
Submitted:
13 October 2025
Posted:
14 October 2025
You are already at the latest version
Abstract
Background Childhood obesity has become a pressing global health challenge. To mitigate its impact and inform effective public health policies, analyzing the efficacy of interventions is crucial. This study aimed to conduct a systematic review of interventions (SRI) targeting school-aged children with obesity. Our goal was to identify the key components that contribute to the success of integrated interventions addressing diet/nutrition (D/N), physical activity (PA), and/or socioemotional skills. Methods: The Cochrane Collaboration methodology and PRISMA statement were followed. The SRI included the following criteria established a priori: studies that addressed obesity in school-aged children, including one or more interventions related to physical activity (PA), diet/nutrition (D/N), or socioemotional skills. Following the PICO (Population, Intervention, Comparison, and Outcome) framework, we searched six digital databases using relevant keywords and MeSH terms. The Mixed Methods Appraisal Tool (MMAT) was used to assess article quality via "function group string" methods. Finally, a thematic synthesis of SRI findings was conducted. The protocol for this study was registered in PROSPERO: CRD4202454214. Results: Initial screening yielded 127 articles. Following critical appraisal with the MMAT, studies with inadequate methodology, solely descriptive designs, unclear results, or interventions shorter than six months were excluded. Ultimately, 10 studies remained, eight of which included two of the three components of interest (D/N or PA). Conclusions: In this overview plenty of interventions were presented for the prevention of overweight and obesity in school-age children: However, methodological and standardized limitations still exist that hinder the establishment of an effective intervention. Engaging families and teachers as active participants in interventions significantly amplified the effectiveness in both the D/N and PA domains. However, an analysis of current interventions highlights a stark gap in multi-sectoral and integrated approaches to tackling childhood obesity. This presents a remarkable opportunity for future initiatives to move beyond fragmented efforts and embrace a holistic model that unites families, schools, and communities to champion healthy lifestyles.
Keywords:
childhood obesity
; school age children
; intervention study
; systematic review
; weight reduction
1. Introduction
Overweight and obesity (OW + Ob) are chronic multifactorial conditions with genetic, environmental, and lifestyle determinants that pose significant health risks including type 2 diabetes, hypertension, dyslipidemia, and cardiovascular diseases [1,2]. The main factors related to OW+ Ob include physical inactivity and consumption of energy-dense foods [3], which present modifiable opportunities for prevention and treatment [4].
The prevalence of obesity in school-aged children has increased, mirroring the global trend, with the World Obesity Federation projecting a substantial increase by 203 [5,6]. This surge is associated with nutritional transition [7,8], marked by the availability of low-cost processed foods, increased fast food consumption, reduced home food preparation time, and heightened exposure to sedentary-inducing products [9,10]. In Latin America, particularly Mexico, Argentina, and Chile, 30% of those aged 5–19 years are affected [11].
Body image and parental perceptions significantly influence children’s access to care [12,13]. Early habits often persist in adulthood, underscoring the need to modify obesogenic environments for children's long-term health [10,13]. Understanding the causal factors is crucial to address the high prevalence of obesity in school-aged children. Education promoting healthy habits, early weight gain detection, and targeted interventions is essential [14].
Public health interventions for childhood obesity vary, with single or multicomponent approaches targeting areas such as education, physical activity, and nutrition policy [9]. Previous reviews have focused on specific settings, such as homes or schools [15,16], yielding mixed findings. Recent systematic reviews have highlighted challenges in evidence quality, intervention group comparisons, and study design clarity [15,16,17].
Additionally, recent meta-analyses have highlighted that while school-based interventions show small but significant benefits on BMI in children aged 5–11 years, these benefits may not be equally distributed across gender and social groups. Evidence suggests interventions tend to be more effective in boys, and there is limited information on whether they reduce health inequities as measured by the PROGRESS framework [18]
A specific review in Mexico underscores the effectiveness of multicomponent interventions combining physical activity, nutrition, and behavioral change to prevent and reduce childhood obesity. The authors emphasize methodological shortcomings, urging the scientific community to develop robust preventive and curative solutions [17].
This systematic review aimed to summarize essential elements in designing interventions for obesity in school-aged children, offering a critical evaluation to address knowledge gaps, despite a high volume of available studies. By informing future researchers, this review aims to guide the development of effective personalized programs for the Mexican school population.
2. Materials and Methods
This systematic review of interventions (SRI) adhered to the methodology proposed by the Cochrane Collaboration [18], and PRISMA statement were followed, with collaboration from trained personnel across five institutions. A team of two authors meticulously examined the compiled studies, assessing risk and quality while standardizing the criteria and fields of interest. Each author independently conducted a blind review of the scientific evidence and assessment measures.
The outcomes of this review serve as the cornerstone for the development of the Community Intervention of Integral Action for Children in Nutritious and Healthy Environments (INCAI in Spanish). The protocol for this review was approved by the Ethics, Biosafety, and Research Committees of the National Institute under Protocol CI:1791 1791 and was registered in PROSPERO: CRD4202454214.
Serch Strategy and Terms
A comprehensive search strategy spanned six digital databases (ScienceDirect, DOAJ, Scielo, EbscoHost, Redalyc, and PubMed), using the PICO framework [19]. Collaborating with authors from five academic institutions provides diverse perspectives. Derived from Rivera Dommarco et al.'s book chapter [20], the search criteria covered themes such as obesity, school-aged population, program design, implementation, and evaluation. Key terms were adapted to the MeSH definitions, accounting for synonyms and MeSH Tree Structures [19].
Search chains utilizing key terms with a PICO structure and Boolean operators were constructed. The inclusion criteria focused on community interventions aimed at enhancing health in local communities, guided by Trickett et al.'s definition [22]. The PICOS framework [23] directs criteria, emphasizing the impact of community interventions on overweight and obesity prevalence in school-aged children.
