
Submitted:
13 September 2025
Posted:
16 September 2025
You are already at the latest version
Abstract
Introduction: Surrogacy is a rapidly evolving area of reproductive health that spans ethical, legal, clinical, and societal dimensions. Policies governing surrogacy vary widely across countries, shaping access to services, safeguarding measures, and the protection of women and children. While some nations permit regulated altruistic or commercial surrogacy, others impose outright bans, creating global disparities and driving reproductive travel. This review examined publicly available surrogacy policies and guidance, with a focus on commissioning decisions, operational processes, and international cross-border complexities. Methods: Following PRISMA guidelines, a systematic search publicly accessible English-language surrogacy policies and guidance documents were identified through a comprehensive search of health service commissioning bodies, government agencies, and professional organisations. Thematic analysis was conducted to explore policy scope, legal frameworks, safeguarding procedures, and international variation. Policies were then compared to assess areas of convergence and divergence across global settings. Results: Globally, surrogacy regulation is highly fragmented. In Europe, most countries prohibit commercial surrogacy and, in some cases, altruistic arrangements, while nations such as the UK, Ireland, and Greece allow tightly controlled altruistic surrogacy. North America shows a patchwork approach, with some US states and Canada permitting altruistic or compensated arrangements under varying levels of regulation. In Asia, historical hubs such as India and Thailand have shifted from permissive commercial surrogacy to restrictive altruistic-only models following concerns over exploitation. Africa remains largely unregulated, except for South Africa’s comprehensive legal framework. Across settings, recurrent themes included safeguarding concerns, ethical debates over exploitation versus autonomy, and challenges in determining legal parentage and nationality. Cross-border arrangements amplify these complexities, often leaving children stateless or without clear legal protections. Conclusion: The absence of harmonised frameworks perpetuates inequities in women’s health and cross-border surrogacy, often exposing individuals to financial, legal, and health risks. These challenges underscore the urgent need for evidence-based policies and fairer, more equitable approaches to surrogacy.
Keywords:
surrogacy
; health policy
; reproductive health
; womens health
; fertility
Background
Surrogacy is an increasingly visible pathway to parenthood, involving an arrangement in which a woman carries and gives birth to a child on behalf of intended parent(s) [1]. While once rare and largely restricted to informal or altruistic arrangements, surrogacy has expanded markedly over the past two decades in response to changing demographic, medical, and social conditions [2]. Rising rates of infertility, delayed childbearing, and advances in assisted reproductive technologies (ART) have created growing demand, particularly among individuals with uterine factor infertility, same-sex couples, and single parents [2,3,4]. Improvements in in vitro fertilisation (IVF), gamete donation, and embryo transfer have made gestational surrogacy feasible and increasingly safe, and international mobility has enabled intended parents to seek arrangements abroad when domestic options are unavailable [5]. Public awareness has also been shaped by the visibility of surrogacy in celebrity culture and social media, which has normalised discussion of surrogacy as a reproductive pathway [6]. Although uterine transplantation offers a potential alternative for individuals with absolute uterine factor infertility, it remains highly restricted due to the cost, scarcity of donors, lifelong immunosuppression, and associated risks, and is therefore not a realistic solution for most patients at present [7,8]. As a result, surrogacy has become a truly global practice, with markets developing in high-income countries such as the United States and Canada, and in low- and middle-income countries (LMICs) such as India, Ukraine, and Kenya, although the regulatory and ethical landscape varies considerably [1].
Two broad types of surrogacy are recognised: traditional surrogacy, in which the surrogate’s own oocytes are used, and gestational surrogacy, in which the surrogate has no genetic link to the child. Within these types, arrangements are further categorised as altruistic, where only reasonable expenses are reimbursed, or commercial, where the surrogate receives additional payment [9]. Globally, these models are unevenly distributed: commercial surrogacy is permitted in certain US states, Ukraine, and Georgia, while altruistic surrogacy predominates in countries such as the United Kingdom (UK), Australia, and Canada [10,11]. However, these opportunities are not equally accessible. Strict eligibility rules, financial costs, immigration restrictions, and the patchwork of legal recognition limit who can benefit from surrogacy [12]. For instance, while gestational surrogacy in the US is highly regulated and offers legal certainty, it is prohibitively expensive for most [13]. In contrast, lower-cost options in LMICs have historically attracted international intended parents but have often raised concerns about exploitation and inequitable treatment of surrogates. This global variability reinforces existing health and social inequalities, as access to surrogacy is often contingent on wealth, geography, and citizenship [1,2,12].
Surrogacy raises complex ethical and governance issues that cut across reproductive autonomy, safeguarding, and human rights [2,12]. Key concerns include the potential exploitation of women in resource-constrained settings, the commodification of children, informed consent, and the enforceability of agreements. Safeguarding challenges arise when surrogates are exposed to coercion, inadequate medical care, or stigma within their communities [1,2,4,12]. At the same time, intended parents and children may face uncertain legal parentage, difficulties in securing nationality, and psychosocial challenges if disputes occur [14,15]. Globally, legislation is fragmented: some jurisdictions, such as Sweden and France, prohibit all forms of surrogacy [16]; others, such as the UK, allow only altruistic models with non-enforceable agreements [17]; while countries such as the Ukraine and select US states permit commercial surrogacy with detailed contractual frameworks [2,10,13]. International human rights discourse has emphasised the need to protect the dignity, autonomy, and health of surrogates while safeguarding the rights of children to legal identity and family life [18]. Yet, without harmonised frameworks, inconsistencies persist, particularly in cross-border cases where national laws may conflict and leave children in legal limbo [2,12].
Rationale
Given this complex backdrop, there is a pressing need to synthesise and critically appraise the policies governing surrogacy globally. While the expansion of surrogacy reflects societal change and medical progress, the limited number of formal policies available, particularly in the English language, means much of the accessible information resides in disparate websites, clinical guidance, or fragmented commissioning statements. The lack of clarity creates challenges for clinicians, policymakers, and families navigating these pathways. A systematic review of surrogacy policies allows for a structured comparison of themes such as commissioning stance, ethical considerations, safeguarding provisions, and legal mechanisms for establishing parentage. By isolating surrogacy-specific elements, this review provides evidence on commonalities and divergences in governance across health systems and jurisdictions. The findings aim to inform debate on the balance between reproductive choice and protection of vulnerable parties, highlight areas of policy coherence and gaps, and guide future research, practice, and legislation.
Methods
Eligibility Criteria
All policies, guidance documents, and commissioning statements that explicitly referred to surrogacy in the context of assisted conception published in English between the 1st of January 1990 and the 1st of August 2025 were included. Both national-level and local-level policies, as well as statutory and operational guidance, provided that they addressed commissioning, regulation, safeguarding, or legal aspects of surrogacy. Documents focusing solely on IVF or assisted conception without mention of surrogacy were excluded, as were media reports and commentary pieces.
Information Sources
A systematic search was conducted between March and August 2025. Primary sources included the websites of Integrated Care Boards (ICBs) and former Clinical Commissioning Groups (CCGs) in England, alongside national governmental portals such as GOV.UK, HM Passport Office (HMPO), and the Human Fertilisation and Embryology Authority (HFEA). Searches were also undertaken on PubMed, Google Scholar, and world health organisation (WHO) databases to identify additional policies, statutes, and professional guidance documents. Snowball searching was performed using the reference lists and linked resources within identified documents to maximise coverage.
Search Strategy
Searches were conducted using combinations of keywords including “surrogacy policy,” “surrogacy commissioning,” “assisted conception surrogacy,” “NHS surrogacy,” “HM Passport Office surrogacy,” and “surrogacy guidance UK.” Advanced search operators were applied in Google and Google Scholar to limit results to English-language and policy-specific documents across Asia, Africa, Oceania, South and North America. Search results were exported into EndNote, and duplicates were removed before screening.
Selection Process
Two reviewers independently screened titles and abstracts of documents for eligibility. Full texts were then reviewed in duplicate to confirm inclusion. Discrepancies were resolved through discussion, with arbitration by a third reviewer if consensus was not reached. A PRISMA flow diagram (Supplementary Figure S1) was used to document the screening and selection process, including reasons for exclusion at the full-text stage.
Data Collection Process
A standardised extraction form was developed and piloted on two policies. Extracted data included: jurisdiction, issuing body, year of publication, scope of policy, commissioning stance, legal framework referenced, definitions of surrogacy, ethical or safeguarding considerations, and links to related fertility policies. Data extraction was conducted independently by two reviewers, with results compared and discrepancies resolved through consensus.
