Submitted:
22 September 2025
Posted:
23 September 2025
You are already at the latest version
Abstract
Transcatheter aortic valve replacement has become a widely accepted alternative to surgical aortic valve replacement even in younger, lower-risk patients with longer life expectancy. The increasing use of transcatheter aortic valve replacement is leading to a rise in the need for surgical explantation of failing transcatheter valves, a complex procedure associated with increased periprocedural risks and technical challenges. The absence of established guidelines for the treatment of this life-threatening condition highlights an important clinical challenge. Published experience with surgical explan-tation of transcatheter aortic valve remains limited. referralsized explantation proto-cols, patient tailored management, careful patient selection, detailed preoperative im-aging, and early surgical referral are essential for improving safety and efficacy. Op-timal outcomes require collaboration among cardiac surgeons, cardiologists, infectious disease specialists, and radiologists.
Keywords:
transcatheter aortic valve explantation
; transcatheter aortic valve failure
; surgical aortic valve replacement
; transcatheter aortic valve replacement
1. Introduction
Over the past twenty years, transcatheter aortic valve implantation (TAVI) technology has undergone ongoing development. Advances in procedural techniques and device design have led to transcatheter aortic valve replacement (TAVR) being considered as an alternative to surgical aortic valve replacement. TAVI is currently approved for patients under 70 years of age and those assessed as lower risk, based on long-term data from the Partner 3 and Evolut Low Risk Trials [1,2].
As TAVR procedures are increasingly performed in younger and lower-risk patients, the number of surgical transcatheter aortic valve explants is expected to rise since there are several clinical scenarios in which surgical removal of a previously implanted transcatheter valve becomes necessary. At present, the surgical replacement of a failing transcatheter aortic valve is one of the fastest-growing cardiac surgery procedures in the United States [3].
The incidence of TAVR-explant is currently estimated at approximately 0.5% to 2%; however, this rate is anticipated to increase substantially in the future [3].
The surgical replacement of a failing transcatheter aortic valve is associated with increased periprocedural risk, reported median 30-day mortality between 15% and 20% and requires specific technical skills and surgical experience. However, there are currently no established guidelines for the surgical management of patients undergoing redo-TAVR [3], [Figure 1].
2. Incidence and Indications for TAVI Explant Surgery
According to the FRANCE 2 and FRANCE TAVI registries, which included 72,850 patients over an eight-year period, the cumulative incidence of overall reintervention in transcatheter aortic valve was 1.7%. Importantly, 62.1% of these reinterventions occurred early, within the first year following the initial procedure [4].
In the EXPLANT-TAVR international registry, which included 391 patients, the median time from TAVI to explantation was 13.3 months [5]. According to this registry, primary reasons for surgical removal are transcatheter valve endocarditis (43.1%), severe paravalvular leak (18.2%), structural transcatheter valve deterioration (20.1%) and severe prosthesis-patient mismatch (10.8%) [5,6], [Figure 1].
Surgical bailout is another indication for transcatheter valve explantation [Figure 1]. Specifically, urgent conversion from TAVI to open-heart surgery, referred to as surgical bailout, may be necessary in cases of complications such as annular rupture, coronary obstruction, or type A aortic dissection. An analysis of the STS and ACC Transcatheter Valve Therapy registry found that, among 47,546 TAVI patients, 1.17% required surgical bailout, with an in-hospital mortality rate of 49.6% [7].
The cumulative incidence of transcatheter aortic valve endocarditis approaches 5% within the initial five years following the procedure. Reported annual incidence rates range from 0.5% to 1.6% among populations monitored for up to five years [8].
Recent analysis from the PARTNER-1 and PARTNER-2 trials, which included 8,530 patients, revealed that the incidence of prosthetic valve endocarditis did not differ notably between patients who underwent TVR and those who received surgical aortic valve replacement [9]. However, additional studies have highlighted the substantial morbidity and mortality associated with TAVR-related endocarditis. Notably, in-hospital mortality rates for TAVR-endocarditis were nearly twice as high as those observed in surgical prosthetic valve endocarditis cases [9].