The reviewers independently evaluated abstracts and titles, prioritizing original articles, controlled cohort studies, and longitudinal studies in Latin America up to December 2023. Outcome measures included reduction in overweight or obesity prevalence, BMI z-score reduction, improved dietary habits, formation of healthy habits, and increased physical activity. This meticulous approach has ensured a comprehensive and diverse exploration of interventions for childhood obesity in the school context.
Data Extraction
Predefined data extraction forms were completed to record study characteristics. Each author was responsible for completing the forms, and the two authors/researchers reviewed and compared the extracts containing the following information:
I) General information: database; search string; PICO elements; Digital Object Identifier (DOI); author; year of publication; title; country; study design and type; language; identification of control or intervention group; total sample size; population evaluated.
II) Intervention details: diagnostic criteria for overweight or obesity, type of intervention (nutritional, physical activity, educational, mixed), study summary, duration of intervention (in months), intervention site, population included in the intervention, and intervention staff.
III) Outcomes: Changes related to the program, such as reduction of obesity components, changes in lifestyle, changes in diet, and changes in physical activity.
III) Results: Program-related changes, such as a reduction in obesity components, lifestyle changes, dietary changes, and physical activity changes.
Strategy for selection and Assessment
After compiling and standardizing the articles using extraction forms, a thorough assessment was conducted using SPSS with group string functions and simple descriptive analyses in the exploratory review.
Dictionaries were created to standardize variable definitions, covering journal names, DOI, country, intervention duration, and evaluated population. A code was devised to associate each country with its region using an international classification system. Mexico was classified separately because of its significant relevance, and other classifications included North America, Latin America, the Caribbean, Asia Pacific, Europe, the Middle East, North Africa, and Southern Africa [24].
For critical assessment, the Mixed Methods Appraisal Tool (MMAT) version 18 was employed [25], utilizing a two-phase scoring system involving base filtration and specific filtration based on the study methodology. The criteria included screening/diagnostic methods and quantitative methods (controlled and non-randomized) [26].
Studies that met the inclusion criteria and passed methodological assessments were independently reviewed by two authors. Key participant and intervention characteristics were summarized using standard templates, and narrative synthesis was employed to report data on favorable or unfavorable outcomes. This meticulous approach ensured a comprehensive and robust evaluation of selected studies on childhood obesity interventions in the school context.
3. Results
3.1. Description of Selected Studies
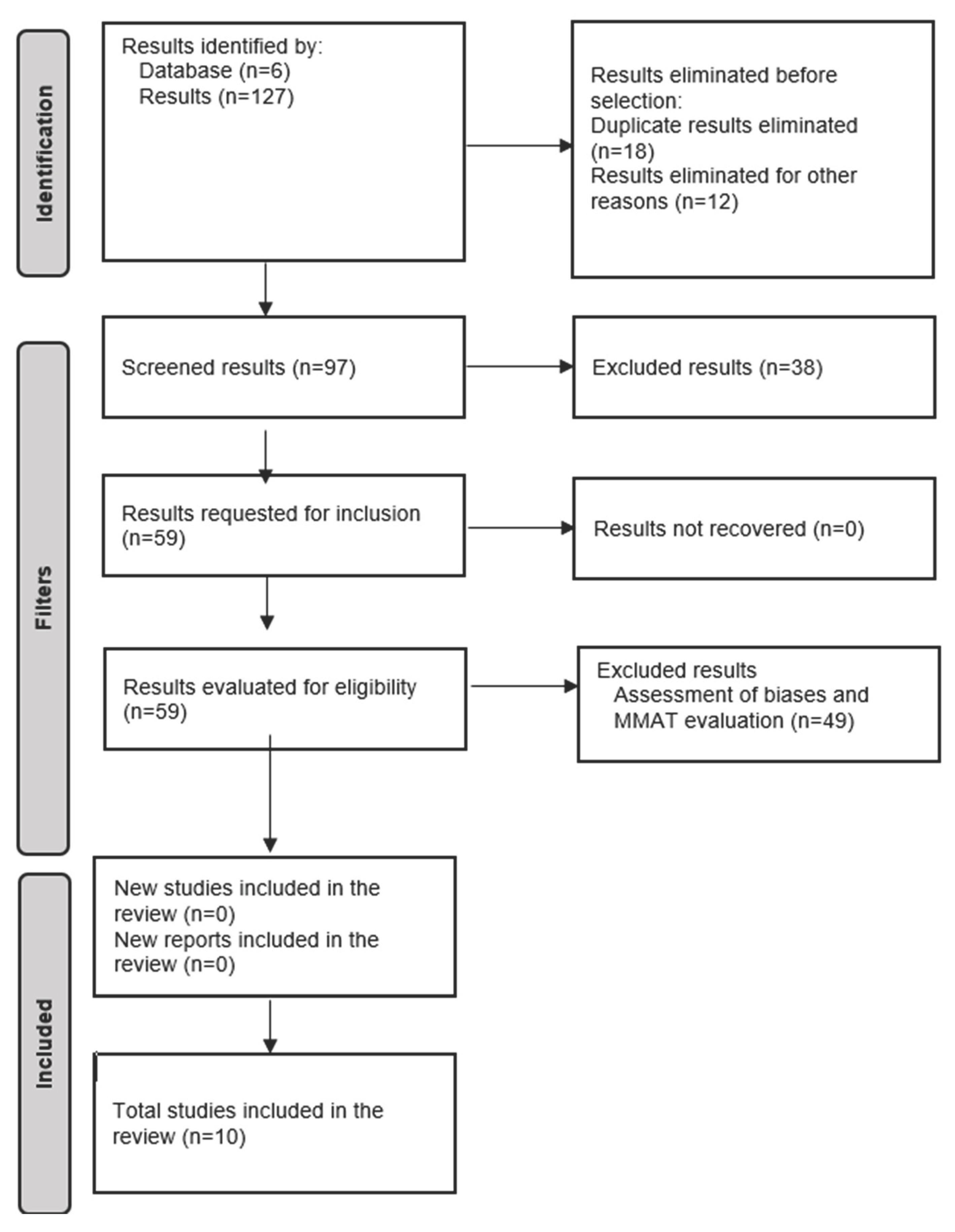
A total of 127 articles were initially collected, and after excluding 30 duplicates and articles without DOI, 97 articles remained (figure 1) [27]. The first exploration eliminated studies with a transversal or descriptive design and those describing the study protocols, resulting in a final set of 59 articles for further analysis. Articles published in English or Spanish within the past 11 years constituted the final selection for the systematic review.
