Submitted:
23 September 2025
Posted:
23 September 2025
You are already at the latest version
Abstract
Vulvovaginal candidiasis (VVC) affects around three quarters of women at least once in their lifetime. Around 10% of these women will experience prolonged or recurrent vulvovaginal candidiasis (RVVC) which fails to respond despite following recommended therapy. Most commonly prescribed therapy involves suppression therapy for usually two weeks which aims at eliminating symptoms by frequent administration of antifungals, followed by maintenance (weekly / monthly) therapy for up to six months. However, following cessation of maintenance therapy, around 50% of these women experience relapse. The vaginal ecology of RVVC can be characterized and it is thought that biofilms and/or the development of antifungal resistance prevent adequate resolution. However, hypersensitivity may also confound management. This review examines the management of VVC and the challenges of current prolonged antifungal therapy. It remains important to investigate the microbiological findings in RVVC and how these may inform rational choices in therapy in an era of rising antimicrobial resistance. Hope exists that studies of the vaginal microbiome highlight that the type of microbiota present may influence the level of inflammation and reduce symptomatology. Future research will continue to explore whether a personalized medicine approach can promote healthy vaginal ecology and prevent the debilitating long-term effects of RVVC.
Keywords:
vaginal candidiasis
; vaginal microbiome
; management recurrent vulvovaginal candidiasis
; community state types
1. Introduction
Vulvovaginal candidiasis (VVC) is estimated to affect at least 70-75% of females sometime during their reproductive life [1] and is uncommon in post-menopausal women unless exogenous estrogen is prescribed [2]. Colonization of the genital area with Candida may be asymptomatic, but some women can experience clinical manifestations including itching, particularly in the vulva area, a curd-like discharge, and stinging or burning on micturition. Oral antibiotics, diabetes, use of hormone therapy and pregnancy has been associated with genital candidiasis in women. Treatment is often initiated by the patient as there are topical and oral anti-fungal medications available without prescription in Australia. For most women, symptoms resolve spontaneously or with anti-fungal treatment.
However, women may present to general practitioners (GPs) when symptoms are prolonged or recurrent. For some women this may entail several visits to the GP and failure to eradicate symptoms despite using recommended therapy, which involves ‘suppressive and maintenance therapy,’ usually for up to six months [3]. Using this therapy, at least 50% of women may experience recurrences once treatment finishes. With failure of mainstream management, the impact on women’s lives can be significant [4,5] and many women seek alternative methods of management [6], which may be independent from or as an adjunct to, mainstream management [7]. The issue then becomes, how do we manage cases of recurrent vulvovaginal candidiasis (RVVC) which can have wide-ranging impacts on the life of sufferers?
RVVC has been arbitrarily defined as four or more episodes of vulvovaginal candidiasis per year and has been reported in up to 9% of sufferers [8,9]. Based on this percentage, Willems et al. [10] estimates that worldwide it would cause around 140 million cases annually. There are several theories for why RVVC occurs in immunocompetent patients. One of these includes relapse or reinfection with the same initiating strain [11]. This may be due to failure to clear the original infection due to the formation of antibiotic impermeable biofilms [12] or the development of antifungal resistance [13]. In other patients it is hypothesized that there may be other factors such as hypersensitivity resulting in symptoms such as itching in the absence of a curd-like discharge or microbiological confirmation of the overgrowth of candida [14]. However, in the majority of cases, no causative factors can be identified [2].
2. The Etiological Agents of VVC
Vaginal candidiasis often presents with pathognomonic symptoms (curd-like discharge, intense itching) different to those of trichomonas vaginitis (green frothy copious discharge) and bacterial vaginosis (grey, malodourous copious discharge). The curd-like discharge is attributed to the overgrowth of Candida spp. on the vaginal walls, but this overgrowth in itself may not be the primary explanation for the intense itching that is also experienced. This is attributed to the inflammatory response and may be unrelated to the numbers of candida organism present [15]. It is also not currently possible to determine if isolated yeast are colonizing rather than causing symptoms, as asymptomatic carriage occurs in 15 – 20% of women [16]. When symptoms do occur, yeast may not be the causative agent [1]. Microscopy demonstrating yeast may aid with diagnosis however microscopy is relatively insensitive thus women with symptoms of VVC should have a fungal culture performed to confirm diagnosis [17].
In the past it has been reported that around 85-90% of these infections are attributed to the one species of yeast, Candida albicans [18]. However, this may vary with the geographical area (Table 1), the year of study [19] and the study methodology e.g., isolation methods that do not use chromogenic medium are more likely to miss mixed cultures [20]. Most studies included in Table 1 describe polyfungal populations having more than one species of yeast isolated in up to 10% of patients studied. Some studies include patients stratified into those with or without RVVC whilst in other studies this is not described (Table 1).
A common theme emerging from the literature and shown by Ratner et al. [21] is that non-albicans Candida (NAC) are increasing in frequency and since these species have higher rates of fluconazole resistance, they are expected to be seen in many patients with RVVC. As many antifungal medicines are available without a prescription, lack of adequate antifungal stewardship may result [22]. This lack of antifungal stewardship both in the use of antifungal agents to control human, animal and crop diseases, as well as its use as an anti-fouling agent and in the preservation of timber, is a risk to the further development of resistance in healthcare isolates [23]. Additionally, tolerance to antifungal drugs and persistence has been described for yeast isolated in VVC [24], thus routine laboratory testing of antimicrobial resistance will fail to describe when this is leading to treatment failure.
Isolation of the yeast is important to confirm the clinical diagnosis of candidiasis [25] although it does not distinguish between colonization and causation of symptoms. With the popularity of diagnosis of STI using molecular tests, some molecular testing platforms also include the detection of yeast DNA. As examples, Navarathna et al. [26] and Lillis et al. [27] include testing for yeast in their molecular vaginitis testing but did not attempt to obtain clinical specificity for candidiasis.
Different methods of identification can also yield different descriptions of the etiological agents. The gold standard for identifying yeast would be nucleotide sequencing [28] however this is expensive and not practical for most diagnostic laboratories. As candida specific agars have widespread use, many laboratories will report species based on the appearance on chromogenic agars such as those compared by Scharmann et al. [29]. Caution should be taken with studies that report species level identification using only chromogenic agar medium. Souza et al. [30] showed that the chromogenic agar they used misidentified Pichia kudriavzevii (formerly Candida krusei) and reported on two other studies that found similar. It has also been reported that chromogenic agars may misidentify Nakaseomyces glabratus (formerly Candida glabrata) [31]. We have found that some batches of chromogenic agar may be inhibitory to low numbers of N. glabratus in clinical samples (unpublished data) and thus in a previous trial involving the isolation of yeast from VVC [32], Saboraud’s dextrose agar was used as a second medium to confirm the absence of yeast in samples. The advantage of chromogenic agars for yeast isolation is that it helps with the identification of mixed yeast cultures as the colonial morphology on non-chromogenic medium may be insufficiently different to identify mixtures of species.
In larger laboratories automated methods for identification of microbes such as Vitek 2 systems (which can also perform susceptibility testing) [33,34] and analyzers to perform mass spectrometry using MALDI-ToF (matrix-assisted laser desorption ionization combined with time of flight) provide excellent accuracy of speciation of the most commonly isolated yeast [35].
In a systematic review of VVC that included 39 studies that met the inclusion criteria, the percentage of infections attributed to C. albicans compared to non-albicans Candida (NAC) was found to range from 39% to 88% [36]. To illustrate this, we have compiled a summary of reports 2021 - 2025 that use chromogenic agar for isolation of yeast and confirmed their identity using either MALDI-ToF or sequencing to describe the most prevalent species reported in patients with clinically diagnosed VVC (Table 1). As NAC are more resistant to the most commonly prescribed group of antifungal drugs (the azoles) (reviewed in Gonçalves et al. [37]), it is important to perform microbiological confirmation of the etiological agent of VVC. As an example of the types of resistance that can be seen, Aboagye et al. [38] found in patients attending an antenatal clinic that less than 50% of the C. albicans isolates were sensitive to fluconazole and itraconazole. Of concern is that Kroustali et al. [39] reported that 36.5% of their isolates were Candida parapsilosis and recently it has been reported that this species is becoming increasingly multi-resistant [40]. It has been shown that the availability of over-the-counter antifungal agents has been linked to inappropriate use [41]. Thus, more needs to be done to promote antifungal stewardship to slow the rise of multi-resistant fungal pathogens, although the widespread availability of antifungal agents that do not require prescriptions make this proposal challenging.
A limitation of studies describing the etiological agents of VVC is that isolation of a yeast does not necessary imply that the organism is the causative agent of the symptoms. Nor does a negative culture rule out the possibility of VVC. To understand the current limitations of testing it is necessary to understand host factors such as the immune response and also the microenvironment of the vagina.
3. The Role of Inflammation in the Host Response
3.1. Early Steps in Infection
VVC can manifest in varying degrees of severity, from asymptomatic to mild symptoms that resolve spontaneously, to more severe forms of the condition which require active management. Sometimes management is tailored according to symptoms experienced and duration of symptomatic episodes [48]. Some authors differentiate between chronic and recurrent VVC because management may differ. Recurrent VVC is generally defined as four or more symptomatic episodes of VVC in a 12-month period [8,9,49]. Chronic VVC may be characterized by prolonged / continuous symptoms [50], while RVVC may be episodic or cyclical [51]. Some authors propose that species isolated from women with RVVC demonstrate less virulence than from those with acute / non-recurrent VVC [52], while other authors consider the severity of symptoms that may occur with both chronic and acute VVC. The severity is thought not to be due to virulence of the yeast but rather the host inflammatory response to the presence of yeast. It is possible that there is no neat delineation between acute, chronic and recurrent VVC, and that overlap may complicate the distinction among these categories. An alternative categorization can be demonstrated in Figure 1.
The first step in initiating inflammation on the vaginal walls in the case of C. albicans is thought to be the switching from the budding form to a form producing hyphal growth that aids in the anchoring and ingress into the epithelial layer of the yeast cells [53]. This is followed by the expression of numerous adhesins and extracellular proteins that will form a matrix and a host immune response is then initiated with the production of cytokines and anti-microbial peptides by epithelial cells [54]. The active form of these pro-inflammatory cytokines needs to be produced through activated cellular inflammasomes and is tightly regulated [55]. This activation is highly inflammatory and leads to cell death, a state called pyroptosis [56]. The sensitivity of the epithelial cell response is thought to be variable enough to enable discrimination between harmless carriage and when an inflammatory response is required due to epithelial cell damage [54]. Moyes et al. [54] comments that the work of Fidel at al. [15] demonstrate, in a human vaginal challenge experiment, that women with RVVC had higher sensitivity to fungal burdens than those without RVVC.
3.2. Internalisation by Macrophages and Subsequent Escape
Activation of inflammasomes is through host-cell receptors’ interactions with the outer cell-wall components of yeast which leads to internalization of the fungus (reviewed in Camilli et al. [55]). When C. albicans is internalized by macrophages, it can survive and continue to grow its hyphal forms and destroy the macrophage [57]. This phenomenon is also seen in the two other Candida spp. that produce hyphal growth, C. dublinensis and C. tropicalis [58] and to a lesser extent in C. parasilosis [59]. Host cell death is also aided by the production of toxins including candidalysin [60]. For those yeast that escape through hyphal-mediated mechanisms, neutrophils attracted to the inflammatory products then attempt to control the fungal infection through the release of neutrophil extracellular traps (NETs) that are composed of neutrophil chromatin and antimicrobial peptides [61]. This activity will be impaired however if the yeast are successful in forming a protective biofilm which is now recognized to be important in yeast survival in RVVC [62].
NAC are also able to survive inside macrophages [63,64] and produce pro-inflammatory cytokines leading to inflammation [65] and in the case of N. glabratus, these cells may enter a dormant state called persister cells [66]. This is thought to explain why in many studies the proportion of isolations of N. glabratus increases in RVVC (Table 1). Although intracellular survival has not yet been demonstrated for C. parapsilosis, they have been shown to have the ability to develop tolerance and resistance to fluconazole and form biofilms [40] which may explain the increased isolation for this species (Table 1).