Surgical explantation of infected TAVI prostheses is relatively rare, being performed in only 2% to 14% of cases, despite clear indications for surgery in more than 80% of affected patients [6,8]. The primary reasons for not proceeding with surgery include high clinical or surgical risk, the need for additional procedures, advanced patient age, limited life expectancy, multiorgan failure, septicemia, and overall poor long-term prognosis. Unfortunately, this approach results in high in-hospital mortality rates and poor short-term survival. Among patients who undergo surgical explantation, postoperative in-hospital mortality has been reported to range from 28% to 47% [8,10].
3. EXPLANT-TAVR Registry: Comparison of Self-Expanding and Balloon-Expandable Valves
The EXPLANT-TAVR international registry provides detailed categorization of the reasons for surgical explantation of transcatheter aortic valves. This registry distinguishes between balloon-expandable valves (BEV) and self-expanding valves (SEV), highlighting notable differences in the indications for explantation between the two device types. The table below outlines the distribution of common indications, such as endocarditis and paravalvular leak, along with the corresponding statistical significance as measured by p-values [5], [Table 1].
Findings from the EXPLANT-TAVR registry show that, among patients with failed SEV, there was a lower rate of urgent, or emergency surgeries and a higher frequency of root replacement procedures compared to those with BEV [Table 2].
According to the EXPLANT-TAVR registry, there were no notable differences in short-term or mid-term mortality and morbidity between BEV and SEV after explantation.
4. Technical Challenges and Expert Insights for TAVR Explantation
Explantation of transcatheter heart valves is a high-risk procedure with specific technical challenges. Patients evaluated for surgical explantation after TAVI failure are often high risk due to prior ineligibility for surgery, significant comorbidities, frailty, challenging anatomy, complex structural issues, previous operations, heavy aortic calcification, or a small aortic annulus. Emerging data—such as from Fukuhara et al.—indicate that even initially low-risk patients experience disproportionately high observed-to-expected mortality when undergoing TAVR explant, underscoring the inadequacy of conventional risk models in this setting [11], [Figure 1].
The Society of Thoracic Surgeons has recently developed updated Adult Cardiac Surgery Risk Calculators, which now incorporate advanced surgical aortic valve replacement evaluations and have been tailored to include patients with a history of prior TAVR procedures [12]. The EuroSCORE II risk score is widely used for assessing surgical risk, but it does not specifically consider the distinct challenges and risks associated with TAVI explantation. Its predictive value for outcomes in this context is, therefore, limited and has been recognized as such.
Previous reports have highlighted that the severe calcification and endothelialization of the transcatheter aortic valve, compounded by the calcification and degeneration of the native valve, can increase the complexity of TAVI surgical explantation. A preoperative contrast-enhanced computed tomography scan (CT) is usually necessary to facilitate a safe surgical explant procedure.
There is limited data comparing earlier versus later interventions. Early TAVI explantation, conducted within one month of the initial procedure, generally enables easier removal of the prosthesis because there is minimal adhesion. In contrast, delayed surgical management—especially following unsuccessful or suboptimal non-surgical approaches such as repeat TAVR—has been associated with less favourable outcomes. This may be due to factors including patient condition, increased device adherence, and the potential requirement for additional procedures [13,14].
The cannulation strategy should be based on the specific TAV type and preoperative CT findings. For supra-annular valves with frames that extend into the ascending aorta, high cannulation in the aortic arch is recommended to provide adequate space for aortic cross-clamping. The TAVI scaffold may reduce available space for placing a cannula or clamp on the ascending aorta, which can lead to the use of peripheral axillary or femoral artery cannulation as an alternative approach [3].
For intra-annular valves, the aortotomy is performed in the standard location, using either a transverse or oblique incision. With supra-annular valves, the aortotomy may be conducted at the top of or within the frame of the valve [3,14].