Variables, such as intervention type, geographic location, language, and publication year, were examined. Most studies were conducted in North America, Europe, Latin America, the Caribbean, Asia Pacific, and Mexico. The selected studies described interventions with a median population of 2,124 participants and a median duration of 17.8 months.
After cleaning the database, additional filters were applied to identify the characteristics of interest. Critical evaluation using the MMAT led to the exclusion of studies that did not meet the methodological criteria or lacked relevant results. Articles were further discarded if they had unclear outcome measure descriptions, lacked critical methodological aspects, or described interventions of less than six months. The final selection of the analysis included 10 studies.
This review focused on articles that specifically addressed obesity in school-aged populations, including one or more interventions (physical activity, diet/nutrition, and socioemotional skills), which were conducted in the school environment, and included community-based components.
The primary measures in the 10 selected studies included reduction in the prevalence of overweight and obesity, reduction in z-score of BMI for age, improvement of dietary habits, promotion of healthy habits, and increase in physical activity. Eight studies were multicomponent, addressing both diet/nutrition and physical activity, while two focused solely on diet/nutrition without utilizing a control group. Three studies considered socioeconomic status (SES) and belonged to indigenous or minority groups. The median study duration was 22 months, ranging from eight–43 months). Four studies specifically considered SES, whereas two did not mention any of the specified characteristics.
Anthropometric measures, particularly height and weight for estimating BMI and nutritional status, were used in all 10 studies, with half utilizing reference values from the World Health Organization. Six studies included additional risk components such as waist circumference, and only one reported the measurement of biochemical markers to detect metabolic syndrome (Table 1).
Due to the specific inclusion criteria prioritizing studies in Mexico and Latin America and the focus on multi-component interventions, the limited number of studies obtained prevented the establishment of a meta-analysis. The heterogeneous results, combined with a lack of methodological rigor in some studies, may compromise the interpretation or lead to unreliable and inconsistent statistical synthesis.
3.2. Figures and Tables
Figure 1.
PRISMA Flowchart
3.3 Diet and Nutrition
The identified interventions predominantly utilized educational lessons, workshops, and sports clubs, focusing on diet/nutrition (D/N). Nine out of ten interventions were implemented within schools, with four including a consistent nutritionist presence. Health sector personnel included physicians, nurses, nutrition educators, and health professionals.
Parental involvement was a significant feature of the eight interventions with D/N components, and only two were extended to the broader community. The effects included an increased demand for healthier foods in school cafeterias, improved food availability, changes in unhealthy food consumption, increased vegetable consumption, and reduced consumption of high-fat snacks. Tarro [28], Bacardi [29], and Waters [30] focused on healthy food selection education, increased fruit and vegetable consumption, and decreased sugary and fatty snack consumption. Others, such as Safdie [31] and Long [32], have enhanced the school food environment by increasing healthy food availability, reducing high-calorie density foods and sugary beverages, and incorporating nutrition education.
Some studies, such as the Kids Nutrition and Fitness (KNF) program [33], provided extracurricular nutrition education, while Vazquez [34] and Scruzzi [35] focused on nutrition education through workshops, evaluating the impact on consumption before, during, and after intervention. Parental involvement and school environment modifications have emerged as promising aspects for success in reducing childhood obesity.
Flynn's study [36] underscored the significance of home interventions and family involvement in preventing obesity in children under five. Active engagement of adults, especially parents and teachers, is crucial for favorable outcomes such as weight reduction and obesity prevention. However, Morgan et al. [37] suggested the need for additional evidence, emphasizing the importance of primary studies detailing intervention designs and outcome measures to establish the value of caregiver involvement.
3.4. Physical Activity
In interventions incorporating physical activity components, physical education teachers played a central role in five of eight cases, with classroom teachers providing support. Only two interventions involved a leading health professional. Four interventions demonstrated positive effects on physical activity levels among school-aged children, emphasizing strength-building activities, additional physical education sessions, and improvements in sports and playground equipment.
All studies focused on interventions during regular school hours, with only one extending the activity to the home. Five studies involved parents, and two showed significant changes, increasing physical activity hours and reducing sedentary time, compared to the control groups.
All studies focused on interventions during regular school hours, with only one extending the activity to the home. Five studies involved parents, and two showed significant changes, increasing physical activity hours and reducing sedentary time, compared to the control groups.
In a review by Liu et al. [38], BMI variations were noted with physical activity; however, no significant differences were found between interventions with multiple components and those focusing on a single component. Ameryoun et al. [39] found that game-based interventions had a consistent but small effect on reducing BMI Z-scores, especially when combined with nutrition and education.
Bleich et al.'s review [40] highlighted that prioritizing physical activity sometimes reduced interventions in education and dietary components. Synthesizing evidence emphasizes the importance of various activities in obesity reduction programs. School-based interventions, particularly strength sports and active games, offer promising opportunities for study. Improving evidence in these areas can help identify effective strategies for reducing excess weight in early childhood.
3.5. Overweight and Obesity
Several studies, including those by Sadeghi [41], Bacardi [29], Tarro [28], and Vazquez [34], demonstrated significant reductions in obesity measures among school-aged children in their interventions compared to control groups. Safdie's [31] basic intervention showed the greatest reduction in the prevalence of overweight or obesity, dropping from 12.1% to 10.9%. Bacardi-Gascon noted a primary change in abdominal obesity percentage, decreasing from 20.6% to 15.2% [29].
