Submitted:
10 September 2025
Posted:
11 September 2025
You are already at the latest version
Abstract
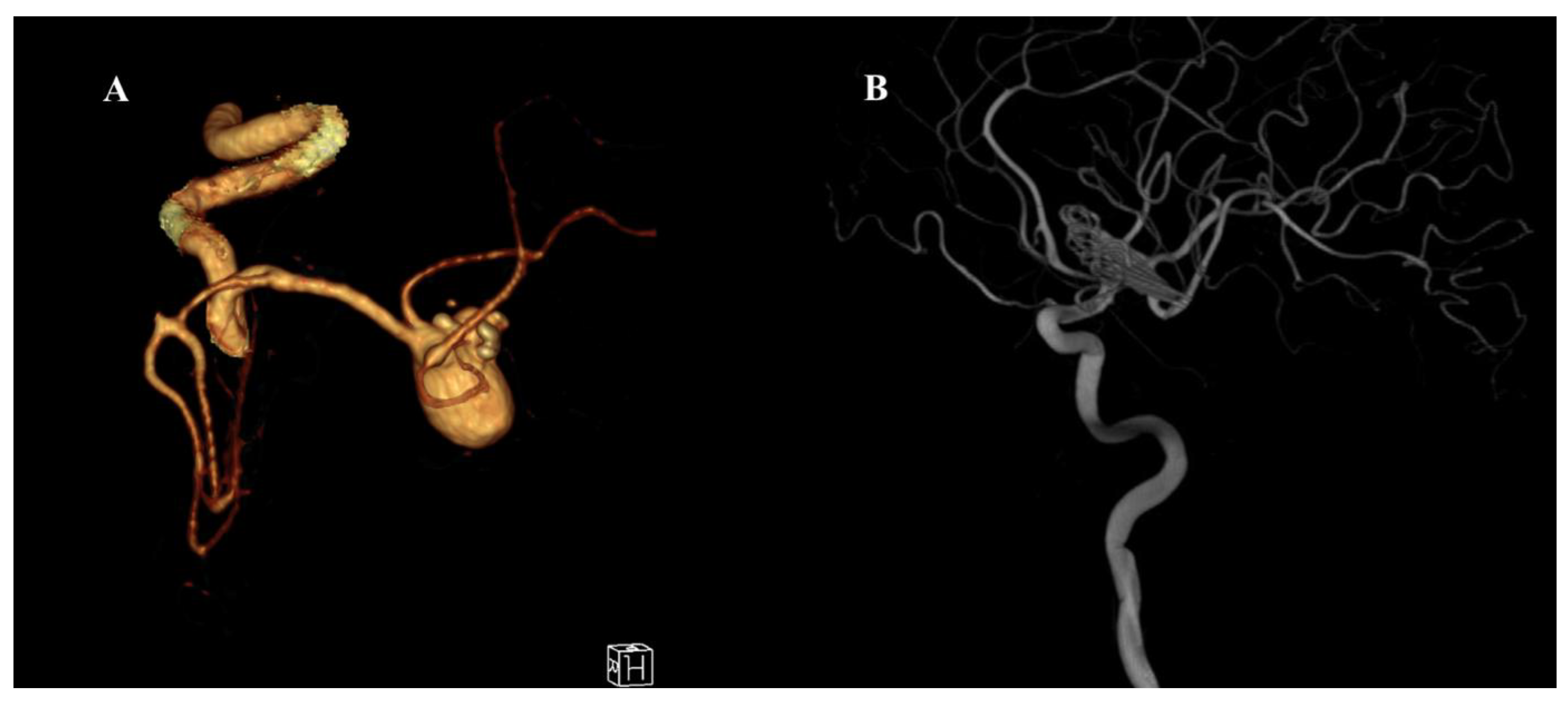
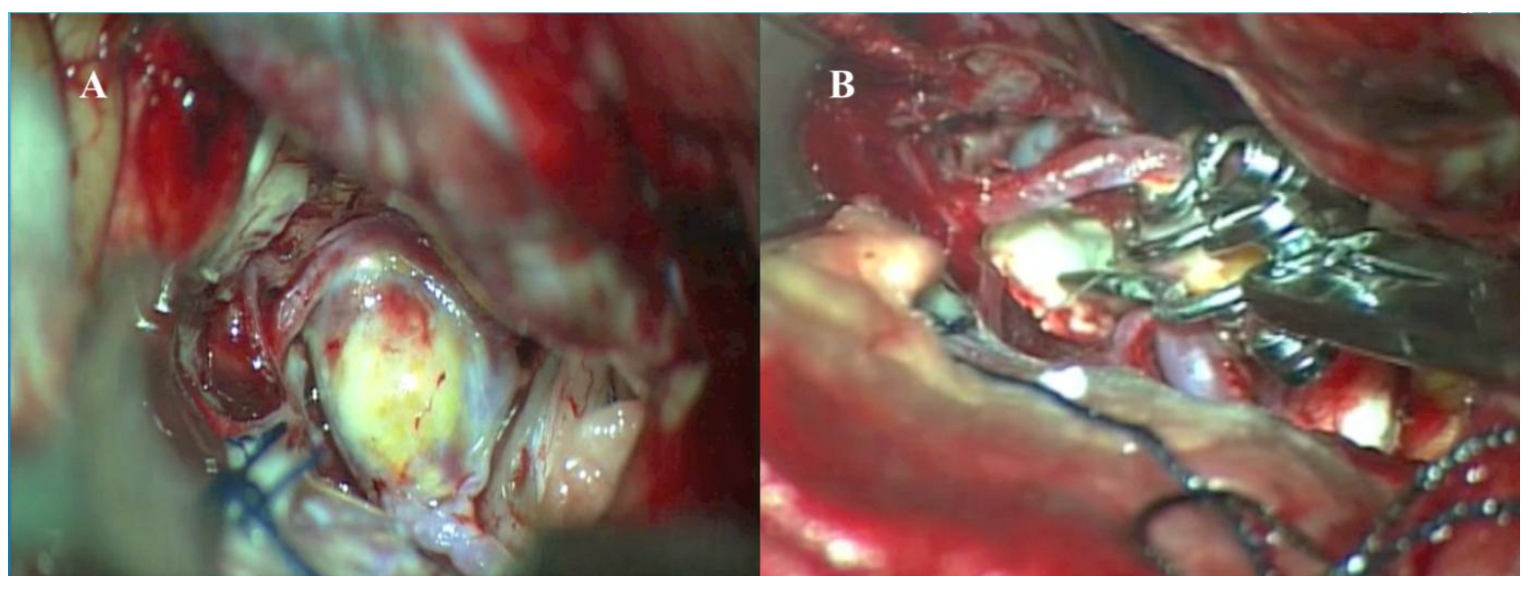
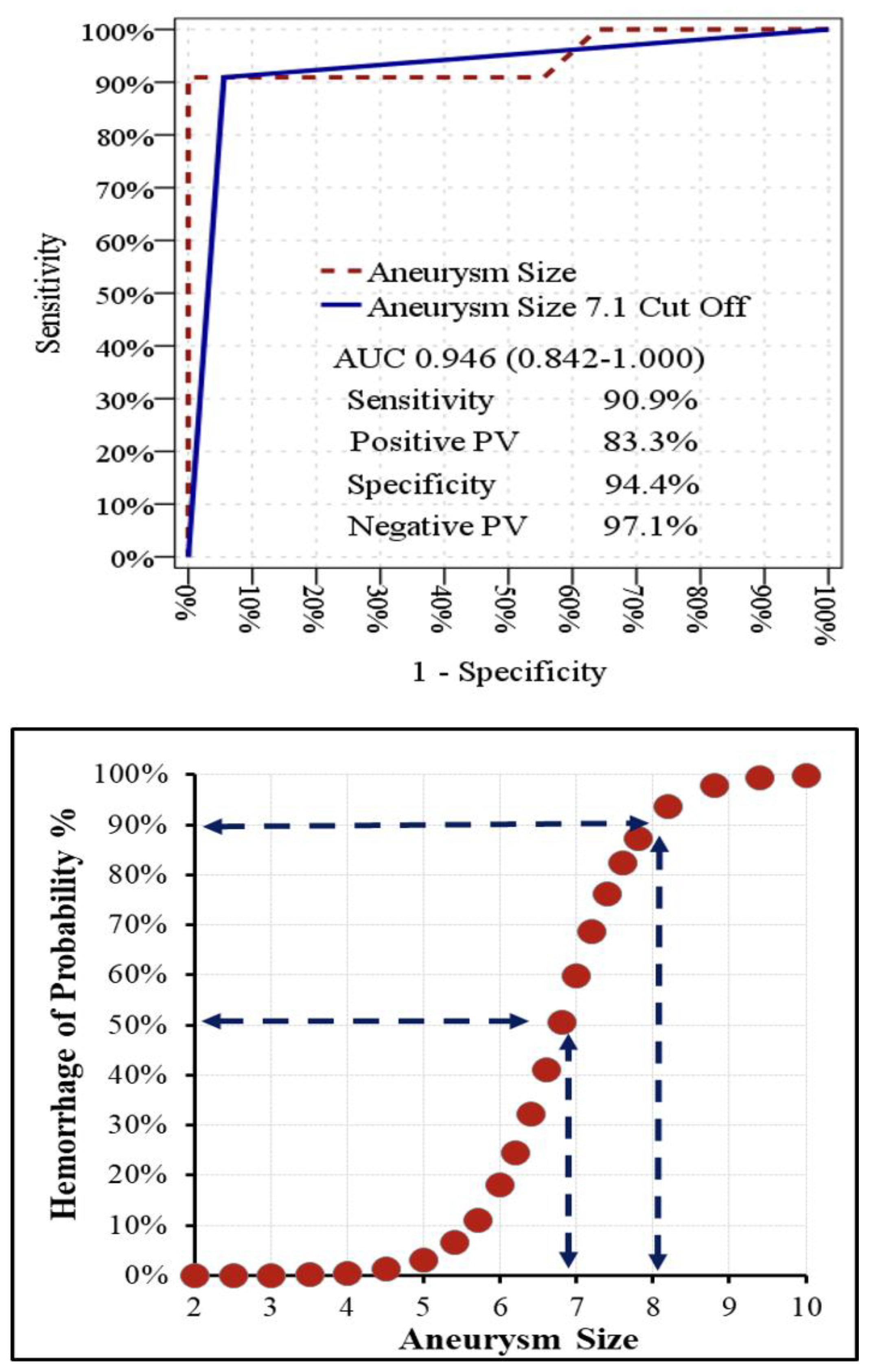
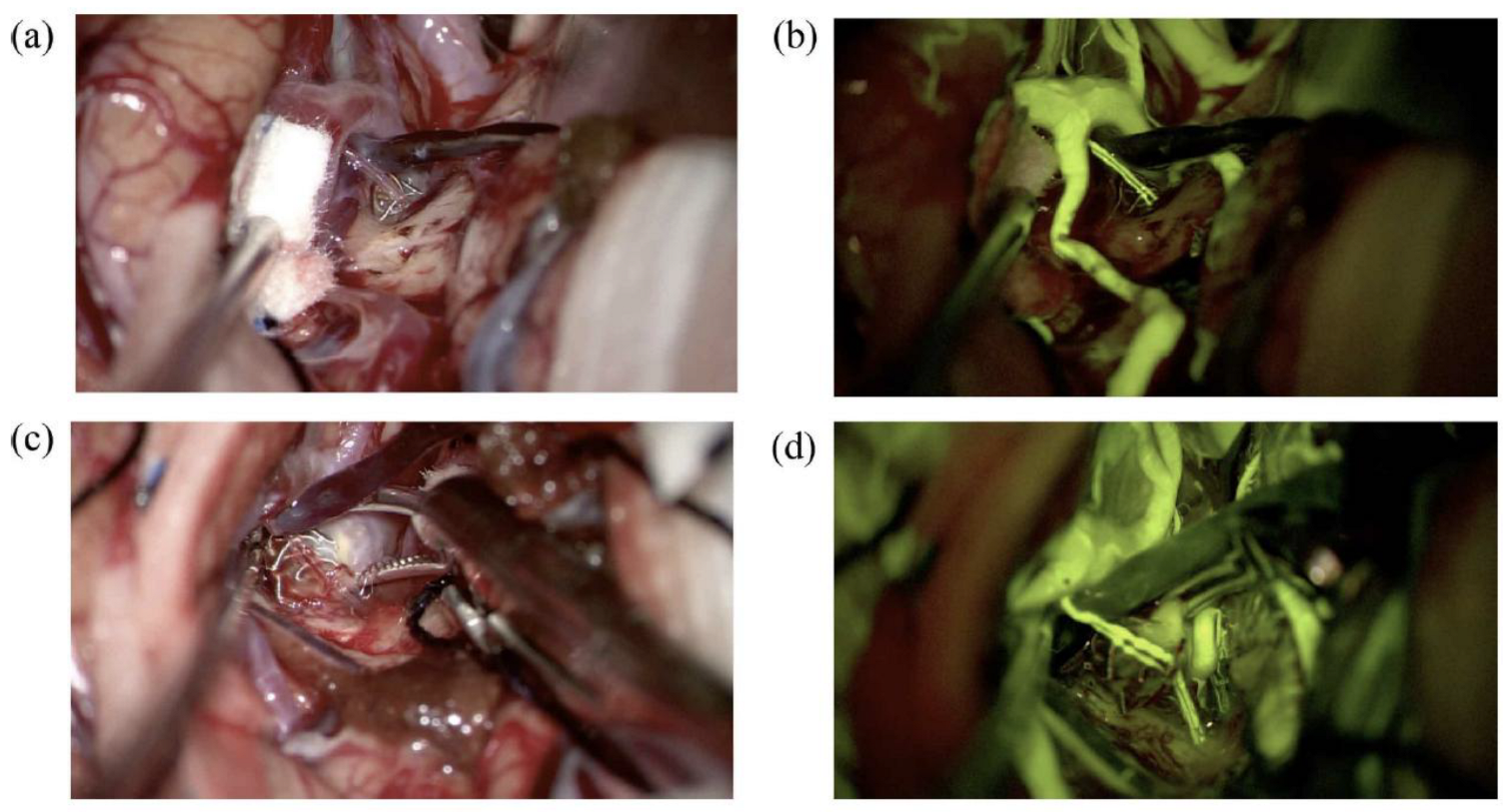
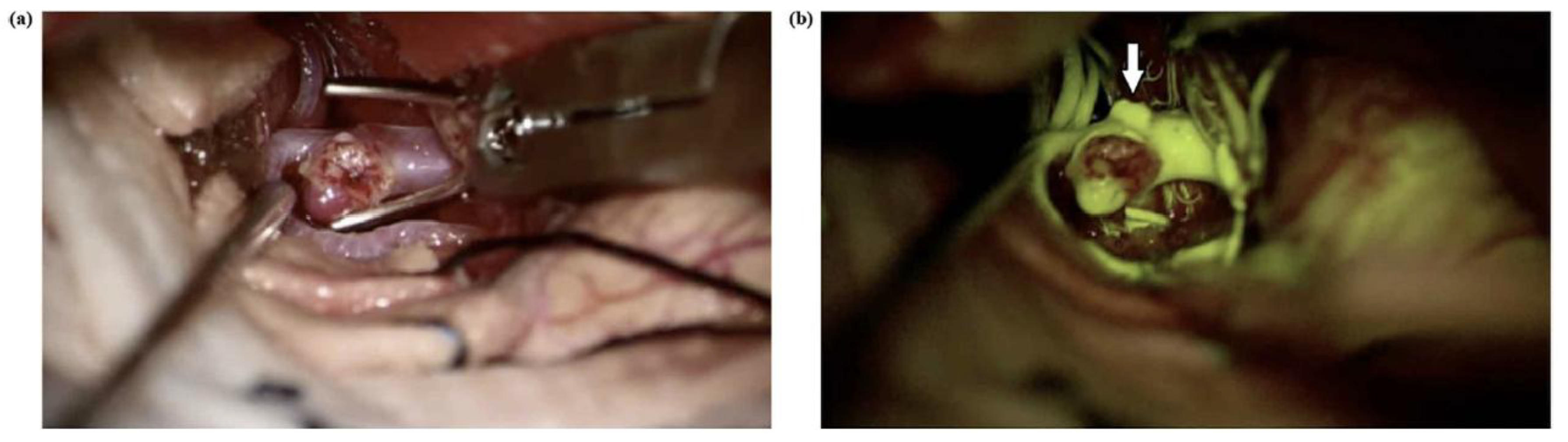
Background and Objectives: To evaluate factors affecting aneurysm rupture, present our surgical experience with intracranial aneurysms, specifically using the picket-fence clipping technique for giant aneurysms, and highlight the complementary roles of sodium fluorescein (Na-Fl) and indocyanine green (ICG) videoangiography in enhancing surgical precision and