Self-expanding valves are taller than balloon-expandable valves, often requiring a higher aortotomy for removal due to their larger stent frame. This can hinder visualization of the aortic annular complex and increase the risk of root damage. Conversely, balloon-expandable valves explantation may be more straightforward for surgeons without TAVR experience, as their stent profile resembles surgical aortic valves. This difference may explain the higher rate of aortic root replacement during SEV explantation compared to BEV [5]. BEV frequently exhibits adhesion at the aortic root, while self-expandable devices tend to adhere at the sinotubular junction; additionally, larger aortic diameters are generally associated with reduced adhesions, which facilitates dissection [14].
Standard antegrade cardioplegia is generally appropriate for intra-annular valves, where the stent frame is short. For supra-annular valves, antegrade cardioplegia cannulation should avoid the tall valve prosthesis, which can typically be palpated through the aorta. Retrograde cardioplegia is commonly used in TAVR explants and is often required for initial cardiac arrest in patients with aortic regurgitation. Access to the coronary ostia prior to valve removal is often limited by the small cell openings of the stent frame [3].
The Double Kocher and Roll techniques are utilized for the explantation of BEV, whereas the Tourniquet or Recapture technique is employed for the explantation of SEV. These techniques are intended to minimize tissue damage and decrease the likelihood of further surgical procedures [3,14,15].
The use of ice-cold saline irrigation is not required for nitinol frames [12]. Detaching the device from native or prosthetic aortic valves is usually uncomplicated, since these tissues can withstand manipulation [14].
The majority of patients undergoing TAVI valve explantation typically require a form of aortic root reconstruction, which may include root enlargement, aortic root endarterectomy, or root replacement [16]. Root replacement is most often performed during TAVR-explant for endocarditis with periannular abscess, or when a deeply endothelialized TAVR valve damages the proximal ascending aorta or sinuses during removal.
Deep implantation of valves, especially with earlier-generation transcatheter heart valves, may affect the aortomitral curtain, anterior mitral leaflet, and membranous septum. If these structures are compromised during TAVR explant, subsequent repair such as ventricular septal defect closure or concomitant mitral surgery may be necessary [5]. Importantly, patients requiring concomitant surgery exhibit a higher mortality rate of 23.8% [15].
In the EXPLANT-TAVR registry, 54.6% of patients underwent concomitant procedures, including root repair (4.8%), ascending aortic replacement (12.2%), mitral valve repair or replacement (32.0%), tricuspid valve repair (8.8%), and combined mitral and tricuspid surgery (7.5%). These procedures were associated with higher mortality rates [6]. According to the same registry, mortality following TAVR-explant was associated with prolonged bypass and cross clamp durations, as well as concomitant mitral or tricuspid valve procedures. After TAVR explant, 30-day mortality was 16% and one-year mortality was 33%. [5].
5. The SURPLUS Hybrid Procedure
Surgical Resection of Prosthetic Valve Leaflets Under Direct Vision (SURPLUS) is a hybrid approach in which the transcatheter aortic valve leaflets are surgically excised while the frame of the valve remains intact, followed by direct implantation of a balloon-expandable valve under both direct visualization and fluoroscopic guidance.
SURPLUS prevents tissue dissection during TAVR-explant, reducing aortic or structural injuries and shortening bypass and cross-clamp times. However, this technique is contraindicated for transcatheter valve endocarditis treatment and does not prevent prosthesis-patient mismatch [3].
6. Discussion
Surgical explantation of transcatheter aortic valves even in low-risk patients, can result in significant morbidity and mortality. Although it occurs infrequently, this procedure has reported 30-day mortality rates between 15% and 20%, with higher rates observed when concomitant procedures or endocarditis are involved.
On the other hand, the TAVI in TAVI technique provides a less invasive option for treating patients with failed transcatheter aortic bioprostheses, although it is associated with higher rates of valve malposition, coronary obstruction, and patient-prosthesis mismatch. It is considered a therapeutic alternative for selected patients, particularly those with structural valve degeneration, low risk of coronary obstruction, and the potential for favorable hemodynamic outcomes. However, this approach may not be appropriate for all TAVR recipients due to anatomical factors or the presence of endocarditis. TAVI in TAVI procedure is linked to a higher rate of reintervention; however, it is associated with reduced technical complexity and lower 30-day mortality compared to surgical reoperation [16].
