Submitted:
09 September 2025
Posted:
10 September 2025
You are already at the latest version
Abstract
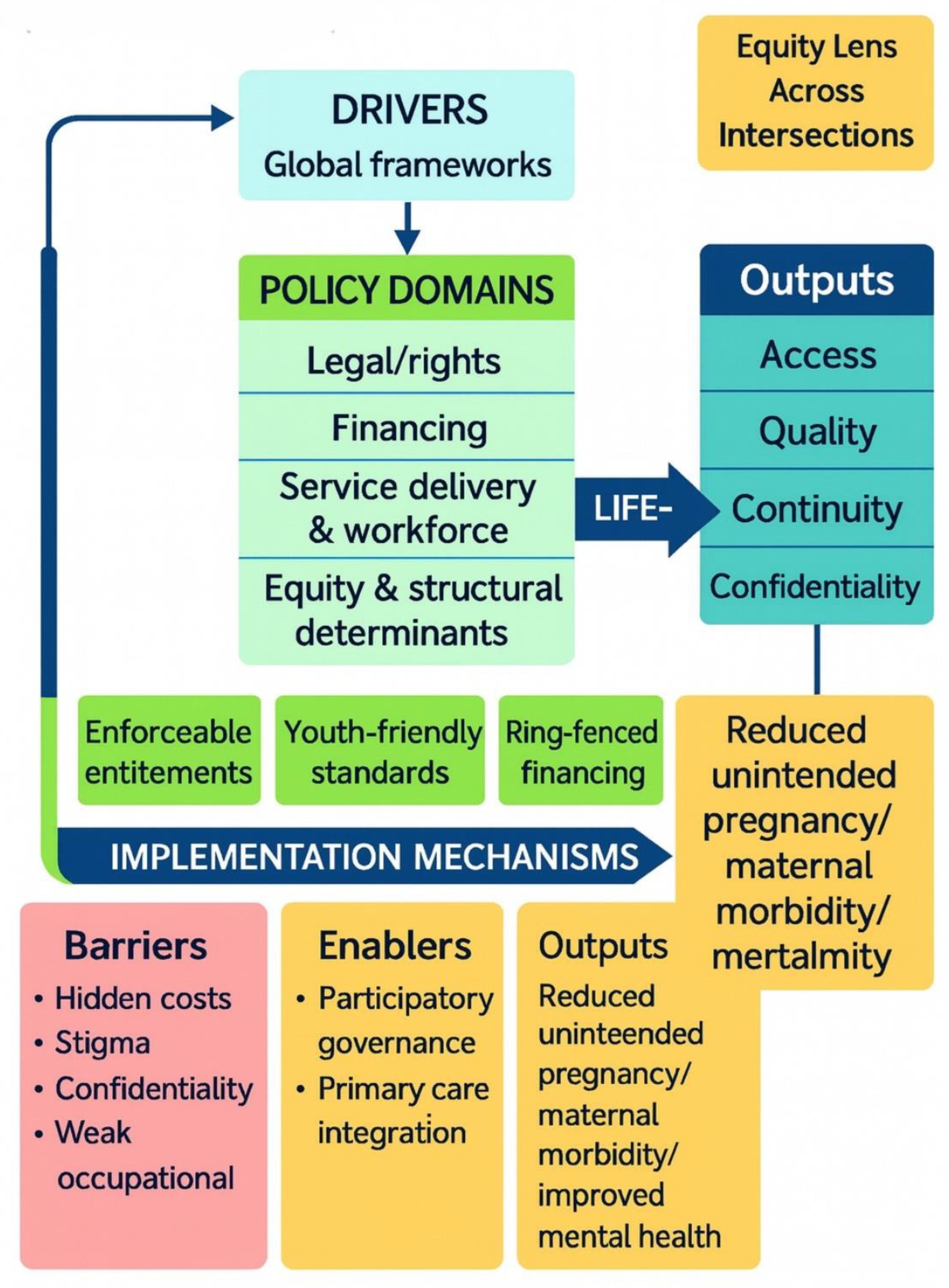
Background: Adolescents and young women represent a critical population in global health policy, yet their needs are often subsumed under broader maternal health agendas. While international frameworks such as CEDAW, the ICPD Programme of Action, the Beijing Platform for Action, and the Sustainable Development Goals have emphasized equity and rights, their translation into adolescent- and youth-sensitive policy remains inconsistent. Methods: We conducted a systematic review of 48 national and international women’s health policies and frameworks published from the 1990s to 2020s, following PRISMA 2020 guidelines. Documents were mapped for contextual features and thematically analyzed to identify patterns in financing, service delivery, equity, and adolescent/youth health priorities. Results: Policies reflected an evolution from maternal survival toward rights-based and life-course approaches, shaped by global frameworks. High-income countries integrated equity and adolescent rights more explicitly, while low- and middle-income countries were constrained by donor-driven priorities and limited fiscal space. Across contexts, adolescents and young women were inconsistently prioritized—acknowledged in some cases (e.g., Sri Lanka, Ghana, Australia) but rarely operationalized into enforceable protections, dedicated financing, or adolescent-friendly services. Persistent barriers included hidden costs, stigma, confidentiality gaps, and weak accountability mechanisms. Conclusion: Despite progress in global commitments, adolescents and young women remain underrepresented and underserved in health policies, in part because their health needs are not sufficiently distinguished. Strengthening adolescent health requires enforceable entitlements, ring-fenced financing, youth-friendly service standards, and participatory governance. Without these measures, policies risk remaining symbolic rather than transformative, leaving adolescents vulnerable to preventable health risks and inequities.