However, Waters [30] and Centeio [42] reported decreased overweight and obesity proportions in both the intervention and control groups, complicating the attribution of results solely to interventions. Brown et al. [43] review suggested that combined physical activity and diet interventions in preschoolers reduce obesity risk and BMI-for-age Z-score. In 6–12-year-olds, physical activity interventions reduced BMI, Z-score, and overweight/obesity prevalence, but the difference was not statistically significant. Dietary interventions in this age group lacked conclusive evidence, whereas combined interventions reduced the BMI Z-score for age.
Cauchi et al. [44] reported small-to-modest impacts on anthropometric outcomes and childhood obesity reduction in most interventions, with no clear link between intervention components and effectiveness. A notable limitation of this review and others is the lack of methodological clarity, especially in statistical power calculations, hindering the precise interpretation of observed variations. Clearer reporting of methodological criteria is essential for a more accurate understanding of effective approaches to address childhood obesity.
3.6. Socioemotional Skills
Few studies have emphasized socioemotional skills and behavioral changes as success factors in treating childhood overweight and obesity. Giannin et al. [45] found that caregivers enrolled children for physical and mental health improvement, especially when medical issues, such as high blood pressure and probable diabetes, were identified. The caregivers acknowledged that small changes at home led to weight loss and habit changes, acting as a catalyst for further positive changes.
Waters et al. [30] and Vásquez et al. [34] integrated psychological aspects into their interventions. Waters included self-esteem promotion, whereas Vasquez included sessions with a psychologist to support behavioral changes related to diet and physical activity. These findings highlight the significance of addressing not only physical health, but also socioemotional well-being and behavioral modifications in effective childhood obesity interventions.
4. Discussion
Our analysis underscores the crucial role of intervention time in addressing childhood obesity and emphasizes its impact on program design and implementation. Among the studies analyzed, nine interventions occurred within the school environment during regular hours, with five extending hours and two involving community components.
Dividing treatments for overweight and obesity, as seen in other reviews, helps reduce result heterogeneity and prioritizes recommendations based on their effectiveness. The review by Long et al. highlights that a long intervention time does not guarantee effective adherence or reduction in obesity, suggesting the need for modifications when transitioning from short-to long-term interventions.
Effective interventions lasting between eight and nine months have proven successful in addressing childhood obesity. Strategies combining proper nutrition, promotion of fruit and vegetable consumption, water intake, and physical activity in schools over 4 to 12 months showed positive effects on maintaining or slightly improving BMI. However, the standardization of design and implementation remains a common need across studies.
Our findings align with global evidence that the effectiveness of obesity prevention interventions may differ across subgroups. As Palmer et al. [17] in 2025 showed in a re-analysis of 81 trials, interventions had greater impact on boys aged 5–11 and did not significantly affect inequities across other PROGRESS domains. These insights support the need for equity-sensitive design in future interventions, especially in Latin American contexts where social and economic disparities are profound.
In Mexico, the "Nutrition on the Go" strategy, which focuses on reducing the energy content of school breakfasts, including fruits and vegetables, and promoting physical activity and water consumption over six months, had a statistically significant effect on reducing the probability of shifting from overweight to obesity categories. This study also documented a decreasing effect of the shift from the normal to overweight categories during the intervention [45].
Long et al.'s study, emphasizing that a longer intervention (36 months) did not guarantee effective results, recognized the limited impact on BMI, potentially due to the extension of a short-term intervention without necessary modifications. In summary, intervention length is a critical factor and careful consideration, and adaptation are essential for effective and sustained outcomes in childhood obesity programs.
Interventions involving family and teachers had greater effects on both diet and physical activity, contributing to positive outcomes. This underscores the importance of collaborative programs that involve multiple stakeholders.
Addressing the Latino and/or Mexican population in the United States is increasingly crucial due to their heightened vulnerability to obesity, which is often tied to their social and economic environments.
Various techniques and theories, such as socio-ecological theory, theory of social education, and ecological methods for healthy habit formation, have been identified in interventions. This was particularly prevalent in programs aimed at instilling habits through education.
The focus on the school-aged population, specifically targeting ages eight to nine, highlights the segmentation of physical and learning activities. In the Mexican context, this corresponds to first-to third-year students in the first group and fourth-to sixth-year students in the second. However, the inclusion of different grades and ages in the assessed studies may limit the generalizability of their findings. Overall, these insights emphasize the importance of tailored approaches, collaboration, and cultural considerations when addressing childhood obesity.
Our study had some limitations, such as the potential lack of studies in certain regions or variability in methods for measuring intervention impacts, and the potential impact of the absence of controlled and randomized studies on the robustness of conclusions. Concerning the evidence, two studies did not include a comparison with a control group. However, these studies were included because of the type of information provided. Regarding the review processes, we consider that some effects could have been estimated using statistics and odds ratios. Nevertheless, this review focused on narrative analysis to identify design strengths for future strategies to be implemented in the design of an intervention program.
5. Conclusions
In this overview plenty of interventions were presented for the prevention of overweight and obesity in school-age children. Interventions aimed at preventing, controlling, or reducing obesity generally lack a multisectoral approach and integrated components. Providing dietary and nutritional education to the entire population is crucial for reducing the prevalence of non-communicable diseases by promoting healthy habits and behaviors.
Implementation of interventions requires collaboration between the health and education sectors, considering the influence of the social determinants of health. Recognizing and addressing obesogenic environments is particularly important. These considerations emphasize the need for methodological rigor, multi-sectoral approaches, and a comprehensive understanding of social determinants in designing effective interventions for childhood obesity.
Intervention policies to prevent obesity in schoolchildren should consider changes within the school environment itself through actions such as improving physical education classes and creating more aggressive nutritional policies. For a greater impact, the inclusion of parents and teachers, as well as government officials, communities, and civil society as elements of healthy lifestyles, as well as the development and well-being of society, is recommended.