patient outcomes. Materials and Methods: We retrospectively analyzed 47 patients who underwent microsurgical clipping of intracranial aneurysms with intraoperative Na-Fl and ICG videoangiography between September 2015 and February 2024. We asses[sed relationships between patient comorbidities, family history of subarachnoid hemorrhage (SAH), smoking history, aneurysm location and size with SAH occurrence. Concordance between intraoperative videoangiography and postoperative digital subtraction angiography (DSA) for detecting residual aneurysms was also evaluated. Results: Of the 47 patients (31 female, 16 male; mean age 51.78 ± 11.16 years), 11 (23.4%) presented with SAH. The most common aneurysm location was the middle cerebral artery (MCA) (68.1%). Hypertension and smoking history were significantly higher in the hemorrhage group (p<0.05). Aneurysm size and anterior communicating artery (AComA) location were also significantly associated with hemorrhage (p<0.05). Aneurysm size demonstrated significant discriminative power for hemorrhage [AUC: 0.884 (0.827–0.941)], with a cutoff of 7.1 mm yielding 90.9% sensitivity and 94.4% specificity. Five giant MCA aneurysms were treated with the picket-fence technique, with intraoperative ICG and Na-Fl confirming parent artery patency and complete aneurysm occlusion, subsequently confirmed by postoperative DSA. Small remnants were detected in 2 cases (4.26%) on postoperative DSA, both in distal ACA aneurysms, which were also detected by intraoperative videoangiography. Conclusions: Hypertension, smoking history, aneurysm size and location were important predictors of aneurysm rupture. Intraoperative ICG and Na-Fl videoangiography provide real-time, high-resolution visualization crucial for complex intracranial aneurysm surgery, including the picket-fence technique for giant aneurysms. Their complementary use enhances surgical safety, guides intraoperative decision-making, and contributes to improved outcomes in challenging cases.