3.3. The Influx of Neutrophils
With the failure of macrophages to destroy the yeast, an influx of neutrophils occurs which is also in part mediated by the candidalysin produced in the early stages of hyphal growth [67] and the pro-inflammatory cytokines produced by inflammasomes. Interestingly, the NAC that also produce hyphal growth (C. dublinensis and C. tropicalis) had less induction of the gene encoding candidalysin [68]. Willems et al. [68] also reported less inflammation in their VVC murine model infected with NAC. The importance of neutrophil recruitment into the vaginal lumen for the major manifestation of inflammation was demonstrated by Fidel et al. [15]. In this seminal experiment of intravaginal inoculation of C. albicans into two groups of women (one naïve to VVC and the other, infrequent sufferers of VVC), 15% of women with no history of VVC acquired symptomatic infection compared to 55% of the group who had previously experienced VVC. They also showed that symptomatic response was associated with an influx of neutrophils and increased yeast burden.
3.4. The Role of Adaptive Immunity
The adaptive immune responses that follow the primary innate response has been reviewed by Netea et al. [69]. They outline that in this arm of immunity it is the dendritic cells that signal to T helper 1 cells that are important for activating macrophage and neutrophil killing of yeast. Richardson et al. [70] reviews the evidence that memory does occur in the innate immune response as it has been shown that monocytes exposed to Candida can undergo a reprogramming such that they produce increased amounts of inflammatory cytokines on their next exposure.
3.5. VVC as an Immunopathology
This failure of both macrophages and neutrophils to kill yeast in the early stages of infection and the resulting inflammation is thought to explain why VVC is considered an immunopathology. This has been reviewed by Yano et al. [71]. Host genetic variation in genes contributing to host defence is thought to explain a small subset of those experiencing RVVC [72]. Diabetes does compromise the host’s ability to control the growth of yeast on mucosal surfaces [73] and with the rising incidence of diabetes this would be expected to lead to more mucosal infections needing treatment.
The evidence for whether VVC can be thought of as a failure of the adaptive immune response has been reviewed by Peters et al. [74]. It is known the patients with cell-mediated immunity (CMI) deficiency are susceptible to mucosal candidiasis [75]. Rosati et al. [72] reviews that current evidence fails to clarify whether adaptive immunity plays a significant role in protection from RVVC as patients with CMI deficiency are no more susceptible to VVC than those who are immunocompetent. Additionally, Wozniak et al. [76] were unable to demonstrate a definitive protective role for antibodies in a mouse vaginitis model.
Significantly in some women who suffer from vulvovaginitis, very few yeast are isolated or it can be difficult to isolate yeast [77]. The first reports suggesting that this symptomatology could be linked to hypersensitivity to Candida were reported in the 1970s [78,79] and this was followed by Witkin et al. [80] who measured elevated IgE in vaginal fluid from some women with this possible hypersensitivity disorder. Bernstein et al. [14] have reviewed the evidence for hypersensitivity to Candida and report that women who are treated with immunotherapy show improvement in symptoms but conclude that studies are required involving double blind placebo trials and further studies into the mechanisms of this possible hypersensitivity need to be performed.
3.6. Opportunities to Mitigate Against Immunopathology
It is possible that different microbial members of the vaginal microenvironment can modulate the local immune response. Niu et al. [81] investigated the use of one strain of lactobacilli (Lactobacillus crispatus American Type Culture Collection 33820) and found that it could ‘attenuate the virulence of C. albicans, modulate the secretion of cytokines and chemokines, and enhance the immune response of VK2/E6E7 cells in vitro’. This study points to important directions for future research to determine whether probiotics and their composition can reduce hypersensitivity in individuals with RVVC.
The response by the host that leads to symptoms in VVC is a localized response rather than systemic [81]. In fact, Fidel et al. [15] showed that in healthy women challenged intra-vaginally with yeast, symptoms were linked with the presence of inflammatory cells rather than their absence. This has been corroborated by the work of Giraldo et al. [82].
Efforts to improve the localized vaginal immune response have been reported by Ricchi et al. [83]. They used a bacterial lysate to stimulate an in-vitro cell culture of human vaginal epithelial cells to increase production of mitochondrial reactive oxygen species. They also used this lysate to stimulate murine macrophages to improve phagocytic killing of C. albicans. It is unknown however whether such stimulation will reduce the recurrence of VVC.
Considering the burden of RVVC being around 8% of women who have experienced VVC, a vaccine to prevent VVC would be welcome. In the light of the virulence traits of hyphal producing Candida, it is hoped that efforts directed to producing neutralizing antibodies to the proteins generated during invasion could lead to protection in some women [84].
Currently there are no approved fungal vaccines [85]. Several vaccines targeting candidiasis are in development or undergoing trials [86,87,88,89,90,91]. Wychrij et al. [85] have reported that their pan-fungal vaccine (based on a peptide conserved in many yeast species), NXT-2, reduced inflammation and provided antibody-mediated protection in a murine model of VVC. Edwards at al. [89] have evaluated the effects of administration of their trial vaccine to 178 women with RVVC. They measured B- and T-cell responses after 1 intramuscular dose. They found immune responses that resulted in a statistically significant number of women experiencing less recurrent symptoms and will continue to further develop their vaccine and guidance for administration. Considering that a subset of these women may be experiencing symptoms due to hypersensitivity rather than overt infection with C. albicans, it will be of great interest to see if a registered vaccine that prevents the initial onset of RVVC is also able to reduce the number of women who go on to develop hypersensitivity. The vaccine designed by Edwards et al. [89] uses a protein from the hyphal tip of C. albicans to elicit immunity. An alternative immunogen reported by Wychrij et al. [85] aims to protect against a wider range of fungal species, which at first glance may seem to hold more promise against the wider range of species reported in RVVC. However, a successful vaccine will reduce the number of women experiencing VVC and thus those going on to develop RVVC and also reduce the pressure towards evolving fungal resistance.
4. The Impact of Biofilm Formation in VVC
Microbial cells can exist freely in solution (a state known as planktonic) or in close association with other cells including those of different species and held together by an extracellular matrix forming what is known as a biofilm. These biofilms help protect the enmeshed microbial cells including yeast from the immune system and antimicrobial drugs [92,93].
It is possible that certain strains of bacteria are able to produce molecules that moderate the action of other microbes growing in the surrounding milieu. Hu at al. [94] have shown that Lactobacillus strains produce metabolites that inhibit the growth of C. albicans. It has also been shown that Lactobacillus crispatus exerts growth inhibition on C. albicans and that women who have a predominance of L. crispatus in their vaginal flora are less likely to have C. albicans in their vaginal microbiota [95]. Parolin et al. [96] have shown that a variety of Lactobacillus species were able to inhibit hyphal formation in yeast and impair biofilm formation. Also, it has been shown that butyrate [97] and allicin from garlic [98] are able to downregulate the production of pseudohyphae in C. albicans.
Donlan [99] notes in a review of biofilms, that microbial cells in biofilms exhibit altered behaviors, including reduced growth rates and differential gene expression. Some of the biofilm-associated genes have been shown to be expressed at higher levels in isolates from patients with RVVC compared to healthy controls [100]. These reduced growth rates and the presence of matrix is thought to impair the efficacy of antimicrobial treatment [62]. Biofilm formation has also been shown to help persistence of candida cells leading to RVVC [62]. Another physiological state that is produced by Candida spp. during biofilm formation is the formation of extracellular vesicles which contribute to the biofilm matrix. These vesicles contain a variety of peptides of which some reports have been shown to be proinflammatory [65,101].
Although many species of bacteria are found within the vaginal microbiota, a study in 2011 found that 95% of the bacteria were lactobacilli [102]. Lactobacilli produce biofilms and recently the question of whether lactobacilli could inhibit the growth of C. albicans was examined by Giordani et al. [103]. They found that biofilm formation by C. albicans was inhibited in a dose dependent manner by the exoplolysaccharides produced by certain lactobacilli and that the effect was stronger in Lactobacillus gasseri than Lactobacillus crispatus. Further to this, it is not only the species of lactobacilli that may be important but also the strain. Bae et al. [104] examined 18 strains of Lactiplantibacillus plantarum but only selected three based on their ability to inhibit the growth and biofilm formation of C. albicans and Gardnerella vaginalis. Additionally, these three strains also eliminated mature biofilm formation by C. albicans in their model.
Future studies should address whether the presence of biofilms containing yeast cells can be eradicated. As outlined above, certain Lactobacilli species can discourage biofilm formation. The inorganic acid Boric acid has been used in mainstream management of azole resistant RVVC [105]. Boric acid can interfere with biofilm formation and the hyphal transition development [106]. However, the elimination of established biofilm is more challenging [107]. What is not known in RVVC is whether specific treatments can help to eradicate established candida-containing biofilms. Wang et al. [107] have addressed this challenge by developing an anti-biofilm hydrogel with nanoparticles that enhanced the penetration and delivery of anti-biofilm signaling molecules in a mouse vaginal candidiasis model that resulted in reduced thickness of biofilm and less inflammation. It will be important to combine these novel therapeutic modalities with probiotics such as the anti-biofilm species mentioned above.
5. Clinical Management of VVC
5.1. Initial Evaluation
At the outset, it is recommended to gain mycological evidence of candida colonization, although due to the daily fluctuations in vaginal colonization of candida, a negative swab result does not always rule out RVVC [108]. Ruling out other conditions such as sexually transmissible infections, or skin conditions causing itching such as lichen sclerosis is also important.
5.2. Management of RVVC
Mainstream management of RVVC usually consists of suppressive and maintenance treatment with oral or topical antifungals (see Table 2), following mycological confirmation on at least one occasion [2]. This is the only method of management supported by a multicenter randomized controlled trial [49] and remains the most widely recommended method of management according to national and international guidelines [51,109,110,111]. However, advising women that this will cure them could be unrealistic, as 50-80% of women undergoing treatment for RVVC will experience recurrences after the maintenance therapy has ceased [3,112].
5.3. Antifungal Agents Used in VVC
There are a number of oral and topical azoles used in management of vulvovaginal candidiasis. Azoles consist of imidazoles (e.g. clotrimazole, miconazole and butoconazole), triazoles (e.g. fluconazole, itraconazole and voriconazole) and tetrazoles (oseconazole) [113]. Table 2 lists the azoles most recommended in some clinical guidelines, but other azoles may also be used.
The use of boric acid in suppression and maintenance therapy has not been evaluated in randomised controlled trials for recurrent vulvovaginal candidiasis. It has been documented for use in non-albicans infections; however, there are concerns regarding its impact on vaginal microbiota. It is often available in compounding pharmacies and is not considered safe during pregnancy.
Fluconazole, a triazole, is most commonly used for suppression and maintenance therapy due to its tolerability, accessibility and cost [114]. Gupta et al. [115] outlines the various side-effects and drug interactions associated with fluconazole. Side-effects such as headache, nausea, stomach pain and rash are generally mild and occur in less than 1:100 people. However, rarely hepatotoxicity can occur with patients with underlying liver conditions and liver function tests are recommended with this group. Other disease interactions include QT prolongation, usually in patients with multiple comorbidities. Fluconazole can also interact with other medications to potentially cause serious side- effects, and care (increased monitoring or dose adjustment) is needed when prescribing fluconazole long-term. Potentially harmful interactions include the blood thinner warfarin, some statins, amiodarone, a common anti-platelet medication clopidogrel, phenytoin and antidepressants such as citalopram.
Older azoles such as itraconazole [116] are not usually recommended as first-line treatment with RVVC due to more frequent dosing needed, and the comparative efficacy of fluconazole.
Donders et al. [48] report that individualized, reducing doses of fluconazole if symptom free over a 12-month period may prevent clinical relapses for women experiencing recurrent vulvovaginal candidiasis. In this study, 117 women started with a loading dose of fluconazole 600mg in the first week, and then for two months took 200mg twice weekly, followed by 200mg every two weeks for four months, then 200mg monthly for six months, according to their individual response. Of the women that commenced the trial and achieved mycological and symptom cure after induction, 90% were disease free after six months and 77% disease free after 12 months (however, only 36 completed the full treatment protocol and final follow-up visit). Of note with this study is the variety of response and fluconazole doses needed to eliminate symptoms and mycological evidence of candida (women were categorized into optimal, sub-optimal and poor responders).
There is no consensus about whether oral or topical therapy is superior in efficacy. One systematic review suggested no difference in efficacy of oral versus topical anti-fungal treatment in VVC [117], and a more recent systematic review concluded that neither method demonstrated superiority in reduced recurrences at six months [118].
Expert consensus concludes that there is rising evidence that women on long-term suppressive therapy may be susceptible to developing resistance to future suppressive regimens [112]; hence change of therapy or increasing strength of therapy may be indicated, although new therapeutic options are urgently needed [119].