Keywords:
Introduction
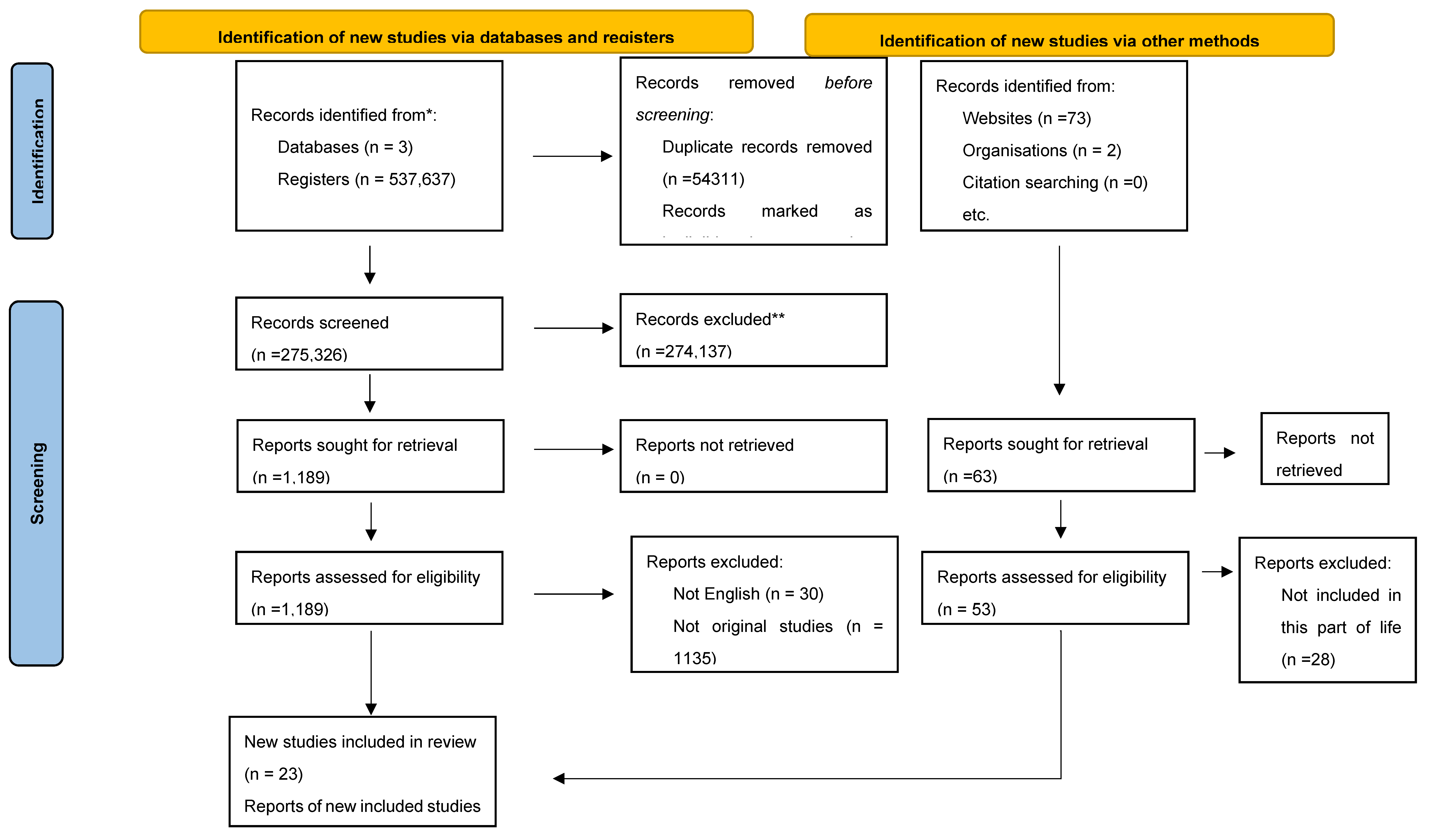
Methods
Search Strategy
Study Selection and Data Extraction
Quality Assessment
Data Analysis
Results
Overview of Included Policies

| Theme | Contextual Evidence | Findings / Patterns | Implications for Adolescents & Young Women |
|---|---|---|---|
| Legal & Policy Frameworks | Spain’s Organic Law (2004) vs. Brazil’s Maria da Penha (2006); Tanzania’s donor-driven 1992 Population Policy; Australia’s 2020–2030 SDG-aligned strategy. | Shift from maternal/child focus to rights-based life-course policies; donor-driven adoption in LMICs often narrowed to fertility control. | Adolescents are acknowledged in some policies (Sri Lanka 1998, Ghana 2014, Australia 2020) but rarely operationalised into enforceable protections. |
| Financing & Coverage | Ghana’s free delivery exemptions showed both equity gains and collapse under debt; Nigeria’s Saving One Million Lives tied funding to performance; Buenos Aires decentralised safe abortion, cutting maternal mortality. | Fee removal and RBF increased utilisation, but donor dependence and hidden costs undermined sustainability. | Adolescents remain highly sensitive to transport costs, informal fees, and mistrust of facilities—often deterring them from early or preventive care. |
| Service Delivery & Workforce | Buenos Aires abortion decentralisation; Sri Lanka MCH life-course expansion; ACEP (U.S.) early pregnancy guideline modernisation. | Nurses/midwives central; decentralised services widened reach; continuity and adolescent confidentiality were weak. | Adolescents often faced stigma, lack of privacy, and inadequate youth-friendly training among providers, deterring service use. |
| Equity & Structural Determinants | WHO 2018 migrant guidance (refugee girls); Baltimore trauma-informed care (post–Freddie Gray); Australia equity focus (Indigenous, rural, LBTI). | Increasing recognition of violence, trauma, migration, and identity-based inequities, though stronger in HICs than LMICs. | Marginalised adolescents face compounded vulnerabilities (violence, poverty, migration). Few policies operationalised equity into targeted, youth-focused programmes. |
| Adolescent & Youth Health | Sri Lanka (1998, 2012), Ghana (2014), Australia (2020), and the WHO migrant guidance. | Youth-specific services are still rare, often framed as behavioural prevention. | Confidentiality gaps, provider stigma, and lack of youth participation undermine rights-based delivery; adolescents remain the least prioritised despite demographic significance. |
Combined Contextual and Thematic Analysis
Policy Drivers and Global Influences
Financing and Health System Capacity
Service Delivery Models and Health Workforce
Equity Considerations
Adolescent and Young Women’s Health
Narrative Synthesis for Adolescents and Young Women
Discussion
Interpretation of Principal Findings
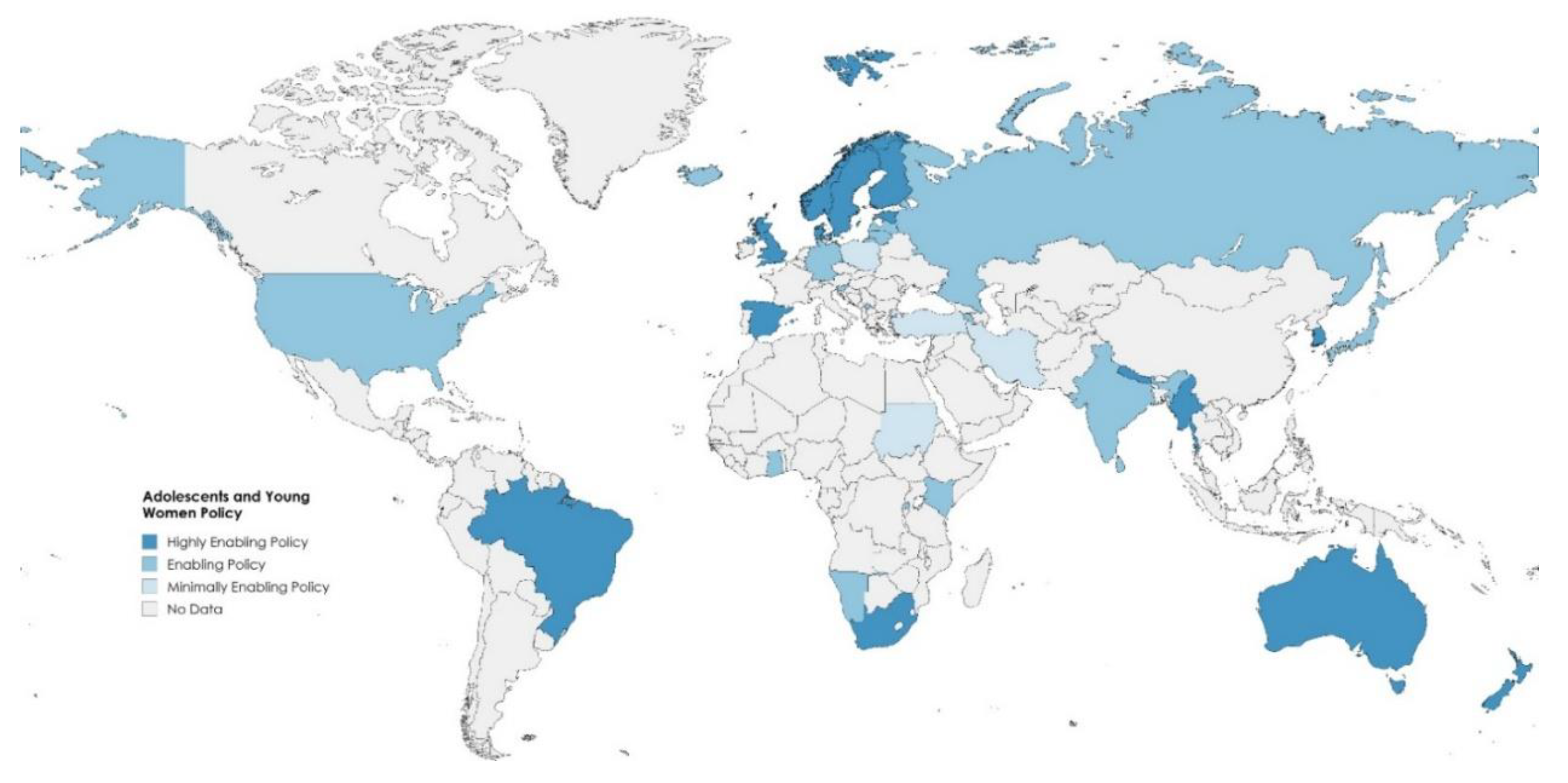
Regional Contrasts
Comparison with Prior Policy Trajectories
Implications for Adolescents and Young Women
| Feature | Explanation | Recommendations |
|---|---|---|