Author Contributions
Conceptualization and methodology TSL and MYDMV, software validation and formal analysis, MYDMV and DGVB.; investigation data curation, MCMR. And LMM writing original draft preparation CGG, LMM. MYDMV, JTC; writing—review and editing, IGFN,TSL and MYDMV. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Gonzalo Río Arronte Foundation, Private Assistance Institution, Project: S.730. The foundation did not participate in the systematic review. This study forms part of the project CI:1791
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
Research Group INCAI (Araceli, Salazar-Coronel¹, Erika, Mayorga-Borbolla¹, Corin, Hernández-Palafox¹,Concepción, Medina-Zacarías¹, Alicia, Muñoz-Espinosa¹, Mónica, Medina-Almanza², Wilbert Solís-Concha⁴, Juan C, Salazar-Rendón⁴, Vanessa, Domingo-Bolio⁴, José L, Torres-Escalante³, Alina, Marín-Cárdenas⁵, Abigail, Aguilar-Moguel⁵, Mariel Triunfo-Sánchez⁵)
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| INCAI | Community Intervention of Integral Action for Children in Nutritious and Healthy Environments |
| MMAT | Mixed Methods Appraisal Tool |
| OW+Ob | Overweight and obesity |
| DOAJ | Directory of Open Access Journals |
| DOI | Digital Object Identifier |
| WHO | World Health Organization |
| BMI | Body Mass Index |
| D/N | Diet or Nutrition |
References
- Waterlander WE, Singh A, Altenburg T, Dijkstra C, Luna Pinzon A, Anselma M, et al. Understanding obesity-related behaviors in youth from a systems dynamics perspective: The use of causal loop diagrams. Obes Rev. 2021 Jul 1;22(7). [CrossRef]
- Reilly, JJ. Obesity in childhood and adolescence: Evidence based clinical and public health perspectives. Vol. 82, Postgraduate Medical Journal. 2006. p. 429–37. [CrossRef]
- Neri D, Steele EM, Khandpur N, Cediel G, Zapata ME, Rauber F, et al. Ultraprocessed food consumption and dietary nutrient profiles associated with obesity: A multicountry study of children and adolescents. Obesity Reviews. 2021 Dec; e13387. Available from: https://onlinelibrary.wiley.com/doi/full/10.1111/obr.13387.
- Campos Nonato I, Cuevas Nasu L, González Castell LD, Hernández Barrera L, Shamah Levy T, González de Cosío Martínez T, et al. Epidemiología de la obesidad y sus principales comorbilidades en México. En: La obesidad en México Estado de la política pública y recomendaciones para su prevención y control. 2018. ISBN: 978-607-511-179-7.
- Lobstein T, Jackson-Leach R, Powis J, Brinsden H, Gray M. World Obesity Atlas 2023. World Obesity Federation. 2023;(March). Available: https://data.worldobesity.org/publications/?cat=19.
- OMS. World Health Organization; 2019 [cited 2025 Jan 29]. OMS 10 datos sobre la obesidad. Available from: https://www.who.int/features/factfiles/obesity/es/.
- Bentham J, di Cesare M, Bilano V, Bixby H, Zhou B, Stevens GA, et al. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. The Lancet. 2017 Dec 16;390(10113):2627–42. [CrossRef]
- Lee EY, Yoon KH. Epidemic obesity in children and adolescents: risk factors and prevention. Front Med. 2018 Dec;12(6):658-666. Epub 2018 Oct 2. [CrossRef] [PubMed]
- García Milian, A. J., & Creus García, E. D. (2016). La obesidad como factor de riesgo, sus determinantes y tratamiento. Revista Cubana de Medicina General Integral, 32(3), 1-13. Available from: http://scielo.sld.cuhttp://scielo.sld.cu2.
- Weihrauch-Blüher, S., & Wiegand, S. (2018). Risk Factors and Implications of Childhood Obesity. Current obesity reports, 7(4), 254–259. [CrossRef]
- UNICEF El sobrepeso en la niñez: un llamado a la prevencion en América Latina y el Caribe [Internet]. Panamá; 2022 Jul [cited 2024 May 27]. Available from: www.unicef.org/lac.
- Sánchez Arenas, J. J. , & Ruiz Martínez, A. O. (2015). Relationship between self-esteem and body image in children with obesity. Revista Mexicana de trastornos alimentarios, 6(1), 38-44.Available from: http://journals.iztacala.unam.mx/index.php/amta/article/view/336. [CrossRef]
- Pérez-Herrera A, Cruz-López M, Cruz Xoxocotlán S, Cruz Xoxocotlán Oaxaca S, Situación CM. Situación actual de la obesidad infantil en México. Nutr Hosp. 2019 Mar 1;36(2):463–9. [CrossRef]
- Rausch Herscovici C, Kovalskys I. Obesidad Infantil. Una revisión de las intervenciones preventivas en escuelas. Revista Mexicana de Trastornos Alimentarios. 2015;6(2):143–51. [CrossRef]
- Pamungkas RA, Chamroonsawasdi K. Home-Based Interventions to Treat and Prevent Childhood Obesity: A Systematic Review and Meta-Analysis. Behavioral Sciences 2019, Vol 9, Page 38. 2019 Apr 12 [cited 2023 Oct 5];9(4):38. Available from: https://www.mdpi.com/2076-328X/9/4/38/htm.
- Van De Kolk I, Verjans-Janssen SRB, Gubbels JS, Kremers SPJ, Gerards SMPL. Systematic review of interventions in the childcare setting with direct parental involvement: Effectiveness on child weight status and energy balance-related behaviours. International Journal of Behavioral Nutrition and Physical Activity. 2019 Nov 21 [cited 2023 Oct 6];16(1):1–28. Available from: https://ijbnpa.biomedcentral.com/articles/10.1186/s12966-019-0874-6.