At the NY Valves 2025 symposium, Fukuhara presented an analysis of 4,443 Medicare beneficiaries who underwent TAVI and later received either redo TAVI (n = 2,553) or TAVI explant (n = 1,890) [14]. The 30-day mortality rate was higher for the TAVI explant group compared to the redo TAVI group (15.3% vs 4.9%). In a propensity score-matched analysis including 1,584 patients in each group, survival rates were higher in the TAVI explant arm than in redo TAVI, with survival curves intersecting at 1.8 years (P < 0.001). The risk associated with TAVI explant dropped below that of redo TAVI in 7 months (HR 0.86; 95% CI 0.77-0.97). Additionally, fewer patients who underwent TAVI explantation required a second reintervention compared to those who had redo TAVI (6.2% vs 31.2%; P = 0.01). Stratification by age showed that explantation conferred a significant survival advantage over redo TAVI in individuals aged 65-70 years (beginning at 1.3 years; P = 0.011), while no survival benefit was observed for those aged over 70 years [17].
The lack of standardized protocols and established guidelines for managing TAVI explantation presents a significant clinical challenge. To date, there is limited published data regarding surgical explantation of transcatheter aortic valves. Further studies may help refine surgical strategies and develop evidence-based protocols for this clinical scenario. Prospective multicenter registries could provide additional data on long-term outcomes after TAVI explantation and contribute to the development of standardized surgical approaches [Figure 1].
A multidisciplinary approach—engaging cardiac surgeons, interventional cardiologists, infectious disease experts, and radiologists—is essential for improving diagnosis, management, and outcomes in this high-risk population.
Careful patient selection and prompt intervention remain essential to improving outcomes in this challenging patient population. Comprehensive preoperative planning utilizing CT can minimize the likelihood of iatrogenic injury and streamline procedural execution. In addition, regular post-TAVR monitoring and timely referral to surgical teams are advised to avoid interventions in patients presenting with advanced pathology [3],[Figure 1].
When TAVR explantation is indicated, it is essential for surgeons to be aware of the complex challenges associated with different TAVI device designs, sizes, and the specific anatomical considerations of each patient. A patient-tailored approach is associated with improved surgical outcomes. A thorough understanding of TAVR system characteristics and their interactions with native anatomical structures is required.
Standardizing surgical THV explantation techniques may reduce complications while improving both safety and reproducibility. Furthermore, such standardization facilitates a more efficient learning process. Limiting TAVR-explant procedures to centers of excellence and high-volume institutions may contribute to decreased rates of morbidity and mortality.
Consequently, when evaluating transcatheter aortic valve implantation for younger patients with aortic stenosis, clinicians should be aware that subsequent surgical explantation and replacement of an infected or degenerative prosthesis may present considerable technical challenges. TAVR explantation carries significant surgical risks that must be considered in lifetime management of aortic stenosis.
7. Conclusions
Over the next decade, a rise in complex aortic valve reoperations following TAVI procedures is expected. Clinical assessment and multidisciplinary collaboration are important for selecting suitable TAVR candidates. Heart teams are advised to clearly communicate potential risks of reoperation during shared decision-making with patients. Outcomes following TAVR-explant could improve among lower-risk patients, with careful monitoring, timely referrals, preoperative planning, patient tailored approach and standardized TAVR-explant techniques. Further large-scale studies are required to optimize surgical approaches and develop robust, evidence-based protocols for managing this complex clinical situation.
“Artificial intelligence tools (ChatGPT, OpenAI, San Francisco, CA, USA) were used to assist in the creation of illustrative figures. The authors take full responsibility for the accuracy and content of all materials.”
Author Contributions
Conceptualization, A.V. ,A.A.R. and T.A.; validation, A.V.,A.X.,K.K.,G.N. investigation, A.V.,K.K.,J.S and A.X.; resources, A.V.,A.X.,J.S. and K.K.; data curation, A.V.,G.N. and P.A.Z.; writing—original draft preparation, A.V.,T.A.,A.X.,K.K.,; writing—review and editing, V.A.,A.A.R. and D.I.; visualization, A.V.,PA.Z.; supervision, A.V., T.A., D.I.,J.S.; All authors have read and agreed to the published version of the manuscript
Funding
This research received no external funding
Institutional Review Board Statement
Not applicable
Informed Consent Statement
Not applicable.