Data Items
The main outcomes of interest were the presence and content of surrogacy-specific commissioning positions, definitions and classifications of surrogacy, safeguards and ethical principles, and references to legislation or international frameworks. Additional data items included the explicit inclusion or exclusion of related costs (e.g., legal, travel, or surrogate expenses), the scope of maternity support for surrogates, and the administrative pathways for parentage transfer or nationality determination.
Study Risk of Bias Assessment
As this review analysed policy documents rather than clinical trials or observational studies, conventional risk of bias tools were not applicable. Instead, we assessed the completeness, transparency, and accessibility of each document, noting whether policies were current, whether consultation processes were documented, and whether they provided sufficient operational detail to inform practice.
Synthesis Methods
We employed a thematic and contextual analysis to synthesise findings across the identified documents. Thematic analysis involved inductive coding of policy content into major domains such as commissioning stance, legal framework, ethical considerations, safeguarding, and cross-border arrangements. Contextual analysis compared how these themes were framed across different issuing bodies, highlighting convergences and divergences. Data were presented narratively, supported by thematic tables to illustrate recurring patterns and contrasts between local and national guidance.
This conceptual framework (Figure 1) was developed through a thematic and contextual analysis of global surrogacy policies, enabling the identification of recurring themes and their relationships within diverse legal and cultural settings. Thematic analysis involved systematically coding policies to reveal core domains, such as ethical considerations, surrogacy models, and child welfare. Contextual analysis then explored how these domains are shaped by broader societal factors, including religion, economics, and human rights frameworks. By integrating these approaches, the framework provides a comprehensive visual representation of how ethical debates influence whether surrogacy is banned or regulated, how financial models shape accessibility and risk, and how legal systems respond to protect children and families. This combined methodology ensures that the framework reflects both the structural patterns in policy and the nuanced socio-political contexts that drive surrogacy practices globally.
Results
Surrogacy-specific policies and guidance documents were identified that were publicly available in English (Table 1), spanning local commissioning policies and national operational guidance. The relatively small number reflects the limited commissioning remit of National Health Service (NHS) bodies, where surrogacy is consistently treated as outside routine funding, resulting in fewer standalone documents compared with broader assisted conception policies. In contrast, a larger volume of information was found on government and professional body websites, where operational detail, statutory interpretation, and public-facing advice are more comprehensively set out than in the short commissioning statements issued by ICBs or CCGs.
Thematic Analysis
Commissioning Stance and Scope
Across English commissioning policies reviewed, assisted conception involving surrogacy is not routinely commissioned. Derby & Derbyshire (EMACC - East Midlands Assisted Conception Collaborative) states [19] that treatments “involving surrogates for any patient group should not routinely be commissioned,” with no funding for any element specific to surrogacy, no payments to surrogates, and no involvement in recruiting surrogates; limited recourse is via Individual Funding Requests (IFR), where “exceptionality” is narrowly defined and unlikely when an identifiable cohort could benefit similarly. Gloucestershire ICB [20] mirrors this position that surrogacy is not supported or funded, and additionally specifies that it will not fund surrogate expenses, legal costs, treatments abroad, or transport. Notably, it clarifies that maternity care for surrogates continues and links to its assisted conception and fertility preservation policies for adjacent care.
Legal Framework and Definitions
Policies converge on the UK’s legal architecture: altruistic surrogacy (reasonable expenses only) is lawful; commercial surrogacy is prohibited; surrogacy agreements are not legally enforceable; the surrogate is the legal mother at birth; and transfer of parentage requires a parental order under the HFEA 2008 [21], with the Surrogacy Arrangements Act 1985 [22] providing the basic framework. HMPO guidance [23] reinforces these points for identity and nationality decisions and distinguishes gestational and traditional surrogacy.
Ethical, Medico-Legal Risk and Safeguarding
Commissioners cite substantial medico-legal exposure (e.g., consent disputes, uncertainty over lawfulness of arrangements) and ethical risks (surrogate keeping the child, rejection of the child by either party, decision-making conflicts, and long-term psychological effects) as central reasons for non-funding. HMPO operational guidance [24] embeds safeguarding and vulnerability checks, including watchlist screening of the child, surrogate and commissioning parents, and explicit referral pathways to the Child Protection and Safeguarding Team where indicators arise.
Parentage Transfer, Nationality and Administrative Pathways
HMPO [23] sets out documentary routes to establish a child’s British nationality, including cases with and without a parental order, and accepts evidence from overseas, including where the underlying arrangement was commercial for the purposes of nationality assessment, while remaining neutral on expenses a matter for the courts. Where urgent travel is needed, HMPO [23] describes coordinated processes with the Foreign, Commonwealth & Development Office (FCDO) for Emergency Travel Documents (ETDs), including evidential requirements and case-noting [23].
Cross-Border Complexity
All documents acknowledge the lack of international harmonisation and the administrative complexity of inter-country surrogacy. HMPO guidance [23] operationalises this complexity by describing step-wise handling when no UK parental order exists and by detailing workflows for ETDs and continued case management until nationality/consent and safeguarding are satisfactorily resolved. Together, these findings demonstrate a high degree of policy coherence in commissioning exclusions, complemented by HMPO’s downstream guidance. Table 2 provides a consolidated overview of these themes, showing how different policy sources align or diverge in scope.
Contextual Analysis
These policies reveal a deliberate boundary between health-service commissioning and family law. ICBs/CCGs [19,20] emphasise resource stewardship and risk containment, declining to fund surrogacy-specific interventions while permitting IFRs in strictly exceptional circumstances; the logic is grounded in ethical and legal uncertainty and institutional limits in validating private arrangements. In parallel, the state still must regularise the child’s status: HMPO [24] cannot ignore outcomes of surrogacy (domestic or overseas) and must assess nationality, identity and consent with robust safeguarding even where NHS commissioning would not have funded the upstream clinical steps. Gloucestershire’s [19] explicit continuation of antenatal and postnatal support for surrogates underscores that while surrogacy creation is out-of-scope, routine maternity care remains in-scope.
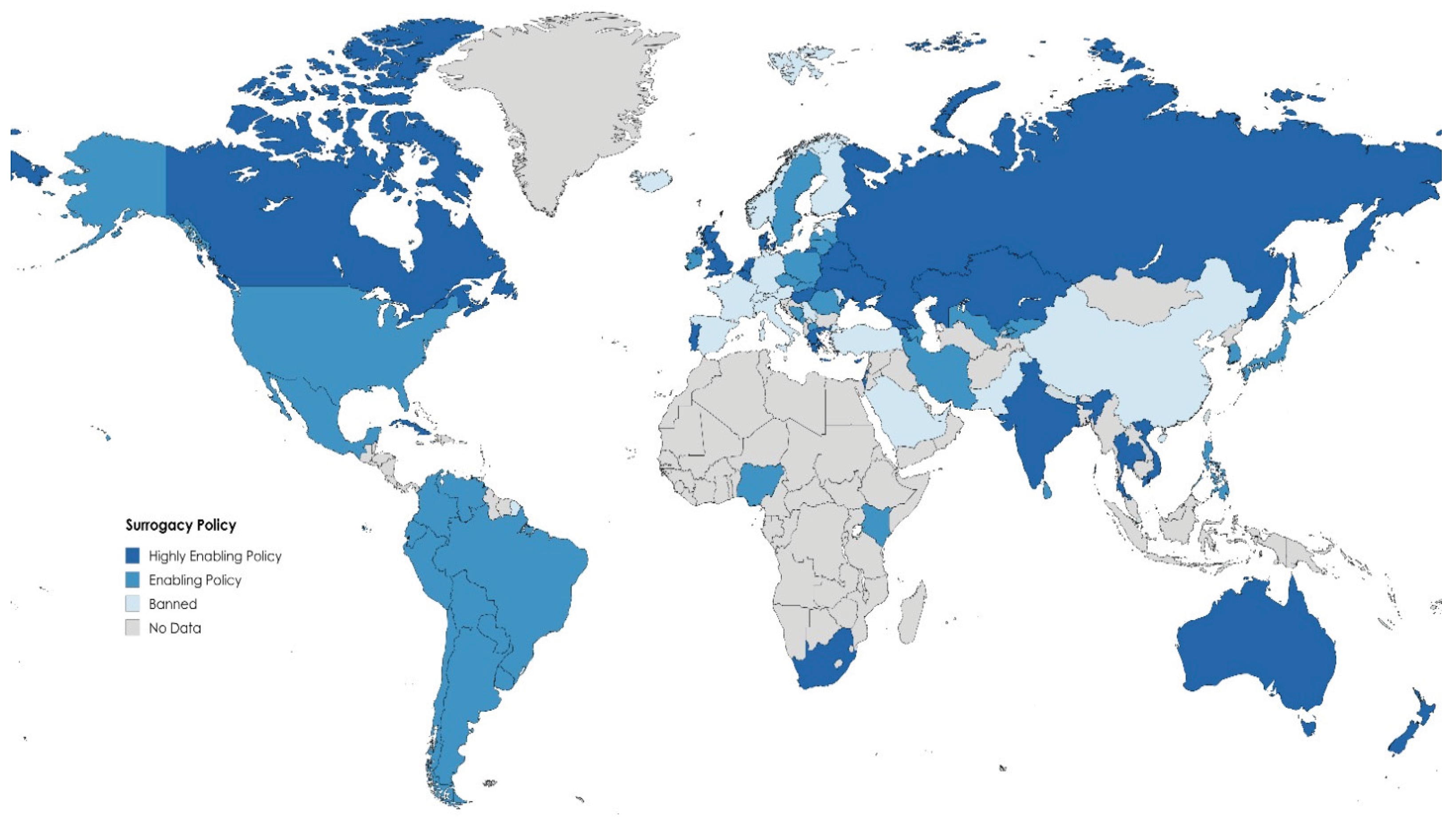