| Clear entitlements | Adolescents require explicit rights to free, confidential contraception, safe abortion, post-violence care, and mental health services. Without enforceable entitlements, services are inconsistently provided and easily deprioritized in budget cycles. | Legally codify adolescent entitlements in national regulations and provider contracts; include grievance redress mechanisms at the facility level; link facility accreditation to compliance with confidentiality and rights standards. |
| Youth-friendly service standards | Standards such as private counseling rooms, opt-out chaperone policies, adolescent-only clinic hours, and provider training for non-judgmental care directly improve care-seeking, confidentiality, and satisfaction. | Mainstream youth-friendly protocols into primary care; create national accreditation for adolescent-friendly facilities; include stigma reduction in continuing medical education. |
| Dedicated adolescent funding | In LMICs, adolescent programs are often diluted during budget execution, leaving young women dependent on under-resourced maternal health frameworks. Dedicated funding protects adolescent priorities from being absorbed into broader maternal programs. | Ring-fence funds for adolescent SRH services; introduce adolescent-specific performance indicators in financing contracts (e.g., % of adolescents accessing contraception or mental health services). |
| Youth participation in governance | Adolescents are often recipients but not co-creators of policy. Participatory mechanisms—youth councils, peer navigators, scorecards—ensure services reflect lived realities and strengthen accountability. | Institutionalize youth representation in health policy governance; provide funding for youth-led monitoring; expand peer-support models integrated into national systems. |
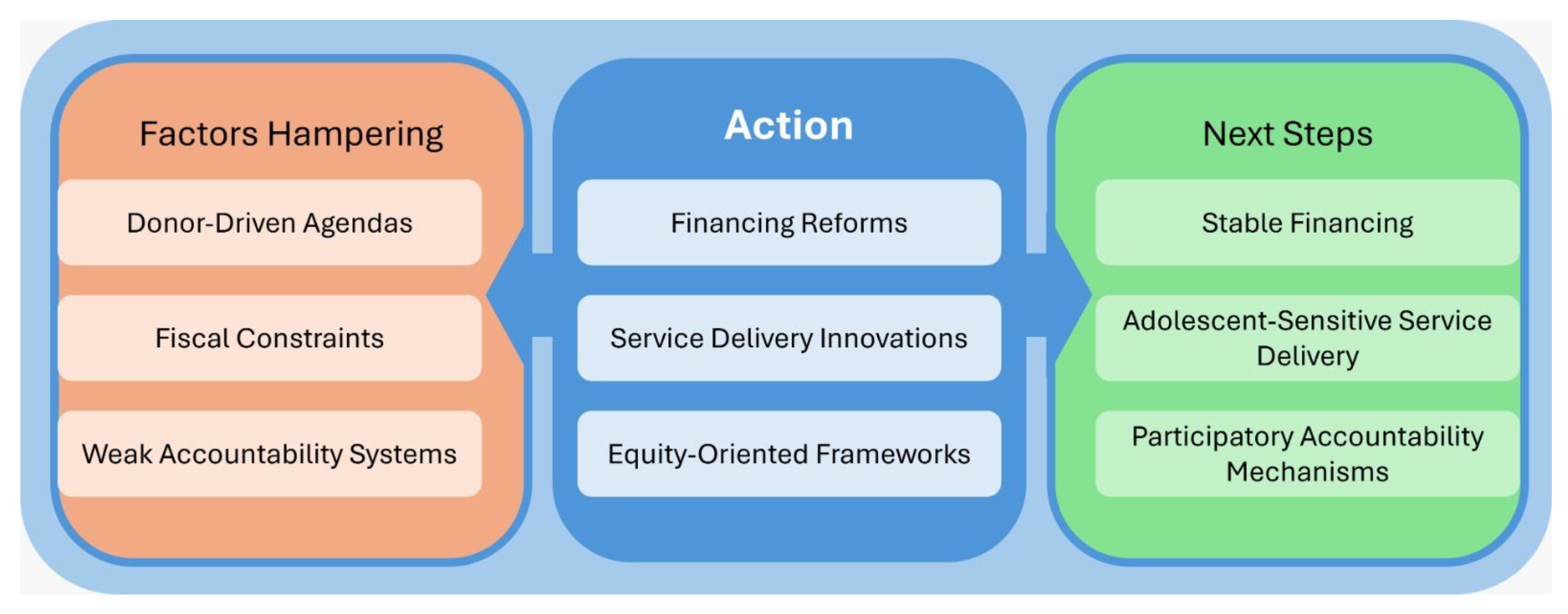
Financing and Delivery: From Access to Assurance
Equity and Intersectionality: From Recognition to Design
Measurement and Accountability
Practice and Policy Implications
Research and Evaluation Priorities
Conclusions
Supplementary Materials
Funding
Conflicts of interest
Availability of data and material
Code availability
Author contributions
Ethics approval
Consent to participate
Consent for publication
Acknowledgements
References
- Remme M, Vassall A, Fernando G, Bloom DE. Investing in the health of girls and women: a best buy for sustainable development. BMJ 2020, 369, m1175. [Google Scholar] [CrossRef]
- Schubert KG, Bird CE, Kozhimmanil K, Wood SF. To Address Women’s Health Inequity, It Must First Be Measured. Health Equity 2022, 6, 881–6. [Google Scholar] [CrossRef]
- World Health Organization. platform.who.int. 2023. Global Strategy for Women’s, Children’s and Adolescents’ Health Data Portal. Available online: https://platform.who.int/data/maternal-newborn-child-adolescent-ageing/global-strategy-data.
- Morris JL, Rushwan H. Adolescent sexual and reproductive health: The global challenges. Int J Gynecol Obstet 2015, 131, S40–2. [Google Scholar]
- Mehta SD, Seeley J. Grand Challenges in Adolescent Sexual and Reproductive Health. Front Reprod Health. 2020, 2. [Google Scholar]
- INFORMATION SERIES ON SEXUAL AND REPRODUCTIVE HEALTH AND RIGHTS UPDATED 2020 ADOLESCENTS [Internet]. Available online: https://www.ohchr.org/sites/default/files/Documents/Issues/Women/WRGS/SexualHealth/INFO_Adolescents_WEB.pdf (accessed on 1 January 2025).
