Submitted:
01 October 2025
Posted:
02 October 2025
You are already at the latest version
Abstract
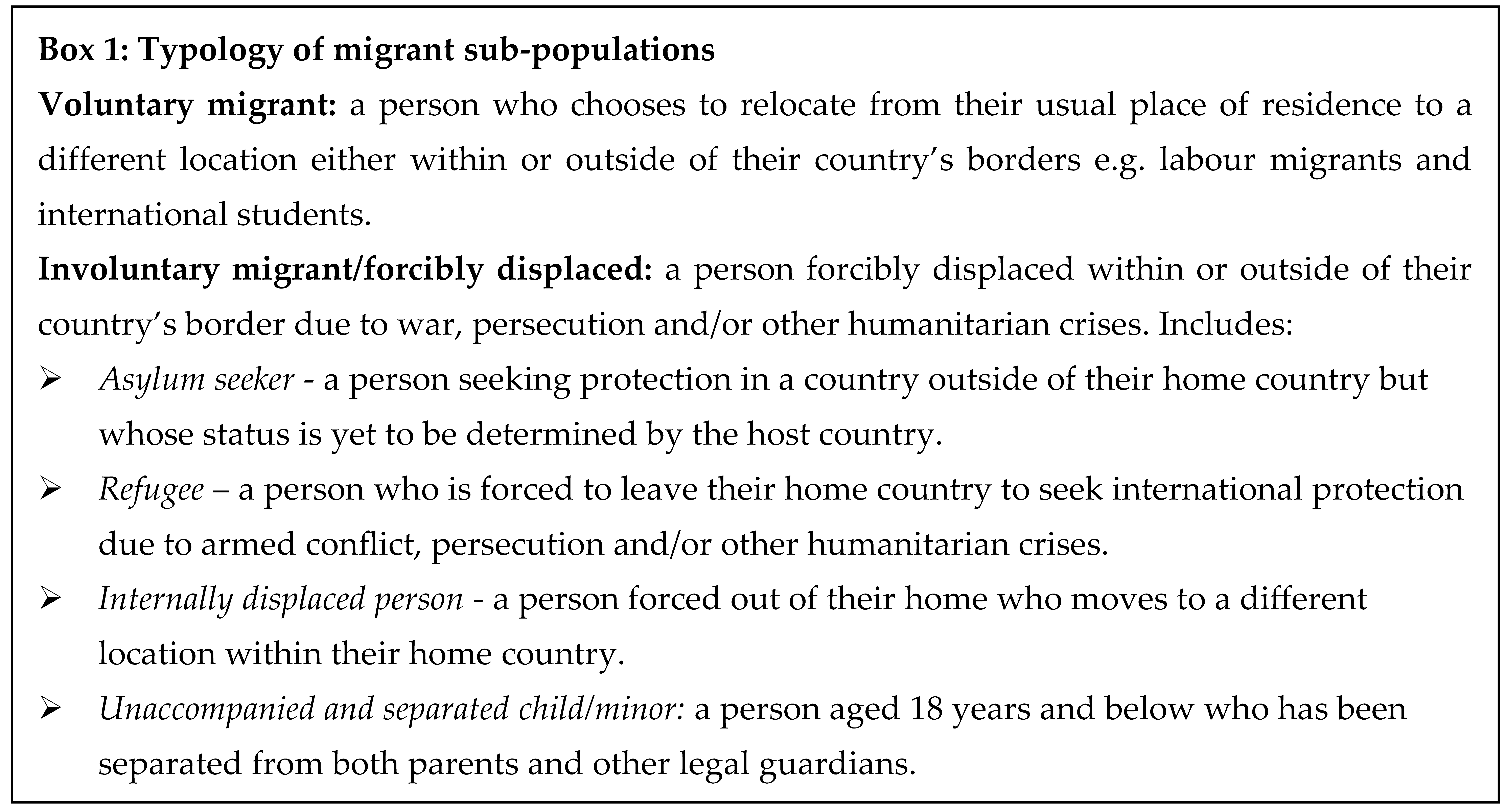
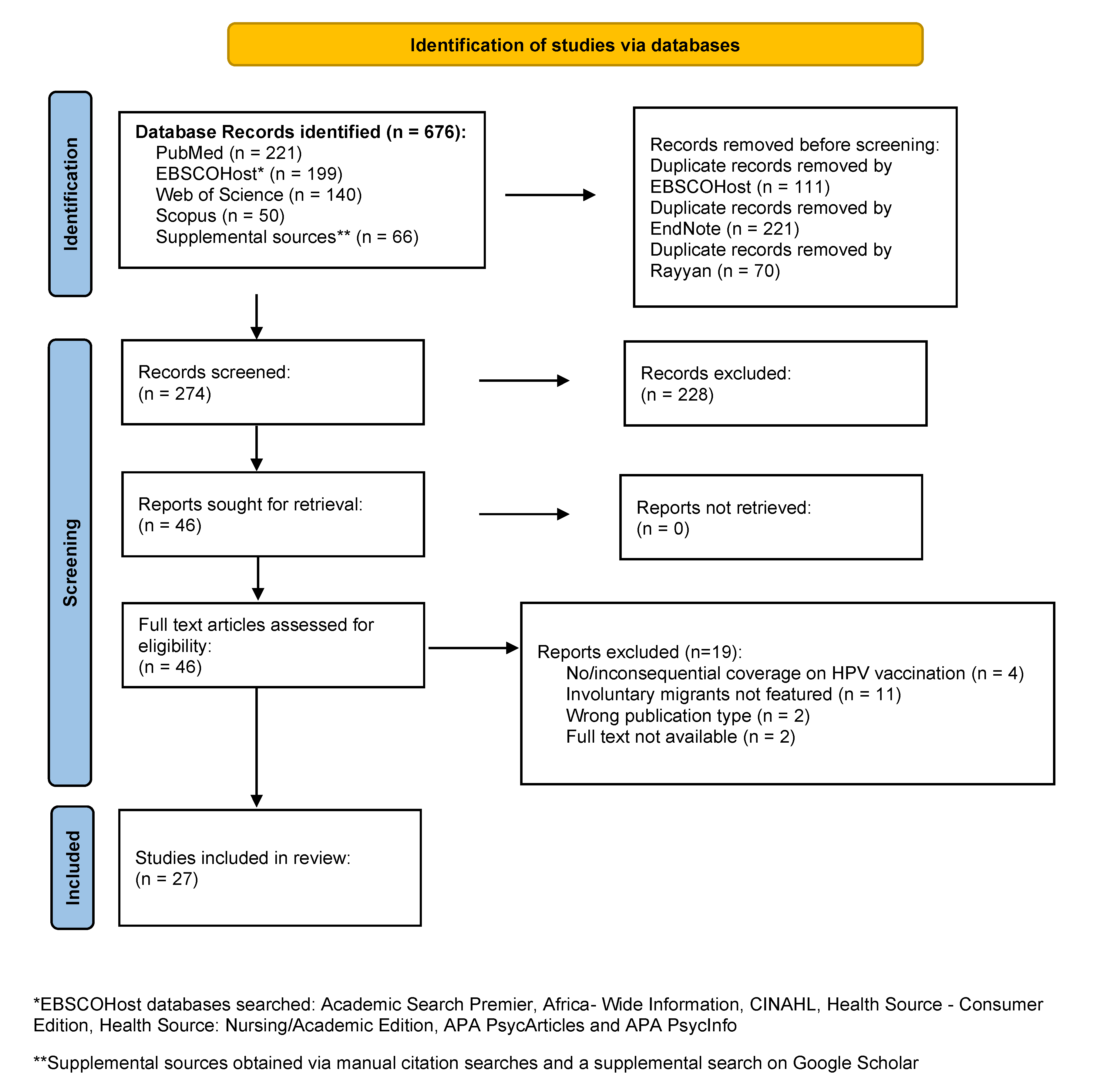
Background: Migrant populations are commonly under-immunised relative to general populations in host countries. The evidence base on routine vaccination among migrant children suggests higher priority is given to infants and younger children compared to adolescents. Though migrants are often classified as a homogenous group, different sub-populations of migrants exist, including voluntary migrants who choose to move, and involuntary migrants forcibly displaced by humanitarian crises. The human papillomavirus (HPV) vaccine, a relatively recent addition to global routine immunisation schedules for adolescents, is a useful proxy for understanding vaccine equity for this under-prioritised group. This qualitative systematic review explores health system determinants of delivery and uptake of HPV vaccination services among involuntary migrants. Methods: A literature search was conducted across ten electronic databases. An analytical framework tailored to the migrant context aided in capturing the complexity and magnitude of systemic factors that determine vaccine delivery and uptake among involuntary migrants. Of the 676 records retrieved, 27 studies were included in this review. Results: Key determinants of vaccine delivery include adaptation of immunisation policies for migrant inclusiveness, implementation of migrant-targeted interventions, health provider recommendations, electronic health records and free vaccines. Uptake determinants include access dependent on legal status, awareness-related determinants akin to culturally appropriate health messaging, and acceptance-related determinants associated with sociocultural beliefs, misinformation and distrust. Conclusion: Prioritising vaccination programmes linked with non-outbreak-related diseases is challenging in the disruptive context of humanitarian crises given fragile health systems, limited resources, loss of health infrastructure and deployment of health personnel to emergency care. We strongly advocate for global actors at all health systems levels to actively reform national HPV vaccination programs to enhance inclusivity of adolescent girls in crises settings or resettled in host countries.
Keywords:
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of interest
Abbreviations
| HPV | Human Papillomavirus |
| LMICs | Low-and-Middle-Income Countries |
| HICs | High-Income Countries |
| WHO | World Health Organization |
| NIPs | National Immunisation Programs |
| USA | United States of America |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| JBI | Joanna Briggs Institute |
| RHAP | Refugee Health Assessment Program |
References
- Bray F, Laversanne M, Sung H, Ferlay J, Siegel RL, Soerjomataram I, Jemal A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: a cancer journal for clinicians. 2024;74(3):229-63.
- Allanson ER, Schmeler KM. Cervical cancer prevention in low-and middle-income countries. Clinical obstetrics and gynecology. 2021;64(3):501-18.
- Hull R, Mbele M, Makhafola T, Hicks C, Wang SM, Reis RM, et al. Cervical cancer in low and middle--income countries. Oncology letters. 2020;20(3):2058-74.
- Guida F, Kidman R, Ferlay J, Schüz J, Soerjomataram I, Kithaka B, et al. Global and regional estimates of orphans attributed to maternal cancer mortality in 2020. Nature medicine. 2022;28(12):2563-72.
- Marques P, Nunes M, Antunes MdL, Heleno B, Dias S. Factors associated with cervical cancer screening participation among migrant women in Europe: a scoping review. International journal for equity in health. 2020;19:1-15.