Data Availability Statement
Data sharing is not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
TAVR transcatheter aortic valve replacement
TAVI transcatheter aortic valve implantation
BEV balloon-expandable valve
SEV self-expanding valve
STS Society of Thoracic Surgeons
ACC American College of Cardiology
CT Computed tomography
References
- Thourani VH, Leon MB, Makkar R, Ascione G, Szeto WY, Madhavan MV, Kodali SK, Hahn RT, Pibarot P, Malaisrie SC, Kapadia SR, Russo MJ, Herrmann HC, Babaliaros V, Guyton R, Genereux P, Cohen DJ, Park B, Clarke S, Gunnarsson M, Szerlip M, Ternacle J, Leipsic J, Blanke P, Webb JG, Smith CR, Mack MJ. Five- Year Outcomes in Low-Risk Patients Undergoing Surgery in the PARTNER 3 Trial. Ann Thorac Surg. 2025 Mar;119(3):555-566.
- Forrest JK, Yakubov SJ, Deeb GM, Gada H, Mumtaz MA, Ramlawi B, Bajwa T, Crouch J, Merhi W, Wai Sang SL, Kleiman NS, Petrossian G, Robinson NB, Sorajja P, Iskander A, Berthoumieu P, Tchétché D, Feindel C, Horlick EM, Saito S, Oh JK, Jung Y, Reardon MJ; Low Risk Trial Investigators. 5-Year Outcomes After Transcatheter or Surgical Aortic Valve Replacement in Low-Risk Patients with Aortic Stenosis.J Am Coll Cardiol. 2025 Apr 22;85(15):1523-1532. [CrossRef]
- Kaneko T, Bapat VN, Alakhtar AM, Zaid S, George I, Grubb KJ, Harrington K, Pirelli L, Atkins M, Desai ND et al.: Transcatheter heart valve explantation for transcatheter aortic valve replacement failure: A Heart Valve Collaboratory expert consensus document on operative techniques. J Thorac Cardiovasc Surg 2025, 169(3):878-889.
- Durand E, Eltchaninoff H, Tchetche D, Levesque T, Garmendia C, Iung B, Benamer H, Cayla G, Van Belle E, Commeau P, Le Breton H, Cuisset T, Akodad M, Verhoye JP, Beurtheret S, du Chayla F, Leclere M, Gilard M; STOP-AS and France TAVI Investigators; Predictors of Outcomes of Reintervention After Transcatheter Aortic Valve Replacement: FRANCE 2 and FRANCE TAVI Registries N. J Am Coll Cardiol. 2025 Mar 11;85(9):896-907. [CrossRef]
- Zaid S, Kleiman NS, Goel SS et al. Impact of transcatheter valve type on out-comes of surgical explantation after failed transcatheter aortic valve replacement: the EXPLANT-TAVR international registry. EuroIntervention 2024;20: e146–57.
- Bapat VN, Zaid S, Fukuhara S, Saha S, Vitanova K, Kiefer P, Squiers JJ, Voisine P, Pi-relli L, von Ballmoos MW, Chu MWA, Rodés-Cabau J, DiMaio JM, Borger MA, Lange R, Hagl C, Denti P, Modine T, Kaneko T, Tang GHL; EXPLANT-TAVR Investigators. Surgi-cal Explantation After TAVR Failure: Mid-Term Outcomes From the EXPLANT-TAVR International Registry. JACC Cardiovasc Interv. 2021 Sep 27;14(18):1978-1991.
- Pineda AM, Harrison JK, Kleiman NS, Rihal CS, Kodali SK, Kirtane AJ, Leon MB, Sherwood MW, Manandhar P, Vemulapalli S, Beohar N. Incidence and Outcomes of Surgical Bailout During TAVR: Insights From the STS/ACC TVT Registry.JACC Cardi-ovasc Interv. 2019 Sep 23;12(18):1751-1764.