- Michaels Aibangbee, Sowbhagya Micheal, Pranee Liamputtong, Rashmi Pithavadian, Hossain SZ, Mpofu E, et al. Barriers to Sexual and Reproductive Health and Rights of Migrant and Refugee Youth: An Exploratory Socioecological Qualitative Analysis. Youth 2024, 4, 1538–66. [Google Scholar] [CrossRef]
- Bratislava, S. A UNFPA Strategy for Gender Mainstreaming in Areas of Conflict and Reconstruction [Internet]. 2002. Available online: https://www.unfpa.org/sites/default/files/pub-pdf/impact_conflict_women.pdf.
- Manar Shalak, Markson F, Manoj Nepal. Gender-Based Violence and Women Reproductive Health in War Affected Area. Korean J Fam Med 2024, 45, 12–7. [Google Scholar] [CrossRef] [PubMed]
- Bishwajit G, Sarker S, Yaya S. Socio-cultural aspects of gender-based violence and its impacts on women’s health in South Asia. F1000Research 2016, 5, 802. [Google Scholar] [CrossRef]
- United Nations. United Nations. 2025. The 17 Sustainable Development Goals. Available online: https://sdgs.un.org/goals.
- www.unfpa.org [Internet]. 2014. Adolescent sexual and reproductive health. Available online: https://www.unfpa.org/resources/adolescent-sexual-and-reproductive-health.
- World Health Organization. World Health Organization. World Health Organization; 2025. Adolescent Health. Available online: https://www.who.int/health-topics/adolescent-health#tab=tab_1.
- Loveless, G. Ballard Brief. 2025. Ballard Brief. Available online: https://ballardbrief.byu.edu/issue-briefs/barriers-to-adequate-healthcare-for-women-in-the-united-states.
- Hopkins J, Narasimhan M, Aujla M, Silva R, Mandil A. The importance of insufficient national data on sexual and reproductive health and rights in international databases. EClinicalMedicine 2024, 70, 102554–102554. [Google Scholar] [CrossRef]
- Alam N, Merry L, Browne JL, Nahar Q. Editorial: Adolescent sexual and reproductive health challenges in low-income settings. Front Public Health. 2023, 11. [Google Scholar]
- www.unicef.org [Internet]. 2020. Early marriage and its devastating effects. Available online: https://www.unicef.org/southsudan/stories/early-marriage-and-its-devastating-effects.
- Chandra-Mouli V, Akwara E. Improving access to and use of contraception by adolescents: What progress has been made, what lessons have been learned, and what are the implications for action? Best Pract Res Clin Obstet Gynaecol [Internet] 2020, 66. [Google Scholar]
- Zangeneh Jolovi S, Tarrahi MJ, Safdari Dehsheshmeh F, Nekuei NS. Barriers to Sexual Health Education for Female Adolescents in Schools from Health Care Providers’ perspective. J Midwifery Reprod Health 2023, 11, 3694–703. [Google Scholar]
- Cumpston M, Li T, Page MJ, Chandler J, Welch VA, Higgins JP, et al. Updated guidance for trusted systematic reviews: a new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst Rev [Internet] 2021, 10. [Google Scholar]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an Updated Guideline for Reporting Systematic Reviews. Int J Surg 2021, 88, 105906. [Google Scholar] [CrossRef]
- Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred Reporting Items for Systematic Reviews and meta-analyses: the PRISMA Statement. PLoS Med [Internet] 2009, 6. [Google Scholar]
- Tyndall, J. AACODS Checklist [Internet]. Adelaide, Australia: Flinders University; 2010. Available online: https://dspace.flinders.edu.au/xmlui/handle/2328/3326.