- Collatuzzo G, Ferrante M, Ippolito A, Di Prima A, Colarossi C, Scarpulla S, et al. Cancer in Migrants: A Population-Based Study in Italy. Cancers. 2023;15(12):12.
- Leinonen MK, Campbell S, Ursin G, Tropé A, Nygård M. Barriers to cervical cancer screening faced by immigrants: a registry-based study of 1.4 million women in Norway. The European Journal of Public Health. 2017;27(5):873-9.
- De Martel C, Plummer M, Vignat J, Franceschi S. Worldwide burden of cancer attributable to HPV by site, country and HPV type. International journal of cancer. 2017;141(4):664-70.
- Amponsah-Dacosta E, Blose N, Nkwinika VV, Chepkurui V. Human Papillomavirus Vaccination in South Africa: Programmatic Challenges and Opportunities for Integration With Other Adolescent Health Services? Frontiers in Public Health. 2022;10.
- World Health Organisation. WHO recommendations for routine immunisation—summary tables. Internet; 2023.
- Dau H, Trawin J, Nakisige C, Payne BA, Vidler M, Singer J, et al. The social and economic impacts of cervical cancer on women and children in low--and middle--income countries: A systematic review. International Journal of Gynecology & Obstetrics. 2023;160(3):751-61.
- World Health Organisation. Global strategy to accelerate the elimination of cervical cancer as a public health problem. Geneva: World Health Organisation; 2020.
- Bruni L, Saura-Lázaro A, Montoliu A, Brotons M, Alemany L, Diallo MS, et al. HPV vaccination introduction worldwide and WHO and UNICEF estimates of national HPV immunization coverage 2010–2019. Preventive medicine. 2021;144:106399.
- Castelli, F. Drivers of migration: why do people move? Journal of travel medicine. 2018;25(1):tay040.
- Giménez-Gómez J-M, Walle YM, Zergawu YZ. Trends in African migration to Europe: Drivers beyond economic motivations. Journal of Conflict Resolution. 2019;63(8):1797-831.
- International Organisation for Migration. International Migration Law: Glossary of Migration. Geneva; 2019.
- World Health Organisation. Ensuring the integration of refugees and migrants in immunization policies, planning and service delivery globally. Geneva: World Health Organization; 2022.
- Babakura B, Nomhwange T, Jean Baptiste AE, Dede O, Taiwo L, Abba S, et al. The challenges of insecurity on implementing vaccination campaign and its effect on measles elimination and control efforts: A case study of 2017/18 measles campaign in Borno state, Nigeria. Vaccine. 2021;39 Suppl 3:C66-c75.
- Ngo NV, Pemunta NV, Muluh NE, Adedze M, Basil N, Agwale S. Armed conflict, a neglected determinant of childhood vaccination: some children are left behind. Human Vaccines and Immunotherapeutics. 2020;16(6):1454-63.
- Crawshaw AF, Farah Y, Deal A, Rustage K, Hayward SE, Carter J, et al. Defining the determinants of vaccine uptake and undervaccination in migrant populations in Europe to improve routine and COVID-19 vaccine uptake: a systematic review. LANCET INFECTIOUS DISEASES. 2022;22(9):E254-E66.
- Deal A, Crawshaw AF, Carter J, Knights F, Iwami M, Darwish M, et al. Defining drivers of under-immunisation and vaccine hesitancy in refugee and migrant populations globally to support strategies to strengthen vaccine uptake for COVID-19: a rapid review. medRxiv. 2023:2023.03. 20.23287477.
- Gorman DR, Bielecki K, Larson HJ, Willocks LJ, Craig J, Pollock KG. Comparing vaccination hesitancy in Polish migrant parents who accept or refuse nasal flu vaccination for their children. Vaccine. 2020;38(13):2795-9.
- Ganczak M, Bielecki K, Drozd-Dąbrowska M, Topczewska K, Biesiada D, Molas-Biesiada A, et al. Vaccination concerns, beliefs and practices among Ukrainian migrants in Poland: a qualitative study. BMC public health. 2021;21(1):1-13.
- Fang H, Yang L, Zhang H, Li C, Wen L, Sun L, et al. Strengthening health system to improve immunization for migrants in China. International journal for equity in health. 2017;16(1):19.
- Ekezie W, Awwad S, Krauchenberg A, Karara N, Dembinski L, Grossman Z, et al. Access to Vaccination among Disadvantaged, Isolated and Difficult-to-Reach Communities in the WHO European Region: A Systematic Review. VACCINES. 2022;10(7).
- Hill DC, Andrade-Romo Z, Solari K, Adams E, Forman L, Grace D, et al. COVID-19 vaccine equity and the right to health for displaced Venezuelans in Latin America. PLOS global public health. 2023;3(3):e0001275.
- Tankwanchi AS, Bowman B, Garrison M, Larson H, Wiysonge CS. Vaccine hesitancy in migrant communities: a rapid review of latest evidence. Current Opinion in Immunology. 2021;71:62-8.
- Deal A, Halliday R, Crawshaw AF, Hayward SE, Burnard A, Rustage K, et al. Migration and outbreaks of vaccine-preventable disease in Europe: a systematic review. The Lancet Infectious Diseases. 2021;21(12):e387-e98.
- UNHCR. Global trends: forced displacement in 2022. Copenhagen: United Nations High Commissioner for Refugees; 2023.