5.4. New Drugs on the Horizon
A novel tetrazole with similar side-effects profile to fluconazole, (oteseconazole) has been approved for use in the USA, as well as ibrexafungerp, a triterpenoid-glucan synthase inhibitor, which may be effective against isolates resistant to fluconazole [120] but approval in other countries is pending. Oteseconazole has a long elimination half-life of 138 days [113] and was found to be 40 times more effective against most Candida spp. It also showed promise, in clinical trials, against fluconazole resistant C. albicans [121]. These therapies have not been included in the most recent clinical practice guidelines, and regimens vary.
New topical treatments are the subject of clinical trials [122]. Sertaconazole shows similar efficacy to clotrimazole [123]. Olorofim, an orotomide (primarily for Aspergillus infections) and fosmanogepix (Gwt-1 inhibitor which may be useful with azole resistance) are expected to be approved by FDA in coming years [121]. Other novel antifungals are also in phase 11 & 111 trials but are primarily used for systemic fungal infections in immunocompromised patients [121].
5.5. Management of VVC in Challenging Conditions
Some conditions pose additional challenges in the management of RVVC, as some therapies are not recommended in certain situations and sometimes, mainstream management may be ineffective.
- Pregnancy
Pregnancy hormones (particularly estrogen) can cause vaginal epithelial cells to become more susceptible to the adherence of candida. Increased vaginal secretion of glycogen can also promote fungal hyphae growth [124]. Topical rather than oral azoles are recommended in RVVC during pregnancy due to possible teratogenic effects of fluconazole [125,126] although some sources dispute this association [127]. Boric acid pessaries are not recommended. Polyenes such as Nystatin may also be used but are less popular due to their more frequent administration. Oral probiotics have not been shown to reduce recurrences of VVC in pregnancy in women with RVVC [128]. There may be a place for amphotericin lozenges inserted vaginally. Some studies show promise [129,130], although it is yet to be evaluated in large clinical trials.
- b. Diabetes
If diabetes is uncontrolled, increased vaginal glycogen can promote adhesion of candida in vaginal tissue [124]. Most management guidelines suggest that a longer period of treatment may be recommended for patients with diabetes, but few recommend specific management strategies for poor responders apart from checking for co-morbid dermatological conditions such as lichen sclerosis [114]. When blood sugar levels are well controlled in diabetic patients, they are less likely to experience flare-ups during anti-fungal therapy. However, certain medications for diabetes which prevent glucose reabsorption in the proximal tubule such as SGLT2 inhibitors can result in glucosuria, which can exacerbate VVC [9,114].
- c. Immunocompromise
Immunocompromised or critically ill patients are more likely to experience invasive candidiasis than healthy women, who are more susceptible to mucocutaneous infection such as vulvovaginal candidiasis [131]. More intensive therapy is usually recommended for immunosuppressed patients [124]. This may include higher doses or more frequent administration of anti-fungal agents.
- d. Fluconazole and other azole resistance
In women with fluconazole and other azole resistance, identification of species is recommended to guide management [131]. Alternatives to fluconazole include nystatin, boric acid, terconazole and amphotericin B vaginal pessaries or cream [113]. Itraconazole may be effective against many clinical isolates of C. parapsilosis, N. glabratus and P. kudriavzevii that are resistant to fluconazole but is less well tolerated [113].
- e. Co-existing infection with bacterial vaginosis
In some populations bacterial vaginosis (BV) and VVC may be linked, although the etiology of this is yet to be confirmed [49]. As management of bacterial vaginosis (BV) is usually with antibiotics, women with concurrent BV and RVVC face management challenges, as antibiotics are considered a predisposing factor for VVC [132]. Alternative management strategies could include boric acid pessaries which penetrates biofilm [106], however the efficacy has yet to be proven in randomized controlled trials. Early in-vitro studies with a biological bacteriostatic agent shows promise but is yet to be evaluated in randomized controlled trials [133].
5.6. Complementary and Alternative Therapies
Generally, the evidence for the use of complementary and alternative medicine (CAM) in genital candidiasis is not strong, although anecdotally many women report improvement of symptoms following use. Some clinical trials have shown promise with CAM such as propolis [134], Ageratina pichinchensis extract [135] and Allium sativum (garlic) [136]. Other clinical trials have found that, despite in-vitro efficacy, some natural products do not provide long-term relief for VVC. Sardi et al. [124] propose that the reason for this is that many of the biologically active constituents of these therapies are ineffectively absorbed. These constituents include flavonoids, tannins and terpenes.
Natural therapies include, but are not restricted to, dietary changes including probiotics and yoghurt; herbal supplements such as pau d’Arco; and Melaleuca alternifolia (tea-tree oil (which can result in irritation, burning and redness). Excess use of other alternative therapies may have systemic effects (e.g. bleeding with garlic) [137]. Where a woman finds relief with a particular alternative or complementary medicine, if it causes no harm, it should not be discouraged, as management should be individualized, whether mainstream or alternative.
6. The Influence of Vaginal Microbiota on Candidiasis Outcomes
6.1. Intestinal Carriage of Candida spp.
The intestinal tract is probably the source from which colonization of the vagina occurs initially [138]. Thus, it is worth considering whether efforts to lower intestinal carriage could prevent VVC. C. albicans has been reported in the intestinal tract of 83% of 695 healthy volunteers by Delavy et al. [139] who investigated the factors influencing the intestinal growth of C. albicans. They found that these factors were multifactorial whilst noting that eating between meals and a low sodium diet was linked to higher intestinal carriage. Of interest was the finding that other members of the host microbiota might be associated with lowered numbers of C. albicans in the intestine. They speculated whether this might be due to higher amounts of short chain fatty acids (SCFAs) produced in these individuals. The positive influence of SCFAs to produce beneficial outcomes in terms of C. albicans colonization has been reviewed by McCrory et al [140] who noted that inhibition of C. albicans growth and switching to the invasive hyphal form as well as down regulation of the surface molecules of yeast that communicate with immune cells. Nguyen et al. [97] have also reported that the SCFA butyrate (which is produced by intestinal bacteria) reduced biofilm formation and enhanced killing by fluconazole in both C. albicans and C. parapsilosis. It also increased macrophage phagocytosis rate and killing of internalised C. albicans.
The role of a high fiber diet in vaginal health, where the SCFAs produced in high fiber diets by intestinal bacteria may control the levels of yeast colonization and the behavior of yeast, may provide important insights. As more people realize the importance of resuming a high-fiber diet that has been lost in Western diets [141], it will be possible to perform large studies comparing the vaginal health history in those with and without a high-fiber diet. There is evidence that a diet high in animal protein derived from red and processed meat, as well as alcohol consumption is associated with less protective vaginal microbiota [142]. Further microbiome studies of the vagina coupled with vaginal health history and probiotic interventions should inform the rational use of probiotics.
6.2. The Importance of Community State Types
In healthy pre-menopausal women, the most predominant member of the local vaginal microbiota is Lactobacillus spp. [102]. Ravel et al. [102] reported that the vaginal microbiomes of 396 asymptomatic women could be characterized into five Community State Type groups (CST), of which four were dominated by different Lactobacillus species: Group I, L. crispatus (26.2% of women); Group II, L. gasseri (6.3%); Group III, L. iners (34.1%); and Group V, L. jensenii (5.3%). Group IV had lower numbers of lactobacilli and a higher proportion of anaerobic species and was found in 27% of women. Some similarities in groupings were reported a year later by Smith et al. [143]; however, only 10 women were included in their study. Kim at al. [144] reported on the CST groups of 40 women with recurrent vaginitis (etiology not determined) and found that 21 (52.5%) were classified as CST IV, eight (20.0%) for CST III, 5 (12.5%) for CST I, two (5.0%) for CST II, one for (2.5%) for CST V, and three (7.5%) for mixed CST, thus confirming the association of a shift in Lactobacillus species predominance in cases of recurrent vaginitis.
6.3. The Use of Probiotics to Improve Vaginal Health
Following on from this, one would expect positive outcomes for the use of oral probiotic supplementation or vaginal administration. However, studies of vaginal probiotic use should be scrutinized for choice of Lactobacillus spp. As an example Jepson et al. [145] published a study titled ‘Probiotic treatment with specific lactobacilli does not improve an unfavorable vaginal microbiota prior to fertility treatment - A randomized, double-blinded, placebo-controlled trial’ yet despite noting from their literature search that Koedooder et al. [146] reported the presence of L. crispatus was associated with greater fertility outcomes, they elected to use the less common species L. gasseri in their study. However, this finding may have also been linked to the choice of strain as Perez et al. [147] found that their strain of L. gasseri was superior to L. crispatus in its colonization ability. Consequently, much more work has been done on L. crispatus and France et al. [148] has reviewed aspects of L. crispatus, concluding that it makes a good candidate for probiotic use.
Tortelli et al. [95] has shown that in women whose lactobacilli were dominated by L. iners, there was a significant association with the presence of C. albicans, whereas conversely women predominantly colonized with L. crispatus had a significantly lowered association with C. albicans. They also found that in vitro, the cell-free supernatent of L. crispatus slowed the growth of C. albicans. This is interesting as L. iners has been associated with disease states, for example van Houdt et al. [149] showed that those with a vaginal composition predominated by L. iners were significantly more likely to be infected with chlamydia over a one-year period. Of additional interest is the finding by McKloud et al. [101] that an in vitro experiment where L. crispatus was co-incubated with a polymicrobial biofilm containing C. albicans resulted in decreased fungal burden in the biofilm over a 48-hour period.
What is less clear, however, is whether the presence of particular species or strains of lactobacilli exert an influence over whether symptoms will occur when Candida spp. grow and the way in which these species grow (switching to hyphal forms, expression of biofilm extracellular components). Evidence is beginning to emerge that it is not only the species of lactobacilli that is important but also the strain. As an example, Armstrong et al. [150] report that L. crispatus strain CTV-05 is able to reduce the recurrence of bacterial vaginosis. However, colonization by this strain is lost in half the women after three months [151].
Thus, assertions that because Lactobacilli are predominant in so many women with VVC that they must not be providing a protective effect, need to be questioned as in the past we have not had the opportunity to provide metagenomic analysis of the microbiome that reveals specific functional characteristics of particular strains. It will be important in the future to perform these metagenomic studies on those who have not experienced VVC or have recovered quickly from VVC and compare these findings to those who suffer from RVVC.
Moreover, as some women with RVVC experience symptoms due to hypersensitivity (described in Section 3: Role of inflammation), the question arises ‘Are some species of lactobacilli able to provide beneficial host immunomodulated responses?’ A reduction in inflammation is seen in women who have vaginal microbiota dominated by L. crispatus [152]. Gosmann et al. [152] also postulated that this reduced inflammation could explain why women with L. crispatus dominated vaginal microbiota had less infection with HIV due to the lowered presence of HIV’s target CD4 T cells. The potential for lowered inflammation and prevention of RVVC in women whose microbiota is predominantly L. crispatus should be explored. This should be followed by research to show whether lasting colonization of L. crispatus can be effected in women with microbiota predisposing to inflammation.
6.4. Efforts to Manipulate the Local Vaginal Microbiota
Transplantation of microflora from healthy donors has been used to ameliorate disease symptoms of the gut [153] and to improve health markers of obesity [154]. Recently vaginal microbiome transplants (VMT) have been performed to treat intractable bacterial vaginosis in five women [155] with repeated administration required in three and failure to resolve symptoms in one recipient. Building on these findings Wrønding et al. [156] showed proof of concept that donor material could be screened, stored and administered with lasting effects in a patient with repeated pregnancy loss and associated vaginal symptoms of bacterial vaginosis. The predominant species in the donor material was L. crispatus. Future studies should report on whether VMT in women with intractable RVVC leads to a lasting repopulation of L. crispatus and resolution of RVVC. Preparation of transplant material is onerous and not without health risks, so should only be performed for research purposes until sufficient evidence leads to regulatory approval.
