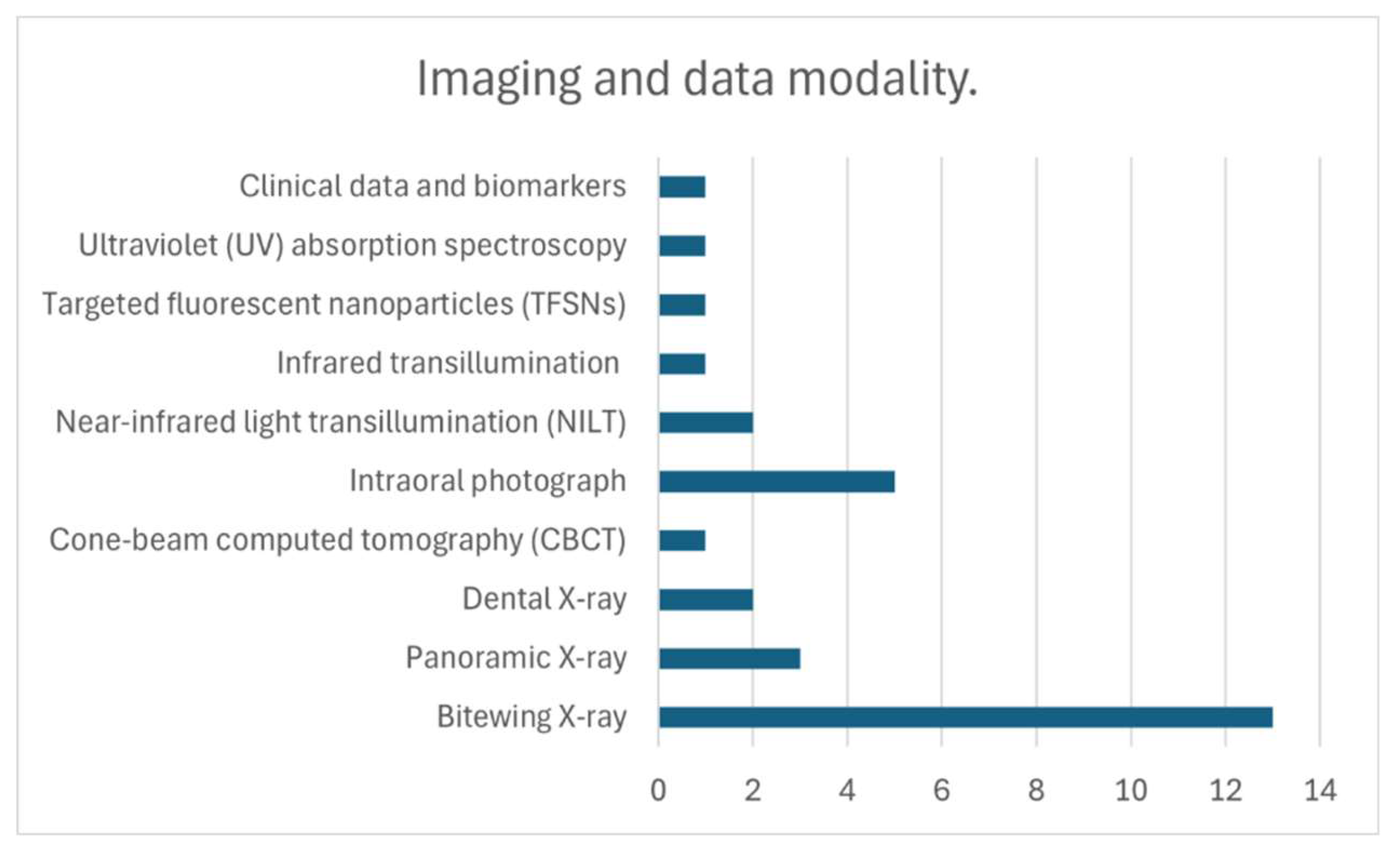

Table 1.
Summary of the main characteristics of the studies included in this systematic review, ordered first by year of publication and then alphabetically by the first author. The table details sample size, imaging modality, AI architecture, performance metrics, and reported outcomes. All reported scores were approximated to two decimal places for consistency.
Table 1.