- Denova-Gutiérrez E, González-Rocha A, Méndez-Sánchez L, Araiza-Nava B, Balderas N, López G, et al. Overview of Systematic Reviews of Health Interventions for the Prevention and Treatment of Overweight and Obesity in Children. Nutrients. 2023 Feb 1;15(3):773. Available from: https://www.mdpi.com/2072-6643/15/3/773/htm.
- Palmer JC, Davies AL, Spiga F, Heitmann BL, Jago R, Summerbell CD, Higgins JPT; Inequity in Obesity Prevention Trialists Collaborative Group. Do the effects of interventions aimed at the prevention of childhood obesity reduce inequities? A re-analysis of randomized trial data from two Cochrane reviews. EClinicalMedicine. 2025 Mar 4;81:103130. [CrossRef]
- Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane handbook for systematic reviews of interventions. Cochrane Handbook for Systematic Reviews of Interventions. 2019 Jan 1 [cited 2023 Jan 24];1–694. Available from: https://onlinelibrary.wiley.com/doi/book/10.1002/9781119536604.
- Venturelli F, Ferrari F, Broccoli S, Bonvicini L, Mancuso P, Bargellini A, Giorgi Rossi P. The effect of Public Health/Pediatric Obesity interventions on socioeconomic inequalities in childhood obesity: A scoping review. Obes Rev. 2019 Dec;20(12):1720-1739. [CrossRef]
- Rivera Dommarco JA, Colchero MA, Fuentes ML, González de Cosío Martínez T, Aguilar Salinas CA, Hernández Licona G, et al. La obesidad en México: Estado de la política pública y recomendaciones para su prevención y control. Primera Ed. Oropeza AC, Reveles CF, Canto RAS, editors. Instituto Nacional de Salud Publica. Cuernavaca, Morelos, México.: Instituto Nacional de Salud Pública; 2018. 190–200 p.
- Trickett EJ, Rauk L. Community well-being, community intervention, and community development: changing community ecology. In: Page-Reeves J, editor. Well-being as a multidimensional concept: understanding connections among culture, community, and health. Lanham, Maryland: Lexington Books; 2019 p75–98. Available from: https://digitalrepository.unm.edu/hsc_facbookdisplay/2.
- Saaiq M, Ashraf B. Modifying “Pico” Question into “Picos” Model for More Robust and Reproducible Presentation of the Methodology Employed in A Scientific Study. World J Plast Surg. 2017 Sep;6(3):390.
- ONU. Metodología. 2022. Standard country or area codes for statistical use (M49). Available from: https://unstats.un.org/unsd/methodology/m49/.
- Hong QN, Pluye P, Fàbregues S, Bartlett G, Boardman F, Cargo M, Dagenais P, Gagnon M-P, Griffiths F, Nicolau B, O’Cathain A, Rousseau M-C, Vedel I. Mixed Methods Appraisal Tool (MMAT), version 2018. Registration of Copyright (#1148552), Canadian Intellectual Property Office, Industry Canada.
- Hong QN, Fàbregues S, Bartlett G, Boardman F, Cargo M, Dagenais P, et al. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Education for Information. 2018 Jan 1;34(4):285–91.
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021 Mar 29; n71. Available from: https://www.bmj.com/lookup/doi/10.1136/bmj.n71.
- Tarro, L. , Llauradó, E., Albaladejo, R., Moriña, D., Arija, V., Solà, R., & Giralt, M. (2014). A primary-school-based study to reduce the prevalence of childhood obesity--the EdAl (Educació en Alimentació) study: a randomized controlled trial. Trials, 15(1), 58. [CrossRef]
- Bacardí-Gascon M, Pérez-Morales ME, Jiménez-Cruz A. Intervención aleatorizada de seis meses en las escuelas, con un seguimiento de 18 meses para la prevención de obesidad infantil en escuelas primarias de México. Nutr Hosp. 2012;27(3):755–62. Available from: https://pubmed.ncbi.nlm.nih.gov/23114940/.
- Waters, E. , Gibbs, L., Tadic, M., Ukoumunne, O. C., Magarey, A., Okely, A. D., Silva, A., Armit, C., Green, J., O'Connor, T., Johnson, B., Swinburn, B., Carpenter, L., Moore, G., Littlecott, H., Gold, L. (2018). Cluster randomised trial of a school-community child health promotion and obesity prevention intervention: findings from the evaluation of fun 'n healthy in Moreland. BMC Public Health, 18(92), 1-16. [CrossRef]
- Safdie, M. , Jennings-Aburto, N., Lévesque, L., Janssen, I., Campirano-Núñez, F., López-Olmedo, N., Aburto, T., & Rivera, J. A. (2013). Impact of a school-based intervention program on obesity risk factors in Mexican children. Salud pública de México, 55 Suppl 3, 374–387. [CrossRef]
- Long, M. W. , Weber, M. R., Allan, M. J., Ma, Y., Jin, Y., Aldous, A., Elliot, A. J., & Burke, H. (2020). Evaluation of a pragmatic trial of a collaborative school-based obesity prevention intervention in a low-income urban district. Preventive medicine, 133, 106020. Advance online publication. [CrossRef]
- Lipton-Inga M, Manzanarez B, Vidmar AP, Garcia S, Fink C, Iverson E, Geffner ME. Kids N Fitness Junior: Outcomes of an Evidence-Based Adapted Weight Management Program for Children Ages Three-Seven Years. Child Obes. 2022 Jan;18(1):56-66. [CrossRef]
- Vásquez, F. Díaz, E. Lera, L. Meza, J. Salas, I. Rojas, P. Atalah, E. Burrows, R. (2013). Efecto residual del ejercido de fuerza muscular en la prevención secundaria de la obesidad infantil. Nutrición hospitalaria. Vol 28. N 2. 333-339. [CrossRef]
- Scruzzi, Graciela, Cebreiro, Cynthia, Pou, Sonia, & Rodríguez Junyent C, Constanza. (2014). Salud escolar: una intervención educativa en nutrición desde un enfoque integral. Cuadernos.info, (35), 39-53. [CrossRef]
- Flynn, A. C. , Suleiman, F., Windsor-Aubrey, H., Wolfe, I., O'Keeffe, M., Poston, L., & Dalrymple, K. V. (2022). Preventing and treating childhood overweight and obesity in children up to 5 years old: A systematic review by intervention setting. Maternal & child nutrition, 18(3), e13354. [CrossRef]
- Morgan, E. H. , Schoonees, A., Sriram, U., Faure, M., & Seguin-Fowler, R. A. (2020). Caregiver involvement in interventions for improving children's dietary intake and physical activity behaviors. The Cochrane database of systematic reviews, 1(1), CD012547. [CrossRef]
- Liu, Z. , Xu, H. M., Wen, L. M., Peng, Y. Z., Lin, L. Z., Zhou, S., Li, W. H., & Wang, H. J. (2019). A systematic review and meta-analysis of the overall effects of school-based obesity prevention interventions and effect differences by intervention components. The international journal of behavioral nutrition and physical activity, 16(1), 95. [CrossRef]