- Sheikh K, Gilson L, Agyepong IA, Hanson K, Ssengooba F, Bennett S. Building the field of health policy and systems research: framing the questions. PLoS medicine. 2011;8(8):e1001073.
- Atun, R. Health systems, systems thinking and innovation. Health policy and planning. 2012;27(suppl_4):iv4-iv8.
- World Health Organisation. Immunization Agenda 2030: A global strategy to leave no one behind. 2021.
- JBI Manual for Evidence Synthesis: The Joanna Briggs Institute (JBI); 2021. Available from: https://synthesismanual.jbi.global. [CrossRef]
- Page M, McKenzie J, Bossuyt P, Boutron I, Hoffmann T, Mulrow C. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. PLoS Med. 2021;18(3):e1003583.
- Githaiga JN, Noll S, Olivier J, Amponsah-Dacosta E. What’s in a name?–How migrant populations are classified and why this matters for (in) equitable access to routine childhood and adolescent immunisation services: A scoping review. Vaccine. 2025;49:126784.
- The EndNote Team. EndNote. EndNote 20 ed. Philadelphia, PA: Clarivate; 2013.
- Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan—a web and mobile app for systematic reviews. Systematic reviews. 2016;5(1):1-10.
- Bednarczyk RA, Chamberlain A, Mathewson K, Salmon DA, Omer SB. Practice-, provider-, and patient-level interventions to improve preventive care: development of the P3 model. Preventive medicine reports. 2018;11:131-8.
- Thomson A, Robinson K, Vallée-Tourangeau G. The 5As: A practical taxonomy for the determinants of vaccine uptake. Vaccine. 2016;34(8):1018-24.
- Vu M, Ta D, Berg CJ, Bednarczyk RA, Huynh VN, King AR, Escoffery C. US Vietnamese Mothers’ HPV Vaccine Decision- Making for Their Adolescents: A Qualitative Study. JOURNAL OF HEALTH CARE FOR THE POOR AND UNDERSERVED. 2022;33(4):1985-2006.
- WHO. Everybody’s business : strengthening health systems to improve health outcomes : WHO’s framework for action. Geneva; 2007.
- Witter S, Palmer N, Balabanova D, Mounier--Jack S, Martineau T, Klicpera A, et al. Health system strengthening—reflections on its meaning, assessment, and our state of knowledge. The International journal of health planning and management. 2019;34(4):e1980-e9.
- Joanna Briggs Institute. Checklist for Qualitative Research. 2017.
- Joanna Briggs Institute. Checklist for Cohort Studies. 2017.
- Joanna Briggs Institute. Checklist for Cohort Studies. 2017.
- Hong QN, Pluye P, Fàbregues S, Bartlett G, Boardman F, Cargo M, et al. Mixed methods appraisal tool (MMAT), version 2018. Registration of copyright. 2018;1148552(10).
- Do H, Seng P, Talbot J, Acorda E, Coronado GD, Taylor VM. HPV vaccine knowledge and beliefs among Cambodian American parents and community leaders. Asian Pacific journal of cancer prevention: APJCP. 2009;10(3):339.
- Allen EM, Lee HY, Pratt R, Vang H, Lightfoot E, Desai JR, Dube A. Facilitators and Barriers of Cervical Cancer Screening and Human Papilloma Virus Vaccination Among Somali Refugee Women in the United States: A Qualitative Analysis. Journal of Transcultural Nursing. 2019;30(1):55-63.
- Burke NJ, Do HH, Talbot J, Sos C, Ros S, Taylor VM. Protecting our Khmer daughters: ghosts of the past, uncertain futures, and the human papillomavirus vaccine. Ethnicity & Health. 2015;20(4):376-90.
- Ghebrendrias S, Pfeil S, Crouthamel B, Chalmiers M, Kully G, Mody S. An Examination of Misconceptions and Their Impact on Cervical Cancer Prevention Practices among Sub-Saharan African and Middle Eastern Refugees. Health Equity. 2021;5(1):382-9.
- Khan A, Abonyi S, Neudorf C, Galea S, Ahmed S. Barriers to and facilitators of human papillomavirus vaccination in an ethnically diverse group of migrant parents: A qualitative mixed methods study. Hum Vaccin Immunother. 2023;19(3):2269721.
- McComb E, Ramsden V, Olatunbosun O, Williams-Roberts H. Knowledge, Attitudes and Barriers to Human Papillomavirus (HPV) Vaccine Uptake Among an Immigrant and Refugee Catch-Up Group in a Western Canadian Province. J Immigr Minor Health. 2018;20(6):1424-8.
- Metusela C, Ussher J, Perz J, Hawkey A, Morrow M, Narchal R, et al. “In my culture, we don’t know anything about that”: sexual and reproductive health of migrant and refugee women. Int J Behav Med. 2017;24:836-45.
- Rubens-Augustson T, Wilson LA, Murphy MSQ, Jardine C, Pottie K, Hui C, et al. Healthcare provider perspectives on the uptake of the human papillomavirus vaccine among newcomers to Canada: a qualitative study. Human Vaccines & Immunotherapeutics. 2019;15(7-8):1697-707.
- Salad J, Verdonk P, de Boer F, Abma TA. “A Somali girl is Muslim and does not have premarital sex. Is vaccination really necessary?” A qualitative study into the perceptions of Somali women in the Netherlands about the prevention of cervical cancer. International journal for equity in health. 2015;14(1):1-13.