Summary of the main characteristics of the studies included in this systematic review, ordered first by year of publication and then alphabetically by the first author. The table details sample size, imaging modality, AI architecture, performance metrics, and reported outcomes. All reported scores were approximated to two decimal places for consistency.
| Year | Reference | Country | Sample | Sample Size | Examiners | Preprocessing | Network architecture | Metrics | Results |
|---|---|---|---|---|---|---|---|---|---|
| 2019 | Casalegno F et al. [22] | Switzerland | Infrared transillumination | 217 images | - | Images scaled to 256 × 320 pixels. Data augmentation techniques such as flipping, zoom, rotation, translation, and contrast and brightness adjustment | U-Net + VGG16 | Intersection-over-union (IoU) (mean) | 0.73 |
| IoU proximal | 0.50 | ||||||||
| IoU occlusal | 0.49 | ||||||||
| Area under the curve (AUC) proximal | 0.86 | ||||||||
| AUC occlusal | 0.84 | ||||||||
| 2019 | Moutselos K et al. [10] | Greece | Intraoral photograph | 88 photographs | 2 examiners | Superpixel segmentation for image annotation | Mask R-CNN (based on Feature Pyramid Network (FPN) and ResNet101) | Accuracy (super pixels) (mean) | 0.64 |
| Accuracy (whole image) (mean) | 0.78 | ||||||||
| 2020 | Cantu AG et al. [13] | Germany | Bitewing X-ray | 3686 X-rays | 4 examiners | Images cropped to 512 × 416 pixels. Transformations such as flipping, central cropping, translation, and rotation were applied, as well as contrast and brightness adjustments | U-Net | Accuracy | 0.80 |
| Sensitivity (SE) | 0.75 | ||||||||
| Specificity (SP) | 0.83 | ||||||||
| Positive predictive value (PPV) | 0.70 | ||||||||
| Negative predictive value (NPV) | 0.86 | ||||||||
| F1-score | 0.73 | ||||||||
| 2020 | Schwendicke F et al. [21] | Germany | Near-infrared light transillumination (NILT) | 226 extracted human teeth | 3 examiners | Images cropped to 224 × 224 pixels. Data augmentation was applied, including resizing, random rotations, and horizontal and vertical flipping. | Resnet18, Resnext50 | AUC | 0.74 |
| Accuracy | 0.69 | ||||||||
| SE | 0.59 | ||||||||
| SP | 0.85 | ||||||||
| PPV | 0.71 | ||||||||
| NPV | 0.73 | ||||||||
| 2020 | Udod OA et al. [23] | Ukraine | Clinical data and biomarkers | 73 patients | - | Patient data were read and normalized using the Pandas library, and one-hot encoding was applied to handle discrete categories | Custom Neural Network | Accuracy | 0.84 |
| 2021 | Bayraktar Y et al. [28] | Turkey | Bitewing X-ray | 1,000 X-rays | 2 examiners | Images cropped to 640 × 480 pixels, and data augmentation was performed through rotation, scaling, zoom, and cropping | DarkNet-53 | Accuracy | 0.95 |
| SE | 0.72 | ||||||||
| SP | 0.98 | ||||||||
| PPV | 0.87 | ||||||||
| NPV | 0.96 | ||||||||
| AUC | 0.87 | ||||||||
| 2021 | Holtkamp A et al. [20] | Germany | NILT | 226 extracted human teeth. 1319 teeth | 4 examiners | Images segmented by tooth, and data augmentation techniques such as random rotations, vertical and horizontal flipping, shifting, and zoom were applied. Images cropped to 224 × 224 pixels. | ResNet | Accuracy (in-vivo train and test) | 0.78 |
| Accuracy (in-vitro train and test) | 0.64 | ||||||||
| 2021 | Mao YC et al. [26] | Taiwan | Bitewing X-ray | 278 X-rays | 3 examiners | Gaussian filtering, Otsu thresholding, horizontal and vertical projection for tooth segmentation, zoom, rotation, translation, contrast and brightness | AlexNet | Accuracy | 0.90 |
| 2021 | Moran M et al. [40] | Brazil | Bitewing X-ray | 112 X-rays | 1 oral and maxillofacial radiologist (OMR) | Adaptive histogram equalization, Otsu thresholding, and morphological operations to improve quality of segmentation, and were cropped to obtain individual images of each tooth | ResNet, Inception | Best Accuracy (Inception) (0.001 learning rate) | 0.73 |