Current interest has been focused on the use of L. crispatus containing probiotics to ameliorate conditions associated with genitourinary health. Liu et al. [157] reported that intravaginal administration of a healthy donor derived strain of L. crispatus (strain chen-01) was able to establish and reduce viral shedding load in human papilloma virus (HPV) infected women. Their work followed the finding that women with cervical cancer were less likely to have L. crispatus predominating in their vaginal microbiota [158]. Hemmerling at al. [159] report that intravaginal administration of L. crispatus was able to lower inflammation and shift microbiota to being lactobacillus predominant in a population of women at risk of HIV infection. El-Baz et al. [160] have performed in vivo experiments to lower group B streptococcal (GBS) colonization with the ultimate aim of effecting less GBS colonization of pregnant women and lowering the need for intra-partum administration of antibiotics. Ideally future studies will establish if L. crispatus can be administered daily with food such as yogurt to effect long-term colonization. An alternative approach has been proposed by Ravel et al. [161] where they combined three strains of L. crispatus to produce a multi-strain consortium with proven ability to inhibit growth of Gardenerella spp. and Candida spp. (C. albicans., C. tropicalis and C. parapsilosis). The formulation of the vaginal tablet also included substates to encourage the growth of the microbial cargo in a slow-release manner. In their trial they found a significant reduction of Candida spp. in the trial participants.
7. Conclusion
Broad principles of management can be applied with RVVC, as the evidence suggests that there is no ‘one size fits all’ approach that will cover every individual who experiences this condition. Management will be dictated by personal preference and tolerance of therapy (oral versus topical; mainstream versus alternative and complementary), individual host response to candida, co-existing diseases or health conditions, availability of antifungal treatment, immune factors, and a complex interplay of vaginal microbiota.
RVVC is a significant problem that is complicated by rising resistance to antifungal agents. In current guidelines, the recommended first-line management of this condition is prolonged antifungal treatment. Alternative considerations include a more nuanced approach to the treatment and monitoring of RVVC. This could involve describing a patient’s vaginal microbiome by sequencing and reporting the community state types present, although this approach is circumvented by widespread self-management due to ready availability of non-prescription antifungals, as well as challenges with health dollar budgetary constraints.
Current research indicates that Lactobacillus crispatus can exert a beneficial control on other organisms present in the microenvironment and reduce inflammation. Based on personalized descriptions of the vaginal microbiome, targeted probiotics could be selected and administered. Ultimately it is hoped that an effective vaccine may help to reduce the incidence of RVVC; however, there are still many challenges associated with its development as the strains of yeast causing RVVC are varied and ubiquitous. However, opportunities abound for research to continue to explore the various strains of beneficial resident vaginal lactobacilli, their administration and whether personalized medicine can move to a preventative phase where candida containing biofilms can be prevented rather than allowed to persist and promote inflammation. Finally, long overdue insights into vaginal ecology are beginning to be described as we move forward into a more positive era of the promotion of vaginal health.
Author Contributions
Conceptualization, D.G and C.J.W; writing—original draft preparation and editing, D.G. and C.J.W. Both authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors do not have any conflicts of interest
Abbreviations
The following abbreviations are used in this manuscript:
| BV | bacterial vaginosis |
| CAM | complementary and alternative medicine |
| CST | community state types |
| GBS | Group B streptococcal |
| GP | General Practioner |
| NAC | non-albicans Candida |
| SCFA | short chain fatty acids |
| RVVC | recurrent vulvovaginal candidiasis |
| VVC | vulvovaginal candidiasis |
References
- Sobel, J.D. Vulvovaginal Candidosis. Lancet 2007, 369, 1961–1971. [Google Scholar] [CrossRef]
- MSHC. Candidiasis (vulvovaginal) Treatment Guidelines. Melbourne Sexual Health Centre Guidelines. 2021. Available online: https://www.mshc.org.au/health-professionals/treatment-guidelines/candidiasis-vulvovaginal-treatment-guidelines (accessed on 4th June 2025).
- Sobel, J.D.; Wiesenfeld, H.C.; Martens, M.; Danna, P.; Hooton, T.M. , Rompalo, A.; Sperling, M.; Livengood, C. 3rd.; Horowitz, B.; Von Thron, J.; et al. Maintenance Fluconazole Therapy for Recurrent Vulvovaginal Candidiasis. N. Engl. J. Med. 2004, 351, 876–883. [Google Scholar] [CrossRef]
- Ehrström, S.; Kornfeld, D.; Rylander, E. Perceived Stress in Women with Recurrent Vulvovaginal Candidiasis. J. Psychosom. Obstet. Gynaecol. 2007, 28, 169–176. [Google Scholar] [CrossRef]
- Aballéa, S.; Guelfucci, F.; Wagner, J.; Khemiri, A.; Dietz, J.P.; Sobel, J.; Toumi, M. Subjective Health Status and Health-related Quality of Life Among Women with Recurrent Vulvovaginal Candidosis (RVVC) in Europe and the USA. Health Qual. Life Outcomes 2013, 11, 169–181. [Google Scholar] [CrossRef]
- Watson, C.J.; Pirotta, M.; Myers, P. Use of Complementary and Alternative Medicine in Recurrent Vulvovaginal Candidiasis-Results of a Practitioner Survey. Complement. Ther. Med. 2012, 20, 218–221. [Google Scholar] [CrossRef]
- Vahedpoor, Z.; Abastabar, M.; Sehat, M. Vaginal and Oral Use of Probiotics as Adjunctive Therapy to Fluconazole in Patients with Vulvovaginal Candidiasis: A Clinical Trial on Iranian Women. Curr. Med. Mycol. 2021, 7, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Foxman, B.; Muraglia, R.; Dietz, J.P.; Sobel, J.D.; Wagner, J. Prevalence of Recurrent Vulvovaginal Candidiasis in 5 European Countries and the United States: Results from an Internet Panel Survey. J. Low. Genit. Tract. Dis. 2013, 17, 340–345. [Google Scholar] [CrossRef] [PubMed]
- Denning, D.W.; Kneale, M.; Sobel, J.D.; Rautemaa-Richardson, R. Global Burden of Recurrent Vulvovaginal Candidiasis: A Systematic Review. Lancet Infect. Dis. 2018, 18, e339–e347. [Google Scholar] [CrossRef]
- Willems, H.M.E.; Ahmed, S.S.; Liu, J.; Xu, Z.; Peters, B.M. Vulvovaginal Candidiasis: A Current Understanding and Burning Questions. J. Fungi (Basel). 2020, 6, 27–46. [Google Scholar] [CrossRef] [PubMed]
- Vazquez, J.A.; Sobel, J.D.; Demitriou, R.; Vaishampayan, J.; Lynch, M.; Zervos, M.J. Karyotyping of Candida albicans Isolates Obtained Longitudinally in Women with Recurrent Vulvovaginal Candidiasis. J. Infect. Dis. 1994, 170, 1566–1569. [Google Scholar] [CrossRef]
- Rodríguez-Cerdeira, C.; Martínez-Herrera, E.; Carnero-Gregorio, M.; López-Barcenas, A.; Fabbrocini, G.; Fida, M.; El-Samahy, M.; González-Cespón, J.L. Pathogenesis and Clinical Relevance of Candida Biofilms in Vulvovaginal Candidiasis. Front. Microbiol. 2020, 11, 544480. [Google Scholar] [CrossRef] [PubMed]
- Marchaim, D.; Lemanek, L.; Bheemreddy, S.; Kaye, K.S.; Sobel, J.D. Fluconazole-resistant Candida albicans Vulvovaginitis. Obstet. Gynecol. 2012, 120, 1407–1414. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, J.A.; Seidu, L. Chronic Vulvovaginal Candida Hypersensitivity: An Underrecognized and Undertreated Disorder by Allergists. Allergy Rhinol. (Providence). 2015, 6, 44–49. [Google Scholar] [CrossRef]
- Fidel, P.L. Jr; Barousse, M.; Espinosa, T.; Ficarra, M.; Sturtevant, J.; Martin, D.H.; Quayle, A.J.; Dunlap, K. An Intravaginal Live Candida Challenge in Humans Leads to New Hypotheses for the Immunopathogenesis of Vulvovaginal Candidiasis. Infect. Immun. 2004, 72, 2939–2946. [Google Scholar] [CrossRef] [PubMed]
- Sobel, J.D.; Faro, S.; Force, R.W.; Foxman, B.; Ledger, W.J.; Nyirjesy, P.R.; Reed, B.D.; Summers, P.R. Vulvovaginal Candidiasis: Epidemiologic, Diagnostic, and Therapeutic Considerations. Am. J. Obstet. Gynecol. 1998, 178, 203–211. [Google Scholar] [CrossRef]
- Nyirjesy, P.; Sobel, J.D. Advances in Diagnosing Vaginitis: Development of a New Algorithm. Curr. Infect. Dis. Rep. 2005, 7, 458–462. [Google Scholar] [CrossRef]
- Martin Lopez, J.E. Candidiasis (vulvovaginal). BMJ Clin. Evid. 2015, 16, 0815. [Google Scholar]
- Li, L.; Zhang, X.; Li, Q.; Zhong, W.; Zou, H. The Increasing Trend of Triazole-Resistant Candida from Vulvovaginal Candidiasis. Infect. Drug Resist. 2024, 17, 4301–4310. [Google Scholar] [CrossRef]
- Ozcan, K.; Ilkit, M.; Ates. , A.; Turac-Bicer, A.; Demirhindi, H. Performance of Chromogenic Candida agar and CHROMagar Candida in Recovery and Presumptive Identification of Monofungal and Polyfungal Vaginal Isolates. Med. Mycol. 2010, 48, 29–34. [Google Scholar] [CrossRef]
- Ratner, J.C.; Wilson, J.; Roberts, K.; Armitage, C.; Barton, R.C. Increasing Rate of non-Candida albicans Yeasts and Fluconazole Resistance in Yeast Isolates from Women with Recurrent Vulvovaginal Candidiasis in Leeds, United Kingdom. Sex. Transm. Infect. 2025, 101, 21–26. [Google Scholar] [CrossRef]
- Ferris, D.G.; Dekle, C.; Litaker, M.S. Women's Use of Over-the-counter Antifungal Medications for Gynecologic Symptoms. J. Fam. Pract. 1996, 42, 595–600. [Google Scholar] [PubMed]
- Fisher, M.C.; Hawkins, N.J.; Sanglard, D.; Gurr, S.J. Worldwide Emergence of Resistance to Antifungal Drugs Challenges Human Health and Food Security. Science 2018, 360, 739–742. [Google Scholar] [CrossRef] [PubMed]
- Berman, J.; Krysan, D.J. Drug Resistance and Tolerance in Fungi. Nat. Rev. Microbiol. 2020, 18, 319–31. [Google Scholar] [CrossRef] [PubMed]
- Nyirjesy, P.; Brookhart, C.; Lazenby, G.; Schwebke, J.; Sobel, J.D. Vulvovaginal Candidiasis: A Review of the Evidence for the 2021 Centers for Disease Control and Prevention of Sexually Transmitted Infections Treatment Guidelines. Clin. Infect. Dis. 2022, 74 (Suppl_2), S162–S168. [Google Scholar] [CrossRef]
- Navarathna, D.H.; Lukey, J.; Coppin, J.D.; Jinadatha, C. Diagnostic Performance of DNA Probe-based and PCR-based Molecular Vaginitis Testing. Microbiol. Spectr. 2023, 11, e0162823. [Google Scholar] [CrossRef]