Surrogacy policies across the globe reveal a strikingly uneven and often polarised landscape shaped by cultural norms, ethical beliefs, economic realities, and political priorities. In Europe [16], regulation is largely restrictive, with all EU member states prohibiting commercial surrogacy under the shared principle that the human body should never be a source of financial gain. Many Western European nations, including France, Germany, Italy, Spain, and Portugal, extend these prohibitions to all forms of surrogacy, criminalising even altruistic arrangements [16]. In these jurisdictions, surrogacy contracts are deemed legally void, and participation can result in criminal prosecution. Italy has gone further, enacting legislation in 2024 to punish citizens who travel abroad to engage in surrogacy, thus extending its domestic ban beyond national borders [25]. However, not all European countries take this absolutist stance. The UK has allowed altruistic surrogacy since the Surrogacy Arrangements Act of 1985 [22], though it tightly controls the process by prohibiting advertising, profit-making, and enforcing post-birth transfer of legal parenthood through a Parental Order. Similar regulated altruistic frameworks exist in Ireland, where the 2024 Health (Assisted Human Reproduction) Act [26] establishes a legal framework for surrogacy, providing protections for intended parents, surrogates, and children, and allowing legal recognition of surrogacy arrangements for the first time. Greece has been a pioneer since 2002, permitting altruistic surrogacy even for foreign intended parents under strict judicial oversight [27]. Cyprus follows a similar regulated model [28], while Portugal’s journey has been fraught with constitutional challenges. Although Portugal has faced constitutional challenges: although laws permit surrogacy in limited medical circumstances, repeated interventions by the Constitutional Court have stalled full implementation, leaving the process technically legal but practically inaccessible [29]. Other European countries, such as Denmark, Belgium, and the Netherlands, adopt a grey-area approach where altruistic surrogacy occurs informally without criminalisation but also without enforceable contracts [16]. In stark contrast, Russia historically permitted both domestic and international commercial surrogacy, establishing itself as a key global hub until 2022, when foreign participation was banned amidst growing concerns about exploitation [30]. Ukraine, before the Russian invasion, had a well-developed commercial surrogacy sector with clear laws recognising intended parents on birth certificates, but the war highlighted the fragility of international arrangements when many infants were left stranded in conflict zones [30].
In North America, the US lacks a federal legal framework, resulting in a patchwork of state-level policies [31]. States such as California and Illinois fully support compensated surrogacy through enforceable contracts, attracting international clients, while others, like Michigan, have historically criminalised it altogether, only decriminalising the practice and allowing enforceable surrogacy contracts from April 1, 2025. [13]. Recent reforms, including New York’s 2021 Child-Parent Security Act [32], illustrate a slow trend towards broader legalisation and regulation. Canada, by contrast, has a uniform national law, the Assisted Human Reproduction Act 2004, which permits only altruistic surrogacy and prohibits payment beyond reasonable expenses. Despite this, enforcement of expense rules is inconsistent, and surrogacy continues to be practised widely through informal arrangements [33].
In Latin America, surrogacy policies are fragmented and fluid. Brazil allows altruistic surrogacy, only within families, under strict medical guidelines, explicitly forbidding commercial surrogacy contracts [34]. Mexico presents a complex picture, with some states historically permitting commercial surrogacy for foreigners, most notably Tabasco, until concerns over exploitation prompted restrictions limiting surrogacy to Mexican citizens on an altruistic basis [35]. Colombia allows commercial surrogacy but has lacked comprehensive legislation, leading to unregulated practices that recently prompted proposals for tighter oversight [36]. Argentina illustrates the volatility of surrogacy regulation: a 2017 court ruling opened the door to both domestic and international arrangements, but subsequent scandals involving trafficking and exploitation triggered emergency measures in 2024, halting registrations and sparking debate over whether to regulate or ban surrogacy entirely [37]. Across the region, many countries, such as Uruguay, explicitly prohibit surrogacy, while others, like Peru and Chile, remain silent on the issue, resulting in legal uncertainty.
Asia has been the epicentre of global “fertility tourism”[5]. In the early 2000s, India became the world’s leading surrogacy hub, with thousands of foreign couples commissioning surrogates annually [5,38]. However, mounting evidence of exploitation led to sweeping reforms: the Surrogacy (Regulation) Act 2021 banned commercial surrogacy and limited altruistic surrogacy to Indian married couples with demonstrated medical need [38]. Similar reversals occurred in Thailand and Nepal, both of which initially flourished as international surrogacy destinations before implementing outright bans [39,40]. Cambodia briefly became a fallback hub before abruptly criminalising surrogacy in 2016, leaving many babies and intended parents in legal limbo [41]. China maintains a strict prohibition on all forms of surrogacy, with underground practices emerging and Chinese citizens increasingly seeking services abroad [42]. Japan lacks explicit laws but effectively blocks domestic surrogacy through medical guidelines, while South Korea treats commercial surrogacy as illegal and fails to recognise altruistic arrangements [43]. Vietnam offers a rare example of a carefully controlled altruistic model, limited to close family members [44]. In the Middle East, Iran stands out for its permissive stance, rooted in Shia Islamic jurisprudence that allows compensated surrogacy under religious oversight. This contrasts sharply with Sunni-majority nations such as Saudi Arabia and Egypt, which ban surrogacy entirely [4]. Israel also permits altruistic surrogacy under robust state regulation, gradually expanding eligibility to include single men and same-sex male couples by 2022 [45]. In the Caucasus region, Georgia and Kazakhstan have capitalised on demand by establishing fully legal commercial surrogacy industries, becoming prominent international destinations following restrictions elsewhere in Asia [46].
In Africa, surrogacy remains rare and largely unregulated, with South Africa providing the continent’s only comprehensive legal framework [47]. Under the Children’s Act 2005, altruistic surrogacy is permitted but requires High Court approval before pregnancy and prohibits compensation beyond expenses, ensuring a child-centric, ethically grounded approach [47]. Elsewhere, including Nigeria, Ghana, and Kenya, surrogacy occurs informally through private clinics without clear legal protections, creating uncertainty and ethical risks. Many North African countries, influenced by Islamic law, ban surrogacy outright, viewing it as incompatible with religious and familial norms [2].
This indicates profound disparities in how surrogacy is conceptualised and governed. Countries with permissive regimes tend to frame surrogacy as a contractual reproductive service, prioritising individual autonomy and market dynamics, while restrictive countries highlight the protection of women and children from commodification and exploitation. These divergent philosophies drive reproductive travel, as intended parents cross borders to access services unavailable at home, often creating complex legal entanglements around citizenship, parentage, and safeguarding. The result is a patchwork system in which the fate of surrogates, intended parents, and children hinges on geography, underscoring the urgent need for harmonised, rights-based global governance.
The global landscape of surrogacy policy is shaped not only by government laws but also by the positions of healthcare organisations, human rights bodies, and advocacy groups. While the World Health Organisation (WHO) has no formal surrogacy policy, it recognises surrogacy as part of assisted reproductive technologies and stresses safeguarding the health of surrogate mothers and children, alongside preventing practices that could constitute the sale of children [48]. Similarly, the International Federation of Gynecology and Obstetrics (FIGO) and national medical associations emphasise strict informed consent and protection against exploitation [49]. For instance, the American Society for Reproductive Medicine (ASRM) and Canadian Fertility and Andrology Society issue guidelines on screening surrogates and reimbursing expenses [50,51], while Brazil’s Federal Medical Council regulates altruistic surrogacy through clear ethical rules [52]. Human rights bodies have highlighted potential harms linked to unregulated surrogacy. In 2018, a United Nations (UN) Special Rapporteur warned that some international practices may equate to child trafficking, prompting the United Nations Children’s Fund (UNICEF) and the non-governmental organization (NGO) Child Identity Protection to call for global safeguards [53]. Their 2023 briefing urged countries to protect surrogacy-born children’s rights by preventing statelessness, ensuring the right to know one’s origins, and regulating cross-border surrogacy so that citizens cannot circumvent domestic bans by seeking services abroad [53].