| 2021 | Vinayahalingam S et al. [19] | Netherlands | Panoramic X-ray | 400 X-rays | 2 examiners | Images cropped to 256 × 256 pixels around the third molar and subjected to histogram equalization and data augmentation techniques such as rotation and flipping | MobileNet V2 | Accuracy | 0.87 |
| SE | 0.86 | ||||||||
| SP | 0.88 | ||||||||
| PPV | 0.88 | ||||||||
| NPV | 0.86 | ||||||||
| F1-score | 0.86 | ||||||||
| AUC | 0.90 | ||||||||
| 2022 | Chen X et al. [39] | China | Bitewing X-ray | 978 X-rays | 2 examiners. 1 OMR | Imagens scaled to 800 pixels on shorter side, and random transformations such as flipping, central cropping, rotation, Gaussian blur, sharpening, and contrast and brightness adjustment | Faster R-CNN | Accuracy | 0.87 |
| SE | 0.72 | ||||||||
| SP | 0.93 | ||||||||
| PPV | 0.77 | ||||||||
| NPV | 0.91 | ||||||||
| F1-score | 0.74 | ||||||||
| 2022 | Estai M et al. [29] | Australia | Bitewing X-ray | 2468 X-rays | 3 examiners | Images cropped to 640 × 480 pixels to train Faster R-CNN model. The detected regions of interest (ROI) were cropped and resized to 299 × 299 pixels to train Inception-ResNet-v2 network | Faster R-CNN, VGG-16 | SE | 0.89 |
| Precision | 0.86 | ||||||||
| SP | 0.86 | ||||||||
| Accuracy | 0.87 | ||||||||
| F1-score | 0.87 | ||||||||
| 2022 | García-Cañas Á et al. [7] | Spain | Bitewing X-ray | 300 X-rays | 2 examiners | Radiographs were processed using the Denti.Ai software | Faster R-CNN, VGG-16 | Accuracy | 0.86 |
| SE | 0.87 | ||||||||
| SP | 0.99 | ||||||||
| PPV | 0.89 | ||||||||
| NPV | 0.95 | ||||||||
| AUC | 0.77 | ||||||||
| 2022 | Jones KA et al. [38] | United States | Targeted fluorescent nanoparticles (TFSNs) | 130 extracted human teeth | 1 examiner | Removal of black background pixels through cropping, resizing images to 299 × 299 pixels, fluorescence extraction | U-Net, NASNet | SE | 0.80 |
| PPV | 0.76 | ||||||||
| 2022 | Kühnisch J et al. [2] | Germany | Intraoral photograph | 2,417 photographs | 1 examiner | Cropping of the images. Exclusion of photographs with non-carious hard tissue defects and blurred images | MobileNetV2. | Accuracy caries detection (CD) | 0.93 |
| SE (CD) | 0.90 | ||||||||
| SP (CD) | 0.94 | ||||||||
| AUC (CD) | 0.96 | ||||||||
| 2022 | Park EY et al. [42] | South Korea | Intraoral photograph | 2348 photographs | 1 examiner | Images were segmented to identify dental surfaces using U-Net. Data augmentation techniques such as image mirroring, shifting, and blurring were applied | U-Net, ResNet-18, Faster R-CNN | AUC | 0.84 |
| Accuracy | 0.81 | ||||||||
| SE | 0.74 | ||||||||
| SP | 0.89 | ||||||||
| Precision | 0.87 | ||||||||
| 2022 | Zhang X et al. [41] | China | Intraoral photograph | 3,932 photogrpahs | 3 examiners | Images cropped to 300 × 300 pixels and underwent data augmentation that included shifting, cropping, scaling, rotation, and changes in image hue, saturation, and exposure | VGG-16 | AUC | 0.86 |
| image-wise SE | 0.82 | ||||||||
| box-wise SE | 0.65 | ||||||||
| 2022 | Zhou X et al. [17] | China | Panoramic X-ray | 304 X-rays | - | Individual teeth were extracted from X-rays using annotation tools, and images were resized | ResNet18 | Accuracy | 0.83 |
| Precision | 0.85 | ||||||||
| SE | 0.88 | ||||||||
| F1-score | 0.87 | ||||||||
| AUC | 0.90 | ||||||||
| 2022 | Zhu Y et al. [6] | China | Dental X-ray | 200 X-rays | - | Images adjusted to a uniform size and subjected to data augmentation techniques such as random changes in brightness, contrast, and horizontal flipping | Faster R-CNN | Precision (mean) | 0.74 |