- Davidson N, Fisher J. “If I know about it of course I would give my son and daughter”, barriers to and enablers of accessing human papillomavirus vaccination among women from refugee and asylum-seeking backgrounds resettling in Melbourne, Australia - A qualitative study. Vaccine. 2025;53:127064.
- Bhatta MP, Johnson DC, Lama M, Maharjan B, Lhaki P, Shrestha S. Cervical Cancer and Human Papillomavirus Vaccine Awareness Among Married Bhutanese Refugee and Nepali Women in Eastern Nepal. Journal of Community Health. 2020;45(3):516-25.
- Dalla V, Panagiotopoulou E-K, Deltsidou A, Kalogeropoulou M, Kostagiolas P, Niakas D, Labiris G. Level of awareness regarding cervical cancer among female Syrian refugees in Greece. Journal of Cancer Education. 2020:1-11.
- Gebre H, Ghamli S, Jackson F, Chavan B, Kingori C. Knowledge, perception and utilization of cervical cancer screening and Human Papillomavirus (HPV) vaccination among immigrants and refugees in Central Ohio. 2021.
- Kepka D, Bodson J, Lai D, Sanchez-Birkhead A, Villalta J, Mukundente V, et al. Factors Associated with Human Papillomavirus Vaccination among Diverse Adolescents in a Region with Low Human Papillomavirus Vaccination Rates. Health Equity. 2018;2(1):223-32.
- Kmeid M, Azouri H, Aaraj R, Bechara E, Antonios D. Vaccine coverage for Lebanese citizens and Syrian refugees in Lebanon. International Health. 2019;11(6):568-79.
- Lee H, Kim M, Kiang P, Shi L, Tan K, Chea P, et al. Factors associated with HPV vaccination among Cambodian American teenagers. Public Health Nursing. 2016;33(6):493-501.
- Napolitano F, Gualdieri L, Santagati G, Angelillo IF. Knowledge and attitudes toward HPV infection and vaccination among immigrants and refugees in Italy. VACCINE. 2018;36(49):7536-41.
- Riza E, Karakosta A, Tsiampalis T, Lazarou D, Karachaliou A, Ntelis S, et al. Knowledge, Attitudes and Perceptions about Cervical Cancer Risk, Prevention and Human Papilloma Virus (HPV) in Vulnerable Women in Greece. Int J Environ Res Public Health. 2020;17(18).
- Snoubar Y, Abusafia B, Turan Z. Factors affecting cervical cancer screening and human papilloma virus vaccination among Middle Eastern refugee women in Türkiye: indicators for social workers and nurses. Ann Med. 2025;57(1):2468261.
- Badre-Esfahani S, Larsen M, Seibæk L, Petersen L, Blaakær J, Andersen B. Low attendance by non-native women to human papillomavirus vaccination and cervical cancer screening–A Danish nationwide register-based cohort study. Preventive Medicine Reports. 2020;19:101106.
- Berman RS, Smock L, Bair-Merritt MH, Cochran J, Geltman PL. Giving It Our Best Shot? Human Papillomavirus and Hepatitis B Virus Immunization Among Refugees, Massachusetts, 2011-2013. PREVENTING CHRONIC DISEASE. 2017;14.
- Elmore CE, Keim-Malpass J, Mitchell EM. Health Inequity in Cervical Cancer Control Among Refugee Women in the United States by Country of Origin. Health Equity. 2021;5(1):119-23.
- Kenny DX, Hsueh K, Walters RW, Coté JJ. Human Papillomavirus Vaccination and Pap Smear Rates Among Burmese Refugee Girls in a Healthcare System in Omaha, Nebraska. Journal of Community Health. 2021;46(6):1170-6.
- Moller SP, Kristiansen M, Norredam M. Human papillomavirus immunization uptake among girls with a refugee background compared with Danish-born girls: a national register-based cohort study. Eur J Cancer Prev. 2018;27(1):42-5.
- Nyanchoga MM, Lee P, Barbery G. Exploring electronic health records to estimate the extent of catch-up immunisation and factors associated with under-immunisation among refugees and asylum seekers in south east Queensland. Vaccine. 2021;39(42):6238-44.
- Lai DJ, Bodson J, Davis FA, Lee D, Tavake-Pasi F, Napia E, et al. Diverse Families’ Experiences with HPV Vaccine Information Sources: A Community-Based Participatory Approach. Journal of Community Health. 2017;42(2):400-12.
- Wilson LA, Quan AML, Bota AB, Mithani SS, Paradis M, Jardine C, et al. Newcomer knowledge, attitudes, and beliefs about human papillomavirus (HPV) vaccination. BMC Family Practice. 2021;22(1).
- Graci D, Piazza N, Ardagna S, Casuccio A, Drobov A, Geraci F, et al. Barriers to and Facilitators for Accessing HPV Vaccination in Migrant and Refugee Populations: A Systematic Review. Vaccines. 2024;12(3):256.
- Netfa F, Tashani M, Booy R, King C, Rashid H, Skinner SR. Knowledge, Attitudes and Perceptions of Immigrant Parents Towards Human Papillomavirus (HPV) Vaccination: A Systematic Review. TROPICAL MEDICINE AND INFECTIOUS DISEASE. 2020;5(2).
- Essa-Hadad J, Gorelik Y, Vervoort J, Jansen D, Edelstein M. Understanding the health system barriers and enablers to childhood MMR and HPV vaccination among disadvantaged, minority or underserved populations in middle-and high-income countries: a systematic review. European Journal of Public Health. 2024;34(2):368-74.