- Lillis, R.A.; Parker, R.L.; Ackerman, R.; Ackerman, J.; Young, S.; Weissfeld, A.; Trevino, E.; Nachamkin, I.; Crane, L.; Brown, J.; et al. Clinical Evaluation of a New Molecular Test for the Detection of Organisms Causing Vaginitis and Vaginosis. J. Clin. Microbiol. 2023, 61, e0174822. [Google Scholar] [CrossRef]
- Morovati, H.; Kord, M.; Ahmadikia, K.; Eslami, S.; Hemmatzadeh, M.; Kurdestani, K.M.; Khademi, M.; Darabian, S. A Comprehensive Review of Identification Methods for Pathogenic Yeasts: Challenges and Approaches. Adv. Biomed. Res. 2023, 12, 187. [Google Scholar] [CrossRef]
- Scharmann, U.; Kirchhoff, L.; Chapot, V.L.S.; Dziobaka, J.; Verhasselt, H.L.; Stauf, R.; Buer, J.; Steinmann, J.; Rath, P.M. Comparison of Four Commercially Available Chromogenic Media to Identify Candida albicans and Other Medically Relevant Candida species. Mycoses 2020, 63, 823–831. [Google Scholar] [CrossRef]
- Souza, M.N.; Ortiz, S.O.; Mello, M.M.; Oliveira Fde, M.; Severo, L.C.; Goebel, C.S. Comparison Between Four Usual Methods of Identification of Candida species. Rev. Inst. Med. Trop. Sao Paulo 2015, 57, 281–287. [Google Scholar] [CrossRef]
- Watson, C.J.; Grando, D.; Fairley, C.K.; Chondros, P.; Garland, S.M.; Myers, S.P.; Pirotta, M. The Effects of Oral Garlic on Vaginal Candida Colony Counts: a Randomised Placebo Controlled Double-blind Trial. BJOG 2014, 121, 498–506. [Google Scholar] [CrossRef]
- Bitew, A.; Abebaw, Y. Vulvovaginal Candidiasis: Species Distribution of Candida and their Antifungal Susceptibility Pattern. BMC Womens Health 2018, 18, 94. [Google Scholar] [CrossRef]
- Posteraro, B.; Martucci, R.; La Sorda, M.; Fiori, B.; Sanglard, D.; De Carolis, E.; Florio, A.R.; Fadda, G.; Sanguinetti, M. Reliability of the Vitek 2 Yeast Susceptibility Test for Detection of in vitro Resistance to Fluconazole and Voriconazole in Clinical Isolates of Candida albicans and Candida glabrata. J. Clin. Microbiol. 2009, 47, 1927–1930. [Google Scholar] [CrossRef] [PubMed]
- Robert, M.G.; Cornet, M.; Hennebique, A.; Rasamoelina, T.; Caspar, Y.; Pondérand, L.; Bidart, M.; Durand, H.; Jacquet, M.; Garnaud, C.; Maubon, D. MALDI-TOF MS in a Medical Mycology Laboratory: On Stage and Backstage. Microorganisms 2021, 9, 1283. [Google Scholar] [CrossRef] [PubMed]
- Teke, L.; Barış, A.; Bayraktar, B. Comparative Evaluation of the Bruker Biotyper and Vitek MS Matrix-assisted Laser Desorption Ionization-time of Flight Mass Spectrometry (MALDI-TOF MS) systems for Non-albicans Candida and Uncommon Yeast Isolates. J. Microbiol. Methods 2021, 185, 106232. [Google Scholar] [CrossRef] [PubMed]
- Sasani, E.; Rafat, Z.; Ashrafi, K.; Salimi, Y.; Zandi, M.; Soltani, S.; Hashemi, F.; Hashemi, S.J. Vulvovaginal Candidiasis in Iran: A Systematic Review and Meta-analysis on the Epidemiology, Clinical Manifestations, Demographic Characteristics, Risk Factors, Etiologic Agents and Laboratory Diagnosis. Microb. Pathog. 2021, 154, 104802. [Google Scholar] [CrossRef]
- Gonçalves, B.; Ferreira, C.; Alves, C.T.; Henriques, M.; Azeredo, J.; Silva, S. Vulvovaginal Candidiasis: Epidemiology, Microbiology and Risk Factors. Crit. Rev. Microbiol. 2016, 42, 905–927. [Google Scholar] [CrossRef]
- Aboagye, G.; Waikhom, S.; Asiamah, E.A.; Tettey, C.O.; Mbroh, H.; Smith, C. , Osei, G.Y.; Asafo Adjei, K.; Asmah, R.H. Antifungal Susceptibility Profiles of Candida and non-albicans Species Isolated from Pregnant Women: Implications for Emerging Antimicrobial Resistance in Maternal Health. Microbiol. Spectr. 2025, 2, e0078725. [Google Scholar] [CrossRef]
- Kroustali, V.; Resoulai, E.; Kanioura, L.; Siopi, M.; Meletiadis, J.; Antonopoulou, S. Epidemiology of Vulvovaginal Candidiasis in Greece: A 2-Year Single-Centre Study. Mycoses 2025, 68, e70026. [Google Scholar] [CrossRef]
- Daneshnia, F.; de Almeida Júnior, J.N.; Ilkit, M.; Lombardi, L.; Perry, A.M.; Gao, M.; Nobile, C.J.; Egger, M.; Perlin, D.S.; Zhai, B.; et al. Worldwide Emergence of Fluconazole-resistant Candida parapsilosis: Current Framework and Future Research Roadmap. Lancet Microbe 2023, 4, e470–e480. [Google Scholar] [CrossRef]
- Szekely, J.; Rakchang, W.; Rattanaphan, P.; Kositpantawong, N. Fluconazole and Echinocandin Resistance of Candida species in Invasive Candidiasis at a University Hospital During pre-COVID-19 and the COVID-19 Outbreak. Epidemiol. Infect. 2023, 151, e146. [Google Scholar] [CrossRef]
- Fernandes, Â.; Azevedo, N.; Valente, A.; Dias, M.; Gomes, A.; Nogueira-Silva, C.; Henriques, M.; Silva, S.; Gonçalves, B. Vulvovaginal Candidiasis and Asymptomatic Vaginal Colonization in Portugal: Epidemiology, Risk Factors and Antifungal Pattern. Med. Mycol. 2022, 60, myac029. [Google Scholar] [CrossRef]
- Trajano, D.T.M.; Melhem, M.S.C.; Takahashi, J.P.F.; Bonfietti, L.X.; de Araújo, M.R.; Corrêa, V.B.; Araújo, K.B.O.; Barnabé, V.; Fernandes, C.G. Species and Antifungal Susceptibility Profile of Agents Causing Vulvovaginal Candidiasis in a Military Population: A Cross-sectional Study. Med. Mycol. 2023, 61, myad025. [Google Scholar] [CrossRef]
- Karakoyun, A.S.; Unal, N.; Sucu, M.; Bingöl, O.; Unal, I.; Ilkit, M. Integrating Clinical and Microbiological Expertise to Improve Vaginal Candidiasis Management. Mycopathologia 2024, 189, 96. [Google Scholar] [CrossRef] [PubMed]
- Anh, D.N.; Hung, D.N.; Tien, T.V.; Dinh, V.N.; Son, V.T.; Luong, N.V.; Van, N.T.; Quynh, N.T.N.; Van Tuan, N.; Tuan, L.Q.; et al. Prevalence, Species Distribution and Antifungal Susceptibility of Candida albicans Causing Vaginal Discharge Among Symptomatic Non-pregnant Women of Reproductive Age at a Tertiary Care Hospital, Vietnam. BMC Infect. Dis. 2021, 21, 523. [Google Scholar] [CrossRef] [PubMed]
- Bignoumba, M.; Onanga, R.; Kumulungui, B.S.; Kassa, R.F.K.; Ndzime, Y.M.; Moghoa, K.M.; Stubbe, D.; Becker, P. High Diversity of Yeast Species and Strains Responsible for Vulvovaginal Candidiasis in South-East Gabon. J. Mycol. Med. 2023, 33, 101354. [Google Scholar] [CrossRef]
- Benhadj, M.; Menasria, T.; Ranque, S. MALDI-TOF Mass Spectrometry Identification and Antifungal Susceptibility Testing of Yeasts Causing Vulvovaginal Candidiasis (VVC) in Tebessa (Northeastern Algeria). Ann. Biol. Clin. (Paris) 2024, 81, 576–584. [Google Scholar] [CrossRef] [PubMed]
- Donders, G.; Bellen, G.; Byttebier, G.; Verguts, L.; Hinoul, P.; Walckiers, R.; Stalpaert, M.; Vereecken, A.; Van Eldere, J. Individualized Decreasing-dose Maintenance Fluconazole Regimen for Recurrent Vulvovaginal Candidiasis (ReCiDiF trial). Am. J. Obstet. Gynecol. 2008, 199, 613.e1–9. [Google Scholar] [CrossRef]
- Sobel, J.D.; Vempati, Y.S. Bacterial Vaginosis and Vulvovaginal Candidiasis Pathophysiologic Interrelationship. Microorganisms 2024, 12, 108. [Google Scholar] [CrossRef]
- Nguyen, Y.; Lee, A.; Fischer, G. 2017. Management of Chronic Vulvovaginal Candidiasis: A Long Term Retrospective Study. Australas. J. Dermatol. 2017, 58, e188–e192. [Google Scholar] [CrossRef]
- Pappas, P.G.; Kauffman, C.A.; Andes, D.R.; Clancy, C.J.; Marr, K.A.; Ostrosky-Zeichner, L.; Reboli, A.C.; Schuster, M.G.; Vazquez, J.A.; Walsh, T.J.; et al. Executive Summary: Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 62, 409–417. [Google Scholar] [CrossRef]
- Faria-Gonçalves, P.; Rolo, J.; Gaspar, C.; Oliveira, A. S.; Pestana, P. G.; Palmeira-de-Oliveira, R.; Gonçalves, T.; Martinez-de-Oliveira, J.; Palmeira-de-Oliveira, A. Recurrent Vulvovaginal Candida spp Isolates Phenotypically Express Less Virulence Traits. Microb, Pathog. 2020, 148, 104471. [CrossRef]
- Desai, J.V. Candida albicans Hyphae: From Growth Initiation to Invasion. J. Fungi (Basel) 2018, 4, 10. [Google Scholar] [CrossRef] [PubMed]
- Moyes, D.L.; Richardson, J.P.; Naglik, J.R. Candida albicans-epithelial Interactions and Pathogenicity Mechanisms: Scratching the Surface. Virulence 2015, 6, 338–346. [Google Scholar] [CrossRef] [PubMed]
- Camilli, G.; Griffiths, J.S.; Ho, J.; Richardson, J.P.; Naglik, J.R. Some Like it Hot: Candida Activation of Inflammasomes. PLoS Pathog. 2020, 16, e1008975. [Google Scholar] [CrossRef] [PubMed]
- Vande Walle, L.; Lamkanfi, M. Pyroptosis. Curr. Biol. 2016, 26, R568–R572. [Google Scholar] [CrossRef]
- McKenzie, C.G.; Koser, U.; Lewis, L.E.; Bain, J.M.; Mora-Montes, H.M.; Barker, R.N.; Gow, N.A.; Erwig, L.P. Contribution of Candida albicans Cell Wall Components to Recognition by and Escape from Murine Macrophages. Infect. Immun. 2010, 78, 1650–1658. [Google Scholar] [CrossRef]
- Wickramasinghe, D.N.; Lyon, C.M.; Lee, S.; Hepworth, O.W.; Priest, E.L.; Maufrais, C.; Ryan, A.P.; Permal, E.; Sullivan, D.; McManus, B.A.; et al. Variations in Candidalysin Amino Acid Sequence Influence Toxicity and Host Responses. mBio. 2024, 15, e0335123. [Google Scholar] [CrossRef]
- Tóth, A.; Zajta, E.; Csonka, K.; Vágvölgyi, C.; Netea, M.G.; Gácser, A. Specific Pathways Mediating Inflammasome Activation by Candida parapsilosis. Sci. Rep. 2017, 7, 43129. [Google Scholar] [CrossRef]
- Konwar, A.; Mathur, K.; Pandey, S.; Bhorali, K.; Thakur, A.; Puria, R. Insights into the Evolution of Candidalysin and Recent Developments. Arch. Microbiol. 2025, 207, 206. [Google Scholar] [CrossRef]
- Branzk, N.; Lubojemska, A.; Hardison, S.E.; Wang, Q.; Gutierrez, M.G.; Brown, G.D.; Papayannopoulos, V. Neutrophils Sense Microbe Size and Selectively Release Neutrophil Extracellular Traps in Response to Large Pathogens. Nat. Immunol. 2014, 15, 1017–1025. [Google Scholar] [CrossRef]
- Pan, Y.; Sun, Y.; Chen, L.; Cheng, Y.; Jin, P.; Zhang, W.; Zheng, L.; Liu, J.; Zhou, T.; Xu, Z.; et al. Candida Causes Recurrent Vulvovaginal Candidiasis by Forming Morphologically Disparate Biofilms on the Human Vaginal Epithelium. Biofilm 2023, 6, 100162. [Google Scholar] [CrossRef]
- Seider, K.; Gerwien, F.; Kasper, L.; Allert, S.; Brunke, S.; Jablonowski, N.; Schwarzmüller, T.; Barz, D.; Rupp, S.; Kuchler, K.; Hube, B. Immune Evasion, Stress Resistance, and Efficient Nutrient Acquisition are Crucial for Intracellular Survival of Candida glabrata Within Macrophages. Eukaryot. Cell 2014, 13, 170–183. [Google Scholar] [CrossRef]
- Tóth, A.; Németh, T.; Csonka, K.; Horváth, P.; Vágvölgyi, C.; Vizler, C.; Nosanchuk, J.D.; Gácser, A. Secreted Candida parapsilosis Lipase Modulates the Immune Response of Primary Human Macrophages. Virulence 2014, 5, 555–562. [Google Scholar] [CrossRef] [PubMed]
- Kulig, K.; Karnas, E.; Woznicka, O.; Kuleta, P.; Zuba-Surma, E.; Pyza, E.; Osyczka, A.; Kozik, A.; Rapala-Kozik, M.; Karkowska-Kuleta, J. Insight into the Properties and Immunoregulatory Effect of Extracellular Vesicles Produced by Candida glabrata, Candida parapsilosis, and Candida tropicalis Biofilms. Front. Cell Infect. Microbiol. 2022, 12, 879237. [Google Scholar] [CrossRef] [PubMed]