- Malvindi PG, Luthra S, Sarvananthan S, Zingale A, Olevano C, Ohri S. Surgical treatment of transcatheter aortic valve infective endocarditis. Neth Heart J. 2021 Feb;29(2):71-77.
- Calcaterra D, Harris K, Goessl M, Dasari G, Kaur N, Chavez I. Findings of prosthetic valve endocarditis in the balloon-expandable trans-catheter aortic valve: review of the literature and tips of management.J Cardiothorac Surg. 2021 Aug 16;16(1):234.
- Pisani A, Hounat F, Brega C, Borghese O, Braham W, Alkhoder S. Infective endocarditis following transcatheter aortic valve implantation. Ann Cardiol Angeiol (Paris). 2020 Oct;69(4):204-206.
- Fukuhara S, Suzuki T, Deeb GM, Ailawadi G, Patel HJ, Yang B. Clinical outcomes of TAVR explant stratified by original risk profile: insights from 110 TAVR explants. Ann Cardiothorac Surg. 2025 Mar 31;14(2):122-130.
- Τhe Society of Thoracic Surgeons. SAVR after TAVR Risk Calculator. Accessed August 19, 2025. https://www.sts.org/resources/savr-after-tavr-risk-calculator and https://savr-after-tavrriskcalc.research.sts.org/.
- Sakakura R, Fukuzawa M, Sugiyama H, Tani K, Yoshida T, Murakami A, Terai H, Ueyama K. Early surgical explantation of a TAVI valve for severe hemolytic outcomes caused by mild paravalvular leak. Gen Thorac Cardiovasc Surg Cases. 2025 Jul 28;4(1):35.
- Fukuhara, S. Safe late explantation of transcatheter aortic bioprosthesis. Ann Thorac Surg. 2020; 110: e555-e558.
- Kurosaka K, Iino K, Yamamoto Y, Takemura H. Recapture technique for the surgical explantation of an infected self-expanding prosthesis after transcatheter aortic valve re-placement prior to surgical aortic valve replacement. Interdiscip Cardiovasc Thorac Surg. 2025 Jun 4;40(6): ivaf135.
- Ogami T, Ridgley J, Serna-Gallegos D, Kliner DE, Toma C, Sanon S, Brown JA, Yousef S, Sultan I. Outcomes of Surgical Aortic Valve Replacement After Transcatheter Aortic Valve Implantation. Am J Cardiol. 2022 Nov 1; 182:63-68.
- Fukuhara S, Kim KM, Yang B, Romano M, Ailawadi G, Patel HJ, Deeb GM. Reoperation following transcatheter aortic valve replacement: Insights from 10 years’ experience. J Thorac Cardiovasc Surg. 2024 Aug;168(2):488-497.e3.
- Fukuhara, S. TAVR reintervention strategies: unveiling trends and outcomes of redo TAVR and TAVR explant., New York Valves 2025, New York, USA, 25/06/2025.
Figure 1.
Challenges and Indications of surgical transcatheter aortic valve explantation.