Among NGOs, there is a deep ideological division. The Alliance Defending Freedom (ADF) International and some women’s rights groups advocate for a global ban, arguing that commercial surrogacy commodifies women and children and fuels exploitation, often shifting to poorer countries until laws catch up [54]. In contrast, fertility advocacy groups and LGBTQIA+ organisations push for regulated, inclusive frameworks to enable family-building while preventing abuse [55]. Legal scholars also suggest moving beyond traditional family law to integrate elements of labour and contract law, thereby better protecting all parties [56].
This dialogue reflects a broader global trend: while some nations continue to permit commercial surrogacy, many are tightening regulations or restricting the practice, especially in response to cross-border complexities and human rights concerns (Table 2).
The documents show high policy coherence in not commissioning surrogacy-specific assisted conception in England, justified by medico-legal exposure, ethical risk, and affordability. While access via IFRs theoretically exists for exceptional cases, approvals for surrogacy are extremely rare [19,20,24]. In contrast, Wales permits commissioning under certain conditions [57]. The legal baseline across the UK is consistent: altruistic (expenses-only) arrangements are lawful, commercial surrogacy is prohibited domestically, agreements are not legally enforceable, the surrogate is considered the legal mother at birth, and parentage is transferred through court-issued Parental Orders. HMPO’s 2025 guidance [23] complements this by detailing nationality, consent and safeguarding pathways, including where there is no parental order and in commercial overseas cases and by outlining FCDO ETD procedures for urgent travel, thereby operationalising child-centred status resolution irrespective of commissioning decisions. Gloucestershire [20] additionally clarifies ongoing maternity care for surrogates and linkages to adjacent fertility policies. Overall, there is a clear upstream/downstream split: commissioners avoid underwriting creation pathways, while HMPO and courts regularise outcomes with robust safeguards for the child [23].
Ethical Debate: Exploitation vs. Autonomy
At the heart of global surrogacy policy lies a fundamental ethical tension between perceptions of exploitation and the defence of personal autonomy. Many countries with restrictive frameworks regard surrogacy, particularly commercial arrangements, as an affront to human dignity [2,11]. Religious leaders, including Pope Francis, have condemned surrogacy as a “violation of the dignity of the woman and the child,” likening it to a system that preys upon the poor [58]. This position is reflected in European Union directives and international conventions, which emphasise the prevention of the commodification of women’s bodies and the sale of children. Similarly, advocacy groups such as ADF International argue that surrogacy constitutes a form of reproductive trafficking, highlighting the power imbalances between wealthy intended parents and economically vulnerable surrogates [54].
Conversely, countries with permissive policies, alongside advocacy groups supporting reproductive rights, emphasise women’s autonomy and the right to form a family [12]. They argue that surrogacy, when conducted ethically, allows individuals unable to conceive to achieve parenthood, while empowering surrogates to make informed choices about their bodies [59]. Research from regulated environments suggests that many surrogates experience a sense of fulfilment and psychological reward from helping others, challenging narratives of universal exploitation. Critics of outright bans accuse opponents of focusing on extreme cases of abuse, thereby ignoring evidence that well-regulated surrogacy can be safe and beneficial [12,60]. This ethical divide strongly influences policymaking: nations prioritising protection from exploitation tend to impose total bans or limit surrogacy to altruistic, unpaid arrangements, while those prioritising autonomy are more inclined to permit compensated surrogacy within robust regulatory frameworks.
Commercial vs. Altruistic Surrogacy
Debates about exploitation and autonomy manifest most clearly in the distinction between commercial and altruistic surrogacy. The dominant global model is to prohibit commercial surrogacy while permitting altruistic arrangements where only “reasonable expenses” are reimbursed [10,11]. Countries such as the UK, Canada, Australia, Denmark, and Brazil adhere to this principle, seeking to prevent financial incentives from coercing women into surrogacy [16,61,62]. However, these altruistic systems face significant challenges. The absence of compensation often limits the number of available surrogates, creating long waiting times and incentivising informal or under-the-table payments. Determining what qualifies as a “reasonable expense” can also be contentious, as illustrated by legal disputes in the UK where courts have had to retrospectively approve payments that verge on compensation.
In contrast, certain jurisdictions, including some US states, Georgia, Ukraine, and Russia, openly allow commercial surrogacy [2,10,11], viewing it as a contractual service. Here, surrogates may receive substantial compensation, and the relationship between intended parents and surrogates is explicitly transactional. Some scholars argue that commercial surrogacy should be treated as a form of labour, suggesting that labour law and workplace protections, such as maternity insurance and regulated working conditions, could better safeguard surrogates. This approach reframes surrogacy as a legitimate form of reproductive work rather than a private family matter. Globally, there remains little consensus, and the debate reflects deeper societal values about whether reproduction should be part of the market economy or remain strictly within the realm of personal relationships [4,5,9,12].
Legal Parentage and Best Interests of the Child
Determining legal parentage is a complex and sensitive issue that lies at the core of surrogacy policy. In many jurisdictions, the woman who gives birth is automatically recognised as the legal mother, creating potential conflicts with the intended parents’ rights. Approaches to resolving this vary considerably. In countries such as the UK and South Africa [47,61], intended parents must apply for a court-issued parental order or pre-birth approval before legal parentage can be transferred. Other nations, including many US states and the Ukraine, directly recognise the intended parents on the birth certificate from the outset, simplifying the process and providing immediate clarity [13,30].
The welfare of the child is paramount. Judicial oversight, as seen in Greece and Portugal, is often used to ensure that surrogacy arrangements serve the best interests of the child [27,29]. However, in countries lacking clear legal frameworks, children can be left in precarious situations, such as being unable to obtain citizenship or travel documents, leading to cases of statelessness. These challenges have prompted calls from organisations like UNICEF and Child Identity Protection for international agreements to guarantee that all children born through surrogacy have secure legal parentage and nationality [48,53].
Another key consideration is the alignment of surrogacy laws with existing adoption rules. Payments to surrogates may be interpreted as paying for a child, potentially breaching international adoption standards such as the Hague Convention. While all countries prohibit the outright sale of children, they differ in whether regulated payments constitute baby-selling. Furthermore, there is growing recognition of the child’s right to know their genetic and gestational origins, with some jurisdictions beginning to introduce systems similar to open adoption. Yet, this remains unevenly implemented, leaving many children without access to crucial information about their identity.
Comparative Analysis
Across the policies reviewed, there is strong alignment in the commissioning stance of Derby & Derbyshire (EMACC) [19] and Gloucestershire ICB [20], both of which categorically exclude NHS funding for surrogacy-specific assisted conception [19,20], citing medico-legal uncertainty, ethical risk, and resource stewardship. While EMACC emphasises non-involvement in surrogate recruitment and refusal to cover any expenses, Gloucestershire expands on this by explicitly excluding legal, transport, and overseas treatment costs, while simultaneously clarifying that maternity care for surrogates remains available, thereby offering greater transparency on service boundaries [19,20]. In contrast, the HMPO guidance addresses the downstream consequences rather than the commissioning stage, focusing on establishing parentage, nationality, and safeguarding procedures for children born through surrogacy [23]. Unlike commissioning bodies that adopt a restrictive, risk-averse stance, HMPO provides structured pathways even for cases involving overseas and commercial surrogacy, demonstrating a complementary role: while ICBs manage upstream treatment access, HMPO ensures that outcomes are legally recognised and that children’s welfare and nationality rights are protected [23].
Figure 2.
Global distribution of Surrogacy policies.
Discussion
The findings of this review reveal a strikingly narrow and restrictive approach to surrogacy within English commissioning policies, with both Derby and Derbyshire (EMACC) [19] and Gloucestershire [20] ICB explicitly excluding surrogacy-related assisted conception from routine NHS funding. While these positions are consistent, they provide only high-level statements with limited operational detail, leaving significant ambiguity for patients and clinicians. In contrast, HM Passport Office guidance [23] illustrates the practical complexities that arise once a child is born, particularly in cross-border cases, where parentage, nationality, and safeguarding must be resolved despite the absence of upstream commissioning support. The limited number of publicly available surrogacy-specific policies in English, and the heavier reliance on supplementary government and professional body websites, underscores the fragmented and incomplete nature of the evidence base. This scarcity of detailed, formalised documents represents a major limitation, as it risks leaving stakeholders without comprehensive guidance and perpetuates inequalities in access to safe and regulated surrogacy pathways.