- United Nations. OHCHR. United Nations; 1979. Convention on the Elimination of All Forms of Discrimination against Women New York, 18 December 1979. Available online: https://www.ohchr.org/en/instruments-mechanisms/instruments/convention-elimination-all-forms-discrimination-against-women.
- UNFPA. www.unfpa.org. 2014. International Conference on Population and Development Programme of Action. Available online: https://www.unfpa.org/publications/international-conference-population-and-development-programme-action.
- UN Women. UN Women. 2015. Beijing Declaration and Platform for Action, Beijing +5 Political Declaration and Outcome. Available online: https://www.unwomen.org/en/digital-library/publications/2015/01/beijing-declaration.
- Population and Reproductive Health Policy [Internet]. Ministry of Health, Indigenous Medicine in 1998; 1998. Available online: https://www.health.gov.lk/wp-content/uploads/2022/10/3_Population-and-Reproductive-1.pdf.
- National Maternal and Child Health Policy Sri Lanka [Internet]. 2012. Available online: https://www.aidscontrol.gov.lk/images/publications/national_maternal_and_child_health_policy.pdf (accessed on 1 January 2025).
- National Reproductive Health Service Policy and Standards [Internet]. Republic of Ghana; 2014. Available online: https://platform.who.int/docs/default-source/mca-documents/policy-documents/policy/gha-cc-10-01-policy-2014-eng-national-reproductive-health-service-policy-and-standards.pdf.
- Australian Government Department of Health. Australian Government Department of Health. 2021. National Women’s Health Strategy 2020–2030. Available online: https://www.health.gov.au/resources/publications/national-womens-health-strategy-2020-2030.
- Improving the health care of pregnant refugee and migrant women and newborn children [Internet]. 2018. Available online: https://iris.who.int/bitstream/handle/10665/342289/9789289053815-eng.pdf?sequence=1&isAllowed=y.
- Richey, LA. Women’s Reproductive Health & Population Policy: Tanzania. Rev Afr Polit Econ 2003, 30, 273–92. [Google Scholar]
- Professor David Ofori-Adjei. Ghana’s Free Delivery Care Policy. Ghana Med J 2007, 41, 94. [Google Scholar]
- National Medical Standard For Reproductive Health Volume I: Contraceptive Services Government of Nepal Ministry of Health and Population Family Welfare Division [Internet]. 2020. Available online: https://nepal.unfpa.org/sites/default/files/pub-pdf/national_medical_standard-_final.pdf.
- Public Health Agency of Sweden. National Strategy for Sexual and Reproductive Health and Rights (SRHR) [Internet]. Solna & Östersund, Sweden; 2022. Available online: https://www.folkhalsomyndigheten.se/contentassets/5ced6a64b90f44ccb0dc56564e701ea1/national-strategy-sexual-reproductive-health-rights-srhr.pdf.
- World Bank [Internet]. World Bank Project : Nigeria - Program to Support Saving One Million Lives - P146583. Available online: https://projects.worldbank.org/en/projects-operations/project-detail/P146583.
- Matía MG, Trumper EC, Fures NO, Orchuela J. A replication of the Uruguayan model in the province of Buenos Aires, Argentina, as a public policy for reducing abortion-related maternal mortality. Int J Gynecol Obstet. 2016, 134. [Google Scholar]
- Maternal Newborn and Child Health Strategic Plan (2018-2024) [Internet]. 2018. Available online: https://www.moh.gov.rw/fileadmin/user_upload/Moh/Publications/Strategic_Plan/Rwanda_MNCH_StrategicPlan_June_costed_v2Draft.pdf.
- Hahn SA, Promes SB, Brown MD, Brown MD, Byyny R, Diercks DB, et al. Clinical Policy: Critical Issues in the Initial Evaluation and Management of Patients Presenting to the Emergency Department in Early Pregnancy. Ann Emerg Med 2017, 69, 241–250.e20. [Google Scholar] [CrossRef]
- Reproductive health policy [Internet]. Ministry of Health, Republic of the Fiji Islands.; Available online: https://www.health.gov.fj/wp-content/uploads/2014/09/1_Reproductive-Health-Policy.pdf.
- Patel, A. Unesco.org. 2000. Reproductive Health, Gender & Rights in Mongolia. Available online: https://healtheducationresources.unesco.org/sites/default/files/resources/14774.pdf.
- Bravo M del MP, Martínez PA, Ruiz IJ. Public Policies, Nursing Role and Health Programs Against Gender Violence. Comparative Study Spain - Brazil. Procedia - Soc Behav Sci 2017, 237, 758–64. [Google Scholar] [CrossRef]
- Tuck SG, Summers AC, Bowie J, Fife-Stallworth D, Alston C, Hayes S, et al. B’More Fit for Healthy Babies: Using Trauma-Informed Care Policies to Improve Maternal Health in Baltimore City. Womens Health Issues 2017, 27, S38–45. [Google Scholar] [CrossRef] [PubMed]
- WHO | Regional Office for Africa [Internet]. National Reproductive, Maternal, Newborn, Child and Adolescent Health (RMNCAH) Policy. Available online: https://www.afro.who.int/publications/sierra-leone-national-reproductive-maternal-newborn-child-and-adolescent-health.
- REPRODUCTIVE, MATERNAL, NEWBORN, CHILD AND ADOLESCENT + HEALTH OF AGEING (RMNCAH+A) STRATEGY [Internet]. Ministry of Health, Royal Government of Bhutan; 2025. Available online: https://moh.gov.bt/wp-content/uploads/2025/06/RMNCAHA-Strategy-2025-29.pdf.
