Submitted:
15 October 2025
Posted:
16 October 2025
You are already at the latest version
Abstract
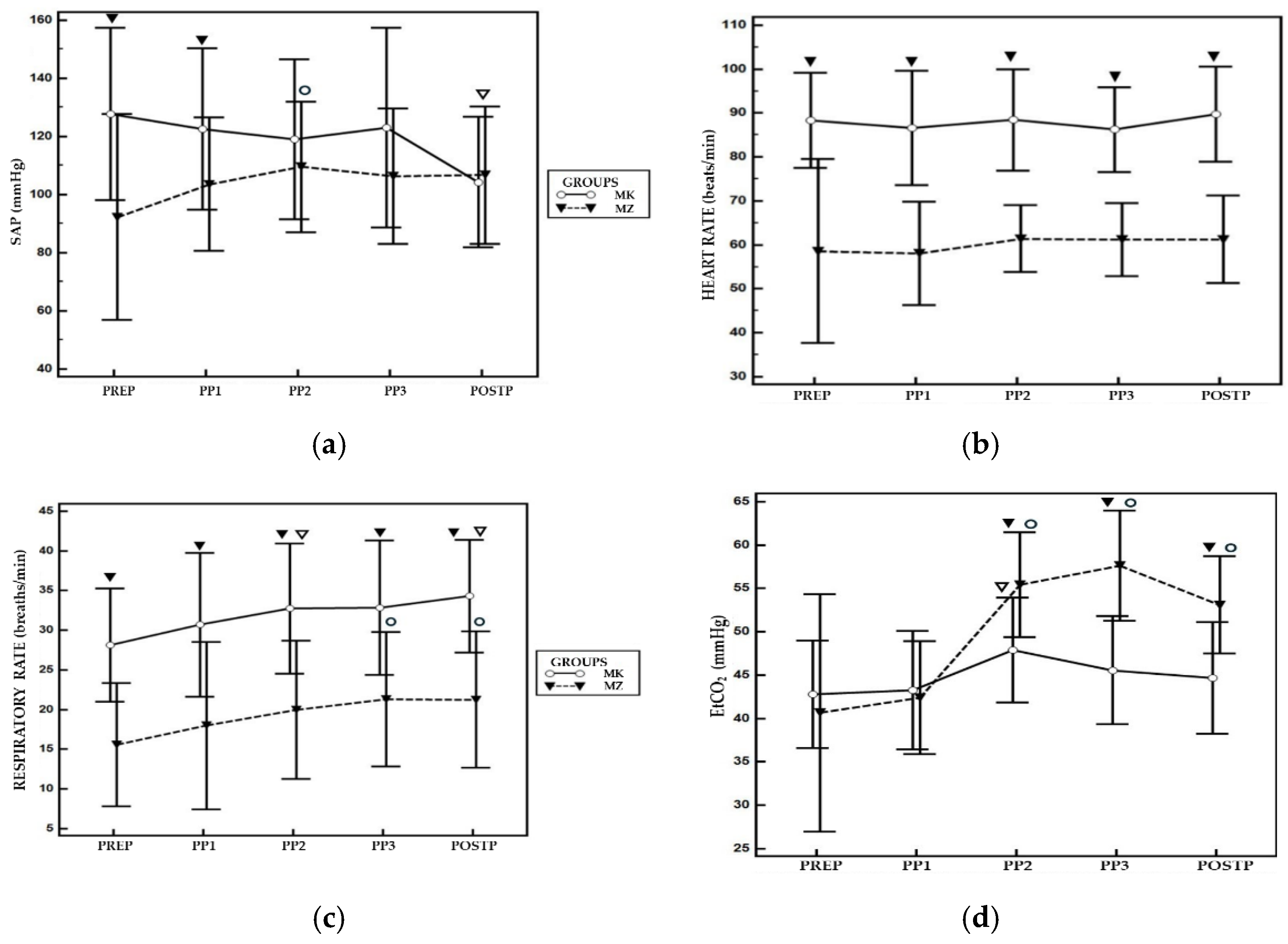
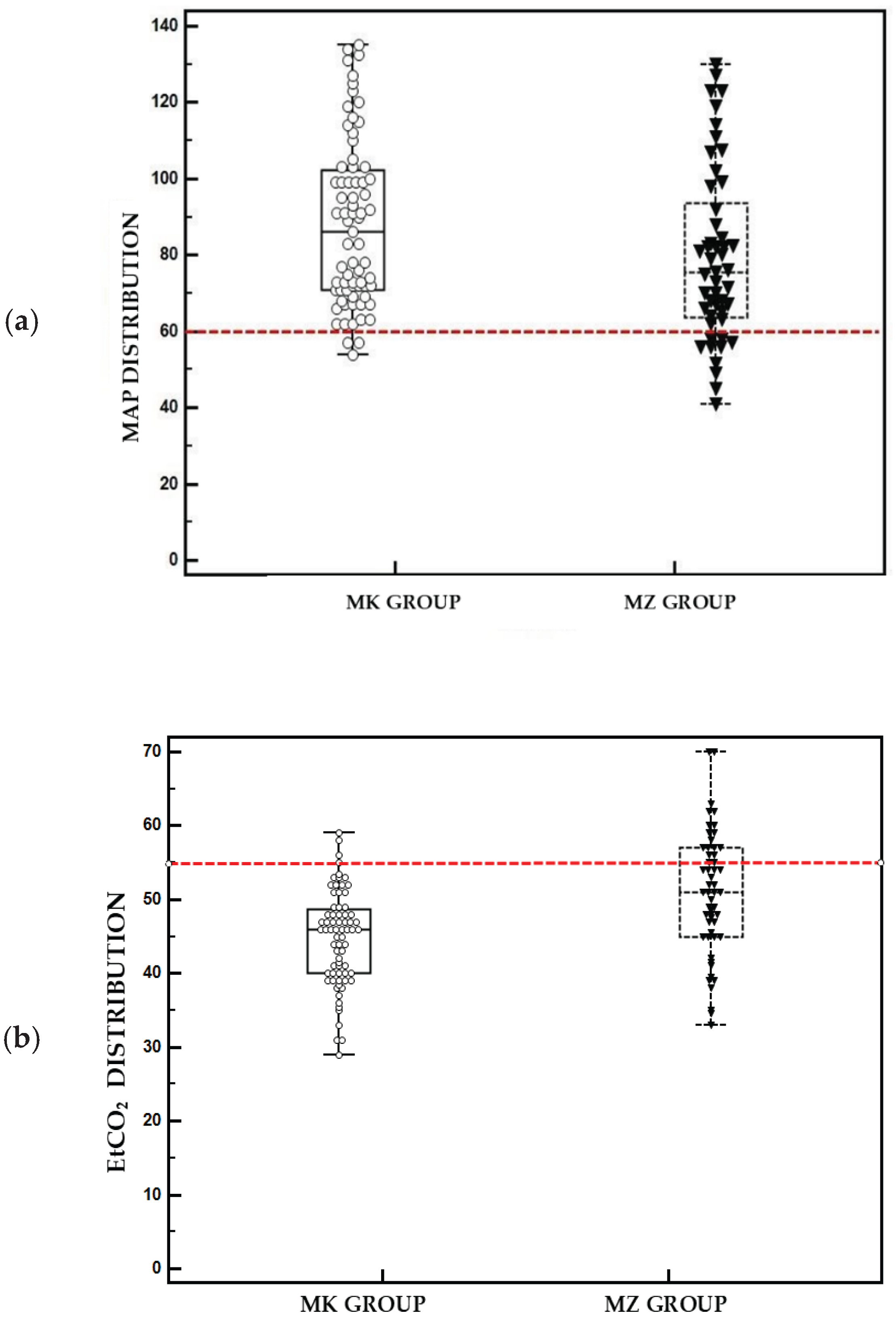
Laparoscopic salpingectomy is a mini-invasive surgery that requires careful anaesthesiologic management due to impact of pneumoperitoneum. In this retrospective study baboons (Papio Hamadryas) were treated with two sedative protocols: medetomidine-ketamine (MK; n=14) or medetomidine-tiletamine-zolazepam (MZ; n=12) via intramuscular injection. A laryngeal mask (LMA) was used for airway management and anaesthesia was maintained with isoflurane. For statistical analysis were considered and analysed via two-way ANOVA: heart rate (HR), respiratory rate (RR), systolic, diastolic and mean arterial blood pressure (SAP, DAP, MAP), end-tidal carbon dioxide (EtCO₂) and peripheral saturation (SpO₂) recorded five minutes before pneumoperitoneum (PREP), immediately after abdominal insufflation (PP1), at 10 (PP2), 20 (PP3) minutes