Keywords:
1. Introduction
2. Materials and Methods

| Table-1 | ||||||||
| Min-Max | Median | Mean±sd/n-% | ||||||
| Age | 30.0 | - | 70.0 | 54.0 | 51.8 | ± | 11.3 | |
| Gender | Female | 31 | 66.0% | |||||
| Male | 16 | 34.0% | ||||||
| Hypertension | 21 | 44.7% | ||||||
| Diabetus Mellitus | 12 | 25.5% | ||||||
| Family History of Subarachnoid Hemorrhage | 8 | 17.0% | ||||||
| Smoking History | 20 | 42.6% | ||||||
| Hemorrhage | 11 | 23.4% | ||||||
| Aneurysm Location | MCA | 32 | 68.1% | |||||
| AcomA | 11 | 23.4% | ||||||
| PcomA | 1 | 2.1% | ||||||
| ACA | 3 | 6.4% | ||||||
| Aneurysm Size | 1.7 | - | 9.5 | 5.0 | 5.4 | ± | 1.8 | |
| Postoperative DSA Remnant Aneurysm | 2 | 4.3% | ||||||
2.1. Picket Fence Techique in Giant Aneurysms
2.2. Illustrative Case-I
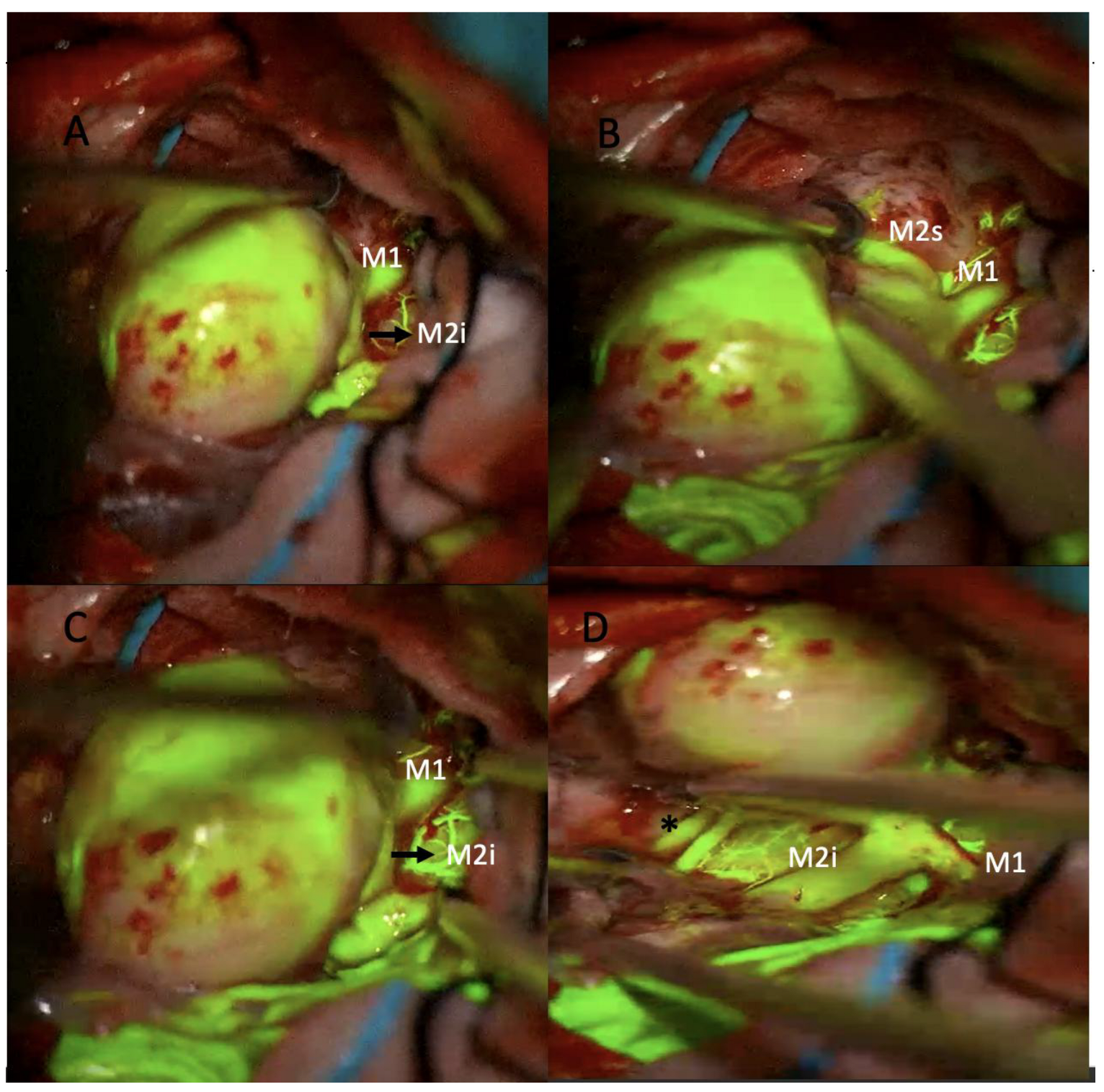
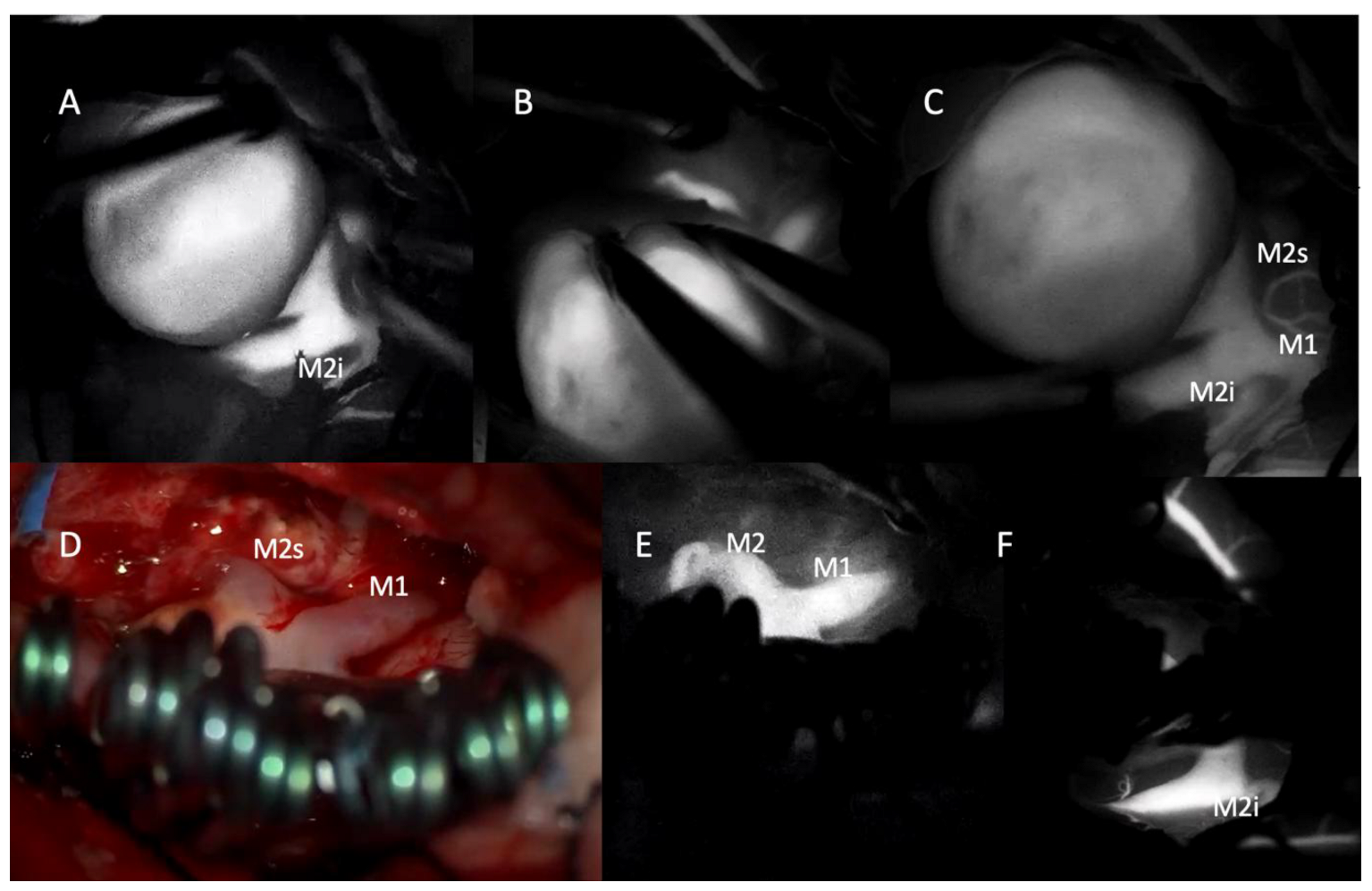
2.3. Illustrative Case-II

2.4. Statistical Analysis
3. Results
| Table-2 | ||||||||||||
| Hemorrhage (-) (n:36) | Hemorrhage (+) (n:11) | p | ||||||||||
| Mean±sd/n-% | Median | Mean±sd/n-% | Median | |||||||||
| Age | 52.9 | ± | 10.7 | 54.5 | 48.1 | ± | 13.0 | 49.0 | 0.218 | m | ||
| Gender | Female | 25 | 69.4% | 6 | 54.5% | 0.361 | X² | |||||
| Male | 11 | 30.6% | 5 | 45.5% | ||||||||
| Hypertension | (-) | 26 | 72.2% | 0 | 0.0% | 0.000 | X² | |||||
| (+) | 10 | 27.8% | 11 | 100% | ||||||||
| Diabetus Mellitus | (-) | 25 | 69.4% | 10 | 90.9% | 0.153 | X² | |||||
| (+) | 11 | 30.6% | 1 | 9.1% | ||||||||
| Family History of Subarachnoid Hemorrhage | (-) | 32 | 88.9% | 7 | 63.6% | 0.073 | X² | |||||
| (+) | 4 | 11.1% | 4 | 36.4% | ||||||||
| Smoking History | (-) | 26 | 72.2% | 1 | 9.1% | 0.000 | X² | |||||
| (+) | 10 | 27.8% | 10 | 90.9% | ||||||||
| Aneurysm Location | MCA | 26 | 72.2% | 6 | 54.5% | 0.271 | X² | |||||
| AcomA | 6 | 16.7% | 5 | 45.5% | 0.048 | X² | ||||||
| PcomA | 1 | 2.8% | 0 | 0.0% | 1.000 | X² | ||||||
| ACA | 3 | 8.3% | 0 | 0.0% | 1.000 | X² | ||||||
| Aneurysm Size | 4.6 | ± | 1.1 | 4.7 | 8.0 | ± | 1.4 | 8.5 | 0.000 | m | ||