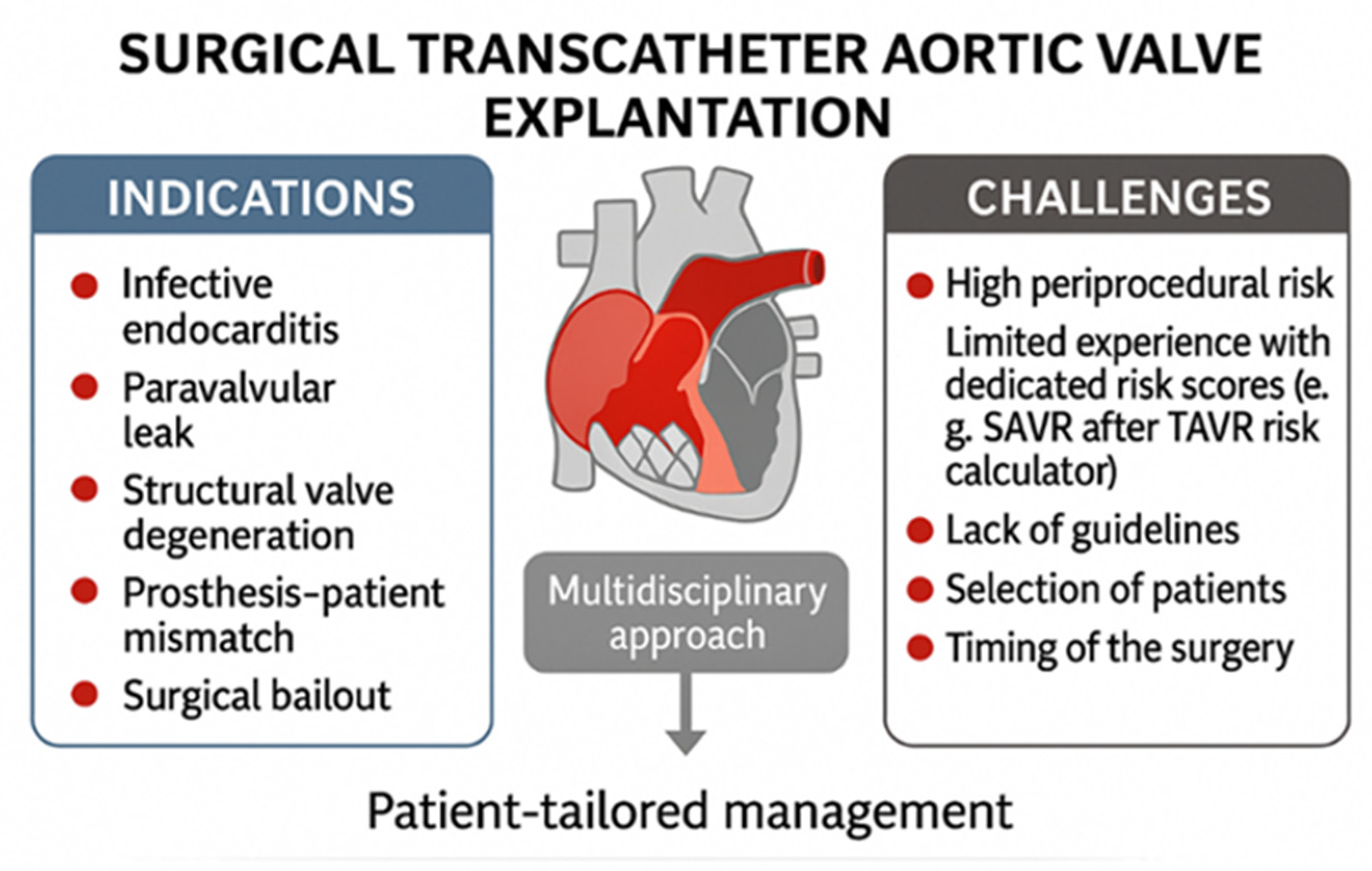

Table 1.
The EXPLANT-TAVR registry distinguishes between balloon-expandable and self-expanding valves in terms of explantation reasons.
Table 1.
The EXPLANT-TAVR registry distinguishes between balloon-expandable and self-expanding valves in terms of explantation reasons.
| Indication | SEV (%) | BEV (%) | p-value |
|---|---|---|---|
| Endocarditis | 36.0 | 55.4 | <0.001 |
| Paravalvular leak | 21.2 | 11.9 | 0.014 |
| Structural valve deterioration | 30.2 | 21.8 | 0.065 |
| Prosthesis-patient mismatch | 8.5 | 10.4 | 0.61 |
Table 2.
The EXPLANT-TAVR registry showed that the SEV valves had fewer urgent or emergency surgeries and more root replacements.
Table 2.
The EXPLANT-TAVR registry showed that the SEV valves had fewer urgent or emergency surgeries and more root replacements.
| Group | Urgent/Emergency Surgeries (%) | p-value (Urgent/Emergency) | Root Replacement (%) | p-value (Root Replacement) |
|---|---|---|---|---|
| SEV | 52.0 | 0.057 | 15.3 | 0.016 |
| BEV | 62.3 | 0.057 | 7.4 | 0.016 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