- Cooper D, Morroni C, Orner P, Moodley J, Harries J, Cullingworth L, et al. Ten Years of Democracy in South Africa. Reprod Health Matters 2004, 12, 70–85. [Google Scholar] [CrossRef]
- Health.gov.za [Internet]. National Department of Health; 2023. Strategic Plan for Maternal, Newborn, Child and Women’s Health (MNCWH) and Nutrition in South Africa | Department of Health Knowledge Hub. Available online: https://knowledgehub.health.gov.za/elibrary/strategic-plan-maternal-newborn-child-and-womens-health-mncwh-and-nutrition-south-africa.
- KENYA NATIONAL POPULATION POLICY FOR SUSTAINABLE DEVELOPMENT SESSIONAL PAPER NO. 1 OF 2023 ON THE NATIONAL TREASURY AND ECONOMIC PLANNING NATIONAL COUNCIL FOR POPULATION AND DEVELOPMENT. 2023.
- Grossman D, Grindlay K, Burns B. Public funding for abortion where broadly legal. Contraception 2016, 94, 453–60. [Google Scholar] [CrossRef]
- McKee MD, Rubin SE, Campos G, O’Sullivan LF. Challenges of Providing Confidential Care to Adolescents in Urban Primary Care: Clinician Perspectives. Ann Fam Med 2011, 9, 37–43. [Google Scholar] [CrossRef]
- Sawyer SM, Ambresin AE, Bennett KE, Patton GC. A Measurement Framework for Quality Health Care for Adolescents in Hospital. J Adolesc Health 2014, 55, 484–90. [Google Scholar] [CrossRef]
- Arije O, Hlungwani T, Madan J. Key informants’ perspectives on policy- and service-level challenges and opportunities for delivering adolescent and youth-friendly health services in public health facilities in a Nigerian setting. BMC Health Serv Res 2022, 22. [Google Scholar]
- Deogan C, Ferguson J, Stenberg K. Resource Needs for Adolescent Friendly Health Services: Estimates for 74 Low- and Middle-Income Countries. Myer L, editor. PLoS ONE 2012, 7, e51420. [Google Scholar]
- Akseer N, Mehta S, Wigle J, Chera R, Brickman ZJ, Al-Gashm S, et al. Non-communicable diseases among adolescents: current status, determinants, interventions and policies. BMC Public Health 2020, 20. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Who.int. World Health Organization: WHO; 2024. Adolescents: Health risks and solutions. Available online: https://www.who.int/news-room/fact-sheets/detail/adolescents-health-risks-and-solutions.
- Jin M, An Q, Wang L. Chronic conditions in adolescents. Exp Ther Med 2017, 14, 478–82. [Google Scholar] [CrossRef]
- Kruk ME, Lewis TP, Arsenault C, Bhutta ZA, Irimu G, Jeong J, et al. Improving health and social systems for all children in LMICs: structural innovations to deliver high-quality services. The Lancet 2022, 399. [Google Scholar] [CrossRef]
- Newby H, Marsh AD, Moller AB, Adebayo E, Azzopardi PS, Carvajal L, et al. A Scoping Review of Adolescent Health Indicators. J Adolesc Health 2021, 69, 365–74. [Google Scholar] [CrossRef]
- Lule E, Rosen JE, Singh S, Knowles JC, Behrman JR. Nih.gov. The International Bank for Reconstruction and Development / The World Bank; 2020. Adolescent Health Programs. Available online: https://www.ncbi.nlm.nih.gov/books/NBK11778 (accessed on 1 January 2025).
- World Bank. World Bank. 2022. The World Bank in Ghana. Available online: https://www.worldbank.org/en/country/ghana/overview.
- The World Bank. Worldbank.org. 2023. Maternal Mortality Ratio (modeled estimate, per 100,000 Live births) | Data. Available online: https://data.worldbank.org/indicator/SH.STA.MMRT.
- World Health Organization. www.who.int. 2019. Maternal health in Nigeria: generating information for action. Available online: https://www.who.int/news/item/25-06-2019-maternal-health-in-nigeria-generating-information-for-action.
- Patel V, Chatterji S, Chisholm D, Ebrahim S, Gopalakrishna G, Mathers C, et al. Chronic diseases and injuries in India. The Lancet 2011, 377, 413–28. [Google Scholar] [CrossRef]
- Meng Q, Mills A, Wang L, Han Q. What can we learn from China’s health system reform? BMJ 2019, 365, l2349. [Google Scholar] [CrossRef]
- Who.int [Internet]. 2025 Chapter 5. Available online: https://www.who.int/initiatives/global-accelerated-action-for-the-health-of-adolescent/aa-ha%21-guidance-2d-edition/chapter-5 (accessed on 1 January 2025).
- Corley AG, Sprockett A, Montagu D, Chakraborty NM. Exploring and Monitoring Privacy, Confidentiality, and Provider Bias in Sexual and Reproductive Health Service Provision to Young People: A Narrative Review. Int J Environ Res Public Health 2022, 19, 6576. [Google Scholar] [CrossRef] [PubMed]
- Bou-Karroum L, Iaia DG, El-Jardali F, Abou Samra C, Salameh S, Sleem Z, et al. Financing for equity for women’s, children’s and adolescents’ health in low- and middle-income countries: A scoping review. Singh A, editor. PLOS Glob Public Health 2024, 4, e0003573. [Google Scholar]
- Women’s Health Strategy for England. August 2022, 2022.
- Briozzo, L. From risk and harm reduction to decriminalizing abortion: The Uruguayan model for women’s rights. Int J Gynecol Obstet. 2016, 134, S3–6. [Google Scholar] [CrossRef]
- Ganchimeg T, Ota E, Morisaki N, Laopaiboon M, Lumbiganon P, Zhang J, et al. Pregnancy and childbirth outcomes among adolescent mothers: a World Health Organization multicountry study. BJOG Int J Obstet Gynaecol. 2014, 121 (Suppl 1), 40–8. [Google Scholar] [CrossRef]
- Richardson E, Birn AE. Sexual and reproductive health and rights in Latin America: an analysis of trends, commitments and achievements. Reprod Health Matters 2011, 19, 183–96. [Google Scholar] [CrossRef] [PubMed]
- Sidamo NB, Kerbo AA, Gidebo KD, Wado YD. Socio-Ecological Analysis of Barriers to Access and Utilization of Adolescent Sexual and Reproductive Health Services in Sub-Saharan Africa: A Qualitative Systematic Review. Open Access J Contracept 2023, 14, 103–18. [Google Scholar] [CrossRef]
- Leite SP, Pellechio A, Zanforlin L, Begashaw G, Fabrizio S, Harnack J. www.imf.org. Ghana: Economic Development in a Democratic Environment--IMF Occasional Paper No. 199. Available online: https://www.imf.org/external/pubs/nft/op/199/.