| Postoperative DSA Remnant Aneurysm | (-) | 34 | 94.4% | 11 | 100% | 1.000 | X² | |||||
| (+) | 2 | 5.6% | 0 | 0.0% | ||||||||
| m Mann-whitney u test / X² Chi-square test (Fischer test) | ||||||||||||
| Table-3 | ||||||||
| Area Under Curve | 95% Confidence Interval | p | ||||||
| Aneurysm Size | 0.884 | 0.827 | - | 0.941 | 0.000 | |||
| Aneurysm Size 7.1 Cut Off | 0.824 | 0.749 | - | 0.898 | 0.000 | |||
| Hemorrhage (-) | Hemorrhage (+) | % | ||||||
| Aneurysm Size | < 7.1 | 34 | 1 | Sensitivity | 90.9% | |||
| ≥ 7.1 | 2 | 10 | Positive PV | 83.3% | ||||
| Specificity | 94.4% | |||||||
| Negative PV | 97.1% | |||||||
| ROC Curve | ||||||||
4. Discussion
5. Conclusion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Molyneux, A.J.; Kerr, R.S.; Yu, L.M.; Clarke, M.; Sneade, M.; Yarnold, J.A.; Sandercock, P. International subarachnoid aneurysm trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised comparison of effects on survival, dependency, seizures, rebleeding, subgroups, and aneurysm occlusion. Lancet 2005, 366, 809–817. [Google Scholar] [CrossRef] [PubMed]
- Pierot, L. Do we still need coils for the endovascular treatment of intracranial aneurysms? 2019, 11, 1173-1173.
- Toader, C.; Serban, M.; Dobrin, N.; Covache-Busuioc, R.A.; Radoi, M.P.; Ciurea, A.V.; Munteanu, O. Complex Anatomy, Advanced Techniques: Microsurgical Clipping of a Ruptured Hypophyseal Artery Aneurysm. J Clin Med 2025, 14. [Google Scholar] [CrossRef] [PubMed]
- Yang, I.; Lawton, M.T. Clipping of complex aneurysms with fenestration tubes: application and assessment of three types of clip techniques. Neurosurgery 2008, 62, ONS371–378. [Google Scholar] [CrossRef] [PubMed]
- Sughrue, M.E.; Saloner, D.; Rayz, V.L.; Lawton, M.T. Giant intracranial aneurysms: evolution of management in a contemporary surgical series. Neurosurgery 2011, 69, 1261–1270. [Google Scholar] [CrossRef] [PubMed]
- Dashti, R.; Laakso, A.; Niemelä, M.; Porras, M.; Hernesniemi, J. Microscope Integrated Indocyanine Green Video-Angiography in Cerebrovascular Surgery. In Intraoperative Imaging, Pamir, M.N., Seifert, V., Kiris, T., Eds.; Springer Vienna: Vienna, 2011; pp. 247–250. [Google Scholar]