| F1-score | 0.68 | ||||||||
| Image time detection | 0.19 s.. | ||||||||
| 2023 | Ahmed W et al. [24] | Saudi Arabia | Bitewing X-ray | 554 X-rays | 2 examiners | Images converted to JPEG format and resized to 512x512 pixels. Brightness and contrast enhancement | U-Net | IoU (mean) | 0.55 |
| F1-score (mean) | 0.54 | ||||||||
| 2023 | Baydar O et al. [25] | Poland | Bitewing X-ray | 500 X-rays | 1 examiner. 1 OMR | Identification and segmentation with CranioCatch | U-Net | SE | 0.82 |
| Accuracy | 0.95 | ||||||||
| F1-score | 0.88 | ||||||||
| 2023 | Dayı B et al. [18] | Turkey | Panoramic X-ray | 504 X-rays | 1 examiner. 1 OMR | Images cropped to 540 × 1300 pixels to focus on the teeth, and then reduced to 256 × 512 pixels for processing | DCDNet | Precision | 0.72 |
| SE | 0.70 | ||||||||
| F1-score | 0.71 | ||||||||
| 2023 | Panyarak W et al. [9] | Thailand | Bitewing X-ray | 2758 X-rays | 3 OMR | Random movements in vertical and horizontal directions, and random rotation of ±15 degrees | ResNet | Accuracy | 0.71 |
| SE | 0.83 | ||||||||
| SP | 0.57 | ||||||||
| Classification error | 0.25 | ||||||||
| 2023 | Qayyum A et al. [16]. | United Kingdom | Dental X-ray | 229 X-rays | 1 team supervised by 1 OMR | Centered cropping of caries regions in the images. Horizontal flipping, rotation | Deeplabv3 | Accuracy (mean) | 0.99 |
| IoU (mean) | 0.51 | ||||||||
| DICE score | 0.50 | ||||||||
| 2024 | Basri KN et al. [15] | Malaysia | Ultraviolet (UV) absorption spectroscopy | 102 saliva spectra | - | Centering measure (CM), auto-scaling (AS), and Savitzky-Golay (SG) smoothing | ANN, CNN | Accuracy (ANN) | 0.85 |
| Precision (ANN) | 1.0 | ||||||||
| Accuracy (CNN + smooth SG) | 1.0 | ||||||||
| Precision (CNN + smooth SG) | 1.0 | ||||||||
| 2024 | Chaves ET et al. [12] | Netherlands | Bitewing X-ray | 425 X-rays | 7 examiners | Data augmentation was used, including random horizontal flipping, resizing, and cropping | Mask R-CNN | AUC primary caries detection | 0.81 |
| AUC secondary caries detection | 0.80 | ||||||||
| F1-score primary caries detection | 0.69 | ||||||||
| F1-score secondary caries detection | 0.72 | ||||||||
| 2024 | Esmaeilyfard R et al. [11] | Iran | Cone-beam computed tomography (CBCT) | 785 CBCT | 2 OMR | Vertical and horizontal flipping, random rotations of 20°, magnification up to 2x. Cropping and splitting in three views, resizing to 96x160 pixels | Deep CNN with multiple inputs | Accuracy | 0.95 |
| SE | 0.92 | ||||||||
| SP | 0.96 | ||||||||
| F1-score | 0.93 | ||||||||
| 2024 | ForouzeshFar P et al. [27] | Iran | Bitewing X-ray | 713 X-rays | - | Images cropped into smaller images with a single tooth and resized to 100 × 100 pixels. Images were rotated and aligned to separate upper and lower teeth | VGG16, VGG19, AlexNet, ResNet50 | Accuracy | 0.94 |
| Precision | 0.93 | ||||||||
| SE | 0.95 | ||||||||
| SP | 0.97 | ||||||||
| F1-score | 0.93 | ||||||||
| 2024 | Pérez de Frutos J et al. [4] | Norway | Bitewing X-ray | 13,887 X-rays | 6 examiners | The images underwent intensity standardization in the range (0, 1), and data augmentation was applied, such as horizontal and vertical flipping with a probability of 50% | RetinaNet (ResNet50), YOLOv5, EficcientNet | Precision (mean) | 0.65 |
| F1-score | 0.55 | ||||||||
| False negative rate (FNR) (mean) | 0.15 | ||||||||
| 2024 | Yoon K et al. [37] | South Korea | Intraoral photograph | 24,578 photographs | 20 labelers. 3 examiners | Data augmentation techniques, resizing, random flipping, photometric distortion, and cut-out | Cascade Region-Based Deep CNN (R-CNN) | SE | 0.73 |
| SP | 0.97 | ||||||||
| Accuracy | 0.95 | ||||||||
| AUC | 0.94 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