- Ameryoun, A., Sanaeinasab, H., Saffari, M., & Koenig, H. G. (2018). Impact of Game-Based Health Promotion Programs on Body Mass Index in Overweight/Obese Children and Adolescents: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Childhood obesity (Print), 14(2), 67–80. [CrossRef]
- Bleich, S. N. , Vercammen, K. A., Zatz, L. Y., Frelier, J. M., Ebbeling, C. B., & Peeters, A. (2018). Interventions to prevent global childhood overweight and obesity: a systematic review. The lancet. Diabetes & endocrinology, 6(4), 332–346. [CrossRef]
- Sadeghi, B. , Kaiser, L.L., Hanbury, M.M., Tseregounis I.E., Shaikh U., Gomez-Camacho R., et al. A three-year multifaceted intervention to prevent obesity in children of Mexican-heritage. BMC Public Health 19, 582 (2019). [CrossRef]
- Centeio, E. E. , McCaughtry, N., Moore, E. W. G., Kulik, N., Garn, A., Martin, J., Shen, B., Somers, C. L., & Fahlman, M. (2018). Building healthy communities: A comprehensive school health program to prevent obesity in elementary schools. Preventive medicine, 111, 210–215. [CrossRef]
- Brown, T., Moore, T. H., Hooper, L., Gao, Y., Zayegh, A., Ijaz, S., Elwenspoek, M., Foxen, S. C., Magee, L., O'Malley, C., Waters, E., & Summerbell, C. D. (2019). Interventions for preventing obesity in children. The Cochrane database of systematic reviews, 7(7), CD001871. [CrossRef]
- Cauchi, D. , Glonti, K., Petticrew, M., & Knai, C. (2016). Environmental components of childhood obesity prevention interventions: an overview of systematic reviews. Obesity reviews: an official journal of the International Association for the Study of Obesity, 17(11), 1116–1130. [CrossRef]
- Giannini, C. , Irby, M. B., & Skelton, J. A. (2015). Caregiver Expectations of Family-based Pediatric Obesity Treatment. American journal of health behavior, 39(4), 451–460. [CrossRef]
- Shamah Levy, T. , Morales Ruán, C., Amaya Castellanos, C., Salazar Coronel, A., Jiménez Aguilar, A., & Méndez Gómez Humarán, I. (2012). Effectiveness of a diet and physical activity promotion strategy on the prevention of obesity in Mexican school children. BMC public health, 12, 152. [CrossRef]

Table 1.
Key characteristics of the studies
| Objective | Summary highlights | Intervention Length (months) | Country | Participants (intervention = I, control = C) | Implementation Area for Dietary, Nutritional, and Physical Activity Components | Measurements used to Estimate Obesity | |
|---|---|---|---|---|---|---|---|
| A six-month randomized school intervention and an 18-month follow-up intervention to prevent childhood obesity in Mexican elementary schools. [22] | |||||||
| To assess the effect of a six-month intervention and an 18-month follow-up intervention on the body mass index, food consumption, and physical activity of 2nd and 3rd grade elementary school children. | A randomized trial with 532 participants showed a significant BMI reduction of -0.82 (p = 0.0001) at six months. At 24 months, there were notable increases in the BMI z-score and waist circumference, with reduced abdominal obesity, 8% remission, and 18% overweight/obesity incidence. Comprehensive intervention increased vegetable intake (p = 0.007) and physical activity (p = 0.0001) while reducing sedentary behaviors and high fat/salty snack consumption. | 24 | Mexico | I: 280, C: 252 | School setting in regular school hours, school setting extracurricular | Weight, Height, BMI, Waist Circumference | |
| Building healthy communities: A comprehensive school health program to prevent obesity in elementary schools [23] | |||||||
| This study examined the impact of a socioecological theory driven by school-wide nutrition and physical activity interventions on 5th graders' central adiposity and obesity levels. | A school-wide program integrating nutrition and physical activity, guided by socioecological theory, reduced central adiposity in 5th graders. Over eight months, 377 treated students saw significant decreases in central adiposity compared to 251 controls, hinting at potential BMI reductions. This finding highlights the effectiveness of holistic school interventions in promoting children's health. | 8 | United States of America | I: 2,019, C: 1,035 | School setting in regular school hours, school setting extracurricular | Weight, Height, BMI, Waist Circumference, Waist-Hip Ratio | |
| Evaluation of a pragmatic trial of a collaborative school-based obesity prevention intervention in a low-income urban district. [24] | |||||||
| To evaluate changes in diet and physical activity in intervention schools using surveys and direct observation | This study explored whether empowering school leaders to choose suitable components from evidence-based programs could overcome barriers to their implementation. A customized intervention was applied from 2013 to 2016 in nine schools across a low-income urban district. While the program demonstrably lowered the BMI of students in the two semesters, the effect did not persist. Despite this, the study proved a valuable method: it empowered school leaders, leveraged existing district resources, and reduced the evaluation burden. These insights offer a promising avenue for future obesity prevention. | 36 | United States of America | I: 3,152, C: 2,730 | School setting in regular school hours, school setting extracurricular and summer camp | Weight, Height, BMI | |
| A three-year multifaceted intervention to prevent obesity in children of Mexican heritage. [25] | |||||||
| To estimate the effects of a multifaceted, community-based intervention on body mass index (BMI) among Mexican heritage children. | This study evaluated the effects of the Niños Sanos and Familia Sana interventions on BMI among Mexican-heritage children in California's Central Valley. Over three years, the multifaceted program included parent workshops, school nutrition lessons, enhanced physical education, and monthly fruit and vegetable vouchers. It significantly slowed BMI growth in boys and reduced BMI in obese girls, underscoring the need to address gender disparities and collaborate with stakeholders to combat childhood obesity. | 36 | United States of America | I: 387, C: 313 | School setting in regular school hours, school setting extracurricular, community involvement | Weight, Height, BMI, Waist Circumference | |