post-insufflation and 5 minutes after pneumoperitoneum interruption (POSTP). HR and RR were statistically significantly higher (p < 0.05) in MK group compared to MZ group at all time points of the study. EtCO₂ was significantly higher (p < 0.05) in MZ group at PP2, PP3, and POSTP time points. The incidence of hypotension was significantly greater in MZ group (45.5%) compared to MK group (6.25%). Hypercapnia was observed in all baboons sedated with MZ protocol compared to 12.5% of MK group. As a result, MK protocol provides greater cardiorespiratory stability during laparoscopic surgery.
Keywords:
1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Anesthetic Management
2.3. Statistics
3. Results
4. Discussion
5. Conclusions
Funding
Author Contributions:
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ANOVA | Analysis of variance |
| CI | Interval confidence |
| CO | Cardiac output |
| CO2 | Carbon dioxide |
| DAP | Diastolic arterial pressure |
| EAZA | European Association Zoos and Acquaria |
| EtCO2 | End-tidal carbon dioxide |
| HR | Heart rate |
| IV | Intravenous |
| LMA | Laryngeal Mask airway |
| MAP | Mean arterial pressure |
| MK | Medetomidine-ketamine group |
| MZ | Medetomidine-tiletamine-zolazepam group |
| NHPs | Non-human primates |
| PaCO2 | Partial pressure of arterial carbon dioxide |
| POSTP | 5 minutes after pneumoperitoneum interruption |
| PP1 | Immediately after starting pneumoperitoneum |
| PP2 | Pneumoperitoneum 10 minutes |
| PP3 | Pneumoperitoneum 20 minutes |
| PREP | Pre-pneumoperitoneum |
| RR | Respiratory rate |
| SAP | Systolic arterial pressure |
| SpO2 | Peripheral oxygen saturation |
References
- Zinner, D. & Schwibbe, Michael & Kaumanns, Werner. (1994). Cycle synchrony and probability of conception in female hamadryas baboons Papio hamadryas. Behavioral Ecology and Sociobiology - BEHAV ECOL SOCIOBIOL. 35. 175-183. [CrossRef]
- AZA Baboon Species Survival Plan®. Hamadryas Baboon Care Manual; Association of Zoos and Aquariums: Silver Spring, MD, USA, 2020.