- Kırış, T.; Akçakaya, M.O. Comparison of intraoperative sodium fluorescein and indocyanine green videoangiography during intracranial aneurysm and arteriovenous malformation surgery. Clin Neurol Neurosurg 2024, 244, 108414. [Google Scholar] [CrossRef] [PubMed]
- Sugita, K.; Kobayashi, S.; Inoue, T.; Banno, T. New angled fenestrated clips for fusiform vertebral artery aneurysms. J Neurosurg 1981, 54, 346–350. [Google Scholar] [CrossRef] [PubMed]
- Sugita, K.; Kobayashi, S.; Kyoshima, K.; Nakagawa, F. Fenestrated clips for unusual aneurysms of the carotid artery. J Neurosurg 1982, 57, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Ichikawa, T.; Suzuki, K.; Watanabe, Y.; Sato, T.; Sakuma, J.; Saito, K. Development of and Clinical Experience with a Simple Device for Performing Intraoperative Fluorescein Fluorescence Cerebral Angiography: Technical Notes. Neurologia medico-chirurgica 2016, 56, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Kakucs, C.; Florian, I.-A.; Ungureanu, G.; Florian, I.-S. Fluorescein Angiography in Intracranial Aneurysm Surgery: A Helpful Method to Evaluate the Security of Clipping and Observe Blood Flow. World Neurosurgery 2017, 105, 406–411. [Google Scholar] [CrossRef] [PubMed]
- Lane, B.; Bohnstedt, B.N.; Cohen-Gadol, A.A. A prospective comparative study of microscope-integrated intraoperative fluorescein and indocyanine videoangiography for clip ligation of complex cerebral aneurysms. J Neurosurg 2015, 122, 618–626. [Google Scholar] [CrossRef] [PubMed]
- Dellaretti, M.; Guimarães Soares, A.; Douglas de Oliveira Lima, A.; Tavares de Melo, M.; Dilella Acherman, N.; Faglioni Junior, W.; Silva Costa, B. Application of fluorescein sodium videoangiography in aneurysm surgery. J Clin Neurosci 2024, 126, 228–233. [Google Scholar] [CrossRef] [PubMed]
- Fritch, C.; Church, E.; Wilkinson, D.A. Advances in Intraoperative Imaging for Vascular Neurosurgery. Neuroimaging Clin N Am 2024, 34, 261–270. [Google Scholar] [CrossRef] [PubMed]