Women’s Health Implications
From a women’s health perspective, the findings underscore deep inequities in access to surrogacy services. In countries such as the US and Canada, surrogacy is more widely regulated and often legally secure, yet it remains prohibitively expensive for most women and couples [13,51]. Accessing these policies remains challenging as it is often maintained in non-digital formats. Conversely, in LMICs where costs are lower, concerns about exploitation, limited safeguarding, and inadequate medical oversight place surrogates at heightened risk of harm [1,2,12]. In England, the absence of commissioning support reflects a cautious, risk-averse stance that limits access to those with financial resources to pursue private or cross-border arrangements. By contrast, Wales permits commissioning of surrogacy-related treatment under defined conditions [57]. This divergence within the UK highlights a broader global tension: surrogacy can empower women through reproductive choice and autonomy [2,11], but it may simultaneously expose others to heightened vulnerability and health risk. Without harmonised governance, women’s health outcomes will continue to diverge along socioeconomic and geographic lines.
Societal Implications
The societal implications of surrogacy extend beyond the individual surrogate or commissioning parent, touching on debates about family structures, reproductive justice, and social stratification. Surrogacy challenges traditional notions of motherhood and parentage, raising complex ethical questions about the commodification of reproduction and the rights of children. The evidence suggests that policies often reflect societal discomfort, privileging restrictive stances over proactive regulation. In contexts where surrogacy is prohibited or under-regulated, informal or cross-border markets flourish, often disproportionately involving women from lower socioeconomic backgrounds who are vulnerable to coercion and inadequate legal protection and heightened medical and psychological risk. For example, double embryo transfer is widely undertaken in less-regulated jurisdictions, increasing the risk of multiple pregnancy, prematurity, and neonatal complications [63]. Surrogates also face a higher risk of severe maternal morbidity, including preeclampsia and postpartum haemorrhage [64], alongside increased rates of depression and new-onset mental illness during or after pregnancy [65,66]. Societies that fail to address these disparities risk entrenching inequities in reproductive opportunity and child welfare, while also fuelling a market where wealthier families access services abroad and poorer women absorb the risks.
Social and cultural factors play a central role in shaping surrogacy laws and policies worldwide. Religious beliefs strongly influence regulation: orthodox Roman Catholic doctrines, which uphold the sanctity of natural procreation [58], underpins outright bans in countries such as Italy [25], and much of Latin America [67], while Sunni Islamic teachings similarly oppose third-party reproduction, leading to prohibitions across most of the Middle East [2,4]. In contrast, Shia-majority countries like Iran have permitted surrogacy under religious rulings [4]. Gender norms and feminist perspectives add further complexity, with some feminists supporting surrogacy as a form of reproductive choice, while others view it as exploitation rooted in patriarchal systems [68]. The level of societal acceptance of LGBTQIA+ families is another determinant; nations more open to diverse family structures, such as Ireland and Israel, have expanded access to surrogacy for same-sex couples [16,45], whereas more traditional societies often restrict it to heterosexual, married couples, as seen in Ukraine, Georgia, and the US. [13,30,69]. for example, Louisiana in the U.S., which under HB 1102 explicitly limits gestational surrogacy to married heterosexual couples using their own egg and sperm, thereby excluding same-sex couples [70]. Demographic pressures, including declining birth rates in some East Asian countries, have sparked debates about legalising wider fertility options, though cultural conservatism in countries like Japan and Singapore has so far maintained restrictions [71,72]. These values influence individuals directly: in conservative settings, women who act as surrogates may face stigma and secrecy, while in more liberal contexts, surrogates may share their experiences openly, shaping policy discourse. Public opinion also plays a powerful role; societies that perceive surrogacy as “baby-selling” tend to favour bans, while those that see it as altruistic generosity are more supportive [15,73]. Media coverage and high-profile cases, such as celebrity surrogacy stories in China [74] and the United States [75], can further shift societal attitudes. Legal systems often reflect these cultural divides through constitutional rulings and “public order” provisions [42]. For example, France nullifies surrogacy contracts as incompatible with national values, while Portugal’s Constitutional Court has allowed altruistic surrogacy under strict safeguards [14,16,29]. Internationally, these cultural variations make consensus difficult, with forums like the Council of Europe acknowledging the ethical challenges of surrogacy but stopping short of a unified position [16].
Clinical Implications
Clinically, these findings have significant consequences for practitioners and patients navigating surrogacy, especially in the context of cross-border arrangements. Intended parents travelling to countries with permissive commercial surrogacy markets must contend with differences in clinical standards, informed consent procedures, and maternal care provision. Surrogates in under-regulated environments may face compromised antenatal care, inadequate safeguarding, and long-term health consequences that are poorly documented or supported. For clinicians in the UK and elsewhere, this creates complex care responsibilities, from managing the medical needs of surrogates domestically to providing postnatal care for infants born abroad. Looking forward, global women’s health policy must prioritise harmonised frameworks that balance reproductive autonomy with robust safeguarding and legal clarity. This will require high-quality research to evaluate health outcomes for surrogates and children, as well as evidence-based policies that reduce exploitation while widening equitable access to safe surrogacy practices.
Conclusions
This review demonstrates that surrogacy policies remain limited in scope, restrictive in commissioning, and fragmented across national and international contexts. While safeguarding and legal clarity are prioritised in national guidance, there remains insufficient operational detail to ensure equitable access and consistent protection for surrogates and children. Global disparities reveal that surrogacy can both empower and endanger women, depending on governance and socioeconomic context. To advance women’s health and reproductive justice, more robust evidence and harmonised policy frameworks are urgently required.
Supplementary Materials
The following supporting information can be downloaded at: Preprints.org.
Availability of Data and Material
Publicly available data was used within this manuscript
Code Availability
Not applicable
Author Contributions
GD developed the ELEMI program and conceptualised this paper as part of the KATHERINE project. GD wrote the first draft and furthered it by all other authors. MH, GD, NR, EL and NW conducted the searches and extracted the data. All authors critically appraised, reviewed, and commented on all versions of the manuscript. All authors read and approved the final manuscript.
Funding
Unfunded
Ethics Approval
Not applicable
Consent to Participate
No participants were involved in this paper
Consent for Publication
All authors consented to publish this manuscript
Acknowledgements
Not applicable
Conflicts of Interest
All authors report no conflict of interest. The views expressed are those of the authors and not necessarily those of the NHS, the National Institute for Health Research, the Department of Health and Social Care or the Academic institutions.
References
- Horsey K. The future of surrogacy: a review of current global trends and national landscapes. Reproductive BioMedicine Online [Internet]. 2024 May 1 [cited 2025 Sep 6];48(5):103764. Available from: https://www.sciencedirect.com/science/article/pii/S1472648323008635.
- Bromfield NF, Rotabi KS. Global Surrogacy, Exploitation, Human Rights and International Private Law: A Pragmatic Stance and Policy Recommendations. Glob Soc Welf [Internet]. 2014 Sep 1 [cited 2025 Sep 6];1(3):123–35. Available from. [CrossRef]
- Graham ME, Jelin A, Hoon AH, Wilms Floet AM, Levey E, Graham EM. Assisted reproductive technology: Short- and long-term outcomes. Dev Med Child Neurol [Internet]. 2023 Jan [cited 2025 Sep 6];65(1):38–49. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9809323/.
- Haddadi M, Hantoushzadeh S, Hajari P, Pouraie RR, Hadiani MY, Habibi GR, et al. Challenges and Prospects for Surrogacy in Iran as a Pioneer Islamic Country in this Field. Arch Iran Med [Internet]. 2025 Apr 1 [cited 2025 May 13];28(4):252–4. Available from: https://journalaim.com/Article/aim-33920.
- Piersanti V, Consalvo F, Signore F, Del Rio A, Zaami S. Surrogacy and “Procreative Tourism”. What Does the Future Hold from the Ethical and Legal Perspectives? Medicina (Kaunas). 2021 Jan 8;57(1):47. [CrossRef]
- Liu Y, Xian X, Du L. Perspectives on Surrogacy in Chinese Social Media: A Content Analysis of Microblogs on Weibo. The Yale journal of biology and medicine. 2022;95(3):305–16.