- Nitsch, F., Stueckle, S., Stahl, D. & Zinner, D. Copulation patterns in captive hamadryas baboons: a quantitative analysis. Primates 52, 373 (2011). [CrossRef]
- Taberer, T. R., Mead, J., Hartley, M. & Harvey, N. D. Impact of female contraception for population management on behavior and social interactions in a captive troop of Guinea baboons (Papio papio). Zoo Biology 42, 254–267 (2023). [CrossRef]
- Yu, P., Weng, C., Kuo, H. & Chi, C. Evaluation of endoscopic salpingectomy for sterilization of female Formosan macaques (Macaca cyclopis). American J Primatol 77, 359–367 (2015). [CrossRef]
- Reiners JK, Gregersen HA. How to plan and provide general anesthesia for a troop of 98 hamadryas baboons (Papio hamadryas) for contraceptive and preventative health interventions. Am J Vet Res. 2024 May 18;85(7): ajvr.23.12.0274. PMID: 38744308. [CrossRef]
- Lacitignola L, Laricchiuta P, Imperante A, Acquafredda C, Stabile M, Staffieri F. Laparoscopic salpingectomy in Papio hamadryas for birth control in captivity. Vet Surg. 2022 Jul;51 Suppl 1:O98-O106. Epub 2022 Jan 5. PMID: 34985139. [CrossRef]
- Di Bella C, Lacitignola L, Fracassi L, Skouropoulou D, Crovace A, Staffieri F. Pulse Pressure Variation Can Predict the Hemodynamic Response to Pneumoperitoneum in Dogs: A Retrospective Study. Vet Sci. 2019 Feb 20;6(1):17. PMID: 30791578; PMCID: PMC6466147. [CrossRef]
- Odeberg-Wernerman S. Laparoscopic surgery-effects on circulatory and respiratory physiology: an overview. Eur J Surg Suppl. 2000;(585):4-11. PMID: 10885548. [CrossRef]
- Di Bella, C. et al. Effects of two alveolar recruitment maneuvers in an “open-lung” approach during laparoscopy in dogs. Front. Vet. Sci. 9, 904673 (2022).
- Jo, Y. Y. & Kwak, H.-J. What is the proper ventilation strategy during laparoscopic surgery? Korean J Anesthesiol 70, 596 (2017). [CrossRef]
- Atkinson, T. M., Giraud, G. D., Togioka, B. M., Jones, D. B. & Cigarroa, J. E. Cardiovascular and Ventilatory Consequences of Laparoscopic Surgery. Circulation 135, 700–710 (2017). [CrossRef]
- Annalaura Scardia et al. Use of Laryngeal Mask and Anesthetic Management in Hamadryas Baboons (Papio hamadryas) Undergoing Laparoscopic Salpingectomy—A Case Series. Veterinary Sciences 10, 158 (2023). [CrossRef]
- Johann, A. & Brüning, N. EAZA Best Practice Guidelines Gelada Baboon (Theropithecus Gelada). (European Association of Zoos and Aquaria, NL, 2021).
- Monkeys and Gibbons. in Zoo Animal and Wildlife Immobilization and Anesthesia pp. 561–571 (Wiley, 2014). [CrossRef]
- Santerre D, Chen RH, Kadner A, Lee-Parritz D, Adams DH. Anaesthetic management of baboons undergoing heterotopic porcine cardiac xenotransplantation. Vet Res Commun. 2001 May;25(4):251-9. PMID: 11432427. [CrossRef]
- Yeung, K. R. et al. Comparison of indirect and direct blood pressure measurements in baboons during ketamine anaesthesia. J of Medical Primatology 43, 217–224 (2014). [CrossRef]
- Lin, H. C., Thurmon, J. C., Benson, G. J. & Tranquilli, W. J. Review: Telazol – a review of its pharmacology and use in veterinary medicine. Vet Pharm & Therapeutics 16, 383–418 (1993). [CrossRef]
- Wilson, R. P., Zagon, I. S., Larach, D. R. & Max Lang, C. Cardiovascular and respiratory effects of tiletamine-zolazepam. Pharmacology Biochemistry and Behavior 44, 1–8 (1993). [CrossRef]
- Gomes, V. H. et al. Anesthetic effects of isoflurane and fentanyl infusion in capuchin monkeys (Sapajus sp) undergoing salpingectomy or deferentectomy, previously chemically restrained with ketamine–midazolam or ketamine–dexmedetomidine. J of Medical Primatology 52, 149–155 (2023). [CrossRef]
- Lee, V. K., Flynt, K. S., Haag, L. M. & Taylor, D. K. Comparison of the Effects of Ketamine, Ketamine–Medetomidine, and Ketamine– Midazolam on Physiologic Parameters and Anesthesia-Induced Stress in Rhesus (Macaca mulatta) and Cynomolgus (Macaca fascicularis) Macaques. Journal of the American Association for Laboratory Animal Science 49, (2010).