- www.unfpa.org [Internet]. UNFPA - United Nations Population Fund. Available online: https://www.unfpa.org/data/dashboard/adolescent-youth.
- Health for the World’s Adolescents [Internet]. Available online: https://iris.who.int/bitstream/handle/10665/112750/WHO_FWC_MCA_14.05_eng.pdf.
- Patton GC, Sawyer SM, Santelli JS, Ross DA, Afifi R, Allen NB, et al. Our future: a Lancet commission on adolescent health and wellbeing. Lancet Lond Engl 2016, 387, 2423–78. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. www.who.int. 2023. Trends in maternal mortality 2000 to 2020: estimates by WHO, UNICEF, UNFPA, World Bank Group and UNDESA/Population Division. Available online: https://www.who.int/publications/i/item/9789240068759.
- Moraes AN, Likwa RN, Nzala SH. A retrospective analysis of adverse obstetric and perinatal outcomes in adolescent pregnancy: the case of Luapula Province, Zambia. Matern Health Neonatol Perinatol 2018, 4. [Google Scholar]
- Laurenzi CA, Gordon S, Abrahams N, du Toit S, Bradshaw M, Brand A, et al. Psychosocial Interventions Targeting Mental Health in Pregnant Adolescents and Adolescent parents: a Systematic Review. Reprod Health [Internet] 2020, 17, https://link.springer.com/article/10.1186/s12978-020-00913–y. [Google Scholar]
- Agampodi SB, Agampodi TC, UKD P. Adolescents perception of reproductive health care services in Sri Lanka. BMC Health Serv Res 2008, 8. [Google Scholar]
- Hewage, P. Sexual and Reproductive Health Research in Sri Lanka: Current Status, Challenges and Directions (2010-2019). Sri Lanka J Soc Sci 2020, 43, 113. [Google Scholar] [CrossRef]
- Savaglio M, O’Donnell R, Hatzikiriakidis K, Vicary D, Skouteris H. The Impact of Community Mental Health Programs for Australian Youth: A Systematic Review. Clin Child Fam Psychol Rev 2022, 25, 573–90. [Google Scholar] [CrossRef]
- World Health Organization. World Health Organization. 2024. Adolescent pregnancy. Available online: https://www.who.int/news-room/fact-sheets/detail/adolescent-pregnancy.
- Group, WB. World Bank. World Bank Group; 2025. Ghana’s Economy Shows Resilience Amid a Challenging Environment. Available online: https://www.worldbank.org/en/news/press-release/2025/08/14/ghana-economy-shows-resilience-amid-a-challenging-environment.
- Akweongo P, Chatio ST, Owusu R, Salari P, Tedisio F, Aikins M. How does it affect service delivery under the National Health Insurance Scheme in Ghana? Health providers and insurance managers perspective on submission and reimbursement of claims. Vaingankar JA, editor. PLOS ONE 2021, 16, e0247397. [Google Scholar]
- Laar AS, Asare M, Dalinjong PA. What alternative and innovative domestic methods of healthcare financing can be explored to fix the current claims reimbursement challenges by the National Health Insurance Scheme of Ghana? Perspectives of health managers. Cost Eff Resour Alloc 2021, 19. [Google Scholar]
- www.who.int [Internet]. Promoting the health of refugees and migrants: Resolution, Seventieth World Health Assembly. Available online: https://www.who.int/publications/i/item/WHA70.15.
- Michaels Aibangbee, Sowbhagya Micheal, Mapedzahama V, Pranee Liamputtong, Rashmi Pithavadian, Syeda Zakia Hossain, et al. Migrant and Refugee Youth’s Sexual and Reproductive Health and Rights: A Scoping Review to Inform Policies and Programs. Int J Public Health. 2023, 68. [Google Scholar]
- Schmidt NC, Fargnoli V, Epiney M, Irion O. Barriers to reproductive health care for migrant women in Geneva: a qualitative study. Reprod Health 2018, 15. [Google Scholar]
- Castleton P, Chaudhry AS, Negin Damabi, Salima Meherali, Lassi ZS. Crossing Borders: SRH Challenges Among Immigrant and Minority Adolescents. Int J Environ Res Public Health 2025, 22, 1101–1101. [Google Scholar] [CrossRef]
- Nalwadda G, Namutebi M, Volgsten H. Health care providers’ perceptions of family planning and contraception education for adolescents in Kampala, Uganda – A qualitative study. Sex Reprod Healthc 2019, 21, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Ezenwaka U, Mbachu C, Ezumah N, Eze I, Agu C, Agu I, et al. Exploring factors constraining utilization of contraceptive services among adolescents in Southeast Nigeria: an application of the socio-ecological model. BMC Public Health 2020, 20. [Google Scholar] [CrossRef]
- Taiwo MO, Oyekenu O, Hussaini RA. Understanding how social norms influence access to and utilization of adolescent sexual and reproductive health services in Northern Nigeria. Front Sociol. 2023, 8. [Google Scholar]
- Tadele Emagneneh, Mulugeta C, Belay Susu, Negesse Belayneh, Tsegaye D. Comparing adverse maternal outcomes among adolescent and adult women in North Wollo Zone governmental hospitals, northern Ethiopia. Front Glob Women Health. 2025, 6. [Google Scholar]
- Olausson PO, Haglund B, Weitoft GR, Cnattingius S. Guttmacher Institute. 2005. Teenage Childbearing and Long-Term Socioeconomic Consequences: A Case Study in Sweden. Available online: https://www.guttmacher.org/journals/psrh/2001/03/teenage-childbearing-and-long-term-socioeconomic-consequences-case-study.
- Komal Abdul Rahim, Egglestone NJ, Tsagareli IG, Usmani W, Salima Meherali, Lassi ZS. Mental health outcomes beyond the post-partum period among adolescent mothers: a systematic review and meta-analysis. Health Psychol Behav Med 2024, 12. [Google Scholar]
- Busse CE, Tumlinson K, Senderowicz L. Contraceptive Use and Discontinuation Among Adolescent Women in 55 Low- and Middle-Income Countries. Demography. 2025.