- Carreras-Abad C, Oliveira-Souto I, Pou-Ciruelo D, Pujol-Morro JM, Soler-Palacin P, Soriano-Arandes A, et al. Health and Vaccination Status of Unaccompanied Minors After Arrival in a European Border Country: A Cross-sectional Study (2017-2020). PEDIATRIC INFECTIOUS DISEASE JOURNAL. 2022;41(11):872-7.
- Fozouni L, Weber C, Lindner AK, Rutherford GW. Immunization coverage among refugee children in Berlin. Journal of global health. 2019;9(1):010432.
- Giambi C, Del Manso M, Marchetti G, Olsson K, Adel Ali K, Declich S. Immunisation of migrants in EU/EEA countries: Policies and practices. Vaccine. 2019;37(36):5439-51.
- Mellou K, Silvestros C, Saranti-Papasaranti E, Koustenis A, Pavlopoulou ID, Georgakopoulou T, et al. Increasing childhood vaccination coverage of the refugee and migrant population in Greece through the European programme PHILOS, 17 to 18. Euro surveillance : bulletin Europeen sur les maladies transmissibles = European communicable disease bulletin. 2019;24(27). 20 April.
- MacDonald, NE. Vaccine hesitancy: Definition, scope and determinants. Vaccine. 2015;33(34):4161-4.
- Dinleyici EC, Borrow R. Meningococcal infections among refugees and immigrants: silent threats of past, present and future. Human vaccines & immunotherapeutics. 2020;16(11):2781-6.
- Gargano LM, Hajjeh R, Cookson ST. Pneumonia prevention: Cost-effectiveness analyses of two vaccines among refugee children aged under two years, Haemophilus influenzae type b-containing and pneumococcal conjugate vaccines, during a humanitarian emergency, Yida camp, South Sudan. Vaccine. 2017;35(3):435-42.
- Saifee J, Franco-Paredes C, Lowenstein SR. Refugee health during COVID-19 and future pandemics. Current tropical medicine reports. 2021;8:1-4.
- Olusola O, Penelope C, Chandrakala J, Dick C, Bibilola O, Christopher Otti A, et al. Integrating immunization services into nutrition sites to improve immunization status of internally displaced persons’ children living in Bentiu protection of civilian site, South Sudan. 2019.
- Kapuria B, Hamadeh RS, Mazloum F, Chaalan K, Aung K, Higgins E, et al. Immunization as an entry point for primary health care and beyond healthcare interventions—process and insights from an integrated approach in Lebanon. Frontiers in Health Services. 2023;3:1251775.
- Mirzoev T, Kane S. What is health systems responsiveness? Review of existing knowledge and proposed conceptual framework. BMJ global health. 2017;2(4):e000486.
- Fiks AG, Nekrasova E, Hambidge SJ. Health systems as a catalyst for immunization delivery. Academic Pediatrics. 2021;21(4):S40-S7.
- Lahariya, C. “Health system approach” for improving immunization program performance. Journal of family medicine and primary care. 2015;4(4):487-94.
- Chee G, Pielemeier N, Lion A, Connor C. Why differentiating between health system support and health system strengthening is needed. The International journal of health planning and management. 2013;28(1):85-94.
- Mitchell H, Lim R, Gill PK, Dhanoa J, Dubé È, Bettinger JA. What do adolescents think about vaccines? Systematic review of qualitative studies. PLOS Global Public Health. 2022;2(9):e0001109.

| Selection Criteria | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Publication Genre | Peer reviewed journal articles | Non-peer reviewed publications/grey literature |
| Study Genre | Primary empirical studies | Secondary studies, including reviews |
| Type of study designs evidence | Qualitative, quantitative, mixed methods | Opinions, perspectives, commentaries |
| Population | Involuntary migrants/forcibly displaced | Studies that do not include involuntary migrants either as the main population or as a sub-population of migrants |
| Intervention | HPV vaccination | Vaccination other than HPV vaccination |
| Outcomes | Health system determinants of delivery and uptake of HPV vaccination services among involuntary migrant populations | Studies that do not include evidence on HPV vaccination services |
| Language | English | Languages other than English |
| Context Forced displacement/ involuntary migration e.g., due to war, persecution, humanitarian crises Global goals/policies: Immunisation Agenda 2030; WHO 2022 Global Evidence Review on Health and Migration; Universal health coverage | |||
|---|---|---|---|
| 5As framework domains | WHO health system building blocks | Indicators of robust health systems | P3 model – health system influences |
| ■ access | ■ service delivery | ■ equity | ■ provider level |
| ■ awareness | ■ medicines/vaccines | ■ quality | ■ patient level |
| ■ acceptability | ■ information systems | ■ resource mobilisation | ■ practice level |
| ■ acceptance | ■ finance | ■ high immunisation coverage | |
| ■ activation | ■ health workforce | ■ social/financial risk protection | |
| ■ leadership/governance | ■responsiveness | ||
| Author/year | Design | Classification of migrants | Home countries/region(s) | Host countries | Actors e.g., providers, patients, caregivers |
|---|---|---|---|---|---|
| Allen et al., 2019 | Qualitative | Refugees | Somalia | USA | mothers |
| Badre-Esfahani et al., 2020 | Cohort | Involuntary vs. voluntary migrants | Central Asia, SE Asia, SSA, Latin America, Western countries; Turkey, Iraq, Lebanon, Pakistan, Afghanistan, Somalia, Iran, Morocco | Denmark | women |