- Pulley, A. C. S., Roberts, J. A. & Lerche, N. W. FOUR PREANESTHETIC ORAL SEDATION PROTOCOLS FOR RHESUS MACAQUES (MACACA MULATTA). Journal of Zoo and Wildlife Medicine 35, 497–502 (2004). [CrossRef]
- Jalanka, Harry H., and Bengt O. Roeken. “The Use of Medetomidine, Medetomidine-Ketamine Combinations, and Atipamezole in Nondomestic Mammals: A Review.” Journal of Zoo and Wildlife Medicine, vol. 21, no. 3, 1990, pp. 259–82. JSTOR. https://www.jstor.org/stable/20095064.
- Watuwa, J., Mbabazi, R., Sente, C., Musinguzi, J. & Laubscher, L. A retrospective study on the immobilisation of captive chimpanzees (Pan troglodytes) at UWEC, Uganda. Vet Record Case Reports 11, e602 (2023). [CrossRef]
- Vié, J.-C. et al. Anesthesia of wild red howler monkeys (Alouatta seniculus) with medetomidine/ketamine and reversal by atipamezole. Am. J. Primatol. 45, 399–410 (1998).
- Langoi, D.L., P.G. Mwethera, K.S.P. Abelson, I.O. Farah, and H.E. Carlsson. "Reversal of Ketamine/Xylazine combination anesthesia by Atipamezole in olive baboons (Papio anubis)." Journal of Medical Primatology 38.6 (2009). [CrossRef]
- Amari, M. et al. Comparison of Three Different Balanced Sedative-Anaesthetic Protocols in Captive Baboons (Papio hamadryas). Veterinary Sciences 12, 859 (2025). [CrossRef]
- Lee JI, Hong SH, Lee SJ, Kim YS, Kim MC. Immobilization with ketamine HCl and tiletamine-zolazepam in cynomolgus monkeys. J Vet Sci. 2003 Aug;4(2):187-91. PMID: 14610374. [CrossRef]
- Atencia R, Stöhr EJ, Drane AL, Stembridge M, Howatson G, Del Rio PRL, Feltrer Y, Tafon B, Redrobe S, Peck B, Eng J, Unwin S, Sanchez CR, Shave RE. HEART RATE AND INDIRECT BLOOD PRESSURE RESPONSES TO FOUR DIFFERENT FIELD ANESTHETIC PROTOCOLS IN WILD-BORN CAPTIVE CHIMPANZEES (PAN TROGLODYTES). J Zoo Wildl Med. 2017 Sep;48(3):636-644. PMID: 28920777. [CrossRef]
- Tusman G, Bohm SH, Suarez-Sipmann F. Advanced Uses of Pulse Oximetry for Monitoring Mechanically Ventilated Patients. Anesth Analg. 2017 Jan;124(1):62-71. PMID: 27183375. [CrossRef]
- Piemontese C, Stabile M, Di Bella C, Scardia A, Vicenti C, Acquafredda C, Crovace A, Lacitignola L, Staffieri F. The incidence of hypoxemia in dogs recovering from general anesthesia detected with pulse-oximetry and related risk factors. Vet J. 2024 Jun;305:106135. [CrossRef]
- Bucknell P, Dobbs P, Martin M, Ashfield S, White K. Cardiorespiratory effects of isoflurane and medetomidine-tiletamine-zolazepam in 12 bonobos (Pan paniscus). Vet Rec. 2023 Feb;192(4):e2589. Epub 2023 Jan 24. PMID: 36692993. [CrossRef]
- Brown LJ, Jamieson SE. Field Evaluation of Tiletamine-Zolazepam-Medetomidine for Immobilization of Raccoons (Procyon lotor) and Striped Skunks (Mephitis mephitis). J Wildl Dis. 2022 Oct 1;58(4):914-918. PMID: 35951023. [CrossRef]