- Pezak, C.M.; Iosue, C.L.; Wykoff, D.D. Simplified J774A.1 Macrophage Assay for Fungal Pathogenicity Demonstrates Non-clinical Nakaseomyces glabratus Strains Survive Better Than Lab Strains. MicroPubl. Biol. 2024, 22, 2024–10.17912. [Google Scholar] [CrossRef]
- Richardson, J.P.; Willems, H.M.E.; Moyes, D.L.; Shoaie, S.; Barker, K.S.; Tan, S.L.; Palmer, G.E.; Hube, B.; Naglik, J.R.; Peters, B.M. Candidalysin Drives Epithelial Signaling, Neutrophil Recruitment, and Immunopathology at the Vaginal Mucosa. Infect. Immun. 2018, 86, e00645–e00717. [Google Scholar] [CrossRef]
- Willems, H.M.E.; Lowes, D.J.; Barker, K.S.; Palmer, G.E.; Peters, B.M. Comparative Analysis of the Capacity of the Candida Species to Elicit Vaginal Immunopathology. Infect. Immun. 2018, 86, e00527–e00618. [Google Scholar] [CrossRef]
- Netea, M.G.; Joosten, L.A.; van der Meer, J.W.; Kullberg, B.J.; van de Veerdonk, F.L. Immune Defence Against Candida Fungal Infections. Nat. Rev. Immunol. 2015, 15, 630–642. [Google Scholar] [CrossRef]
- Richardson, J.P.; Moyes, D.L.; Ho, J.; Naglik, J.R. Candida Innate Immunity at the Mucosa. Semin. Cell Dev. Biol. 2019, 89, 58–70. [Google Scholar] [CrossRef]
- Yano, J.; Peters, B.M.; Noverr, M.C.; Fidel, P.L. Jr. Novel Mechanism behind the Immunopathogenesis of Vulvovaginal Candidiasis: "Neutrophil Anergy". Infect. Immun. 2018, 86, e00684–e00717. [Google Scholar] [CrossRef]
- Rosati, D.; Bruno, M.; Jaeger, M.; Ten Oever, J.; Netea, M.G. Recurrent Vulvovaginal Candidiasis: An Immunological Perspective. Microorganisms 2020, 8, 144. [Google Scholar] [CrossRef]
- Rodrigues, C.F.; Rodrigues, M.E.; Henriques, M. Candida sp. Infections in Patients with Diabetes Mellitus. J. Clin. Med. 2019, 8, 76. [Google Scholar] [CrossRef]
- Peters, B.M.; Yano, J.; Noverr, M.C.; Fidel, P.L. Jr. Candida Vaginitis: When Opportunism Knocks, the Host Responds. PLoS Pathog. 2014, 10, e1003965. [Google Scholar] [CrossRef] [PubMed]
- Ashman, R.B. Protective and Pathologic Immune Responses against Candida albicans Infection. Front. Biosci. 2008, 13, 3334–3351. [Google Scholar] [CrossRef] [PubMed]
- Wozniak, K.L.; Wormley, F.L. Jr; Fidel, P.L. Jr. Candida-specific Antibodies During Experimental Vaginal Candidiasis in Mice. Infect. Immun. 2002, 70, 5790–5799. [Google Scholar] [CrossRef] [PubMed]
- Linhares, L.M.; Witkin, S.S.; Miranda, S.D.; Fonseca, A.M.; Pinotti, J.A.; Ledger, W.J. Differentiation Between Women with Vulvovaginal Symptoms who are Positive or Negative for Candida species by Culture. Infect. Dis. Obstet. Gynecol. 2001, 9, 221–225. [Google Scholar] [CrossRef]
- Hosen, H. Chronic Monilial Vaginitis. Ann. Allergy 1971, 29, 499. [Google Scholar]
- Kudelko, N.M. Allergy in Chronic Monilial Vaginitis. Ann. Allergy 1971, 29, 266–267. [Google Scholar]
- Witkin, S.S.; Jeremias, J.; Ledger, W.J. A Localized Vaginal Allergic Response in Women with Recurrent Vaginitis. J. Allergy Clin. Immunol. 1988, 81, 412–416. [Google Scholar] [CrossRef]
- Niu, X.X.; Li, T.; Zhang, X.; Wang, S.X.; Liu, Z.H. Lactobacillus crispatus Modulates Vaginal Epithelial Cell Innate Response to Candida albicans. Chin. Med. J. (Engl). 2017, 130, 273–279. [Google Scholar] [CrossRef]
- Giraldo, P.C.; de Carvalho, J.B.; do Amaral, R.L.; da Silveira Gonçalves, A.K.; Eleutério, J. Jr; Guimarães, F. Identification of Immune Cells by Flow Cytometry in Vaginal Lavages from Women with Vulvovaginitis and Normal Microflora. Am. J. Reprod. Immunol. 2012, 67, 198–205. [Google Scholar] [CrossRef]
- Ricchi, F.; Kenno, S.; Pedretti, N.; Brenna, G.; De Seta, F.; Ardizzoni, A.; Pericolini, E. Cutibacterium acnes Lysate Improves Cellular Response against Candida albicans, Escherichia coli and Gardnerella vaginalis in an in vitro Model of Vaginal Infection. Front. Cell. Infect. Microbiol. 2025, 15, 1578831. [Google Scholar] [CrossRef]
- Cassone, A.; De Bernardis, F.; Santoni, G. Anticandidal Immunity and Vaginitis: Novel Opportunities for Immune Intervention. Infect. Immun. 2007, 75, 4675–4686. [Google Scholar] [CrossRef]
- Wychrij, D.A.; Chapman, T.I.; Rayens, E.; Rabacal, W.; Willems, H.M.E.; Oworae, K.O.; Peters, B.M.; Norris, K.A. Protective Efficacy of the Pan-fungal Vaccine NXT-2 Against Vulvovaginal Candidiasis in a Murine Model. NPJ Vaccines 2025, 10, 112. [Google Scholar] [CrossRef]
- Ahmadifar, F.; Balali, E.; Khadivi, R.; Hashemi, M.; Jebali, A. The Evaluation of a Novel Multi-epitope Vaccine Against Human Papillomavirus and Candida albicans. J. Genet. Eng. Biotechnol. 2025, 23, 100489. [Google Scholar] [CrossRef]
- Costa-Barbosa, A.; Pacheco, M.I.; Gomes, A.C.; Collins, T.; Vilanova, M.; Pais, C.; Correia, A.; Sampaio, P. Pre-clinical Evaluation of a Divalent Liposomal Vaccine to Control Invasive Candidiasis. NPJ Vaccines 2025, 10, 124. [Google Scholar] [CrossRef] [PubMed]
- De Bernardis, F.; Amacker, M.; Arancia, S.; Sandini, S.; Gremion, C.; Zurbriggen, R.; Moser, C.; Cassone, A. A Virosomal Vaccine Against Candidal Vaginitis: Immunogenicity, Efficacy and Safety Profile in Animal Models. Vaccine 2012, 30, 4490–4498. [Google Scholar] [CrossRef]
- Edwards, J.E. Jr; Schwartz, M.M.; Schmidt, C.S.; Sobel, J.D.; Nyirjesy, P.; Schodel, F.; Marchus, E.; Lizakowski, M.; DeMontigny, E.A.; Hoeg, J.; et al. A Fungal Immunotherapeutic Vaccine (NDV-3A) for Treatment of Recurrent Vulvovaginal Candidiasis-A Phase 2 Randomized, Double-Blind, Placebo-Controlled Trial. Clin. Infect. Dis. 2018, 66, 1928–1936. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.A.; Khan, A.; Alnuqaydan, A.M.; Albutti, A.; Alharbi, B.F.; Owais, M. Targeting Azole-Resistant Candida albicans: Tetrapeptide Tuftsin-Modified Liposomal Vaccine Induces Superior Immune Protection. Vaccines (Basel) 2025, 13, 630. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.A.; Mousa, A.M.; Alradhi, A.E.; Allemailem, K. Efficacy of Lipid Nanoparticles-based Vaccine to Protect Against Vulvovaginal Candidiasis (VVC): Implications for Women's Reproductive Health. Life Sci. 2025, 361, 123312. [Google Scholar] [CrossRef]
- de Barros, P.P.; Rossoni, R.D.; de Souza, C.M.; Scorzoni, L.; Fenley, J.C.; Junqueira, J.C. Candida Biofilms: An Update on Developmental Mechanisms and Therapeutic Challenges. Mycopathologia 2020, 185, 415–424. [Google Scholar] [CrossRef]
- Gulati, M.; Nobile, C.J. Candida albicans Biofilms: Development, Regulation, and Molecular Mechanisms. Microbes Infect. 2016, 18, 310–321. [Google Scholar] [CrossRef] [PubMed]
- Hu, T.; Meng, Y.; Zhao, C.; Sheng, D.; Yang, S.; Dai, J.; Wei, T.; Zhang, Y.; Zhao, G.; Liu, Y.; et al. Genome-scale Metabolic Modelling Reveals Specific Vaginal Lactobacillus Strains and Their Metabolites as Key Inhibitors of Candida albicans. Microbiol. Spectr. 2025, 13, e0298424. [Google Scholar] [CrossRef] [PubMed]
- Tortelli, B.A.; Lewis, W.G.; Allsworth, J.E.; Member-Meneh, N.; Foster, L.R.; Reno, H.E.; Peipert, J.F.; Fay, J.C.; Lewis, A.L. Associations Between the Vaginal Microbiome and Candida Colonization in Women of Reproductive Age. Am. J. Obstet. Gynecol. 2020, 222, 471.e1–471.e9. [Google Scholar] [CrossRef] [PubMed]
- Parolin, C.; Croatti, V.; Giordani, B.; Vitali, B. Vaginal Lactobacillus Impair Candida Dimorphic Switching and Biofilm Formation. Microorganisms 2022, 10, 2091. [Google Scholar] [CrossRef]
- Nguyen, L.N.; Lopes, L.C.; Cordero, R.J.; Nosanchuk, J.D. Sodium Butyrate Inhibits Pathogenic Yeast Growth and Enhances the Functions of Macrophages. J. Antimicrob. Chemother. 2011, 66, 2573–2580. [Google Scholar] [CrossRef]
- Said, M.M.; Watson, C.; Grando, D. Garlic Alters the Expression of Putative Virulence Factor Genes SIR2 and ECE1 in Vulvovaginal C. albicans Isolates. Sci. Rep. 2020, 10, 3615. [Google Scholar] [CrossRef]
- Donlan, R.M. Biofilms: Microbial Life on Surfaces. Emerg. Infect. Dis. 2002, 8, 881–90. [Google Scholar] [CrossRef]
- McKloud, E.; Delaney, C.; Sherry, L.; Kean, R.; Williams, S.; Metcalfe, R.; Thomas, R.; Richardson, R.; Gerasimidis, K.; Nile, et al. Recurrent Vulvovaginal Candidiasis: A Dynamic Interkingdom Biofilm Disease of Candida and Lactobacillus. mSystems 2021, 6, e0062221. [Google Scholar] [CrossRef]
- Zarnowski, R.; Noll, A.; Chevrette, M.G.; Sanchez, H.; Jones, R.; Anhalt, H.; Fossen, J.; Jaromin, A.; Currie, C.; Nett, et al. Coordination of Fungal Biofilm Development by Extracellular Vesicle Cargo. Nat. Commun. 2021, 12, 6235. [Google Scholar] [CrossRef]
- Ravel, J.; Gajer, P.; Abdo, Z.; Schneider, G.M.; Koenig, S.S.K.; McCulle, S.L.; Karlebach, S.; Gorle, R.; Russell, J.; Tacket, C.O.; et al. Vaginal Microbiome of Reproductive-age Women. Proc. Natl. Acad. Sci. U S A. 2011, 108, 4680–4687. [Google Scholar] [CrossRef]
- Giordani, B.; Naldi, M.; Croatti, V.; Parolin, C.; Erdoğan, Ü.; Bartolini, M.; Vitali, B. Exopolysaccharides from Vaginal Lactobacilli Modulate Microbial Biofilms. Microb. Cell Fact. 2023, 22, 45. [Google Scholar] [CrossRef] [PubMed]
- Bae, W.Y.; Lee, Y.J.; Jo, S.; Shin, S.L.; Kim, T.R.; Sohn, M.; Seol, H.J. Effects of Lactiplantibacillus plantarum LM1215 on Candida albicans and Gardnerella vaginalis. Yonsei Med. J. 2024, 65, 727–740. [Google Scholar] [CrossRef] [PubMed]
- Powell, A.; Ghanem, K. G.; Rogers, L.; Zinalabedini, A.; Brotman, R. M.; Zenilman, J.; Tuddenham, S. Clinicians' Use of Intravaginal Boric Acid Maintenance Therapy for Recurrent Vulvovaginal Candidiasis and Bacterial Vaginosis. Sex. Transm. Dis. 2019, 46, 810–812. [Google Scholar] [CrossRef] [PubMed]
- De Seta, F.; Schmidt, M.; Vu, B.; Essmann, M.; Larsen, B. Antifungal Mechanisms Supporting Boric acid Therapy of Candida vaginitis. J. Antimicrob. Chemother. 2009, 63, 325–36. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, Z.; Li, Q.; Feng, Y.; Li, J.; Lu, Y.; Zhang, J.; Ke, X. A "Three-in-one" Thermosensitive Gel System that Enhances Mucus and Biofilm penetration for the Treatment of Vulvovaginal Candidiasis. J. Control. Release 2025, 382, 113666. [Google Scholar] [CrossRef]
- Watson, C.J.; Grando, D.; Garland, S.M.; Myers, S.; Fairley, C.K.; Pirotta, M. Premenstrual Vaginal Colonization of Candida and Symptoms of Vaginitis. J. Med. Microbiol. 2012, 61, 1580–1583. [Google Scholar] [CrossRef]
- CDC, 2021. Sexually Transmitted Infections Treatment. Vulvovaginal Candidiasis (VVC). 2021. Available online: https://www.cdc.gov/std/treatment-guidelines/candidiasis.htm (accessed on 4th June 2025).