| Berman et al., 2017 | Cohort | Refugees | Predominantly Iraq, Bhutan Somalia & other SSA | USA | Adolescent males and females (9-26 years) |
| Bhatta et al., 2020 | Cross-sectional | Refugees | Bhutan | Nepal | women |
| Burke et al., 2015 | Qualitative | Refugees | Cambodia | USA | mothers |
| Dalla et al., 2022 | Cross-sectional | Refugees | Syria | Greece | women |
| Davidson & Fisher, 2025 | Qualitative | Refugees and asylum seekers | Myanmar, Iraq, Syria, Iran, Sri Lanka, Colombia, Indonesia, Lebanon, Malaysia, Togo, Pakistan | Australia | women |
| Do et al., 2009 | Qualitative | Refugees/migrants | Cambodia | USA | parents and community leaders |
| Elmore et al., 2021 | Cohort | Refugees | Afghanistan, Bhutan, Burma, Colombia, DRC Congo, El Salvador, Eritrea, Iran, Iraq, Moldova, Nepal, Syria, Russia, Sudan, Syria, Ukraine | USA | women |
| Gebre et al., 2021 | Cross-sectional | Refugees/migrants | Somalia and Mexico | USA | women |
| Ghebrendrias et al., 2021 | Qualitative | Refugees | Sudan, Somalia, Kenya, Ethiopia, Eritrea, Congo, Uganda, Syria, Iraq, Egypt, and Morocco | USA | women |
| Kenny et al., 2021 | Cohort | Refugees | Burma | USA | adolescent females (11-26 years) |
| Kepka et al., 2018 (see Lai sequel study) | Mixed Methods | Refugees | Burundi, Congo, Rwanda, Liberia, Tanzania | USA | Parents, legal guardians, caregivers |
| Khan et al. 2023 | Qualitative | Migrants including refugees | Refugees from West Asia; migrants from South and Southeast Asia | Canada | parents |
| Kmeid et al., 2019 | Cross-sectional | Refugees | Syria | Lebanon | Parents and legal guardians |
| Lai et al., 2017 (see Kepka sequel study) | Mixed Methods | Refugees | Burundi, Congo, Rwanda, Liberia, Tanzania | USA | Parents, legal guardians, caregivers |
| Lee et al., 2016 | Cross-sectional | Refugees | Cambodia | USA | mothers |
| McComb et al., 2018 | Qualitative | Immigrants including refugees | Africa, Asia, South America | Canada | women (16-26 years old) |
| Metusela et al., 2017 | Qualitative | Refugees/migrants | Afghanistan, Iraq, Somalia, Sudan. Sri-Lankan (Tamil), Indian (Punjabi), South, South America (Latina) Sudan |
Canada & Australia | women |
| Moller et al., 2018 | Cohort | Refugees | Afghanistan, Asia, Eastern Europe (incl. Bosnia-Herzegovina, former Yugoslavia Middle East and North Africa (incl. Iraq, Stateless Palestinians) SSA (incl. Somalia) | Denmark | adolescent females |
| Napolitano et al., 2018 | Cross-sectional | Refugees/immigrants | mainly SSA (64.5%), East Europe, South Asia, North Africa, South America, Central Asia | Italy | adolescent females (12-26 years) and parents |
| Nyanchoga et al., 2021 | Cohort | Refugees and asylum seekers | 42 countries - listed ones: Middle East (Afghanistan, Iran, Iraq); Asia (Myanmar, India, Pakistan, Sri Lanka); SSA (DRC, Eritrea, Ethiopia, Kenya, Somalia, Sudan); Papua New Guinea, Solomon Islands | Australia | children, adolescents and adults |
| Riza et al., 2020 | Cross-sectional | Involuntary vs. voluntary migrants | Middle East incl. Syria, Afghanistan, and Iran; SSA incl. Nigeria, Ethiopia, Cameroon, and Kenya; Eastern European countries incl. Albania, Bulgaria and Georgia | Greece | women |
| Rubens-Augustson et al., 2019 | Qualitative | Immigrants including refugees | Not given | Canada | health providers |
| Salad et al., 2015 | Qualitative | Refugees | Somalia | Netherlands | women |
| Snoubar et al., 2025 | Cross-sectional | Refugees | Iraq, Palestine, Syria, Yemen | Türkiye | women |
| Wilson et al., 2021 | Mixed Methods | Immigrants including refugees | SSA (36%); MENA (58%); Other (6%) | Canada | adolescents (16-27 years) and caregivers |
| Building Blocks | Enablers (+) | Impediments (-) |
|---|---|---|
| 1. Leadership/ governance |
1.1 policies prioritising migrants’ health needs | 1.1(a) HPV vaccination policies not implemented in some countries |
| 1.2 decentralised governance and variations in immunisation policy implementation | 1.2(a) decentralised governance and variations in immunisation policy implementation | |
| 1.3 governments as gatekeepers in migrant-inclusive immunisation policy implementation | ||
| 2. Service delivery AND Medicines/ Vaccines |
2.1 school-based HPV vaccination programs | 2.1(a) no HPV vaccination program available |
| 2.2 supplementary catch-up vaccination | 2.2(a) HPV vaccination available in NIP but as voluntary routine not mandatory routine vaccination | |
| 2.3 migrant-targeted interventions | 2.3(a) health messaging targets limited audience | |
| 2.4 integrated services | 2.4(a) limited access e.g., schools, holding camps, eligibility based on legal status | |
| 2.5 public-private partnerships |
||
| 3. Health workforce |
3.1 health provider recommendation | 3.1(a) no health provider recommendation |
| 3.2 health provider main source of HPV vaccination-related information | 3.2(a) health provider time constraints – limited time to discuss HPV vaccination | |
| 3.3 vaccine administration (including consent) | 3.3(a) health provider reticence to recommend vaccination | |
| 3.4(a) health provider inadequately trained to serve migrant populations | ||
| 4. Health information systems |