- Gerak, L. R., Brandt, M. R. & France, C. P. Studies on benzodiazepines and opioids administered alone and in combination in rhesus monkeys: ventilation and drug discrimination. Psychopharmacology 137, 164–174 (1998). [CrossRef]
- Parada, E., Schwartz, H., Lam, A. Y., Baca-Montero, O. & Laubscher, L. Utilisation of dexmedetomidine, ketamine and midazolam for immobilisation and health assessment of captive white-bellied spider monkeys (Ateles belzebuth) in the Amazon rainforest of Iquitos, Peru. Vet Record Case Reports 12, (2024). [CrossRef]
- Johnson, J. A., Atkins, A. L. & Heard, D. J. Application of the Laryngeal Mask Airway for Anesthesia in Three Chimpanzees and One Gibbon. Journal of Zoo and Wildlife Medicine 41, 535–537 (2010). [CrossRef]
- Cerveny, S. N., D’Agostino, J. J., Davis, M. R. & Payton, M. E. COMPARISON OF LARYNGEAL MASK AIRWAY USE WITH ENDOTRACHEAL INTUBATION DURING ANESTHESIA OF WESTERN LOWLAND GORILLAS (GORILLA GORILLA GORILLA). Journal of Zoo and Wildlife Medicine 43, 759–767 (2012). [CrossRef]
- Klonner, M. E., Springer, S. & Braun, C. Complications secondary to endotracheal intubation in dogs and cats: A questionnaire-based survey among veterinary anaesthesiologists. Veterinary Anaesthesia and Analgesia 50, 220–229 (2023). [CrossRef]
- Ip, J. Y. C. & Lo, K.-M. Perioperative management of patients with aspiration risk. Anaesthesia & Intensive Care Medicine 25, 550–554 (2024). [CrossRef]

| Parameters | Group | PREP | PP1 | PP2 | PP3 | POSTP |
|
HR (beats/min) |
MZ | 59 (45-72) | 58 (50-66) | 61 (56-67) | 61 (56-67) | 51 (55-68) |
| MK | 88 (83-94) ▼ | 87 (80-94) ▼ | 88 (82-95) ▼ | 86 (77-95) ▼ | 90 (84-95) ▼ | |
|
MAP (mmHg) |
MZ | 74 (52-96) | 73 (59-88) | 85 (64-105) | 77 (57-96) | 82 (65-99) |
| MK | 93 (82-105) | 92 (81-104) | 88 (77-100) | 89 (66-113) | 78 (68-89) | |
|
DAP (mmHg) |
MZ | 62 (40-83) | 61 (45-78) | 66 (44-88) | 63 (44-81) | 66 (49-83) |
| MK | 77 (66-88) | 78 (67-88) | 75 (64-85) | 73 (53-93) | 65 (55-76) | |
|
SAP (mmHg) |
MZ | 92 (67-118) | 104 (88-119) | 110 (92-127) | 106 (89-124) | 107 (91-123) |
| MK | 128 (109-141)▼ | 123 (108-137)▼ | 119 (104-134) | 123 (91-155) | 104 (92-116) | |
| EtCO2 (mmHg) | MZ | 41 (32-49) | 42 (38-47) | 55 (51-60) | 58 (53-62) | 53 (49-57) |
| MK | 43 (40-46) | 43 (40-47) | 48 (45-51) ∇ | 46 (40-51) | 45 (41-48) ∇ | |
| RR (breaths/min) | MZ | 16 (11-21) ▼ | 18 (11-26) ▼ | 20 (14-26) ▼ | 21 (15-27) ▼○ | 21 (16-27) ▼○ |
| MK | 28 (24-32) | 31 (26-36) | 33 (28-37) | 33 (25-41) | 34 (31-38) | |
| SpO2 | MZ | 97 (95-98) | 97 (96-99) | 98 (97-99) | 98 (96-99) | 98 (98-99) |
| MK | 98 (98-99) | 98 (97-99) | 97 (96-98) | 97 (94-99) | 97 (95-98) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