- ASHM, The Australasian Society for HIV, Viral Hepatitis and Sexual Health Medicine (ASHM). Australian STI management guidelines for use in primary care. Candidiasis. 2024. Available online: https://sti.guidelines.org.au/sexually-transmissible-infections/candidiasis/ (accessed on 4th June 2025).
- Farr, A.; Effendy, I.; Frey Tirri, B.; Hof, H.; Mayser, P.; Petricevic, L.; Ruhnke, M.; Schaller, M.; Schaefer, A.P.A.; Sustr, V.; et al. Guideline: Vulvovaginal Candidosis (AWMF 015/072, level S2k). Mycoses 2021, 64, 583–602. [Google Scholar] [CrossRef]
- Donders, G.; Sziller, I.O.; Paavonen, J.; Hay, P. , de Seta, F.; Bohbot, J.M.; Kotarski, J.; Vives, J.A.; Szabo, B.; Cepuliené, R.; Mendling, W. Management of Recurrent Vulvovaginal Candidosis: Narrative Review of the Literature and European Expert Panel Opinion. Front. Cell. Infect. Microbiol. 2022, 12, 934353. [Google Scholar] [CrossRef]
- Quindos, G.; Marcos-Arias, C.; Miranda-Cadena, K. The Future of Non-invasive Azole Antifungal Treatment Options for the Management of Vulvovaginal Candidiasis. Expert Rev. Anti Infect. Ther. 2025, 23, 571–584. [Google Scholar] [CrossRef]
- Day, T.; Sobel, J.D. Genital Cutaneous Candidiasis versus Chronic Recurrent Vulvovaginal Candidiasis: Distinct Diseases, Different Populations. Clin. Microbiol. Rev. 2025, 38, e0002025. [Google Scholar] [CrossRef]
- Gupta, A.K.; Katz, H.I.; Shear, N.H. Drug Interactions with Itraconazole, Fluconazole, and Terbinafine and their Management. J. Am. Acad. Dermatol. 1999, 41, 237–49. [Google Scholar] [CrossRef]
- Fong, I.W. The Value of Chronic Suppressive Therapy with Itraconazole versus Clotrimazole in Women with Recurrent Vulvovaginal Candidiasis. Genitourin. Med. 1992, 68, 374–377. [Google Scholar] [CrossRef] [PubMed]
- Denison, H.J.; Worswick, J.; Bond, C.M.; Grimshaw, J.M.; Mayhew, A.; Gnani Ramadoss, S.; Robertson, C.; Schaafsma, M.E.; Watson, M.C. Oral versus Intra-vaginal Imidazole and Triazole Anti-fungal Treatment of Uncomplicated Vulvovaginal Candidiasis (Thrush). Cochrane Database Syst. Rev. 2020, 8, CD002845. [Google Scholar] [CrossRef] [PubMed]
- Cooke, G.; Watson, C.; Deckx, L.; Pirotta, M.; Smith, J.; van Driel, M.L. Treatment for Recurrent Vulvovaginal Candidiasis (Thrush). Cochrane Database Syst. Rev. 2022, 1, CD009151. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sobel, J. D.; Sobel, R. Current Treatment Options for Vulvovaginal Candidiasis Caused by Azole-resistant Candida species. Expert Opin. Pharmacother. 2018, 19, 971–977. [Google Scholar] [CrossRef]
- Sobel, J.D. New Antifungals for Vulvovaginal Candidiasis: What is their Role? Clin. Infect. Dis. 2023, 76, 783–785. [Google Scholar] [CrossRef] [PubMed]
- Kriegl, L.; Eggar, M.; Bayer, J.; Hoenigl, M.; Krause, R. New Treatment Options for Critically Important WHO Fungal Priority Pathogens. Clin. Microbiol. Infect. 2025, 31, 922–930. [Google Scholar] [CrossRef]
- A Phase 11b / 111 Study of prof-001 for the Treatment of Recurrent Vulvovaginal Candidiasis (RVVC). Available online: https://ctv.veeva.com/study/a-phase-iib-iii-study-of-prof-001-for-the-treatment-of-patients-with-recurrent-vulvovaginal-candidia (accessed on 4th June 2025).
- Chayachinda, C.; Thamkhantho, M.; Rekhawasin, T.; Klerdklinhom, C. Sertaconazole 300 mg versus Clotrimazole 500 mg Vaginal Suppository for Treating Pregnant Women with Acute Vaginal Candidiasis: A Double-blinded, Randomized Trial. BMC Pregnancy Childbirth 2024, 24, 235. [Google Scholar] [CrossRef]
- de Cássia Orlandi Sardi, J.; Silva, D.R.; Anibal, P.C.; de Campos Baldin, J.J.C.M.; Ramalho, S.R.; Rosalen, P.L.; Macedo, M.L.R.; Hofling, J.F. Vulvovaginal Candidiasis: Epidemiology and Risk Factors, Pathogenesis, Resistance, and New Therapeutic Options. Curr. Fungal Infect. Rep. 2021, 15, 32–40. [Google Scholar] [CrossRef]
- Howley, M.M.; Carter, T.C.; Browne, M.L.; Romitti, P.A.; Cunniff, C.M.; Druschel, C.M. National Birth Defects Prevention Study. Fluconazole use and Birth Defects in the National Birth Defects Prevention Study. Am. J. Obstet. Gynecol. 2016, 214, e1–9. [Google Scholar] [CrossRef]
- Papadopoulos, E.A.; Howley, M.M.; Fisher, S.C.; Van Zutphen, A.R.; Werler, M.M.; Romitti, P.A.; Browne, M.L. National Birth Defects Prevention Study. Antifungal Medication Use During Pregnancy and the Risk of Selected Major Birth Defects in the National Birth Defects Prevention Study, 1997-2011. Pharmacoepidemiol. Drug Saf. 2024, 33, e5741. [Google Scholar] [CrossRef]
- Mølgaard-Nielsen, D.; Pasternak, B.; Hviid, A. Use of Oral Fluconazole During Pregnancy and the Risk of Birth Defects. N. Engl. J. Med. 2013, 369, 830–839. [Google Scholar] [CrossRef]
- Nachum, Z.; Suleiman, A.; Colodner, R.; Battino, S.; Wattad, M.; Kuzmin, O.; Yefet, E. Oral Probiotics to Prevent Recurrent Vulvovaginal Infections During Pregnancy-Multicenter Double-Blind, Randomized, Placebo-Controlled Trial. Nutrients. 2025, 17, 460. [Google Scholar] [CrossRef]
- Burhanuddin, H.; Enggi, C.K.; Tangdilintin, F.; Saputra, R.R.; Putra, P.P.; Sartini, S.; Aliyah, A.; Agustina, R.; Domínguez-Robles, J.; Aswad, M.; Permana, A.D. Development of Amphotericin B Inclusion Complex Formulation in Dissolvable Microarray Patches for Intravaginal Delivery. Daru 2024, 33, 5. [Google Scholar] [CrossRef] [PubMed]
- Patil, M.U.; Rajput, A.P.; Belgamwar, V.S.; Chalikwar, S.S. Development and Characterization of Amphotericin B Nanoemulsion-loaded Mucoadhesive Gel for Treatment of Vulvovaginal Candidiasis. Heliyon 2022, 8, e11489. [Google Scholar] [CrossRef] [PubMed]
- Cornely, O.; Sprute, R.; Bassetti, M.; Chen, S.C.; Groll, A.H.; Kurzai, O.; Lass-Flörl, C.; Ostrosky-Zeichner, L. , Rautemaa-Richardson, R. , Revathi, G.; et al. Global Guideline for the Diagnosis and Management of Candidiasis: An Initiative of the ECMM in Cooperation with ISHAM and ASM. Lancet Infect. Dis. 2025, 25, e280–e293. [Google Scholar] [CrossRef] [PubMed]
- Radesca Moncayo, Y. Vaginal Candidiasis, Predisposing Factors, Symptoms and Treatment. SCT Proc. Interdiscip. Insights Innov. 2024, 2, 347. [Google Scholar] [CrossRef]
- Zeng, Z.; Li, P.; Lu, J.; Li, X.; Li, M.; Wu, Y.; Zheng, M.; Cao, Y.; Liao, Q.; Ge, Z.; Zhang, L. A Non-antibiotic Antimicrobial Drug, a Biological Bacteriostatic Agent, is useful for Treating Aerobic Vaginitis, Bacterial Vaginosis, and Vulvovaginal Candidiasis. Front. Microbiol. 2024, 15, 1341878. [Google Scholar] [CrossRef]
- Imhof, M.; Lipovac, M.; Kurz, C.; Barta, J.; Verhoeven, H.C.; Huber, J.C. Propolis Solution for the Treatment of Chronic Vaginitis. Int. J. Gynecol. Obstet. 2005, 89, 127–32. [Google Scholar] [CrossRef] [PubMed]
- Romero-Cerecero, O.; Islas-Garduño, A.L.; Zamilpa, A.; Tortoriello, J. Effectiveness of Ageratina pichinchensis Extract in Patients with Vulvovaginal Candidiasis. A Randomized, Double-blind, and Controlled Pilot Study. Phytother. Res. 2017, 31, 885–890. [Google Scholar] [CrossRef]
- Ebrahimy, F.; Dolatian, M.; Moatar, F.; Alavi, M.H. Comparison of the Therapeutic Effects of Garcin® and Fluconazole on Candida Vaginitis. Singapore Med. J. 2015, 56, 567–572. [Google Scholar] [CrossRef] [PubMed]
- Hatfield, J. , Saad, S., Housewright, C. Dietary Supplements and Bleeding. Proc. (Bayl. Univ. Med. Cent). 2022, 35, 802–807. [Google Scholar] [CrossRef] [PubMed]
- Bertholf, M.E.; Stafford, M.J. Colonization of Candida albicans in Vagina, Rectum, and Mouth. J. Fam. Pract. 1983, 16, 919–924. [Google Scholar] [PubMed]
- Delavy, M.; Sertour, N.; Patin, E.; Le Chatelier, E.; Cole, N.; Dubois, F.; Xie, Z.; Saint-André, V.; Manichanh, C.; Walker, A.W.; et al. Unveiling Candida albicans Intestinal Carriage in Healthy Volunteers: The role of Micro- and Mycobiota, Diet, Host Genetics and Immune Response. Gut Microbes 2023, 15, 2287618. [Google Scholar] [CrossRef]