- Jones B, Saso S, Bracewell-Milnes T, Thum M, Nicopoullos J, Diaz-Garcia C, et al. Human Uterine transplantation: a Review of Outcomes from the First 45 Cases. BJOG: An International Journal of Obstetrics & Gynaecology. 2019;126(11):1310–9. [CrossRef]
- Testa G, McKenna GJ, Wall A, Bayer J, Gregg AR, Warren AM, et al. Uterus Transplant in Women With Absolute Uterine-Factor Infertility. JAMA. 2024;332(10):817–817. [CrossRef]
- Patel NH, Jadeja YD, Bhadarka HK, Patel MN, Patel NH, Sodagar NR. Insight into Different Aspects of Surrogacy Practices. J Hum Reprod Sci [Internet]. 2018 [cited 2025 Sep 6];11(3):212–8. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6262674/. [CrossRef]
- Brandão P, Garrido N. Commercial Surrogacy: An Overview. Rev Bras Ginecol Obstet [Internet]. 2022 Dec 29 [cited 2025 Sep 6];44(12):1141–58. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9800153/.
- Attawet J, Alsharaydeh E, Brady M. Commercial surrogacy: Landscapes of empowerment or oppression explored through integrative review. Health Care Women Int. 2024 Jan 22;1–19. [CrossRef]
- Banaras, F. Cross-Border Surrogacy: Legal and Ethical Challenges in Global Assisted Reproduction. 2023.
- Surrogacy in the USA · Growing Families [Internet]. Growing Families. [cited 2025 Sep 6]. Available from: https://www.growingfamilies.org/surrogacy-in-the-usa/.
- Marinelli S, Negro F, Varone MC, Paola LD, Napoletano G, Lopez A, et al. The legally charged issue of cross-border surrogacy: Current regulatory challenges and future prospects. European Journal of Obstetrics and Gynecology and Reproductive Biology [Internet]. 2024 Sep 1 [cited 2025 Sep 6];300:41–8. Available from: https://www.ejog.org/article/S0301-2115(24)00343-9/fulltext.
- Gunnarsson Payne J, Korolczuk E, Mezinska S. Surrogacy relationships: a critical interpretative review. Ups J Med Sci [Internet]. [cited 2025 Sep 6];125(2):183–91. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7721025/.
- Surrogacy: The legal situation in the EU | Think Tank | European Parliament [Internet]. [cited 2025 Sep 6]. Available from: https://www.europarl.europa.eu/thinktank/en/document/EPRS_BRI(2025)769508.
- GOV.UK [Internet]. [cited 2025 Sep 6]. The surrogacy pathway: surrogacy and the legal process for intended parents and surrogates in England and Wales. Available from: https://www.gov.uk/government/publications/having-a-child-through-surrogacy/the-surrogacy-pathway-surrogacy-and-the-legal-process-for-intended-parents-and-surrogates-in-england-and-wales.
- Aramesh K. Ethical Assessment of Monetary Relationship in Surrogacy. Journal of Reproduction & Infertility [Internet]. 2008 Apr 1 [cited 2025 Sep 6];9(1):36–42. Available from: https://www.jri.ir/article/304.
- East Midlands Affiliated Commissioning Committee (EMACC). Surrogacy Involving Assisted Conception Policy [Internet]. Derby and Derbyshire CCG: East Midlands Affiliated Commissioning Committee (EMACC); 2025 Apr. Available from: https://www.derbyshiremedicinesmanagement.nhs.uk/assets/Clinical-Policies/Clinical_Policies/PLCV/gynae_and_fertility/Surrogacy_Involving_Assisted_Conception.pdf.
- Gloucestershire Integrated Care Board (ICB). Surrogacy: Interventions not normally funded (INNF) [Internet]. Gloucestershire, UK: Gloucestershire ICB; 2025 Oct. Available from: https://www.nhsglos.nhs.uk/wp-content/uploads/2025/06/Surrogacy.pdf.
- Participation E. Human Fertilisation and Embryology Act 2008 [Internet]. Statute Law Database; [cited 2025 Sep 3]. Available from: https://www.legislation.gov.uk/ukpga/2008/22/contents.
- Participation E. Surrogacy Arrangements Act 1985 [Internet]. Statute Law Database; [cited 2025 Sep 6]. Available from: https://www.legislation.gov.uk/ukpga/1985/49.
- GOV.UK [Internet]. [cited 2025 Sep 6]. Surrogacy: caseworker guidance (accessible). Available from: https://www.gov.uk/government/publications/surrogacy-caseworker-guidance/surrogacy-caseworker-guidance-accessible.
- GOV.UK [Internet]. [cited 2025 Sep 6]. Children born through surrogacy. Available from: https://www.gov.uk/government/publications/getting-a-uk-passport-if-your-child-was-born-through-surrogacy/children-born-through-surrogacy.
- Italy bans citizens from seeking surrogacy abroad | The BMJ [Internet]. [cited 2025 Sep 6]. Available from: https://www.bmj.com/content/387/bmj.q2316.
- Book (eISB) electronic IS. electronic Irish Statute Book (eISB) [Internet]. Office of the Attorney General; [cited 2025 Sep 6]. Available from: https://www.irishstatutebook.ie/eli/2024/act/18/enacted/en/html.
- Everingham S. Major Change to Greek Surrogacy Laws: What It Means for International Intended Parents · Growing Families [Internet]. Growing Families. 2025 [cited 2025 Sep 6]. Available from: https://www.growingfamilies.org/blog/major-change-to-greek-surrogacy-laws-what-it-means-for-international-intended-parents/.
- admin. Surrogacy in Cyprus | Best Surrogacy Center in USA & Overseas [Internet]. Surrogacy4all - IVF Surrogacy, Surrogate Mother and Egg Donation Center in New York. [cited 2025 Sep 6]. Available from: https://www.surrogacy4all.com/cyprus-surrogacy/.
- Raposo VL. The new Portuguese law on surrogacy - The story of how a promising law does not really regulate surrogacy arrangements. JBRA Assist Reprod [Internet]. 2017 [cited 2025 Sep 6];21(3):230–9. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5574646/.
- Chen J. Intimate strangers: commercial surrogacy in Russia and Ukraine and the making of truth. Sex Reprod Health Matters [Internet]. [cited 2025 Sep 6];32(1):2328474. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11005867/.
- Haddadi M, Hedayati F, Hantoushzadeh S. Parallel paths: abortion access restrictions in the USA and Iran. Contracept Reprod Med [Internet]. 2025 Jul 25 [cited 2025 Sep 4];10(1):44. Available from: https://doi.org/10.1186/s40834-025-00382-3. [CrossRef]
- The New York State Child-Parent Security Act: Gestational Surrogacy [Internet]. [cited 2025 Sep 6]. Available from: https://www.health.ny.gov/community/pregnancy/surrogacy/.
- Branch LS. Consolidated federal laws of Canada, Assisted Human Reproduction Act [Internet]. 2020 [cited 2025 Sep 6]. Available from: https://laws-lois.justice.gc.ca/eng/acts/a-13.4/.
- International Child Custody Lawyer in Brazil – Dr. Mauricio Ejchel [Internet]. 2023 [cited 2025 Sep 6]. Available from: https://internationallawyerbrazil.com/surrogacy-in-brazil/.
- Surrogacy in Mexico · Growing Families [Internet]. Growing Families. 2025 [cited 2025 Sep 6]. Available from: https://www.growingfamilies.org/surrogacy-in-mexico/.
- Mahtani N. EL PAÍS English. 2024 [cited 2025 Sep 6]. The limbo of surrogacy in Colombia: ‘What is not forbidden is permitted.’ Available from: https://english.elpais.com/health/2024-02-26/the-limbo-of-surrogacy-in-colombia-what-is-not-forbidden-is-permitted.html.
- Turconi, PL. Assisted Regulation: Argentine Courts Address Regulatory Gaps on Surrogacy. Health Hum Rights. 2023 Dec;25(2):15–28.
- Kashyap S, Tripathi P. The Surrogacy (Regulation) Act, 2021: A Critique. Asian Bioeth Rev. 2023 Jan;15(1):5–18. [CrossRef]
- Atreya A, Kanchan T. The ethically challenging trade of forced surrogacy in Nepal. Int J Gynaecol Obstet. 2018 Feb;140(2):254–5. [CrossRef]
- Attawet, J. Reconsidering Surrogacy Legislation in Thailand. Med Leg J. 2022 Mar;90(1):45–8. [CrossRef]
- Cambodia releases surrogate mothers who agree to keep children [Internet]. [cited 2025 Sep 7]. Available from: https://www.bbc.com/news/world-asia-46466888.