| Impact of a school-based intervention program on obesity risk factors in Mexican children. [25] | |||||||
| To evaluate the impact of an 18-month intervention to prevent obesity in 4th and 5th grade students grounded on the ecological model of healthy behaviors in Mexico. | This study was guided by ecological principles and formal research. Employing a randomized controlled trial (RCT) design, 27 schools were assigned to basic or plus interventions and control conditions in a sample of 830 students. Over two years, data on the school environment, children's eating and physical activity, and BMI were collected from 830 students. Intervention schools showed an increased availability of healthy foods and decreased unhealthy options, with a similar trend in food intake. No significant increase in moderate-to-vigorous physical activity (MVPA) during PE or recess was observed; however, an increase in steps taken was noted. | 18 | Mexico | I: 526+262 | School setting in regular school hours | Weight, Height, BMI | |
| School Health: An Educational Nutrition Intervention from a Comprehensive Approach [27] | |||||||
| To encourage healthy lifestyles among school-age children attending a public school in Córdoba, Argentina (2013-2014). | An interdisciplinary intervention (2013-2014) aimed to promote healthy lifestyles through diagnoses, food education, and healthy kiosks. The findings highlight concerns such as being overweight, sugary drink consumption, and school food kiosks. The project successfully achieved its goals by emphasizing the importance of family and school communities in shaping healthy eating habits. | 12 | Argentina | I: 127 C: N/A | School setting in regular school hours, school setting extracurricular, did not include a physical activity component | Weight, Height, BMI | |
| A primary-school-based study to reduce the prevalence of childhood obesity--the EdAl (Educacio en Alimentacio) study: a randomized controlled trial [28]. | |||||||
| The aims of the study were: 1) to design a health promotion program for implementation by HPAs in primary schools, and 2) to evaluate the effects of a 3-year school-based program of lifestyle improvement, including diet and physical activity over a period of 28 months, on the prevalence of obesity. | In a randomized comparison, the intervention group showed a 2% reduction in obesity prevalence among boys, resulting in a significant drop in BMI z-scores. More intervention boys achieved the recommended physical activity levels, with increased fish consumption protecting against obesity, emphasizing the effectiveness of university student-led interventions in reducing childhood obesity. | 24 | España | I: 1,222, C: 717 | School setting in regular school hours, school setting extracurricular | Weight, Height, BMI, Waist Circumference | |
| Residual effect of muscle strength exercise in the secondary prevention of childhood obesity [29]. | |||||||
| To evaluate the residual effect of muscular strength exercise on body fat, metabolic syndrome, and physical fitness in schoolchildren with obesity. | This study explored the long-term effects of a 3-month muscle strength training program combined with nutritional and psychological support for obese schoolchildren in Santiago, Chile. While the program yielded positive results in terms of body fat reduction, increased walking distance, and improvement in metabolic syndrome within the 3-month period, these benefits largely faded by 9 months after the program ended. These findings suggest that long-term interventions and support systems are crucial for sustainable improvement of the health of obese children. | 9 | Chile | I: 111, C: 111 | School setting in regular school hours | Weight, Height, BMI, Waist Circumference, lipids, and elements of metabolic syndrome | |
| Cluster randomized trial of a school-community child health promotion and obesity prevention intervention [30]. | |||||||
| The community-based child obesity prevention study, fun 'n healthy in Moreland, emerged as a research group and a local community health service with the aim of making a difference to the adverse health outcomes experienced through child disadvantage in an inner-city area of Melbourne, Australia. | "Fun 'n healthy in Moreland!" A multiyear school-based program aimed at reducing childhood obesity in a disadvantaged area in Australia. While it did not significantly impact children's body mass index after 3.5 years, the intervention did show success in other areas. Despite not demonstrating a direct impact on BMI, the intervention's success in promoting healthy behaviours, policy changes, and parental engagement suggests its potential long-term benefits. | 42 | Australia | I: 1,426, C: 1,460 | School setting in regular school hours, home | Weight, Height, BMI, Waist Circumference | |
| Improving healthy dietary behaviours, nutrition knowledge, and self-efficacy among underserved school children with parent and community involvement [31]. | |||||||
| To measure over a 1-year period whether a CSHP with parental, school, and home-based components to promote optimal nutrition will reduce BMI percentiles and z-scores and improve dietary behaviors in a sample of low-income school-aged children. | A school-based program partnering with parents and the community showed promise in tackling childhood obesity among low-income Mexican American children. This one-year study enrolled 251 children in a program that combined after-school nutrition and fitness education, school-based wellness initiatives, and parent focus groups. Compared to the control group, children in the program experienced significant improvements: their BMI and BMI z-scores decreased; vegetable, fruit, and fruit juice intake increased; and self-efficacy for healthy food choices improved. Moreover, parental and community involvement surged to 100% by the end of the year. | 12 | United States of America | I: 251 C: N/A | School setting in regular school hours, school setting extracurricular, community involvement, did not include a physical activity component | Weight, Height, BMI | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