- McCrory, C. , Lenardon, M., Traven, A. Bacteria-derived Short-chain Fatty Acids as Potential Regulators of Fungal Commensalism and Pathogenesis. Trends Microbiol. 2024, 32, 1106–1118. [Google Scholar] [CrossRef]
- Cronin, P.; Joyce, S.A.; O'Toole, P.W.; O'Connor, E.M. Dietary Fibre Modulates the Gut Microbiota. Nutrients 2021, 13, 1655. [Google Scholar] [CrossRef]
- Djusse, M.E.; Prinelli, F.; Camboni, T.; Ceccarani, C.; Consolandi, C.; Conti, S.; Dall'Asta, M.; Danesi, F.; Laghi, L.; Curatolo, F.M.; et al. Dietary Habits and Vaginal Environment: Can a Beneficial Impact be Expected? Front. Cell. Infect. Microbiol. 2025, 15, 1582283. [Google Scholar] [CrossRef]
- Smith, B.C.; McAndrew, T.; Chen, Z.; Harari, A.; Barris, D.M.; Viswanathan, S.; Rodriguez, A.C.; Castle, P.; Herrero, R.; Schiffman, M.; Burk, R.D. The Cervical Microbiome over 7 Years and a Comparison of Methodologies for its Characterization. PLoS One 2012, 7, e40425. [Google Scholar] [CrossRef]
- Kim, M.J.; Lee, S.; Kwon, M.Y.; Kim, M. Clinical Significance of Composition and Functional Diversity of the Vaginal Microbiome in Recurrent Vaginitis. Front. Microbiol. 2022, 13, 851670. [Google Scholar] [CrossRef]
- Jepsen, I.E.; Saxtorph, M.H.; Englund, A.L.M.; Petersen, K.B.; Wissing, M.L.M.; Hviid, T.V.F.; Macklon, N. Probiotic Treatment with Specific Lactobacilli does not Improve an Unfavorable Vaginal Microbiota Prior to Fertility Treatment - A Randomized, Double-blinded, Placebo-controlled Trial. Front. Endocrinol. (Lausanne) 2022, 13, 1057022. [Google Scholar] [CrossRef]
- Koedooder, R.; Singer, M.; Schoenmakers, S.; Savelkoul, P.H.M.; Morré, S.A.; de Jonge, J.D.; Poort, L.; Cuypers, W.J.S.S.; Beckers, N.G.M.; Broekmans, F.J.M.; et al. The Vaginal Microbiome as a Predictor for Outcome of in Vitro Fertilization with or without Intracytoplasmic Sperm Injection: A Prospective Study. Hum. Reprod. 2019, 34, 1042–1054. [Google Scholar] [CrossRef]
- Perez, M.; Armengol, E.; Del Casale, A.; Campedelli, I.; Aldea-Perona, A.; Pérez Otero, M.; Rodriguez-Palmero, M.; Espadaler-Mazo, J.; Huedo, P. Lactobacillus gasseri CECT 30648 Shows Probiotic Characteristics and Colonizes the Vagina of Healthy Women after Oral Administration. Microbiol. Spectr. 2025, 13, e0021125. [Google Scholar] [CrossRef]
- France, M.; Alizadeh, M.; Brown, S.; Ma, B.; Ravel, J. Towards a Deeper Understanding of the Vaginal Microbiota. Nat. Microbiol. 2022, 7, 367–378. [Google Scholar] [CrossRef]
- van Houdt, R.; Ma, B.; Bruisten, S.M.; Speksnijder, A.G.C.L.; Ravel, J. , de Vries, H.J.C. Lactobacillus iners-dominated Vaginal Microbiota is Associated with Increased Susceptibility to Chlamydia trachomatis Infection in Dutch Women: A case-control Study. Sex. Transm. Infect. 2018, 94, 117–123. [Google Scholar] [CrossRef]
- Armstrong, E.; Hemmerling, A.; Miller, S.; Huibner, S.; Kulikova, M.; Crawford, E.; Castañeda, G.R.; Coburn, B.; Cohen, C.R.; Kaul, R. Vaginal Lactobacillus crispatus Persistence Following Application of a Live Biotherapeutic Product: Colonization Phenotypes and Genital Immune Impact. Microbiome. 2024, 12, 110. [Google Scholar] [CrossRef] [PubMed]
- Cohen, C.R.; Wierzbicki, M.R.; French, A.L.; Morris, S.; Newmann, S.; Reno, H.; Green, L.; Miller, S.; Powell, J.; Parks, T.; Hemmerling, A. Randomized Trial of Lactin-V to Prevent Recurrence of Bacterial Vaginosis. N. Engl. J. Med. 2020, 382, 1906–1915. [Google Scholar] [CrossRef] [PubMed]
- Gosmann, C.; Anahtar, M.N.; Handley, S.A.; Farcasanu, M.; Abu-Ali, G.; Bowman, B.A.; Padavattan, N.; Desai, C.; Droit, L.; Moodley, A.; et al. Lactobacillus-Deficient Cervicovaginal Bacterial Communities Are Associated with Increased HIV Acquisition in Young South African Women. Immunity. 2017, 46, 29–37. [Google Scholar] [CrossRef] [PubMed]
- van Nood, E.; Vrieze, A.; Nieuwdorp, M.; Fuentes, S.; Zoetendal, E.G.; de Vos, W.M.; Visser, C.E.; Kuijper, E.J.; Bartelsman, J.F.; Tijssen, J.G.; et al. Duodenal Infusion of Donor Feces for Recurrent Clostridium difficile. N. Engl. J. Med. 2013, 368, 407–415. [Google Scholar] [CrossRef]
- Wilson, B.C.; Zuppi, M.; Derraik, J.G.B.; Albert, B.B.; Tweedie-Cullen, R.Y.; Leong, K.S.W.; Beck, K.L.; Vatanen, T.; O'Sullivan, J.M.; Cutfield, W.S.; Gut Bugs Study Group. Long-term Health Outcomes in Adolescents with Obesity Treated with Faecal Microbiota Transplantation: 4-year Follow-up. Nat. Commun. 2025, 16, 7786. [Google Scholar] [CrossRef]
- Lev-Sagie, A.; Goldman-Wohl, D.; Cohen, Y.; Dori-Bachash, M.; Leshem, A.; Mor, U.; Strahilevitz, J.; Moses, A.E.; Shapiro, H.; Yagel, S.; Elinav, E. Vaginal Microbiome Transplantation in Women with Intractable Bacterial Vaginosis. Nat. Med. 2019, 25, 1500–1504. [Google Scholar] [CrossRef]
- Wrønding, T.; Vomstein, K.; Bosma, E.F.; Mortensen, B.; Westh, H.; Heintz, J.E.; Mollerup, S.; Petersen, A.M.; Ensign, L.M.; DeLong, K.; et al. Antibiotic-free Vaginal Microbiota Transplant with Donor Engraftment, Dysbiosis Resolution and Live Birth After Recurrent Pregnancy Loss: A Proof of Concept Case Study. EClinicalMedicine 2023, 61, 102070. [Google Scholar] [CrossRef]
- Liu, Y.; Zhao, X.; Wu, F.; Chen, J.; Luo, J.; Wu, C.; Chen, T. Effectiveness of Vaginal Probiotics Lactobacillus crispatus chen-01 in Women with High-risk HPV infection: A Prospective Controlled Pilot Study. Aging (Albany NY) 2024, 16, 11446–11459. [Google Scholar] [CrossRef] [PubMed]
- So, K.A.; Yang, E.J.; Kim, N.R.; Hong, S.R.; Lee, J.H.; Hwang, C.S.; Shim, S.H.; Lee, S.J.; Kim, T.J. Changes of Vaginal Microbiota During Cervical Carcinogenesis in Women with Human Papillomavirus Infection. PLoS One 2020, 15, e0238705. [Google Scholar] [CrossRef] [PubMed]
- Hemmerling, A.; Mitchell, C.M.; Demby, S.; Ghebremichael, M.; Elsherbini, J.; Xu, J.; Xulu, N.; Shih, J.; Dong, K.; Govender, V.; et al. Effect of the Vaginal Live Biotherapeutic LACTIN-V (Lactobacillus crispatus CTV-05) on Vaginal Microbiota and Genital Tract Inflammation Among Women at High Risk of HIV Acquisition in South Africa: A Phase 2, Randomised, Placebo-controlled Trial. Lancet Microbe 2025, 6, 101037. [Google Scholar] [CrossRef] [PubMed]
- El-Baz, N.; Kyser, A.; Mahmoud, M.Y.; Farrell, C.Z.; Ginocchio, S.; Frieboes, H.B.; Doster, R.S. Modulation of Group B Streptococcus Infection and Vaginal Cell Inflammatory signaling in vitro by Lactobacillus crispatus-loaded Electrospun Fibers. Infect. Immun. 2025, 0, e0017025. [Google Scholar] [CrossRef]
- Ravel, J.; Simmons, S.; Jaswa, E.G.; Gottfried, S.; Greene, M.; Kellogg-Spadt, S.; Gevers, D.; Harper, D.M. Impact of a Multi-strain L. crispatus-based Vaginal Synbiotic on the Vaginal Microbiome: A Randomized Placebo-controlled Trial. NPJ Biofilms Microbiomes 2025, 11, 158. [Google Scholar] [CrossRef]
Figure 1.
Alternate characterization of the types of VVC.

Table 1.
Relative proportion of most common species reported to cause VVC in recent studies where chromogenic agar was used to aid in identification of mixed yeast and using at least MALDI-ToF spectroscopy or sequencing to confirm identity of isolates (in brackets where RVVC counted).
Table 1.
Relative proportion of most common species reported to cause VVC in recent studies where chromogenic agar was used to aid in identification of mixed yeast and using at least MALDI-ToF spectroscopy or sequencing to confirm identity of isolates (in brackets where RVVC counted).
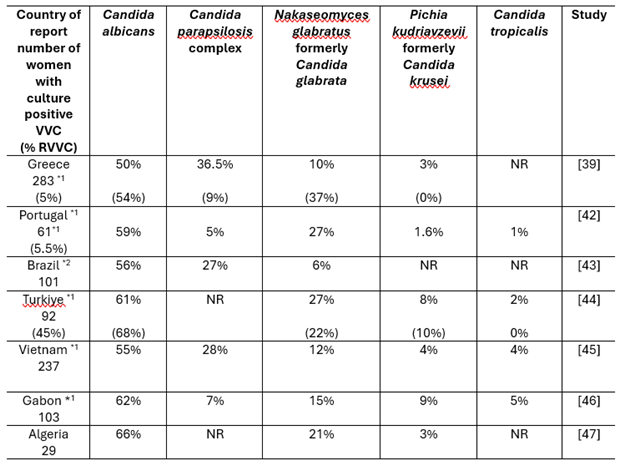 |
Notes: *1 Reported to have mixed Candida infections (7 – 10%). *2 Study of military recruits. NR – not reported.
Table 2.
Antifungal agents and recommended dosing.
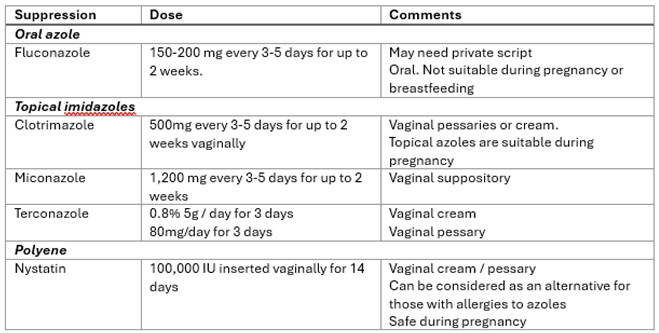 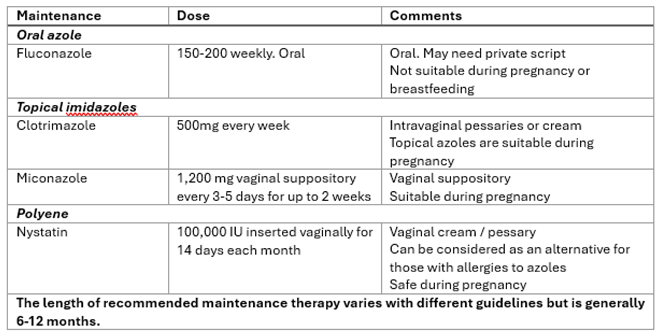 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