- You W, Feng J. Legal regulation of surrogacy parentage determination in China. Front Psychol [Internet]. 2024 Sep 6 [cited 2025 Sep 7];15:1363685. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11414016/.
- South Korea - Eastern and Western Perspectives on Surrogacy [Internet]. [cited 2025 Sep 7]. Available from: https://www.cambridge.org/core/books/abs/eastern-and-western-perspectives-on-surrogacy/south-korea/778B382D9190B8B380198D77BBC18AAD.
- Hibino, Y. Non-commercial surrogacy among close relatives in Vietnam: policy and ethical implications. Hum Fertil (Camb). 2019 Dec;22(4):273–6. [CrossRef]
- Library of Congress, Washington, D.C. 20540 USA [Internet]. [cited 2025 Sep 7]. Israel: Supreme Court Authorizes Surrogacy Arrangements for Gay Men. Available from: https://www.loc.gov/item/global-legal-monitor/2021-07-29/israel-supreme-court-authorizes-surrogacy-arrangements-for-gay-men/.
- Hibino Y. Ongoing Commercialization of Gestational Surrogacy due to Globalization of the Reproductive Market before and after the Pandemic. Asian Bioeth Rev [Internet]. 2022 Aug 18 [cited 2025 Sep 7];14(4):349–61. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9386202/.
- Children’s Act 38 of 2005 | South African Government [Internet]. [cited 2025 Sep 7]. Available from: https://www.gov.za/documents/childrens-act.
- UNICEF and CHIP: Briefing note on children’s rights and surrogacy – Child Identity Protection [Internet]. [cited 2025 Sep 7]. Available from: https://www.child-identity.org/unicef-and-chip-briefing-note-on-childrens-rights-and-surrogacy/.
- Surrogacy - Milliez - 2008 - International Journal of Gynecology & Obstetrics - Wiley Online Library [Internet]. [cited 2025 Sep 7]. Available from: https://obgyn.onlinelibrary.wiley.com/doi/10.1016/j.ijgo.2008.04.016.
- Luk J, Petrozza JC. Evaluation of compliance and range of fees among American Society for Reproductive Medicine-listed egg donor and surrogacy agencies. J Reprod Med. 2008 Nov;53(11):847–52.
- White PM. Canada’s Surrogacy Landscape is Changing: Should Canadians Care? Journal of Obstetrics and Gynaecology Canada [Internet]. 2017 Nov 1 [cited 2025 Sep 7];39(11):1046–8. Available from: https://www.jogc.com/article/S1701-2163(17)30575-3/abstract.
- Ribeiro G, de Menezes JB. Brazil. In: Fenton-Glynn C, Scherpe JM, Espejo-Yaksic N, editors. Surrogacy in Latin America [Internet]. Intersentia; 2023 [cited 2025 Sep 7]. p. 65–82. (Intersentia Studies in Comparative Family Law). Available from: https://www.cambridge.org/core/books/surrogacy-in-latin-america/brazil/9386B14ED39762C3F0A6C6E929488D86.
- UNICEF’s Action against Child Trafficking | UNICEF [Internet]. [cited 2025 Sep 7]. Available from: https://www.unicef.org/reports/unicefs-action-against-child-trafficking.
- Surrogacy, Law & Human Rights [Internet]. ADF International. [cited 2025 Sep 7]. Available from: https://adfinternational.org/resources/surrogacy-law-human-rights.
- Mayers L. From Choice to Justice. Health Hum Rights [Internet]. 2024 Dec [cited 2025 Sep 7];26(2):13–24. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11683579/.
- Full article: Legal parenthood in surrogacy: shifting the focus to the surrogate’s negative intention [Internet]. [cited 2025 Sep 7]. Available from: https://www.tandfonline.com/doi/full/10.1080/09649069.2024.2344935.
- Specialised Services Commissioning Policy: CP38 Specialist Fertility Services [Internet]. 2017 [cited 2025 Jan 1]. Available from: https://whssc.nhs.wales/commissioning/nwjcc-policies/fertility/specialist-fertility-services-commissioning-policy-cp38-april-2025/.
- Pope calls for surrogacy ban | CNN [Internet]. [cited 2025 Sep 7]. Available from: https://edition.cnn.com/2024/01/08/world/pope-ban-surrogacy.
- Mitra S, Schicktanz S. Failed surrogate conceptions: social and ethical aspects of preconception disruptions during commercial surrogacy in India. Philos Ethics Humanit Med [Internet]. 2016 Sep 19 [cited 2025 Sep 7];11:9. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5075174/.
- Wade K. The regulation of surrogacy: a children’s rights perspective. Child Fam Law Q [Internet]. 2017 Jun 29 [cited 2025 Sep 7];29(2):113–31. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5540169/.
- Surrogacy: legal rights of parents and surrogates: Overview - GOV.UK [Internet]. [cited 2025 Sep 7]. Available from: https://www.gov.uk/legal-rights-when-using-surrogates-and-donors.
- Surrogacy in Australia [Internet]. [cited 2025 Sep 7]. Available from: https://www.surrogacy.gov.au/.
- Rodriguez-Wallberg KA, Arturo Reyes Palomares, Nilsson H, Öberg S, Lundberg FE. Obstetric and Perinatal Outcomes of Singleton Births Following Single- vs Double-Embryo Transfer in Sweden. JAMA Pediatrics. 2023;177(2):149–149. [CrossRef]
- Davis N. the Guardian. The Guardian; 2024. Surrogates face higher risk of pregnancy complications, study finds. Available from: https://www.theguardian.com/lifeandstyle/2024/sep/23/surrogates-face-higher-risk-of-pregnancy-complications-study-finds.
- Davis N. the Guardian. The Guardian; 2025. Surrogates at greater risk of new mental illness than women carrying own babies, study finds. Available from: https://www.theguardian.com/lifeandstyle/2025/jul/25/surrogates-gestational-carriers-risk-mental-illness-pregnancy-canada.
- Lamba N, Jadva V, Kadam K, Golombok S. The psychological well-being and prenatal bonding of gestational surrogates. Human Reproduction (Oxford, England). 2018;33(4):646–53. [CrossRef]
- Espejo-Yaksic N, Fenton-Glynn C, Scherpe JM, editors. Surrogacy in Latin America [Internet]. Intersentia; 2023 [cited 2025 Sep 7]. (Intersentia Studies in Comparative Family Law). Available from: https://www.cambridge.org/core/books/surrogacy-in-latin-america/8B4B09CDFE6966681B1A2F400A790DFE.
- Holmstrom-Smith A. Free Market Feminism: Re-Reconsidering Surrogacy [Internet]. Rochester, NY: Social Science Research Network; 2021 [cited 2025 Sep 7]. Available from: https://papers.ssrn.com/abstract=3896014.
- Сomparison of Surrogacy Conditions in Ukraine and Georgia [Internet]. [cited 2025 Sep 6]. Available from: https://www.mother-surrogate.com/surrogacy-in-georgia-and-ukraine-where-are-the-conditions-better.html.
- Surrogate.com | [Internet]. 2025 [cited 2025 Jan 1]. LGBT Surrogacy Laws in Louisiana: Complete Guide. Available from: https://surrogate.com/surrogacy-by-state/louisiana-surrogacy/lgbt-surrogacy-laws-louisiana/.
- Boydell V, Mori R, Shahrook S, Gietel-Basten S. Low fertility and fertility policies in the Asia-Pacific region. Glob Health Med [Internet]. 2023 Oct 31 [cited 2025 Sep 7];5(5):271–7. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10615026/.
- Semba Y, Chang C, Hong H, Kamisato A, Kokado M, Muto K. Surrogacy: Donor Conception Regulation in Japan. Bioethics. 2009 Nov 1;24:348–57. [CrossRef]
- Blazier J, Janssens R. Regulating the international surrogacy market:the ethics of commercial surrogacy in the Netherlands and India. Med Health Care Philos [Internet]. 2020 [cited 2025 Sep 7];23(4):621–30. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7538442/.
- Prada drops Chinese actress over alleged surrogacy row. BBC [Internet]. 2021; Available from: https://www.bbc.com/news/world-asia-china-55729437?
- Calvario L. Entertainment Tonight. 2019 [cited 2025 Jan 1]. Everything Kim Kardashian Has Said About Surrogacy. Available from: https://www.etonline.com/everything-kim-kardashian-has-said-about-surrogacy-116451.