- Raabe, A.; Nakaji, P.; Beck, J.; Kim, L.J.; Hsu, F.P.; Kamerman, J.D.; Seifert, V.; Spetzler, R.F. Prospective evaluation of surgical microscope-integrated intraoperative near-infrared indocyanine green videoangiography during aneurysm surgery. J Neurosurg 2005, 103, 982–989. [Google Scholar] [CrossRef]
- Küçükyürük, B.; Korkmaz, T.; Nemayire, K.; Özlen, F.; Kafadar, A.M.; Akar, Z.; Kaynar, M.Y.; Sanus, G.Z. Intraoperative Fluorescein Sodium Videoangiography in Intracranial Aneurysm Surgery. World Neurosurg 2021, 147, e444–e452. [Google Scholar] [CrossRef] [PubMed]
- Campos Cardoso, L.J.; Ferreira, M.Y.; Scherer, R.T.; Fukunaga, C.K.; Bocanegra-Becerra, J.E.; Günkan, A.; Ferreira, C.; Ellis, J.; Serulle, Y.; Langer, D. Sodium fluorescein video Angiography-Assisted clipping of intracranial Aneurysms: A systematic review and Meta-Analysis. J Clin Neurosci 2025, 134, 111081. [Google Scholar] [CrossRef]
- Matano, F.; Mizunari, T.; Murai, Y.; Kubota, A.; Fujiki, Y.; Kobayashi, S.; Morita, A. Quantitative Comparison of the Intraoperative Utility of Indocyanine Green and Fluorescein Videoangiographies in Cerebrovascular Surgery. Oper Neurosurg (Hagerstown) 2017, 13, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Belykh, E.; Cavallo, C.; Valli, D.; Gandhi, S.; Preul, M.C.; Vajkoczy, P.; Lawton, M.T.; Nakaji, P. Application of Fluorescein Fluorescence in Vascular Neurosurgery. Front Surg 2019, 6, 52. [Google Scholar] [CrossRef] [PubMed]
- Dashti, R.; Laakso, A.; Niemelä, M.; Porras, M.; Hernesniemi, J. Microscope-integrated near-infrared indocyanine green videoangiography during surgery of intracranial aneurysms: the Helsinki experience. Surg Neurol 2009, 71, 543–550. [Google Scholar] [CrossRef]
- Washington, C.W.; Zipfel, G.J.; Chicoine, M.R.; Derdeyn, C.P.; Rich, K.M.; Moran, C.J.; Cross, D.T.; Dacey, R.G., Jr. Comparing indocyanine green videoangiography to the gold standard of intraoperative digital subtraction angiography used in aneurysm surgery. J Neurosurg 2013, 118, 420–427. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