- Smylie J, Firestone M. Back to the basics: Identifying and addressing underlying challenges in achieving high quality and relevant health statistics for Indigenous populations in Canada. Stat J IAOS 2015, 31, 67–87. [Google Scholar] [CrossRef]
- Trudgett S, Griffiths K, Farnbach S, Shakeshaft A. A framework for operationalising Aboriginal and Torres Strait Islander data sovereignty in Australia: Results of a systematic literature review of published studies. eClinicalMedicine 2022, 45, 101302. [Google Scholar] [CrossRef] [PubMed]
- Khaki JJ, Molenaar J, Karki S, Olal E, Straneo M, Mosuse MA, et al. When health data go dark: the importance of the DHS Program and imagining its future. BMC Med [Internet]. 2025, 23. Available online: https://pmc.ncbi.nlm.nih.gov/articles/PMC12023666/ (accessed on 1 January 2025).
- Morgan R, Garrison-Desany H, Hobbs AJ, Wilson E. Strengthening effectiveness evaluations through gender integration to improve programs for women, newborn, child, and adolescent health. Glob Health Action. 2022, 15. [Google Scholar]
- Ambresin AE, Bennett K, Patton GC, Sanci LA, Sawyer SM. Assessment of Youth-Friendly Health Care: A Systematic Review of Indicators Drawn From Young People’s Perspectives. J Adolesc Health 2013, 52, 670–81. [Google Scholar] [CrossRef]
- Adolescent friendly health services: supervisory/self-assessment checklist and user’s guide [Internet]. World Health Organization; 2021. (Who.int). Available online: https://www.who.int/publications/i/item/9789290228325.
- Wai D, Goi A, Salm MF, Juma Kupewa, Getrud Mollel, Yassin Mninda, et al. Through the looking glass: empowering youth community advisory boards in Tanzania as a sustainable youth engagement model to inform policy and practice. Front Public Health. 2024, 12. [Google Scholar]
- Squires F, Martin Hilber A, Cordero JP, Boydell V, Portela A, Lewis Sabin M, et al. Social accountability for reproductive, maternal, newborn, child and adolescent health: A review of reviews. Munro-Kramer ML, editor. PLOS ONE 2020, 15, e0238776. [Google Scholar]
- Rich C, Goncalves A, Guardiani M, O’Donnell E, Strzelecki J. Teen Advisory Committee: lessons learned by adolescents, facilitators, and hospital staff. Pediatr Nurs 2014, 40, 289–96. [Google Scholar]
- Choudhary M, Kukreja R, Chutani N. The Hindu. 2024. Gap between allocations for health, outcomes in States. Available online: https://www.thehindu.com/opinion/op-ed/gap-between-allocations-for-health-outcomes-in-states/article68606390.ece.
- Fox E, Reyna A, Malcolm NM, Rosmarin RB, Zapata LB, Frederiksen BN, et al. Client Preferences for Contraceptive Counseling: A Systematic Review. Am J Prev Med 2018, 55, 691–702. [Google Scholar] [CrossRef]
- Srivastava A, Singh D, Montagu D, Bhattacharyya S. Putting women at the center: a review of Indian policy to address person-centered care in maternal and newborn health, family planning and abortion. BMC Public Health 2017, 18. [Google Scholar] [CrossRef]
- Napit K, Shrestha KB, Magar SA, Paudel R, Thapa B, Dhakal BR, et al. Factors associated with utilization of adolescent-friendly services in Bhaktapur district, Nepal. J Health Popul Nutr 2020, 39. [Google Scholar]
- Jain N, Bahl D, Mehta R, Bassi S, Sharma K, Arora M. Progress and challenges in implementing adolescent and school health programmes in India: a rapid review. BMJ Open 2022, 12, e047435. [Google Scholar] [CrossRef]
- Taylor EM, Hayman R, Crawford F, Jeffery P, Smith J. The Impact of Official Development Aid on Maternal and Reproductive Health Outcomes: A Systematic Review. Middleton P, editor. PLoS ONE 2013, 8, e56271. [Google Scholar]
- Ungar, L. AP News. 2024. Maternal mortality review panels are in the spotlight. Here’s what they do. Available online: https://apnews.com/article/maternal-mortality-cdc-abortion-georgia-texas-idaho-10dae96d52503709f4beb698a3f12db5.
- Kabue MM, Palestra F, Katwan E, Moran AC. Availability of priority maternal and newborn health indicators: Cross-sectional analysis of pregnancy, childbirth and postnatal care registers from 21 countries. Faizi N, editor. PLOS Glob Public Health 2023, 3, e0000739. [Google Scholar]
- Bauserman M, Thorsten VR, Nolen TL, Patterson J, Lokangaka A, Tshefu A, et al. Maternal Mortality in Six Low and lower-middle Income Countries from 2010 to 2018: Risk Factors and Trends. Reprod Health [Internet]. 2020, 17, https://reproductive-health-journal.biomedcentral.com/articles/10.1186/s12978-020-00990–z. [Google Scholar]
- Boerma JT, Sommerfelt AE. Demographic and health surveys (DHS): contributions and limitations. World Health Stat Q Rapp Trimest Stat Sanit Mond 1993, 46, 222–6. [Google Scholar]
- Alatinga KA, Hsu V, Abiiro GA, Kanmiki EW, Gyan EK, Moyer CA. Why “free maternal healthcare” is not entirely free in Ghana: a qualitative exploration of the role of street-level bureaucratic power. Health Res Policy Syst 2024, 22, 142. [Google Scholar] [CrossRef]
- Witter S, Adjei S, Armar-Klemesu M, Graham W. Providing free maternal health care: ten lessons from an evaluation of the national delivery exemption policy in Ghana. Glob Health Action 2009, 2, 1881. [Google Scholar] [CrossRef]
- James N, Lawson K, Acharya Y. Evidence on result-based financing in maternal and child health in low- and middle-income countries: a systematic review. Glob Health Res Policy 2020, 5. [Google Scholar]
- Kemp CG, Jarrett BA, Kwon CS, Song L, Jetté N, Sapag JC, et al. Implementation science and stigma reduction interventions in low- and middle-income countries: a systematic review. BMC Med 2019, 17. [Google Scholar]
- Agumasie Semahegn, Tsegahun Manyazewal, Hanlon C, Getachew E, Bethelhem Fekadu, Assefa E, et al. Challenges for research uptake for health policymaking and practice in low- and middle-income countries: a scoping review. Health Res Policy Syst 2023, 21. [Google Scholar]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