4.1 electronic health databases with migrants’ records (including immunisation data) | 4.1(a) no vaccination records available for migrant populations |
| 4.2(a) no centralised or synchronised electronic databases with migrants’ immunisation data | ||
| 5. Financing |
5.1 HPV vaccination free for all (including migrants) via NIPs and other support programs | 5.1(a)cost for ineligible, partially covered and uninsured migrants |
| Determinants of uptake (5As) | Enablers (+) | Impediments (-) |
|---|---|---|
| 1. Access | 1.1 easy access/convenience | 1.1(a) legal status |
| 1.2 navigating language barriers | 1.2(a) unfamiliarity with host country’s health care system | |
| 1.3(a) language barriers | ||
| 2. Affordability | 2.1 free vaccination |
2.1(a) cost prohibitive |
| 2.2 willingness to vaccinate |
||
| 3. Awareness and Acceptance | 3.1 adequate knowledge about HPV vaccination: ■ culturally appropriate health promotion materials and forums ■ information sources |
3.1(a) low/lack of knowledge about HPV vaccination: ■ language barriers ■ misinformation ■ mistrust of governments’ intentions ■ living conditions |
| 3.2 framing/perception of HPV vaccination: ■ protective and/or preventive ■ a western disease |
3.2(a) concerns about long term effects and effectiveness of vaccine | |
| 3.3 length of stay in host country | 3.3(a) length of stay in host country | |
| 3.4(a) sociocultural and religious attitudes, beliefs and practices ■ sex deemed a taboo topic ■ allowing HPV vaccination is endorsing pre-marital sex and promiscuity ■ young girls are not sexually active ■ preference for traditional medicine |
||
| 4. Activation | 4.1 health provider recommendation | 4.1(a) health provider reticence to recommend HPV vaccination |
| 4.2 women’s agency and family support | 4.2(a) mothers’ disapproval | |
| 4.4 assumption that HPV vaccination is compulsory | 4.4(a) preventive care not prioritised | |
| 4.5 incentives |
| Health system performance indicators | Practice-level influences | Provider-level influences | Patient-level influences | WHO building blocks/delivery determinants | 5As of uptake |
|---|---|---|---|---|---|
| Equity | Delivery: enabler - policy adaptation and implementation to include migrants | Delivery: enabler - policy implementation to include migrants impediment - differential implementation (exclusion of certain migrant sub-populations) |
Uptake: enabler - easy, convenient, free access impediments – access contingent on legal status, language, knowledge/awareness-related barriers |
Leadership/ governance/ policy |
Access Affordability |
| Quality | Delivery: enabler - updated, synchronised electronic health databases with migrants’ immunisation records impediment – no records of migrant immunisation data |
Delivery: enablers – public private partnerships impediments – health provider time constraints, limited/lack of training, reticence to recommend HPV vaccine |
Delivery: impediments – no records of migrant immunisation data (could result in under- and/or over-immunisation) | Health information systems Service delivery Medicines/vaccines |
Access Awareness |
| Resource mobilisation | Delivery: enablers – school-based programs, supplementary catch-up, migrant-specific interventions, integrated services | Delivery: enablers – school-based programs, supplementary catch-up, migrant-specific interventions, integrated services | Delivery: enablers – school-based programs, supplementary catch-up, migrant-specific interventions, integrated services | Service delivery Medicines/ vaccines |
Access |
| High immunisation coverage | Delivery: enablers – public private partnerships Uptake: enablers – culturally appropriate health messaging |
Delivery: enablers – public private partnerships, health provider recommendations; impediments – no health provider recommendation | Uptake: enablers - easy, convenient, free access, health provider recommendation, incentives impediments – difficult to access, socio-cultural beliefs |
Service delivery Medicines/vaccines Health workforce |
Access Awareness Acceptance Activation |
| Social/financial risk protection | Delivery & uptake: enabler – free HPV vaccine regardless of legal status impediment – HPV vaccine cost partially covered or at own cost |
Delivery & uptake: enabler – free HPV vaccine regardless of legal status impediment – HPV vaccine cost partially covered or at own cost |
Delivery & uptake: enabler – free HPV vaccine regardless of legal status impediment – HPV vaccine cost partially covered or at own cost |
Health financing | Affordability Access Awareness |
| Responsiveness | Delivery: impediment – health promotion materials in English are not understood | Uptake: enablers – health provider recommendations, framing HPV vaccination as protective impediments – no health provider recommendation, limited/lack of training, reticence to recommend HPV vaccine |
Uptake: enablers – health provider recommendations, framing HPV vaccination as protectiveUptake: impediments – language barriers, mistrust of host country governments, misinformation, no health provider recommendation, under-prioritisation of preventive care | Service delivery | Access Awareness Acceptance Activation |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