Figure 1.
is a conceptual framework. The conceptual framework illustrates the interconnections between key domains of surrogacy policies. At its centre, represented by the dark blue box, are surrogacy policies, encompassing the full spectrum of laws, guidelines, and practices that govern surrogacy at local, national, and international levels. Surrounding this core are three thematic domains. The ethical debate (purple) captures the moral discourse underpinning policy decisions, ranging from the protection of human dignity, which seeks to prevent the commodification of women and children, to the promotion of personal autonomy and reproductive rights that enable individuals and families to make informed choices about family building. The commercial versus altruistic surrogacy domain (orange) explores different models of surrogacy, contrasting policies that ban for-profit arrangements with those that permit and regulate compensation, ensuring transparency and safeguarding against exploitation. Finally, the legal parentage and best interests of the child domain (green) highlights the mechanisms required to establish clear legal parentage for intended parents and safeguard the welfare, citizenship, and fundamental rights of children born through surrogacy. Together, these domains provide a comprehensive lens through which to examine and evaluate global surrogacy policies.
Figure 1.
is a conceptual framework. The conceptual framework illustrates the interconnections between key domains of surrogacy policies. At its centre, represented by the dark blue box, are surrogacy policies, encompassing the full spectrum of laws, guidelines, and practices that govern surrogacy at local, national, and international levels. Surrounding this core are three thematic domains. The ethical debate (purple) captures the moral discourse underpinning policy decisions, ranging from the protection of human dignity, which seeks to prevent the commodification of women and children, to the promotion of personal autonomy and reproductive rights that enable individuals and families to make informed choices about family building. The commercial versus altruistic surrogacy domain (orange) explores different models of surrogacy, contrasting policies that ban for-profit arrangements with those that permit and regulate compensation, ensuring transparency and safeguarding against exploitation. Finally, the legal parentage and best interests of the child domain (green) highlights the mechanisms required to establish clear legal parentage for intended parents and safeguard the welfare, citizenship, and fundamental rights of children born through surrogacy. Together, these domains provide a comprehensive lens through which to examine and evaluate global surrogacy policies.
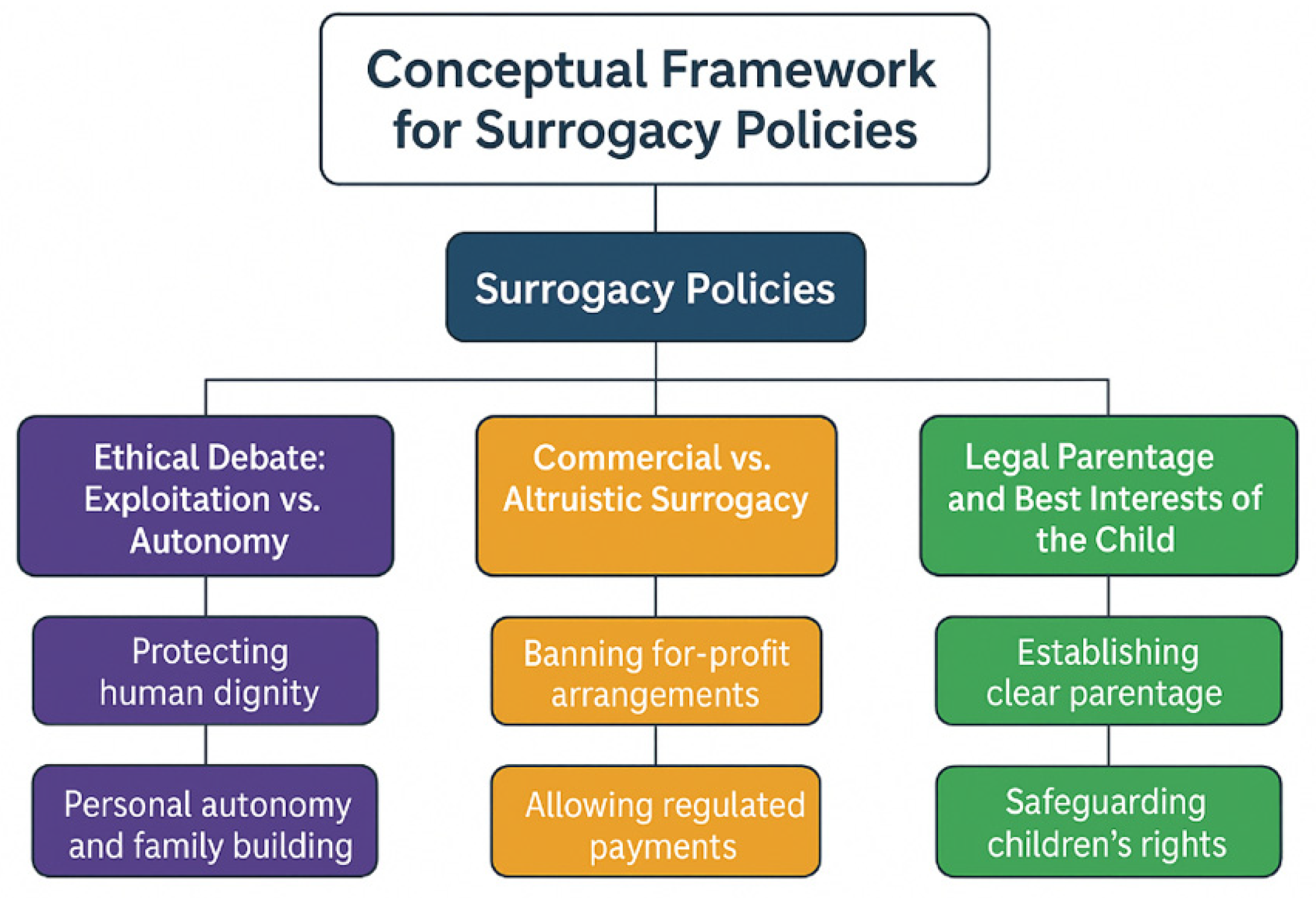

Table 2.
indicates themes and sub-themes identified in the sample.
| Theme | Sub-themes | Example indicator | Exposure (who/what) | Determinants | Potential intersections | Relevant law / guidance | Policy strength | Policy weakness |
| Commissioning stance | “Not normally funded”; no payments; no recruitment | Policy text: no routine commissioning; no funding of surrogacy-specific elements or expenses | Intended parents seeking NHS-funded surrogacy-related ART | Medico-legal risk; affordability; enforceability | Same-sex couples; uterine-factor infertility; prior IVF failure | EMACC 2022; Gloucestershire ICB 2025 | Clear signal; consistent stance | Drives cross-border care; equity concerns. |
| Exceptionality / IFR | Strict, cohort rule | Exceptionality unlikely if a broader cohort would benefit similarly | IFR applicants | Resource stewardship; precedent aversion | Rare medical indications | EMACC IFR criteria | Transparent gatekeeping | Narrow access; opaque for patients. |
| Legal status | Altruistic vs commercial; unenforceable agreements; parental order | Surrogate legal mother at birth; transfer via court | Surrogates; commissioning parents; child | UK statutory framework | Overseas commercial contexts | Surrogacy Arrangements Act 1985; HFE Act 2008; HFEA info | Strong legal clarity | Practical friction with cross-border cases. |
| Parentage & nationality | Parental orders; nationality proof; consent hierarchies | HMPO accepts cases with/withoutparental order; sets consent steps | Child born via surrogacy; HMPO examiners | Safeguarding; identity; documentation | Birth jurisdiction; DNA | HMPO Surrogacy v11.0 (2025) | Child-centred, structured pathway | Administrative burden; delays. |
| Ethical/psychosocial risk | Disputes; child rejection; long-term psychological effects | Ethical list underpinning non-funding | Surrogate, intended parents, child | Uncertain outcomes; non-enforceability | Mental health; family dynamics | EMACC policy | Candid risk articulation | Limited mitigations beyond non-funding. |
| Safeguarding & fraud | Vulnerability checks; CPST referrals | Watchlist checks; CPST escalation | Applicants in inter-country cases | Unregulated markets; coercion | Trafficking risk; agencies | HMPO operational guidance | Robust safeguards | High evidential thresholds in emergencies. |
| Cross-border navigation | ETDs; no parental order handling | FCDO ETD workflow; continued case-holding | Families abroad; infants | Legal heterogeneity across states | Ukraine/other hubs | HMPO ETD process | Practical routes for urgent return | Prolonged separation; complexity. |
| Connected NHS care | Maternity care continuity | ICB commits to antenatal/postnatal support for surrogates | Surrogates in pregnancy care | Commissioning boundaries | Fertility preservation signposting | Gloucestershire ICB 2025 | Clarifies what isfunded | Fragmented patient journey across policies. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



